
Abstract

Introduction
Heart failure remains a highly prevalent condition with poor outcomes. The Canadian Cardiovascular Society has committed to a yearly update of the important issues surrounding the management of this condition. In 2006 the focus was on the diagnosis and management of heart failure. 1 –3 This year's update focuses on prevention of heart failure, management of heart failure during intercurrent illness, treatment of acute decompensated heart failure, and the current and future role of biomarkers in heart failure care. 4 In this summary, we have outlined some of the most relevant aspects of the guidelines for pharmacists. Readers are encouraged to view the entire documents and other materials online at www.hfcc.ca for further details.
Prevention of heart failure
Patients at risk of developing heart failure
Most preventive measures for heart failure parallel those for the most common cause of heart failure, namely, coronary artery disease. Risk factors for the development of heart failure are outlined in Table 1. Recommendations include:
Risk factors for heart failure development 4
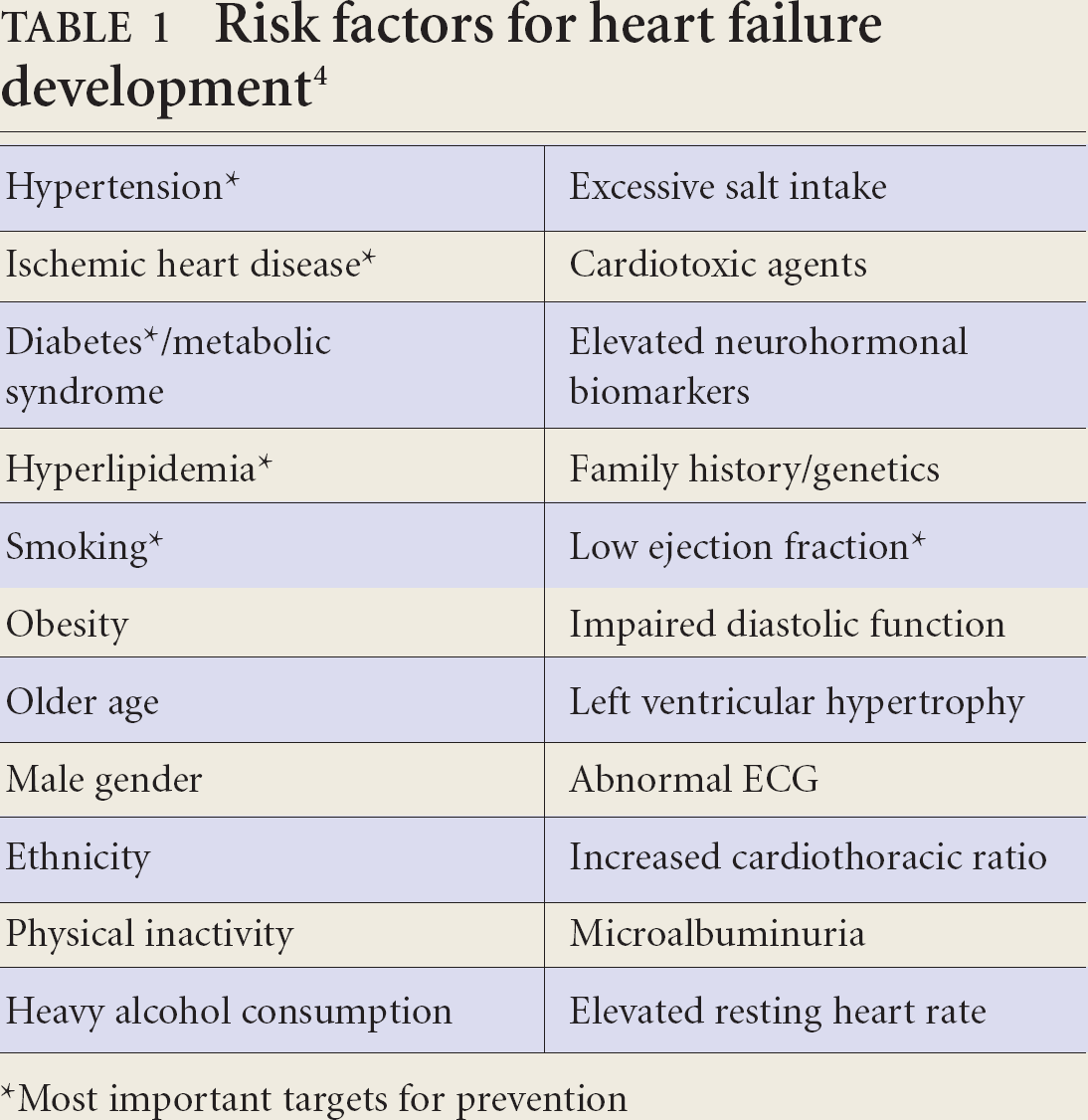
Most important targets for prevention
Clinical assessment in all patients to identify known or potential risk factors for heart failure (e.g., hypertension, ischemic heart disease, diabetes, hyperlipidemia, and smoking) (class I, level C — see Box 1 for information on grading of evidence). All modifiable risk factors for heart failure, including those for coronary artery disease, such as hypertension, diabetes, and hyperlipidemia, should be treated in accordance with current national guidelines (class I, level A). Pharmacists can play a major role in identification and management of cardiovascular risk factors, and these should be routinely assessed in patients at risk.
Patients with asymptomatic left ventricular dysfunction
ACE inhibitors should be used in all asymptomatic patients with left ventricular dysfunction and ejection fraction less than 40% (class I, level A-B) Beta blockers should be considered in all patients with asymptomatic left ventricular dysfunction and ejection fraction less than 40% (class I-IIa, level B-C).
Patients with heart failure and intercurrent illness
The possibility of heart failure increases with advancing age, therefore the presence of other significant medical conditions becomes more likely. Indeed, the average patient with heart failure suffers from 5 or 6 concomitant medical conditions.
Heart failure in the elderly
Elderly or frail heart failure patients who present with acute illness should be assessed for incidence of delirium and, before discharge, cognitive impairment (class IIa, level C).
Heart failure and diabetes
Diabetes is present in more than one-third of patients with heart failure. Elevated blood glucose in patients with heart failure should be treated according to current Canadian Diabetes Association guideline recommendations — aim for a target HbA1C level of 7% or fasting/preprandial blood glucose of 4.4 mmol/L to 7.0 mmol/L (class I, level A). Metformin may be considered a first-line agent for diabetes (concerns over lactic acidosis are likely overstated; however, caution should be taken in patients with creatinine clearance less than 30 mL/min). Thiazolidinediones (glitazones) often cause fluid retention and unstable patients with heart failure should be followed more closely.
Heart failure with renal dysfunction
Renal dysfunction commonly occurs in patients with heart failure and is one of the strongest predictors of poor outcomes.
Heart failure patients with stable renal function (serum creatinine levels less than 200 μmol/L) should receive standard therapy with an ACE inhibitor, ARB, or spironolactone, but monitoring of serum potassium and creatinine levels should be more frequent, especially if combination thearapy is used or in the case of an acute concomitant illness that causes dehydration (class I, level B). In heart failure patients with severe or unstable renal dysfunction (serum creatinine >250 μmol/L), routine use of ACE inhibitors, ARBs or spironolactone is not recommended (class IIa, level C). Patients with heart failure who continue to experience volume overload or increasing serum creatinine levels should be assessed for reversible causes such as concomitant medications (e.g., nonsteroidal anti-inflammatory drugs), hypovolemia, hypotension, urinary tract obstruction, or infection (class I, level C). The indications for the use of digoxin should be re-evaluated in heart failure patients with severe renal dysfunction; the trough digoxin level (at least 8 hours after a dose) should be checked and the dose should be adjusted to maintain a trough level less than 1 nmol/L. For patients with more rapid deterioration in renal function, digoxin should be withheld and re-evaluated once renal function has stabilized (class I, level C).
Grading of evidence 4
Heart failure and acute intercurrent medical illness
Beta blockers should be initiated as soon as possible after diagnosis of heart failure, including during the index hospitalization, provided that the patient is clinically stable. Clinicians should not wait until hospital discharge to start a beta blocker in stabilized patients (class I, level B). Beta blockers should be continued in patients hospitalized with acute heart failure, unless they develop cadiogenic shock, refractory volume overload, or symptomatic bradycardia (class IIa, level C). Beta blockers and ACE inhibitors should be continued at their usual dose during acute intercurrent illness, unless they are not tolerated (class IIa, level C). In a life-threatening complication, beta blockers and ACE inhibitors or ARBs may be discontinued abruptly, but generally, if there is concern about their use, the dose should be decreased by one-half and the patient should be assessed. If the dose is reduced, it should be uptitrated to the previous well-tolerated dose as soon as safely possible (class IIa, level C). In an acute dehydrating illness with risk of worsening renal function, spironolactone should be temporarily withheld because hyperkalemia is more common in this setting (class I, level C). Colchicine should be considered for acute gouty attack in heart failure patients. An oral or intra-articular steroid may also be considered (class IIa, level C).
Acute heart failure
Acute heart failure is a serious condition requiring urgent medical attention. Common presenting symptoms include rapid onset of shortness of breath on minimal effort or lying down, cough, increasing abdominal girth, edema, and fatigue.
Any identified precipitating cause should be promptly corrected when possible (class I, level B). Oxygen should be given initially to all patients presenting with acute heart failure and hypoxia (class I, level C). Intravenous diuretics should be given as first-line therapy for patients with acute heart failure and congestion (class I, level B). Vasodilators should be considered for patients with dyspnea at rest (class I, level C). Positive inotropes should be reserved for patients in cardiogenic shock and/or volume overload with diuretic resistance. This should be used for short-term therapy to stabilize the patient. In hypotensive patients (systolic BP of 90 mmHg), dobutamine is preferred over milrinone (class I, level C). ACE inhibitors are not recommended routinely the first few hours of acute heart failure. They should be introduced when the patient has stabilized (class I, level B). Calcium channel blockers are not recommended in acute heart failure; specifically diltiazem and verapamil are to be avoided in acute heart failure with systolic dysfunction (class III, level B). Diltiazem may be used in acute heart failure with preserved systolic function in the setting of atrial fibrillation with rapid ventricular response (class I, level C).
Pharmacists should be watchful for drug-induced heart failure due to negative inotropes (non-dihydropyridine calcium channel blockers, anti-arrhythmic agents, or during initiation of beta blockers), or drugs causing fluid retention (celecoxib, other NSAIDs, or thiazolidinediones). 5
Conclusions
Heart failure is a complex clinical syndrome and it is best managed through individualized evidence-based medical therapy. This improves patient outcomes but requires a team approach. Pharmacists have a unique role to play in the management of heart failure and are encouraged to get involved with optimizing therapeutics and patient education. Indeed, a recent systematic review of the addition of pharmacist care in patients with heart failure demonstrated an impressive 31% reduction in heart failure hospitalization. 6 Given that heart failure is one of the leading reasons for hospitalization of patients in Canada, there is compelling reason for pharmacists to become more engaged in the management of heart failure.
The treatment recommendations from 2006 have been combined with those for prevention from 2007 to create a new summary algorithm for the management of heart failure (Figure 1). A review of evidence-based drug therapy and target doses for the prevention and treatment of heart failure is outlined in Table 2.
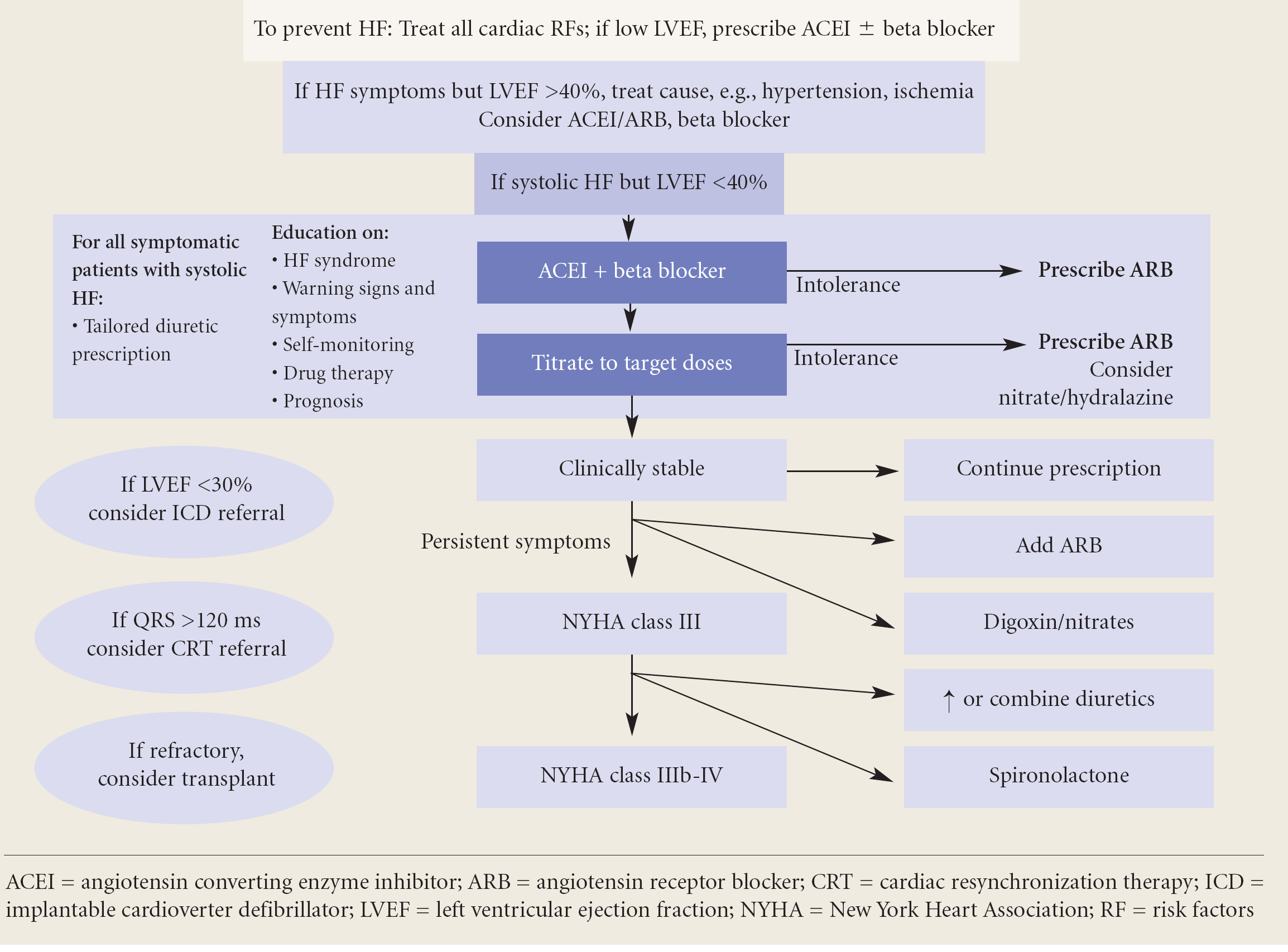
Algorithm for the prevention and treatment of heart failure
Evidence-based drugs and doses for the prevention and treatment of heart failure
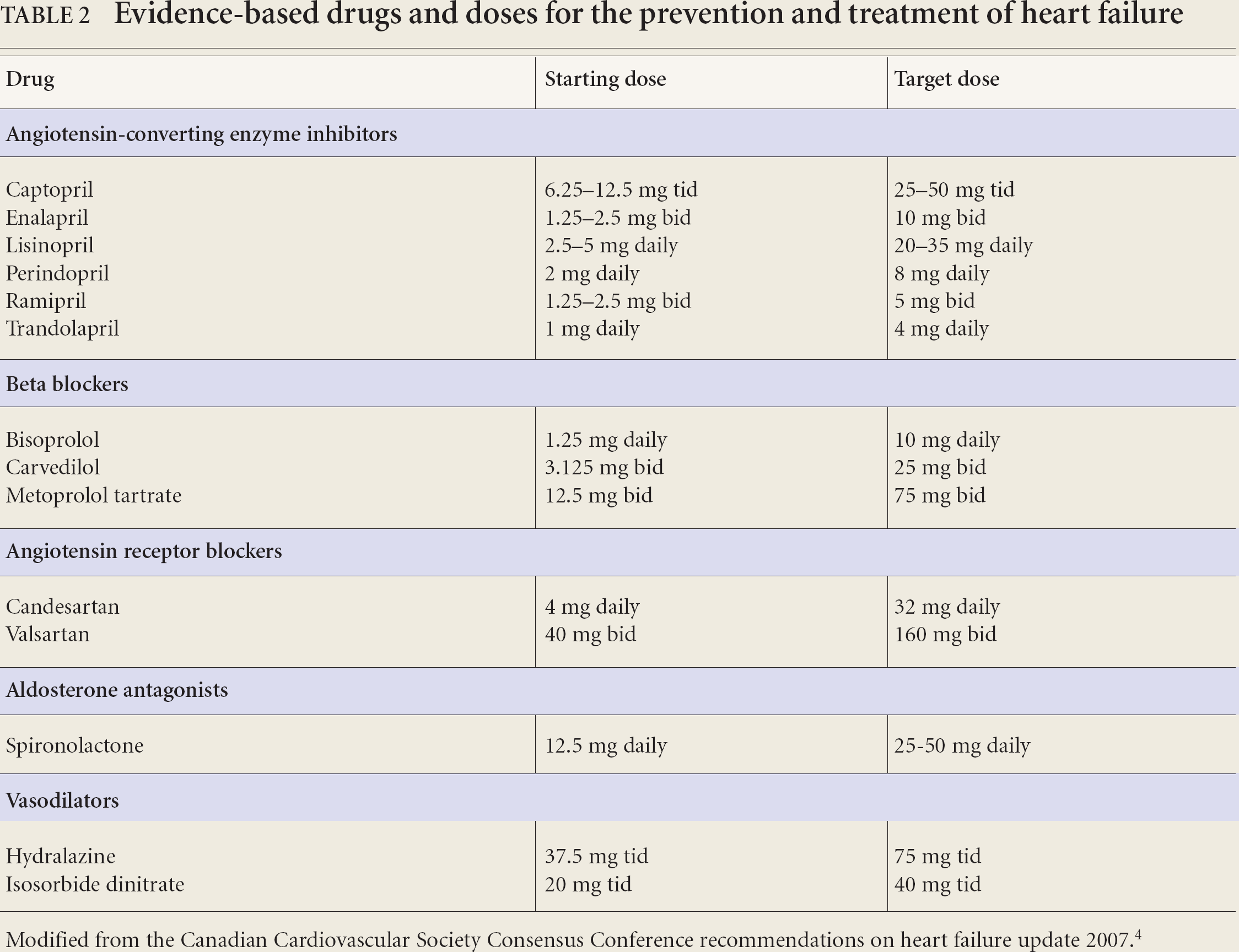
Modified from the Canadian Cardiovascular Society Consensus Conference recommendations on heart failure update 2007. 4
We have committed to providing pharmacists with yearly updates for the management of this rapidly changing field. The 2008 guidelines were released in January 2008. 8 The focus topics include issues relating to transfer of care between institutions and between health care providers, as well as cardiomyopathies.
Footnotes
This information was originally published in and/or adapted from The Canadian Journal of Cardiology 2007; 23(1):21–45.