
Abstract
Domestic violence is common and serious. Many convicted men are court-ordered to receive cognitive behavioural therapy (CBT) in order to end their violence. Most men do not voluntarily seek such therapy but participate either after being pressured by their partners or after being legally required to do so.
This Campbell Systematic Review sought all randomised controlled evaluations about the effects of CBT on physical violence worldwide, but found only six small trials with 2,343 participants met the inclusion criteria. The evidence from the included studies is insufficient to draw any conclusions.
Abstract
Background
In national surveys between 10 % and 34 % of women have reported being physically assaulted by an intimate male partner. Cognitive behavioural therapy (CBT) or programmes with elements of CBT are frequently used treatments for physically abusive men. Participants either enrol voluntarily or are obliged to participate in CBT by means of a court order. CBT not only seeks to change behaviour using established behavioural strategies, but also targets the thinking patterns and beliefs that are thought to contribute to violence.
Objectives
To measure the effects of CBT and similar interventions on men's physical abuse of their female partners.
Search strategy
We searched the Cochrane Controlled Trials Register (CENTRAL), C2-SPECTR, MEDLINE, EMBASE, CINAHL, PsycINFO, ERIC, Care Data/Social Care Online, Sociological Abstracts, Criminal Justice Abstracts, Bibliography of Nordic Criminology (all to late 2006), and SIGLE to 2003. Santé mentale au Québec was handsearched from 1976 to 2003 and reference lists of articles. We also contacted field experts and the authors of included studies.
Selection criteria
Randomised controlled trials (including cluster-randomised and quasi-randomised trials) of cognitive behavioural therapy with men who physically abuse their partners and reporting effects on continued violence.
Data collection & analysis
Two review authors independently assessed trial quality and extracted data. We contacted study authors for additional information.
Main results
Six trials, all from the USA, involving 2343 people, were included. A meta-analysis of four trials comparing CBT with a no-intervention control with 1771 participants, reported that the relative risk of violence was 0.86 (favouring the intervention group) with a 95% confidence interval (95% CI) of 0.54 to 1.38. This is a small effect size, and the confidence interval is so wide that there is no clear evidence for an effect. One study (Wisconsin Study) compared CBT with process-psychodynamic group treatment and found a relative risk of new violence of 1.07 (95% CI 0.68 to 1.68). Even though the process-psychodynamic treatment did marginally better than CBT, this result is also equivocal. Finally, one small study (N = 64) compared a combined treatment for substance abuse and domestic violence (SADV) with a Twelve-Step Facilitation (TSF) group. An analysis involving 58 participants investigated the effect on reduction in frequency of physical violence episodes. The effect size was 0.30 (favouring TSF) with 95% confidence interval from -0.22 to 0.81.
Reviewers’ conclusions
There are still too few randomised controlled effect evaluations to conclude about the effects of cognitive behaviour therapy on domestic violence.
Linked article:
Linked article:
Synopsis
Cognitive behavioural therapy for men who physically abuse their female partner
Domestic violence is common and serious. Many convicted men are court-ordered to receive cognitive behavioural therapy (CBT) in order to end their violence. Most men do not voluntarily seek such therapy but participate either after being pressured by their partners or after being legally required to do so. The review sought all randomised controlled evaluations about the effects of CBT on physical violence worldwide, but found only six small trials with 2343 participants met the inclusion criteria. The evidence from the included studies is insufficient to draw any conclusions.
Background
Violent behaviour constitutes a serious problem in societies worldwide. Intimate partner abuse is especially problematic because it takes place in the private family sphere, making it a difficult arena for intervention and help. The physical abuse of women by their male partner is a serious concern because “it affects a distressingly high percentage of the population and it results in physical, psychological, social, and economic consequences” (CDCP 2003). The World Health Organisation (WHO) reported that “the overwhelming health burden of partner violence is borne by women at the hands of men” (WHO 2002). The WHO also provided evidence about the extent of the problem: in national surveys between 10 % and 34 % of the women reported being physically assaulted by an intimate male partner (WHO 2002).
Domestic violence occurs in the family and takes many different forms, including sexual, psychological, emotional and physical abuse. In this review the focus is solely on physical abuse. Domestic violence can occur between spouses/partners and between adults and children in the family. This review focuses only on partnership abuse, and specifically on men who physically abuse their female partner or ex-partner. The term domestic violence is therefore too broad to give meaning for this review, and more useful terms are physical abuse, battering, and intimate partner abuse. Another important limitation is that this review does not focus on the causes of violent behaviour. Several biological, psychological and sociological studies have attempted to find the one answer to what causes men to commit violent actions. In general there is now more focus on the correlation of different behavioural variables leading to violence. Therefore this review sets out to include more outcome variables than strictly physical violence, for example self-esteem, substance use and emotional problems.
US batterer intervention programmes were initially introduced as an alternative to incarceration for men arrested for domestic violence. This was a controversial strategy because many policy makers/advocates felt that this diversion sent the message that abuse was a mental health problem rather than a crime, and because funding these programmes may have diverted funds from programmes for abused women. The stated goals for the batterer intervention programmes differ widely, from statistically measurable reductions in violence, to holding men accountable to preparing men to take action against the woman battering culture.
One of the most frequently used treatment programmes for physically abusive men is a psychological intervention called cognitive behavioural therapy (CBT). CBT not only seeks to change behaviour using established behavioural strategies, but also targets the thinking patterns and beliefs that are thought to contribute to violence. CBT is “designed to help the patient test certain maladaptive cognitions and assumptions” (Beck 1979). CBT techniques aim to identify thoughts and beliefs that precede violent behaviour, challenging the patterns that violent men use to justify their violence after the event. The goal is to bring about changes in the way that physically abusive men think about violence and the circumstances which lead to violence, thereby interrupting the chain of events that lead to physical abuse. The CBT can be given in individual, couple or group format. A common intervention called the Duluth Model (Pence 1993) has many cognitive-behavioural components and is included in this review.
An American review of state and provincial programmes for intervening in spouse abuse cases reported simply “the jury remains out on the effectiveness of these programmes” (Arias 2002). When spouse abusers are sent on programmes, it is important to know the positive or negative effect. If a programme does not work or has adverse outcomes, we risk putting women in danger of future abuse.
The scope of this review is to determine the effectiveness of cognitive behavioural therapy delivered to men engaged in physical abuse, against their female partner. A previous review of cognitive therapy (Butler 2000) for violent offenders did not include physically violent spouse abusers, but concluded that the therapy had a beneficial effect for those with problems such as marital distress and anger. To date, we know of no systematic review of the effects of CBT for men who are physically violent toward their partners that has employed a search strategy aiming to locate every randomised controlled study worldwide regarding this question. Davis and Taylor (Davis 1999) reviewed the literature but did not report a search strategy. A later review (Babcock 2004) searched only PsychINFO and used only four search terms. The results from the present review are of importance for perpetrators and victims of this form of violence, and those who seek this form of treatment for the problem, and also for therapists, researchers, the judiciary, and the general public.
Objectives
To measure the effects of cognitive behavioural therapy (CBT) and similar interventions on men's physical abuse of their female partners.
Criteria for considering studies for this review
Types of studies
Randomised controlled trials, including quasi- and cluster randomised controlled trials, were included in this review. The control group consisted of persons who received no intervention, other interventions, or were on a waiting list.
Types of participants
Men who physically abuse their female partner/spouse/wife. Primary studies where the focus is on women who abuse their partner/spouse were excluded from this review. In the event of trials having a mixed population of men who have been violent against women and those who have been violent against men, we requested data separately from the trial investigators. We recorded whether the perpetrators were living with their partners or whether they were ex-partners. Trials in which the participants attended the treatment programme voluntarily or were court-ordered to participate were included, and results were separately reported.
Types of interventions
Interventions stated by the authors to be cognitive behavioural or recognisably so (for example, Duluth Model) from the description provided. Programmes may be individual, couple or group based and delivered in any setting.
Types of outcome measures
The primary outcome measure was physically violent behaviour. We also included other violent behaviour, like verbal aggression and hostile attitudes. Other, secondary outcome measures were: improved self-esteem, reduced substance abuse and anger management. Regarding self-esteem, substance abuse, and emotional distress, these were recorded for both perpetrators and victims wherever possible. Measures of outcome data were grouped in to short follow-up time (0 to 6 months), intermediate 7 to 18 months, and long-term (19 months and beyond). Any formats for measuring the outcome were included but were separately reported (e.g. self reports, victim reports, judicial and police reports). Both standardised and unstandardised measures were included.
Search strategy for identification of studies
We searched the Cochrane Controlled Trials Register (CENTRAL) (The Cochrane Library Issue 4, 2006), MEDLINE (1966 to September week 3 2006), EMBASE (1980 to 2006 week 39), CINAHL (1982 to September 2006), PsycINFO (1806 to October 2006), ERIC (1966 to September 2006), C2-SPECTR (searched December 2006), Care Data/Social Care Online (searched September 2006), Sociological Abstracts (1963 to September 2006), Criminal Justice Abstracts (1968 to September 2003), Bibliography of Nordic Criminology (1999 to December 2006), and SIGLE (1980 to September 2003). Criminal Justice Abstracts and SIGLE were only searched until 2003 because we did not have access in 2006.
We handsearched Santé mentale au Québec, an online scientific journal, from 1976 to 2003. The review authors contacted field experts and the authors of retrieved studies in order to find additional studies. Conference papers were searched also, in order to minimise the threat of publication bias. Reference lists in included studies were searched for relevant literature. Studies were included regardless of language and country of origin.
Below is the search strategy used to search CENTRAL. The search strategies for the other electronic databases were modified to suit each database. They are included in Table 02, Table 03, Table 04, Table 05, Table 06, Table 07, Table 08 and Table 09.
Search strategy used in CENTRAL, The Cochrane Library Issue 4, 2006 (Sigrun Espelien Aasen)
#1MeSH descriptor Battered Women, this term only
#2MeSH descriptor Domestic Violence, this term only
#3MeSH descriptor Spouse Abuse, this term only
#4((familiy or domestic or conjugal or partner*) near/3 violence):ti,ab,kw
#5((abus* or batter*or beat* or assault*) near/3 (wom*n or partner* or spouse* or female* or wife or wives or domestic* or fiance or cohabitant* or live-in)):ti,ab,kw
#6((male* or men or man or partner* or spouse* or husband or fiance or cohabitant* or live-in) near/3 (batter* or perpetrator* or abus* or violen* or beat* or assault)):ti,ab,kw
#7(#1 OR #2 OR #3 OR #4 OR #5 OR #6)
#8MeSH descriptor Behavior Therapy, this term only
#9MeSH descriptor Cognitive Therapy, this term only
#10MeSH descriptor Psychotherapy, Rational-Emotive, this term only
#11(cognitive* near/3 (therap* or train* or techni* or question* or approach* or assessment*)):ti,ab,kw
#12((behavior* or behaviour*) near/3 (therap* or train* or modif* or experiment*)):ti,ab,kw
#13(rational* near/3 emotive*):ti,ab,kw
#14(cbt):ti,ab,kw
#15(schemas or schematas):ti,ab,kw
#16MeSH descriptor Imagery (Psychotherapy), this term only
#17(imager*):ti,ab,kw
#18((cognitive* or mental*) near/3 (map* or model*)):ti,ab,kw
#19(Socratic* near/3 (question* or method* or dialogue* or strateg* or sequence*)):ti,ab,kw
#20(dysfunctional near/2 (thought* or assumption* or rule* or appraisal* or belief* or attitude* or scheme*)):ti,ab,kw
#21(automatic near/3 (thought* or process*)):ti,ab,kw
#22(nat or nats):ti,ab,kw
#23(reattribution*):ti,ab,kw
#24((key or core) near/2 belief*):ti,ab,kw
#25(#8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24)
#26(#7 AND #25)
Methods of the review
Selection of studies
Selection of primary studies was based on the inclusion criteria described above. The Reference Manager database was transferred to SRS (software for electronic screening and data abstraction) (SRS 2005). At the first screening level, approval from a single review author took a citation to the second level, then two review authors working independently had to approve of a citation for it to be forwarded to Level 3 (and ordered in full text). Data from all relevant trials at Level 3 were extracted and presented in the ‘Characteristics of included studies’ table. All review authors contributed in this process. If two authors disagreed, a third author mediated, and the decision whether to include or exclude was reached through consensus.
Data extraction and management
Two review authors independently extracted data from the included studies using an online data extraction form. Any disagreement between review authors generated a conflict in SRS which had to be solved through a discussion. If disagreement persisted, a third review author was consulted. If outcome or other vital information was missing from the original reports, we contacted the author(s) by e-mail in an attempt to retrieve the necessary data for the analysis. The following data from the included studies were extracted:
Participants: age, socio-economic status, ethnicity, previous history of violent behaviour and treatment for it, current substance abuse, additional problems/disorders, and marital status.
Quality assessments of included studies
Since “variation in validity can explain variation in the results of the studies included in a systematic review” (Higgins 2005) we assessed the internal validity of included studies. Two review authors independently assessed each selected study against quality categories described below. Uncertainty or disagreement was solved by discussion with a third reviewer. The review authors were not blinded to the authors or other information about the publication when assessing study validity. Whenever information about study quality, or other information about the study, was missing, we contacted the author(s) of the study, to minimise the danger of measuring the quality of the reporting, rather than of the study. Our aim was to get an overall assessment of internal validity based on a summary of the following six methodological criteria.
Generation of allocation sequence
MET = Resulting sequences are unpredictable (explicitly stated use of either computer-generated random numbers, table of random numbers, drawing lots or envelopes, coin tossing, shuffling cards, or throwing dice).
UNCLEAR = Statement that the study was randomised but not describing the generation of the allocation sequence.
NOT MET = Explicit description of inadequate generation of sequence, e. g. (e.g., using case record numbers, alternation, date of admission, date of birth).
Concealment of allocation sequence
MET = Neither participants nor investigators can foresee assignment (e.g. central randomisation performed at a site remote from trial location; or, use of sequentially numbered, sealed, opaque envelopes).
UNCLEAR = Statement that the study was randomised but not describing the concealment of allocation.
NOT MET = Explicit statement that allocation was not concealed OR statement indicating that participants and investigators can foresee upcoming assignment (e. g., open allocation schedule, unsealed or non-opaque envelopes).
Prevention of performance bias
MET = Interventions other than cognitive behavioural programmes avoided or controlled for across comparison groups.
UNCLEAR = Use of interventions other than cognitive behavioural programmes not reported and cannot be verified by contacting the investigators.
NOT MET = Dissimilar use of interventions other than cognitive behavioural programmes across comparison groups, i.e. differences in the care provided to the participants in the comparison groups other than the intervention under investigation.
Prevention of detection bias
MET = Assessor unaware of the assigned treatment when collecting outcome measures
UNCLEAR = “Blinding” of assessor not reported and cannot be verified by contacting investigators.
NOT MET = Assessor aware of the assigned treatment when collecting outcome measures.
Prevention of attrition bias
MET = Losses to follow up less than 20% and equally distributed (as judged by two reviewers) between comparison groups (e.g. 18% and 16%).
UNCLEAR = Losses to follow up not reported.
NOT MET = Losses to follow up 20% or greater, or not equally distributed (as judged by two reviewers) between comparison groups.
Intention-to-treat
MET = Intention to treat analysis performed or possible with data provided.
UNCLEAR = Intention to treat not reported, and cannot be verified by contacting the investigators.
NOT MET = Intention to treat analyses not done and not possible for reviewers to calculate independently.
Data analysis and presentation
We expressed binary outcome measures (for example, violent/not violent) as risk ratios (relative risks). Continuous measures were calculated as mean differences or (when different scales were used) standardised mean differences. We reported the 95% confidence intervals for all of the above.
If the primary studies were sufficiently homogenous, we performed a fixed-effect meta-analysis. Homogeneity was tested with the Q-test (Chi-square, P-value) and we measured degree of heterogeneity with I2 (I-squared, Higgins 2002). But a decision did not rest solely on the outcome of these procedures. In addition to the formal procedures, we also took into account common sense, the nature of the measures, etc. If there was statistically significant heterogeneity among studies’ effect sizes, a random-effects model was used. Effect sizes were pooled across studies using the DerSimonian and Laird method for random-effect models. For fixed-effect models we used the Mantel-Haenszel method for dichotomous data (except for data analysed using Peto's method) or the inverse variance method for continuous or generic inverse variance data. We also checked forest plots for detecting heterogeneity.
Cluster-randomised trials
No such trials were identified in this version of the review. See Table 10 for plans for future updates.
Dealing with dependent outcomes
In some primary studies, several different outcomes are measured on the same participants. Sometimes the same outcome is measured at multiple points in time. As these data are from the same sample of participants, and, therefore, are not independent estimates of treatment effect, we aimed to analyse the data in such a way that any analysis contained a single, most recent, outcome (one measure from a single point in time) from each sample. The rationale for using the most recent outcome was that we opted for the longest possible follow-up time. In cases with several treatment arms, we compared only one of the treatment arms with the control group. The decisions and rationale for this are reported separately for each study in the Results section.
Heterogeneity
When there was statistically significant heterogeneity among primary outcome studies, the following factors were considered as possible explanations:, voluntary or mandatory participation, intensity or length/period of the intervention, and differences in participant characteristics. If the primary studies were too heterogeneous to be grouped according to these characteristics, a meta-analysis was not performed. If there were many primary studies, we classified them according to these variables in order to identify possible sources of heterogeneity. We considered performing moderator analyses (stratification on subgroups, meta-analysis analogue to ANOVA, meta-regression) to explore how observed variables were related to heterogeneity.
Assessment of publication bias
We used a funnel plot (Fig 01 - Funnel plot) to explore the likelihood of publication bias. Asymmetry of the funnel plot may indicate possible publication bias in this review, but may also indicate other methodological or sample size issues within the trials. If asymmetry of the funnel plot was found, the clinical diversity of the studies was examined (Egger 1997).
Sensitivity analyses
Sensitivity analysis was inappropriate for this version of the review. See Table 10 for plans for future updates.
Description of studies
Results of the search.
From the initial search, 1969 records were identified, of which 1724 records were excluded as clearly irrelevant. Of the remaining 245 possibly relevant records, 75 were identified for further examination.
Included studies.
After reading the full text reports, 12 records were included. They reported results from six randomised trials conducted in the USA. None of the studies were cluster-randomised. There were two types of comparisons; four studies compared CBT with a non-intervention control, while two studies compared CBT with another active treatment (See Fig 02 -Flowchart).
CBT versus Control.
In the Bronx Exp. 2005 (Bronx Exp. 2005), 420 convicted male domestic violence offenders were randomised into four experimental conditions:(1) batterer programme plus monthly judicial monitoring, (2) batterer programme plus graduated monitoring, (3) monthly monitoring only, and (4) graduated monitoring only. The model assumes that battering is rooted in societal norms that support male abuse of women. In order to measure the effect of the batterer programme we chose to combine the two groups receiving the batterer programme with the two other groups not receiving the batterer programme. The men were tracked for 12 months after court-ordering, and for up to eighteen months for most of them. The programme was in a group format and lasted for 26 weeks.
In the Brooklyn Exp. 2000 (Brooklyn Exp. 2000), 376 court-mandated offenders were randomly assigned to batterer treatment or to a treatment irrelevant to the violence problem (40 hours of community service). The length of the batterer treatment was 39 hours, but some men were assigned to complete the treatment in 26 weeks and others in 8 weeks. Interviews with victims and offenders were attempted at six and twelve months after the court-order date. Records of criminal justice agencies were also checked to determine if new crime reports or arrests had occurred involving the same defendant and victim.
A total of 404 men convicted of misdemeanour in Broward County, Florida (Broward Exp. 2000) were randomly assigned to a batterer programme using the Duluth Model or to a control group involving one year probation. The Duluth Model includes a feminist, cognitive psychoeducational curriculum provided in a group session. Its intent is to help domestic violence offenders develop an understanding of how battering is part of a range of male behaviours that seek to control women. The researchers hypothesised that men with a high stake in conformity would have a lower likelihood of recidivating than those with a low stake in conformity. The offenders were interviewed at time of adjudication and six and twelve months post-adjudication. Probation records and computer checks with the local police for all new arrests were used to track the defendants for one-year post-adjudication.
The largest study in this review was conducted in the military (San Diego Navy 2000). Participants were servicemen in the navy who had been substantiated as having physically assaulted their wives. The 861 couples in the study were randomly assigned to four groups: a men's group (N = 218), a conjoint group (the men participating with their wives) (N = 216), a rigorously monitored group (N = 213), and a control group (N = 214). The men's group met weekly for six months and then monthly for another six months and included both didactic and process activities. In the didactic part of the sessions, group leaders addressed perpetrator attitudes and values regarding women and violence toward women and taught the men a variety of skills thought to be important to the successful elimination of the continued abuse of women (e. g. cognitive restructuring, empathy enhancement, communication skills, anger modification, and jealousy). The process part of the sessions involved dealing with issue raised in the didactic segments of the session as well as with other issues that emerged. The conjoint group was similar to the men's group except for the presence of wives. The rigorously monitored group was formed based on a “stake in conformity” strategy to determine if male perpetrators held accountable for their abusiveness toward their wives, using systematized and official monitoring procedures, would stop the continued abuse. The interventions were cognitive-behavioural and outcome data were collected both from the male servicemen and their female partners at roughly six-month intervals over the approximate 18-month experimental period. The interventions lasted for 12 months. We chose to compare the men's group with the control group because we thought that this comparison would be the most similar to the other included studies.
CBT versus Other therapy
In one study (Wisconsin Study 1996), 218 men were randomly assigned to receive either feminist-cognitive-behavioural group treatment (FCBT) or process-psychodynamic group treatment (PPT). FCBT focused on progressive relaxation, using coping thoughts, and becoming aware of feelings. PPT focused on childhood losses and rejections, childhood experience with violence and emotional safety in the group. FCBT also used leader role-play, lectures and giving advice, while PPT emphasised self-disclosure. Treatment integrity was verified through audio-taped recordings of each session. The partners of 79 % of the 136 treatment completers gave reports of the men's behaviour an average of two years post-treatment. There were also arrest records and self-reports by the men.
One study (Yale Study 2007), which was conducted in the state of Connecticut, randomly assigned substance dependent offenders with reported intimate partner violence to one of the following interventions: A 12-week substance abuse & domestic violence group (grounded in CBT) (N = 32) or a 12-week twelve-step facilitation group (N = 32). Data were collected using the SCID (Structured Clinical Interview for DSM-IV-TR), Addiction Severity Index, Substance Abuse Calendar, Conflict Tactics Scale Revised, breath samples, urine toxicology screens, and collateral reports from female partners at baseline, monthly, and post-treatment periods.
Methodological quality of included studies
All included trials were reported as randomised and the method of randomisation was adequate in four out of the six studies. Concealment of allocation was judged as adequate in three studies (Bronx Exp. 2005; San Diego Navy 2000, Yale Study 2007). In four studies it was clear that there were no systematic differences in treatment between groups aside from the experimental intervention (low risk of performance bias). Detection bias was unclear in all studies except for Yale Study 2007, that is, it was not clear whether the persons collecting the results were blind to treatment group allocation. It should be noted, however, that this may not be important whenever the outcomes are written criminal justice records. There were high or unclear attrition in five out of six studies. Only the Navy (San Diego Navy 2000) managed to keep most of the participants in the intervention. Intention-to-treat was met in all studies. The randomisation was frequently compromised by judges overriding the allocation because they did not want certain of the defendants to be in the control group. In sum, all studies had a high risk of bias except for the San Diego Navy 2000 Experiment (San Diego Navy 2000) which we judged to have a moderate risk of bias.
Results
CBT versus Control
Proportion new violence
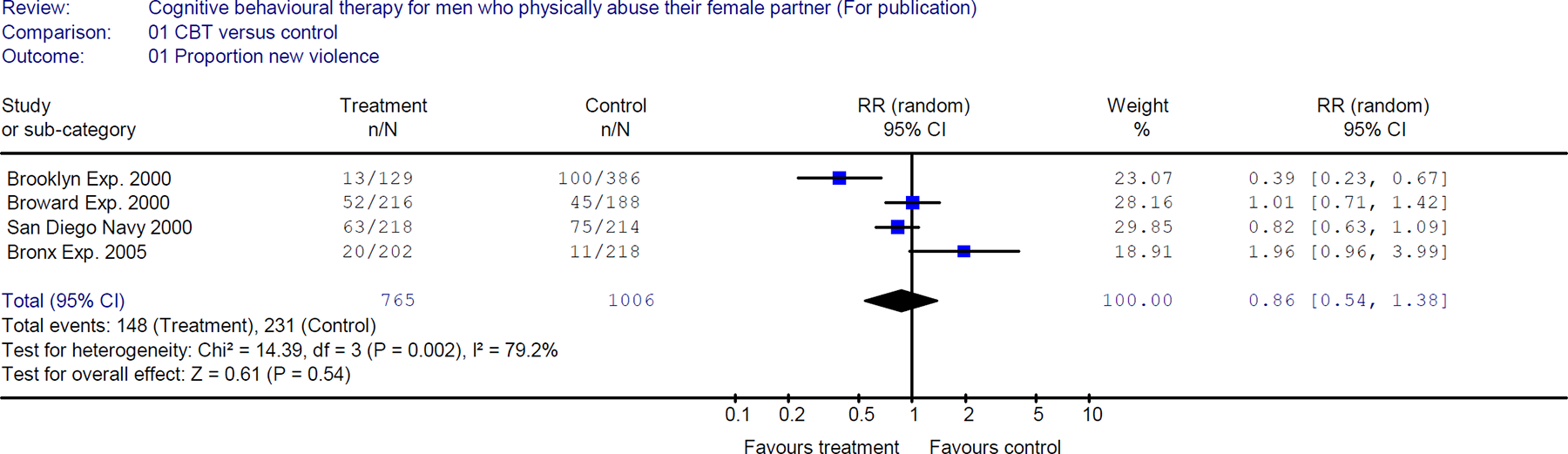
The relative risk of 1.96 in the Bronx Exp. 2005 (Bronx Exp. 2005) indicated that CBT had a harmful effect on new violence, but the 95% confidence interval from 0.96 to 3.99 was wide and not statistically significant. The CBT in the Brooklyn Exp. 2000 (Brooklyn Exp. 2000) had a clearly positive effect on new violence (relative risk: 0.39, 95% CI 0.23 to 0.67). This means that the intervention on average reduced violence by 61% relative to the control group. The relative risk in the Broward Exp. 2000 (Broward Exp. 2000) was 1.01 (no effect) with 95% confidence interval from 0.71 to 1.42. The results of the San Diego Navy 2000 Study (San Diego Navy 2000) showed a positive effect of the intervention compared to the control group (relative risk 0.82), but the effect was not statistically significant (95% CI 0.63 to 1.09).
In summary, four of the six included studies compared CBT with a control group looking at new violence. The effects were heterogeneous, with large effects in both directions. Only one study (Brooklyn Exp. 2000) showed a statistically significant effect, and it was positive. A meta-analysis involving 1771 men showed a risk ratio of 0.86, but the 95% confidence interval included zero difference (from 0.54 to 1.38).
CBT versus Other therapy
Wisconsin Study 1996 (FCBT versus PPT)
Proportion new violence
The risk ratio (1.07) of the Wisconsin Study 1996 (Wisconsin Study 1996) was not statistically significant (95 percent confidence interval from 0.68 to 1.68).
Yale Study 2007 (SADV versus twelve step facilitation)
Frequency of new violence
In the Yale study (Yale Study 2007), the mean number of reported violent episodes per month was higher at post-treatment in the SADV group (0.95) than in the TSF group (0.73). This corresponds to a standardised mean difference of 0.30 (95% CI: -0.22 to 0.81).
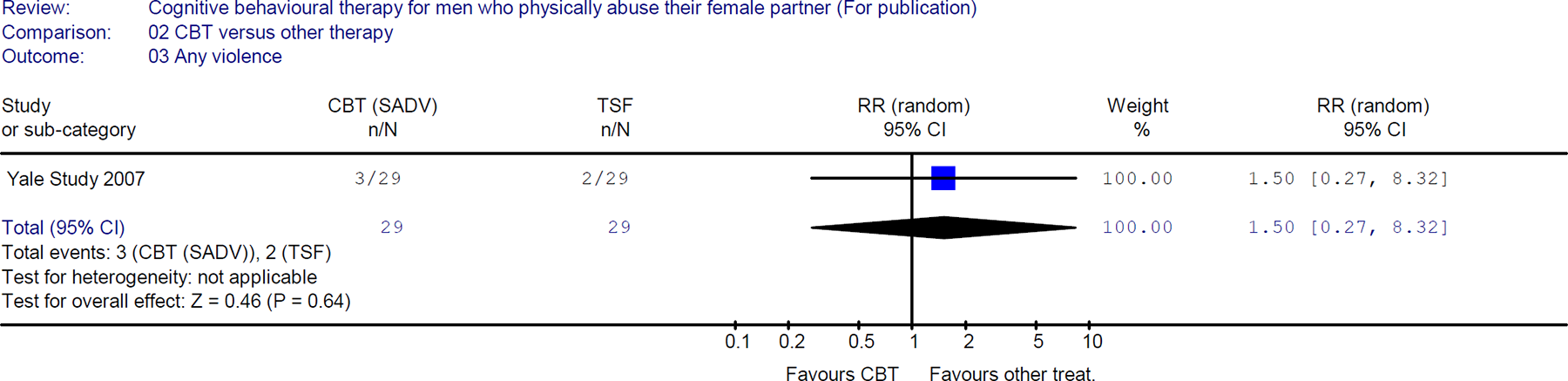
Presence of new violence
There were reports of violence for three of the men in the SADV group and for two men in the TSF group. This corresponds to a risk ratio of 1.50 (95% CI: 0.27 to 8.32).
Discussion
There have been few randomised evaluations of cognitive behavioural therapy for men who physically abuse their female partner. All such studies have so far been conducted in the USA. The studies also have relatively small sample sizes, the largest study having 861 participants. This review has employed an extensive search strategy with no restrictions on publication language or geographical region. Because there were so few studies, we could not model sources of heterogeneity using e. g. meta-regression or stratified analyses. Only one meta-analysis was performed. The results were inconsistent and heterogeneous, but there was no clear evidence for publication bias (Figure 01). The number of studies in this funnel plot (N = 4) is, however, so small that great caution should be taken in its interpretation. The methodological quality of the included studies was generally low (Table 01). The concealment of the random allocation sequence was mostly unclear or not met. Furthermore, it was mostly unclear whether the assessors of the results were aware of group allocation. Finally, the attrition was either unclear or high. Unclear concealment of allocation and high attrition both contribute to high risk of selection bias, but blinding of the assessors is probably not of serious concern because criminal justice records are in written form.
Two anonymous peer-reviewers pointed to a number of issues pertaining to contemporary US debates which should be mentioned here. The partners of the male perpetrators were offered some support. This support might have made the partners more able to report new violence, independently of the effect of the interventions on the men. This review focuses exclusively on effects on physical violence. But even where interventions may have an impact on physical violence, perpetrators may continue or possibly increase the use of emotionally controlling behaviours (Dobash 2000). Reliance on criminal justice records is also problematic because much violence is never recorded by the police. Some authors have been worried about whether assignment to a batterer intervention programme actually sends an implicit message that contradicts its official aim, namely that battering will not be taken seriously. This raises another debate: although some form of monitoring for compliance was present in all of the studies reviewed, sanctions for noncompliance are very rare. Moreover, the issue of attendance versus drop-out raises the important issue of selection bias, namely whether men who complete programmes are more motivated to stop their violence than those who never attend or drop out. While randomised controls should eliminate selection bias, the poor ways in which compliance is monitored suggest this may not be so. This review focuses on behaviour change, but many programmes actually view behavioural change as unlikely. They focus more on message sending and re-education or education.
CBT is a broad category that encompasses many different approaches. The most widely used model in the US, the Duluth Model, is included in this review because it has components of CBT. Not to include this model would eliminate most batterer intervention programmes in the US. But the fact that it has such components does not mean that everyone recognises it as a form of CBT. The Duluth Model includes strong elements of anti-sexist messaging, for instance, whereas traditional CBT approaches do not.
Care should be taken when generalising the results of this review to other parts of the world. First, there may be different baseline risk of violence across populations. Second, the motivation to comply with the treatment might vary greatly across populations of violent men. Men have different reasons for being in therapy. Their wives might have threatened to leave them if they do not enter therapy, or the men might have been court-ordered to take part. The men differ in their degree of stake in conformity, and such variables (employment and age) have predicted both attendance at treatment and re-offending (Broward Exp. 2000).
Reviewers’ conclusions
Implications for practice
The research evidence is insufficient to draw conclusions about the effectiveness of cognitive behavioural interventions for spouse abusers in reducing or eliminating male violence against female partners. Note that this does not mean that there is evidence for no effect. We simply do not know whether the interventions help, whether they have no effect, or whether they are harmful.
Implications for research
In the USA, and in other countries, there is a need for more, and larger-scale, randomised interventions. This has been possible in other fields, such as welfare-to-work (Smedslund 2006), where the weight of evidence involves randomised evaluations with more than 400,000 participants. Each primary study has randomised several thousands of participants. In the rest of the world there has been a complete lack of randomised interventions. Such interventions are highly needed in order to estimate the effects of CBT on domestic violence, even though this might not be as easy to accomplish with domestic violence as it was with welfare-to-work.
Internal sources of support
Norwegian Knowledge Centre for the Health Services, NORWAY
External sources of support
Nordic Campbell Centre, DENMARK
Contribution of reviewers
Dalsbo and Smedslund wrote the protocol.
All reviewers independently screened literature, reviewed potential trials, and extracted data. Smedslund analysed the data. Smedslund wrote the text of the completed systematic review. Steiro, Winsvold and Clench-Aas contributed by giving comments, assessing studies and acting as mediators if necessary. Responsibility for updating the review is jointly shared between Dalsbo and Smedslund.
Acknowledgements
Many thanks to Torill Johme for contributing to the planning of the study, for literature screening, hand-searching, and for performing the initial searches in 2003.
Thanks to Sigrun Espelien Aasen for carrying out updated searches in November-December 2006. We also want to acknowledge the Norwegian Directorate for Health and Social Affairs, which housed us and funded us during the initial phase of the development of this review. We are also grateful for the support by Andy Oxman during the start-up. Last, but not least, we want to thank Jane Dennis, the review group coordinator of the Cochrane Developmental, Psychosocial and Learning Problems Group for her continuous support and help in dealing with a number of different review authors and with different drafts leading up to the final review.
This review is co-registered within the Cochrane Developmental, Psychosocial and Learning Problems Group (Cochrane Collaboration).
Potential conflict of interest
None known.
Characteristics of included studies
Characteristics of excluded studies
Footnotes
Table of comparisons
01 CBT versus control
01 Proportion new violence
02 CBT versus other therapy
01 Proportion new violence
02 Frequency of violence
03 Any violence
Additional tables
Additional tables
Additional tables
Additional tables
Additional tables
Additional tables
Additional tables
Additional tables
Additional tables
Additional tables
Additional figures
Notes
Contact details for co-reviewers
Asbjørn Steiro
The Norwegian Health Services Research Centre
PB 7004 St. Olavs plass
Oslo
NORWAY
N-0130
E-mail:
Aina Winsvold
Norwegian Knowledge Centre for Heatlh Services
PB7004
Oslo
NORWAY
N-0130
E-mail:
Jocelyne Clench-Aas
Norwegian Institute of Public Health
PO BOX 4404 Nydalen
Oslo
NORWAY
N-0403
Telephone 1: +47 23408361
E-mail:
Therese K Dalsbø
Almeveien 36
Oslo
NORWAY
0855
Telephone 1: +47 48271234
E-mail:
Review: Cognitive behavioural therapy for men who physically abuse their female partner (Version 04)
| Comparison or outcome | Studies | Participants | Statistical method | Effect size |
|---|---|---|---|---|
| 01 CBT versus control | ||||
| 01 Proportion new violence | 4 | 1771 | RR (random), 95% CI | 0.86 [0.54, 1.38] |
| 02 CBT versus other therapy | ||||
| 01 Proportion new violence | RR (random), 95% CI | No total | ||
| 02 Frequency of violence | 1 | 58 | SMD (random), 95% CI | 0.30 [-0.22, 0.81] |
| 03 Any violence | 1 | 58 | RR (random), 95% CI | 1.50 [0.27, 8.32] |


*
indicates the primary reference for the study