
Abstract
This Campbell systematic review examines the effectiveness of teenage pregnancy prevention programs in promoting abstinence, encouraging the use of contraception and reducing the likelihood of pregnancy among teens.
A thorough literature search was conducted up to April 2006. The review summarises findings from 31 studies which included 37,000 youth conducted in the US or in developed countries with higher than average rates of unplanned teen pregnancy, such as Canada, England, New Zealand, and Australia.
This review finds no consistent evidence that the types of pregnancy prevention programs evaluated rigorously to date will alter in intended ways the sexual activity or pregnancy risks of youth. However, this overall pooling of studies mixes results of different program types serving different populations of adolescents.
This review highlights the relative dearth of evidence to judge the overall effectiveness of particular intervention strategies. For this reason, further research and evaluation is necessary, including studying programs that have not yet been evaluated rigorously and programs that have been replicated and are serving new populations of adolescents in different communities.
Linked article:
ACKNOWLEDGEMENTS
Financial support for this review was provided by the Smith Richardson Foundation, the William and Flora Hewlett Foundation, and from the American Institutes for Research (through funding from the U.S. Department of Health and Human Services).
Many individuals contributed in important ways to the conception and conduct of this review. This includes several individuals who were pursuing other reviews under a collaborative effort supported by the Smith Richardson Foundation and the William and Flora Hewlett Foundation to improve the methods for and expand the application of systematic reviews in education, criminal justice and social welfare. These include, Mark Lipsey, Jeff Valentine, Harris Cooper, Steve Glazerman, David Myers, and Anthony Petrosino. Several colleagues at the Urban Institute and at the University of Pennsylvania aided in the coding of studies and provided various other forms of support throughout the review process. We are especially grateful to Jane Reardon-Anderson, Jennifer Macomber, Cay Bradley and Susan Zief for this ongoing help. The Campbell Collaboration reviewers provided timely and valuable feedback on both the protocol and the review. Finally, we are especially appreciative of the ongoing guidance and support we received throughout the process from the Campbell Collaboration Social Welfare Coordinating Group editors—Geraldine MacDonald and Julia Littell.
EXECUTIVE SUMMARY
This review synthesizes the evidence on the effectiveness of programs aimed at reducing sexual risk-taking among teens. By including only rigorous randomized controlled trials that meet additional methodological criteria, it uses meta-analytic techniques to estimates the average effects that interventions have on reducing sexual experience, unprotected sexual activity, and pregnancy rates. It focuses on four main types of interventions: (1) one-time consultations; (2) sex education programs with an abstinence focus (and no contraceptive focus); (3) sex education programs with a contraception component; and (4) multi-component youth development programs. In total, this review presents findings based on over 37,000 youth who were the subjects of 31 studies that reported on a total of 38 randomized trials of interventions aimed at reducing teen sexual activity and pregnancy.
This review finds no consistent evidence that the types of pregnancy prevention programs evaluated rigorously to date will alter in intended ways the sexual activity or pregnancy risks of youth. However, this overall pooling of studies mixes results of different program types serving different populations of adolescents. When looking more specifically by intervention type, the following results were found: Too little evidence to make specific judgments about one-time consultations. Limited evidence regarding sex education programs with an abstinence focus. Studies evaluated rigorously showed pooled statistically significant effect favoring the control group on pregnancy rates. However, none of the rigorously evaluated programs is representative of abstinence-only programs that have grown in popularity over the course of the past decade, and thus these results cannot be used to generalize to the broader set of abstinence focused interventions currently in operation. No consistent evidence that that sex education programs altered the likelihood that youth would initiate sex, would risk pregnancy, or would become (or get someone) pregnant. Notably, there is great variability in the nature of the programs included within this category, as well as a high degree of variability in the size, direction, and statistical significance of the impact estimates for the various programs. However, a number of individual studies have found positive program effects, particularly related to increased contraception use, and have been considered by advocates to be models to be replicated (Solomon and Card, 2004). As more replication study results become available, it will be possible to pool more similar programs to assess systematically the effects of particular program models. The most promising results are for the more intensive multi-component youth development programs serving higher risk adolescents. Moreover, within this category, the results tend to be most favorable for females. However, there is a paucity of rigorous evaluations of such programs, and further replication and evaluation is warranted.
While the body of knowledge in this field is continually growing, this review highlights the relative dearth of evidence to judge the overall effectiveness of particular intervention strategies. For this reason, further research and evaluation is necessary, including studying programs that have not yet been evaluated rigorously and programs that have been replicated and are serving new populations of adolescents in different communities. Once a larger body of more similar programs have been evaluated rigorously and reported consistently, then it will be possible to pool the evidence to make more concrete conclusions regarding program efficacy.
BACKGROUND
This review examines the effectiveness of teen pregnancy prevention programs in delaying first intercourse, in reducing the likelihood teens will engage in intercourse without using contraception, and in reducing the likelihood of pregnancy among teens. The review also examines evidence regarding the relative effectiveness of different types of and settings for interventions. Teens who become pregnant, and especially those who give birth at a young age, face negative economic and social consequences, both in the short-term and as they transition to adulthood (Maynard, 1997; McLanahan, 1994; Moore et al, 1993). Although the rates of teen sexual activity, pregnancy and births in the United States have fallen over the past decade, they remain high and, by a considerable margin, the U.S. rates are the highest of all industrialized countries (Centers for Disease Control and Prevention 2005; Darroch et al., 2001a). The persistently high rates of sexual activity, pregnancy rates, and births among teens in the U.S., in particular, has led to a wide range of programmatic initiatives aimed at reducing teen pregnancy and birth rates. Most of these strategies promote abstinence from sexual activity. Some programs focus mainly on promoting contraception. But, most often, programs encourage abstinence, but also promote contraception among sexually active teens.1
Extensive research has been conducted exploring the antecedents to heterosexual risk-taking behaviors. For example, the research has identified numerous correlates of sexual-risk taking among teens, including community characteristics; school characteristics; family characteristics; biological factors; psychological factors; relationships with peers, parents, and school; as well as attitudes and beliefs concerning sex (Bearman et al, 1999; Blum et al, 2000; Costa et al., 1996; Jaccard et al. 1996; Kirby, 2001; Miller, 1998; Resnick et al., 1997; Weinstein and Thornton, 1989; and Wu and Martinson, 1993). These findings have guided program and policy decisions regarding the design and targeting of pregnancy prevention interventions.
The policy response to adolescent sexual risk-taking in the U.S. and other developed countries with relatively high rates of teen pregnancies has been similarly varied. Interventions implemented over the past few decades have emphasized different combinations of the antecedents identified above. Furthermore, these various intervention strategies have been implemented by a multitude of actors, ranging from schools to community-based organizations to religious organizations (U.S. Department of Health and Human Services, 2000; Sonfield and Gold, 2001).
Policymakers, researchers, and practitioners have engaged in ongoing debates concerning the content and timing of pregnancy prevention programs. Specifically, two major issues have engendered considerable controversy: (1) whether sex education programs should have an abstinence-only focus or whether such programs also should include information and education on contraception, and (2) whether pregnancy prevention programs should be aimed at younger versus older teens. To date, no consensus has emerged from the literature regarding either the effectiveness of particular intervention strategies or their implementation in particular settings.
Twenty (20) reviews of evidence on the effectiveness of teen pregnancy prevention programs conducted over the past decade yield inconsistent conclusions (see Table 1). The reviews differ in their criteria for including studies and how they analyze the results of included studies. One important difference among reviews is whether they include only findings of randomized controlled trials, both randomized control trials and quasi-experimental design studies, or all studies (including those with no matched control group). A few of the reviews included statistical meta-analyses. However, most provided only a narrative description of findings. Finally, some of these reviews are outdated and some have a primary focus that differs from this review. In general, among the more recent reviews that narratively pool studies, there is a growing consensus that certain programs and program components appear to be effective.2 However, no consistent meta-analytic results, to date, have validated these claims.
This review seeks to improve upon the prior reviews in six ways. First, this review focuses on a clear and policy relevant set of questions in terms of both the interventions and the outcomes. It focuses only on interventions with a primary goal of reducing heterosexual risk-taking behaviors and that measure at least one of three key outcomes: (1) sexual experience (ever had vaginal sexual intercourse), (2) pregnancy risk (unprotected sexual intercourse versus either intercourse with contraceptives or abstinence), and/or (3) pregnancy.
Second, this review statistically pools findings from evaluations of programs operating in a broader set of geographical contexts than have most prior reviews. Yet, the review is restricted to programs that have operated in developed countries with relatively high rates of unplanned teen pregnancy.
Third, this review includes only those studies with a reasonable potential for generating credible (internally valid) findings. Specifically, the review includes only well-designed and reasonably well-implemented randomized control trials (RCTs). However, the review findings are complemented by an exploratory analysis of the sensitivity of the review findings to the inclusion of outcomes from reasonably well-implemented quasi-experimental design studies.
Fourth, this review explores differences in outcomes among clusters of programs defined by seemingly important programmatic features. These features include dimensions of program content, intensity, and implementation setting.
Fifth, this review evaluates the extent to which the research base adequately represents the range of programs currently in operation and it assesses the appropriateness of combining impact estimates across and within various types of interventions. Toward this end, we inventory strategies to prevent teen pregnancy (based on summary reports by government and non-government entities) and compare this with the range of program types and settings for which there is credible evidence of the impacts, in order to gauge the generalizability of the current corpus of evidence.
Finally, this review maintains a list of those studies that have been excluded due to data limitations and study quality considerations and provides information on the primary reasons for their exclusion.
Findings Reported in Narrative Reviews and Meta-Analyses of Programs Designed to Affect Adolescent Heterosexual Risk-taking Behaviors
OBJECTIVES OF THE REVIEW
This review summarizes the evidence regarding the effectiveness of interventions designed to reduce heterosexual risk-taking behaviors and pregnancy among adolescents. Specifically, this review explores the following questions: What is the corpus of evidence regarding the effectiveness of programs aimed at reducing heterosexual risk-taking behaviors and pregnancy among teens? What types of programs have been rigorously evaluated and how representative are these programs to the range of programs that exist? What are the estimated study-specific and average impacts on sexual experience (ever had vaginal sexual intercourse), pregnancy risk (unprotected sexual intercourse versus either intercourse with contraceptives or abstinence), and pregnancy? What are the estimated study-specific and average impacts of the four main types of interventions that have been studied in randomized control trials: (1) one-time consultations; (2) sex education programs with an abstinence focus (and no contraceptive focus); (3) sex education programs with a contraception component; and (4) multi-component youth development programs? What are the estimated impacts of programs targeted at different age groups of youth? What are the estimated impacts of programs for males and for females? How sensitive are the results to key aspects of study quality? How would the results of this review have differed had they included evidence from quasi-experimental design studies?
METHODOLOGY
This review was conducted following a protocol approved by the Campbell Collaboration (http://www.campbellcollaboration.org/doc-pdf/scherteenpregnancyprot.pdf). This protocol specifies in advance of the review the criteria for including or excluding studies, the search and coding procedures and the research synthesis methods.
Study inclusion criteria
This review includes all studies identified through an extensive search of the literature (published and unpublished) that meet nine criteria:
Search procedures
A broad-based, thorough literature search was conducted for this review in Fall 2002 and this search was updated in Spring 2006. Our search strategy made use of electronic data bases, hand searching of journals, internet searches, and personal contacts. All searches focused on documents written or published from 1980 until April 2006.
Databases searched included: Cochrane Controlled Trials Register; Database of Abstracts of Reviews of Effectiveness (DARE) (evidence-based medicine); Dissertation Abstracts; Franklin (University of Pennsylvania library book search); Econlit; ERIC; HealthSTAR; Index to Current Urban Documents; International Bibliography of the Social Sciences; Inter-university Consortium for Political and Social Research (ICPSR); MEDLINE; The National Criminal Justice Reference Service Abstracts Database; PolicyFile; POPLINE; PsychInfo; Public Affairs Information Service (PAIS International); Sage Family Studies Abstracts; Social Science Electronic Data Library; Social Science Research Network; Social Services Abstracts; Social Work Abstracts; and Sociological Abstracts. Within each database, we searched on the following (pregnancy or pregnant) AND (evaluation or adolescent or teen or prevention) (sex AND education) (sex education) AND (evaluation or adolescent or teen or prevention) abstinence AND (evaluation or adolescent or teen or prevention) clinic AND (evaluation or adolescent or teen or prevention) (HIV or AIDS) AND (evaluation or adolescent or teen or prevention)
The first author collected and reviewed abstracts for all seemingly relevant studies. If the abstract appeared appropriate, then the full study was obtained and reviewed.
In addition, the first author and a graduate student hand-searched titles and abstracts from 1995 to April 2006 from the following ten journals: AIDS Education and Prevention; American Journal of Public Health; Family Planning Perspectives (currently known as “Perspectives on Sexual and Reproductive Health); Journal of Adolescent Health; Journal of Adolescent Research; Journal of Health and Social Behavior; Journal of School Health; Journal of Sex Research; and Pregnancy Prevention and Youth. Other sources of data collection included: the use of personal contacts, examining reference lists from prior reviews, and basic internet search engine queries.7
Data extraction and coding
Data extraction. Based on information in the titles and abstracts, all potentially relevant studies were retrieved and reviewed to determine their appropriateness for the review. Bibliographic information and basic information concerning both the study design and intervention were coded for all studies retrieved. For those studies not meeting the review criteria, reasons for rejection were coded; and, for those meeting the inclusion criteria, detailed information about the intervention, the study design and implementation, and the outcomes were coded.8
Data coding and reliability. Two individuals coded the first five studies to resolve differences in coding decisions and clarify coding policies. Thereafter, a random sample of the studies (20 percent) was selected to be double coded. Reliability was based on the consistency of coding in the 20 percent sample.9
Data inconsistencies. There were occasions where multiple reports were available concerning specific RCTs. In most of these cases, earlier reports either represented a smaller subgroup of adolescents or followed the larger group over a shorter follow-up period. In such cases, we resolved these discrepancies by focusing on the largest sample for the longest follow-up period, meaning the last follow-up that retained at least 60 percent of the original study sample. In two cases where inconsistencies across reports still occurred, we attempted to reach the primary study authors, but were not able to resolve discrepancies in such a manner. In these cases, we chose to focus on the most recent usable information available.
Study yield
One primary researcher [LS] conducted the literature search, with the assistance of a graduate student. Two primary researchers [LS and RM] discussed and resolved issues when there were controversies or questions concerning study inclusion. The database search strategy yielded over 2,000 “hits.” Many of these hits were duplicative or were ruled out upon review of the titles.
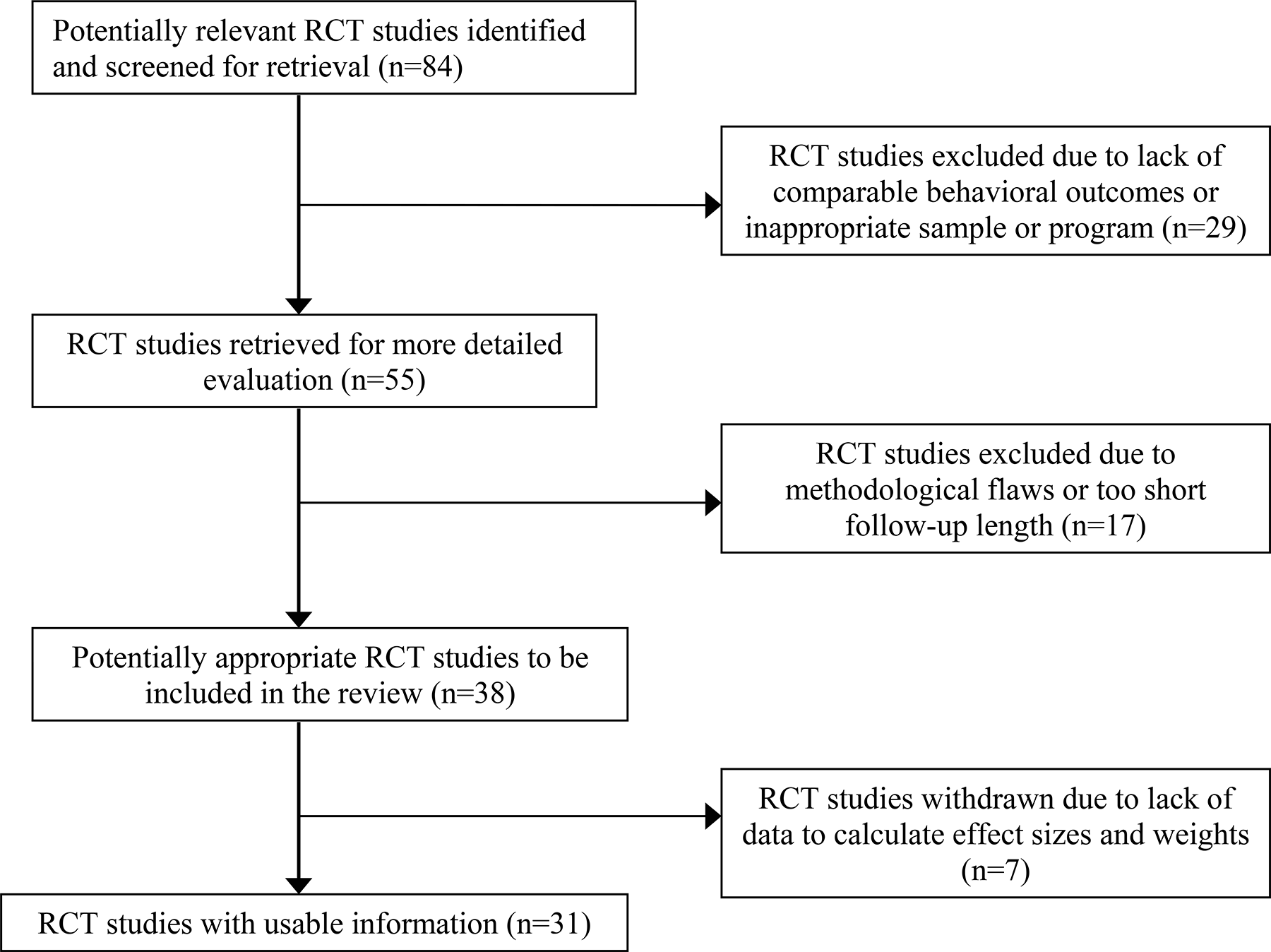
A total of 286 abstracts were reviewed. Of these, 84 were randomized controlled trial studies. Of the RCT studies, 29 were excluded due to a lack of behavioral outcomes or due to inappropriate samples (for example, programs targeting primarily college-aged adolescents) or program types (for example, reducing sexual activity not a primary focus of the program) (Figure 1).
Seventeen of the remaining studies were then excluded due to significant methodological flaws such as only partial randomization or too short a follow-up period. Finally, seven studies met all of our inclusion criteria, but either did not provide sufficient sample size data to calculate effect sizes and weights. Thus, ultimately, 31 studies were included in the review.
Appendix A provides detailed characteristics these 31 studies, sorted by intervention type. For each study, it describes the intervention, documents the research sample and analysis strategy, and presents both the author's original findings and notes any differences between these findings and the findings presented in this review. Appendix B provides a list of the excluded randomized control trials and describes the primary reasons for exclusion.
Number of Randomized Controlled Trials Included and Excluded from the Review
Outcomes and the numbers of impact estimates identified
This review analyzed findings for three outcomes—sexual experience, pregnancy risk, and pregnancy. For ease of interpretation, all three outcome measures are dichotomous and, thus, are reported as percentages and percentage point differences. The specific definitions of the outcome measures reported in this review are as follows:
Sexual experience: The percent of youth in the program and control groups who reported in their follow-up surveys having ever had vaginal sexual intercourse. In total, 40 independent estimates of program impacts on sexual experience rates were reported in 21 separate studies.
Pregnancy risk: The percent of youth who, at follow-up, reported engaging in sexual intercourse but not using an effective method of contraception.10 Primary studies often assess contraception use only for the sub-sample of adolescents who are sexually active at follow-up. This measure may have confounding effects if the program changed youth's decisions regarding sexual experience. The “pregnancy risk” measure considers all non-sexually active youth as not at “pregnancy risk.” There are 34 independent estimates of program impacts on pregnancy risk from 24 studies.
Pregnancy: The percent of female sample members who, at follow-up, reported that they had ever experienced a pregnancy or the percent of male sample members who reported causing a pregnancy. There are 25 independent estimates of program impacts from 13 separate studies.
Self report. Nearly all of the outcomes measured in primary studies are based on adolescent self-reported sexual behaviors. Evidence from other studies indicates that use of self reports could lead to systematic under or over-reporting, depending on the particular samples being surveyed, the method of obtaining reports, and the wording of questionnaires (Sonenstein, 1997; Catania et al., 1996, Card, 1993). However, in general, there is no reason to expect differential under- or over-reporting between the intervention and the comparison groups.
Multiple follow-up waves. In cases where a study reported outcomes for multiple waves of follow-up, this review includes data for the latest follow-up for which a minimum of 60 percent of the baseline sample has been retained. Sensitivity analysis was conducted to assess whether there would be differences in pooled estimates depending on whether the first follow-up results or those for the most recent follow-up measure with the 60 percent minimum response rate was used. Generally, the results were robust to the reference period for the outcome measures used. However, as will be discussed in the results section, differences across studies can vary depending on the length of follow-up. Because the subset of studies that provide multiple effect sizes over time is limited, we do not have the ability to explore this issue in detail. These findings do suggest a need for future analyses of effects within and between studies across follow-up periods once more studies with outcomes over time become available.
Multiple independent estimates. Multiple measures of an outcome from a study are included only in those cases where multiple randomized trials were conducted within a study or where outcomes were reported separately by gender. In all but one study that had multiple treatments with a shared control group, only one treatment/control comparison was included in a pooled estimate. Appendix C presents separate impact estimates for the three studies that had multiple treatments with a shared control group, and describes the rational for the selection of comparisons included in pooled estimates. In one study (Sikkema et al., 2005), two intervention groups shared controlled group. Since the two interventions are of different program types, we included both treatment/control comparisons in our analysis since the pooled effects by program type (the focus of our analysis) are independent. The effect size for all studies combined includes a weighted average of the effects.
Clustered randomized trials. In studies using clustered randomized designs (i.e., randomizing groups such as classrooms or schools), we have adjusted the standard deviation to account for between-group variation. As a result, the level of statistical significance that we report is more conservative than that reported in an original study that used a clustered randomized trial design, but did not account for clustering in the analysis. Since none of clustered-randomized trials in this review provided the between-group and total variance estimates needed to adjust the statistical significance, we relied on our own estimates from the nationally representative sample of adolescents clustered in schools represented in the Longitudinal Survey of Adolescent Health to make adjustments to author-reported significance levels. In doing so, we applied the adjustment methodology used by the What Works Clearinghouse (http://www.whatworks.ed.gov). Discrepancies between our results and findings from the original authors due to this cluster adjustment are noted in analysis tables and in Appendix A.
Pooling methods. The review tabulates the full set of findings from all studies meeting the review criteria and computes and reports the results of statistical meta-analyses of the findings overall and for subgroups of studies by program type. Overall and subgroup pooled impact estimates were computed using Comprehensive Meta-Analysis random effects estimation models (Hedges & Vevea, 1998; Borenstein & Rothstein, 1999). Throughout this analysis, statistical significance at alpha=.10 level was determined using a two-tailed t-test since the expected direction of program effects is uncertain. We chose the less conservative alpha=.10 threshold in order to detect any evidence of effect based on prior research on the topic suggesting potentially modest effects might appear in either direction.
FINDINGS
In total, this review presents findings based on over 37,000 youth who were the subjects of 31 studies that reported on a total of 38 randomized trials of interventions aimed at reducing teen sexual activity and pregnancy (Table 2). Most of the interventions included in this review were school-based and very limited in duration. Only six of the 31 studies included programs with more than 30 hours of service. The majority of the interventions targeted middle school youth, among whom percentages having sexual intercourse prior to the intervention ranged from 4 to 45 percent. However, nine of the studies focused on high school youth who tended to report relatively higher baseline rates of sexual intercourse ranging from 37 percent to 100 percent (Table 2, page 1, column 4). Most of the interventions served both males and females. However, eight studies focused on interventions for only males or females (Table 2, page 1, column 3).
Characteristics of Studies included in the Review
Notes:
A program is labeled as predominantly serving a particular gender if more than 90 percent of the sample is of one gender.
A program is labeled as serving middle school or high school aged adolescents if it specifically targeted younger or older adolescents. If all school-aged adolescents were targeted, then the program is labeled as “mixed.”
Response rates reported in this table are based on the data available for use in the meta-analysis. Response rates therefore may be slightly different from primary authors' reported response rates that are documented in Appendix A.
Follow-up length noted in this table is based on the latest follow-up with less then 40 percent sample attrition. Appendix A describes all of the follow-up lengths, regardless of sample attrition. Also, information in this table varies from published reports noted in Appendix A when primary authors calculated follow-up length from a program's conclusion rather than baseline.
Outcomes included in this table are only those that met the criteria for inclusion in the meta-analysis. In some cases, outcomes reported in the primary studies (note in Appendix A) are excluded from this meta-analysis for one or more technical reasons such as response rates falling below the threshold applied for this review.
Separate baseline sample sizes and response rates were not reported the two sets of programs randomized at the classroom level.
Latest follow-up for this study was 36 months. However, due to sample retention of less than 60%, outcome for males in the study are based on the 24-month follow-up measure (87% retention). 36-month effects were included for the female sample where attrition was within acceptable range (71%).
Programs in this category that have met the inclusion criteria for this review vary widely in terms of the youth they served and their program characteristics. Just under one-quarter (4 of 18) of the programs served high school aged adolescents, half (9 programs) served middle-school aged adolescents only, and five programs served a mixture of ages. Eleven of the 18 programs studied (61 percent) served predominantly virgins. Only one of the programs offered 30 hours or more of service, and 6 of the 18 programs offered fewer than ten hours of service. Most (11 of 18) took place at least partially in schools, while others (7 studies) operated solely in clinics or community-based organizations. For more detailed information, see Appendix A, programs 8 through 25.
Most of the multi-component/youth development programs included in this review entail over 50 hours (often more than 100 hours) of program-related activities for participating youth. Often these hours include paid work or community services hours. Most programs target youth at “elevated risk” (for example, based on school counselor or social service referrals), while others serve broader populations of adolescents (but who are often living in areas where the majority of the population is considered to be “at risk”). Between 12 and 73 percent of youth served by the programs evaluated had initiated sex prior to entering the program. Some of these programs operated outside of schools and others operated in schools. All offer a diverse set of activities that may include one or more of the following: volunteer experiences, paid work experiences, and mentorship programs, life skills classes, academic support and remediation, and contraception education and/or services. For more detailed information, see Appendix A, programs 26 through 31.
The Corpus of Evidence and Its Representativeness of Programs that Exist
A number of organizations such as the Alan Guttmacher Institute (AGI), the Kaiser Family Foundation (KFF), the National Campaign to Prevent Teen Pregnancy (NCTPTP), the Sexuality and Education Council of the United States (SIECUS), and Advocates for Youth have attempted to inventory and/or documents the kinds of pregnancy and HIV prevention efforts available to adolescents. It is difficult to determine the exact proportion of programs and services that exist and are offered to different subgroups within the population. Yet, four general conclusions emerge from information provided by these organizations and through descriptive analysis of data from a nationally representative sample of adolescents in the United States (Longitudinal Study of Adolescent Health). First, sex education is nearly universal in this country. Nearly all adolescents receive such education at some point during their secondary schooling. At any given moment, adolescents who have recently received sex education tend to be younger, less sexually experienced, and have fewer risk factors and more protective factors for teen pregnancy as compared to those who have not recently experienced sex education. Second, within the subgroup of sex education programs, there has been a substantial increase in the proportion of school-based programs that focus solely on abstinence. Third, other reproductive services such as family planning counseling and services, diagnosis and/or treatment for STDs, and contraceptive distribution programs also serve a large proportion of adolescents. These programs are often provided by non-private medical providers such as family planning clinics and tend to target higher-risk adolescents. Fourth, there has been a movement towards multi-component programs operated in and outside of schools that combine traditional pregnancy prevention education and services with additional supports and programs such as mentoring, service learning, recreation, and basic or occupational skills training.
Within the four categories of intervention types explored in this review, there is reason to believe that programs evaluated rigorously using experimental designs may not be representative of programs that have been or are currently in operation. While one-time consultations included in the review are diverse geographically and with regard to subjects served, four studies cannot represent the full sample of one-time consultations.
Similarly, only three studies of abstinence-only sex education programs met the criteria for inclusion in this review and, as mentioned above, they are not representative of programs in operation, particularly since there has been a tremendous growth in such programs over the past decade that include a variety of established curricula on the topic, and none of the included studies too place in the past decade.
It is much more difficult to determine the representativeness of the sex education programs with a contraception component. On the one hand, the eighteen studies included in this review do vary widely (for example, with regard to the populations served, curricular focus, and geographic location), and there is good evidence to suggest that programs in operation also are quite diverse. However, there is not enough information available from external sources to suggest, with certainty, whether the variety of programs evaluated rigorously mimics the variety of programs in operation. Indeed, it is unlikely that eighteen studies will be able to capture the variety available across the population of programs in operation.
Six of the seven multi-component/youth development programs served primarily low income, minority populations and the one program that served a primarily white population, targeted adolescents who were at “elevated risk” of pregnancy. Therefore, one should not generalize these results to a less “at-risk” population of adolescents. Since it is likely that program operators will invest in more costly and intensive multi-component programs for those adolescent most in need of such services, there may be some element of representativeness of multi-component programs in operation. However, the fact that only seven studies are included in this review may limit their ability to represent the varied multi-component efforts that have been gaining in popularity.
Estimated Program Impacts
This review finds no consistent evidence that the types of pregnancy prevention programs evaluated rigorously to date will alter in intended ways the sexual activity or pregnancy risks of youth. Regardless of the sign and significance of the estimated impacts, the magnitude of the differences in the percentages of program and the control group youth reporting having engaged in sex, having sex without using contraception, and becoming or getting someone pregnant generally are modest in size—typically under five percentage points. Furthermore, across all intervention studies, the weighted average estimated impacts generated using random effects models are approximately one percentage point or less in magnitude (favoring the intervention group) for each of the three outcome measures examined, and none of the pooled impact estimates is statistically different from zero (Table 3).
While this overall finding is important, it should not be interpreted to mean that programs do not work for two main reasons. First, this overall pooling of studies mixes results of different program types serving different populations of adolescents. Statistical heterogeneity tests from these analyses suggest that the effect sizes differ beyond what would be expected from sampling error. This heterogeneity exists because certain studies have significantly larger or smaller effect sizes than the overall “average” effect size. This variation may be the result of differences in methodological characteristics, program models, target populations, and/or subgroups served. For this reason, the remainder of this analysis will focus primarily on outcomes by program type.
Second, from a statistical standpoint, our analysis suggests that we are unable to reject our “null hypothesis” which states that there are no differences in sexual behavior outcomes between intervention and control group adolescents. This means that we have not found consistent evidence that programs studied work, not vice versa. Again, this suggests a need to dig deeper into subgroup analyses to get a better sense, at least correlationally, of whether there are impacts for specific kinds of programs or for particular adolescents.
Pooled Impact Estimates, by Outcome
Note: Estimates are based on random-effects models estimated using Comprehensive Meta-analysis (Borenstein and Rothstein 1999). None of the pooled impact estimates is statistically significant.
Results for Sexual Experience Rates (Ever Had Vaginal Intercourse) Based on Experimental Design Studies
Source: Full citations for and descriptions of the referenced studies are presented in Appendix A.
Note: Estimates are based on random-effects models estimated using Comprehensive Meta-analysis (Borenstein and Rothstein 1999).
Although this estimate was initially statistically significant, after our analysis adjusted for clustering within groups (for example, classrooms or schools), the effect no longer remained significant.
The estimate used in the meta-analysis exploring sexual experience was for the abstinence focused intervention, whose primary goal was to reduce sexual initiation (but made limited mention of contraception). See Appendix C for impacts for the Safer Sex intervention.
Sikkema included two intervention groups with a shared controlled group. Since the interventions are of different program types, both are included in this table. However, the effect size for all studies combined (last row of this table) includes a weighted average of the effects.
p <.01, ** p<.05, * p<.10.
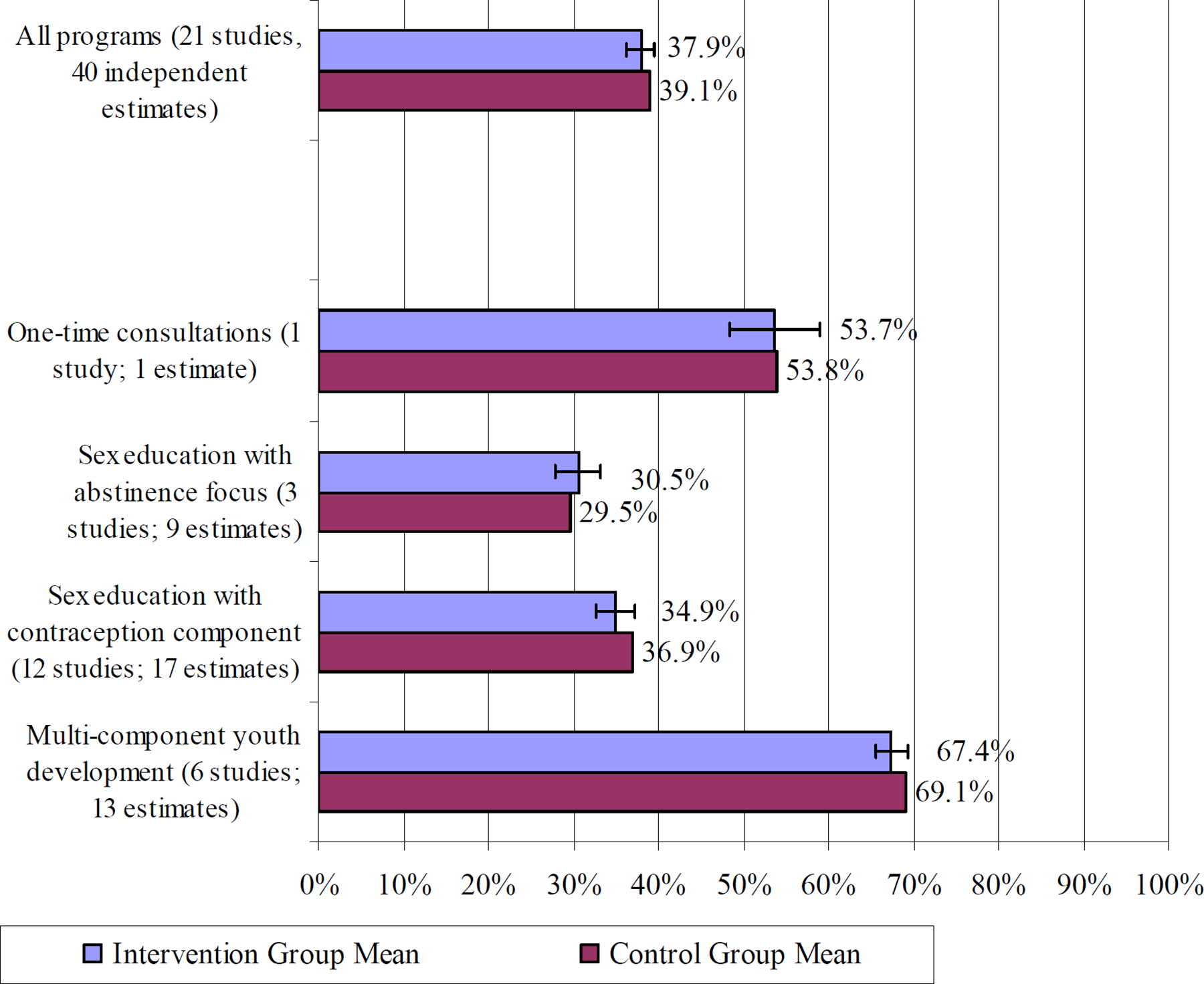
Intervention and Control Group Sexual Experience Rates for All Programs and by Program Type
Among the subgroups of programs with more similar impact estimates, the only statistically significant effect on pregnancy risk is for multi-component/youth development programs (Figure 3). Across these three studies, there was an estimated 6.0 percentage point decline in rates of unprotected sexual intercourse. At least one statistically significant effect was found in each of the three studies (Table 5).
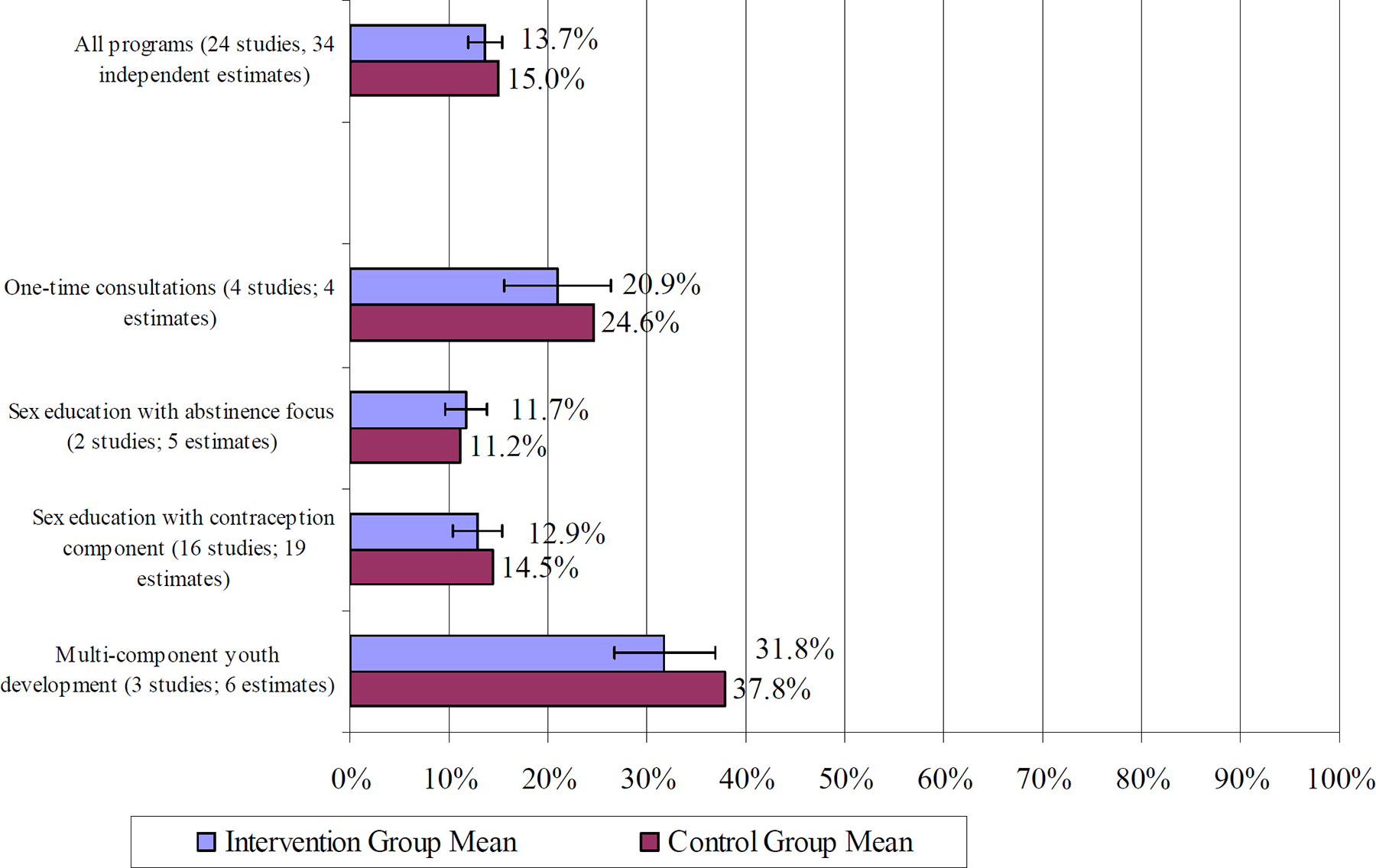
Estimated Impacts on Pregnancy Risk Rates for All Programs and by Program Type
The pooled impacts for one-time consultations and sex education with an abstinence focus are not statistically significant. For one-time consultations, which are primarily focused on reducing unprotected sexual intercourse, the pooled effect was a non-significant 3.7 percentage point reduction in pregnancy risk.
Sex education programs with an abstinence focus do not cover issues concerning contraception use, and thus, we would not expect increases in contraception use. However, such programs could reduce pregnancy risk by decreasing the number of adolescents engaging in sexual intercourse. The pregnancy risk measure incorporates both of these issues into its calculation.14 Thus, there is a chance that abstinence-focused programs could reduce (or possibly increase) pregnancy risk. Based on the limited information currently available, there is no evidence that these programs either increase or decrease pregnancy risk. The pooled impact estimate of 0.5 percentage points favoring the control group has a confidence interval three times as large (Table 5).
Results for Pregnancy Risk Rates Based on Experimental Design Studies
Source: Full citations for and descriptions of the referenced studies are presented in Appendix A.
Note: Estimates are based on random-effects models estimated using Comprehensive Meta-analysis (Borenstein and Rothstein 1999).
Although this estimate was initially statistically significant, after our analysis adjusted for clustering within groups (for example, classrooms or schools), the effect no longer remained significant.
The estimate used in the meta-analysis exploring pregnancy risk was for the Safer Sex intervention, whose primary goal was to reduce unprotected sex. See Appendix C for impacts for the abstinence intervention.
Sikkema included two intervention groups with a shared controlled group. Since the interventions are of different program types, both are included in this table. However, the effect size for all studies combined (last row of this table) includes a weighted average of the effects.
p <.01
p<.05
p<.10.
The most variation in impact estimates occurs for studies of sex education programs with a contraception component, making it imprudent to interpret the pooled effects on pregnancy risk. Five of the 19 estimates for sex education programs with a contraception component are statistically significant, four favoring the treatment group and one favoring the control group.15 The average effect—1.6 percentage points—is not statistically significant, but is not particularly telling due to the variation across studies within this intervention type.

Estimated Impacts on Pregnancy Rates for All Programs and by Program Type
Although small sample sizes limit the power of the test, there is no evidence of heterogeneity in the pooled pregnancy rate impacts once studies are grouped by intervention type. The point estimate of effects for the single study of a one-time consultation was statistically significant favoring the treatment group (-4.8 percentage points). Among the two sex education intervention types, the magnitude of the pooled impacts is quite small. However, it is notable that the pooled estimate from two studies of sex education program with an abstinence focus (six of seven of the impacts from one study) is statistically significant favoring the control group (1-percentage point). While all five studies of sex education programs with a contraception component favor the treatment group, none are statistically significant after adjusting for clustering, and the pooled impact is near zero (-.7 percentage points).
Multi-component/youth development programs showed the greatest evidence of favorable impacts on pregnancy rates. The pooled estimate for the five studies (12 estimates) is moderate in size (-3.9 percentage points) and is statistically significant.
Results for Pregnancy Rates Based on Experimental Design Studies
Source: Full citations for and descriptions of the referenced studies are presented in Appendix A.
Note: Estimates are based on random-effects models estimated using Comprehensive Meta-analysis (Borenstein and Rothstein 1999).
Although this estimate was initially statistically significant, after our analysis adjusted for clustering within groups (for example, classrooms or schools), the effect no longer remained significant.
p <.01
p<.05
p<.10.
For all three outcome measures, the pooled impact estimates (Table 7, top panel) based on a random effects model are small (less than one percentage point) and not statistically significant for the programs targeting middle school youth. They are larger (-0.9 to -11.1 percentage points, favoring the intervention group) for those programs targeting high school youth. However, only the -11.1 percentage point impact on pregnancy risk rates is statistically significant. In addition, there were statistically significant effects favoring the intervention group on both sexual experience rates and pregnancy rates for programs aimed at mixed ages.
When looking at the more homogeneous group of interventions by program type, sample sizes limit comparisons across ages served. Comparisons were assessed only in cases where there were at least two effect size estimates per age category. No comparisons can be made for one-time consultations or sex education programs with an abstinence focus. With regard to sex education programs with a contraception component, there was a significant difference (p<.05) in the magnitude of the effect sizes for pregnancy risk depending on the age served, with the smallest estimated effects on middle school aged adolescents (-.2 percentage points) and the largest effects for programs serving high school age adolescents (-14.6 percentage points). However, none of the pooled effect sizes by age subgroup were statistically significant.
Within the subgroup of multi-component/youth development programs, there was a statistically significant difference (p<.10) in sexual experience rates depending on ages served, with a 0.0 percentage point difference among the five estimates of programs serving high school age adolescents, a statistically significant 5.8 percentage point effect among the five estimates of programs serving a mixture of ages, and a non-significant difference of 9.2 percentage points among the three estimates of programs aimed at middle school aged adolescents.
These few differences that were found suggest that age may be an important factor to consider when determining differences in program effects. However, due to sample size limitations, this analysis has not found any clear patterns with regard to differences in effects based on ages served.
Pooled Estimates of the Percentage Point Impacts of Programs on Sexual Experience, Pregnancy Risk, and Pregnancy, by Grade Levels of Youth Targeted
Source: Full citations for and descriptions of the referenced studies are presented in Appendix A.
Note: Estimates are based on random-effects models estimated using Comprehensive Meta-analysis (Borenstein and Rothstein 1999).
n.a. means not applicable due to either no studies or only one study in this category.
p<.01
p<.05
p<.10.
This review includes estimated impacts for all studies meeting the stated inclusion criteria, separating the estimates by gender whenever possible (Table 8, top panel). The available evidence shows no overall program impacts for males or for females. The pooled impact estimates are small (-2.9 percentage points or less) for all three outcomes and not statistically significant for either gender.
Pooled Estimates of the Percentage Point Impacts of Programs on Sexual Experience, Pregnancy Risk, and Pregnancy, by Gender of Youth
Source: Full citations for and descriptions of the referenced studies are presented in Appendix A.
Note: Estimates are based on random-effects models estimated using Comprehensive Meta-analysis (Borenstein and Rothstein 1999). n.a. means not applicable due to either no studies or only one study in this category.
p<.01
p<.05
p<.10.
Again, sample size limitations prevent drawing any clear conclusions regarding differences in impacts for males versus females, particularly among one-time consultations. There were no significant differences in impacts of either sex education programs with an abstinence focus or sex education programs with a contraception component for either males or females, and there were no differences in the estimated impacts by gender. There were statistically significant differences in impacts for both pregnancy risk rates (p<.05) and for the pregnancy rates (p<.10), with the impacts for females more pronounced than the impacts for males. Specifically, the pooled effects for males in multi-component/youth development programs were not statistically significant for any outcomes. However, for females, the pooled effects were larger and statistically significant for pregnancy risk (10.2 percentage point reduction) and pregnancy rates (5.9 percentage point reduction).
Pooled Estimates of the Impacts of Programs on Sexual Experience, Pregnancy Risk, and Pregnancy, by Study Characteristics
Source: Full citations for and descriptions of the randomized control trial studies are presented in Appendix A.
Note: Estimates are based on random-effects models estimated using Comprehensive Meta-analysis (Borenstein and Rothstein 1999).
Asterisks above a set of impact estimates denotes statistical differences among or between the estimates in the cluster.
These p-values are biased downward (suggesting greater statistical significance) in so far as none of the studies that used cluster randomization appears to have accounted for clustering in the analysis (Raudenbush and Bloom 2005).
“Usual prevention services include: sex education program in existence prior to the new program and/or reproductive clinic services such as contraception consultation or distribution. General health programs or examinations, recreation services, or summer jobs are considered as “no prevention services.”
n.a. means not applicable.
p<.01
p<.05
p<.10.
One example relates to the results for the sexual experience outcome for studies with different sample retention rates. The pooled impact estimate for the studies with the largest rates of sample retention (80 percent or higher) are significantly larger in magnitude (nearly -5.0 percentage points favoring the intervention) than for the two groups with lower sample retention (-2.3 and 0.4 percentage points, respectively). Differences for the pregnancy risk outcome across retention rate categories mimic the same pattern as the sexual experience outcome.
The pooled impact estimates also vary significantly depending on whether the control group received usual prevention services rather than no services or services unrelated to pregnancy prevention. For both the pregnancy risk and the pregnancy outcomes, studies of interventions where control group adolescents received no pregnancy prevention services tended to have more positive impacts than did studies where control group adolescents received the usual pregnancy prevention services offered in their schools and communities. This makes intuitive sense, since the presence of an alternative treatment likely diminishes the net change in services provided and, thus, the expected program impact.
Finally, particularly for pregnancy rate outcome, the pooled impact estimates varied by the length of time between sample enrollment and the follow-up data collection. The pooled estimates of impacts for all three outcomes are largest among those studies with the shortest follow-up period. For the pregnancy outcome, in particular, the strongest pooled impact is among the studies that follow-up their samples for less than one year, a nearly 7 percentage point reduction (p<.01). The only statistically significant impact favoring the control group is the small (0.6 percentage point, p =.058) impact on pregnancy rates for studies with 12 to 23 months of follow-up. However, this result is driven by a single study of ENABL (Kirby, 1995), which makes it is impossible to determine whether this variation is related to the ENABL itself or to the duration of follow-up.16 None of the pooled estimates based on studies with two or more years of follow-up is statistically significant for any of the outcome measures.
What if the review included quasi-experimental design studies?
As noted above, there is considerable debate among the evaluation community as to the credibility of impact estimates based on quasi-experimental designs. Guyatt et al. (2000) examined impact estimates generated from pregnancy prevention program evaluations based on both experimental and quasi-experimental design studies (QEDs). They concluded that there were meaningful differences in the estimates associated with study design and, thus, they chose to focus only on randomized controlled trials.
This review also includes only results from randomized control trials. However, as a supplement to the review, the results of the experimental design studies that met the review criteria are compared with those of 16 quasi-experimental design studies that had been included in one of the prior reviews—that by Kirby (2001)—and that otherwise met the criteria for this review. Due to resource limitations, the comparison between RCT and QED pooled findings has not been systematically explored and should be considered as exploratory. Because the majority of the experimental studies included in this review overlap with those included in Kirby's narrative review, we have less reason to believe that differences in pooled impacts for treatment versus control group are due to varied search strategy and inclusion criteria of the reviewers. However, a more systematic research synthesis would be necessary to verify this conclusion.
Ten (10) of the sixteen quasi-experimental studies examine one of the four categories of interventions for which there is one or more randomized control trial. However, six of the studies are of comprehensive clinic-based interventions, which have not been evaluated using randomized control trials. Appendix D provides a detail of the individual findings from all 16 studies, organized by program type and Appendix E provides full citations.
A total of 12 studies included 25 independent estimates of program impacts on sexual experience, with 9 of these estimates relating to one of the four intervention types for which there also is evidence of impacts from randomized control trials. Ten (10) of the studies contain 22 independent estimates of impacts on pregnancy risk, with 6 of these estimates pertaining to the interventions for which there also is evidence from randomized control trials. And, 8 of the quasi-experimental design studies contain 20 independent estimates of impacts on pregnancy rates. However, only five of the impact estimates pertain to one of the four types of interventions for which there is evidence of intervention effectiveness from a randomized controlled trial.
In general, the pooled impact estimates from the randomized controlled trials are smaller than those from the quasi-experimental design studies (Table 10, top panel).
In addition, looking at the results by type of intervention, there is a tendency for the results from the quasi-experimental design studies, which have lower internal validity, to suggest impacts more favorable to the interventions than do those results based on the randomized control trials. In four of the six cases where pooled estimates show evidence of intervention effects, the pooled impact estimates based on the randomized controlled trials are smaller and have lower statistical significance than do those based on the quasi-experimental design studies. For example, the pooled impact for sexual experience rates for sex education programs with a contraception component among the 17 RCT effect sizes is a statistically insignificant 2.0 percent reduction. The six QED effect size estimates have a pooled effect of 6.5 percent reduction in sexual experience rates. In the two remaining cases, both of which are for multi-component/youth development programs, the RCT impacts are stronger than the QED impacts (for the pregnancy risk and pregnancy outcomes).
There is one class of programs—comprehensive community-based programs—that has been evaluated only using quasi-experimental design studies. This is because the community-wide nature of the interventions precludes randomizing youth within a community to intervention or control group status. The results of the five studies (15 to 16 independent effect sizes for each outcome measure) show no evidence of impacts on initiation of sex or on pregnancy and small impacts favoring the intervention group on pregnancy risk (-2.7 percentage points). However, both due to the lower causal validity of these estimates in general and the fact that there is evidence of considerable heterogeneity in the impact estimates, it seems prudent to treat these results with some degree of caution (Q=72.32, I2=79.3, df=15, p<.001).
Pooled Estimates of Program Impacts for Random Controlled Trial Studies and Quasi-Experimental Design Studies, Overall and by Type of Intervention
Source: Full citations for and descriptions of the randomized control trial studies are presented in Appendix A. Citations for the quasi-experimental design studies are presented in Appendix E.
Note: Estimates are based on random-effects models estimated using Comprehensive Meta-analysis (Borenstein and Rothstein, 1999). n.a. means not applicable.
p<.01
p<.05
p<.10.
DISCUSSION
The experimental data presented in this analysis suggests that there is no consistent evidence that programs designed to delay sexual initiation, reduce pregnancy risk, and prevent teen pregnancy achieve these goals. There are a handful of interventions for which the estimated impacts are statistically significant and a few impact estimates that are large (a difference of more than 10 percentage points). While the majority of the statistically significant impact estimates favor the intervention group, a non-trivial number favor the control group.
One should not conclude from these findings that pregnancy prevention efforts are futile for four reasons. First, the particular programs that have been evaluated are not representative of programs in operation. Thus, the generally null findings could reflect the fact that the most successful efforts have not yet been evaluated using methods that are expected to yield internally valid impact estimates. Second, the adolescents served in the programs included in this review are not representative of all adolescents. Notably, the majority of the programs evaluated were targeted interventions that often focused on urban, high-risk youth.17 Third, most of the control group youth in the programs evaluated had access to some type of sex education and pregnancy prevention services in their schools and communities, and thus instead of exploring the overall impacts, this review often explores the relative impacts of programs aimed at reducing sexual risk-taking compared with other services. This is consistent with national statistics showing that roughly 90 percent of school age adolescents receive some form of health and sex education in school (tabulations from the National Survey of Adolescent Health). And, fourth, the studies followed sample youth for relatively short periods of time. Particularly for those programs serving middle school youth, most youth in the study samples have not yet become sexually active by the time the follow up data for the study were collected.
The results of the review highlight the danger in relying heavily on the pooled impact estimates in judging the effectiveness of particular types of interventions. Homogeneity tests revealed significant variation in impact estimates across the various types of interventions, and even within some program types such as sex education programs with a contraception component. In concept, it should be more appropriate to pool evidence across subgroups of studies that focus on particular types of interventions or that target particular subgroups of youth. Yet, the small numbers of independent impact estimates within these subgroups generally means that there is insufficient power to judge the homogeneity of the estimates. Thus, the pooled estimates by type of intervention, by grade levels of youth targeted and by gender simply offer descriptive summaries of the results for these groups based on the present corpus of evidence.
With all the above noted caveats in mind, the current evidence base on which to judge the effectiveness of various types of interventions can be summarized as follows:
While the body of knowledge in this field is continually growing, this review highlights the relative dearth of evidence to judge the overall effectiveness of particular intervention strategies. For this reason, further research and evaluation is necessary, including studying programs that have not yet been evaluated rigorously and programs that have been replicated and are serving new populations of adolescents in different communities. Researchers should also increase the breadth of evaluations to estimate more routinely program impacts for key subgroups of youth defined by factors such as age, gender, and family background. Once a larger body of more similar programs have been evaluated rigorously and reported consistently, then it will be possible to pool the evidence to make more concrete conclusions regarding program efficacy. Having access to solid information about whether particular types of interventions are effective, as well as information regarding for whom programs are effective and not effective, will help policy makers and practitioners better address the sexual health risks of youth.
Footnotes
Appendix A
Appendix B
Appendix C
Appendix E
1
Throughout this review, we use the terms teen pregnancy and childbearing to refer to unplanned or mistimed pregnancies and births among teens. In the past two decades, it has been relatively uncommon for teens in the United States and most similarly developed countries to become pregnant and give birth intentionally (Brown and Eisenberg 1995). Since the primary interest for this systematic review is in preventing teen pregnancies, sexual activity has been defined as heterosexual intercourse. Reviewers who are interested in HIV prevention may choose to define sexual activity more broadly. In addition, reviewers interested in HIV prevention may choose to include studies from a broader set of countries including developing countries where many programs aimed at reducing teen sexual risk-taking are primarily HIV prevention efforts.
2
See, for example, Kirby (2001), Solomon and Card (2004), and ![]() .
.
3
For example, in cases where an author reports outcomes for sexual initiation rates for the full sample and contraceptive use rates among those who had initiated sex, it is possible to compute impact estimates for pregnancy risk among the full sample.
4
The reason for excluding studies prior to 1980 is based on the fact that changes in social norms and contraceptive options have changed sufficiently over the years that research published prior to 1980 would not likely be relevant today. In reality, this bound on the search likely had no effect on the pool of studies included in the review.
5
For example, we would have excluded a study in which the data for the program group were collected by the program staff, while independent data collectors conducted surveys with the control group, unless the study provided convincing evidence that this difference in data collection method did not lead to differential survey response bias.
6
The decision to apply a 60 percent response rate threshold for including a study in the sample reflects an effort to balance two competing goals: excluding randomized controlled studies that lack internal validity due to non-response bias and including as rich an evidence base for reader consideration as possible.
7
An initial set of studies was accumulated through the library Douglas Kirby collected while conducting a similar review in 2001. Basic internet search engine queries yielded a unreasonable number of hits, which, upon basic examination, did not yield any additional information. Thus, this search method was abandoned. However, internet searches of Department of Health and Human Services website, teen pregnancy prevention websites, and policy research firm websites were conducted including:
9
Since inter-rater reliability was high (less than 10 percent discrepancies) among the critical data fields, we chose not to double code all studies, as was outlined in our protocol.
10
If available, an “anchor” measure of “always” using contraception was used to compute pregnancy risk. If this measure was not available, then use of contraception at most recent intercourse was used. In the rare cases where neither of the above measures was available, any use/non-use of contraception was used. Sensitivity analyses showed that the estimated impacts did not depend on how this variable was measured.
11
This study reported on four different randomized controlled trials. Two of them randomized at the classroom level (one adult-led and one peer-led program), one randomly assigned schools, and a fourth randomly assigned adolescents. This fourth program provided outcomes for less than 60 percent of the original sample and, thus, was excluded from this review.
12
After adjusting for clustering within groups, statistical homogeneity tests were non-significant for all pooled effects within program types.
13
Prior to adjusting for clustering within groups, there was a statistically significant effect favoring the intervention group for sex education programs with a contraception component.
14
Numerator is having unprotected sex, denominator is either engaging in contraceptively protected sex or not engaging in any sexual intercourse.
15
Three of the four programs that found statistically significant positive program effects were theory-based and culturally sensitive HIV prevention programs serving primarily African American adolescents. See Appendix A for study details.
16
17
For example, none of the programs evaluated focused solely on suburban or rural youth, and the majority of studies in this review focused exclusively on urban youth.
18
Comparisons across intervention types have not been derived experimentally, and thus it is not possible to use the information from this analysis to suggest that one particular intervention type is more or less effective than another. For example, intervention types could be confounded with other study features such as study design and methods or subgroups served.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.