
Abstract
Adolescent parents face a range of problems. They are often from very deprived backgrounds; they can experience a range of mental health problems and a lack of social support; they often lack knowledge about child development and effective parenting skills, and they have developmental needs of their own. Possibly for these reasons, the children of teenage parents often have poor outcomes.
A range of interventions are being used to promote the well-being of teenage parents and their children. Parenting programmes have been found to be effective in improving psychosocial health in parents more generally (including reducing anxiety and depression, and improving self-esteem), alongside a range of developmental outcomes for children. This review therefore investigated the impact of parenting programmes aimed specifically at teenage parents on outcomes for both them and their children.
The findings are based on eight studies measuring a variety of outcomes, using a range of standardised measures. It was possible to combine results (meta-analysis) for nine comparisons. Results from four of these meta-analyses suggest that parenting programmes may be effective in improving parent responsiveness to the child, and parent child interaction, both post-intervention and at follow-up. Infant responsiveness to the mother also showed improvement at follow-up. The results of the other five meta-analyses we carried out were inconclusive.
Further rigorous research is needed that provides both short- and long-term follow-up of the children of teenage parents, and that assesses the benefits of parenting programmes for young fathers as well as young mothers.
Abstract
Background
Parenting programmes are a potentially important means of supporting teenage parents and improving outcomes for their children, and parenting support is a priority across most Western countries. This review updates the previous version published in 2001.
Objectives
To examine the effectiveness of parenting programmes in improving psychosocial outcomes for teenage parents and developmental outcomes in their children.
Search strategy
We searched to find new studies for this updated review in January 2008 and May 2010 in CENTRAL, MEDLINE, EMBASE, ASSIA, CINAHL, DARE, ERIC, PsyclNFO, Sociological Abstracts and Social Science Citation Index. The National Research Register (NRR) was last searched in May 2005 and UK Clinical Research Network Portfolio Database in May 2010.
Selection criteria
Randomised controlled trials assessing short-term parenting interventions aimed specifically at teenage parents and a control group (no-treatment, waiting list or treatment-as-usual).
Data collection and analysis
We assessed the risk of bias in each study. We standardised the treatment effect for each outcome in each study by dividing the mean difference in post-intervention scores between the intervention and control groups by the pooled standard deviation.
Main results
We included eight studies with 513 participants, providing a total of 47 comparisons of outcome between intervention and control conditions. Nineteen comparisons were statistically significant, all favouring the intervention group. We conducted nine meta-analyses using data from four studies in total (each meta-analysis included data from two studies). Four meta-analyses showed statistically significant findings favouring the intervention group for the following outcomes: parent responsiveness to the child post-intervention (SMD -0.91, 95% CI -1.52 to -0.30, P = 0.04); infant responsiveness to mother at follow-up (SMD -0.65, 95% CI -1.25 to -0.06, P = 0.03); and an overall measure of parent-child interactions post-intervention (SMD -0.71, 95% CI -1.31 to -0.11, P = 0.02), and at follow-up (SMD -0.90, 95% CI -1.51 to -0.30, P = 0.004). The results of the remaining five meta-analyses were inconclusive.
Authors' conclusions
Variation in the measures used, the included populations and interventions, and the risk of bias within the included studies limit the conclusions that can be reached. The findings provide some evidence to suggest that parenting programmes may be effective in improving a number of aspects of parent-child interaction both in the short- and long-term, but further research is now needed.
Plain language summary
Parenting programmes for teenage parents and their children
Adolescent parents face a range of problems. They are often from very deprived backgrounds; they can experience a range of mental health problems and a lack of social support; they often lack knowledge about child development and effective parenting skills, and they have developmental needs of their own. Possibly for these reasons, the children of teenage parents often have poor outcomes.
A range of interventions are being used to promote the well-being of teenage parents and their children. Parenting programmes have been found to be effective in improving psychosocial health in parents more generally (including reducing anxiety and depression, and improving self-esteem), alongside a range of developmental outcomes for children. This review therefore investigated the impact of parenting programmes aimed specifically at teenage parents on outcomes for both them and their children.
The findings are based on eight studies measuring a variety of outcomes, using a range of standardised measures. It was possible to combine results (meta-analysis) for nine comparisons. Results from four of these meta-analyses suggest that parenting programmes may be effective in improving parent responsiveness to the child, and parent-child interaction, both post-intervention and at follow-up. Infant responsiveness to the mother also showed improvement at follow-up. The results of the other five meta-analyses we carried out were inconclusive.
Further rigorous research is needed that provides both short- and long-term follow-up of the children of teenage parents, and that assesses the benefits of parenting programmes for young fathers as well as young mothers.
Background
Description of the condition
The rate of births to teenage parents
Research examining the rate of births to women aged 15 to 19 in the Organisation for Economic Co-operation and Development (OECD) countries showed that the lowest birth rates (2.9 to 6.5 per 1,000) were to be found in Korea, Japan, Switzerland, the Netherlands, and Sweden, and that the highest birth rates (52.1 per 1,000) were to be found in the USA, which has about four times the European Union average, and the UK, which has the highest teenage birth rate in Europe (30.8 per 1,000) (
Outcomes of teenage pregnancy
Although there is some recognition that teenage pregnancy can be a positive experience, particularly in the later teenage years (
Young parenthood is often viewed as reinforcing social disadvantage because of the perceived consequences in terms of the teenage mother's life chances (
Research also suggests that the children of teenage parents may have poorer outcomes in terms of educational attainment, emotional and behavioural problems, and higher rates of illness, accidents and injuries (
Description of the intervention
Parenting programmes for teenage parents
Services targeting teenage parents remain a policy priority in many Western countries including the UK (
Standard parenting programmes are focused short-term interventions aimed at helping parents improve their functioning as a parent, and their relationship with their child, and preventing or treating a range of child emotional and behavioural problems by increasing the knowledge, skills and understanding of parents. They typically involve the use of a manualised and standardised programme or curriculum, and are underpinned by a number of theoretical approaches (including Behavioural, Family Systems, Adlerian, and Psychodynamic). They can involve the use of a range of techniques in their delivery including discussion, role play, watching video vignettes, and homework. They are typically offered to parents over the course of eight to 12 weeks, for about one to two hours each week, in a range of settings including hospital/social work clinics and community-based settings such as GP surgeries, schools and churches.
Although parenting programmes that are explicitly designed for teenage parents have much in common with standard parenting programmes, there may be important variations. For example, parenting programmes for teenagers may devote more time to factors that affect this ‘hard-to-reach’ group in terms of influencing their uptake and continuation with the programme, and in specifically addressing their communication needs. Such programmes may also focus more explicitly on aspects of parenting that research suggests may be difficult for teenage parents, such as understanding the developmental needs of their child.
How the intervention might work
The evidence suggests that adolescent parents have unmet developmental needs of their own; that they are often from very deprived backgrounds; that they may be experiencing a range of mental health problems and lack of social support, and that they often lack knowledge about child development and effective parenting skills. The evidence suggests that parenting programmes have learning components that appear to address many of the issues confronting teenage parents. For example, a meta-ethnography of qualitative studies suggests that the acquisition of knowledge, skills and understanding, together with feelings of acceptance and support from other parents in the parenting group, are important in enabling parents to regain control, and in the development of feelings of being able to cope, which then leads to a reduction in feelings of guilt and social isolation, increased empathy with their children, and greater confidence in dealing with their behaviour (
Why it is important to do this review
While recent reductions in the rates of births to teenagers may be testament to the success of some of the many prevention initiatives now targeting teenage parents, the prevalence of teenage pregnancy continues to be high. Interventions such as parenting programmes that potentially address some of the aetiological factors involved in the transmission of poor outcomes from teenage parents to their children (for example, by improving parental mental health and maximizing parenting skills) may be crucial in optimising well-being for both teenage parents and their children (
Objectives
To evaluate the effectiveness of individual and group-based parenting programmes in improving the psychosocial health of teenage parents and the developmental health of their children.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials and quasi-randomised trials in which participants were allocated to an experimental or a control group, the latter being a waiting-list or no-treatment group (including treatment-as-usual or normal service provision).
Types of participants
Parents aged 20 or under, from either clinical or population samples, and their infants/children. The upper age limit of 20 was used because this is consistent with the WHO definition of adolescent parents, thereby enabling the inclusion of international studies.
Types of interventions
Studies evaluating parenting programmes that met all of the following criteria were included in the review: Individual or group-based format; Offered ante- and post-natally or just post-natally to teenage mothers and/or teenage fathers; Based on the use of a structured format; Focusing on the improvement of parenting attitudes, practices, skills/knowledge, or well-being.
Parenting programmes which met any of the following criteria were excluded from the review: Standard antenatal programmes specifically addressing the pregnancy care needs of teenagers, and programmes provided during the ante-natal period only; Programmes not specifically aimed at adolescent parents; Evaluations of programmes that were aimed at parents of disabled children, children with long-term health problems or pre-term infants; Programmes involving direct work with the children of teenage parents; Programmes that were aimed exclusively at the prevention or reduction of teenage pregnancy; Programmes in which the parenting programme was combined with a home visiting intervention.
While home visiting programmes, and parenting programmes combined with home visiting programmes, have been excluded from this review, manualised, short-term (i.e. less than 20 week) parenting programmes that are delivered on a one-to-one basis in the home have been included. This reflects the fact that home-visiting programmes are qualitatively different interventions (for example, broad based support which is provided on a frequent basis over an extended period of time) to parenting programmes that are delivered in the home (for example, brief, structured programmes with a specific focus on parenting).
Types of outcome measures
Primary outcomes
psychosocial heath; parenting knowledge; parenting behaviours and skills; sense of competence in the parenting role; parent interaction with child.
child cognitive development; child interaction with parent.
any combined parent-child interaction.
Within each generic category of outcome there are sub-outcomes, which will also be included; for example, parental psychosocial health includes depression, anxiety and stress, and self-esteem. Child health and development similarly covers a wide range of outcomes such as cognitive and language development, both of which may have further sub-outcomes. Outcomes were measured using a range of standardised and validated parent-report and objective assessment instruments (see ‘Outcomes’ below).
Search methods for identification of studies
Electronic searches
For this update we searched the following electronic databases: MEDLINE (1950 to May 2010) searched 6 May 2010 MEDLINE (1966 to January 2008) searched 24 January 2008 EMBASE (1980 to current) searched 6 May 2010 and 24 January 2008 CENTRAL (2010, Issue 2) searched 6 May 2010; (2008, Issue 10) searched 24 January 2008 DARE (The Cochrane Library 2010, Issue 4) searched 6 May 2010; DARE (The Cochrane Library 2008 Issue 1) searched 24 January 2008 CINAHL (1982 to May 2010) searched 6 May 2010 and 24 January 2008 PsyclNFO (1872 to May 2010) searched 6 May 2010 and 24 January 2008 Social Science Citation Index (1956 to 6 May 2010) searched 6 May 2010 and 24 January 2008 ASSIA (1980 to 6 May 2010) searched 6 May 2010 and 24 January 2008 Sociological Abstracts (1963 to May 2010) searched 6 May 2010 and 24 January 2008 ERIC (1966 to 6 May 2010) searched 6 May 2010 and 24 January 2008 UK Clinical Research Network Portfolio Database searched 6 May 2010 National Research Register 2005 (Issue 1)
The search strategies used at this update, for each database, can be found in Appendix 1; Appendix 2; Appendix 3; Appendix 4; Appendix 5; Appendix 6; Appendix 7: Appendix 8; Appendix 9. An RCT filter was not used to ensure that the search was as inclusive as possible, and no language or date restrictions were applied. The original searches were run in 2000. We repeated the searches in 2008 and 2010 with the exception of the National Research Register which had ceased to exist by the time of this update.
Search terms and the databases used in the previous published version of the review can be found in Appendix 10.
Searching other resources
Reference lists of articles identified through database searches were examined to identify further relevant studies. Bibliographies of systematic and non-systematic review articles were also examined to identify relevant studies. We contacted trial investigators for further information where details of trial conditions or outcome data were needed. No additional handsearching was conducted but the results of handsearches carried out by all Cochrane review groups are added to CENTRAL.
Data collection and analysis
Selection of studies
For the first published versions of the review, we reviewed titles and abstracts of studies identified through searches of electronic databases, to determine whether they met the inclusion criteria. Esther Coren (EC) identified titles and abstracts and EC and Jane Barlow (JB) read and reviewed these. Two independent review authors (EC and JB) assessed full copies of those papers which appeared to meet the inclusion criteria. We resolved uncertainties concerning the appropriateness of studies for inclusion in the review by consultation with a third person (Sarah Stewart-Brown). For the updated review produced in 2010, Nadja Smailagic (NS) and Nick Huband (NH) carried out the eligibility assessments in consultation with EC, JB and Cathy Bennett (CB). JB had overall responsibility for the inclusion or exclusion of studies in this review.
Data extraction and management
For the updated review, data were extracted independently by two reviewers (NS and NH) using a data extraction form and entered into Review Manager 5. Where data were not available in the published trial reports, we contacted trial investigators to ask them to supply missing information.
Assessment of risk of bias in included studies
For each included study, two authors (NS and NH) independently completed the Cochrane Collaboration's tool for assessing risk of bias ( the allocation sequence was adequately generated (‘sequence generation’); the allocation was adequately concealed (‘allocation concealment’); knowledge of the allocated interventions was adequately prevented during the study (‘blinding’); incomplete outcome data were adequately addressed; reports of the study were free of suggestion of selective outcome reporting; and the study was free of other problems that could put it at high risk of bias.
Each domain was allocated one of three possible categories for each of the included studies: ‘Yes’ for low risk of bias, ‘No’ for high risk of bias, and ‘Unclear’ where the risk of bias was uncertain or unknown.
Measures of treatment effect
We present the standardized mean differences (SMD) and 95% confidence intervals for individual outcomes in individual studies. The SMD was calculated by dividing the mean difference in post-intervention scores between the intervention and control groups by the pooled standard deviation.
Unit of analysis issues
The randomisation of clusters can result in an overestimate of the precision of the results (with a higher risk of a Type I error) where their use has not been compensated for in the analysis. To address the effects of including cluster randomised trials in the meta-analyses, we conducted sensitivity analyses to assess the influence of clustering, using plausible values of ICC. None of the included studies involved cross-over randomisation.
Dealing with missing data
We assessed missing data and drop-outs for each included study.
Assessment of heterogeneity
An assessment was made of the extent to which there were between-study differences including the extent to which there were variations in the population, intervention or outcomes. While thresholds for the interpretation of I2 can be misleading since the importance of inconsistency depends on several factors, I2 > 50% was treated as evidence of substantial heterogeneity, the importance of the observed value of I2 being dependent on the magnitude and direction of effects and strength of evidence for heterogeneity (for example, the P value from the chi-squared test, or a confidence interval for I2) (
Data synthesis
Where appropriate, we used meta-analyses to combine comparable outcome measures across studies, using a fixed-effects model. The weight given to each study in each meta-analysis represents the inverse of the variance, such that the more precise estimates (i.e. from larger studies with more events), have been given more weight. Where there was evidence of statistically significant heterogeneity, we tested the robustness of the results using a random effects model.
Results
Description of studies
Results of the search
The updated electronic searches in January 2008 produced 2,666 records. Two reviewers (NS and NH) independently examined the titles and abstracts. The majority of articles reviewed were written in English. We obtained a translation of one German study (
Included studies
Four new studies (
Outcomes and outcome measures in the included studies
The full references to each scale given in this table appear in the bibliographies of the included studies and are not supplied in this review.
All eight included studies were randomised controlled trials.
Two studies comprised cluster randomised controlled trials (
Five studies were single-centre trials (
The majority of studies were two-condition comparisons of individual or group-based teenage parenting programmes compared with a control group (
None of the included studies provided details regarding the sample size calculations or information about the size of the changes that the study was powered to detect. One large multi-centre trial (
In total, the eight studies included 351 participants in their analyses, with a range from 16 to 95 participants.
Two studies were conducted in Canada (
Two studies recruited participants from outpatient settings on the basis of age (
Four studies (
Participants comprised primary carer-index child pairs. All the studies targeted primary carers below the age of 20, who were adolescent mothers or were pregnant. The age range was 13 to 20 years. The mean age was 17 years in seven studies. One study (
The studies included in this review were largely directed at teenage mothers alone. While one study included two adolescent fathers, their results were excluded from the analysis (
Three of the included studies evaluated the effectiveness of standard group-based parenting programmes delivered over the course of between six to 10 weeks (
The included studies used a range of instruments to measure outcomes, using a wide range of scales, and sub-scales. Many of these could not be combined because they were not measuring sufficiently similar underlying conditions. For example, although depression and self-esteem are both aspects of psychosocial well-being, we did not consider that it was appropriate to combine them (see Table 1).
We provide an overview of the outcomes and the instruments used to measure them in
A) Parental psychosocial
All eight included studies reported parental psychosocial outcomes. Two studies (
B) Child health and development
Three studies (
C) Combined parent-child relationship
Two studies (
Five studies provided an assessment of outcome immediately post-intervention (
Excluded studies
In the previous published version of the review, we excluded 19 studies. Following the updated searches in 2008 (2666 records), we obtained 40 full text copies, and we excluded 36. We discarded eleven of these 36 of these as irrelevant; 22 of these 36 appear in the excluded studies table (
From the searches in May 2010, we excluded seven studies (
Of the 48 excluded studies, 20 were not randomised or the allocation method was unclear (with no further details available from the trial investigator) (
Risk of bias in included studies
We assessed risk of bias for the eight included studies (see
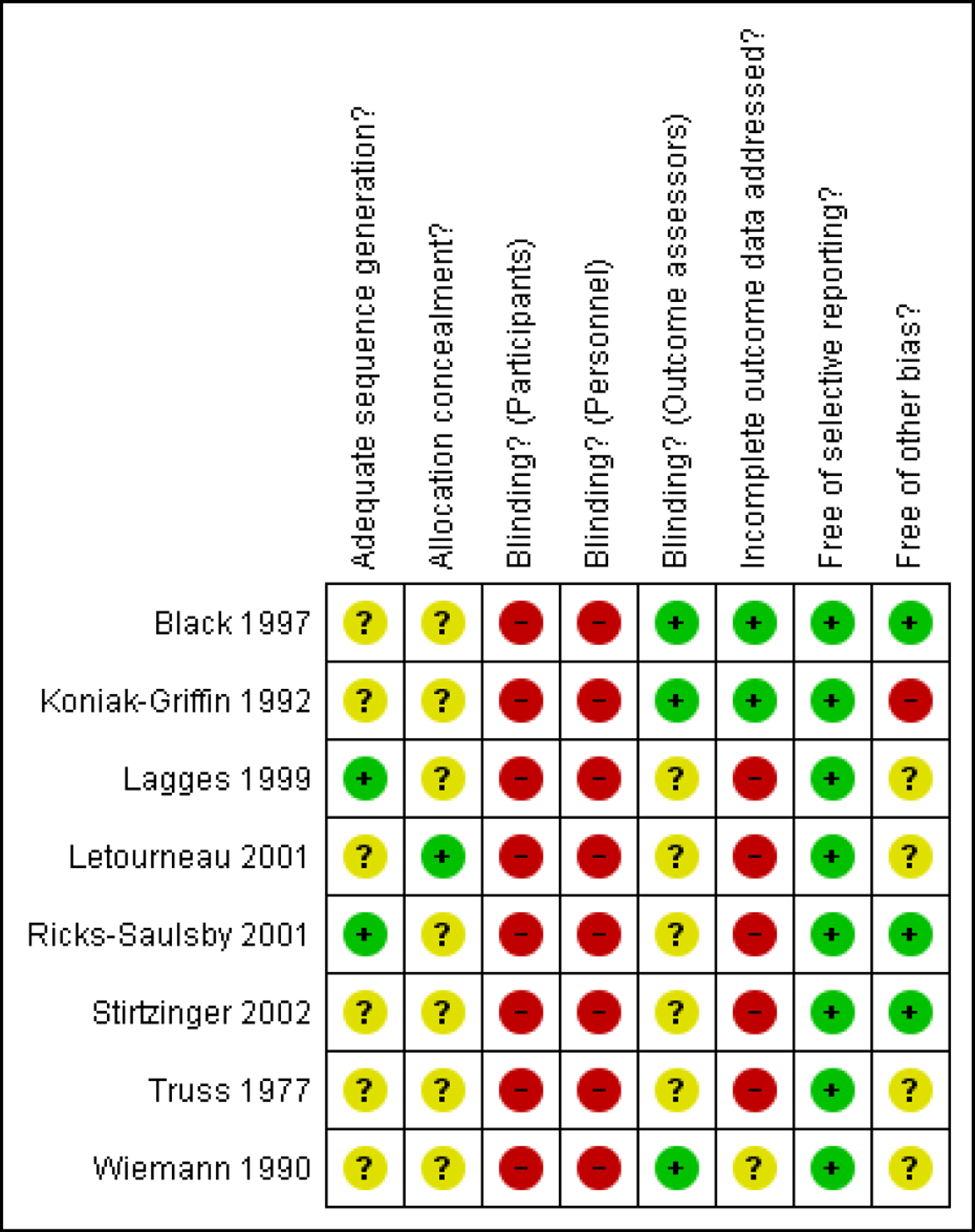
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Only one study described the method of sequence generation (
Blinding
No study adequately blinded participants and personnel because it is not possible to fully blind either participants or personnel in this type of study. This constitutes a source of potential bias. Only two studies blinded assessors for all outcomes (
Incomplete outcome data
One study provided information concerning the reason for incomplete data (
Selective reporting
We did not identify any indications of bias due to selective reporting in the eight included studies.
Other potential sources of bias
While the use of randomisation should in theory ensure that any possible confounders are equally distributed between the arms of the trial, the randomisation of small numbers may result in an unequal distribution of confounding factors. It is therefore important that the distribution of known potential confounders is either (i) compared between the different study groups at the outset, or (ii) adjusted for at the analysis stage.
Six studies provide information about the distribution of potential confounders (
Effects of interventions
The included studies reported data that had been collected using a range of outcome instruments. We were unable to combine much of the reported data using meta-analysis because of the following: i) a wide range of divergent outcomes were measured; ii) the outcomes were not measured at comparable time points; iii) assessments were reported for the same group of participants using a number of subscales (i.e. which would have led to double counting of the participants).
The results presented in the
Table 1 provides full details of the individual outcomes reported in each of the included studies, and the results of the meta-analyses. This table also lists the outcome measures that we combined using meta-analysis and directs the reader to the relevant analysis. Table 1 also provides additional information about the time-point at which measurement was undertaken, and the direction of the scales used (i.e. whether a high score represents improvement or deterioration).
A narrative summary is provided below of the individual study results for each primary outcome and the results of the meta-analyses.
The eight included studies provided data on a total of 47 comparisons of outcome between intervention and control conditions. Nineteen of these comparisons were statistically significant, either at post-intervention or follow-up, each favouring the intervention. These are organised by outcome and by time point in Analyses 1 to 7.
We were able to carry out meta-analyses of parent-training versus control for four outcomes: Parent psychosocial outcomes - sense of competence in parental role; Parent psychosocial outcomes - parent interaction with child; Child health and development outcomes - child interaction with parent; Combined parent-child relationship - any combined parent-child interaction.
The results presented below are organised by outcome and measurement time-point (Analyses 8 to 11). The results are presented as effect-sizes with 95% confidence intervals. A minus sign indicates that the result favours the intervention group. We used post-intervention scores and follow-up scores to calculate effect sizes rather than change scores (i.e. pre- to post-scores for each group). This reflects the fact that a change standard deviation is required to calculate change scores, and these data were not available for any of the included studies.
We combined data for three outcomes assessing different aspects of parent-infant interaction (for example, parent responsiveness; infant responsiveness; combined interaction) derived from two studies, producing a total of five metaanalyses. We also combined data from two further studies assessing parenting competence in four meta-analyses, producing nine meta-analyses in total. Four of five meta-analyses using data from the two studies
The fifth meta-analysis using data from
The four meta-analyses of parenting competence using data from two further studies
Parental psychosocial outcomes
One study (
No studies used validated outcome scales to measure parenting behaviour or skills (see Table 1).
Non-significant results at both time points were reported for self-confidence in infant care, measured by the ‘Pharis Self-Confidence Scale’ (PS-CS) - mother report (
Two outcome measurements from passive learning versus control comparisons indicated significant results favouring the control group: AAPI-Appropriate developmental expectations of children (at post-intervention: SMD 0.73; 95% CI 0.08 to 1.38;
The remaining outcomes from
No other results were significant for the parent-child interaction outcomes reported by
Child health and development outcomes
None of the individual study results were statistically significant at post-intervention or follow-up. Follow-up data from two studies (
Combined parent-child relationship
Five post-intervention parent-child outcome measurements were available from two studies (
The NCATS-Total score (i.e. teaching scale) (SMD -1.14 85%CI -2.22 to -0.06;
NCATS-Contingency at post-intervention and follow-up (
The remaining follow-up results (
Parental psychosocial outcomes
Two studies (
Child health and development outcomes
Two studies (
Combined parent-child relationship
Two studies (
At follow-up, two studies (
Discussion
Summary of main results
Although the addition of four studies to the four included in the original review has increased the overall number of participants, we could not combine many of the data in a meta-analysis due to the diversity of the outcomes measured. Furthermore, there was considerable diversity amongst the parenting programmes in terms of their duration and content (see below for further discussion).
It was only possible to combine data for a limited number of outcomes from four studies, producing a total of nine meta-analyses (Analyses 8 to 11). Four meta-analyses assessed parental attitudes to child rearing using the Adult-Adolescent Parenting Inventory and were not able to establish if parent training was effective or not. The remaining five meta-analyses assessed parent interactions with infants, using a number of sub-scales of the Nursing Child Assessment Teaching Scale (NCATS), and, while it is difficult to draw conclusions from one of these due to high heterogeneity, four found large effect sizes (ranging from 0.65 through to 1.07) favouring the intervention group.
Of the remaining 47 individual study assessments of outcome, 19 produced statistically significant effect sizes favouring the intervention group. These results suggest that parenting programmes directed specifically at teenage parents may be effective in improving important infant and child outcomes such as the infant's response to the parent, the clarity of the infant's cues and the child's ability to understand and respond to language. One study reported large significant changes in maternal sensitivity, maternal identity, maternal self-confidence, and the cognitive growth-fostering capacities of the mother (
Overall completeness and applicability of evidence
The included studies reflect the wide range of settings in which interventions for teenage parents are provided, including schools (
The generalisability of the results obtained from the included studies is limited for a number of reasons. Some studies targeted teenage parents experiencing very specific problems (for example, teenage parents with depressive symptoms (
Although the interventions were delivered using both individual and group-based formats, it was not possible to examine the impact of individual or group format on outcomes for parents and their children. Peer group relations may be an important component of such interventions for teenage parents, and although the potential role of the group process in interventions with teenage mothers has been acknowledged, there is very little research available to date that addresses its impact (
All of the included studies involved parents who had volunteered to take part in the study. Parents who volunteer to take part in parenting programmes may not be representative of the wider group of parents, perhaps most importantly due to the fact that volunteers are very often better motivated than parents who have been referred by professional agencies. This, once again, limits the generalisability of the results.
Although there is some recognition that parenting programmes can have adverse effects such as increasing the tension between parents when only one parent attends the programme (
Quality of the evidence
Overall, the evidence base for teenage parent parenting programmes is of poor quality with many threats to internal validity and significant risk of bias.
Potential biases in the review process
We did not attempt to identify evidence of harmful outcomes in this review, and indeed, none of the included studies identified evidence of harm.
Agreements and disagreements with other studies or reviews
The wider evidence with regard to parenting programmes for parents generally suggests that they are largely effective with diverse populations of parents, and to that extent the largely positive, albeit statistically non-significant, findings of the current review, are consistent with the broader evidence base on this topic. However, teenage parents are a highly vulnerable group with very specific needs relating to their age and stage of development. Home visiting programmes, which comprise a more intensive intervention (i.e. often beginning ante-natally and continuing for up to two years postnatally), and that target much broader outcomes aimed explicitly at addressing the issue of social exclusion (i.e. parental education, training and return to work), may be better suited to meeting their needs. Parenting programmes may therefore have a more limited role in terms of providing support to teenage parents, and should possibly be used alongside more intensive forms of provision.
Authors' conclusions
Implications for practice
Although the included studies suggest some benefits of parenting programmes for teenage parents and their children, particularly those that focus on improving early parent-infant interaction, the methodological quality of the included studies was poor, and there was significant clinical heterogeneity in terms of the focus and duration of the interventions, and indeed the age of the children targeted. As such, it is not possible at the current time to be clear what the necessary ingredients of successful parenting programmes for teenage parents comprise or which outcomes they have most impact on, and further research is required.
Implications for research
This review shows that the available evidence on the effectiveness of parenting programmes for teenage parents is wide ranging (for example, varying widely in content, duration and format), and there is a need for further evidence that explicitly evaluates the impact of different programmes. For example, the evidence suggests that brief video-interaction guidance can help improve the interactions of teenage parents with their babies and further research should be undertaken to evaluate the effectiveness of this particular format of provision.
The conclusions that can be reached at the current time are limited by the lack of consistent measurement across the various studies both in terms of the outcomes measured, and also the time points at which measures were assessed. This review points to the need for more consistent measurement of the effectiveness of both individual and group-based parenting programmes in improving both parental and infant/child outcomes. There is also a need for studies that recruit larger numbers of teenage parents thereby improving the external validity of the research. Future studies should include parents other than volunteers, i.e. parents who have been referred to parenting programmes. There is also a need to include teenage fathers or fathers of the children of teenage mothers in studies of the effectiveness of parenting programmes targeting teenage parents.
None of the included studies discussed the role of process factors, for example, group processes and facilitator skills, and future research should address their impact on the effectiveness of these programmes for teenage parents.
Acknowledgements
We thank the Cochrane Developmental, Psychosocial and Learning Problems Group for supporting the update of this review, and the following colleagues who provided further information about studies that we assessed for eligibility during this update of the review: Dr O Westney, Dr U Ziegenhain, Dr B Donovan, Dr C Norlin. We also thank Ms Verena Roloff, PhD Student, MRC Cambridge, Cambridge, UK for her advice on adjusting for the effects of cluster randomised trials. Ms Roloff provided advice, the explanatory text used in the review and sample calculations.
Contributions of authors
JB: edited the review, took overall responsibility for selection of the included and excluded studies, and updated the Background and Discussion sections.
NS: reviewed the draft and scope of the review with the contact author of the review. Searched for potential included studies from searches run by the Cochrane DPLP Group, identified included studies, checked old excluded studies and excluded newly found studies which did not fit the inclusion criteria. Carried out data extraction and entry. Completed the tables of characteristics of studies, extracted data, competed risk of bias tables (RoB), extracted data for use in analysis, constructed outcomes tables, checked the existing included studies data, set up the analyses in the updated review, entered data into analysis table, wrote up methods and results section, inserted analysis results into text, entered and checked references, attended progress meetings, was responsible for working collaboratively with other authors to meet publication deadlines.
CB: worked with all review authors to ensure that the review met publication deadlines, contributed to the methods section, analyses, recorded outcomes for drafts of the additional tables, and excluded studies table, set up the analyses in the updated review, and provided general review and publication support.
NH: assisted in identifying potential included studies, extracted data, and provided advice on analyses.
HJ: constructed the RoB tables, extracted RoB data from new included studies, and checked RoB tables with NS.
EC: contributed to the update of Background and Discussion sections and to the selection of studies, discussed the Methods, gave advice about the set up of the analyses, and took overall responsibility for ensuring data in the review are correct.
Declarations of interest
Jane Barlow - None known Nadja Smailagic - None known Cathy Bennett - I am employed by Systematic Research Ltd. and I received a consultancy fee for my contributions to this review Nick Huband - None known Hannah Jones - None known Esther Coren - None known
Differences between protocol and review
We defined the inclusion criteria to state more clearly we included manualised, short-term (i.e. less than 12 week) parenting programmes, which are delivered on a one-to-one basis in the home. This reflects the fact that home visiting programmes are qualitatively different interventions (for example, broad based support which is provided on a frequent basis over an extended period of time) to parenting programmes which are delivered in the home (for example, brief, structured programmes with a specific focus on parenting). This is not a departure from protocol but we have clarified it because in the protocol and previously published versions of the review we implied but did not state clearly the conditions under which parenting programmes are delivered.
The upper age limit of 20 years was also clarified in terms of its consistency with the WHO definition of adolescent parents, thereby enabling the inclusion of international studies.
The inclusion criteria originally stated that the intervention should be “offered ante- or post-natally to pregnant or parenting teenagers, to teenage mothers or teenage fathers”. The wording was changed to state “offered ante- and post-natally or just post-natally to teenage mothers and/or teenage fathers”, to make it clear that ante-natal parenting programmes would be excluded because they may have pregnancy care components rather than being focused on parenting outcomes (such as improvement of parenting attitudes, practices, skills or knowledge).
Previously published versions of the review did not specify that studies aimed at parents of disabled infants or infants with long-term health problems or pre-term infants were excluded, although such studies appear in the excluded studies list (for example,
We also specified the primary outcomes more clearly, and the outcome ‘knowledge of parent child development’ was changed to ‘knowledge about parenting skills’, and parent and child interactions were also defined as a primary outcome. We also added combined parent-child interaction as an outcome category.
In the first published version of the review, the reporting of outcomes or mode of reporting (validated scales) was an inclusion criterion. In this version of the review we did not exclude any study solely on the basis of the outcomes reported or the absence of standardised measures (we provide all reasons for the exclusion in the Excluded studies table).
We added the methods for analysing cluster randomised trials in this updated version of the review.
Published notes
Change in author line.
Characteristics of studies
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Wiemann 1990
Risk of bias table
Footnotes
Aracena 2009
Barlow 2006
Footnotes
Footnotes
Footnotes
Footnotes
| Outcome or Subgroup | Studies | Participants | Statistical Method | Effect Estimate |
|---|---|---|---|---|
| 1.1 |
1 | Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 1.1.1 Post-intervention | 1 | Mean Difference (IV, Fixed, 95% CI) | No totals |
| Outcome or Subgroup | Studies | Participants | Statistical Method | Effect Estimate |
|---|---|---|---|---|
| 2.1 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 2.1.1 Follow up | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 2.2 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 2.2.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 2.3 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 2.3.1 Post intervention |
|
Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 2.4 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 2.4.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% |
No totals |
| Outcome or Subgroup | Studies | Participants | Statistical Method | Effect Estimate |
|---|---|---|---|---|
| 3.1 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.1.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.2 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.2.1 Follow up | 1 | Std. Mean Difference (IV, Fixed, 95% |
No totals | |
| 3.3 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.3.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.3.2 Follow up | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.4 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.4.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.4.2 Follow up | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.5 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.5.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.5.2 Follow up | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.6 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.6.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.7 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.7.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.8 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.8.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.9 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.9.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.10 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.10.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.11 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.11.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.12 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.12.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.13 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.13.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.14 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.14.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.15 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.15.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.16 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.16.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.17 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.17.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.18 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.18.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.19 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.19.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.20 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.20.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.21 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.21.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.22 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.22.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.23 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.23.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.24 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.24.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.25 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 3.25.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals |
| Outcome or Subgroup | Studies | Participants | Statistical Method | Effect Estimate |
|---|---|---|---|---|
| 4.1 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 4.1.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 4.2 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 4.2.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 4.2.2 Follow up | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 4.3 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 4.3.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 4.3.2 Follow up | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 4.4 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 4.4.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 4.4.2 Follow up | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 4.5 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 4.5.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 4.5.2 Follow up | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals |
| Outcome or Subgroup | Studies | Participants | Statistical Method | Effect Estimate |
|---|---|---|---|---|
| 5.1 |
|
Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 5.1.1 Follow up when child was 1 year old |
|
Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 5.1.2 Follow up when child was 2 years old |
|
Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 5.2 |
|
Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 5.2.1 Follow up when child was 1 year old |
|
Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 5.2.2 Follow up when child was 2 years old |
|
Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 5.3 |
|
Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 5.3.1 Follow up when child was 2 years old |
|
Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 5.4 |
|
Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 5.4.1 Follow up |
|
Std. Mean Difference (IV, Fixed, 95% CI) | No totals |
| Outcome or Subgroup | Studies | Participants | Statistical Method | Effect Estimate |
|---|---|---|---|---|
| 6.1 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 6.1.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 6.1.2 Follow up | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 6.2 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 6.2.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 6.2.2 Follow up | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 6.3 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 6.3.1 Follow up | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals |
| Outcome or Subgroup | Studies | Participants | Statistical Method | Effect Estimate |
|---|---|---|---|---|
| 7.1 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 7.1.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 7.1.2 Follow up | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 7.2 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 7.2.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 7.2.2 Follow up | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 7.3 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 7.3.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 7.3.2 Follow up | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 7.4 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 7.4.1 Post intervention | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 7.4.2 Follow up | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 7.5 |
1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 7.5.1 Post interventionNew Subgroup | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals | |
| 7.5.2 Follow up | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | No totals |
| Outcome or Subgroup | Studies | Participants | Statistical Method | Effect Estimate |
|---|---|---|---|---|
| 8.1 |
2 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 8.1.1 Post intervention | 2 | 70 | Std. Mean Difference (IV, Random, 95% CI) | 0 17 [-0 96 1 30] |
| 8.2 |
2 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 8.2.1 Post intervention | 2 | 69 | Std. Mean Difference (IV, Random, 95% CI) | 0 02 [-1.46 1.50] |
| 8.3 |
|
Std. Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 8.3.1 Post-intervention |
|
|
Std. Mean Difference (IV, Fixed, 95% CI) | 0.26 [-0.22, 0.73] |
| 8.4 |
2 | Std. Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 8.4.1 Post intervention | 2 | 70 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.09 [-0.38, 0.56] |
| Outcome or Subgroup | Studies | Participants | Statistical Method | Effect Estimate |
|---|---|---|---|---|
| 9.1 |
2 | Std. Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 9.1.1 Post intervention | 2 | 46 | Std. Mean Difference (IV, Fixed, 95% CI) | -0.91 [-1.52,-0.30] |
| 9.1.2 Follow up (fixed effect model) | 2 | 47 | Std. Mean Difference (IV, Fixed, 95% CI) | -1.07 [-1.80,-0.34] |
| 9.2 |
2 | 47 | Std. Mean Difference (IV, Random 95% CI) | -6.11 [-16.99, 4.77] |
| Outcome or Subgroup | Studies | Participants | Statistical Method | Effect Estimate |
|---|---|---|---|---|
| 10.1 |
2 | Std. Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 10.1.1 Follow up | 2 | 47 | Std. Mean Difference (IV, Fixed, 95% CI) | -0.65 [-1.25,-0.06] |
| Outcome or Subgroup | Studies | Participants | Statistical Method | Effect Estimate |
|---|---|---|---|---|
| 11.1 |
2 | Std. Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 11.1.1 Post intervention | 2 | 46 | Std. Mean Difference (IV, Fixed, 95% CI) | -0.71 [-1.31,-0.11] |
| 11.1.2 Follow up | 2 | 47 | Std. Mean Difference (IV, Fixed, 95% CI) | -0.90 [-1.51,-0.30] |