
Abstract
This Campbell systematic review examines whether kinship care is more effective than foster care in ensuring the safety, permanency and wellbeing of children removed from their home for maltreatment. The review summarizes findings from 102 studies involving 666,615 children. 71 of these studies were included in meta-analyses.
Kinship care is a viable option for the children that need to be removed from the home for maltreatment. However, policy issues remain to balance the cost-effectiveness of kinship care with a possible need for increased levels of caseworker involvement and service delivery. A considerable number of the included studies showed weaknesses in their methodologies and designs. There is a need to conduct more high quality quantitative studies of the effects of kinship care based on robust longitudinal designs and psychometrically sound instruments
Abstract
BACKGROUND
Every year a large number of children around the world are removed from their homes because they are maltreated. Child welfare agencies are responsible for placing these children in out-of-home settings that will facilitate their safety, permanency, and well-being. However, children in out-of-home placements typically display more educational, behavioural, and psychological problems than do their peers, although it is unclear whether this results from the placement itself, the maltreatment that precipitated it, or inadequacies in the child welfare system.
OBJECTIVES
To evaluate the effect of kinship care placement compared to foster care placement on the safety, permanency, and well-being of children removed from the home for maltreatment.
SEARCH METHODS
We searched the following databases for this updated review on 14 March 2011: the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, PsycINFO, CINAHL, Sociological Abstracts, Social Science Citation Index, ERIC, Conference Proceedings Citation Index-Social Science and Humanities, ASSIA, and Dissertation Express. We handsearched relevant social work journals and reference lists of published literature reviews, and contacted authors.
SELECTION CRITERIA
Controlled experimental and quasi-experimental studies, in which children removed from the home for maltreatment and subsequently placed in kinship foster care were compared with children placed in non-kinship foster care for child welfare outcomes in the domains of well-being, permanency, or safety.
DATA COLLECTION AND ANALYSIS
Two review authors independently read the titles and abstracts identified in the searches, and selected appropriate studies. Two review authors assessed the eligibility of each study for the evidence base and then evaluated the methodological quality of the included studies. Lastly, we extracted outcome data and entered them into Review Manager 5 software (RevMan) for meta-analysis with the results presented in written and graphical forms.
RESULTS
One-hundred-and-two quasi-experimental studies, with 666,615 children are included in this review. The 'Risk of bias' analysis indicates that the evidence base contains studies with unclear risk for selection bias, performance bias, detection bias, reporting bias, and attrition bias, with the highest risk associated with selection bias and the lowest associated with reporting bias. The outcome data suggest that children in kinship foster care experience fewer behavioural problems (standardised mean difference effect size -0.33, 95% confidence interval (CI) -0.49 to -0.17), fewer mental health disorders (odds ratio (OR) 0.51, 95% CI 0.42 to 0.62), better well-being (OR 0.50, 95% CI 0.38 to 0.64), and less placement disruption (OR 0.52, 95% CI 0.40 to 0.69) than do children in non-kinship foster care. For permanency, there was no difference on reunification rates, although children in non-kinship foster care were more likely to be adopted (OR 2.52, 95% CI 1.42 to 4.49), while children in kinship foster care were more likely to be in guardianship (OR 0.26, 95% CI 0.17 to 0.40). Lastly, children in non-kinship foster care were more likely to utilise mental health services (OR 1.79, 95% CI 1.35 to 2.37).
AUTHORS' CONCLUSIONS
This review supports the practice of treating kinship care as a viable out-of-home placement option for children removed from the home for maltreatment. However, this conclusion is tempered by the pronounced methodological and design weaknesses of the included studies.
Linked article:
Linked article:
Plain language summary
Child abuse and neglect are common problems across the world that result in negative consequences for children, families, and communities. Children who have been abused or neglected are often removed from the home and placed in residential care or with other families, including foster families. Foster care was traditionally provided by people that social workers recruited from the community specifically to provide care for children whose parents could not look after them. Typically they were not related to the children placed with them, and did not know them before the placement was arranged. In recent years many societies have introduced policies that favour placing children who cannot live at home with other members of their family or with friends of the family. This is known as ‘kinship care’ or ‘families and friends care’. We do not know what type of out-of-home care (placement) is best for children.
This review was designed to help find out if research studies could tell us which kind of placement is best. We found 102 studies with 666,615 children that met the methodological standards we considered acceptable. Wherever possible we combined the data from studies looking at the same outcome for children, in order to be more confident about what the research was telling us. Current best evidence suggests that children in kinship foster care may do better than children in traditional foster care in terms of their behavioural development, mental health functioning, and placement stability. Children in traditional foster care placements may do better with regard to achieving adoption and accessing services they may need. There were no negative effects experienced by children who were placed in kinship care. The major limitation of this systematic review is that the quality of research on kinship care is weakened by the poor methods of the included studies. Implications for practice and future research are discussed.
1 Background
1.1 DESCRIPTION OF THE CONDITION
Every year a large number of children around the world are removed from their homes because they are abused, neglected, or otherwise maltreated. For example, there were 408,425 children in foster care in the United States as of September 2010 (USDHHS 2011a), 64,400 looked-after children in England as of March 2010 (DFE 2010), 35,895 children in out-of-home care in Australia as of 2010 (AIHW 2012), 15,892 looked-after children in Scotland as of July 2010 (Scottish Government 2011), 8408 children in out-of-home therapeutic placement in Israel as of 2010 (CBS 2011), 5419 looked-after children in Wales as of March 2011 (NAW 2011), and 7270 looked-after children in state custody in Norway as of 2011 (Statistics Norway 2011). Except for the United States which has experienced a 20% decrease in the number of children in foster care from 2005, the other countries all experienced an increase in the number of children placed in foster care. Specifically, England had a 5% increase from 2005, Israel had an 8% increase, Wales had a 16% increase, Norway had a 21% increase, Scotland had a 23% increase, and Australia had a 50% increase from 2005. The main reasons for the removal of children in the United States are neglect, physical abuse, sexual abuse, psychological maltreatment, abandonment, threats of harm, and drug addiction (USDHHS 2011b). Abuse and neglect are the most prevalent causes of children being removed from the home in other countries as well (e.g., Wales) (NAW 2011).
Internationally, child welfare systems are accountable for the safety, permanency, and well-being of children in their care. For children removed from the home, child welfare professionals are responsible for placing them in out-of-home settings that will facilitate these outcomes. Specifically, the primary placement options are traditional foster care, kinship care, institutional care, and group homes (AIHW 2012; USDHHS 2011a). Children in out-of-home placements typically display more educational, behavioural, physical, and psychological problems than do their peers (Gleeson 1999), although it is unclear whether this results from the placement itself, the maltreatment that precipitated it, or inadequacies in the child welfare system. In addition to experiencing poor adult outcomes, these children are at risk for drifting in out-of-home care until, in some cases, they ‘graduate’ from the system because of age (Zuravin 1999).
1.2 DESCRIPTION OF THE INTERVENTION
1.2.1 Kinship Care
Kinship care is broadly defined as, “the full-time nurturing and protection of children who must be separated from their parents, by relatives, members of their tribes or clans, godparents, stepparents, or other adults who have a kinship bond with a child” (CWLA 1994, p. 2). This is contrasted with traditional foster care or non-kinship foster care, which is the placement of children removed from the home with unrelated foster parents. Kinship care is known by many other names around the world, including family and friends care in the United Kingdom, kith and kin care in Australia, and kinship foster care in the United States. For this review, kinship care will refer to kinship foster care placements, while foster care will refer to non-kinship foster care placements.
There are several variations of kinship care, including formal, informal, and private placements. Formal kinship care is a legal arrangement in which a child welfare agency has custody of a child (Ayala-Quillen 1998). Informal kinship care is when a child welfare agency assists in the placement of a child but does not seek custody (Geen 2000). Private kinship care is a voluntary arrangement between the birth parents and family members without the involvement of a child welfare agency (Dubowitz 1994a).
The most commonly perceived benefits are that kinship care “enables children to live with persons whom they know and trust, reduces the trauma children may experience when they are placed with persons who are initially unknown to them, and reinforces children's sense of identity and self esteem which flows from their family history and culture” (Wilson 1996, p. 387). The primary aims of kinship placements are family preservation, in which the permanency goal is reunification with birth parents, and substitute care, in which kinship care is considered to be a long-term arrangement when restoration is not possible or the permanency goal is adoption or guardianship by kin caregivers (Scannapieco 1999). Kinship care is also considered to be the least restrictive (Scannapieco 1999) and safest setting (Gleeson 1999) on the continuum of out-of-home placements.
1.2.2 Intervention context
Although an ancient practice in many cultures, formal kinship care is a newer placement paradigm in countries like the United States and Australia, due to its recent adoption by the child welfare field as the placement of choice, when appropriate, in the continuum of out-of-home care services for children (Ainsworth 1998; Geen 2000; Scannapieco 1999). For example, the Personal Responsibility and Work Opportunity Reconciliation Act of 1996 explicitly required U.S. states to give preference to family members when placing a child outside of the home (Leos-Urbel 2002). The Adoption and Safe Families Act of 1997 continued this federal commitment towards promoting and supporting kinship care (Ayala-Quillen 1998). In Australia, the Aboriginal Child Placement Principle has resulted in the increased use of kinship placements, although this differs by state or territory (Paxman 2006). In addition, the New South Wales Children and Young Persons (Care and Protection) Act 1998 encourages the ‘least intrusive’ principle, which is interpreted by caseworkers as placements with kin (Spence 2004). In some European countries, there has also been a shift in policy regarding kinship placements. Specifically, the Children Act 1989 (United Kingdom), the Children Act 1995 (Scotland), and the Children Order 1995 (Northern Ireland) are generally supportive of kinship care (Broad 2005a), as are regulations from 2003 in Norway (MCESI 2003). However, there is no legislation in Israel concerning kinship care, and a lack of consensus about how to define and serve the population of children at risk for maltreatment (Schmid 2007).
For the countries included in this review (i.e., Australia, Ireland, Israel, Netherlands, Norway, Spain, Sweden, United Kingdom, and U.S.), there are essential differences in child welfare policy and practice for placing children in out-of-home care. Outside of the U.S., long-term foster or kinship care is the preferred placement, which implies that parents have right of access to their child provided it is not considered damaging, and also a right to express their opinion on important issues like education and religion. In Australia, Israel, Netherlands, Norway, and Sweden, foster care placement is not time-limited and can be extended until the child emancipates from care (e.g., Strijker 2003). As the preferred option is long-term stable placements, there are foster children in Norway and Sweden who remain in foster homes throughout their entire childhood (e.g., Sallnas 2004). The concept of breakdown (premature termination of placement), therefore, is a more relevant measure in the evaluation of foster care than is reunification or adoption (Sallnas 2004).
During the past 25 years in many countries, there has been a rapid increase in the number of children removed from home and placed with relatives (Cuddeback 2004). The main reasons for the growth of this placement option include an influx of abused and neglected children into out-of-home care (Berrick 1998), concern about poor outcomes for children leaving care (Broad 2005b), a persistent shortage in foster care homes (Berrick 1998), and a shift in policy toward treating kin as appropriate caregivers with all of the legal rights and responsibilities of foster parents (Leos-Urbel 2002). In New South Wales, Australia, the most important factor accounting for historically high numbers of children in foster care is the low use of residential care (Tarren-Sweeney 2006a). This trend toward lower use of residential care also exists in the United Kingdom (Berridge 1998). Although the use of residential care has increased for older children in Israel and Sweden (Mosek 2001; Sallnas 2004), this practice runs counter to official childcare policies in Sweden (Sallnas 2000).
Similar to other child welfare interventions, kinship care is faced with its fair share of controversial issues. The major controversy centres on the unequal financial support (Brooks 2002) and service provision received by kinship caregivers compared with traditional foster parents (Dubowitz 1994a). The licensing and certification of kinship caregivers is also a source of much disagreement and dissatisfaction (Gibbs 2000). Relatedly, the appropriate level of oversight of kinship caregivers by child welfare agencies is another area of discord (Cohen 1999). One of the key debates is over the appropriate level of involvement for biological parents prior to and after the removal of their children (Ayala-Quillen 1998).
In a comprehensive review of the American literature, Cuddeback 2004 confirmed much of the conventional wisdom about kinship care while identifying many of the weaknesses of quantitative research on the topic. Cuddeback found that kinship caregivers are more likely to be older, single, less educated, unemployed, and poor than are foster parents and non-custodial grandparents. Furthermore, Cuddeback reported that kin caregivers report less daily physical activity, more health problems, higher levels of depression, and less marital satisfaction. Cuddeback also concluded that kinship care families receive less training, services, and financial support than do foster care families. In addition, Cuddeback reported that birth parents rarely receive family preservation services, which means that children in kinship care are less likely than children in foster care to be reunified. Lastly, Cuddeback found inconclusive evidence that children in kinship care have greater problems related to overall functioning than do children in foster care.
1.3 WHY IT IS IMPORTANT TO DO THIS REVIEW
In 2004, Geen argued that, “despite the centrality of kinship foster care in child welfare, our understanding of how best to utilize and support kin caregivers, and the impact of kinship foster care on child development, is limited” (
Ethical standards preclude the random assignment of children to kinship or foster care, as these placements typically are based on the appropriateness and availability of kinship caregivers or foster parents (Barth 2008a). However, recent studies have used propensity score matching as a means of statistically simulating random assignment to placement conditions (Barth 2008b).
Even the better-designed studies need to be brought together and appropriately synthesised to provide child welfare professionals with an accessible summary of research on which to make evidence-based decisions (
In 2005, we identified a need to undertake a systematic review of the available evidence from those quasi-experimental study designs best able to provide ‘good enough’ evidence of the effectiveness of kinship care. That review was published in January 2009. Unfortunately, the best available evidence on kinship care was seriously lacking in many ways, especially in regard to controlling for baseline differences in non-randomised studies. In keeping with Cochrane Collaboration Policy we have updated this review, which now includes studies published between March 2007 and March 2011.
2 Objectives
To evaluate the effect of kinship care placement compared to foster care placement on the safety, permanency, and well-being of children removed from the home for maltreatment.
3 Methods
3.1 CRITERIA FOR CONSIDERING STUDIES FOR THIS REVIEW
3.1.1 Types of studies
Controlled experimental and quasi-experimental studies, in which children placed in kinship care are compared cross-sectionally or longitudinally with children placed in foster care. The types of eligible quasi-experimental designs include studies that employ matching, covariates, or ex post facto comparisons of children in kinship care and foster care. Studies that compare kinship care to more restrictive out-of-home settings (e.g., residential treatment centres) were not considered for this review. Relative to children who are placed in kinship or foster care, children placed in more restrictive settings tend to differ in important ways. These differences complicate inferences about the effects of placement and as such, the review focuses on kinship and foster care placements only.
3.1.2 Types of participants
Children and youth under the age of 18 who were removed from the home for abuse, neglect, or other maltreatment, and subsequently placed in kinship care.
3.1.3 Types of interventions
Formal kinship care placements, irrespective of whether the kin caregivers were licensed (paid) or unlicensed (unpaid). Thus, studies that exclusively examine informal or private kinship care arrangements were not considered. Studies were considered if participants experienced other placement types in conjunction with the kinship care intervention. For example, the treatment group may include children for whom kinship care was their first, last, or only placement in out-of-home care. However, these children must have spent the majority (i.e., more than 50%) of their total time in out-of-home care in kinship care.
3.1.4 Types of outcome measures
Eligible studies must analyse child welfare outcomes in the well-being, permanency, or safety domains. Although caregiver and birth parent outcomes are very relevant, they were not considered in this review because child outcomes are what drive the policy and practice of kinship care. However, these outcomes may mediate or moderate the effect of kinship care on child welfare outcomes and should be explored in future research on the topic.
Primary outcomes for the review are behavioural development, mental health, placement stability, and permanency. Secondary outcomes include educational attainment, family relations, service utilisation, and re-abuse. The following list of outcome domains is meant to be exhaustive, although the examples in each domain are illustrative of the outcomes to be considered in this review.
3.1.4.1 Behavioural development
Behaviour problems, adaptive behaviours, delinquency.
Measured by case records, caregiver reports, teacher reports, self reports, and standardised instruments.
3.1.4.2 Mental health
Psychiatric illnesses, psychopathological conditions, well-being. Measured by case records, caregiver reports, self reports, and standardised instruments.
3.1.4.3 Placement stability
Number of placements, re-entry, length of stay.
Measured by child welfare administrative databases.
3.1.4.4 Permanency
Reunification, adoption, guardianship.
Measured by child welfare administrative databases.
3.1.4.5 Educational attainment
Graduation, grades, test scores, attendance, academic success.
Measured by school and case records, caregiver reports, self reports, and standardised instruments.
3.1.4.6 Family relations
Problem-solving, tolerance, commitment, conflicts, emotional availability, home environment.
Measured by caregiver reports, self reports, and standardised instruments.
3.1.4.7 Service utilisation
Mental health services, foster support groups, family therapy, developmental services, physician services.
Measured by medical records, caregiver reports, self reports, and child welfare administrative databases.
3.1.4.8 Re-abuse
Recurrence of abuse, institutional abuse.
Measured by child welfare administrative databases.
3.2 SEARCH METHODS FOR IDENTIFICATION OF STUDIES
Preliminary searches indicated that a narrowing of the search strategy using a methodological filter resulted in the exclusion of potentially relevant studies so we ran the searches without a study methods filter. The original search strategies (Appendix 1) were revised for this update by adding appropriate controlled vocabulary terms for foster care, where they were available. We also included additional free text phrases (for example ‘custodial grandparent’) to increase the sensitivity of the updated search strategies (Appendix 2). We ran the updated searches from the inception of each database and imported the records into Procite. We compared these with records from the previous searches and discarded any duplicates. New records identified by the updated searches were imported records into Reference Manager 11/12 for screening. Searches were not limited by language, date, or geographic area.
3.2.1 Electronic searches
We ran updated searches of the following databases in March 2011: Cochrane Central Register of Controlled Trials (CENTRAL), 2011 Issue 1, part of The Cochrane Library; Ovid MEDLINE,1948 to March Week 1 2011; PsycINFO, 1887 to 14 March 2011; CINAHL, 1937 to current; Sociological Abstracts, 1952 to current; Social Sciences Citation Index (SSCI), 1970 to 12 March 2011; Conference Proceedings Citation Index -Social Science and Humanities (CPCI-SSH), 1990 to 12 March 2011; ERIC, 1966 to current; Applied Social Sciences Index and Abstracts (ASSIA), 1987 to current; Dissertation Abstracts (via Dissertation Express), last searched 14 March 2011.
We could not update the searches of the following three databases because they have either ceased to function or are no longer available to us: Campbell Collaboration's Social, Psychological, Educational, and Criminological Trials Register (C2-SPECTR), last searched 9 March 2007; Social Work Abstracts, last searched February 2007; Family and Society Studies Worldwide, last searched February 2007.
3.2.2 Searching other resources
For the original review, we handsearched volumes of Child Abuse & Neglect, Children and Youth Services Review, Child Welfare, Research on Social Work Practice, and Families in Society from 2006 and 2007. We contacted several authors of studies included in this review for knowledge of other studies not yet identified. Lastly, we screened the reference lists of published literature reviews for relevant studies.
3.3 DATA COLLECTION AND ANALYSIS
The procedures for collecting and analysing the data for this review are detailed below.
3.3.1 Selection of studies
Two review authors independently read the titles and abstracts of identified articles and reports to select those that described an empirical study of kinship care. A study was obtained if either review author believed it was appropriate. Once the studies were retrieved, two review authors used a ‘keywording’ rubric to categorise each study by the type of design, participants, intervention, and outcome measure(s). Two review authors then determined if each study was eligible for selection based on the aforementioned criteria for considering studies for this review. When we could not reach a consensus regarding selection decisions, we resolved it through discussion with a third review author.
3.3.2 Data extraction and management
We entered citations for all selected studies into Reference Manager 11/12, which is an interactive literature management software package. We then uploaded the citations for included studies into The Cochrane Collaboration's Review Manager 5 software (RevMan). We extracted outcome data from studies and entered them into RevMan, where they were meta-analysed for this review. We present the statistical results in both narrative form, and in figures and tables. Specifically, RevMan-generated forest plots are used to display effect size estimates and confidence intervals from the meta-analyses. We use funnel plots generated from RevMan to examine the presence of publication bias in the evidence base. In addition, we present data from the quality assessment process in a table created in RevMan.
3.3.3 Assessment of risk of bias in included studies
Existing scales for measuring the quality of controlled trials have not been properly developed, are not well-validated, and are known to give differing (even opposing) ratings of trial quality in systematic reviews (Moher 1999). At present, evidence indicates that “scales should generally not be used to identify trials of apparent low quality or high quality in a given systematic review. Rather, the relevant methodological aspects should be identified a priori and assessed individually” (Juni 2001, p. 45). Thus, studies were assessed in regard to the following research quality dimensions: selection bias, performance bias, detection bias, reporting bias, and attrition bias (Higgins 2011).
Two review authors independently extracted data from each study before coming to consensus on the assessment of risk of bias for each of the following domains for each study. The methodological criteria were operationalised as follows:
Selection bias: Was group assignment determined randomly or might it have been related to outcomes or the interventions received? The studies rated at high risk did not attempt to equate the kinship care and foster care groups through matching or controlling for covariates AND did not provide evidence on the comparability of the groups on setting (e.g., urbanicity), placement characteristics (e.g., age at placement, removal reason), or child demographics (e.g., gender, ethnicity). The studies rated at unclear risk either attempted to equate the groups OR provided evidence on the comparability of the groups. The studies rated at low risk attempted to equate the groups AND provided evidence on the comparability of the groups. For example, these studies provided evidence that the groups were comparable at baseline in regard to placement history, visits to biological parents, and caregiver characteristics (e.g., family composition, age, education).
Performance bias: Could the services provided have been influenced by something other than the interventions being compared? In the studies that were rated at high risk, the kinship care and foster care groups experienced different exposure to the intervention (e.g., length of stay) AND received different services during placement (e.g., caseworker contact). In the studies that were rated at unclear risk, the groups either experienced different exposure OR received different services. In the studies that were rated at low risk, the groups did not experience different exposure AND did not receive different services.
Detection bias: Were outcomes influenced by anything other than the constructs of interest, including biased assessment or the influence of exposure on detection? In the studies rated at high risk, the kinship care and foster care groups were not defined in the same way (e.g., caregiver licensure, caregiver characteristics) AND there was evidence of biased assessment resulting from the type of placement (e.g., caregiver reports only). In the studies rated at unclear risk, the groups were not defined in the same way OR there was evidence of biased assessment. In the studies rated at low risk, the groups were defined in the same way AND there was no evidence of biased assessment.
Reporting bias: Were the outcomes, measures, and analyses selected a priori and reported completely? Were participants biased in their recall or response? In the studies rated at high risk, the instrumentation used to measure the outcomes was not specified completely (e.g., data collection procedures) AND reliability with or without validity information was not reported for the instrumentation. In the studies rated at unclear risk, the instrumentation used to measure the outcomes was specified completely OR reliability with or without validity information was reported for the instrumentation. In the studies rated at low risk, the instrumentation was completely specified AND reliability with or without validity information was reported.
Attrition bias: Could deviations from protocol, including missing data and dropout, have influenced the results? In the studies rated at high risk, not all participants were accounted for in the reporting of results (e.g., low response rate, missing outcome data) AND attrition could have influenced the results (e.g., significant difference between participants and non-participants). In the studies rated at unclear risk, not all participants were accounted for OR attrition could have influenced the results. In the studies rated at low risk, all participants were accounted for AND attrition could not have influenced the results.
3.3.4 Measures of treatment effect
3.3.4.1 Continuous data
We computed a standardised mean difference (SMD) effect size for the continuous outcome variables. For this review, we created a corrected Hedges' g by dividing the difference between group means by the pooled and weighted standard deviation of the groups. Specifically, Hedges' g corrects for a bias (overestimation) that occurs when the uncorrected standardised mean difference effect size is used on small samples. The combined effect size for each outcome was computed as a weighted mean of the effect size for each study, with the weight being the inverse of the square of the standard error. Thus, a study was given greater weight for a larger sample size and more precise measurement, both of which reduce standard error. We computed a 95% confidence interval for each combined effect size to test for statistical significance; if the confidence interval did not include zero, we rejected the null hypothesis that there is no difference between the group means.
3.3.4.2 Dichotomous data
We computed Mantel-Haenszel odds ratios (ORs) for the dichotomous outcome variables. Based on the assumption of proportional odds, ORs can be compared between variables with different distributions, including very rare and more frequent occurrences. Specifically, the odds of an event (e.g., reunification) were calculated for each group by dividing the number of events (i.e., re-entry, reunification) by the number of non-events (i.e., re-entry, no reunification). We then calculated an OR by dividing the odds of the kinship care group by the odds of the foster care group. In addition, we calculated and reported 95% confidence intervals for the dichotomous effect size estimates.
3.3.5 Unit of analysis issues
The unit of analysis for this review was children. There were no unit of analysis issues identified for the included studies.
3.3.6 Dealing with missing data
Although studies with incomplete outcome data (e.g., missing means, standard deviations, sample sizes) were included in the review, they were excluded from the meta-analyses unless the review authors could calculate an effect size from the available information. When outcome data were missing from an article or report, we made reasonable attempts to retrieve these data from the original researchers. Attrition overall and by group were accounted for in the quality assessment and sensitivity analyses.
3.3.7 Assessment of heterogeneity
We assessed the consistency of results using the I2 statistic (Higgins 2002; Higgins 2003). If there was evidence of heterogeneity (P value from test of heterogeneity < 0.1 coupled with an I2 value of 25% or greater), we also considered sources of methodological and practice diversity according to prespecified subgroup and sensitivity analyses (see below). The values of the Q heterogeneity statistic and the between-studies variance component Tau2 were also reported.
3.3.8 Assessment of reporting biases
With the additional studies identified in the updated review, we assessed publication bias through the use of funnel plots. This method of assessing reporting bias was only used for outcomes that included meta-analytic findings from at least 10 studies (Higgins 2011).
3.3.9 Data synthesis
As heterogeneity is to be expected with similar interventions provided under different circumstances and by different providers, we used a random-effects model for data synthesis. If a study reported multiple effect sizes (e.g., grades, behaviour problems), the results were included in the meta-analysis for each outcome. If a study reported effect sizes for multiple samples (e.g., male, female), we aggregated the results for the main effects meta-analyses before splitting them for the subgroup meta-analyses. We conducted data synthesis for outcomes in which at least three studies contributed effect sizes to the meta-analysis.
3.3.10 Subgroup analysis and investigation of heterogeneity
We considered subgroup analyses to explore different effects of the intervention (if any) by gender, ethnicity, and age at placement.
3.3.11 Sensitivity analysis
We planned sensitivity analyses to explore the impact of the risk of bias dimensions on the specific outcomes of the review. Specifically, we considered the following planned comparisons: Studies that used matching or covariates versus studies that did not control for confounders; Studies with outcomes measured by caregiver or teacher reports versus studies with outcomes measured by self-reports; Studies at low risk of attrition bias versus studies at high risk of attrition bias; Studies at low risk of selection bias versus studies at high risk of selection bias.
We conducted the sensitivity analyses using simple unweighted ANOVA models.
4 Results
4.1 DESCRIPTION OF STUDIES
The included studies are described in terms of the location, participants, interventions, and outcome measures.
4.1.1 Results of the search
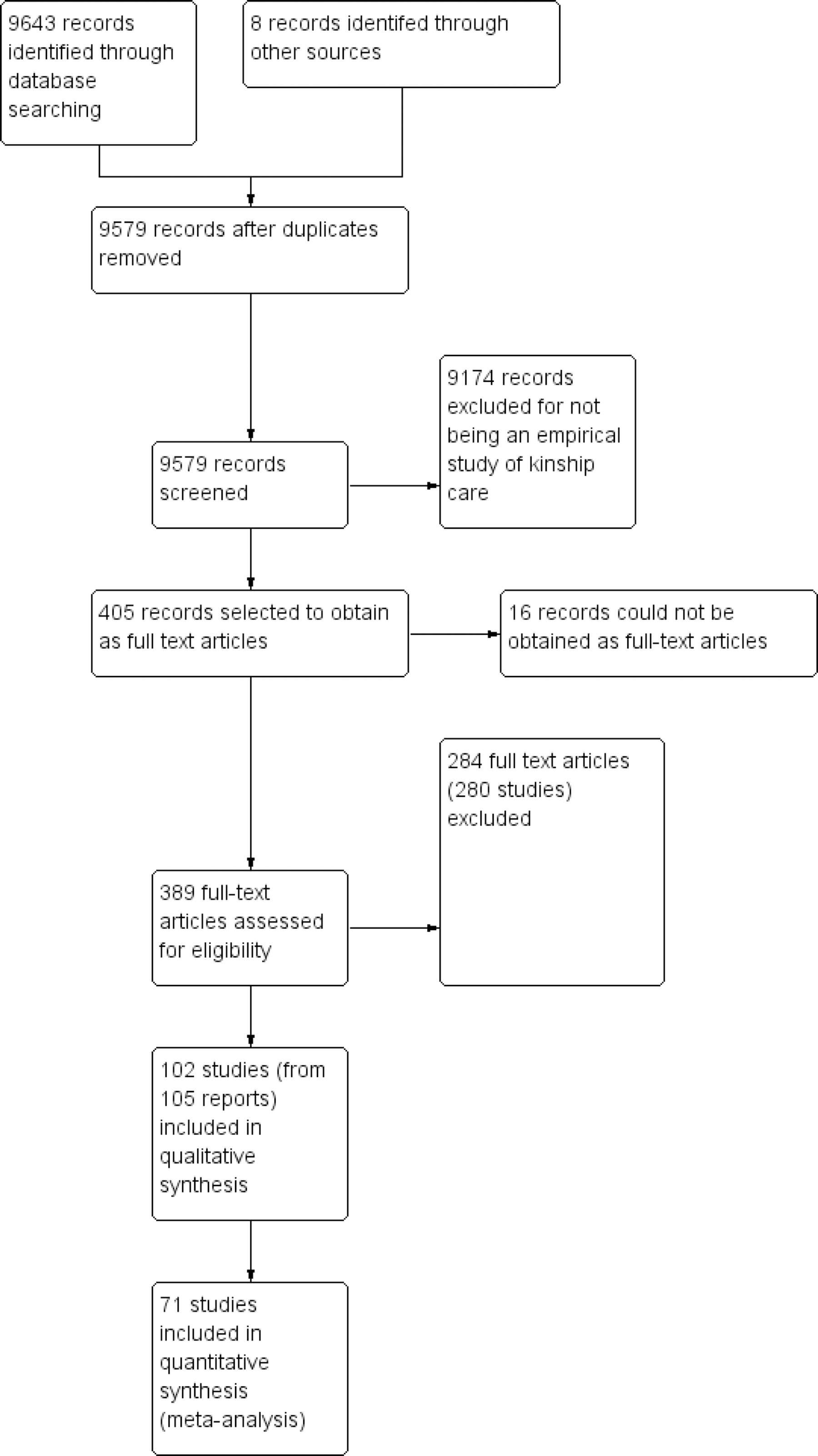
As displayed in the study flow diagram (Figure 1), a comprehensive electronic search of the kinship care literature base up until March 2011 yielded 9643 records with eight additional records identified through other sources. After 72 duplicates were removed, there were 9579 records with 4797 records from the search during the original review and 4782 records from the search during the updated review (of which 2728 were records found using the modified search strategy for the period covered by the original review).
Study flow diagram (complete review)
4.1.2 Included studies
9174 studies, which were not empirical studies of kinship care, were eliminated by screening titles and abstracts . We made every effort to retrieve the full text of the remaining 405 records (271 records from the original search and 134 records from the updated search). Of these 405 records, 16 were intractably unavailable as fulltext articles and were transferred to the excluded studies. We assessed the remaining 389 full-text articles for eligibility and identified studies which had multiple reports: 102 studies (comprised of 105 papers) met the inclusion criteria and 280 studies (comprised of 284 papers) were excluded. Thus, a total of 102 studies were identified and included in the qualitative synthesis (62 from the original review and 40 from the updated review, of which six were published pre-2007), while 71 studies were included in the meta-analysis (46 from the original review and 25 from the updated review, of which none was published pre-2007).
4.1.2.1 Location of Studies
All but 13 of the 102 studies were conducted in the U.S. The 13 international studies were Del Valle 2009 and Palacios 2009 conducted in Spain, Holtan 2005 conducted in Norway, Lernihan 2006 conducted in Ireland, Lutman 2009 conducted in the United Kingdom, Mosek 2001 conducted in Israel, Sallnas 2004 conducted in Sweden, Strijker 2003 and Strijker 2008 conducted in the Netherlands, and Tarren-Sweeney 2006a, Tarren-Sweeney 2006b, Tarren-Sweeney 2008a, and Tarren-Sweeney 2008b conducted in Australia.
4.1.2.2 Participants
As displayed in the Participant Baseline Characteristics Table (
For age at entry into the specific placement, there was an overall unweighted mean age at placement of 7 years 10 months, based on 14 studies. Eleven studies reported a mean age at placement by placement type. For the kinship care group, the unweighted mean age at placement was 4 years 10 months. For the foster care group, the unweighted mean age at placement was also 4 years 10 months.
For gender, there were overall unweighted frequencies of 52% female and 48% male children, based on 57 studies. Furthermore, 33 studies reported gender frequencies by placement type. For the kinship care group, the unweighted frequencies were 50% female and 50% male. For the foster care group, the unweighted frequencies were 52% female and 48% male.
For ethnicity, there was an overall unweighted frequency of 45% African-American children, based on 53 studies. There was an overall unweighted frequency of 22% Hispanic children based on 45 studies. Furthermore, 25 studies reported the frequency of African-American children by placement type. For the kinship care group, the unweighted frequency was 51% African-American. For the foster care group, the unweighted frequency was 44% African-American. In addition, 20 studies reported the frequency of Hispanic children by placement type. For the kinship care group, the unweighted frequency was 24% Hispanic. For the foster care group, the unweighted frequency was 26% Hispanic.
For removal reason, there was an overall unweighted frequency of 60% of children removed for neglect, based on 31 studies. Furthermore, 15 studies reported the frequency of children removed for neglect by placement type. For the kinship care group, the unweighted frequency was 67% of children removed for neglect. For the foster care group, the unweighted frequency was 63% of children removed for neglect.
For urbanicity, there was an overall unweighted frequency of 80% of children from urban settings, based on 17 studies. In addition, there was an overall unweighted frequency of 13% of children from rural settings based on four studies. However, no studies reported the urbanicity of children by placement type.
4.1.2.3 Interventions
As displayed in
For caregiver licensure, nine studies reported information on whether kinship caregivers were licensed or unlicensed. Specifically, six studies included licensed kinship placements, two studies included unlicensed kinship placements, and one study included both licensed and unlicensed kinship placements.
For the timing of placement, 40 studies reported information on whether children were in their first, last, or only kinship or foster placement. Specifically, the kinship or foster placement was the first in 29 of the studies, the last in eight of the studies, the only placement in one study, and either the first or last placement depending on the outcome being measured in two studies.
For length of stay, there was an unweighted mean length of placement of 36.0 months for the kinship care group and 34.2 months for the foster care group, based on 16 studies. In addition, there was an unweighted mean length of stay in out-of-home care of 48.7 months for the kinship care group and 45.5 months for the foster care group based on 14 studies.
For the timing of data collection, 62 studies used a cross-sectional data collection approach while 40 studies used a longitudinal data collection approach with a follow-up ranging from one year to 10 years.
4.1.2.4 Outcome measures
There were eight outcome categories and 29 specific outcomes considered in this review (including the same outcome measured both dichotomously and continuously). The following narrative contains the definitions and instrumentation used to measure the outcome variables in which bivariate data were extracted for the meta-analyses. The Outcomes Measures Table (
4.1.2.5 Behavioural development
The two behavioural development outcomes were behaviour problems and adaptive behaviours. Behaviour problems were defined dichotomously as the presence or absence of internalising (e.g., withdrawn, passive) and externalising (e.g., aggressive, delinquent) problem behaviours and continuously as the level of these behaviours. The continuous outcome was measured by the total problems scale of the Child Behavior Checklist (CBCL) in 12 studies (Davis 2005; Ford 2007; Holtan 2005; Jones-Karena 1998; Lawler 2008; Linares 2010; Orgel 2007; Rudenberg 1991; Strijker 2003; Tarren-Sweeney 2006a; Timmer 2004; Villagrana 2008), the Behaviour Problems Index (Brooks 1998), and caregiver reports in two studies (Metzger 1997; Surbeck 2000). The dichotomous outcome was measured by the CBCL in two studies (Ringeisen 2009; Sakai 2011), the Behavioural Assessment Scoring System for Children (McCarthy 2007), an administrative database (Ryan 2010a), and case records in two studies (Iglehart 1994; Landsverk 1996). Adaptive behaviours were defined continuously as the level of competence or positive behaviours and were measured by the total competence scale of the CBCL in three studies (Holtan 2005; Tarren-Sweeney 2006a; Villagrana 2008), the adaptive composite score on the Vineland Adaptive Behavior Scales (VABS) in three studies (Belanger 2002; Jones-Karena 1998; Villagrana 2008), and caregiver reports (Surbeck 2000).
4.1.2.6 Mental health
The two mental health outcomes were psychiatric disorders and well-being. Psychiatric disorders were defined dichotomously by the presence or absence of mental illness and continuously by scores on a measure of psychopathology. The dichotomous outcome was measured by the Composite International Diagnostic Interview (Keller 2010), the Child Depression Inventory and Trauma Symptoms Checklist for children (Sakai 2011), paid claims data (Bilaver 1999), the DSM-IV (McMillen 2005), and case records in two studies (Harris 2003; Iglehart 1994). The continuous outcome was measured by the Devereaux Scales of Mental Disorders (Belanger 2002) and the Columbia Impairment Scale and the Self-Perception Profile of Adolescents (Mennen 2010). Well-being was defined dichotomously by the presence or absence of positive emotional health and continuously by the level of well-being or self worth. The dichotomous outcome was measured by the Foster Care Questionnaire (Dunn 2010), child self reports (Wilson 1999), the R.C. Monitoring Protocol (Harris 2003), and caseworker reports (Tompkins 2003). The continuous outcome was measured by the Personal Attribute Inventory for Children (Metzger 1997) and a measure from the National Longitudinal Study of Adolescent Health (Farruggia 2009).
4.1.2.7 Placement stability
The four placement stability outcomes were number of placements, length of stay, placement disruption, and re-entry as measured by secondary data from administrative databases for all studies except for case records in two studies (Strijker 2008; Valicenti-McDermott 2008), and caseworker reports in two studies (Del Valle 2009; Sakai 2011). Number of placements was measured both continuously by the number of out-of-home placements and dichotomously by experiencing either two or fewer or three or more placement settings. The dichotomous outcome was used in six studies (Courtney 1997b; Harris 2003; Metzger 1997; Pabustan-Claar 2007a; Ryan 2010a; Zimmerman 1998). The continuous outcome was used in six studies (Belanger 2002; Davis 2005; Ryan 2010a; Sakai 2011; Strijker 2008; Winokur 2008). Length of stay in placement was measured continuously in six studies (Berrick 1994; Brooks 1998; Cole 2006; Davis 2005; Surbeck 2000; Valicenti-McDermott 2008). Length of stay in out-of-home care was measured continuously in nine studies (Belanger 2002; Clyman 1998; Jenkins 2002; Ryan 2010a; Sivright 2004; Strijker 2008; Tompkins 2003; Valicenti-McDermott 2008; Winokur 2008). It should be noted that longer lengths of stay in placement or in out-of-home care are considered negative outcomes in the U.S., as reunification within 12 months is the primary permanency goal for children placed in short-term kinship or foster care. Placement disruption was measured dichotomously by whether the kin or foster placement ended without permanency in five studies (Del Valle 2009; Koh 2008b; Rubin 2008; Sallnas 2004; Testa 2001). Re-entry was measured dichotomously by whether there was a re-entry to out-of-home care after achieving permanency in two studies (Frame 2000; Winokur 2008).
4.1.2.8 Permanency
The four permanency outcomes were reunification, adoption, guardianship, and still in placement. All four outcomes were measured dichotomously by secondary data from administrative databases in 15 studies (Akin 2011; Barth 1994; Berrick 1999; Johnson 2005; Koh 2008b; McIntosh 2002; Pabustan-Claar 2007a; Sivright 2004; Smith 2002; Smith 2003; Testa 1999; Testa 2001; Wells 1999; Winokur 2008; Zimmerman 1998) and case records or caseworker reports in four studies (Del Valle 2009; Lutman 2009; Sakai 2011; Valicenti-McDermott 2008). Reunification was defined as a return home to biological or birth parents after placement in out-of-home care. Adoption was defined as a termination of parental rights with legal custody transferred to adoptive parents (in most cases non-relatives). Guardianship was defined as an allocation of parents' rights with legal custody to relative caregivers (in most cases relatives). ‘Still in placement’ was defined as remaining in either kinship or foster care at the time data were collected for the study.
4.1.2.9 Educational attainment
The three educational attainment outcomes were repeating a grade, graduation, and grade level, and all were measured dichotomously. It should be noted that these outcomes are all U.S. measures of educational attainment. Repeating a grade was defined by whether a child had been retained in one or more grades as measured by caregiver or self reports in five studies (Berrick 1994; Brooks 1998; Ford 2007; Metzger 1997; Sripathy 2004) and case records (Valicenti-McDermott 2008). Graduation was defined by whether a child completed high school and was measured by case records (Christopher 1998). Grade level was defined by whether a child's academic performance was below their actual grade level and was measured by child self reports (Iglehart 1995) and case records (Iglehart 1994).
4.1.3 Family relations
The three family relations outcomes were attachment, conflict, and home environment. Attachment was defined as perceived level of relatedness or attachment between child and caregiver and was measured continuously by child self reports (Chapman 2004), the Attachment Q-Sort Version 3 Assessment (Chew 1998), caregiver reports (Strijker 2003), the Assessment of Interpersonal Relations (Davis 2005), and the Child Well-Being Scales (Surbeck 2000). Attachment was measured dichotomously by the Ainsworth Strange Situation Procedure (Cole 2006), case records (Jenkins 2002), the Offer Self-Image Questionnaire (Mosek 2001), and the Relationship Story Completion Test (Orgel 2007). Conflict was defined continuously as the level of family functioning as measured by the Index of Family Relations (Berrick 1997). Home environment was defined as the milieu within the foster and kinship care households (e.g., emotional climate, paternal involvement, and family participation) and was measured by the Elementary HOME Inventory (Ford 2007).
4.1.3.1 Service utilisation
The three service utilisation outcomes were mental health services, physician services, and developmental services defined dichotomously as whether a child actually received services (not just referral). Mental health service utilisation was measured by paid claims data (Bilaver 1999), caseworker reports in two studies (Metzger 1997; Tompkins 2003), case records in three studies (Jenkins 2002; Scannapieco 1997; Sivright 2004), caregiver reports in three studies (Berrick 1994; Sakai 2011; Sripathy 2004), The Young Kids Early Services Assessment (TYKES) (Clyman 1998), and the Child and Adolescent Services Assessment in three studies (Farmer 2010; Ringeisen 2009; Villagrana 2008). Physician service utilisation was measured by paid claims data (Bilaver 1999), caseworker reports (Tompkins 2003), case records in two studies (Scannapieco 1997; Valicenti-McDermott 2008), caregiver reports in two studies (Sakai 2011; Schneiderman 2010), and the TYKES (Clyman 1998). Developmental services were measured by paid claims data (Bilaver 1999), the TYKES (Clyman 1998), and the Child and Adolescent Services Assessment (Ringeisen 2009).
4.1.3.2 Re-abuse
The two re-abuse outcomes were recurrence of abuse and institutional abuse, as measured dichotomously by secondary data from administrative databases. Recurrence of abuse was defined as whether a new substantiated incident of intrafamilial abuse or neglect (by birth or biological parent(s) not kin caregiver(s) or foster parent(s)) occurred after a previous substantiated incident and was reported in one study (Fuller 2005). Institutional abuse was defined as whether a substantiated incident of abuse or neglect occurred in an out-of-home placement setting (by kin caregiver(s) or foster parent(s) not birth or biological parent(s)) and was reported in three studies (Benedict 1996a; Winokur 2008; Zuravin 1993).
4.1.4 Excluded studies
As displayed in the
4.2 RISK OF BIAS IN INCLUDED STUDIES
The included studies were assessed for risk of selection bias, performance bias, detection bias, reporting bias, and attrition bias. Specifically, each study was rated either at low risk, unclear risk, or high risk based on two sub-questions for each of these areas. The ‘Risk of bias’ tables included with the
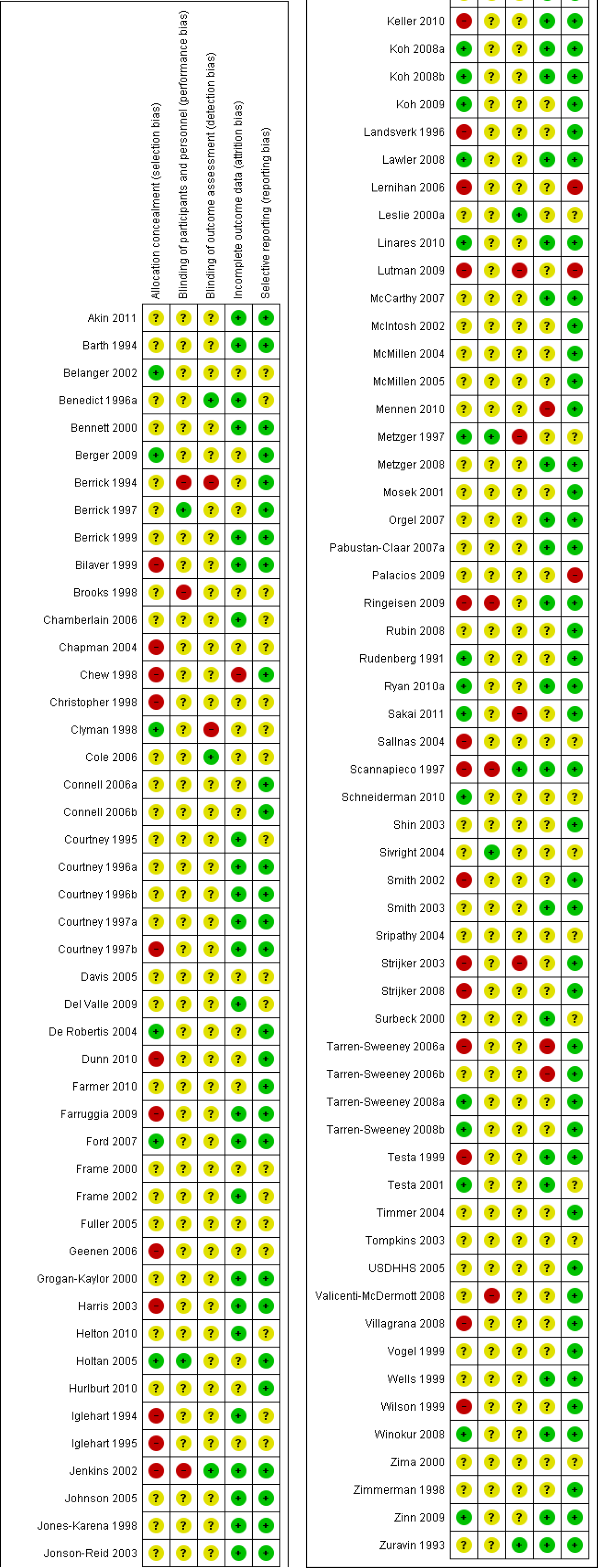
Risk of bias summary: Review authors' judgements about each risk of bias item for each included study.
4.2.1 Allocation (selection bias)
For selection bias, 21 studies (Belanger 2002; Berger 2009; Clyman 1998; De Robertis 2004; Ford 2007; Holtan 2005; Koh 2008a; Koh 2008b; Koh 2009; Lawler 2008; Linares 2010; Metzger 1997; Rudenberg 1991; Ryan 2010a; Sakai 2011; Schneiderman 2010; Tarren-Sweeney 2008a; Tarren-Sweeney 2008b; Winokur 2008; Testa 2001; Zinn 2009) were rated at low risk, 55 studies were rated at unclear risk, and 26 studies were rated at high risk. The primary reasons that studies were assessed to have unclear or high risk for selection bias were the lack of equating procedures and uncertainty or non-reporting for placement and demographic data.
4.2.2 Blinding (performance bias and detection bias)
For performance bias, four studies (Berrick 1997; Holtan 2005; Metzger 1997; Sivright 2004) were rated at low risk, 92 were rated at unclear risk, and six were rated at high risk. The primary reasons that studies were assessed to have unclear or high risk for performance bias were uncertainty regarding both the length of stay and receipt of services during placement.
For detection bias, six studies (Benedict 1996a; Cole 2006; Jenkins 2002; Leslie 2000a; Scannapieco 1997; Zuravin 1993) were rated at low risk, 90 were rated at unclear risk, and six were rated at high risk. The primary reasons that studies were assessed to have unclear or high risk for detection bias were uncertainty in how the groups were defined and the use of only caregiver or self reports to measure the outcome. Although biased assessment is not necessarily due to the type of placement, it may differentially impact the detection of a placement's effect on child welfare outcomes.
4.2.3 Incomplete outcome data (attrition bias)
For attrition bias, 44 studies were rated at low risk, 54 studies were rated at unclear risk, and four studies were rated at high risk. The primary reason that studies were assessed to have unclear or high risk for attrition bias was the loss of participants due to missing outcome data.
4.2.4 Selective reporting (reporting bias)
For reporting bias, 71 studies were rated at low risk, 28 studies were rated at unclear risk, and three studies were rated at high risk. The primary reason that studies were assessed to have unclear or high risk for report bias was the lack of reliability and/or validity information.
4.2.5 Other potential sources of bias
There were no other potential sources of bias assessed.
4.3 EFFECTS OF INTERVENTIONS
4.3.1 Meta-analyses
There were sufficient data for meta-analysis for 21 of the 29 outcomes in the review. As a result, we generated at least one meta-analysis for each outcome category. We report the results for these 21 outcomes as the statistical significance of the effect, the direction and magnitude of the effect size, the 95% confidence interval around the effect size estimate, and the evidence of heterogeneity for the individual effect sizes. The effect sizes were drawn exclusively from the studies reporting bivariate data, and thus do not reflect adjustment by covariates (although bivariate data from studies that used matching designs were included in the effect size analyses). It should be noted that all standardised mean difference (SMD) effect sizes that are negative indicate better outcomes for the kinship care group, while all odds ratio (OR) effect sizes that are less than 1.0 also indicate better outcomes for the kinship care group.
4.3.1.1 Behavioural Development
There was a statistically significant overall effect size for the 15 studies (Brooks 1998; Davis 2005; Ford 2007; Holtan 2005; Jones-Karena 1998; Lawler 2008; Linares 2010; Metzger 1997; Orgel 2007; Rudenberg 1991; Strijker 2003; Surbeck 2000; Tarren-Sweeney 2006a; Timmer 2004; Villagrana 2008) that reported sufficient bivariate continuous data to generate effect size estimates for behaviour problems. Specifically, the overall effect size estimate was g = -0.33, 95% confidence interval (CI) -0.49 to -0.17 (see
There was a statistically significant overall effect size for the six studies (Iglehart 1994; Landsverk 1996; McCarthy 2007; Ringeisen 2009; Ryan 2010a; Sakai 2011) that reported sufficient bivariate dichotomous data to generate effect size estimates for behaviour problems. Specifically, the overall effect size estimate was reported OR 0.62, 95% CI 0.41 to 0.93 (see
There was a statistically significant overall effect size for the six studies (Belanger 2002; Holtan 2005; Jones-Karena 1998; Surbeck 2000; Tarren-Sweeney 2006a; Villagrana 2008) that reported sufficient bivariate data to generate effect size estimates for adaptive behaviours. Specifically, the overall effect size estimate was g = -0.42, 95% CI -0.61 to -0.22 (see
4.3.1.2 Mental health
There was a statistically significant overall effect size for the six studies (Bilaver 1999; Harris 2003; Iglehart 1994; Keller 2010; McMillen 2005; Sakai 2011) that reported sufficient bivariate dichotomous data to generate effect size estimates for psychiatric disorders. Specifically, the overall effect size estimate was OR 0.51, 95% CI 0.42 to 0.62 (see
There was a statistically significant overall effect size for the four studies (Dunn 2010; Harris 2003; Tompkins 2003; Wilson 1999) that reported sufficient bivariate dichotomous data to generate effect size estimates for well-being. Specifically, the overall effect size estimate was reported OR 0.50, 95% CI 0.38 to 0.64 (see
4.3.1.3 Placement stability
There was a statistically significant overall effect size for the six studies (Courtney 1997b; Harris 2003; Metzger 1997; Pabustan-Claar 2007a; Ryan 2010a; Zimmerman 1998) that reported sufficient bivariate dichotomous data to generate effect size estimates for placement settings. Specifically, the overall effect size estimate was OR 0.39, 95% CI 0.33 to 0.45 (see
There was a statistically significant overall effect size for the six studies (Belanger 2002; Davis 2005; Ryan 2010a; Sakai 2011; Strijker 2008; Winokur 2008) that reported sufficient bivariate continuous data to generate effect size estimates for number of placements. Specifically, the overall effect size estimate was g = -0.38, 95% CI -0.58 to -0.17 (see
There were six studies (Berrick 1994; Brooks 1998; Cole 2006; Davis 2005; Surbeck 2000; Valicenti-McDermott 2008), with a total sample size of N = 634 for the kinship care group and N = 883 for the foster care group, that reported sufficient bivariate data to generate effect size estimates for length of placement. The overall effect size estimate was g = 0.90, 95% CI -0.66 to 2.46 (see
There were nine studies (Belanger 2002; Clyman 1998; Jenkins 2002; Ryan 2010a; Sivright 2004; Strijker 2008; Tompkins 2003; Valicenti-McDermott 2008; Winokur 2008), with a total sample size of N = 129503 for the kinship care group and N = 201218 for the foster care group, that reported sufficient bivariate data to generate effect size estimates for length of stay in out-of-home care. The overall effect size estimate was g = 0.02 with a confidence interval of -0.04 to 0.09 (see
There was a statistically significant overall effect size for the five studies (Del Valle 2009; Koh 2008b; Rubin 2008; Sallnas 2004; Testa 2001) that reported sufficient bivariate data to generate effect size estimates for placement disruption. Specifically, the overall effect size estimate was OR 0.52, 95% CI 0.40 to 0.69 (see
4.3.1.4 Permanency
There were 13 studies (Akin 2011; Berrick 1999; Del Valle 2009; Koh 2008b; McIntosh 2002; Pabustan-Claar 2007a; Smith 2002; Testa 1999; Testa 2001; Valicenti-McDermott 2008; Wells 1999; Winokur 2008; Zimmerman 1998), with a total sample size of N = 22907 for the kinship care group and N = 44496 for the foster care group, that reported sufficient bivariate data to generate effect size estimates for reunification. The overall effect size estimate was OR 1.09, 95% CI 0.85 to 1.40 (see
There was a statistically significant overall effect size for the 12 studies (Akin 2011; Barth 1994; Berrick 1999; Del Valle 2009; Koh 2008b; Pabustan-Claar 2007a; Smith 2002; Testa 1999; Testa 2001; Valicenti-McDermott 2008; Winokur 2008; Zimmerman 1998) that reported sufficient bivariate data to generate effect size estimates for adoption. Specifically, the overall effect size estimate was OR 2.52, 95% CI 1.42 to 4.49 (see
There was a statistically significant overall effect size for the eight studies (Akin 2011; Berrick 1999; Koh 2008b; Pabustan-Claar 2007a; Testa 1999; Testa 2001; Winokur 2008; Zimmerman 1998) that reported sufficient bivariate data to generate effect size estimates for guardianship. Specifically, the overall effect size estimate was OR 0.26, 95% CI 0.17 to 0.40 (see
There was a statistically significant overall effect size for the 11 studies (Barth 1994; Berrick 1999; Johnson 2005; Lutman 2009; Sakai 2011; Sivright 2004; Smith 2002; Smith 2003; Testa 2001; Winokur 2008; Zimmerman 1998) that reported sufficient bivariate data to generate effect size estimates for the still-in-placement outcome. Specifically, the overall effect size estimate was OR 1.18, 95% CI 0.77 to 1.80 (see
4.3.1.5 Educational attainment
There were six studies (Berrick 1994; Brooks 1998; Ford 2007; Metzger 1997; Sripathy 2004; Valicenti-McDermott 2008), with a total sample size of N = 546 for the kinship care group and N = 673 for the foster care group, that reported sufficient bivariate data to generate effect size estimates for the ‘repeated a grade’ outcome. The overall effect size estimate was OR 0.73, 95% CI 0.50 to 1.07 (see
4.3.1.6 Family relations
There were five studies (Chapman 2004; Chew 1998; Davis 2005; Strijker 2003; Surbeck 2000), with a total sample size of N = 217 for the kinship care group and N = 282 for the foster care group, that reported sufficient bivariate continuous data to generate effect size estimates for the attachment outcome. The overall effect size estimate was g = -0.01, 95% CI -0.30 to 0.28 (see
There were four studies (Cole 2006; Jenkins 2002; Mosek 2001; Orgel 2007), with a total sample size of N = 163 for the kinship care group and N = 212 for the foster care group, that reported sufficient bivariate dichotomous data to generate effect size estimates for the attachment outcome. The overall effect size estimate was OR 1.21, 95% CI 0.56 to 2.59 (see
4.3.1.7 Service utilisation
There was a statistically significant overall effect size for the 13 studies (Berrick 1994; Bilaver 1999; Clyman 1998; Farmer 2010; Jenkins 2002; Metzger 1997; Ringeisen 2009; Sakai 2011; Scannapieco 1997; Sivright 2004; Sripathy 2004; Tompkins 2003; Villagrana 2008) that reported sufficient bivariate data to generate effect size estimates for mental health service utilisation. Specifically, the overall effect size estimate was OR 1.79, 95% CI 1.35 to 2.37 (see
There were three studies (Bilaver 1999; Clyman 1998; Ringeisen 2009), with a total sample size of N = 14314 for the kinship care group and N = 33744 for the foster care group, that reported sufficient bivariate data to generate effect size estimates for developmental service utilisation. The overall effect size estimate was OR 0.94, 95% CI 0.38 to 2.32 (see
There were seven studies (Bilaver 1999; Clyman 1998; Sakai 2011; Scannapieco 1997; Schneiderman 2010; Tompkins 2003; Valicenti-McDermott 2008), with a total sample size of N = 74354 for the kinship care group and N = 139651 for the foster care group, that reported sufficient bivariate data to generate effect size estimates for physician service utilisation. The overall effect size estimate was OR 1.37, 95% CI 0.48 to 3.93 (see
4.3.1.8 Re-abuse
There was a statistically significant overall effect size for the three studies (Benedict 1996a; Winokur 2008; Zuravin 1993) that reported sufficient bivariate data to generate effect size estimates for institutional abuse. Specifically, the overall effect size estimate was OR 0.27, 95% CI 0.10 to 0.71 (see
4.3.2 Multivariate analyses
As studies that reported multivariate data controlled for covariates, such as age at placement, gender, ethnicity, socioeconomic status, geographic region, behaviour and health problems, placement reason and history, and caregiver variables, they potentially provide a stronger level of evidence regarding the effect of kinship care on child welfare outcomes. Thus, results from the weaker quasi-experimental designs comprising the meta-analytical data could also be considered stronger evidence if corroborated by the multivariate results which are summarised in the Outcomes for Studies with Multivariate Analysis Table (
For behavioural development, Bennett 2000, Holtan 2005, Rubin 2008, and Sakai 2011 found that children in kinship care had significantly lower likelihood of behaviour problems than did children in foster care. Furthermore, three studies reporting multivariate adaptive behaviours data (Belanger 2002; Bennett 2000; Brooks 1998) found that children in kinship care had significantly greater adaptive behaviours than did children in foster care. However, De Robertis 2004, Linares 2010, Mennen 2010, Surbeck 2000, Tarren-Sweeney 2008b, and Zima 2000 did not find a significant difference between the groups on behaviour problems, while Berger 2009 found that time spent in foster care homes was associated with decreased externalising behaviour problems. Again, Zima 2000 did not find a significant difference between the groups on adaptive behaviours.
For mental health, Belanger 2002 and Metzger 1997 found that children in kinship care had significantly better reported well-being and fewer psychiatric disorders than did children in foster care. However, Ford 2007, Mennen 2010, and Tarren-Sweeney 2008a found that type of placement was not a significant predictor of well-being, while McMillen 2005 and Tarren-Sweeney 2006a found no significant difference between the groups on psychiatric disorders. Sakai 2011 found that children in kinship care had a lower risk of depression but a higher risk of post-traumatic stress disorder (PTSD).
For service utilisation, Clyman 1998, Farmer 2010, Leslie 2000a, McMillen 2004, and Sakai 2011 found that children in foster care were significantly more likely to utilise mental health services than were children in kinship care. As for physician service utilisation, Clyman 1998 found no significant difference between the groups, while Schneiderman 2010 found that children in kinship care had a greater likelihood of utilising physician service than did children in foster care.
The greatest amount of multivariate data was reported for the permanency outcomes. Similar to the nonsignificant meta-analysis results for reunification, the findings from the 12 studies reporting multivariate data were also inconclusive. Specifically, four studies (Akin 2011, Berrick 1999; Courtney 1996a; Grogan-Kaylor 2000) found that children in kinship care were more likely to reunify, while two studies (Connell 2006a; Courtney 1996b) found that children in foster care were more likely to reunify. Furthermore, Courtney 1997a, Frame 2002, Wells 1999, and Zimmerman 1998 found no significant difference between the groups on reunification, while Koh 2008a reported mixed findings on reunification depending on the state being analysed. As for adoption, Akin 2011, Barth 1994, and Courtney 1996b found that children in foster care were significantly more likely to be adopted than were children in kinship care. However, Courtney 1996a found that children in kinship care were more likely to be adopted, while Connell 2006a found no significant difference between the groups, and Koh 2008a reported mixed findings on adoption depending on the state being analysed. Berrick 1999 and Smith 2003 found that children in foster care were significantly less likely to still be in placement than were children in kinship care, while Frame 2002 and Johnson 2005 found no significant difference between the groups, and Koh 2008a reported mixed findings on this permanency outcome depending on the state being analysed.
For placement stability, Chamberlain 2006, Connell 2006b, Helton 2010, Hurlburt 2010, Koh 2008a, Koh 2009, and Testa 2001 found that children in kinship care were less likely to disrupt from placement than were children in foster care. Perhaps the most compelling evidence from the multivariate analyses was for re-entry, in that seven studies (Berrick 1999; Courtney 1995; Courtney 1997a; Frame 2000; Frame 2002; Jonson-Reid 2003; Wells 1999) reported that children in kinship care were significantly less likely to re-enter care than were children placed in foster care, while only one study (Koh 2008a) reported mixed findings on re-entry depending on the state being analysed. Vogel 1999 found that children in kinship care had significantly longer lengths of stay than did children in foster care, while Koh 2008a reported that children in kinship care were less likely to experience three or more placements within a year.
For the safety outcomes, Benedict 1996a and Zuravin 1993 found that children in kinship care were less likely to experience institutional abuse than were children in foster care. However, the multivariate results were inconclusive for recurrence of abuse, as Jonson-Reid 2003 found that children in kinship care were less likely to experience recurrence of abuse, while Fuller 2005 found that children in kinship care were more likely to experience recurrence of abuse.
For family relations, the USDHHS 2005 study reported that children in kinship care had higher levels of attachment, while Davis 2005 and Lawler 2008 found that type of placement was not a significant predictor of relatedness or emotional availability, respectively. Finally, for educational attainment, Shin 2003 found that children in kinship care had significantly higher reading scores than did children in foster care, while Zinn 2009 found no difference between the groups on educational attainment.
4.3.3 Bivariate analyses
As summarised in the Outcomes for Studies with Bivariate Analysis Table (
For mental health, Mosek 2001 and Tarren-Sweeney 2008a found that children in kinship care had significantly higher well-being than did children in foster care, while Palacios 2009 found that foster parents reported greater well-being in regard to basic needs and educational supervision, and Valicenti-McDermott 2008 found no difference in well-being or psychiatric disorders between the groups. For family relations, Metzger 2008 and USDHHS 2005 found higher levels of attachment for children in kinship care than for children in foster care. For educational attainment, Geenen 2006 found that children in foster care had significantly higher grade point averages and earned credits than did children in kinship care, although there were no differences for attendance, number of grades retained, and test scores.
For placement stability, two studies, Scannapieco 1997 and Zimmerman 1998, found that children in foster care had significantly shorter placement lengths than did children in kinship care, while Metzger 1997 found that children in kinship care had significantly shorter lengths of placement, and Lernihan 2006 found no differences between the groups on length of placement. The bivariate results were similar for length of stay in out-of-home care, as Zimmerman 1998 found that children in foster care had significantly shorter lengths of stay than did children in kinship care, while Sakai 2011 found no difference between the groups on length of stay in out-of-home care. Helton 2010 found that children in kinship care had significantly lower rates of placement disruption, while Strijker 2008 and Tarren-Sweeney 2008a found no difference between the groups on placement disruption. Zimmerman 1998 found no difference between the groups on re-entry rates. Lastly, Zinn 2009 found no differences between the groups on the permanency outcomes of reunification and adoption.
4.3.3.1 Sensitivity analyses
Sensitivity analyses comparing studies with high risk of attrition bias and low risk of attrition bias were planned but were not conducted because only four studies were rated at high risk. Furthermore, attrition rates could not be accurately determined for the quasi-experimental studies included in the review. Specifically, all of these studies were post-test only, so there were often incomplete data on how many children were originally placed in kinship or foster care and no pre-measures to indicate how many children ‘dropped out’ of the study by the time of the post-measures data collection. There were missing data in some of the studies, in that multiple measures had different sample sizes, presumably because data were either not available from case files or not collected. However, the missing data are presumed to be missing at random, so no sensitivity analysis is warranted.
Sensitivity analyses comparing studies with child self reports and parent/teacher/caregiver reports were planned for the review, but were not conducted because of the lack of such comparisons for the included outcomes. For example, there were no studies that measured behavioural development by child self report and only one study each that measured service utilisation and educational attainment by child self report. Furthermore, there were only two studies that measured mental health by child self report. Lastly, three studies used child self reports for family relations, but there were no studies that measured family relations by caregiver reports.
Sensitivity analyses comparing studies that controlled for confounders with those that did not were not possible using statistical techniques because of differences in the type of data reported. Specifically, the studies that controlled for confounders used multivariate analyses rather than matching (except for Koh 2008a; Rudenberg 1991; Testa 2001; Winokur 2008). As such, many of the multivariate data were reported as correlation and beta coefficients or odds and risk ratios. These data could not be used in the meta-analyses to generate multivariate effect sizes to compare with the bivariate data effect sizes. However, we employed vote counting for the multivariate studies to provide some comparison with the results from the bivariate studies.
We conducted sensitivity analyses comparing studies at low, unclear, and high risk for selection bias, as there were 21 studies rated at low risk, 55 studies rated at moderate risk, and 26 studies rated at high risk. Specifically, we conducted sensitivity analyses for selection bias on behaviour problems and mental health service utilisation because these two outcomes had at least three studies in each of the risk groups. For the continuous behaviour problems outcome, we used a simple unweighted ANOVA model with the risk groups as the independent variable and the standard mean difference from each study as the dependent variable. The following are the mean effect sizes and 95% confidence intervals for the low risk group: -0.65 (95% CI -1.56 to 0.24), the unclear risk group: -0.23 (95% CI -0.36 to -0.10); and the high risk group: -0.17 (95% CI -0.66 to 0.33). The result was nonsignificant (F = 1.53, P = 0.257), which indicates that the effect sizes for behaviour problems are similar between the low risk (Ford 2007; Holtan 2005; Lawler 2008; Linares 2010; Metzger 1997; Rudenberg 1991), the unclear risk (Brooks 1998; Davis 2005; Orgel 2007; Surbeck 2000; Timmer 2004), and the high risk (Jones-Karena 1998; Strijker 2003; Tarren-Sweeney 2006a; Villagrana 2008) for selection bias groups. For the mental health service utilisation outcome, we used a simple unweighted ANOVA model with the risk groups as the independent variable and the odds ratios as the dependent variable. Before conducting the ANOVA, the odds ratios were transformed into standard mean differences using a method from Chinn 2000, in which the log transformation of each odds ratio is divided by 1.81. The following are the mean effect sizes and 95% confidence intervals for the low risk group: 0.39 (95% CI -0.84 to 1.62), the unclear risk group: 0.19 (95% CI -0.13 to 0.51); and the high risk group: 0.39 (95% CI 0.19 to 0.60). The result was nonsignificant (F = 0.75, P = 0.496), which indicates that the effect sizes for mental health service utilisation are similar between the low risk (Clyman 1998; Metzger 1997; Sakai 2011), unclear risk (Berrick 1994; Farmer 2010; Sivright 2004; Sripathy 2004; Tompkins 2003), and high risk groups (Bilaver 1999; Jenkins 2002; Ringeisen 2009; Scannapieco 1997; Villagrana 2008) for selection bias.
4.3.3.2 Subgroup analyses
There were insufficient data to examine different effects of the intervention by gender, ethnicity, and age at placement. Specifically, only three studies (Farruggia 2009; Holtan 2005; Ryan 2010a) reported outcome data by gender for each placement type, only Farruggia 2009 and Smith 2002 reported outcome data by ethnicity for each placement type, and no studies reported outcome data by age at placement for each placement type.
5 Discussion
5.1 SUMMARY OF MAIN RESULTS
Based on the preponderance of the available evidence, it appears that children in kinship care experience better outcomes in regard to behaviour problems, adaptive behaviours, psychiatric disorders, well-being, placement stability (placement settings, number of placements, and placement disruption), guardianship, and institutional abuse than do children in foster care. There were no detectable differences between the groups on reunification, length of stay (in placement or out-of-home care), educational attainment, family relations, developmental service utilisation, and physician service utilisation. However, children placed with kin are less likely to achieve adoption and to utilise mental health services, while being more likely to still be in placement than are children in foster care. Although there were some findings of no difference between the groups for certain outcomes, the multivariate results generally support the findings from the meta-analyses while indicating that children in kinship care are less likely to re-enter out-of-home care than are children in foster care. However, these conclusions are tempered by the pronounced methodological and design weaknesses of the included studies and particularly the absence of conclusive evidence on the comparability of groups. It is clear that researchers and practitioners must do better to mitigate the biases that cloud the study of kinship care.
Although this review supports the practice of treating kinship care as a viable out-of-home placement option for children removed from the home for maltreatment, policies mandating kinship placements may not always be in the best interest of children and families. Professional judgement from child welfare practitioners must also be used to assess the individual needs of children and the ability of kin caregivers to attend to these needs.
5.2 OVERALL COMPLETENESS AND APPLICABILITY OF EVIDENCE
With the inclusion of 40 new studies and an overall evidence base of 102 studies, this systematic review represents the most complete synthesis of kinship care research to date. The findings presented here are robust, in that the addition of the 40 studies did not change any of the previous results and in fact consolidated many of them. Although two years have passed since the updated search date of March 2011, it would take an additional 40 studies with dramatically different results to have any impact on the findings. Furthermore, the context in which kinship care is practised (at least in the U.S.) has not changed in the past two years, as kinship care is still the preferred out-of-home placement option. Thus, the decision was made to proceed with the publication of the updated systematic review to maximise the applicability of the evidence for child welfare practitioners and policymakers. All studies produced after March 2011 will be considered for the next update of this systematic review.
Overall, a very secure picture of the outcomes for kinship care has emerged. However, the applicability of the evidence is still worth considering, especially for the key outcomes. For example, the lack of a baseline measurement of initial behavioural functioning makes ambiguous the conclusion that children in foster care have lower levels of current behavioural functioning. Furthermore, caregiver reports may be biased because foster parents have more incentive to report behavioural and mental health issues, whereas relatives are more apt to view the behaviour as acceptable and thus less likely to report it as problematic.
The mixed findings for the permanency outcomes could be interpreted in the context that long-term kinship care arrangements satisfy the definition of permanency in many countries, as kinship caregivers are allocated the parental rights for a child. Thus, an undesirable outcome (e.g., remaining in care) might actually be desirable if the kinship care placement is considered to be safe and stable. Adoption and guardianship are secondary permanency goals, which are considered only after reunification has been ruled out. Furthermore, these permanency outcomes are fundamentally dependent on the public and legal policy of individual countries. For example, adoption is not a viable permanency option in many countries outside of the U.S., including Australia, Israel, Netherlands, and the Nordic nations.
The commonly-held idea that foster parents are more ‘system involved’ may explain the greater propensity for children in foster care to receive mental health services. Furthermore, the training and supervision of foster parents may contribute to the higher identification of mental health problems, and as such contribute to higher levels of service utilisation. The lower licensure rate for kin caregivers may be another factor in the unequal receipt of services for children in kinship care. However, the greater likelihood for children in foster care to utilise mental health services may have less to do with the type of placement and more to do with these children having a greater need for services.
5.3 QUALITY OF THE EVIDENCE
The major limitation encountered in this systematic review is the weak standing of quantitative research on kinship care (Cuddeback 2004). Specifically, the “differences between the children who enter kinship care and those who enter nonkinship care” lead to a lack of confidence regarding the comparability of groups and the subsequent lack of control over contaminating events such as family preservation services (Barth 2008b, p. 218). In general, the included studies also have unclear to high risks of performance, detection, reporting, and attrition bias, which compromise the tenability of the findings from the systematic review. However, the sensitivity analyses indicate that the results for behavioural development and mental health service utilisation are more robust, in that the effect sizes for studies with low, unclear, and high risk of selection bias were comparable.
Another concern regarding the quality of evidence is the potential misalignment between the intervention and child welfare outcomes, in that the fullest representation of the effects of kinship care has yet to be truly measured (Cuddeback 2004). When compared to traditional foster care, in which the relationship between foster parents and the ‘system’ is more standardised, the effect of kinship care may be more difficult to detect. For example, there is seemingly a lack of implementation fidelity within and across countries in regard to kinship care. Furthermore, kinship placements, especially with unlicensed caregivers, are often more private and out of the control of child welfare agencies than are foster placements. The concepts, terminology, and outcomes typically ascribed to out-of-home care may not always be appropriate for kinship placements. As a result of these limitations, it is more appropriate to research kinship care after it has been fully and consistently integrated into the fabric of child welfare policy and practice.
5.4 POTENTIAL BIASES IN THE REVIEW PROCESS
One potential bias in the review process is that the robustness of the meta-analysis results is weakened by challenges confronted during the effect size calculations. Specifically, the heterogeneity statistic was significant for 17 of the 21 outcomes, which indicates that the effect sizes were not always consistent within the same outcome. In addition, bivariate data were not reported in every study, which restricted the meta-analysis of some outcomes to the bare minimum of three studies and eliminated other outcomes from consideration. Another potential bias is that many studies analysed a small sample of children, while others utilised a much larger dataset. However, this was somewhat mitigated by the use of random-effects weighting, which gave more weight to the studies with smaller sample sizes and less weight to the studies with larger sample sizes, than would a fixed-effect analysis.
The presence of publication bias in this review was examined for behavioural problems (continuous), reunification, adoption, still in placement, and mental health service utilisation, as these outcomes had at least 10 studies included in the respective meta-analyses. Overall, a visual inspection of the funnel plots suggests that publication bias is likely not present for these outcomes. Specifically, the funnel plots for behavioural problems, mental health service utilisation, reunification, and still in placement appear symmetrical. The funnel plot for adoption (Figure 3) appears asymmetrical with a gap in the bottom left corner of the graph. However, the three studies represented in the bottom right corner have the smallest sample sizes, the largest effect sizes, and the largest standard errors, which may indicate poor methodological quality rather than publication bias. Furthermore, these three studies are in favour of the control condition, so it does not appear that any studies that may be ‘missing’ are missing because of negative findings.
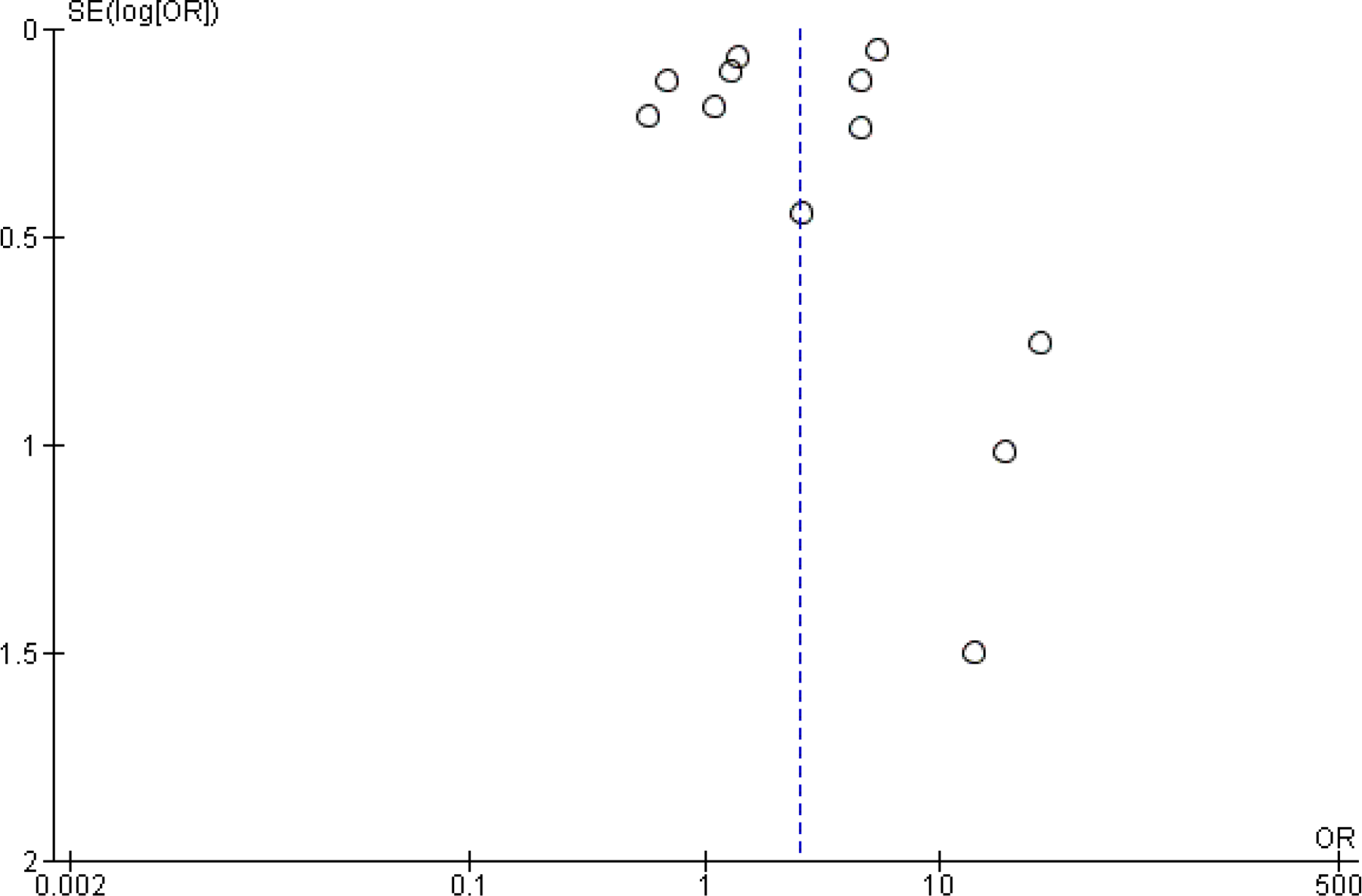
(Analysis 4.2)
5.5 AGREEMENTS AND DISAGREEMENTS WITH OTHER STUDIES OR REVIEWS
The results of this review are in strong agreement with the only previous narrative review of kinship care, conducted by Cuddeback 2004.
6 Authors' conclusions
6.1 IMPLICATIONS FOR PRACTICE
Several implications for social work professionals and policymakers emerged from this review, although they are dependent on how individual countries interpret the results. If the goal of kinship care is to enhance the behavioural development, mental health functioning, well-being, and placement stability of children, then the evidence base is supportive. However, the findings from the review do not support implementing kinship care solely to increase the permanency rates and service utilisation of children in out-of-home care.
The primary implication for practitioners to consider is whether kinship placements would be even more effective with increased levels of caseworker involvement and service delivery (Geen 2000). However, the potential benefits of greater financial and therapeutic support must be weighed against the independence that some kin caregivers demand. Relatedly, the main implications for policymakers is whether licensing standards should be required for kin caregivers (Geen 2000), and whether additional financial resources should be made available to these providers (Hornby 1996).
On the other hand, there may be a cost-effectiveness component to placing children with relatives in light of the comparable permanency outcomes, and lower payments and fewer services offered to kin caregivers. As such, this could play an important role in how child welfare agencies view their current approach to kinship care. That being said, foster care should continue to be an essential out-of-home care option, as children in these placements also experience positive outcomes and appropriate kinship placements are not always available.
6.2 IMPLICATIONS FOR RESEARCH
To address the major limitations of research on kinship care, there is a demand for studies that employ generalisable samples, equivalent groups, and repeated measurements (Berrick 1994a). Cuddeback 2004 advocates longitudinal designs to investigate the outcomes of children over time, the development of psychometrically sound instruments of family and child functioning that allow for more reliable comparisons across groups and studies, and greater emphasis on controlling and understanding selection bias through the use of emerging statistical models (e.g., meta-regression analysis). Furthermore, the duration effect or the relationship between length of stay and child welfare outcomes should be explored in greater depth. For example, survival analysis could be used to investigate the timeliness of achieving reunification and other permanency outcomes for children in out-of-home care. There is also a need to disaggregate the effects of kinship care across important subgroups of target participants, settings, and intervention variations. For example, there are few studies that reliably measure the effect of kinship care on caregiver outcomes (Gibbs 2000).
As for other topics, Testa 1992 calls for research on the financial implications of kin caregivers becoming licensed, while Cuddeback 2004 recommends studies that examine the relationship between certification and the provision of services to kin caregivers. Studies that focus on the educational outcomes of children in kinship care are certainly warranted, as education is essential to effective integration into adult life. In addition, research on informal and voluntary kinship care arrangements should be a top priority for child welfare researchers.
Qualitative research that explores the underlying dynamics of kinship care along with the factors associated with positive outcomes is a natural outgrowth of this systematic review. Specifically, investigating the lived experiences of different types of kin caregivers (e.g., grandparents, other relatives, family friends) would greatly enhance our understanding of this placement option.
As research on this topic is predominantly U.S.-based, studies from other countries are sorely needed, especially as kinship care is increasing in popularity elsewhere in the western world. For example, the different permanency goals should be examined in greater depth to determine which outcome offers greater practical permanency to children removed from the home.
For kinship care to remain a viable option in the social work repertoire, researchers must work more closely with practitioners to design, implement, and disseminate innovative studies of the intervention. For example, new predictor variables and outcome measures should be included in data collection instruments to facilitate richer analyses of the effect of kinship care.
Lastly, the Methods for Future Updates Table (
8 Contributions of authors
Marc Winokur, Amy Holtan, and Deborah Valentine contributed to the writing and revising of the original review. Marc Winokur, Amy Holtan, and Keri Batchelder contributed to the writing and revising of the updated review. The original search strategy was developed with Jo Abbott, Trial Search Co-ordinator for the Cochrane DPLPG. The updated search strategy was developed with Margaret Anderson, Trial Search Co-ordinator for the Cochrane DPLPG. Marc Winokur will be responsible for updating this review as additional evidence accumulates and as funding becomes available.
9 Declarations of interest
Marc Winokur, Amy Holton and Keri Batchelder - the original review was funded by the Applied Research in Child Welfare Project (USA), SFI Campbell (Denmark), and the University of Tromsø, Center for Child and Adolescent Mental Health (Norway), and the updated review was funded by the Applied Research in Child Welfare Project (USA) and UiT The Arctic University of Norway, Regional Centre for Child and Youth Mental Health and Child Welfare (Norway). There are no competing interests that influenced, or may give the appearance of potentially influencing, what we wrote in the submitted work.
10 Differences between protocol and review
There were no substantive differences between the protocol and review. There were some differences between the review and the update. Specifically, sensitivity analyses and reporting bias analyses were conducted with the addition of the 40 new included studies. The methods section was enhanced with additional information on the assessment of risk of bias and the assessment of heterogeneity. The results section was enhanced with additional information on the effects of the interventions, the interpretations of the meta-analytic and odds ratios results, and the sensitivity analyses. The discussion section was enhanced with additional information on the overall completeness and applicability of the evidence and potential biases in the review process. The plain language summary was enhanced with additional information on adverse effects and limitations. Meta-analyses with less than three studies were removed from the review. The risk of bias table was changed to a risk of bias figure. Lastly, studies awaiting classification were moved to excluded studies as being intractably unavailable.
11 Published notes
This review is co-registered within the Campbell Collaboration.
12 Characteristics of studies
12.1 CHARACTERISTICS OF INCLUDED STUDIES
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
Risk of bias table
AFCARS: Adoption and Foster Care Analysis and Reporting System
AFDC: Aid to Families with Dependent Children
CPS: Child Protection Services
DCFS: Department of Children and Family Services
DHHS: Department of Health and Human Services
DOCS: Department of Community Serives
DSS: Department of Social Services
GPA: Grade Point Average
IDCFS: Illinois Department of Children and Family Services
LONGSCAN: Longitudinal Studies of Child Abuse and Neglect
NSCAW: National Survey of Child and Adolescent Well-being
OOH: out-of-home
RCSA: Relative Caregiver Social Assessment
12.2 CHARACTERISTICS OF EXCLUDED STUDIES
Ajduković 2005
Marinković 2004
Marinković 2007
13 Additional tables
13.1 PARTICIPANT BASELINE CHARACTERISTICS
O: Overall
K: Kinship
F: Foster
13.2 INTERVENTION CHARACTERISTICS
OOH: out-of-home
13.3 OUTCOME MEASURES
AFCARS: Adoption and Foster Care Analysis and Reporting System
GPA: Grade point average
OOH: out-of-home
PTSD: Post-traumatic Stress Disorder
13.4 OUTCOMES FOR STUDIES WITH MULTIVARIATE ANALYSIS
AFDC: Aid to Families with Dependent Children
BIA: Behavioural Influences Analysis
CBCL: Child Behaviour Checklist
DSMD: Devereux Scales of Mental Disorder
OOH: Out-of-home
VABS: Vineland Adaptive Behaviour Scales
13.5 OUTCOMES FOR STUDIES WITH BIVARIATE ANALYSIS
CBCL: Child Behaviour Checklist
GPA: Grade point average
HR: hazard ratio
OOH: Out-of-home
M: mean
13.6 METHODS FOR FUTURE UPDATES
16 Data and analyses
Behavioural Development
Mental Health
Placement Stability
Permanency
Educational Attainment
Family Relations
Service Utilisation
Re-abuse
18 Sources of support
SFI Campbell, Denmark
Applied Research in Child Welfare Project, USA
University of Tromsø, Norway
Footnotes
19 Appendices
7 Acknowledgements
Thank you to SFI Campbell (previously the Nordic Campbell Center), Danish National Institute of Social Research and the Applied Research in Child Welfare (ARCH) Project (USA) for funding this review. Thank you to Laura MacDonald, Trine Bak Nyby, Krystyna Kowalski, Jane Dennis, Geraldine Macdonald, and Julia Littell for their timely feedback and generous support during the writing of the protocol, original review, and updated review. Thank you to Margaret Anderson and Jo Abbott, Trial Search Co-ordinators for the Cochrane Developmental, Psychosocial and Learning Problems Group (DPLPG), and Merinda McLure, Applied Human Sciences Librarian at Colorado State University (CSU), for assistance in developing and executing the search strategy for the review. Thank you to Toby Lasserson (Cochrane Airways Group, London, UK), Celia Almeida (Cochrane DPLPG, Bristol, UK), Soyna Curtis, and Professor Jelena Marinkovic and Dr. Jelena Marinkovic both from University of Belgrade, Serbia for translating the foreign language articles for the review. Thank you to Jeff Valentine and the content reviewers along with Brian Cobb and Jeffrey Gliner of CSU for their helpful suggestions. Special thanks to Stephanie Mace of CSU for her assistance in acquiring the studies, extracting data, and conducting quality assessments for the updated review. Thank you to Frank Ainsworth, Marianne Berry, Morten Blekesaune, and Amy Holtan, as this protocol incorporates elements of their jointly registered Cochrane and Campbell Collaboration protocol prepared in 2004 on the same topic.