
Abstract
This Campbell systematic review examines the effectiveness of school-based Mindfulness-based interventions (MBIs) on cognition, behavior, socio-emotional outcomes and academic achievement. The review summarizes 61 studies and synthesizes 35 studies, with a total of 6,207 student participants.
MBIs have a small, statistically significant positive effect on cognitive and socio-emotional outcomes. But there is not a significant effect on behavioral and academic outcomes.
There was little heterogeneity for all outcomes, besides behavioral outcomes, suggesting that the interventions produced similar results across studies on cognitive, socio-emotional and academic outcomes despite the interventions being quite diverse.
Plain language summary
Mindfulness-based interventions in schools have positive effects on cognitive and socio-emotional processes but do not improve behavior and academic achievement
MBIs have a small, positive effect on cognitive and socio-emotional outcomes, but not a significant effect on behavioral and academic outcomes.
The review in brief
The use of mindfulness-based interventions (MBIs) in schools has been on the rise. Schools are using MBI's to reduce student stress and anxiety and improve socio-emotional competencies, student behavior and academic achievement.
MBIs have small, positive effects on cognitive and socio-emotional processes but these effects were not seen for behavioral or academic outcomes. The studies are mostly of moderate to low quality. Therefore, further evidence from independent evaluators is needed to be able to evaluate the effectiveness of this type of intervention.
What did this review study?
With the diverse application and findings of positive effects of mindfulness practices with adults, as well as the growing popularity with the public, MBIs are increasingly being used with youth. Over the past several years, MBIs have received growing interest for use in schools to support socio-emotional development and improve behavior and academic achievement.
This review examines the effects of school-based MBIs on cognitive, behavioral, socio-emotional and academic achievement outcomes with youth in a primary or secondary school setting. MBIs are interventions that use a mindfulness component, broadly defined as “paying attention in a particularly way: on purpose, in the present moment, non-judgmentally”, often with other components, such as yoga, cognitive-behavioral strategies, or relaxation skills training.
What studies are included?
Included studies used a randomized controlled trial, quasi-experimental, single group pre-post test or single subject design and reported at least one of these outcomes: cognition, academic performance, behavior, socio-emotional, and physiological. Study populations include preschool, primary and secondary school students.
A total of 61 studies are included in the review, but only the 35 randomized or quasi-experimental studies are used in the meta-analysis. Most of the studies were carried out in North America, and others in Asia, Europe and Canada. All interventions were conducted in a group format. Interventions ranged in duration (4-28 weeks) and number of sessions (6-125 sessions) and frequency of meetings (once every two weeks to five times a week).
What is the aim of this review?
This Campbell systematic review examines the effectiveness of school-based MBIs on cognition, behavior, socio-emotional outcomes and academic achievement. The review summarizes 61 studies and synthesizes 35 studies, with a total of 6,207 student participants.
What are the main results in this review?
MBIs have a small, statistically significant positive effect on cognitive and socio-emotional outcomes. But there is not a significant effect on behavioral and academic outcomes.
There was little heterogeneity for all outcomes, besides behavioral outcomes, suggesting that the interventions produced similar results across studies on cognitive, socio-emotional and academic outcomes despite the interventions being quite diverse.
What do the findings in this review mean?
Findings from this review indicate mixed effects of MBIs in schools. There is some indication that MBIs can improve cognitive and socio-emotional outcomes, but no support for improvement in behavior or academic achievement. Despite the growing support of MBIs for adults, youth may not benefit in the same ways or to the same extent as adults.
While not well studied, anecdotal evidence indicates costs and adverse effects of these types of interventions that should be better studied and weighed against the small to no effects on different types of outcomes when considering adoption of MBIs in schools.
These findings should be read with caution given the weakness of the evidence produced by the studies. The high risk of bias present in the studies means that further evidence is needed to evaluate the effectiveness of this type of intervention. The evidence from this review urges caution in the widespread adoption of MBIs and encourages rigorous evaluation of the practice should schools choose to implement it.
How up-to-date is this review?
The review authors searched for studies published until May 2015. This Campbell systematic review was published in March 2017.
Executive summary
BACKGROUND
Due to educational policy initiatives over the last two decades, school districts across the United States have placed more emphasis on improving academic standards and accountability. Indeed, children are spending between 20 to 25 hours per year on meeting federal, state and local school-district testing requirements (Hart et al., 2015). This increased emphasis on academic standards and high stakes testing has, at least in part, been blamed for the increasing levels of stress and anxiety children are experiencing (APA, 2009; Merkangas et al., 2010; Pope, 2010). In addition to changes in education policy requiring an increased emphasis on academic standards and accountability, schools are increasingly expected to attend to the social, emotional, and behavioral needs and problems of students. Given that as many as 13% to 20% children in the U.S. are experiencing one or more mental disorders (Center for Disease Control and Prevention, 2013), schools are increasingly challenged to respond to the growing emotional and behavioral needs of their students. Moreover, socioemotional development and competencies have been linked to learning and academic achievement, and have thus become a target for school-based interventions as a means of improving learning and academic achievement (Durlak, Weisberg, Dymnicki, Taylor, & Schhellinger, 2011; Eisenberg, Spinrade, & Eggum, 2010; Zins & Elias, 2006).
One approach to supporting improvements in socioemotional development and competencies that has received growing interest for use in schools is mindfulness-based interventions (MBIs). Mindfulness is defined as “paying attention in a particular way: on purpose, in the present moment, nonjudgementally” (Zabat-Zinn, 1994, p. 4). Research suggests positive effects of MBIs for adults with chronic conditions, mental health diagnoses, psychiatric disorders, and stress (Chiesa, Calati, & Serretti, 2011; deVibe et al., 2012; Cramer, Haller, Lauche, & Dobos, 2012; Vollestad, B. Nielsen, & H. Nielsen, 2012. Moreover, studies suggest that mindfulness based practices may improve performance on a variety of socioemotional outcomes, including self-regulation, stress, and mood disturbance (Cheisa & Serretti, 2009; Regehr, Glancy, & Pitts, 2013). There has been increasing interest in MBIs with children and adolescents, and schools are often seen as a convenient setting to implement MBIs with children and youth. Some of the more popular MBIs used in schools are Mindfulness Based Stress Reduction (MBSR; Kabat-Zinn, 1979; Bootzin & Stevens, 2005), Mindfulness Based Cognitive Therapy for Children (MBCT-C; Segal, Williams, & Teasdale, 2002; Semple, Reid, & Miller, 2005), Meditation of the Soles of the Feet (SoF; Singh et al., 2007), and Learning to Breath (LTB; Broderick & Metz, 2009). Despite the dramatic increase in the use of MBIs in schools to affect socioemotional and academic outcomes, little effort has been invested to systematically examine the body of evidence using rigorous methods, particularly for behavioral and academic outcomes of MBIs implemented in school settings.
This review contributes to the literature by including the most recent research on MBIs in school settings, including outcomes that have not been examined in prior reviews of school-based mindfulness interventions, including behavioral and academic outcomes, and employing stringent criteria for search, selection, coding, and analysis as specified in the Campbell Collaboration policies and guidelines to inform educational policy and practice and identify gaps in the current evidence base to guide future research in this growing area of practice and research.
OBJECTIVES
The purpose of this review is to examine and synthesize evidence of mindfulness-based interventions implemented in school settings with primary and secondary school students on achievement, behavior and socioemotional outcomes to inform education practice and policy. Specifically, the primary aim of this review is designed to answer the following research question: What are the effects of mindfulness-based interventions on cognition, academic achievement, behavior and socioemotional outcomes?
Moreover, within the context of this review, we aim to describe: The types of mindfulness-based interventions being evaluated in school settings. The state and quality of evidence of intervention outcomes studies of mindfulness-based interventions in school settings?
SEARCH METHODS
We attempted to identify and retrieve both published and unpublished studies through a comprehensive search that included multiple electronic databases, research registers, grey literature sources, and reference lists of reviews and relevant studies. We searched 13 electronic databases, research registers, relevant clearinghouse, government and research center websites, conference abstracts/proceedings, reference lists of prior reviews and included studies, and contact with experts and researchers in the area of school-based mindfulness interventions.
SELECTION CRITERIA
Studies were included in this review if they met the following criteria:
Cognition (e.g., executive function, memory, cognition, attention) Academic performance (e.g., standardized achievement tests, measures of content mastery, reading, grades) Behavior (e.g., disciplinary referrals, aggression and other externalizing behaviors, time on task, compliance, attendance) Socioemotional (e.g., anxiety, stress, engagement, social skills, self-esteem, emotion regulation, grit, internalizing behaviors) Physiological (e.g., cortisol, heart rate, brain activity)
DATA COLLECTION AND ANALYSIS
Titles and abstracts of the studies found through the search procedures were screened for relevance by two reviewers for most electronic databases, with the exception of the Australian Education Index, the British Education Index, and CBCA Education which were reviewed by one author. Documents that were not obviously ineligible or irrelevant based on the title and abstract review were retrieved in full text for final eligibility screening. Two reviewers independently reviewed each full text report using a screening form to determine final inclusion. Any discrepancies between the reviewers were discussed and resolved through consensus. For all studies that passed the eligibility screening process described above, two reviewers independently coded each eligible study using a structured data extraction form. Following independent coding of studies, coders then compared coding and identified and discussed discrepancies, which were resolved through consensus. If consensus could not be reached between the two coders, a third member of the review team was consulted to resolve the discrepancy.
We conducted descriptive analyses on variables of interest from all included studies to provide information regarding participant, setting, intervention characteristics for all studies that met eligibility criteria. For those that met criteria for inclusion in the meta-analysis, we estimated effect sizes for each included RCT and QED study when enough data was reported in the study or provided by study authors. For RCT and QED studies, we calculated the magnitude of effect using the standardized mean difference effect size with Hedges’ g correction for continuous outcomes and odds ratios for outcomes presented as dichotomous variables.
Following the estimation of individual study level effects, we conducted separate meta-analyses using Comprehensive Meta-Analysis, version 3.0 (CMA; Borenstein, Hedges, Higgins, & Rothstein, 2014) for the following outcome domains of interest: cognitive, academic, behavioral and socioemotional outcomes. To synthesize effects across studies, a weighted mean effect was calculated by weighting each study level effect size by the inverse of its variance. Random effects statistical models were used throughout. RCT and QED studies were pooled to allow for greater statistical power in all meta-analyses (heterogeneity between RCT and QED studies was not statistically significant in any of the meta-analyses). Following the estimation of summary effects, we conducted a test of homogeneity (Q-test) to compare the observed variance to what would be expected from sampling error. The I2 statistic was used to describe the percentage of total variation across studies due to the heterogeneity rather than chance. We also constructed a forest plot displaying study-level mean effect sizes and 95% confidence intervals for the included studies to provide opportunity for visual analysis of the precision of the estimated effect sizes, detection of studies with extreme effects, and information regarding heterogeneity of studies. Publication bias was assessed using funnel plots. When there was significant heterogeneity across studies, we conducted moderator analyses to examine the following variables: study type (RCT, QED), provider (classroom teacher, trained instructor), researcher involvement (yes/no), homework (yes/no), manualized program (yes/no), and number of weeks (# of weeks of the intervention).
RESULTS
Of the 61 studies that met criteria for inclusion in this review, 25 were RCT studies, 19 were QED studies, 9 were SGPP studies and 8 were SSD studies. Of the 44 RCT and QED studies, 35 provided enough data to calculate an effect size and were included in one or more of the meta-analyses, depending on which outcomes of interest were reported in the studies. Of the 44 RCT and QED studies, seven were unpublished reports, with the remaining being published studies in peer-reviewed journals. The interventions represent a wide range of mindfulness intervention types, but most interventions were at least partially manualized and of shorter duration. The interventions were delivered by primarily a classroom teacher (31%) or by a mindfulness-trained interventionist (60%) external to the school system.
Meta-analytic findings indicate small, yet statistically significant effects on cognitive outcomes (k = 10; g = 0.25 (95% CI [0.06, 0.43], p = .01) and socioemotional outcomes (k = 28; g = 0.22 (95% CI [0.14, 0.30], p < .001), and small and non-significant effects on academic outcomes (k = 5; g = 0.27 (95% CI [-0.04, 0.57], p = .08.) and behavioral outcomes (k = 13; g = 0.14 (95% CI [-0.02, 0.30], p = .08). Heterogeneity was small and not statistically significant in all meta-analyses with the exception of behavioral outcomes (I 2 = 48%; T2 = .034; Q = 22.96, p = .03). Six studies measured physiological factors, with three of those studies from the same author team. Due to the nature of these measures, the time dependency of some of these measures (cannot compare AM cortisol to PM cortisol for example), and that so few studies measured these outcomes, quantitatively synthesizing these outcomes across these studies was not warranted.
Overall, there wasa moderate to high risk of bias across the 35 studies included in the meta-analyses, with variation in high risk areas across studies. Twenty-one studies (60%) were rated low risk and 14 studies (40%) were rated high risk of bias for random sequence generation. Only one study reported that participants and study and school staff were blinded to program allocation (Sibinga et al., 2013), although they did not specify how they blinded study and school staff to condition. The remaining studies were rated as high risk (86%) or unclear risk (11%). Most of the studies in this review were rated as low risk of attrition bias (74%). For the studies included in the meta-analyses, most studies were assessed as unclear risk for reporting bias as we could not find any protocols of studies with which to compare planned to actual reported outcomes. It must be noted, however, that several studies reported to use, and then only reported data for, subscales of measures rather than reporting the full measure score or all subscale scores. Thus, it is unclear whether the a priori intentions of these authors were to only use certain subscales or if the participants did complete the full measure and the study authors only described the use of and reported data for the subscale only. We also coded for additional factors related to potential bias in this corpus of studies: researcher allegiance bias, funding source bias, and confounding factors. Of the 35 studies included in the meta-analysis, we were able to clearly identify an author role in the development and/or delivery of the intervention in 18 (51%) of the studies. The funding source was often not reported, or the studies were not funded. In four of the studies (11%), the authors identified a funding source that was also an entity involved in the development or the delivery of the intervention. We also examined whether there were confounding factors with either the treatment or comparison groups. Thirteen studies (37%) were assessed as having a confound at the level of the instructor (n = 7; only one instructor in treatment, control or both conditions) or at the school/classroom level (n = 6; one classroom or school in the treatment, control or both conditions). A larger mean effect was observed for studies in which a confound was present, thus likely upwardly biasing results; however, we conducted sensitivity analysis and found that the difference in magnitude of effect between studies with and without confounds was not statistically significant.
AUTHORS’ CONCLUSIONS
Results indicate mixed results of school-based mindfulness interventions across the outcomes of interest in this review, with finding favorable impacts of mindfulness interventions on those processes that are likely more directly targeted by mindfulness interventions, namely cognitive and socioemotional outcomes. We found a lack of support at posttest to indicate that those positive effects on cognitive and socioemotional outcomes then translate into favorable outcomes for academic and behavioral outcomes as is hypothesized. The lack of heterogeneity for all outcomes with the exception of the behavioral outcomes indicate that the interventions in this review, although quite diverse in their characteristics, produced similar results across studies on cognitive, socioemotional and academic outcomes. These findings provide some support for the use of school-based mindfulness interventions for some outcomes, but do not provide overwhelming support of MBIs as being the panacea as some have advocated. The quality of the evidence varied, with some important risks of bias present across a large proportion of studies which threatens the internal validity of the included studies and is cause for caution in interpreting the results of this review.
Overall, the evidence from this review urges caution in the enthusiasm for, and widespread adoption of, school-based mindfulness interventions for children and youth. While the evidence points to positive effects on socioemotional and cognitive outcomes, there is a lack of evidence of effects on academic and behavioral outcomes. Despite the empirical support of mindfulness-based interventions for adults, children and adolescents may not benefit from mindfulness-based interventions similarly to adults. Children and adolescents may not be developmentally ready for the complex cognitive tasks, focus and level of awareness that mindfulness-based interventions require. Moreover, we know little about the costs and adverse effects of school-based mindfulness interventions—the costs of implementing these programs may not be justified, and there are some indications that mindfulness-based interventions may have some adverse effects on children and youth; however, these have not been adequately examined. If schools do want to implement mindfulness-based interventions, we urge schools to evaluate the practice in a rigorous way and monitor outcomes and costs.
1 Background
1.1 THE PROBLEM, CONDITION OR ISSUE
Evidence suggests that students today are experiencing high levels of stress as well as other emotional and developmental challenges that may impede their ability to learn and succeed in school (APA, 2009; Merikangas et al., 2010; Pope, 2010). Approximately 13%-20% of children in the U.S. experience at least one mental disorder, and these rates have been on the rise since 2005 (Centers for Disease Control and Prevention, 2013). The increased prevalence of stress and anxiety, and at earlier ages than prior generations, has been at least partially attributed to school-related stress—particularly, high stakes testing, increased academic pressure, and the overscheduling of students in multiple extracurricular activities (APA, 2009; Gregor, 2005; Pope, 2010; Suldo et al., 2009). Indeed, students report school-related stress as being their greatest source of stress (APA, 2009) and teachers rate behaviors associated with anxiety as some of the most common problems of children and adolescence (Harrison, Vannest, Davis & Reynolds, 2012). The prevalence and levels of student stress and anxiety has become a concern for schools as emerging evidence suggests strong links between stress and anxiety with academic performance as well as with emotion regulation, behavioral functioning, and brain and cognitive development, which are also strongly linked to academic performance (Andersen, 2003; Andersen & Teicher, 2009; Sandler et al., 2000; Shonkoff et al., 2009; Suldo et al., 2009; Teicher et al., 2002; Wolchik et al., 2006).
Social-emotional development and competencies have also been linked to learning and academic achievement and increasingly viewed as a target for school-based interventions (Zins & Elias, 2006; Eisenberg, Spinrad, & Eggum, 2010; Durlak, Weissberg, Dymnicki, Taylor, & Schellinger, 2011). A growing body of evidence has found numerous social and emotional factors, including emotion regulation, effortful control, social and self-awareness, self-management, relationships skills and decision-making, to be directly and indirectly related to academic performance, school engagement, and externalizing and internalizing behaviors (Brackett & Rivers, 2014; Denham & Brown, 2010; National Center for Educational Statistics, 2002; Wang et al., 1997). Social-emotional competencies are positively related to academic success, greater impulse control, better concentration and attention in school, whereas a lack of social-emotional skills is linked to academic, social and behavioral problems (See Eisenberg et al., 2010 and Denham & Brown, 2010). For example, an inverse relationship between emotion regulation and effortful control has been found with externalizing behavior problems in pre-school age children through adolescence (Eiden et al., 2007, Eisenberg et al., 2004; Gardner et al., 2008). Conversely, students who exhibit greater ability to self-regulate are more likely to demonstrate better ability to concentrate and pay attention in school and exhibit better impulse control and fewer externalizing behaviors, leading to improved functioning and success in school (Eigsti et al, 2006; Eisenberg et al., 2010; McClelland et al., 2007; Mischel et al., 1989).
The increased prevalence of stress, anxiety, mental health problems and other social, emotional, and behavioral risk factors, along with the increase in knowledge of the impact of these factors on learning and achievement, has prompted schools and policy-makers to begin to more explicitly attend to students’ social and emotional functioning through both curricula and ancillary programs (Zins & Elias, 2006). Indeed, for students to succeed in school, it seems ever more apparent that schools need to provide strong social and emotional components and support students’ well-being in addition to providing strong academic curriculum and instruction (Zins, Weissberg, Wang, & Walberg, 2004).
As schools have struggled to find ways to support students’ overall well-being, one approach receiving growing interest is the use of mindfulness practices. Mindfulness, commonly defined as “paying attention in a particular way: on purpose, in the present moment, nonjudgmentally” (Kabat-Zinn, 1994, p. 4), has become mainstream and practiced by high profile stars and athletes as a means of improving health, well-being and athletic performance. Indeed, mindfulness was featured on 60 Minutes, free lessons in mindfulness are given as perks at companies like Google (Walton, 2014), and meditation is an integral part of the Seattle Seahawks training regimen (Roenigk, 2013). Google “mindfulness” and millions of news articles, video and audio files, images, books, practice guides and links to various centers for mindfulness will be listed in the results. From a simple Google search, it appears that mindfulness is a common topic in the public sphere.
While mindfulness seems to be a popular trend being adopted by individuals, it is also beginning to be considered in various areas of public policy, including education policy. Over the past decade, interest in mindfulness has been growing and mindfulness-based approaches to improving health and well-being, particularly with adults, has spread across fields, including psychology, healthcare, neuroscience, and business. This burgeoning interest in mindfulness is due, at least in part, to a significant and growing body of evidence pointing to positive effects of mindfulness training on cognitive processes. Evidence suggests that mindfulness practice improves performance on a variety of measures of self-regulation (Lo & Allen, 2008; Heeren, Van Broek, & Philippot, 2009) and emotion regulation (e.g., Speca et al., 2000; Fincune & Mercer, 2006), as well as enhancing cognitive functions such as attention, working memory and some executive functions (Chiesa, Calati, & Serretti, 2011), all of which are important to success in school. Indeed, Mindfulness interventions have been found to alter brain structure and function, including increased blood flow to and thickening of the cerebral cortex (Davidson, 2008) and increased gray matter concentration in areas of the brain involved with emotion regulation, learning and memory (Holzel et al., 2011). A meta-analysis of 21 neuroimaging studies found consistent differences between meditators and non-meditators in eight regions of the brain key to meta-awareness, body awareness, memory and self and emotion regulation (Fox et al., 2014).
Moreover, mindfulness has been found to be effective in the treatment of a myriad of health, social and psychological problems. Numerous studies and meta-analyses have investigated the use of mindfulness-based interventions (MBIs) in medicine, with mindfulness training and practice being found to help patients with chronic conditions manage pain (e.g., Cramer, Haller, Lauche, & Dobos, 2012; Veehof, Oskam, Schreurs, & Bohlmeijer, 2011), fibromyalgia symptoms (i.e., Lauche, Holger, Dobos, Langhorst, & Schmidt, 2013), and reduce stress in breast cancer patients (i.e., Zainal, Booth, & Huppert, 2013). Additionally, syntheses and meta-analyses have found positive effects of MBIs in treating individuals with mental health diagnoses, such as anxiety (deVibe et al., 2012; Vollestad, B. Nielsen, & H. Nielsen, 2012), psychiatric disorders (i.e., Chiesa, Calati, & Serretti, 2011), psychosis (Khoury, Lecomte, Gaudiano, & Paquin, 2013), personal development and quality of life (deVibe et al., 2012) as well as stress in healthy people (i.e., Cheisa & Serretti, 2009) including university students (Regehr, Glancy, & Pitts, 2013). Indeed, the use of mindfulness has greatly expanded into various fields to aid in the treatment of a vast array of conditions as well as to more generally enhance health and wellbeing.
While the vast majority of research on mindfulness has historically been focused on adults, the increase in promising research based on the diverse application of MBIs with adults and the growing popularity of mindfulness with the general public has naturally led to the extension of mindfulness to the application with children and youth (Zenner et al., 2014). It has been argued that children could benefit from mindfulness in ways similar to adults (Davis, 2012; Hooker & Fodor, 2008), and initial reviews suggest that MBIs are feasible with children and adolescents with adaptations (Burke, 2009; Zelazo & Lyons, 2012). Mindfulness-based interventions (MBIs) have been adapted from adult interventions or developed specifically for youth for a range of clinical conditions as well as more generally to enhance health and well-being, and applications for use in schools are also gaining attention.
The use of MBIs is on the rise in schools across the United States and United Kingdom as more and more schools have begun implementing various mindfulness-based programs and integrating mindfulness into the curricula (e.g., MindUP, The Inner Resilience Program, South Burlington Wellness and Resilience Program, Mindful Schools, Learning to Breathe, Mindfulness in Schools Project, Still Quiet Place, Stressed Teens, and Wellness Works in Schools). Moreover, efforts to promote mindfulness practices are being included in public policy initiatives. In the United Kingdom, for example, members of parliament have received training in mindfulness and have heard testimony of the evidence and benefits of mindfulness, including testimony from thousands of school children who have experienced mindfulness training in school. Also, an all-party parliamentary group was launched in the United Kingdom to conduct a nine-month inquiry into the potential role of mindfulness in areas of public policy, including education (Booth, 2014). The third session of the all-party parliamentary group focused on “mindfulness in health and education”, and members considered possible applications of mindfulness, with discussion of challenges for scaling up mindfulness programs to be included in teacher training as well as other potential policy actions (http://parliamentarywellbeinggroup.org.uk).
Although the use of MBIs appears to be on the rise in schools, and policy makers are calling for more mindfulness in education policy, it is unclear whether mindfulness-based approaches do indeed positively impact academic, emotional, and behavioral outcomes in students. While there is a growing body of studies of MBIs on a range of cognitive, social, and psychological outcomes including working memory, attention, academic skills, social skills, and emotional regulation (Meiklejohn et al., 2012), few studies have synthesized this literature using systematic and quantitative methods and few have focused specifically on school-based interventions. As schools develop practices and policies to try to more effectively and efficiently improve student outcomes, it is important that researchers, practitioners, policy makers, and other key stakeholders have access to evidence of effects of MBIs to make informed decisions rather than rely on anecdotal evidence and follow current popular trends. This information is critical as schools must make important academic, curricular and budgetary decisions. If a particular psychosocial intervention has large positive effects, then the use of academic time and limited school resources may be warranted to implement such a program during the school day; however, if the effects are minimalor adverse, then the use of academic time and limited school resources may not be worth those costs.
1.2 THE INTERVENTION AND HOW IT MIGHT WORK
Mindfulness was defined by Kabat-Zinn (1994) as “paying attention in a particularly way: on purpose, in the present moment, and non-judgmentally” (p. 4). Mindfulness is a type of practice derived from the Buddhist contemplative practices and traditions of Vipassana and Zen/Chan (Chiesa, Calati, & Serretti, 2011; Eberth & Sedlmeier, 2012), which is characterized by awareness of the current state of the mind and body without judgment, elaboration, or attachment (Burke, 2010; Eberth & Sedlmeier, 2012). Many scholars have embraced a two component model of mindfulness which includes self-regulation of attention and attending to the present moment. Self-regulation of attention refers to bringing awareness to a point of full attention to one's thoughts, feelings, and sensations. This includes maintaining sustained attention, keeping attention flexible, focusing on direct/current experience and inhibiting elaborate processing. The second component, orientation to the present moment, refers to the attitude or approach one takes in attending to the present moment and is exemplified by curiosity, openness, and acceptance (Bishop et al., 2004). Shapiro and colleagues (2006) conceptualized mindfulness as being comprised of three core components: intention, attention and attitude. The second and third components are similar to the two-component model described above. It's in the first component, intention, that their model differs. Intention involves the ability to regulate attention in a conscious and purposeful way. Shapiro and colleagues assert that one's intention for undertaking mindfulness practice (e.g., self-regulation, self-exploration, self-liberation) has been largely overlooked, but is important and may evolve over time.
While several models have been put forth to describe components of mindfulness and explain processes by which MBI's may work (e.g., Grabovac et al., 2011; Howell & Buro, 2011;Jankowski & Holas, 2013; Melbourne Academic Mindfulness Interest Group, 2006; Shapiro et al., 2006; Shapiro et al., 2011; Zelazo & Lyons, 2012), the specific mechanisms of mindfulness have not been fully explicated. Most models propose on one or more possible mechanisms, including cognitive, psychological and neurobiological mechanisms. We will focus on mechanisms that are most relevant to school-related outcomes of interest to this review (see Figure 1).
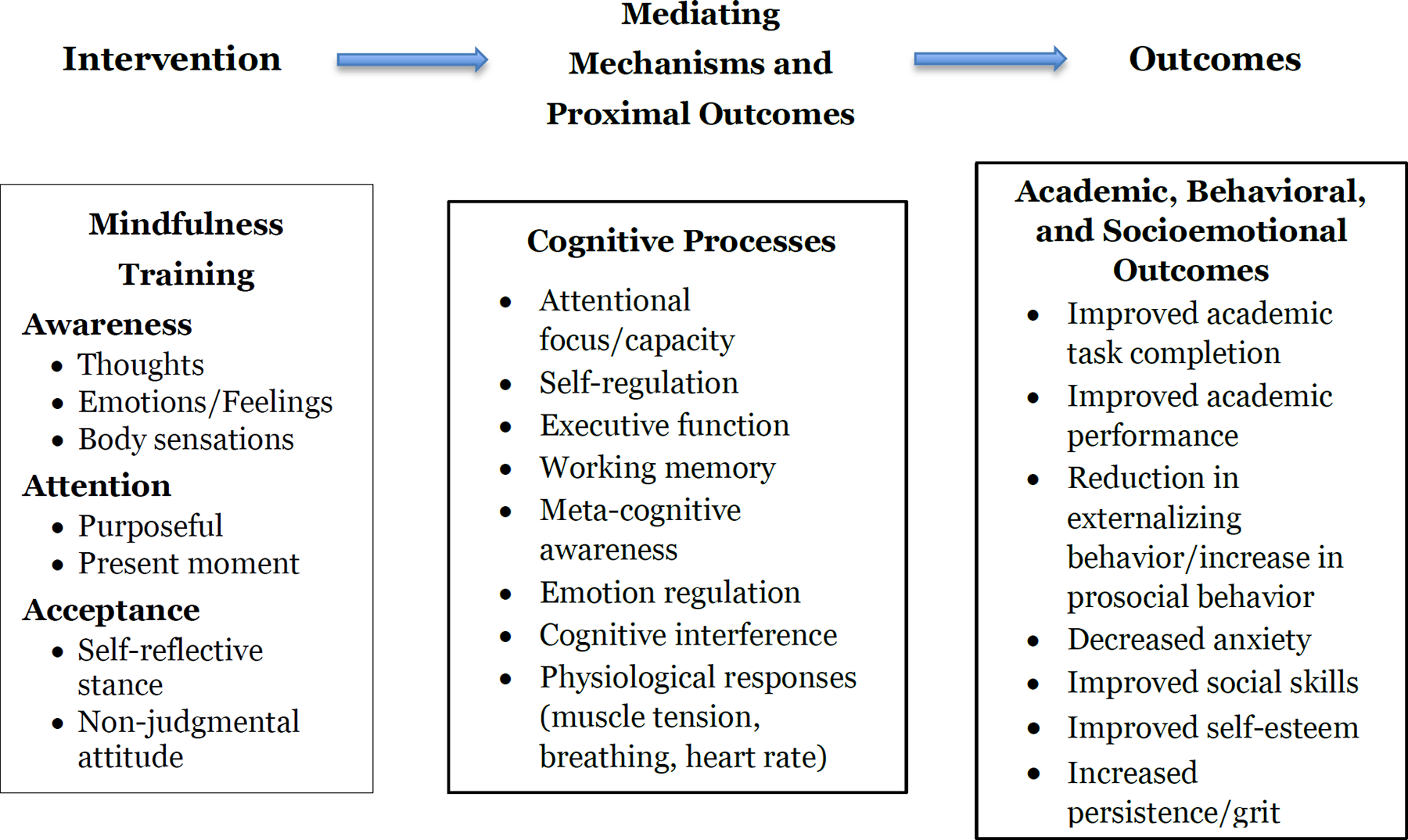
Logic model for MBIs with school students
Evidence suggests that mindfulness invokes cognitive processes and functions that are important to academic achievement, socioemotional functioning and behavior, namely attention, self-regulation, working memory, executive function, and metacognitive awareness (Grabovec et al., 2011; Melbourne-Based Mindfulness Interest Group, 2006; Zelazo et al., 2012; Shapiro et al., 2006). Some of these constructs are fairly broad, have overlapping components or are described or classified in the literature differently, thus making discussing the mechanisms involved in mindfulness interventions somewhat challenging. For example, self-regulation is conceptualized in terms of encompassing attention in some literature, but maintained as distinct constructs in others. Despite the variation across the literature in the ways in which cognitive processes are defined and measured, it is well recognized that cognitive processes are targeted and affected by MBI's and are important to academic achievement and socioemotional and behavioral outcomes.
As noted above, “paying attention” is a key component of mindfulness practice, requiring one to focus and direct attention in specific ways. Evidence suggests that mindfulness can enhance various aspects of attention or affect brain structure in areas related to attention (Carmody, 2009; Chiesa et al., 2011; Napoli et al., 2005). Given that a student's ability to sustain attention in class and on the right things is critical, and that performance and behavior are positively associated with attention (Hart, 2004; Rudasill, Gallagher, & White, 2010), MBI's could improve school achievement and behavior by helping students focus and sustain attention in school.
Self-regulation is another mechanism by which mindfulness may positively affect school-related outcomes. Self-regulation generally refers to monitoring and controlling our thoughts, actions and emotions (Zelazo & Lyons, 2012). It is often divided into cognitive self-regulation (including executive function, attention, planning) and emotional self-regulation (behavior and mental health; Duncan & Magnuson, 2009) and studied under the umbrella of executive function, which may also include working memory, cognitive flexibility, and inhibitory control (Zelazo & Lyons, 2012). The ability to monitor and control one's thoughts, behaviors and emotions plays an important role across all life domains, including school related outcomes. Self-regulation has been found to be related to, or a predictor for, a number of outcomes important to student success in school, such as externalizing and internalizing problems, classroom behaviors and disciplinary incidents, and math and reading (Berking & Wupperman, 2012; Ponitz et al., 2009; Quinn & Fromme, 2010; Richardson et al., 2012; Setken et al., 2010; Wyman et al., 2010). Evidence suggests that mindfulness positively effects self-regulation, as operationalized and measured in a variety of ways, and has been associated with changes in brain regions underlying self-regulation (Holzel et al., 2011). MBIs target self-regulation in that mindfulness practice requires one to attend to one's thoughts in the present moment and accept those thoughts without trying to change the thoughts or engage in action, promoting sustained attention and cognitive flexibility while also reducing emotional reactivity (Zelazo & Lyons, 2012). The emphasis on attending with acceptance and with a nonjudgmental attitude enables students to engage in more socially appropriate behavior and promote well-being by viewing situations through a different perspective and engaging in a type of detachment, which allows one to consider other potential responses and disrupt typical patterns of thinking and acting (Hart, 2004; Zelazo & Lyons, 2012). Thus, through cognitive and emotional self-regulation, MBIs may improve academic and behavioral outcomes, reduce mental health symptoms, and improve socioemotional well-being.
While mindfulness has been associated with a number of positive outcomes and may invoke a variety of potential mechanisms, mindfulness is a broad construct and interventions using mindfulness vary. This review will focus on MBIs with preschool, primary and secondary students in school settings. A number of MBI's being used in schools are being adapted from MBIs used with adults and others are being developed specifically for use with youth. For example, Mindfulness Based Stress Reduction (MBSR; Kabat-Zinn, 1979) and Mindfulness-Based Cognitive Therapy for Children (MBCT-C; Semple, Reid, & Miller, 2005), are MBIs that were originally developed for adults and have been adapted for youth. MBSR, a group intervention aimed at reducing stress, is composed of eight weekly 2.5-hour sessions with a daily 45-minute homework assignment (Grossman, Niemann, Schmidt, & Walach, 2004). Participants receive instruction in various aspects of mindfulness, including mindful awareness during meditation, yoga, and are taught to engage in continuous awareness of physical, mental, and emotional states without judgment or evaluation. Mindfulness based cognitive therapy (MBCT) was originally developed by Segal, Williams, and Teasdale (2002) as a treatment to reduce relapse of recurrent major depressive episodes in adults and was later adapted for use with children (MBCT-C; Semple, Reid & Miller, 2005; Semple, Lee, Rosa & L. Miller, 2010) to address anxiety. Researchers have adapted and implemented MBSR with children in clinical settings (Bootzin & Stevens, 2005), community settings (Saltzman & Goldin, 2008) and school settings (Bakosh, 2013; Bakosh, 2015; Sibinga, 2013; Sibinga, 2015). Both MBCT (for adults) and MBCT-C combine mindfulness-based practices such as attention on the breath and awareness of the present moment with cognitive interventions to achieve “affective self-regulation” (p. 222), but the children's version has been reduced from 12 weeks to 8 weeks in duration, there is less amount of time of each seated period and group size is smaller (Semple et al., 2010). Another distinction between the adult and child programs is that MBCT-C encourages parental involvement in the form of information sessions, brief mindfulness training exercises, and home practice of meditation with children. Since its development, several studies of MBCT-C in school settings have been conducted (i.e., Semple et al., 2005), as well as in other settings (e.g., Lee, Semple, Rosa, & L. Miller, 2008; Bogels, Hoogstad, van Dun, DeShutter, & Restifo, 2008).
Learning to BREATHE (L2B; Broderick & Metz, 2009) is an example of an MBI that was designed specifically for the classroom setting. The curriculum “tailors mindfulness-based approaches to the developmental needs of adolescents” (p. 38) by helping students be mindful of their present situation through lessons on body, thought, and emotion awareness, reducing self-judgment, and being mindful in everyday life (Broderick & Metz, 2009). L2B is a brief, six, twelve, or sixteen week curriculum conducted in a group setting that has been integrated into school curriculum in health class (Broderick & Metz, 2009) or choir class (Metz, Frank, Reibel, Cantrell, Sanders, & Broderick, 2013). Each lesson includes a short overview of the mindfulness principle being studied, group discussion, time to practice mindfulness by applying the principle, and home meditation practice assignments with supporting materials provided (Broderick and Metz, 2009; Metz et al., 2013).
In the descriptions of these approaches, one can discern that there are more similarities between MBI approaches than differences. For example, all of the approaches incorporate a training period of guided meditation techniques focusing on mindful attention and awareness of breath, body, or mind and followed by independent practice. The interventions differ in their intended purposes, such as treatment of anxiety and stress, managing aggressive behaviors, emotional regulation, and overall health promotion and how they are implemented in school settings. MBIs have been implemented in “core” content classes (reading and Language Arts, math, science, or social studies), in “elective periods” such as physical education classes (Napoli et al., 2008), choir classes (Metz et al., 2013), enrichment or intervention periods, or in time outside the regular school day (e.g., after-school tutoring or summer school). The type of setting is often determined by the purposes or outcomes measured, as well as the practical and systemic constraints and requirements in the school. For example, Broderick & Metz (2009) examined outcomes related to mental health by conducting the intervention in students’ health classes.
While many of the MBIs discussed to this point intervene directly with the youth, there are MBIs that also involve parents or teachers, either as a supplement to student training or as the primary target of the intervention. For example, Semple and colleagues (2010) conducted parent-training sessions in mindfulness, which provided an overview of the program their children would be receiving at school, as well as some opportunities for the parents to engage in mindfulness practice. Parents were also encouraged to participate in their child's home practice sessions; however, no data were collected or analyzed as a result of these parent-training sessions. It is yet unclear whether parent or teacher participation in the intervention provides any added benefit or enhances student outcomes. Other MBIs have been conducted with teachers or parents as the primary or only recipient of the intervention. In these interventions, the intent of providing teacher or parent training is to affect parent or teacher outcomes, with some hypothesizing indirect outcomes on students through changes in parent or teacher behavior from mindfulness practice. For example, Jennings and colleagues (2011) examined the effects of Cultivating Awareness and Resilience in Education (CARE), a mindfulness-based professional development program designed for teachers to reduce stress, improve teachers’ performance, and prevent “burnout.” Instruction in CARE provides teachers with training in a series of mindfulness activities, with periods of silent reflection and opportunities to extend the practices into daily classroom routines. Teachers reported high satisfaction with the CARE training, but there were no measures of student performance. Because MBIs that target teachers or parents as the primary recipient of the MBI focus on different outcomes (teacher and parent outcomes versus student outcomes, with perhaps some secondary student outcomes), we believe it is most appropriate to separate interventions targeting students from studies targeting teachers or parents as the primary recipient of the intervention. Therefore, we will focus this review on interventions in which students are the primary recipients of the MBI.
1.3 PRIOR REVIEWS
While several reviews have been conducted on mindfulness-based interventions with adults for a myriad of problems and outcomes, less attention has been given to reviewing the literature on outcomes of mindfulness-based approaches for children and youth, particularly outcomes relevant to education. To date, we have located nine reviews of mindfulness-based interventions that include studies with children or youth. One of the reviews focused on health-related effects of sitting-meditative practices (Black, Milam, & Sussman, 2009) and two reviews were not specifically focused on children or education, but did include some studies of mindfulness-based approaches with children and/or youth with intellectual disabilities (Chapman, 2013) and developmental disabilities (Hwang & Kearney, 2013). The remaining five reviews examined effects of MBIs with children and youth and are more relevant to the proposed review, thus will be discussed in more depth.
Meiklejohn and colleagues (2012), Greenberg and Harris (2012), and Thompson and Gauntlett-Gilbert (2006) published traditional narrative reviews describing mindfulness interventions with children and youth. Meikeljohn and colleagues focused on literature related to integrating mindfulness training in primary and secondary education, whereas Greenberg and Harris and Thompson and Guantlett-Gilbert reviewed mindfulness practices in clinical settings or prevention or health promotion contexts. All three reviews described a variety of mindfulness-based approaches and two summarized findings of intervention studies. These reviews concluded that mindfulness-based approaches are feasible and promising, but cautioned that additional and more rigorous research was needed. While these reviews provide an overview of MBIs with children and youth, the authors did not describe their search, selection, or coding procedures and did not quantitatively synthesize effects of the interventions, thus limiting the conclusions that can be drawn regarding the effects of MBIs with children and youth.
In addition to several narrative reviews, three reviews were identified that used systematic review methods (Burke, 2010; Zenner, Hernleben-Kurz, & Walach, 2014; Zoogman, Goldberg, Hoyt, & Miller, 2014), two of which also quantitatively synthesized effects using meta-analytic methods (Zenner et al., 2014; Zoogman et al., 2014). Burke (2010) conducted a systematic review of mindfulness-based approaches with children and adolescents. Burke identified 15 studies (6 used a between-group design) that met review criteria that included articles written in English and studies that used secular contemplative mindfulness mediation techniques. The author conducted a search for studies in 12 research databases and, although the author did not limit the review to published studies, a comprehensive search for grey literature was not conducted and dissertations or conference papers were not accessed. This review included studies of mindfulness with clinical and non-clinical samples, but not all included studies were relevant to education (e.g., outpatient gastroesophageal reflux, body weight) and only four were conducted in school settings. Eight of the studies included in the Burke review were also included in the Meiklejohn review. Burke concluded that the studies provided evidence of the feasibility and acceptability of mindfulness-based approaches for children and adolescents, but the research base is limited by a lack of rigorous efficacy studies, which was attributed, in part, to the early stage of research in this area.
Two meta-analyses of MBIs with children and youth have been published. Zoogman et al., (2014) reports the first published meta-analysis of mindfulness meditation with youth. The search was conducted in 2011 and was limited to peer-reviewed journal articles published in English. Twenty studies (13 RCTs, 1 QED, and 6 within group pre-post test studies) reporting effects of mindfulness interventions with clinical and non-clinical samples were included in the meta-analysis. The mean effect of the included interventions was 0.227 [CI 0.148, 0.305] and heterogeneity was not significant. Of the 12 moderators tested, only one moderator was significant—studies using clinical samples reported significantly larger effect sizes than studies using non-clinical samples. Additional analyses performed found significantly greater effects for psychological symptoms than measures of other outcomes. Zenner and colleagues (2014) conducted a systematic review and meta-analysis of MBis in schools with a focus on psychological outcomes (cognitive performance, emotional problems, stress and coping, and resilience). The authors conducted a comprehensive search in 2012 for published and unpublished reports yielding 24 studies (10 RCTs, 8 QEDs, 1 two-armed cohort study, and 5 non-controlled trials). The mean effect of the 19 studies using a comparison group design was g = 0.40 [0.21, 0.58]. The authors found significant effects on cognitive performance, resilience, and stress measures and non-significant effects on emotional problems. The authors found significant heterogeneity between studies. The included studies were often underpowered and small, and a wide variety of programs were evaluated, with many researchers implementing their own programs. The authors concluded that mindfulness-based approaches in schools are promising and the available evidence justifies allocating resources to mindfulness intervention implementation and evaluation. They recommended that larger studies employing more robust and well-validated measures be used in future research.
1.4 WHY IT IS IMPORTANT TO DO THE REVIEW
The aforementioned reviews contribute to our understanding of mindfulness-based approaches with children and youth; however prior reviews are limited in several ways. First, most prior reviews used non-systematic search methods and narrative synthesis methods, are not directly relevant to education settings, or were limited by including only published studies, thus limiting their applicability to informing practice and policy in education. This systematic review expands and improves upon prior work in several ways. First, this review focused on a range of outcomes relevant to educational settings and included academic performance outcomes. As academic performance outcomes have not been included in prior reviews, the present review provides timely information that can be used in school policy and practice decisions. Second, this review employeda systematic and transparent process for searching, retrieving, and coding studies, and in cluded searches for unpublished studies. Using a systematic method to conduct the review of outcome research limits bias and reduces chance effects, leading to more reliable results (Cooper, 1998). Further, explicitly and transparently describing the review process allows for others to replicate and expand the review to include new studies or criteria.
In short, this review contributes to the literature by including the most recent research on MBIs in school settings, including outcomes that have not been included in prior reviews of school-based MBIs, and employing stringent criteria for search, selection, coding, and analysis as specified in the Campbell Collaboration policies and guidelines. Thus, this review provides the most up-to-date and rigorous review of MBIs to inform educational policy and practice and identify gaps in the current evidence base to guide future research.
2 Objectives
The purpose of this review is to examine and synthesize evidence of mindfulness-based interventions implemented in school settings with primary and secondary school students on achievement, behavior, socioemotional and physiological outcomes to inform education practice and policy. Specifically, the primary aim of this review is designed to answer the following research question:
What are the effects of mindfulness-based interventions on cognition, academic achievement, behavior, socioemotional and physiological outcomes?
Moreover, within the context of this review, we also aim to describe: the types of MBIs being evaluated in school settings. the state and quality of evidence of intervention outcomes studies of MBIs in school settings.
3 Methods
The study protocol that guided this review (Maynard et al., 2013) can be accessed at https://campbellcollaboration.org/library/mindfulness-based-interventions-primary-and-secondary-school-students.html.
3.1 CRITERIA FOR CONSIDERING STUDIES FOR THIS REVIEW
3.1.1 Types of studies
To be included in this review, studies must have used one of the following research designs: randomized controlled trial (RCT), quasi-experimental design (QED; studies using a comparison group design, but assigned groups to condition non-randomly), single-group pre-post test design (SGPP) or single subject design (SSD). For RCT and QED studies, wait list control, no treatment, treatment-as-usual and alternative treatment groups were considered acceptable comparison groups. The type of comparison group used in each study was coded and examined as a moderator. We did not require that studies provide pre-test data or make statistical adjustments; however, we coded such data for use in analysis. To be eligible for inclusion, SSD studies must have employed one of the following designs: alternating treatments, multiple baseline, or withdrawal. Although it is not typical for single-group or single subject designs to be included in Campbell reviews, this is a relatively nascent area of research and we believe it is important to provide a comprehensive picture of the state of evidence related to mindfulness-based interventions in school settings. These studies were included in this review to provide a description of MBIs being used in schools and the means and extent to which interventions are being assessed. We quantitatively synthesized effects separately by study design. Limitations and biases related to study designs that are inherently weaker were explicitly recognized and discussed.
3.1.2 Types of participants
Participants were children in pre-school, primary and secondary school grades in regular education, special education or alternative education settings from any country. As we anticipated, and as prior reviews have suggested, effects of MBIs may differ based on whether the sample is comprised of students that are high risk or come from a clinical population or from the general population of students. Therefore, we included MBIs that were implemented with any sample of students (e.g., general population, ADHD, special education) and coded the studies accordingly. Because we were interested in informing education policy, studies that included participants in inpatient hospital or residential settings were excluded from this review. Studies in which parents or teachers were the primary recipients of the intervention were excluded, although studies that included a parent or teacher component of an MBI intervention with students were included.
3.1.3 Types of interventions
Interventions of interest included those that were a) conducted in a school setting (during the school day or in a school-based after school program) and b) used a mindfulness component/strategy. Mindfulness was broadly defined as “self-regulation of attention to the conscious awareness of one's immediate experiences while adopting an attitude of curiosity, openness, and acceptance” (Bishop et al., 2004, p. 174). While definitions and mindfulness practices vary across studies, “most involve focusing non-judgmental attention on moment-to-moment private experiences, such as breath, thoughts, physical sensations, or other external aspects of the environment” (Thompson & Gauntlett-Gilbert, 2008, p. 398). For the purposes of this review, mindfulness-based interventions included methods for teaching mindfulness awareness where participants are encouraged to focus their attention either on a covert activity (e.g., thoughts, feelings, urges) or overt activity (e.g., lights, sounds, smells). Mindfulness interventions could include present moment work, meditation, relaxation skills training, breathing techniques and awareness of moment techniques delivered in vivo, via formal meditation practices or informal mindfulness exercises. Some specific interventions eligible included, but were not limited to, Mindfulness Based Stress Reduction (MBSR), Mindfulness Based Cognitive Therapy (MCBT), Learning to BREATHE, Inner Kids Program, and Acceptance and Commitment Therapy (ACT).
We included studies that used multi-component interventions as long as one of the components was a mindfulness strategy. We coded for the various components used in addition to mindfulness and reported this information in the description of the interventions.
We excluded Transcendental Meditation (TM) interventions. TM is another meditation-based intervention that has been implemented in schools (e.g., Quiet Time Program by David Lynch Foundation; Barnes et al., 2013) and examined for the reduction of stress in adolescents (e.g., Barnes, Trieber, & Davis, 2001). While MBIs and TM share a component of meditation, TM based interventions were not considered for this review for several reasons. While TM is a concentrative technique in which the meditator focuses the mind using a mantra, a picture, or a physical experience (Sedlmeier et al., 2012), there is concern about the religious aspect of TM, which is not usually present in MBIs. In fact, in one area, school administrators cancelled plans to implement TM due to concerns by parents that it would be promoting a religion (The Associated Press, 2006). Further, a United States federal appeals court (1979) called TM a form of religious teaching and ruled that the practice could not be taught as an elective in public high schools in the state of New Jersey, United States (Malnak v. Yogi, 1979). While some MBIs may also have a religious component, MBIs are generally recognized and taught as a secular intervention, whereas religious aspects are consistently present with TM. Moreover, MBIs typically contain a practice of generalizing the skill of mindfulness into day-to-day activities such as academic tasks or the regulation of attention, whereas TM is primarily viewed a period of meditation in order to “take a break” from day-to-day activities. Due to the differences in nature and intent between MBIs and TM, interventions utilizing TM were excluded from this review.
3.1.4 Types of outcome measures
Studies must have reported at least one of the following outcomes: Cognition (e.g., executive function, memory, cognition, attention) Academic performance (e.g., standardized achievement tests, measures of content mastery, reading, grades) Behavior (e.g., disciplinary referrals, aggression and other externalizing behaviors, time on task, compliance, attendance) Socioemotional (e.g., anxiety, stress, engagement, social skills, self-esteem, emotion regulation, grit, internalizing behaviors) Physiological (e.g., cortisol, heart rate, brain activity)
Measurement of above outcomes could have been conducted using standardized or unstandardized instruments and self-, parent-, or teacher reported or researcher administered measures were eligible. To be included in the meta-analysis, primary study authors must have reported enough information to calculate an effect size. If sufficient information to calculate an effect size was not provided, every effort was made to contact primary study authors to request the necessary information.
For studies in which the author reported both the total scale score and individual subscale scores for a measure, we did the following. For measures in which the total scale and all subscales were coded as the same outcome construct (as defined above), we usedonly the total scale score for analysis. For measures in which the subscales were measuring different outcome constructs (as defined above), we kept only the subscales scores for analysis.
3.1.5 Duration of follow-up
It was anticipated that most studies would report outcomes at post-test and thus post-test outcomes were the primary focus of this review; however, we noted studies that reported follow-up data or a subsequent report was published with outcomes examined at a follow-up time point.
3.1.6 Types of settings
The review included interventions conducted in a school setting.
3.1.7 Other criteria
Studies were included if they were conducted or published between 1990 and present. We selected 1990 as the cut off as MBIs implemented in school settings is a newer phenomenon and we wanted the literature to be relevant to current practices. No additional criteria wereapplied. The search was not restricted by geography, language, publication status or other study characteristics.
3.2 SEARCH METHODS FOR IDENTIFICATION OF STUDIES
3.2.1 Electronic searches
We included all studies that met the inclusion criteria outlined above. We attempted to identify and retrieve both published and unpublished studies through a comprehensive search that included multiple electronic databases, research registers, grey literature sources, and reference lists of reviews and relevant studies.
Electronic Databases
. Academic Search Complete . Australian Education Index . British Education Index . CBCA Education . Education Complete . ERIC . MEDLINE . ProQuest Dissertations and Theses . PsycINFO . Social Science Citation Index . Social Service Abstracts . Sociological Abstracts . SPORTDiscus
Research Registers and Websites
. Cochrane Collaboration Library . Database of Abstracts of Reviews of Effectiveness . National Technical Information Service . System for Information on Grey Literature . Evidence for Policy Practice Information and Coordinating Centre (EPPI-Centre) . Association for Mindfulness in Education (mindfuleducation.org) . Mindfulness in Schools Project (mindfulnessinschools.org)
Intervention: mindful* OR meditat* OR yoga OR “breath* technique” OR “mindfulness based stress reduction” OR MBSR OR “Mindfulness-based cognitive therapy” OR MBCT OR “learning to breathe” OR MindUP OR “Meditation on the Soles of the Feet” OR “non-judgmental awareness” OR “present-moment”)
AND Report type: evaluation OR intervention OR treatment OR outcome OR program OR trial OR experiment OR “control group” OR “controlled trial” OR “quasi-experiment*” OR random*
AND Targeted population:“elementary school” OR “primary school” OR “high school” OR “secondary school” OR “middle school” OR kindergarten OR pre-kindergarten
The full search strategy for each database is reported in Appendix 8.1.
3.2.2 Searching other resources
Grey literature sources
. Social Science Research Network . Authors of prior studies were contacted in an attempt to obtain unpublished studies, studies in process and published studies missed in the database search. . Conference abstracts and proceedings were reviewed to identify potentially relevant studies. Conference searches included: . The Society for Research on Educational Effectiveness (https://www.sree.org/pages/conferences/index.php), and the . American Educational Research Association Repository (http://www.aera.net/EventsMeetings/tabid/10063/Default.aspx. . Society for Research on Child Development (SCRD) . Society for Research on Adolescence (SRA) . Clearinghouses, research centers and government websites were reviewed to identify potential sources of relevant data: . The US Department of Education's web site contains reports of funded programs and initiatives: http://www2.ed.gov/about/offices/list/opepd/ppss/reports.html
. The Institution of Education Sciences, What Works Clearinghouse contains reports of intervention investigations: http://ies.ed.gov/funding/grantsearch/index.asp
. . Garrison Institute's Contemplative Education Database: www.garrisoninstitute.org
The reference lists from prior reviews and included studies were reviewed for potential studies. We also conducted forward citation searching using Google Scholar to search for studies citing our included studies.
3.3 DATA COLLECTION AND ANALYSIS
3.3.1 Selection of studies
Titles and abstracts of the studies found through the search procedures were screened for relevance by two reviewers for most electronic databases, with the exception of the Australian Education Index, the British Education Index, and CBCA Education. The three databases noted above were searched by a search specialist contracted to conduct searches in those databases, as the review authors did not have access. For the search results in those three databases, one reviewer screened titles and abstracts for relevance. Titles and abstracts that were obviously ineligible or irrelevant were screened out at the title/abstract stage. For example, studies that were deemed inappropriate at the title/abstract review stage were those that did not involve the target population (e.g., they involved college students or adults), did not involve an intervention, or were theoretical in nature. If there was any question as to the appropriateness of the study at this stage by either of the abstract screeners, the full text document was obtained. Documents that were not obviously ineligible or irrelevant based on the title and abstract review were retrieved in full text for final eligibility screening. Two reviewers independently reviewed each full text report using a screening form to determine final inclusion. Any discrepancies between the reviewers were discussed and resolved through consensus.
3.3.2 Data extraction and management
For all studies that passed the eligibility screening process described above, two reviewers independently codedeach eligible study using a structured data extraction form (Appendix 8.2; see also Maynard et al., 2015). The data extraction form, which was pilot tested by the coders, included items related to bibliographic information and source descriptors; methods and procedures; context, nature, and implementation of the intervention; sample characteristics; and outcome data needed to calculate effect sizes. Due to the large number of studies, four trained coders on the review team contributed to coding primary studies: Brandy Maynard, Michael Solis, Veronica Miller, and Kristen Brendel. Following independent coding of studies, coders then compared coding and identified and discussed discrepancies, which were resolved through consensus. If consensus could not be reached between the two coders, a third member of the review team was consulted to resolve the discrepancy.
3.3.3 Assessment of risk of bias in included studies
Two review authors independently assessed risk of bias in RCT and QED studies using the Cochrane Collaboration's risk of bias tool (Higgins et al., 2011). We assessed risk of bias for each of the six following domains: sequence generation, allocation, blinding, complete outcome data, and selective reporting. We also coded for additional factors related to potential bias in this corpus of studies: researcher allegiance bias, funding source bias, and confounding factors. In terms of allegiance bias and funding source bias, we assessed whether the study authors were directly involved in either the development or delivery of the intervention or were funded by an entity that had some stake in the intervention. Because studies are more likely to be biased in favor of the treatment intervention when study authors have a direct role in the development or the implementation of the study (Luborsky et al., 1999; Munder et al., 2013), or when funded by a source that has a stake in the intervention (Lundh et al., 2012), we believe it was important to assess for these biases in this review. We also examined whether there were confounding factors with either the treatment or comparison groups. Specifically, we examined whether there was one unit (e.g., teacher, classroom, school) in one or both conditions. When the treatment or comparison condition is confounded in this way, it is impossible to distinguish between the effect of that unit and the effect of the intervention and thus unobserved factors may be contributing to the outcome.
Each study was coded as “low”, “high”, or “unclear” risk of bias on each of the domains. Following independent coding by two authors, coders met to identify any discrepancies and all discrepancies were resolved through consensus. If consensus could not be reached between the two reviewers, a third member of the review team was consulted. Risk of bias in each domain was reported within and across studies in the results section using narrative and graphs. We anticipated that most studies included in this review would be at high risk of bias, thus we did not plan to restrict analyses based on risk of bias.
3.3.4 Synthesis procedures and statistical analysis
We conducted descriptive analyses on variables of interest from all included studies to provide information regarding: Study participants (e.g., risk level/subgroups, gender, race, income level, grade, age), Settings where studies are situated (e.g., school type, classroom type, geographical location/country, community characteristics), Relevant intervention characteristics (e.g., mindfulness strategies used, involvement of parents/teachers, duration of intervention, modality of intervention, implementer training). Risk of bias across RCT and QED studies included in the meta-analyses on each domain
Following descriptive analysis, we estimated effect sizes for each included RCT and QED study when enough data was reported in the study or provided by study authors. For RCT and QED studies, we calculated the magnitude of effect using the standardized mean difference effect size with Hedges’ g correction for continuous outcomes and odds ratios for outcomes presented as dichotomous variables. For studies in which the unit of assignment (e.g., classroom, school) did not match the unit of analysis (e.g., student) and the primary study authors did not account for clustering in their analysis (or the data extracted from the studies used for calculating effect sizes was not adjusted), we followed recommendations in the Cochrane Handbook (cite, 2011, 16.3.4) to derive approximately correct analysis by reducing the size of each trial to its ‘effective sample size’ (Rao, 1992) by dividing the sample size for each group by the ‘design effect’ (1 + (M-1) ICC). We applied this correction only to findings that were statistically significant as nonsignificant findings will remain nonsignificant without the correction (WWC manual). With the exception of Kuyken et al. (2013) and Metz et al. (2013), ICCs were not reported by study authors. In cases where study authors reported ICCs, we used the ICCs reported by the authors. For studies in which ICCs were not reported, we used an ICC of .20 for achievement outcomes and .10 for behavioral and socioemotional outcomes (cite WWC procedures manual). The direction of effect sizes were transformed to a positive effect to indicate the treatment group performed more favorably than the control group and a negative effect to indicate the control group performed more favorably than the treatment group.
Following the estimation of individual study level effects, we conducted separate meta-analyses using Comprehensive Meta-Analysis, version 3.0 (CMA; Borenstein, Hedges, Higgins, & Rothstein, 2014) for the following outcome domains of interest: cognitive, academic, behavioral and socioemotional outcomes. Within each of these domains, several included studies used multiple measures and/or multiple reports (e.g., parent, teacher) of the same measure. These circumstances created statistical dependencies that violate assumptions of standard meta-analytic methods. In order to ensure independence of study-level effect sizes, the mean of the measures was taken to estimate a study-level average across the measures within each outcome domain so that only one effect size estimate from each independent sample on each outcome domain was used in the meta-analyses. We followed standard procedures in CMA version 3.0 to use the mean of the selected outcomes for studies with multiple measures of the same outcome construct. In cases where multiple points of follow-up were provided, we coded follow-up points to conduct a separate analysis for effect sizes comparing studies with similar points of follow-up; however, there were not a sufficient number of studies measuring points beyond post-test, thus we only post-test effects were synthesized. One study provided data on two treatment groups—one group of general population students and another group of homeless students (Viafora et al., 2015). In this case, we used the data from the general population group for analysis (there was no comparison group for the homeless student group).
To synthesize effects across studies, a weighted mean effect was calculated by weighting each study level effect size by the inverse of its variance. Random effects statistical models were used throughout. The random effects variance component was estimated using the methods of moments method. RCT and QED studies were pooled to allow for greater statistical power in all meta-analyses (heterogeneity between RCT and QED studies was not statistically significant in any of the meta-analyses).
Following the estimation of summary effects, we conducted a test of homogeneity (Q-test) to compare the observed variance to what would be expected from sampling error. The I2 statistic was used to describe the percentage of total variation across studies due to the heterogeneity rather than chance. We also constructed a forest plot displaying study-level mean effect sizes and 95% confidence intervals for the included studies to provide opportunity for visual analysis of the precision of the estimated effect sizes, detection of studies with extreme effects, and information regarding heterogeneity of studies. Publication bias was assessed using funnel plots and the Egger's test, both conducted in CMA version 3.0.
When there was significant heterogeneity across studies, as determined by a statistically significant Q, we conducted moderator analyses using a random effects ANOVA for categorical variables. We did not assume a common among-study variance component across subgroups; tau-squared was computed within groups and not pooled across groups. The categorical variables examined per our protocol included: study type (RCT, QED), provider (classroom teacher, trained instructor), researcher involvement (yes/no), homework (yes/no), and manualized program (yes/no). For the one continuous variable we examined (number of weeks of the intervention), we used random effects meta-regression. All moderator analyses were conducted in CMA version 3.0.
3.4 DEVIATIONS FROM THE PROTOCOL
We experienced circumstances that required us to deviate from the protocol at times. During the literature search, the CINHAL and FRANCIS databases were undergoing technical difficulties and we were not able to access those databases, thus we did not search those databases as planned. We found six studies that measured physiological outcomes. While six studies measured physiological outcomes, not all studies measured the same, or enough of the same conceptually similar outcomes to warrant meta-analysis. Thus, we did not quantitatively synthesize effects of physiological outcomes, but rather provided a descriptive analysis of these studies. Also of note is that we did not originally plan to document adverse outcomes, but decided post-hoc to review studies for reporting of adverse outcomes.
4 Results
4.1 RESULTS OF SEARCH
Electronic searches of bibliographic databases and searches of other sources identified a total of 1353 citations. Titles and abstracts were screened for relevance and 1260 were excluded as duplicates or deemed inappropriate. The full text of the remaining 93 potential studies was reviewed and screened for eligibility by two independent coders. Sixty-onestudies passed full-text screening and were included in the review. See Figure 4.1 for the flow chart of the study selection process.
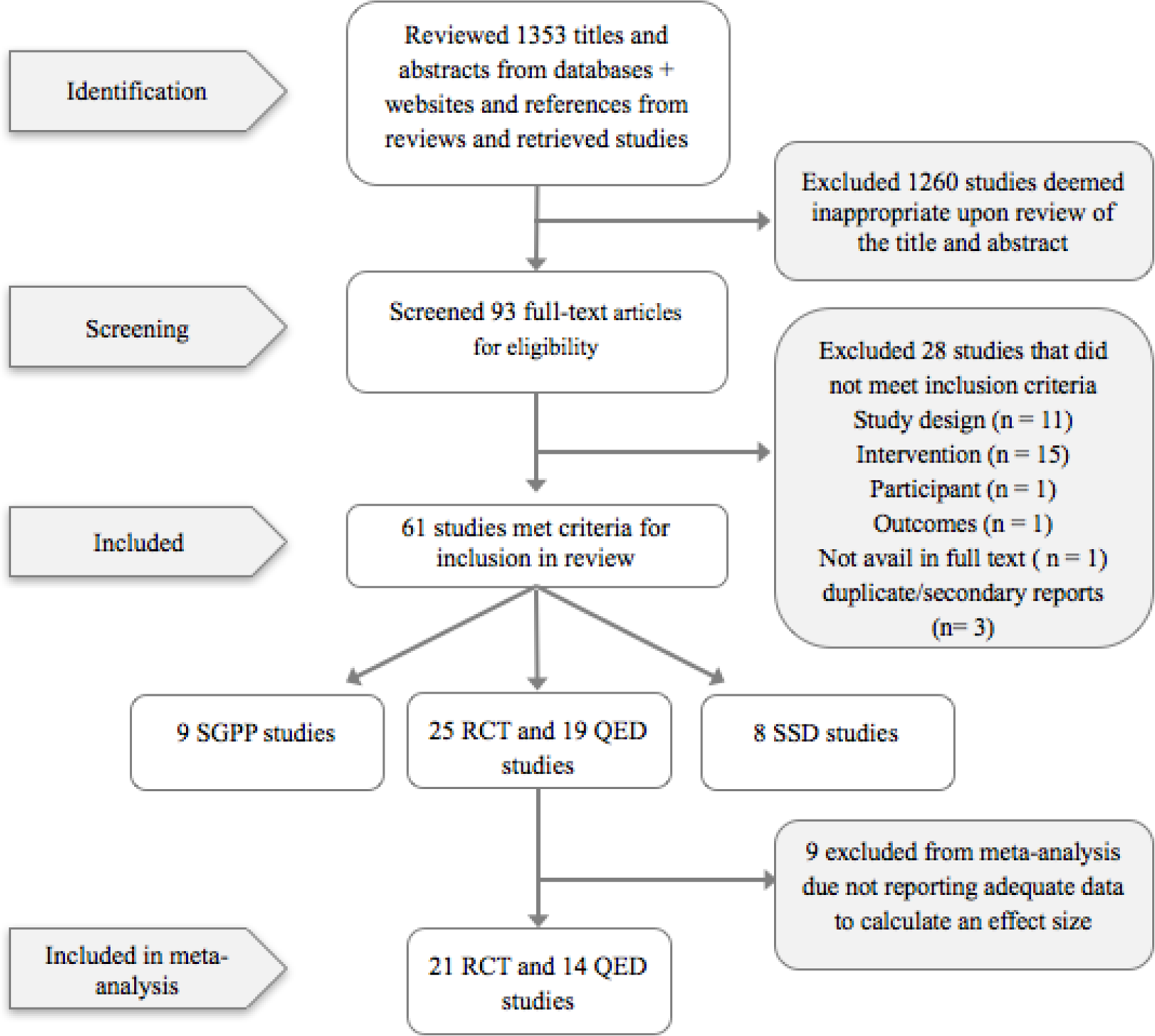
Flow chart of study selection process
4.1.1 Included studies
Of the 61 studies that met criteria for inclusion in this review, 25 were RCT studies, 19 were QED studies, 9 were SGPP studies and 8 were SSD studies. Of the 44 RCT and QED studies, 35 provided enough data to calculate an effect size and were included in one or more of the meta-analyses, depending on which outcomes of interest were reported in the studies. Characteristics of included RCT and QED studies is reported in Appendix 8.3, SGPP studies are reported in Appendix 8.4 and SSD studies are reported in Appendix 8.5.
4.1.2 Excluded studies
Twenty–eightreports were excluded and three others were identified as secondary reports of included studies during the full-text screening stage. The majority of studies were excluded due to not meeting criteria for study design (e.g., the article did not report results of an intervention, used a mindfulness comparison group; n = 11). The remaining studies were excluded due to not meeting criteria related to intervention characteristics (i.e., not a school-based intervention; n = 15), participant characteristics (e.g., teachers; n=1), outcomes (n = 1) or were not available in full text (n=1). A list of excluded studies and reasons for exclusion is presented in Appendix 8.6.
4.2 DESCRIPTION OF INCLUDED RCT & QED STUDIES
Of the 44 RCT and QED studies, seven were unpublished reports, with the remaining being published studies in peer-reviewed journals. Most of the studies were conducted in North America (74%), with others conducted in Asia (5%), Europe (16%) and Canada (5%). All studies were written in English, with the exception of Justo et al. (2011) written in Spanish. Sample sizes ranged from 23 to 557, with a mean sample size of 141. The studies measured one or more of the outcomes of interest: 10 studies measured cognitive outcomes, 5 measured academic outcomes, 13 measured behavioral outcomes, 28 measured socioemotional outcomes and 6 measured physiological outcomes. No studies reported adverse outcomes. See Table 4.1 for a summary of characteristics across the included 44 studies as well as the subgroup of the 35 studies included in at least one meta-analysis.
Characteristics of included RCT and QED studies
4.2.1 Participant characteristics
A total of 6,207 students were participants in the studies included in the meta-analyses. The mean age of participants across studies that reported age (n = 32) was 12.64 years. Approximately one third of the studies were conducted with elementary students and one third with high school students. Two studies were conducted with pre-school students, seven with middle school students, and six with students across grade levels. Most studies that reported the gender of the sample (n = 41) included a balanced mix of male and female students, although two studies included only male students and three included only female students. The majority of studies (84%) included students from the general population of regular education schools. The seven studies that included a special population included students who were at risk of dropout, African American students at risk of cardiovascular disease, urban boys with financial need and academic potential, at-risk high school girls, students with autism spectrum disorders, Special education needs (including emotional, behavioral, and learning difficulties) and at risk for being excluded from school, and students at risk students attending a disciplinary alternative education program.
4.2.2 Intervention characteristics
The included studies examined a range of MBIs. Of the 44 RCT and QED studies included in this review, almost half of the interventions were based on MBCT or MSBR (n = 20) and/or incorporated yoga (n = 21). Most of the interventions were either fully manualized or partially manualized interventions (n = 38). All of the interventions were delivered in a group format, with most programs delivered during the school day (n = 40) and the remaining programs delivered after school (n = 4). Interventions ranged in duration and frequency. For studies reporting adequate information, interventions ranged from 4 to 28 weeks (N = 42, M= 10.5, SD = 5.5) and were provided in 6 to 125 sessions (N = 42, M = 26, SD = 25). Interventions also varied in terms of how frequently students met to receive the intervention from one time every other week to 5 times a week, for an average of 13 hours of mindfulness instruction (SD = 11). Most interventions incorporated breathing techniques/breath awareness, present moment work (86%), and meditation (84%). Relaxation skills training was reported in 61% of the interventions and body scan in 45% of the interventions. At home practice was assigned or encouraged in about half (45%) of the studies. Some interventions included other components in addition to mindfulness, such as cognitive and/or behavioral strategies (n = 8), yoga (n = 11) or other strategies, such as talk/discussion, touch therapy, psychoeducation, aromatherapy, and/or literature (n = 11). Most studies (77%) did not measure fidelity of the intervention.
4.3 RISK OF BIAS IN INCLUDED RCT & QED STUDIES
Overall, there was a moderate to high risk of bias across the 35 studies included in the meta-analyses, with variation in high risk areas across studies. (See Figure 4.3 for a summary of risk across studies, Appendix 8.7 for a Table reporting each domain of risk for each study and Appendix 8.xx for a for Risk of bias within studies.
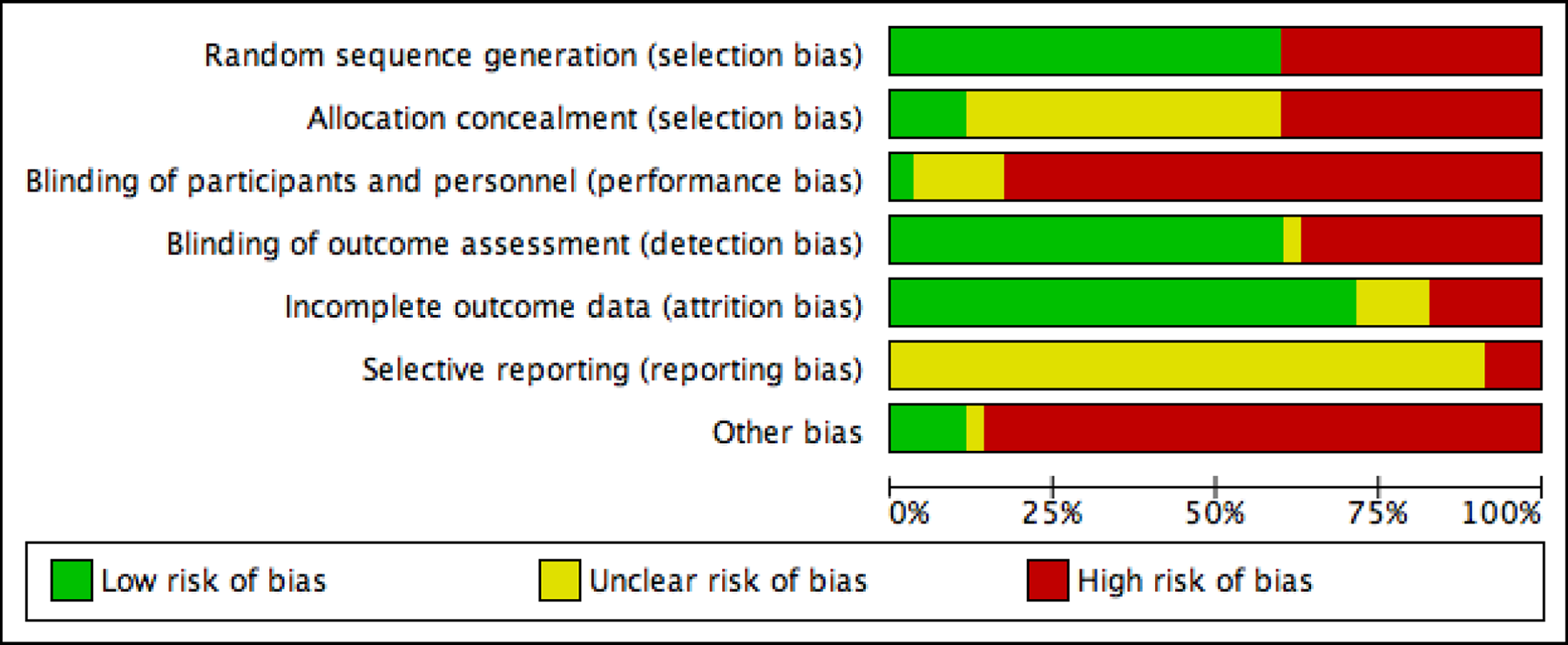
Risk of bias across studies
4.3.1 Selection bias
Selection bias is composed of random sequence generation and allocation concealment. We rated a study as being low risk on random sequence generation if they reported that they used randomization to assign participants to treatment and control groups. Twenty-one studies (60%) were rated low risk and 14 studies (40%) were rated high risk of bias for random sequence generation. In education and social science research, very rarely do studies report enough information to rate the level of risk on allocation concealment; therefore, we rated studies as unclear risk if they were randomized trials and high risk if they were non-randomized trials, unless study authors provided information about concealment procedures. Only four studies (11%) provided sufficient information to rate studies as low risk of bias on allocation concealment (Bluth et al., 2015; Flook et al., 2015; Haden et al., 2014; Noggle et al., 2012).
4.3.2 Performance and detection bias
For the types of interventions in this study, it is not typical, nor often practical, to blind study participants or personnel. Therefore, as we expected, most of the studies in this review were rated high risk for performance bias. Only one study reported that participants and study and school staff were blinded to program allocation (Sibinga et al., 2013), the remaining studies were rated as high risk (86%) or unclear risk (11%). For detection bias, expecting assessors to be blinded to condition is possible and a reasonable expectation for these study designs. We rated studies as low risk of bias if they reported blinding of outcome assessors or used only self-report measures. Overall, 60% of the included studies were rated as low risk of detection bias either because outcome assessors were blinded (n= 2) or studies used solely self-report questionnaires (n = 19).
4.3.3 Attrition bias
Most of the studies in this review were rated as low risk of attrition bias (74%). Four were rates as unclear risk, primarily because it was unclear what the analytic sample size was for the analyses or they were not clear on the initial sample size and thus we could not adequately calculate attrition. Five studies were rated at high risk of bias because their overall attrition rate was greater than 20% or there was high differential attrition between groups and the authors did not use any analytic approaches to impute missing data.
4.3.4 Reporting bias
We were not able to locate a study protocol for any of the included studies; therefore, we judged most of the included studies to be at unclear risk of selective reporting bias. Because we don't have study protocols for the studies included in this review to compare what they had planned to measure to what they actually reported, it is uncertain whether these studies reported results for all outcomes they actually measured. One study mentioned the use of a study protocol (Schonert-Reichl et al., 2015), but no other information regarding the publishing of the protocol was provided and it could not be located. It must also be noted that several studies reported data for subscales of measures rather than reporting data for the full measure or all of the other subscale scores. Thus, it is unclear whether the a priori intentions of these authors were to only use certain subscales or if the participants did complete the full measure and the study authors only reported data for the subscale only.
Because some studies were not included in the meta-analysis due to not reporting sufficient data to calculate an effect size, several studies that would have been rated as high risk due to not providing sufficient data to calculate an effect size were not included in the meta-analysis.
4.3.5 Other biases
We coded for additional factors related to potential bias in this corpus of studies: researcher allegiance bias, funding source bias, and confounding factors. Coding for allegiance bias and funding source bias was challenging, as study authors were often not explicit about their role or relationship in the study development or implementation and rarely acknowledged conflicts of interest. Of the 35 studies included in the meta-analysis, we were able to clearly identify an author role in the development, adaptation, and/or delivery of the intervention in 19 (54%) of the studies, one study in which an author had some affiliation with the organization delivering the intervention and another study in which one author was employed at the school where the intervention was delivered. In all other studies, it was unclear whether the author was independent or just did not report their involvement. We conducted sensitivity analyses to examine researcher involvement on magnitude of effect size. Larger effects were found in studies with researcher involvement compared to those with no researcher involvement on behavioral outcomes but smaller effects were found in studies with researcher involvement on socioemotional, academic, and cognitive outcomes, although the differences between groups were not statistically significant for any outcome.
In terms of the funding source, most authors either did not report the funding source or the studies were not funded. In four of the studies (11%), the authors identified a funding source that was also an entity involved in the development or the delivery of the intervention.
We also examined whether there were confounding factors with either the treatment or comparison groups. Specifically, we examined whether there was one unit (e.g., teacher, classroom, school) in one or both conditions. When the treatment or comparison condition is confounded in this way, it is impossible to distinguish between the effect of that unit and the effect of the intervention and thus unobserved factors may be contributing to the outcome. Fourteen studies (40%) were assessed as having a confound at the level of the instructor (n = 7; only one instructor in treatment, control or both conditions) or at the school/classroom level (n = 7; one classroom or school at the treatment, control or both conditions). A larger mean effect was observed on all outcomes for studies in which a confound was present compared to those without confounds, thus likely upwardly biasing results; however, the differences in magnitude of effect between studies with and without confounds was not statistically significant.
4.4 SYNTHESIS OF RESULTS
4.4.1 Mean effects on cognitive outcomes
Twenty effect sizes from 10 studies were synthesized to examine effects on cognitive outcomes. Results indicate that the overall mean effect (Hedges’ g) at post-test on cognitive measures was 0.25 (95% CI [0.06, 0.43], p = .01). Heterogeneity analysis indicated a low amount of heterogeneity (I 2 = 25%) that was not statistically significant (Q = 12.10, p = .21). The mean effect size and confidence intervals for each study are shown in the forest plot in Figure 4.4 below. See Appendix 8.8 for a full list of all measures of cognitive outcomes included in this meta-analysis by study.
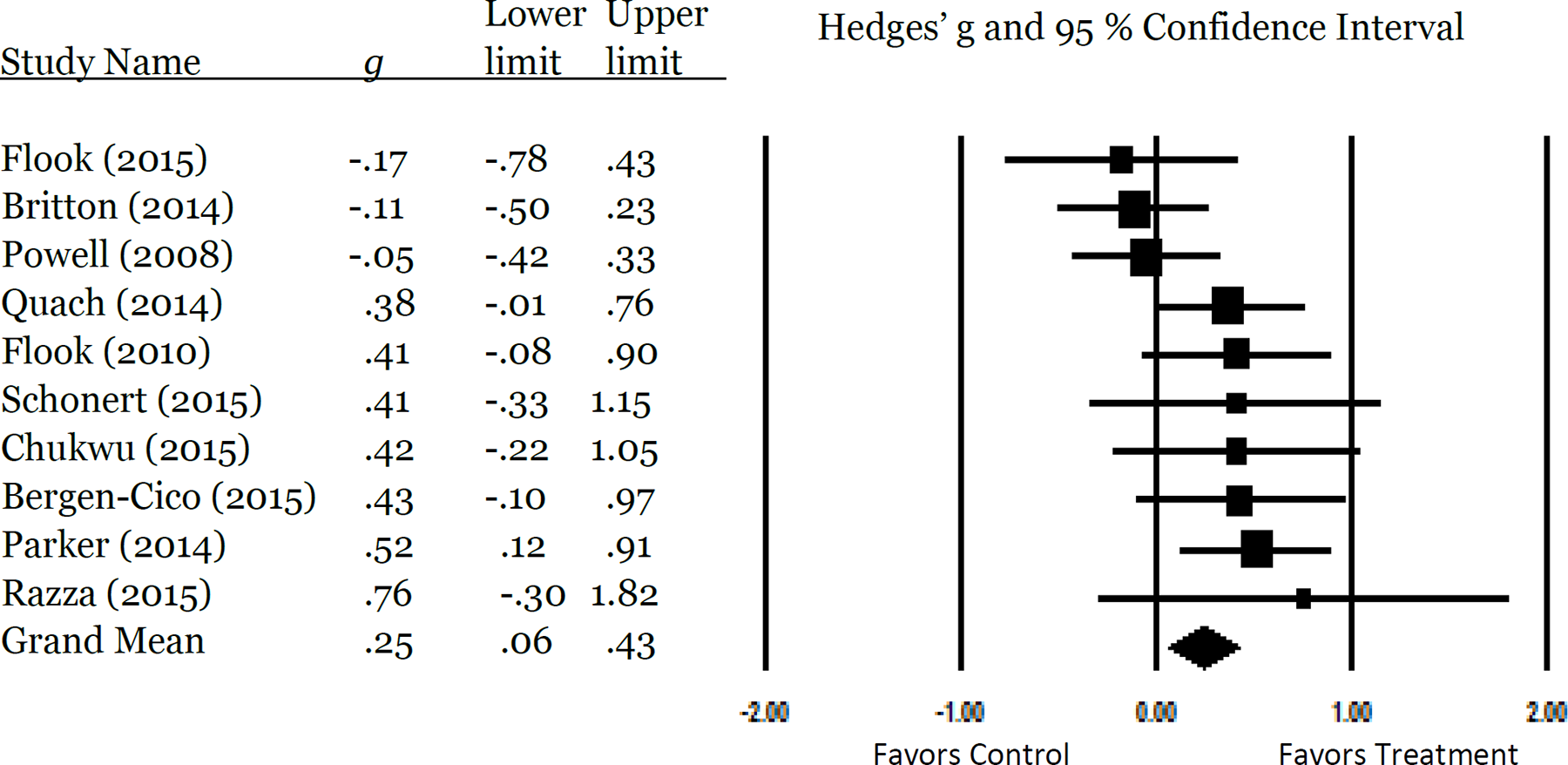
Forest plot of mean effects on cognitiveoutcomes
4.4.2 Mean effects on academic outcomes
Fifteen effect sizes from five studies were synthesized to examine effects on academic outcomes. Results indicate that the overall mean effect (Hedges’ g) at post-test on academic outcomes was 0.27 (95% CI [-0.04, 0.57], p = .08.). Heterogeneity was not significant (I2 = 0%; Tau2 = .00Q = 0.52, p= .97). The mean effect size and confidence intervals for each study are shown in the forest plot in Figure 4.5 below. See Appendix 8.9 for a full list of all measures included in this meta-analysis by study.
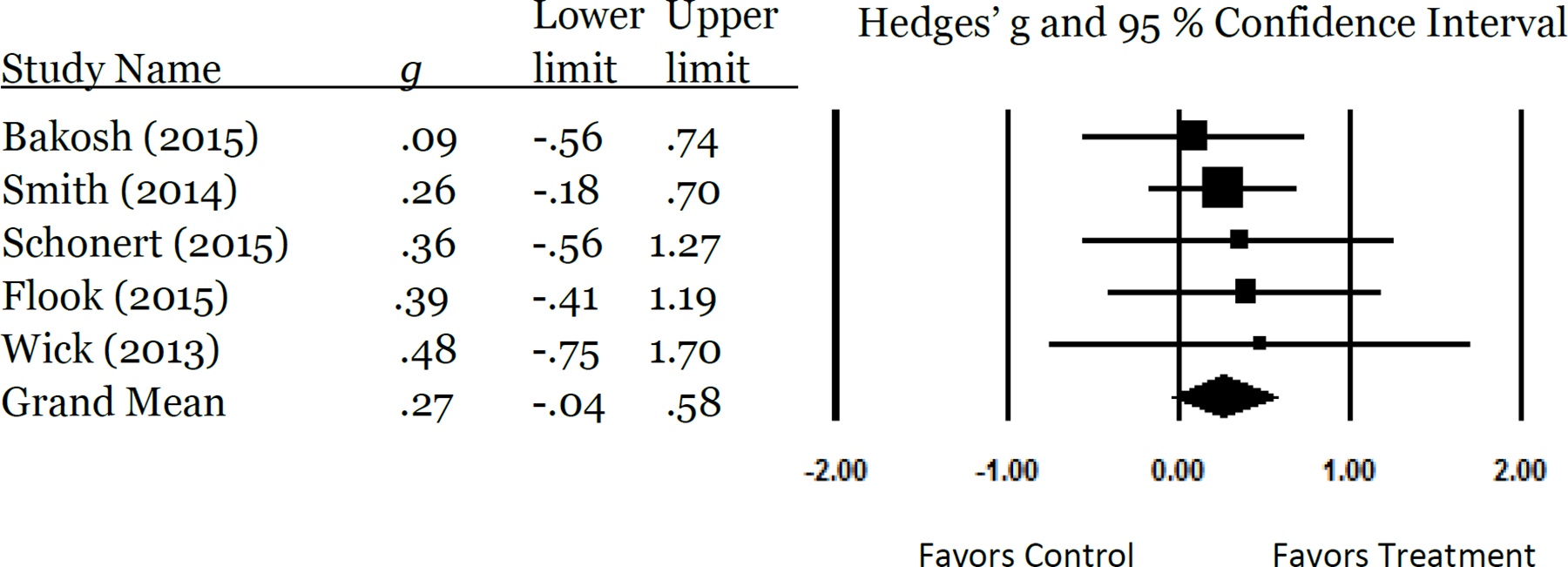
Forest plot of mean effects on adademic outcomes
4.4.3 Mean effects on behavioraloutcomes
Twenty-eight effect sizes from 13 studies were synthesized to examine effects on behavioral outcomes. Results indicate that the overall mean effect (Hedges’ g) at post-test on behavioral outcomes was 0.14 (95% CI [-0.02, 0.30], p = .08). It is important to note that there was a moderate amount of heterogeneity (I 2 = 48%; T2 = .034; Q = 22.96, p = .03). The mean effect size and confidence intervals for each study are shown in the forest plot in Figure 4.6 below. See Appendix 8.10 for a full list of all measures included in this meta-analysis by study.
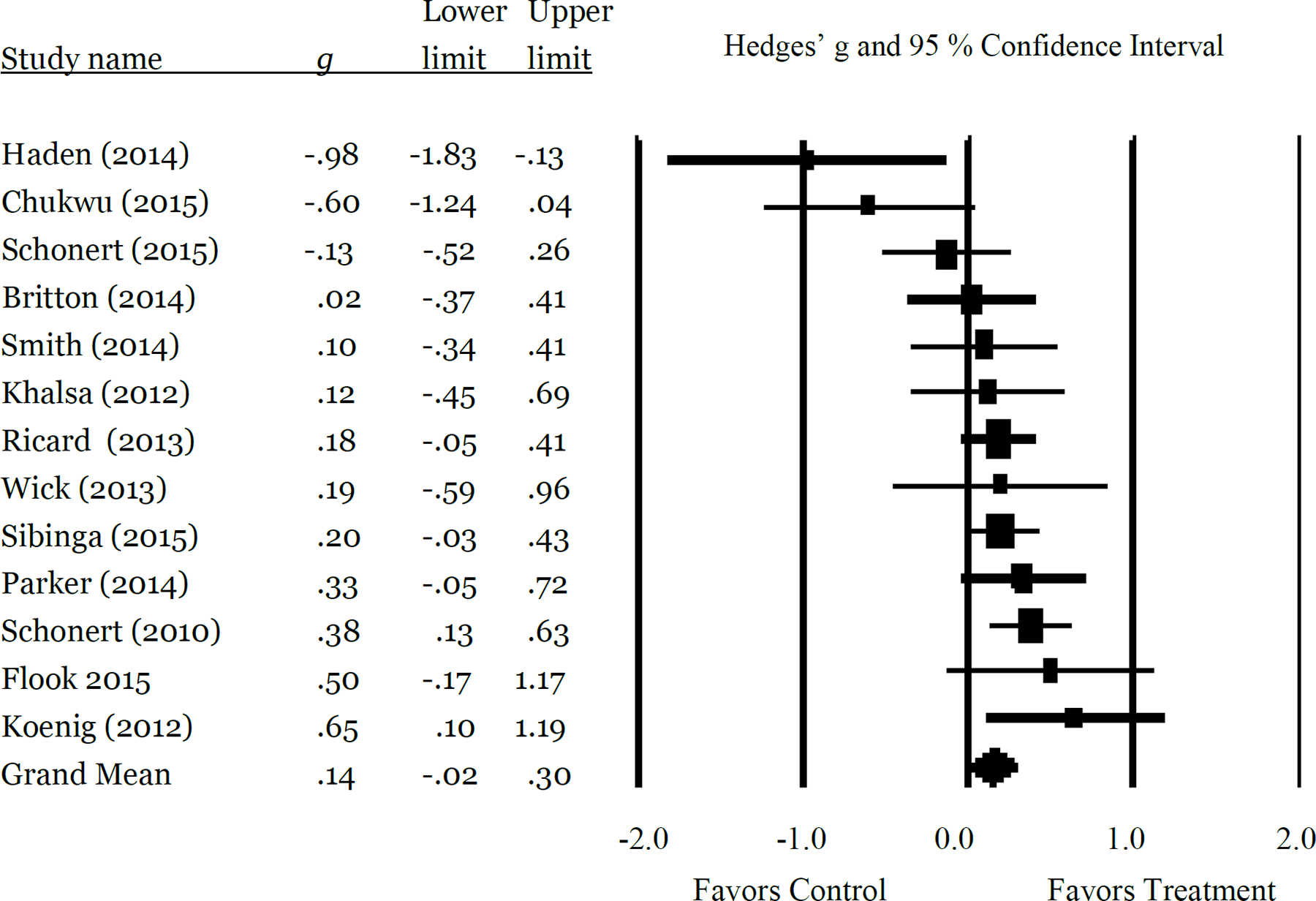
Forest plot of mean effects on behavioral outcomes
4.4.3.1 Moderator analysis for behavioral outcomes
We conducted moderator analyses to examine whether study or intervention characteristics could explain the variation observed across studies. None of the moderators examined were statistically significant: study type (Q b = 3.51; p = .06), provider (Q b = 0.71; p = .40), homework (Q b = 0.28; p = .60), manualized program (Q b = 7.27; p = .06), number of weeks(Q = .003; p = .97).
4.4.4 Mean effects on socioemotional outcomes
One hundred sixty-eight effect sizes from 28 studies were synthesized to examine effects on socioemotional outcomes. Results indicate that the overall mean effect (Hedges’ g) at post-test on socioemotional outcomes was 0.22 (95% CI [0.14, 0.30], p < .001). There was a small amount of heterogeneity (I 2 = 14%; Q = 31.20, p = .263; Tau2 = .01). The mean effect size and confidence intervals for each study are shown in the forest plot in Figure 4.7 below. See Appendix 8.11 for a full list of all measures included in this meta-analysis by study.
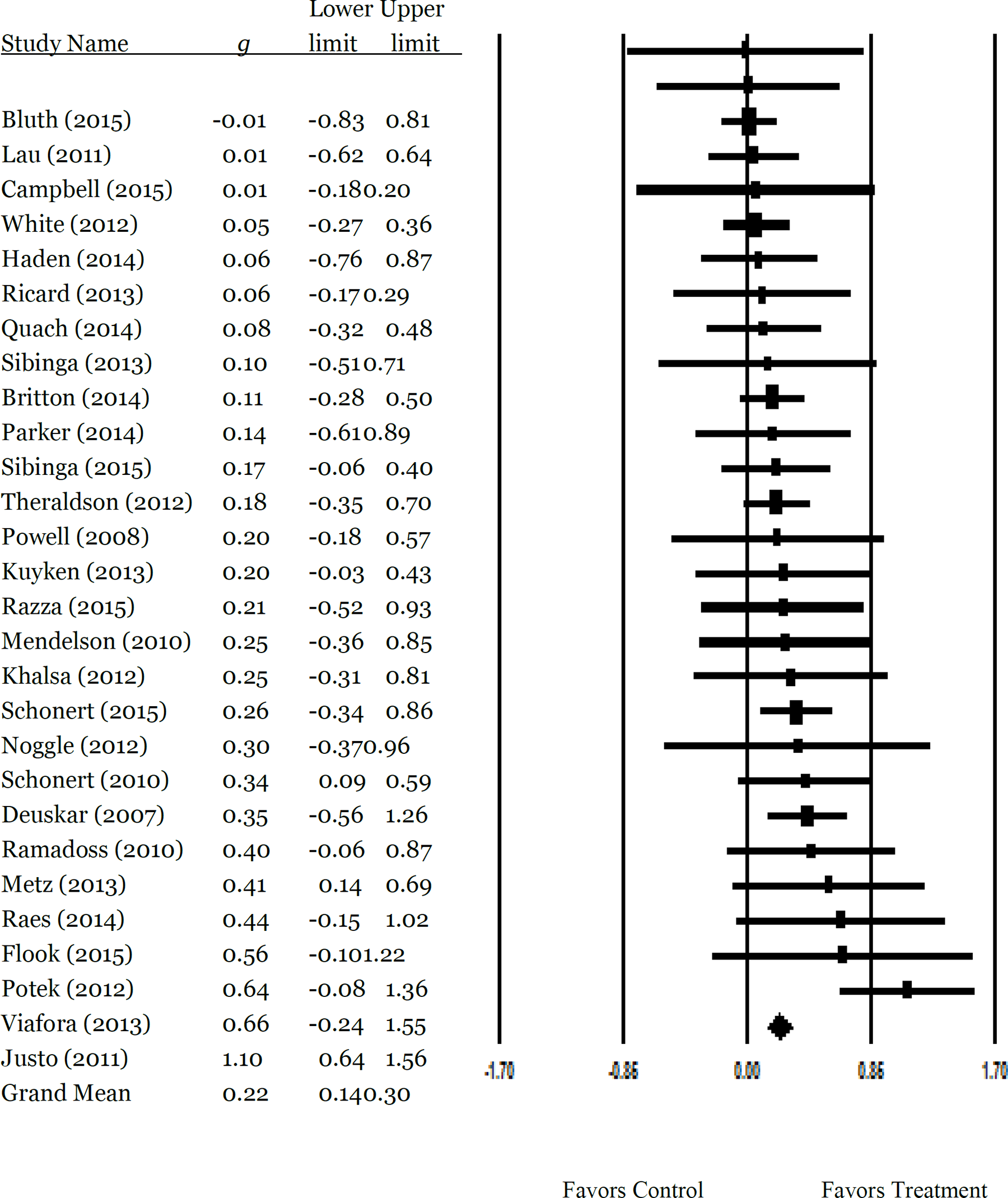
Forest plot of mean effects on socioemotional outcomes
4.4.5 Physiological outcomes
Six studies measured physiological factor in their study; three of those studies were conducted by the same author team (Barnes et al., 2004; Barnes et al., 2008; Gregoski et al., 2011). Two studies measured cortisol; one study measured cortisol at three time points during the day (AM, pre-lunch, and afternoon; Shonert-Reichl, 2015) while the other study measured total cortisol output (Sibinga et al., 2013). One study measured sleep (Sibinga et al., 2013), two studies measured sodium excretion rates (Barnes et al., 2008; Gregoski et al., 2011) and three studies measured systolic and diastolic blood pressure and heart rate (Barnes et al., 2004; Barnes et al., 2008; Gregoski et al., 2011). Due to the nature of these measures, the time dependency of some of these measures (cannot compare AM cortisol to PM cortisol for example), and that so few studies measured these outcomes, quantitatively synthesizing these outcomes across these studies was not warranted.
4.5 PUBLICATION BIAS
There was a sufficient number of studies to examine publication bias for cognitive, behavioral and socioemotional outcomes using funnel plots (see Figure 8.12 in Appendix) and for socioemotional outcomes using Egger's linear regression approach (a minimum of 17 studies is recommended; Card, 2012). In examining the funnel plot for behavioral outcomes, the funnel plot appears relatively symmetrical, but the funnel plot for cognitive and socioemotional outcomes appears to be somewhat asymmeterical, with a larger number of studies clustering on the right side of the funnel. Results of Egger's regression for socioemotional outcomes was not significant (t = 1.76, p = .09), indicating an absence of publication bias in the studies contributing effect sizes for socioemotional outcomes. The funnel plot for cognitive outcomes, however, is less symmetrical, and few small sample studies with small effects were observed, indicating the possibility of publication bias.
5 Discussion
5.1 SUMMARY OF MAIN RESULTS
The present review identified a total of 61 studies that met review criteria, including 44 randomized or quasi-experimental studies and an additional 17 studies that used a single-group pre-posttest design or single subject study design to examine effects of a school-based mindfulness intervention on a cognitive, academic, behavioral, socioemotional or physiological outcome. It is interesting to note that we observed an increase in the number of MBI studies over time, as a higher proportion of the included studies were published more recently. Of the included studies, 35 provided adequate effect size data to be included in a meta-analysis for at least one of the outcomes of interest for this review. Results indicate mixed results of school-based mindfulness interventions across the outcomes of interest in this review, with small positive effects observed on cognitive and socioemotional outcomes and positive, yet non-significant effects on academic and behavioral outcomes. The lack of heterogeneity for all outcomes with the exception of the behavioral outcomes indicate that the interventions in this review, although quite diverse in their characteristics, produced similar results across studies on cognitive, socioemotional and academic outcomes. These findings provide some support for the use of school-based mindfulness interventions for some outcomes, but do not provide overwhelming support of mindfulness interventions as being the panacea as some have advocated. Given the quality and high risk of bias across studies in several areas, caution must be used in the interpretation of the study results.
First, the results of this review largely correspond to what we would expect given the mechanisms by which mindfulness interventions are hypothesized to work. The proximal processes targeted by mindfulness interventions are cognitive processes, which are then hypothesized to impact more distal outcomes—academic, behavioral, and socioemotional outcomes. Our results provide support for favorable impacts of mindfulness interventions on those processes that are likely more directly targeted by mindfulness interventions, namely cognitive outcomes. Socioemotional outcomes may be a more proximal target as well as many of the measures were linked to emotional regulation processes that are invoked in mindfulness training. There is no direct support, at least not at posttest, to indicate that more distal outcomes, such as behavior and academic achievement, which are hypothesized to be impacted through improved cognitive and socioemotional outcomes, are affected by MBIs. It could also be that the effects found for cognitive and socioemotional outcomes may be due to the type of self-report measures typically used to measure these types of outcomes versus the administrative measures used to measure academic outcomes and observational measures to measure behavioral outcomes.
The mixed effects found in this review could be due to several possible explanations. First, as alluded to above, mindfulness interventions are most directly targeting cognitive and psychological/socioemotional processes. Thus, we expected that we would be more likely to find positive effects on those outcomes than behavioral or academic outcomes, which are arguably more distal outcomes. Mindfulness interventions may not be powerful enough to affect cognitive and socioemotional process sufficiently to mediate academic or behavioral outcomes as hypothesized by proponents of MBIs. Alternatively, since the vast majority of participants were not clinical or special needs populations, and were likely functioning within normal ranges across these measures (and thus have less opportunity to improve greatly), there may have been less opportunity for substantial improvement in the populations being studied, and thus small effects observed. Using mindfulness based interventions as a universal intervention with those already in normal ranges on cognitive, socioemotional and behavioral measures may be unnecessary, or perhaps measures need to be more sensitive to smaller changes to find effects when testing MBIs as a universal prevention strategy. It could also be that MBIs may have greater impact with students who are experiencing clinical, or high levels of, distress, anxiety or stress and could then have a greater impact on behavioral and academic outcomes. These issues require further exploration- examining differential impacts of MBIs with clinical versus non-clinical populations could provide some needed nuance to the MBI effectiveness literature.
The MBIs in this review were also shorter-term interventions. It is possible that MBIs may have a greater impact with greater dosage over longer durations. A number of authors and proponents of MBIs often cite the short duration as a limitation in observing effects of mindfulness on various outcomes (Carmody, & Baer, 2008; Carson, Carson, Gil, & Baucom, 2004; Chiesa, Calati, & Serretti, 2011; Jha, Stanley, Kiyonaga, Wong, & Gelfand, 2010), and some studies indicate that a longer duration would have greater effects (Mathew, Whitford, Kenny, & Denson, 2010; Miller, Fletcher, & Kabat-Zinn, 1995). Also, we examined effects of interventions at posttest, thus we are unsure what the longer-term effects of MBIs on proximal and distal outcomes. Academic outcomes are often more difficult to change immediately, and given that the studies in this review measured grades, it may take a longer measurement period to see meaningful change in grades, as well as the other outcomes of interest.
5.2 QUALITY OF THE EVIDENCE
The quality of the evidence varied, with some important risks of bias present across a large proportion of studies which threatens the internal validity of the included studies and is cause for caution in interpreting the results of this review. Overall, a large proportion of included studies presented with a high risk of bias related to allocation concealment and performance bias. In most studies, reporting bias was rated as unclear risk of bias, which is problematic as reporting bias is a potential threat and we could not adequately assess it in this body of literature. Publication bias may also be present in this literature, as some funnel plots were asymmetrical, thus indicating potential for publication bias on at least some of the outcomes. A large proportion of the studies included in this review were conducted by researchers who were likely invested in the programs (involved in development or implementation) and had tacit knowledge of the interventions, and participants and personnel were not blinded in the majority of the studies- thus we are concerned that this body of evidence is biased in favor of the MBIs due to allegiance and experimenter expectancy effects. In examining the results of the meta-analyses, the confidence intervals were fairly wide, with the exception of socioemotional outcomes, which were much narrower. This is reasonable in that we had a much larger number of studies and low heterogeneity across studies included in the meta-analysis for socioemotional outcomes. Thus, we can be more confident in the estimate of the average effect for socioemotional outcomes and less so in the average effect observed for cognitive, academic and behavioral outcomes. Also, a number of studies were confounded and, while the differences in mean effects were not significantly different for those studies that had a confound and those that did not, the magnitude of effects were larger in those that had a confound, and thus could be upwardly biasing the mean effect. Overall, there is room for improvement in the current evidence of effects of school-based mindfulness interventions.
5.3 LIMITATIONS AND POTENTIAL BIASES IN THE REVIEW PROCESS
We made every attempt to search for published studies; however, the majority of the studies included in this review were published journal articles, with approximately 20% being unpublished dissertations. Three of the databases were reviewed by only one of the authors, thus there may be a greater chance of errors in identifying potential studies from these three databases. The review authors did not use a formal method to assess the quality of the body of evidence; the authors did however assess risk of bias and reported on study characteristics that are indicators of study quality. There is some indication of publication bias present, which could be upwardly biasing the mean effect for all or some outcomes examined in this review.
5.4 AGREEMENTS AND DISAGREEMENTS WITH OTHER STUDIES OR REVIEWS
The findings of the present review largely correspond with other systematic reviews and meta-analyses of MBIs with children and youth. Narrative reviews, including those by Meiklejohn and colleagues (2012), Greenberg and Harris (2012), and Thompson and Gauntlett-Gilbert (2006) concluded that mindfulness-based approaches were feasible and promising, but cautioned that additional and more rigorous research was needed. Findings from a systematic review of 15 studies (6 between-group designs) of mindfulness-based approaches with children and adolescents (Burke, 2010) concluded that the studies provided evidence of the feasibility and acceptability of mindfulness-based approaches for children and adolescents, but the research base was limited by a lack of rigorous efficacy studies. Finally, two meta-analyses of MBIs with children and youth found positive and significant effects of MBIs on primarily psychological outcomes. Zoogman et al., (2014) reported a synthesis of studies examining mindfulness meditation with youth across outcomes, including psychological and non-psychological symptoms (specific outcomes are not reported). The search was conducted in 2011 and was limited to peer-reviewed journal articles published in English. Twenty studies (13 RCTs, 1 QED, and 6 within group pre-post test studies) were included in the review, yielding an overall mean effect of 0.227 [CI 0.148, 0.305], with lager mean effects found across studies using clinical samples compared to studies using non-clinical samples. Zenner and colleagues (2014) conducted a systematic review and meta-analysis of mindfulness-based interventions in schools with a focus on psychological outcomes. The authors conducted a search in 2012 for published and unpublished reports yielding 24 studies (10 RCTs, 8 QEDs, 1 two-armed cohort study, and 5 non-controlled trials). The mean effect across all outcomes of the 16 studies using a comparison group design was g = 0.40 [0.21, 0.58], with significant heterogeneity between studies. In the current meta-analysis of socioemotional outcomes (the outcome category that most closely aligns with the Zoogman et al. and Zenner et al. reviews), the mean effect of 0.21 is similar to the mean effect of 0.227 estimated by Zoogman et al. and smaller than the mean effect estimated by Zenner et al. The differences in mean effects between the present review and Zoogman et al. could be due to the inclusion of different outcomes, studies and effect size estimation procedures. The present review provides the first synthesis of effects specifically on cognitive, academic and behavioral outcomes in addition to the socioemotional outcomes reported in prior reviews.
6 Authors’ conclusions
6.1 IMPLICATIONS FOR PRACTICE AND POLICY
The number and types of MBIs being implemented in schools is expanding significantly, and intervention research is beginning to shed more light onto the effects and mechanisms of mindfulness interventions on a range of outcomes. Up to this point, much of the arguments and enthusiasm for the broad implementation of mindfulness-based approaches with children, as well as those in schools, have been predicated on generalizing the positive evidence from mindfulness research with adults and from expert opinion, or the use of cherry-picking studies in favor of MBIs to promote mindfulness interventions with children. This review adds to the body of evidence examining MBIs for children, and for the use of MBIs in school settings specifically. While the results of this review found positive effects favoring mindfulness interventions on cognitive and socioemotional outcomes, we urge caution in the use of these findings to support further implementation of MBIs in schools.
Schools often justify the implementation of socioemotional programs, including mindfulness-based training, on the premise that those programs will, in turn, promote positive behavior and improve academic achievement. The evidence to support MBIs to improve behavioral and academic outcomes, at least in the short-term, is not yet supported by the evidence. There is also seemingly widespread belief that MBIs, given the positive effects with adults, have great potential for direct and indirect benefits for students. Moreover, those who argue for an expansion of MBIs with children do not adequately, if at all, consider the costs or potential negative effects. Although rarely discussed and more rarely studied, adverse effects of mindfulness and meditation are gaining more attention, as Willoughby Britton, a mindfulness researcher at Brown, has begun to map and analyze accounts of harmful effects of contemplative practices, which include mindfulness and meditation (Rocha, 2014; Britton & Lindahl, 2015), through interviews with meditation teachers and practitioners from across a range of contemplative practice traditions. Some of her preliminary findings indicate that meditation can result in difficult or challenging experiences and cause or worsen symptoms. None of the studies included in this review measured potentially adverse outcomes, and if they didn't find positive effects, authors were more likely to provide justifications for why their intervention did not work rather than to consider that their intervention was not effective. There were exceptions to this, however. For example, Tharaldsen (2002) found that participants in their study experienced deterioration in life satisfaction and no improvement in psychological symptoms. They considered the possibility that their results “may be a result of an increased focus on troublesome emotions due to awareness training and a maladaptive use of distraction skills that lead to avoidance” and that “certain aspects of mindfulness can be more confusing than beneficial to adolescents” (Tharaldsen, 2012, p. 120). Indeed, children and adolescents may not benefit from mindfulness-based interventions similarly to adults, and there may be some adverse effects, because children and adolescents may not be developmentally ready for the complex cognitive tasks, focus and level of awareness that mindfulness-based interventions require (Melbourne Academic Mindfulness Interest Group, 2006; Shapiro, 1992).
There are also direct and indirect costs in implementing these interventions, and the cost-benefit of mindfulness-based intervention is largely ignored. The direct costs of implementing mindfulness-based interventions are those that are obvious to the implementation of any intervention in schools, namely the cost of materials and personnel needed to implement the intervention. The included studies did not provide sufficient information to calculate the total cost of the interventions that schools would be responsible for if they were to adopt these interventions. Indirect costs, but nonetheless important, are opportunity costs, specifically the cost of lost instructional time or not implementing something else that could be more effective (Melbourne Academic Mindfulness Interest Group, 2006). Some of these interventions were very short in duration, in that they only took up a few minutes of the school day on a daily basis and thus resulted in little lost instructional time. However, other interventions used more class time, or even an entire class period. It is unclear if the small effects gained from these interventions on cognitive and socioemotional outcomes are worth the lost instructional time. If the primary focus of schools is to enhance academic outcomes, then using instructional time to provide a universal MBImay not be a good use of time, considering that we found a lack of evidence for significant effects on academic outcomes. However, there remains yet much we do not know about the effects of MBIs, specifically whether students near or in the clinical range of anxiety or other emotional disorders may benefit more than students in the general population of the school. Prior reviews found some evidence for greater effects with children and adolescents from clinical populations (Zoogman et al., 2014), and thus there may be some students for which MBIs may be worth the cost and time.
Overall, the evidence from this review urges caution in the enthusiasm for, and widespread adoption of, MBIs for children and youth—specifically for use in schools. While the evidence points to positive effects on socioemotional and cognitive outcomes, there is a lack of evidence of effects on academic and behavioral outcomes. Moreover, we know little about the costs and adverse effects of school-based mindfulness interventions. The costs of implementing these programs may not be justified, and there are some indications that MBIs may have some adverse effects on children and youth that have not received adequate attention. If schools do want to implement MBIs, we urge schools to evaluate the practice in a rigorous way and monitor outcomes and costs.
6.2 IMPLICATIONS FOR RESEARCH
The number of studies examining effects of MBIs have expanded considerably, particularly over just the past few years. Clearly, there is much interest in examining the effects of school-based mindfulness interventions. However, a large proportion of studies in this review were conducted by authors who clearly had some involvement in the development, adaptation, or delivery of the intervention and thus were not independent evaluators. Moreover, several of the studies were funded by bodies that had an interest in the success of the MBIs being evaluated. Overall, authors engaged in the evaluation of school-based mindfulness interventions appear to be largely biased in favor of mindfulness interventions. This is problematic in that studies in which authors have some allegiance to the intervention or are otherwise involved in the development or implementation of the intervention are more likely to find positive effects than studies that are not conducted by authors with a vested interest in the outcomes of the interventions. The large proportion of studies in which authors had some role in the development and delivery of the interventions under investigation in this review may have biased the mean effect in favor of mindfulness interventions and overestimated the effects of these interventions. Moreover, the tacit knowledge that researchers who develop or implement the interventions they are testing may positively skew the outcomes in such a way that would not be replicable if someone with less knowledge or investment were implementing the intervention. It is recommended that future evaluations of MBIs be conducted by an independent third party investigator, and when possible, that personnel and assessors be blinded to group assignment.
Also, a significant number of studies in this review had major and troublesome confounds that clearly limits the extent to which we can draw causal inferences from this body of research. For each outcome examined in this review, all studies with confounds were biased in favor of the treatment group, thus resulting in an upward bias of the mean effect across studies. Future studies should avoid confounds in their study designs.
Other important areas in which to further develop school-based mindfulness intervention research is to move beyond mean effects of interventions and begin to explicitly examine the mechanisms of change (e.g., what are the pathways and mediators), which components of mindfulness interventions are effective and/or necessary (e.g., is home practice necessary and how much? Does yoga/movement enhance mindfulness practice), what works for whom and under what circumstances, and examine adverse effects of these interventions.