
Abstract
The objectives of this Campbell systematic review were: To describe the range and diversity of interventions available for addressing the low labour market participation of adults with physical and/or sensory disabilities in developing country contexts. To systematically identify, assess, and synthesise the evidence on the effects of interventions on labour market outcomes for disabled adults in low- and middleincome countries. As part of this, to critically analyse the evidence along the causal chain framework, linking interventions with intermediate outcomes and final impacts, and document the level/strength of evidence on potential pathways of impact using the framework. To assess if effects are moderated by characteristics of the participants, interventions, and/or settings. To provide an explanation for the intervention effects by examining what participants in the included studies reported about why the interventions did, or did not, work for them.
A total of 14 studies met the eligibility criteria. Publication dates of included studies ranged between 1992 and 2012, with six studies published in the four-year period 2010-2013. A key finding of this review is the overall scarcity of robust evidence, as indicated by the relatively few studies that met the inclusion criteria. Although the evidence in general showed positive results, we need to be wary of drawing strong inferences from the findings of this body of literature. Not only is the number of impact evaluations limited, but most used designs in which conclusively attributing causality is not possible.
Our assessment of the evidence does not allow us to develop practical suggestions on what interventions are likely to work, for whom, and when. Clearly, there is an urgent need for investment in high quality impact evaluations of interventions to support people with disabilities in accessing the labour market in low- and middle income settings. To build the evidence base further, it is therefore important that many more of the interventions currently in existence in low- and middle-income countries are rigorously evaluated, and the results are reported and disseminated widely. The methodological inconsistencies and weaknesses of the current evidence base, and specific knowledge gaps, suggest a number of future research priorities.
Executive Summary
BACKGROUND
Disability is a development issue, with widespread poverty, inequality and violation of human rights. Recent estimates suggest that more than one billion people are living with some form of disability. Persons with disabilities are over-represented among the world's poor, and significant labour market disadvantage helps maintain the link between poverty and disability in many country contexts. The costs of disability are particularly acute in low- and middle-income countries (those with gross national income per capita of less than $12,616), where up to 80% of people with disabilities of working age can be unemployed, around twice that for their counterparts in high-income countries. When people with disabilities do work, they generally do so for longer hours and lower incomes, have fewer chances of promotion, are more likely to work in the informal labour market, and are at greater risk of becoming unemployed for longer periods. The barriers faced by people with disabilities globally in accessing and sustaining paid work is a profound social challenge. There is now growing recognition of employment as a key factor in the process of empowerment and inclusion into society, and the role of interventions to improve labour market outcomes for disabled people is receiving increased international attention. It is therefore both vital and timely to increase understanding of the impacts of available programmes, in order to ensure that they are effective in delivering positive outcomes for people with disabilities and provide value for money. Although several reviews have attempted to summarise the existing research in this area, there are a number of substantive and methodological limitations to these reviews. Thus, there is a need to systematically examine the evidence base to provide an overview of the types of interventions being used to improve employment outcomes, to identify those that are effective and ineffective, and to identify areas in which more research needs to be conducted.
OBJECTIVES
To describe the range and diversity of interventions available for addressing the low labour market participation of adults with physical and/or sensory disabilities in developing country contexts. To systematically identify, assess, and synthesise the evidence on the effects of interventions on labour market outcomes for disabled adults in low- and middle-income countries. As part of this, to critically analyse the evidence along the causal chain framework, linking interventions with intermediate outcomes and final impacts, and document the level/strength of evidence on potential pathways of impact using the framework. To assess if effects are moderated by characteristics of the participants, interventions, and/or settings. To provide an explanation for the intervention effects by examining what participants in the included studies reported about why the interventions did, or did not, work for them.
SELECTION CRITERIA
To be included in the review, studies were required to meet several eligibility criteria. First, studies must have evaluated an intervention with the means to improve the labour market situation of adults with disabilities. Such interventions could take the form of a device, policy, programme, strategy, or other type of action. Second, studies must have investigated outcomes for adults aged 16-65 years with physical and/or sensory impairments associated with disability. Third, the study setting must have been a low-or middle-income country (LMIC). Fourth, studies must have utilised one of the following: (a) randomised experimental design, (b) rigorous quasi-experimental design that used robust methods for removing biases due to non-random assignment of treatment, or (c) quasi-experimental design that used less rigorous methods for constructing the counterfactual, including uncontrolled studies. Fifth, studies must have reported at least one quantitative employment-related outcome variable. Sixth, the date of publication or reporting of the study must have been within the period 1 January 1990 to 31 December 2013. Finally, no language or form of publication restrictions was applied.
SEARCH STRATEGY
A systematic and comprehensive search was used to locate both published and unpublished studies. Ten major bibliographic databases were electronically searched, along with 32 specialist databases and library catalogues, and 59 websites of relevant organisations. Six journals were manually searched and search engines used. The reference lists of previous reviews and included studies were examined, and forward citation checking exercises were conducted. Finally, information was requested from authors of included studies and other relevant stakeholders.
DATA COLLECTION AND ANALYSIS
Each study was subject to a rigorous process of data extraction and quality assessment, conducted independently by pairs of reviewers using a coding tool specifically designed for this review. Descriptive analysis was undertaken to examine and describe data related to the characteristics of the included studies and interventions. The findings from the included studies were combined descriptively using a narrative approach to synthesis.
RESULTS
The literature search yielded a total of 20,417 potentially relevant reports, 479 of which were retrieved for full-text screening. A total of 14 studies met the eligibility criteria. Publication dates of included studies ranged between 1992 and 2012, with six studies published in the four-year period 2010-2013.
Studies were conducted in nine different LMICs in Asia, Africa and Latin America: Bangladesh (three studies); Brazil (two studies); China (one study); India (four studies); Kenya (one study); Nigeria (one study); Philippines (one study); Vietnam (one study) and Zimbabwe (one study). The majority of studies examined outcomes for adults with physical impairments. There was variation in sample sizes. One study had a sample size greater than 500 participants, the sample size was between 251 and 500 in three studies, and the remaining ten studies had a sample size of less than 250.
Different methodologies were employed to construct the counterfactual and evaluate the impacts of the interventions. The majority were uncontrolled before-and-after studies. One quasi-experiment (ex-post) utilised propensity score matching techniques and one study applied logistic regression to pre-test/post-test data. The remaining studies used a non-equivalent groups design. All 14 studies were assessed as high risk of bias.
The 14 studies examined 15 different interventions grouped as follows: treatment & therapy (four interventions); assistive devices and accommodations (two interventions); occupational rehabilitation services (four interventions); financial services (one intervention); and community-based rehabilitation (four interventions). Thirteen were multi-component programmes. All 15 interventions were targeted at people with disabilities, with some designed for people with a specific impairment or diagnosis. Six interventions targeted persons with specific types of physical impairment, and a further two interventions were available to adults with any type of physical impairment. Three interventions were targeted at persons with visual impairments. Finally, four interventions were available to persons with any/multiple impairments. Non-governmental organisations (NGOs) were the most common source of funding. The main aim of eight interventions was to improve employment prospects for persons with disabilities. The other interventions sought improvements in a wider range of outcomes. The interventions were designed and implemented on different scales, with the majority available over a large geographical area, such as one or more districts, provinces or regions. Information about duration of the interventions was often not reported, but typically they were available for periods of less than six months.
All 14 studies measured relevant labour market outcomes and assessed the following impacts: motivation to work (one study); professional social skills (one study); employment participation (12 studies); self-employment (two studies); income (four studies) and hours worked (one study). Five studies measured additional outcomes: health-related outcome (four studies); social outcomes (five studies); and empowerment-related outcome (one study). Several studies relied solely on self-reported outcome data. The majority of study reports did not provide clear information about the timing of outcome measurement. Only one study examined longer-term outcomes, evaluating impacts after two and four years of participants entering the programme.
In all 14 studies, the direction of effect was positive for the outcome variables measured. Five studies reported results of tests for statistical significance and indicated study findings were significant.
Seven of the 14 included studies explored variation in treatment effects. The variables considered were gender (three studies), participants' size of business (one study), impairment severity (one study), type of intervention (one study), and duration of follow-up (two studies). Four of the seven studies tested whether results were statistically significant. Overall, these seven studies were not sufficiently similar to detect meaningful differences in outcomes.
Two studies investigating occupational rehabilitation services reported participants' observations, experiences and views about why the intervention they received had worked for them. The following factors were cited: general health & well-being; cooperation in the family/community; motivation; attitudes in the workplace; attitudes in the community; and appropriateness of the training.
Three studies reported participants' observations, experiences and views about why the intervention they received had not worked for them. Two examined occupational rehabilitation services and the other evaluated the provision of free wheelchairs. The following barriers to the success of the interventions were cited: discriminatory attitudes of prospective employers; attitudes of family members and/or wider community; health and well-being; physical inaccessibility (workplace and/or broader environment); lack of ‘start-up’ funds for self-employment; shortcomings of the training (i.e., mismatch between it and participant's skills, abilities and financial resources); lack of education and skills; and motivation.
AUTHORS' CONCLUSIONS
A key finding of this review is the overall scarcity of robust evidence, as indicated by the relatively few studies that met the inclusion criteria. Although the evidence in general showed positive results, we need to be wary of drawing strong inferences from the findings of this body of literature. Not only is the number of impact evaluations limited, but most used designs in which conclusively attributing causality is not possible.
Our assessment of the evidence does not allow us to develop practical suggestions on what interventions are likely to work, for whom, and when. Clearly, there is an urgent need for investment in high quality impact evaluations of interventions to support people with disabilities in accessing the labour market in low- and middle-income settings. To build the evidence base further, it is therefore important that many more of the interventions currently in existence in low- and middle-income countries are rigorously evaluated, and the results are reported and disseminated widely. The methodological inconsistencies and weaknesses of the current evidence base, and specific knowledge gaps, suggest a number of future research priorities.
1 Introduction
1.1 RATIONALE
1.1.1 The Problem
Disability is a key development issue. Recent estimates suggest that more than one billion people (or about 15% of the world's population) are living with some form of disability---80% of whom live in low- and middle-income countries (World Health Organization [WHO], 2011). 1 People with disabilities are over-represented among the world's poor, and many experience multiple deprivations at higher rates and in higher breadth, depth, and severity than people without disabilities (Mitra, Posarac, & Vick, 2013; Samman & Rodriguez-Takeuchi, 2013). The lack of access to paid work and/or wider economic activity is a significant social disadvantage and helps maintain the link between poverty and disability in many country contexts (Braitwaite & Mont, 2009; Haveman & Wolfe, 1990; Hoogeveen, 2005; Peiyun & Livermore, 2008; WHO, 2011; Zaidi & Burchardt, 2005). The Millennium Development Goals (MDGs) on eliminating poverty, launched by the United Nations in 2000, are unlikely to be achieved unless explicit and specific efforts are undertaken to support disabled people's participation in labour market activities (Department for International Development [DFID], 2000; Groce & Trani, 2009).
There is no single, universally accepted definition of disability and defining it remains complex and controversial. In this study, disability is understood following the International Classification of Functioning, Disability and Health (ICF) which was developed by the WHO in 2001 in a long process involving academics, clinicians, and---importantly---people with disabilities (WHO, 2001). Representing a workable compromise between medical and social models, the ICF understands disability as arising from the interaction of health conditions with contextual factors (both environmental and personal). Disability is thus viewed not as a static feature of an individual, but rather as a complex, multi-dimensional, and changing experience for the individual (Schneider & Hartley, 2006). An implication of the ICF model of disability is that by removing barriers, persons with health conditions can be enabled to function and participate.
In many countries data on the employment of people with disabilities are not systematically available. Yet, where data exist, individuals with disabilities are found to be disadvantaged in both accessing and sustaining work and other forms of economic activity. Employment participation rates for people with disabilities are below that of the overall population; and, when disabled people do work, they generally do so for longer hours and lower incomes, have fewer chances of promotion, are more likely to work in the informal labour market, and are at greater risk of becoming unemployed for longer periods (Coleridge, 2005; Contreras, Ruiz-Tagle, Garces, & Azocar, 2006; Houtenville, Stapleton, Weathers, & Burkhauser, 2009; Mete, 2008; Mitra, 2008; Mitra et al., 2013; Mitra & Sambamoorthi, 2006; Mizunoya & Mitra, 2012; Roulstone, 2012; Roulstone, Gradwell, Price, & Child, 2003). Using data from 27 countries, a recent study from the Organization for Economic Co-operation and Development (OECD) found that people with disabilities are half as likely to be in paid work as their non-disabled counterparts (44% compared with 75%) (OECD, 2010).
Across the globe, people with disabilities find it difficult overcoming barriers to the workplace. Although this is not simply an issue in certain countries or even continents, the costs of disability are particularly acute in LMICs, where up to 80% of people with disabilities of working age can be unemployed, around twice that for their counterparts in industrialised countries (Contreras et al., 2006; Groce, Kembhavi, Wirz, Lang, Trani, & Kett, 2011; Houtenville et al., 2009; International Disability Rights Monitor, 2004; Mete, 2008; Mitra, 2009; Mitra et al., 2013; OECD, 2010). Rates of employment vary widely from country to country, from lows of 30% in South Africa to highs of 92% in Malawi (Loeb & Eide, 2004; 2004; Mitra, 2008). In many developing countries, a significant proportion of people work in the informal economy, and so are further disadvantaged. In India, for example, 87% of people with disabilities who work are in the informal sector (Mitra & Sambamoorthi, 2006a). It is less clear, however, whether the wage gap between disabled and non-disabled persons is as marked in developing counties as it is in industrialised countries (Mitra & Sambamoorthi, 2006b; OECD, 2003; WHO, 2011). Recent studies in India, for example, have produced mixed results (Mitra & Sambamoorthi, 2008, 2009).
Not all people with disabilities are equally disadvantaged. In practice, the extent of the negative effect of disability on employment is likely to vary depending on a variety of factors (Goertz, van Lierop, Houkes, & Nijhuis, 2010; Ingstad & Reynolds-Whyte, 1995; Kidd, Sloane, & Ferko, 2000; Mitra et al., 2013; OECD, 2010; Sena-Martins, 2010; World Bank, 2009). These include personal factors such as age, sex, level of education, motivation to work, and lack of financial resources. Women with disabilities, for instance, are recognised to be multiply disadvantaged, experiencing exclusion on account of their gender and their disability. There is evidence that disabled women tend to have less access to jobs, lower employment rates, and considerably lower earnings than male peers in similar jobs (Emmett, 2006; Mitra & Sambamoorthi, 2006; Mitra et al., 2013). Data for 51 countries from the World Health Survey, for example, show that employment rates are 19.6% for women with disability and 52.8% for men with disability (WHO, 2011). The links between disability and employment also vary considerably across impairment categories, severity and duration (WHO, 2011; World Blind Union, 2004). There is some evidence, for example, that individuals with mental health difficulties or intellectual impairments experience the lowest employment rates (Thornicroft, 2006) and those with more significant impairments are least likely to obtain work.
A range of environmental and personal factors can present barriers for persons with health conditions to function and participate in economic life. For example, the physical accessibility of local workplaces and transport facilities, available accommodations, and social attitudes can restrict participation in the labour market (Baldwin & Johnson, 2006; Bound & Burkhauser, 1999; Mitra & Sambamoorthi 2008). Lack of access to education and training or to financial resources can result in exclusion from the labour market, and social protection systems may create disincentives for people with disabilities to enter the labour market. There is also some evidence that people with disabilities seeking to access and sustain employment in competitive, tight labour markets are especially disadvantaged (Mitra, 2009). The policy context is relevant, too. The particular educational facilities, employment supports, health services, disability benefit systems, and other interventions that are available in a given context can influence whether, and to what extent, disability has employment consequences.
1.1.2 Why it is Important to do this Review
The barriers faced by people with disabilities globally in accessing and sustaining paid work is a profound social challenge. Many reasons are provided as to why these barriers exist and new policy visions are frequently offered up. Yet, efforts to promote development and poverty reduction have not always adequately included disability; for example, people with disabilities are not explicitly included in any of the MDG targets and indicators (WHO, 2011). Disability issues are, however, slowly being brought into the mainstream of development policy and practice, and over the past two decades there has been a noticeable change in the legal and policy responses of many governments and bilateral and multilateral donor agencies (DFID, 2000, 2007; Thomas, 2005). In 2002, for example, the World Bank embarked on mainstreaming disability into Bank operations and analysis (Mont, 2007). A major catalyst has been the Convention on the Rights of Persons with Disabilities (CRPD) adopted by the United Nations in 2006, which marked a significant advance in the recognition of the rights of disabled persons, including the right to work, on an equal basis with others (United Nations [UN], 2006). With increasing recognition of employment as a key factor in the process of empowerment and inclusion into society of people with disabilities, a shift to a broader framework for action has occurred, and the role of interventions to improve labour market outcomes is receiving increased international attention (DFID, 2000; International Labour Organization [ILO], 2008; WHO, 2004). Nevertheless, translating policy commitments into better lives for people with disabilities remains a profound social challenge. Establishing a firm evidence base to support the implementation of the CRPD is therefore a priority. Building a clearer understanding of which measures are effective at improving employment outcomes, and under which circumstances, can provide such an evidence base for policy development and contribute to the development of practical suggestions for meeting this challenge.
The existence of a growing body of evidence on interventions to increase the labour market participation of people with disabilities is highlighted in a recent comprehensive review of the literature in this area (Waddell, Burton, & Kendall, 2008). Taking a broad definition of vocational rehabilitation, and focusing on the conditions that account for two-thirds of long-term sickness absence in developed countries---mild/moderate musculoskeletal, mental health, and cardio-respiratory conditions---the study reviews the data from a large number of scientific reports and literature reviews, covering a wide range of intervention strategies. While the authors conducted a systematic search, assessed the strength of the evidence, and included data in evidence tables, they did not report effect sizes or perform a meta-analysis, making it difficult to judge and compare the effectiveness of the interventions. Other systematic reviews are more limited in scope, focusing on (a) specific countries (e.g., Bambra, Whithead, & Hamilton, 2004; Clayton et al., 2011); (b) single aspects of disability/illness, such as autism (e.g., Westbrook et al., 2012), mental illness (e.g., Crowther, Marshall, Bond, & Huxley, 2001; Underwood, Thomas, Williams, & Thieba, 2006), multiple sclerosis (e.g., Khan, Ng, & Turner-Stokes, 2009), traumatic brain injury (e.g., Graham & West, 2012), low back pain (e.g., Tveito, Hysing, & Eriksen, 2004) or spinal cord injury (e.g., Lidal, Huynh, & Biering-Sørensen, 2007); or (c) particular intervention types, such as interventions based on an empowerment perspective (e.g., Varekamp, Verbeek, & Dijk, 2006), workplace disability management programmes (e.g., Gensby et al., 2012) or workplace-based return-to-work interventions (e.g., Franche et al., 2005). Some of these reviews use meta-analytic synthesis methods, but several are quite dated and none explicitly focus on programmes conducted in LMICs.
There are a small number of recently published reviews in this area that focus on developing countries. The literature on assistive technology in LMICs is examined in two non-systematic reviews (Andrysek, 2010; Borg, Lindstrom, & Larsson, 2011). Some evaluative activities were identified, none of which measured employment outcomes. Another recent LMIC-focused non-systematic review (Velema, Ebenso, & Fuzikawa, 2008) examines evidence for the effectiveness of community-based rehabilitation (CBR) programmes for people with disabilities on a range of outcomes, including employment. A descriptive overview of the literature is presented, with no pooling of data. A non-systematic literature review by Mitra and Sambamoorthi (2006a) focused on impact evaluations conducted in India of the
People with Disabilities (PWD) Act and government programmes designed to promote employment among people with disabilities. More recently, a protocol was submitted for a joint Campbell/Cochrane systematic review of CBR for people with physical and mental disabilities in LMICs (Iemmi et al., 2012). Data will be collected on a number of functional outcomes (including employment) for different types of interventions, and variation of effects for different subject populations will be examined.
In sum, whilst existing reviews provide some evidence about the effectiveness of programmes to support the inclusion of persons with disabilities in the labour market, a number of them are now quite dated and specific gaps in the evidence base remain. Taking into account current policymaker priorities, this suggests a need to comprehensively assess the full evidence base relating to low- and middle-income countries, using appropriate methods to evaluate the impact of a range of different intervention types supporting the employment of adults with physical and/or sensory disabilities.
1.2 TYPE OF INTERVENTION
1.2.1 The Intervention
The scope of this review is not limited to one type of intervention. Rather, it extends to any intervention likely to help adults with disabilities in LMICs enter, re-enter, or maintain employment. Such interventions may take the form of a device, policy, programme, strategy, or other type of action. For the purposes of this review, a typology of intervention types was developed prior to undertaking the review, with a view that we would refine it on the basis of the review findings, if appropriate. The broad groupings are presented in Table 1.1. The characteristics of eligible interventions are broad. They (i) encompass complex, specialised, multidimensional programmes that implement multiple strategies as well as much simpler interventions based on a single strategy; (ii) may be implemented in any setting, including the workplace, health care facility, home, or community; (iii) include both routine and structured/tailored interventions; (iv) can vary not only by type but also by intensity; (v) can be delivered at various stages of the employment process (pre-employment, transition to employment, and post-employment); and (vi) need not have the core objective of restoring capacity for work.
INTERVENTION CATEGORIES
1.2.2 How the Intervention Might Work
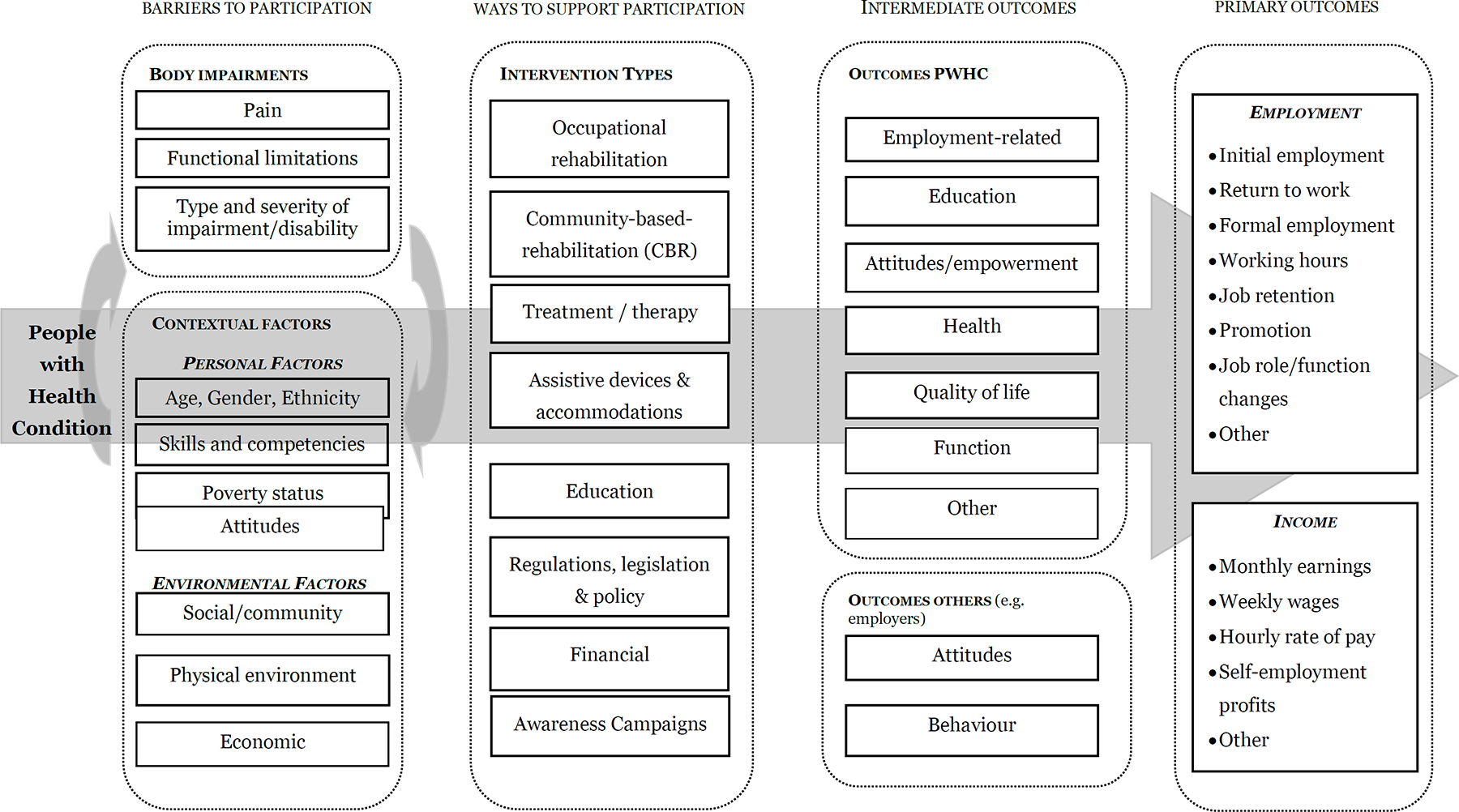
Conceptual understanding of the causal pathways through which available interventions may influence the employment prospects of people with disabilities in developing country contexts is under-developed. It was necessary, therefore, to develop a logic model specifically for this review. Originating from the field of programme evaluation, logic models (also known as theoretical, conceptual, or impact models) are typically diagrams or flow charts that illustrate pathways between inputs, strategies, outputs, and short-term, intermediate and longer-term outcomes (Anderson et al., 2011; Joly et al., 2007). Designed to read from left to right, they provide a valuable road map that spells out how, and for whom, a programme is meant to produce the desired outcomes. We hypothesised that the types of interventions detailed in Table 1.1 affect a range of different labour market outcomes for people with disabilities through various mechanisms. The model shown in Figure 1.1 illustrates both intermediary factors through which the intervention may exert its impact, and additional personal and contextual factors that may modify or inhibit the desired effect.
Logic Model
2 Objectives of the Review
Review Objective 1. To describe the range and diversity of interventions available for improving the labour market situation of adults with physical and/or sensory disabilities in developing country contexts.
Review Objective 2. To systematically identify, assess, and synthesise the evidence on the effects of interventions on employment-related outcomes for disabled adults in low- and middle-income countries. As part of this, to critically analyse the evidence along the causal chain framework, linking interventions with intermediate outcomes and final impacts, and document the level/strength of evidence on potential pathways of impact using the framework.
Review Objective 3. To assess if effects are moderated by characteristics of the participants, interventions, and/or settings.
Review Objective 4. To provide an explanation for the intervention effects by examining what participants in the included studies reported about why the interventions did, or did not, work for them.
3 Methods
3.1 TITLE REGISTRATION AND REVIEW PROTOCOL
The title for this systematic review was published in The Campbell Collaboration Library of Systematic Reviews on March 1, 2013. The review protocol was published on November 1, 2013. Both the title registration and protocol are available at: http://www.campbellcollaboration.org/library/php.
3.2 ELIGIBILITY CRITERIA
A preliminary scoping exercise conducted by the authors and reviews in this area both suggested a scarcity of relevant research literature. Therefore, prior to conducting the review we made the decision of making the selection criteria intentionally broad. Studies were included in the systematic review if they met the following eligibility criteria.
3.2.1 Types of Participants
Study participant characteristics:
Geographical location: Low- or middle-income country, as classified by the World Bank for the fiscal year 2013-2014, ending on June 30 2014 (see Table 9.2, Appendix I). The World Bank's country classifications are based on estimates of gross national income (GNI) per capita for the previous year. For the fiscal year starting 1 July 2013, these are: low income ($1,035 or less), middle income ($1,036 to $12,615).
Age: Working age adults, defined for this review as individuals aged 16-65 years.
Gender: Male or female.
Impairment category: Physical and/or sensory impairments (i.e., health conditions) associated with disability. See below for further details.
Employment status: Study participants may be in paid work or out of work at time of service receipt. Studies that have included those in work at time of service receipt may be relevant to this review if, for example, they have examined changes in the number of hours worked as a result of programmes received. Those out of work at time of service receipt may be employees on sick leave or unemployed individuals who are seeking (or otherwise eligible for) paid employment. Study samples made up solely of employed or non-employed individuals are eligible, as are those that contain a mix of both. See Section 2.2.3 for details of outcome measures.
Employment-related experience: Any prior work experience, vocational skills or achievements, or level of education.
Widely used by researchers and policy makers when addressing disability issues in the global development literature, the ICF is adopted as the conceptual framework for this systematic review. Disability is therefore understood as an umbrella term embracing impairments, activity limitations, and participation restrictions (WHO, 2001). The term impairment implies specific problems in body functions and structures, often identified as symptoms or signs of health conditions (i.e., diseases, injuries, and disorders). 2 The following additional definitions and restrictions also apply.
Definitions. Physical impairment is defined as problems with the structure, development, or function of the bones, muscles, joints, and/or central nervous system. Physical characteristics may include paralysis; altered muscle tone (ranging from loss of muscle mass to uncontrolled muscle contraction); an unsteady gait; loss of, or inability to use, one or more limbs; difficulty with gross-motor skills (such as walking); and/or difficulty with fine-motor skills (such as writing). Sensory impairment is defined as full or partial loss of one or more senses (e.g., sight, hearing, smell, touch, taste, and/or spatial awareness), causing difficulty with communication, gross-motor skills, fine-motor skills, and/or access to information.
Eligible studies. The focus is on impairments that meet customary and/or statutory definitions of disability. These are usually long-standing, for example, lasting at least one year, and have a substantial impact on a person's ability to do normal daily activities, such as getting dressed. The impairment/health condition may be acquired or congenital. It may be acute, chronic, progressive, or intermittent, and may or may not need ongoing medical intervention.
Studies of participants with the following types of health condition/physical impairments were eligible for the review: communicable diseases (e.g., leprosy); metabolism disorders (e.g., diabetes); respiratory conditions (e.g., asthma); neurological impairments (e.g., multiple sclerosis, epilepsy, those associated with brain injury); musculoskeletal conditions (e.g., arthritis, amputations); cardiovascular diseases; and body disfigurements (e.g., burn injuries). For sensory impairments, eligibility for the review was restricted to studies of the two most common types: visual impairment (full and partial loss of sight); hearing loss.
Where study participants were described as multiply disabled, the study was included if physical and/or sensory impairment was the primary diagnosis. Where study samples were comprised of people with different disabilities, we included the study if: (a) the majority of the sample was physically and/or sensory disabled; or (b) the authors reported disaggregated results according to type of disability.
Studies focused on work-related and non-work related health conditions were both eligible for inclusion in the review. Finally, eligibility for the review was extended to both primary studies that incorporated the ICF diagnostic framework in identifying and selecting its subjects and studies that did not use this framework.
Non-eligible studies. Studies focused solely on (i) people with mental health conditions and/or intellectual impairments, (ii) those with chronic illnesses that predominate in later life (e.g., chronic obstructive pulmonary disease (COPD), cancer, stroke, and renal disease), or (iii) HIV/AIDS were not eligible for this review, on the grounds that these groups have different rehabilitation needs.3 The review focuses on long-term disability, rather than persons with minor health problems, such as fractured bones or allergic rhinitis (hay fever). Therefore, evaluations of return-to-work (RTW) interventions for employees on short-term sick leave were outside the scope of this review.
3.2.2 Types of Interventions
The scope of this review extends to any intervention with the means to help adults with disabilities in LMICs gain or maintain employment. Such interventions may take the form of a device, policy, programme, strategy, or other type of action. Examples of relevant interventions were detailed in Section 1.2.
3.2.3 Types of Outcome Measures
To be eligible for this review, studies must have measured/reported at least one quantitative labour market outcome. Eligible outcomes include primary outcomes and intermediate outcomes.
Primary outcomes: People with disabilities in LMICs are often prevented from work, constrained in the type and amount of work that they do, and/or have difficulty sustaining work. As a consequence, they are predominantly employed in the informal sector, which is characterised by low pay. In consideration of this, the primary labour market outcomes of interest are those relating to the general constructs (a) employment participation (b) work productivity/performance, and (c) income.
For employment participation, examples of relevant indicators are: gaining initial employment; return-to-work (e.g., from non-employment, or from long-term sick leave); gaining formal employment (i.e., a ‘better’ job in that it has written contract, etc.); job retention; promotion (i.e., vertical job mobility); change in job role/function (i.e., horizontal job mobility).
For work productivity/performance, examples of relevant indicators are: number of weekly hours worked; number of days worked per month.
For income, examples of relevant indicators are: overall annual income; monthly earnings; weekly wages; average hourly rate of pay; and profits or income from self-employment.
Unless otherwise stated, employment refers to paid employment and self-employment. The following definitions of paid employment and self-employment apply to this review.
Paid employment: defined as jobs involving some form of contractual relationship between the individual worker and an employer over time for remuneration. Employment contracts may be explicit (written or oral) or implicit. Remuneration is typically in the form of wages and salaries, but people may also be paid by commission from sales, from piece-rates, bonuses, or in-kind payments such as food (ILO, 1993, para. 6). Those workers employed in the informal economy, over which there is little or no official control, are likely to be paid in cash. Within the definition of ‘paid employment’, the review includes both (a) competitive paid employment, broadly defined as jobs that are available on the open market and open to anyone who applies, and that offer payments and benefits that are comparable to industry/sector standards, and (b) jobs in an integrated work setting for individuals with disabilities who are working toward competitive employment with ongoing support services.
Self-employment: defined as jobs where ‘the remuneration is directly dependent upon the profits (or the potential for profits) derived from the goods or services produced … The incumbents make the operational decisions affecting the enterprise, or delegate such decisions while retaining responsibility for the welfare of the enterprise. In this context “enterprise” includes one-person operations’ (ILO, 1993, para. 7). Self-employment may take place anywhere: in the worker's home, fields, or any public place. Within the definition of self-employment, the review includes hawking, vending, and other street entrepreneurial activities (such as rickshaw pulling), but excludes other forms of making a living, such as begging, foraging, and scavenging.
Intermediate outcomes: Intermediate outcomes reflect the pathways through which the primary outcomes may be influenced. Studies that measured an intermediate job-related outcome (i.e., where individuals are still in the process of preparing for, and gradually moving closer to, work) were eligible for inclusion in the review. Studies that only reported non-work-related intermediate outcomes were not eligible.
Work-related intermediate outcomes may include, but are not limited to: attitudes to work, job search skills, job-related self-efficacy/confidence, career management skills, work readiness, job applications, and job interviews.
Other (non-work related) outcomes may include, but are not limited to: educational outcomes (e.g., attainment and attendance), health outcomes (e.g., intensity/severity of pain), functional limitations (e.g., range of movement), health care resource utilisation, and quality of life.
If any of the included studies measured outcomes for employers or other relevant stakeholders (e.g., co-workers, supervisors), in addition to outcomes for people with disabilities, we collected this outcome data.
Notes: The focus of this review is on economically productive ‘work’; therefore, it is not concerned with unpaid productivity, such as voluntary work, internships, household work, and family responsibilities/caring. It is also important to note that participation in education and training (including job training) is not defined as an employment outcome in this review. This takes into consideration growing evidence that many people with disabilities, particularly the young, are trapped in a ‘revolving door’ of training and vocational preparation abstracted from any real job opportunities (Corrigan & McCraken, 2005).
3.2.4 Types of Study Designs
As the literature was expected to be scarce, eligibility was extended to (a) randomised experiments, (b) rigorous quasi-experimental designs (QEDs) that used some method for removing biases due to non-random assignment of treatment (e.g., regression adjustment, difference-in-differences estimation, instrumental variables regression, fixed effects regression, regression discontinuity, matching, or inverse-propensity-weighted estimation), and (c) QEDs those that used less credible methods for constructing the counterfactual (including those that rely exclusively on before-and-after comparisons). 4
Eligible designs include those in which one of the following is true:
Experimental designs
participants are randomly assigned to the treatment and control groups by the investigator, using a process of random allocation, such as a random number generation (randomised controlled trial); a non-random (including quasi-random) method of assignment to treatment and control groups has been used by the investigators, for example, allocation by date of birth or day of the week (non-randomised controlled trial);
Quasi-experimental designs
decisions about which individuals receive the intervention and which serve as the controls are not in the hands of the investigator; instead, this is decided by the individuals themselves or by other circumstances (includes, for example, designs commonly referred to as controlled before-and-after studies and natural experiments) observations are made at multiple time points before and after an intervention in an attempt to detect whether the intervention has had an effect significantly greater than any underlying trend over time (time-series designs); participants in receipt of an intervention are compared with a group for whom data were collected earlier (historical control design); observations are made on a group of individuals before and after an intervention, with participants acting as their own controls (single-group pretest post-test design).
Studies collecting data at baseline and endline, and those collecting only endline data, were eligible for inclusion in the review (conditional on meeting all other criteria). Individually-allocated and cluster-allocated studies were also both eligible. The review included studies that adjust for confounders at either the design or analysis stage (e.g., studies using propensity score matching or regression analysis) and studies that have made no attempt to account for differences between the groups. No restriction was placed on the timing of outcome measurements (i.e., duration of follow up).
Although they fail to protect against most threats to internal validity (Shadish, Cook, & Campbell, 2002), studies using historical control and single-group pre-test/post-test (SGPPT) designs were included in the review as prior reviews and our preliminary scoping exercise suggested a scarcity of randomised controlled trials (RCTs) and robust quasi-experimental designs in this area. This decision was made prior to conducting the review. The inclusion of studies using weaker designs can help provide a fuller picture of strategies that are being utilised in the field and to
determine if the research base adequately represents the range of programmes currently in operation.
3.2.5 Date, Language and Form of Publication
For this review, eligibility extended to studies published or reported within the period 1 January 1990 to 31 December 2013. Studies published in any language were eligible, provided they met all other criteria. Studies were included regardless of their publication type (i.e., we did not exclude specific forms of publication, such as unpublished working papers, theses or dissertations).
3.3 LITERATURE SEARCH
Review management software, EPPI-Reviewer 4, was used to manage the entire review process (Thomas, Brunton, & Graziosi, 2010).
A comprehensive search strategy was used to search the international research literature for qualifying published and unpublished studies. To reduce the omission of relevant studies, a wide range of sources was used, many of which had a specific focus on low- and middle-income countries. Both electronic and manual searching techniques were used. The search period was 1 January 1990 to 31 December 2013.
The review did not involve a specific search for studies providing qualitative evidence. To address Review Objective 4, which sought to provide an explanation for why the interventions that are included in the quantitative synthesis did or did not work, relevant qualitative data was identified and extracted from the quantitative studies themselves.
Bibliographic databases and library catalogues. Ten major commercial electronic bibliographic databases were searched (see Table 10.3, Appendix I). A tailored search query was developed for each database using controlled vocabulary and/or free-text terms. The search queries for the ASSIA, ERIC, IBSS, Medline, Sociological Abstracts and Social Services Abstracts databases are provided in Table 10.4 (Appendix I), with others available from the first author on request.
In addition, 32 specialist databases and library catalogues were searched (see Table 10.5, Appendix I). These included databases of existing and ongoing impact evaluations, regional databases (some of which provide multilingual coverage5), grey literature databases, and databases/libraries specialising in information on employment, disability, and/or international development.
Websites. Fifty-nine websites were manually searched, including those for relevant research institutions, government-related aid agencies, non-governmental organisations (NGOs), and development banks (see Table 10.6, Appendix I). A further 36 organisations were contacted directly (see Table 10.7, Appendix I).
Backward citation tracking. The bibliographic information contained within the reference lists of included studies and relevant reviews was scanned for studies that meet the eligibility criteria. The following reviews were searched (Franche et al., 2005; Khan et al., 2009; Varekamp et al., 2006; Velema et al., 2008; Waddell et al., 2008; Westbrook et al., 2012).
Forward citation tracking. Studies that have cited the included studies since their publication were checked for relevance. Citation tracking was performed through Web of Knowledge and Google Scholar. All the hits from each citation search were screened.
Personal contacts. Specialists in the field, including authors of included studies and relevant ongoing research, were contacted with a request for information about potentially relevant studies, named programmes or other interventions.
Networks. Requests for relevant literature were made by posting a bulletin board/listserv message to members of several networks (see Table 10.8, Appendix I). A specific request for assistance with the location of studies published in languages other than English was made.
Search engines. Keyword searches were conducted using Google to follow up on potentially relevant programmes that came to light during the course of the review. Organisations and programmes were identified via snowballing from excluded studies. Google Scholar was used to track citations of included studies (see above).
Conference proceedings, dissertations and theses. One specialist source for dissertations and theses was searched (ProQuest Dissertations & Theses: UK & Ireland). Most of the major bibliographic databases also index this type of publication (ERIC, for example, includes over 14,000 dissertations/theses published since 1990). As part of the Web of Science search a specific search for conference proceedings was undertaken (Table 10.3, Appendix I).
Journals. The online versions of the Table of Contents of several journals were manually examined (see Table 10.9, Appendix I). Information provided by publishers about journal focus and content suggested that these were the most relevant to search. Many of the articles published in ALTER are in French.
3.4 STUDY SELECTION PROCESS
Potentially relevant items identified through the electronic searches were automatically imported into EPPI-Reviewer. A piloting exercise based on a 10% sample of reports was undertaken to ensure consistency in the application of the selection criteria described in Section 3.2. After finalising the criteria and associated guidance, each title and abstract was examined by a single reviewer for possible inclusion. Articles that did not meet the selection criteria were excluded. Reviewers were required to err on the side of caution, and where titles/abstracts did not contain sufficient information to determine inclusion or exclusion the full text copies were obtained. Bibliographic details of all potentially relevant studies identified through hand searching were entered manually into EPPI-Reviewer, and the full texts obtained. Two researchers independently read the full texts of all the articles retained after the first stage to further determine their suitability based on the specified criteria for inclusion. Any uncertainties and discrepancies were resolved by discussion, further review of the respective study reports and, where necessary, consultations with a third reviewer.
3.5 DATA COLLECTION
3.5.1 Criteria for Determination of Independent Findings
Efforts were made to identify all affiliations between studies/reports before coding commenced. Information on study sample sizes, intervention details, grant numbers, and so on were used to identify multiple reports from single studies. In cases where several different reports relating to a single study exist, reviewers classified the publication containing the most complete data set as the main report; when extracting data, the full set of relevant reports was used.
3.5.2 Data Extraction and Quality Appraisal
A coding tool was developed to capture study design characteristics, participant characteristics, intervention characteristics, outcome characteristics, data for effect size calculation (and/or other outcome data) and other substantive and descriptive study features.
Each study was appraised to determine its internal validity---that is, make sure that the study has been designed and conducted in such a way as to minimise the risk of bias, and that the outcomes are likely to be attributable to the intervention being assessed, rather than some other factor.
Included studies were coded on the following domains:
Potential for selection bias/confounding due to non-random assignment, no adjustment for differences in baseline measurements, etc. Potential bias due to attrition, compliance or otherwise missing data. Potential for performance bias due to systematic differences in the care provided to participants (e.g., spill-over, non-intervention based differences in treatment, or other types of interference across intervention and non-intervention units). Potential bias due to systematic differences in outcomes assessment among groups being compared (detection bias). Selective outcome and analysis reporting based on systematic differences between reported and unreported findings.
For each of these domains, we coded the paper as ‘Yes’ if it addressed the issue, ‘No’ if it did not, ‘Unclear’ if it was unclear, and ‘Not relevant’ if the issue was not applicable for that particular study. For those domains with two parts (‘a’ and ‘b’), both parts had to be answered ‘Yes’ for the study to score ‘Yes’ overall for that domain. We then aggregated to an overall risk of bias as follows:
Low Risk of Bias (bias, if present, is unlikely to alter the results of the research): ‘Yes’ for four or five categories. Medium Risk of Bias (a risk of bias that raises some doubts about the results): ‘Yes’ for three categories. High Risk of Bias (bias likely to seriously alter the results): ‘Yes’ for two or less categories.
The coding tool was pilot tested and modified as necessary. Members of the review team worked independently on a purposive sample of eligible studies, which were selected to test the tool on the full range of relevant study designs, before meeting to compare their decisions. Reviewers were retrained on any coding items that showed discrepancies during this process and the coding manual was adapted accordingly. This process was repeated until a very high level of consistency in reviewers' application of the codes was achieved, at which point the tool was finalised. A draft version of the codebook for data collection is presented in the study protocol. The risk of bias section of the tool is detailed in Table 10.10 (Appendix I).
The EPPI-Reviewer software was used to collect data necessary for the description, analysis and quality appraisal of studies. All studies included in the review were independently evaluated by two reviewers who came together to compare their decisions. Any uncertainties and discrepancies were resolved by discussion, further review of the respective study reports and, where necessary, consultations with a third reviewer.
Data were collected for all labour market outcomes reported (both positive and negative), relevant sub-groups and where studies include multiple follow-up time periods. For the data analysis, where studies used several indicators for a particular outcome variable, our approach was to drop indicators. This involved selecting the indicator most similar to those used by other studies in that category and retaining only the data for that outcome indicator in the analysis. The reviewers attempted to contact the authors of study reports that were missing data that would allow the computation of effect sizes.
Efforts were made to identify all affiliations between studies/reports before coding commenced, using information on study sample sizes, intervention details, grant numbers, and so on. In cases where a single report described more than one study, each study was coded separately (i.e., as if they had been published separately).
3.6 DATA ANALYSIS
The method of synthesis used in this review reflects the nature of the included studies. Statistical meta-analysis was neither feasible nor appropriate. As shown in the next chapter, the reviewed body of literature is broad in terms of population and intervention characteristics. In addition, the majority of studies used a repeated measures design and presented data in the form of proportions or frequencies. Odds ratios (ORs) are the usual effect size metric for dichotomous variables, but ORs are typically used for independent group designs (Lipsey & Wilson, 2001); calculating odds ratio effect sizes was not appropriate for the single-group pre-test/post-test (SGPPT) design studies. Most of the included studies using independent groups did not report sufficient data to allow for effect size calculations.
On balance, it was felt that a narrative approach to data synthesis was the most appropriate method for this review. Narrative synthesis involves the arrangement of studies into relatively homogenous groups according to a standard format, with similarities and differences compared across studies (Barnett-Page & Thomas, 2009). We drew on the logic model framework detailed in Figure 1.1 and structured the findings according to outcome variable, with consideration also given to participant characteristics. For each outcome, the results are reported and analysed separately by impairment category (i.e., grouped according to the target population for each intervention). We have presenting the direction, magnitude and statistical significance of findings (as reported by the original investigators), together with information about the sample size and risk of bias. These should be considered when interpreting the findings. There was no statistical pooling of data, so we did not analyse the SGPPT studies separately from the more robust quasi-experiments (as specified in the protocol).
4 Search Results
4.1 LITERATURE SEARCH AND STUDY IDENTIFICATION
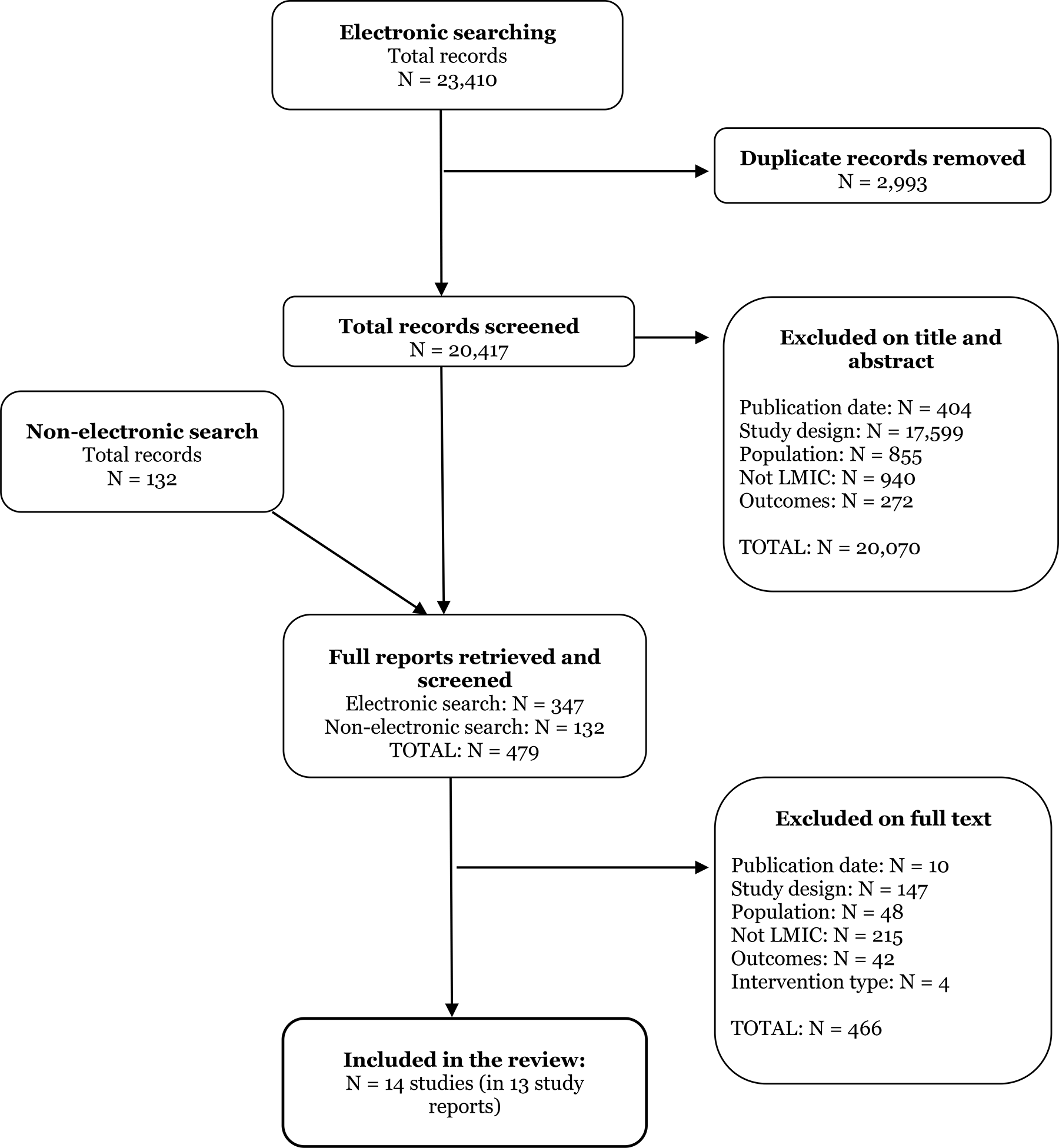
Figure 4.1 details the search and study selection process. Initially, 23,410 citations were identified by electronically searching the major bibliographic databases. After removal of 2,993 duplicates, the remaining 20,417 items were manually screened against the eligibility criteria on title and abstract. This resulted in the exclusion of 20,070 studies, leaving 347 references as potentially relevant to the review. Searches of additional sources yielded a further 132 potentially relevant studies, and these were added to the 347 studies from the main electronic search. The full length reports of these 479 studies were identified and read independently by two researchers. Upon careful examination against the selection criteria, 466 study reports reviewed at this stage did not meet the eligibility requirements. The most common reason for excluding studies was that they were not located in a low- or middle-income country. Bibliographic details of the 466 excluded studies are available on request.
Fourteen studies (reported in thirteen papers) met all requirements and were selected for analysis. These are listed in Section 9.1. Six of the included studies were identified through electronic searches of the major bibliographic databases, and the remainder through other sources.
Two of the study reports excluded on date (both published in 2014) were identified as providing further follow-up data relating to a study already included in the review. These “linked reports” are listed in Section 9.2. Two additional excluded papers provide further information about interventions evaluated in the included studies. These as “companion reports” are listed in Section 9.3.
Flow of Literature Through the Review
5 Descriptive Findings
Fourteen studies met the criteria for inclusion in the synthesis. To fully explore the data, we conducted several types of analyses. This chapter presents a descriptive profile of the included studies. Section 5.1 details important study characteristics, such as publication, sample, and methodological characteristics. Section 5.2 describes the range and diversity of interventions evaluated in the included studies (Review Objective 1). In Chapter 6, we present the synthesis of study findings (Review Objective 2).
5.1 STUDY CHARACTERISTICS
In this section, we present key features of the included research. Tables 5.1, 5.2 and 5.3 summarise the substantive and methodological characteristics of the 14 included studies. Information on each separate study is provided in Table 10.12 (Appendix I).
General characteristics of included studies
Shore and Juillerat (2012) collected data from a total of three countries: India and Vietnam, both lower-middle income countries, and Chile, which was reclassified as a high-income country in the fiscal year starting 1 July 2013. This is treated as one study in this review. One study report details the author's evaluation of two different programmes across two continents and is treated as two studies in this review. 6
The majority of included studies were conducted in Asia: seven in South Asian countries (Bangladesh and India), and three in East Asia and the Pacific (China, Philippines and Vietnam). Three studies were undertaken in Sub-Saharan African countries (Kenya, Nigeria and Zimbabwe) and two were located in the Latin America and the Caribbean region (Brazil).
All impairment types were represented in the impact assessments, with the majority (eight studies) examining outcomes for people with physical impairments (Gershon & Srinivasan, 1992; Guarino et al., 2007; Hansen et al., 2007; Metts & Oleson, 1995; Momin, 2004; Pereira-Guizzo et al., 2012; Shore & Juillerat, 2012; Tang et al., 2011). Two impact assessments focused exclusively on people with sensory disabilities (Eniola & Adebiyi, 2007; Finger et al., 2012). The study samples of the remaining four evaluations included participants with any/multiple types of disability, predominantly those with physical and sensory impairments (Biggeri et al., 2012; Lagerkvist, 1992a; Lagerkvist, 1992b; Nuri et al., 2012).
All 14 studies were conducted with adults aged 16 years and over, although one study report did not provide clear details of participants' ages. Four studies also included children in the sample population. One study focused exclusively on young adults (Eniola & Adebiyi, 2007). A single study included males only (Tang et al., 2011); the remainder were mixed sex. In 12 of the 14 studies, at least some participants had previous work experience.
Sample characteristics
Seven of the 14 included studies examined variability of treatment effects, e.g., across interventions and sub-groups (Biggeri et al., 2012; Eniola & Adebiyi, 2007; Hansen et al., 2007; Metts & Oleson, 1995; Nuri et al., 2012; Pereira-Guizzo et al., 2012; Shore & Juillerat, 2012).
Timing of outcome measurement varied between studies. Short-term outcomes were measured in five of the 14 included studies. One study examined longer-term outcomes, evaluating impacts on participants after two and four years of entering the programme. The remaining eight reports did not provide clear information about this aspect of the study.
Methodological characteristics
5.2 INTERVENTION CHARACTERISTICS
The 14 included studies covered 15 different interventions. One study report (Eniola & Adebiyi, 2007) compared two interventions, as well investigating impacts for the sample as a whole. As noted above, Lagerkvist (1992) investigated two separate evaluations of programmes operating in different countries and is treated as two studies in this review. 7 Sections 5.2.1 to 5.2.5 describe the key features of the interventions, grouped according to intervention type and disability category. Table 5.4 summarises the intervention characteristics. Information on each separate intervention is provided in Table 10.13 (Appendix I).
Intervention characteristics
5.2.1 Treatment/Therapeutic Interventions
Four treatment/therapeutic interventions were assessed in three of the included studies (see Table 5.5). One study was set in Brazil and evaluated a small-scale intervention for people with physical impairments (Pereira-Guizzo et al., 2012). The remaining three interventions in this category were designed for the visually impaired: two small-scale interventions in Nigeria (Eniola & Adebiyi, 2007) and a regional programme operating in India (Finger et al., 2012).
Treatment / therapeutic interventions
Pereira-Guizzo et al. (2012) evaluated the Program for the Development of Social Skills for the Work Environment, which aimed to develop disabled people's work-related social skills and include them into the labour market. The intervention was delivered at institutions in two cities in the state of São Paulo, Brazil - the Municipal Bureau of social welfare and a philanthropic association. It was composed of 16 group sessions, carried out twice a week, lasting approximately 90 minutes each. The overall structure of the programme was based on the experiential method associated with cognitive-behavioural techniques. It appeared to have been designed by the authors of the study.
Eniola and Adebiyi (2007) assessed the impact of two interventions (labelled as ‘emotional intelligence’ and ‘goal setting’ techniques) upon the motivation to work among visually impaired students attending the School for Handicapped Children, Ibadan and Osogbo, Nigeria. Both interventions were delivered over six weeks (two sessions per week) and entailed a number components, including lectures, home assignments, and other activities. The authors of this pilot study appear to have designed the interventions, and do not clearly report how the two techniques differed.
Finger et al. (2012) examined the impact of a multi-component cataract outreach programme in South India. This regional programme was available in the rural area of Tamil Nadu state, and was operated by a community eyecare provider, Sankara Eye Care Services, Coimbatore. Patients underwent cataract surgery and received a one-month follow up at the outreach centre. Patients' transport, surgery and inpatient hospital stays were provided free by the hospital as patients all fell under the poverty threshold. The study was embedded within routine services provided by Sankara Eye Care.
5.2.2 Assistive Devices & Accommodations
Two included studies evaluated assistive devices designed to improve general well-being (see Table 5.6). Both interventions were targeted at individuals with mobility impairments (Guarino et al., 2007; Shore & Juillerat, 2012).
Assistive devices and accommodations
The study by Guarino et al. (2007) assessed the benefits for lower-limb amputees of using a prosthesis. Patients attended a university-based rehabilitation centre, the Lar Escola Sao Francisco Rehabilitation Centre, Universidade Federal de São Paulo (UNIFESP), in the city of São Paulo, Brazil. A charge was made for the prosthetics.
Shore and Juillerat (2012) evaluated the impact of wheelchairs distributed by an international NGO, the Free Wheelchair Mission (FWM). As of 2012, FWM has distributed over 600,000 wheelchairs in developing countries. Wheelchairs are provided free of charge to recipients, made possible through local and national fundraising efforts. The cost to produce, ship, assemble and deliver the chair to recipients was under US$60 worldwide.
5.2.3 Occupational Rehabilitation
Four studies evaluated multi-component occupational rehabilitation programmes (see Table 5.7). Three of the four programmes in this category were managed by the Centre for the Rehabilitation of the Paralysed (CRP), an NGO that has operated in several regions of Bangladesh since 1979---the only organisation of its kind in the country (Hansen et al., 2007; Momin, 2004; Nuri et al., 2012). The remaining programme was a national initiative in China. Three programmes were targeted at people with physical disabilities, whereas the fourth programme was open to adults with any type of disability.
Occupational rehabilitation services
Hansen et al. (2007) evaluated a tailored work rehabilitation programme based in Savar, an area about 25km from Dhaka, Bangladesh. The initiative was delivered by CRP. It provides specialised services for people with spinal cord injuries, and aims at returning participants to their previous employment or a suitable alternative. The study focus is on a sample of those who completed the programme in the three-year period 2002-2005.
Momin (2004) evaluated another CRP run rehabilitation programme for people with spinal cord injuries. In this study, participants lived in the Dhaka, Narayangonj, Gazipur, Manikgonj, Munshigonj and Narshingdi districts of Bangladesh, and had received services between 1994 and 1999. Services focused on the person's whole life. Vocational training was provided, support was extended once the person returned to the community, and families were encouraged to become active participants in the rehabilitation process
Tang et al. (2011) evaluated a multi-dimensional return-to-work (RTW) programme provided by the Guangdong Provincial Work Injury Rehabilitation Center, the first and leading institution of occupational rehabilitation in China. The demonstration centre is located in the southeast of the country and has offered training courses nationwide since 2004. It is available to persons with occupational injuries who are on long-term absence from work or short-term sick leave. It is based on a case management approach and includes both social and occupational rehabilitation as well as follow-up after return to work. Clients attend the centre for three months and then receive six months follow-up support.
Nuri et al. (2012) evaluated the effectiveness of the Madhab Memorial Vocational Training Institute (MMVTI) programme in Bangladesh, which is part of the Centre for the Rehabilitation of the Paralysed (CRP). Disabled participants were selected from five districts across central Bangladesh. Data was also collected from 10 non-disabled key informants (local leaders, employers, and project staff). This programme specialises in the occupational rehabilitation of persons with disabilities through specifically designed vocational training and job placements. Individuals are carefully matched to courses after a full assessment by a multidisciplinary team of doctors, social workers and other professionals.
5.2.4 Financial Services
One study evaluated the impact of a financial programme (see Table 5.8). It was available to adults with physical disabilities (Metts & Oleson, 1995).
Financial services
Metts and Oleson (1995) evaluated the initial phase of the Disabled persons Loan Scheme, a multi-component programme funded by the United National Development Programme (UNDP). At the time of the study, it was available in 20 rural districts of Kenya. The typical loan recipient had an orthopaedic disability. Potential beneficiaries received basic business training and assistance with the process of apply for loans through Barclay's Bank of Kenya. Clients were identified by Kenya's Ministry of Culture and Social Services and selected by District Loan Review Committees. Business training and assistance with loan applications were provided by three sub-contracted NGOs, and beneficiaries received them for the duration of the loan repayment period. Loans were provided at market rates of interest and guaranteed by a credit guarantee fund deposited with the bank.
5.2.5 Community-Based Rehabilitation
Four studies evaluated the impact of four community-based rehabilitation (CBR) programmes (see Table 5.9). Three programmes were open to people with any/multiple types of impairment (Biggeri et al., 2012; Lagerkvist, 1992a; Lagerkvist, 1992b) and one was designed specifically for people with leprosy (Gershon & Srinivasan, 1992).
Community-based rehabilitation
In the study by Biggeri et al. (2012) approximately three-quarters of the sample were described as having a physical and/or sensory impairment. This study was conducted in neighbouring districts in South Karnataka State, southern India. The authors indicated that the programme covered all five areas of the CRB matrix (health, education, livelihood, social and empowerment) and included activities such as home visits, health awareness, therapy services, referral services, aids/appliance support, and legal support. It was implemented through a participatory development approach with active participation of persons with disabilities at all levels.
In Zimbabwe, Lagerkvist (1992a) evaluated a CBR programme run by the Red Cross in two districts since 1985. Two rehabilitation assistants with 1-2 years medical education were responsible for assessment of clients, analysing a rehabilitation plan for each client, and training local coordinators and volunteers. Local coordinators were committee workers with some medical training, and responsible for 300-400 disabled persons in an area.
Lagerkvist (1992b) assessed the impact of a CBR programme that had operated in the Philippines since 1981. This programme had a different style of management to the one in Zimbabwe. It was managed and supervised from a rehabilitation centre and was based on local supervisors who were community workers recruited from the villages. Each one was expected to work one to two days a week with four to eight disabled persons. World Health Organization (WHO) training packages were used.
6 Synthesis of Results
6.1 INTRODUCTION
The previous two chapters describe the search results and the main features of the included studies and interventions (Review Objective 1). In this chapter, we provide the results of the analysis to determine the overall effects of the reviewed interventions (Review Objective 2) including possible moderators of treatment effects (Review Objective 3). Finally, a synthesis of the qualitative evidence from these studies is presented (Review Objective 4).
6.2 WHAT DOES THE QUANTITATIVE EVIDENCE SAY?
The second (and primary) objective of the review is to systematically identify, appraise and synthesise evidence from impact evaluations to answer the following review question:
What are the effects of interventions on the labour market situation of adults with physical and sensory disabilities in low- and middle-income countries?
Fourteen eligible studies with a range of designs were identified and are represented in this synthesis. Statistical meta-analysis was neither feasible nor appropriate. As shown in Chapter 5, the evidence base is heterogeneous, with the reviewed body of literature broad in terms of population and intervention characteristics. In addition, the majority of evaluation designs were unsuitable, and/or authors did not report sufficient data, for effect size calculations. A narrative approach was therefore taken for data synthesis.
Intervention / outcome
In reviewing the available evidence, we drew on the logic model framework detailed in Figure 1.1 and report the findings of the review by outcome variable. The following sub-questions were used to structure the synthesis. In answering each question, the results are reported and analysed separately by impairment category (i.e., grouped according to the target population for each intervention). As all studies were judged to be of low quality, there was no scope to report and analyse results separately by risk of bias status.
What effects do interventions to support adults with disabilities have on motivation to work?
What effects do interventions to support adults with disabilities have on professional social skills?
What effects do interventions to support adults with disabilities have on paid employment?
What effects do interventions to support adults with disabilities have on self-employment?
What effects do interventions to support adults with disabilities have on income?
What effects do interventions to support adults with disabilities have on the number of hours worked?
6.2.1 What effects do interventions to support adults with disabilities have on motivation to work?
One study addressed this sub-question (see Table 10.18, Appendix I). It focused on persons with visual impairments. The direction of effect was positive and statistically significant.
6.2.2 What effects do interventions to support adults with disabilities have on professional social skills?
One study addressed this sub-question (see Table 10.19, Appendix I). It examined an intervention for people with physical impairments. The direction of effect was positive and statistically significant.
6.2.3 What effects do interventions to support adults with disabilities have on paid employment?
Twelve studies examining 12 different interventions addressed this sub-question (see Table 10.14, Appendix I). Different measures of paid employment were used, ranging from engagement in any type of income-generating activity to formal employment. Baseline samples ranged in size from 1 to 620. Seven studies evaluated interventions designed for persons with physical disabilities and one focused on an intervention for the visually impaired. An additional four studies evaluated interventions that were open to individuals with any/multiple impairments. The direction of effect in all 12 studies was positive. Three study reports (Biggeri et al., 2012; Finger et al., 2012; Shore & Juillerat, 2012) presented results of tests for statistical significance and indicated study findings were significant.
6.2.4 What effects do interventions to support adults with disabilities have on self-employment?
Two studies addressed this sub-question (see Table 10.15, Appendix I). Both evaluated interventions for persons with physical impairments. The direction of effect in both studies was positive. Neither study reported results of tests for statistical significance.
6.2.5 What effects do interventions to support adults with disabilities have on income?
Four studies addressed this sub- question (see Table 10.16, Appendix I); all utilised a single group pre-test/post-test design. Of these, one study (Finger et al., 2012) used logistic regression. Baseline samples ranged in size from 55 to 620. Three studies evaluated interventions for persons with physical disabilities and one focused on an intervention for the visually impaired. The direction of effect in all four studies was positive. Two studies (Finger et al., 2012; Shore & Juillerat, 2012) reported results of tests for statistical significance and indicated study findings were significant.
6.2.6 What effects do interventions to support adults with disabilities have on number of hours worked?
One study addressed this sub-question (see Table 10.17 Appendix I). It evaluated an intervention for persons with physical impairments. The direction of effect was positive. The study did not report results of tests for statistical significance.
6.3 WHAT DO THE STUDIES REPORT ABOUT VARIABILITY IN EFFECTS?
A further objective of this review was to examine variability of treatment effects, e.g., across interventions, settings and sub-groups (Review Objective 3). Seven of the 14 included studies provided relevant data (Biggeri et al., 2012; Eniola & Adebiyi, 2007; Hansen et al., 2007; Metts & Oleson, 1995; Nuri et al., 2012; Pereira-Guizzo et al., 2012; Shore & Juillerat, 2012). The variables considered were gender, participants' size of business, impairment severity, type of intervention, and duration of follow-up. Overall, these seven studies were not sufficiently similar to detect meaningful differences in outcomes.
Three studies considered the influence of participants' gender on treatment effects. In their evaluation of an occupational rehabilitation programme in Bangladesh, Nuri et al. (2012) found that the proportion of participants who secured some form of employment was higher for females (71%) than for males (53%). In contrast, the group means in the study by Eniola and Adebiyi (2007) of two therapeutic programmes in Nigeria suggest that the increase in employment was driven by males, although the authors noted that the difference was not statistically significant. As part of their assessment of the Disabled Persons Loan Scheme (DPLS) in Kenya, Metts & Oleson (1995) examined the influence of gender on net income and reported that women appeared to benefit more than men (74% increase for women compared with 33% for men), though men had higher net incomes than women, both before and after the loans.
One study examined whether participants' size of business made a difference (Metts & Oleson, 1995). The authors observed that the impacts of the DPLS on net income varied with participants' size of the business, with the smallest businesses (those earning less than 1000 Kenyan Shillings per month before the loan) experiencing the largest gains.
One study examined the influence of impairment severity. Hansen et al. (2007), in their study of occupational rehabilitation services in Bangladesh, found some evidence that wheelchair users may find re-employment more challenging compared to those who only depend on crutches (p<0.028, χ2=4.847, df=1).
One study considered whether type of intervention was important (Eniola & Adebiyi, 2007). Two different types of therapeutic techniques were compared, with the pretest/post-test group means suggesting that Emotional Intelligence had a more positive impact than Goal Setting (mean score increase of 10.2 compared with 2.9). However, a significant interaction was not found.
Two studies measured the effects of duration of follow-up. Biggeri et al. (2012) evaluated a CBR programme in India and found it had a small but significant effect on employment after two years implementation (ATT=0.05, SD=0.014, t=3.714), whereas the four-year effect on the same variable was around 16% (ATT=0.164, SD=0.035, t=4.638). In their study of the Program for the Development of Social Skills for the Work Environment in Brazil, Pereira-Guizzo et al. (2012) measured three different indicators of professional social skills several times over an eight-month period. In the follow-up assessments, both intervention groups maintained the improvements that were obtained through the programme (no data reported).
6.4 WHAT DOES THE QUALITATIVE EVIDENCE SAY?
Where available, qualitative data relating to people's observations, experiences and views about why the interventions they received did, or did not, work for them was drawn from the studies in an attempt to provide an explanation for the observed effects (Review Objective 4).
Three of the 14 included studies collected qualitative data to try to understand more fully why programmes achieve or fail to achieve an impact on labour market outcomes. The interventions in these studies were either targeted at individuals with physical impairments (Hansen et al. 2007; Shore & Juillerat, 2012) or open to those with any type of impairment (Nuri et al., 2012).
6.4.1 What were participants' observations, experiences and views about why the intervention they received had worked for them?
Two studies answered this question (Hansen et al., 2007; Nuri et al., 2012). Both examined occupational rehabilitations programmes managed by the same NGO in Bangladesh. The following factors were cited:
General health & well-being (one study) Cooperation in the family/community (one study) Motivation (one study) Attitudes in the workplace (one study) Attitudes in the community (one study) Appropriateness of the training (one study)
6.4.2 What were participants' observations, experiences and views about why the intervention they received had not worked for them?
Three studies answered this question (Hansen et al. 2007; Nuri et al., 2012; Shore & Juillerat, 2012). Two studies examined occupational rehabilitations programmes in Bangladesh and one study evaluated the impact of providing manual wheelchairs to persons with mobility impairments in India and Vietnam. The following barriers to the success of the interventions were cited:
Discriminatory attitudes of prospective employers (one study) Attitudes of family members and/or wider community (two studies) Health and well-being (one study) Physical inaccessibility (workplace and/or broader environment) (two studies) Lack of ‘start-up’ funds for self-employment (one study) Shortcomings of the training (i.e., mismatch between it and participant's skills, abilities and financial resources) (one study) Lack of education and skills (one study) Motivation (one study)
7 Conclusions
7.1 SUMMARY
In the past, the lack of data on people with disabilities living in LMICs has contributed to the invisibility of disability as a development priority. This is beginning to be addressed. While the Millennium Development Goals (MDGs) did not specifically mention disability, it is increasingly being recognised that the new post-MDG development agenda will be impossible to achieve without inclusion of people with disabilities. This systematic review examined the current evidence on the effectiveness of different interventions to improve the labour market participation of adults with disabilities in LMICs. The review scope covered a wide range of intervention strategies, populations, settings and evaluation designs. This allowed us to draw on a broader range of evidence.
Research in this area has received very little attention. Despite an extensive search, only 14 eligible impact evaluations published across the 20-year period 1992-2012 were identified. Not only is the total number of studies low, but there are also multiple sources of heterogeneity and specific knowledge gaps. As it was neither possible nor appropriate to conduct meta-analysis, we could not use statistical methods to detect programme effects and so we do not have a pooled estimate of effect. Results were examined narratively. The key findings are summarised below and are discussed further in section 7.2.
Eniola & Adebiyi (2007) investigated two motivation skills interventions -emotional intelligence (EI) and goal setting (GS) therapeutic techniques - for visually impaired students in Nigeria.
Pereira-Guizzo et al. (2012) assessed the impact of the Program for the Development of Social Skills for the Work Environment on persons with any type of physical impairment in Brazil.
Seven studies evaluated different types of support for persons with physical disabilities, with five of the seven interventions designed for people with a specific impairment. These included provision of prostheses to lower limb amputees in Brazil (Guarino et al., 2007); manual wheelchair provision for persons with limited mobility in India and Vietnam (Shore & Juillerat, 2012); an occupational rehabilitation programme for spinal cord patients in Bangladesh (Hansen et al., 2007); a community-based rehabilitation programme for people affected by leprosy in India (Gershon & Srinivasan, 1992); and an occupational rehabilitation programme for persons with work injuries in China (Tang et al., 2011). Two programmes were available to persons with any type of physical impairment: the Disabled Persons Loan Scheme in Kenya (Metts & Oleson, 1995) and an occupational rehabilitation programme in Bangladesh (Momin, 2004). One study (Finger et al., 2012) focused on an intervention for the visually impaired. It evaluated a cataract outreach programme in India. Four studies (reported in three papers) evaluated four interventions that were open to individuals with any/multiple types of impairments. These included community-based rehabilitation programmes in India (Biggeri et al., 2012), Zimbabwe (Lagerkvist, 1992) and the Philippines (Lagerkvist, 1992), and an occupational rehabilitation programme in Bangladesh (Nuri et al., 2012).
Both studies evaluated interventions open to persons with any type of physical impairment. These included the Disabled Persons Loan Scheme in Kenya (Metts & Oleson, 1995) and an occupational rehabilitation programme in Bangladesh (Momin, 2004).
Three studies evaluated interventions designed for persons with physical disabilities. Of these, two were for people with a specific impairment: a community-based rehabilitation programme (CBR) for people affected by leprosy in India (Gershon & Srinivasan, 1992) and manual wheelchair provision in India and Vietnam Chile (Shore & Juillerat, 2012). One programme was available to persons with any type of physical impairment: the Disabled Persons Loan Scheme in Kenya (Metts & Oleson, 1995). One study (Finger et al., 2012) focused on an intervention for the visually impaired. It evaluated a cataract outreach programme in India.
Metts and Oleson (1995) evaluated the Disabled Persons Loan Scheme for persons in Kenya with any type of physical impairment.
7.2 DISCUSSION AND CONCLUSIONS
Many existing international development reviews contain only a small number of studies (Waddington et al., 2012), and our preliminary searches suggested this was likely to be the case for the area in which we were working. Therefore, to avoid an empty, or near-empty, review we did two things. First, we set the quality threshold bar low a priori and included uncontrolled before-and-after studies. Second, the review was intentionally broad in scope, involving a range of different intervention strategies, populations and geographical settings. Rather than set the question around a discrete intervention, any intervention with the potential to help adults with disabilities in the labour market was eligible for inclusion in the review. The review scope also extended to two of the main impairment categories, physical and sensory, and all LMICs as currently defined by the World Bank. Yet, despite the broad review scope, and an extensive search for published and unpublished studies, only 14 eligible impact evaluations were identified. Furthermore, they were conducted in a limited range of LMICs. Only five countries in Asia, three in Africa and one in Latin America were represented: three were low-income economies (Bangladesh, Kenya, Zimbabwe), four were lower-middle income (India, Nigeria, Philippines, Vietnam), and two were upper-middle income (Brazil, China). We are not aware of any on-going primary studies.
Populations with all impairment types were represented in the impact assessments, although most were focused on persons with physical impairments. Some groups of disabled people were under-represented in the review. No impact evaluations of intervention designed specifically for persons with hearing impairments were identified. Disabled women are particularly disadvantaged in the labour market, experiencing exclusion on account of both their gender and their disability. However, no interventions specifically targeted at women were identified. Also important is the distinction between those who are disabled during childhood and those who are disabled later in life, after entering work, since they face very different labour market issues (Baldwin & Johnson, 2001). The first group may face discrimination in education and upon entry to work, whereas the second group can be affected by discrimination when returning to work after illness. One included study investigated a programme aimed at returning injured workers to employment, but none of the other interventions we reviewed took timing of disability onset into consideration.
While over recent decades there has been a paradigm shift in the way disability rights are treated, with policy-makers now focusing on how to make society more inclusive of people with disabilities, this is not reflected in the review. First, the interventions we found are predominantly individual-focused, with only the CBR programmes attempting to tackle the environment that leads to the disadvantage that people with disabilities experience. Second, we did not identify any disability inclusive mainstream policy, programmes or services, which may suggest that NGOs and other funders are not yet supporting this approach to disability inclusion in LMICs and/or such efforts have yet to be subject to impact assessment. Also, existing impact evaluations are skewed towards certain types of interventions, while evaluation of other types has lagged. Therefore, they cannot be generalised to the population of programmes in existence. As of April 2011, 99 of the 147 signatories had ratified the Convention on the Rights of Persons with Disabilities, and many LMICs now have anti-discrimination and other disability-specific laws. In spite of this, the review identified no evaluations of regulations, legislation or policy frameworks. According to the WHO, CBR is currently implemented in over 90 countries throughout the world to address the needs of people with disabilities and their family members. Yet, despite ‘livelihood’ being one of the five strands in the systematic framework developed by the WHO for organising and analysing CBR activities, only four impact evaluations have measured employment outcomes over a twenty-year period. Although CBR often involves a component of raising public awareness of disability issues, no separate impact evaluations of awareness campaigns were identified. Our review reaffirms the findings of Borg et al. (2011) that the scarce literature on assistive devices and technology is dominated by product-oriented research on leg prostheses and manual wheelchairs. There is a particular lack of evidence on interventions to increase hearing or vision capacities, including hearing aids, visual aids, and specialised computer software and hardware. Further gaps in the evidence base include impact assessments of accommodations in the workplace, such as installation of ramps or flexible working practices, and financial grants and microfinance programmes.
There are numerous methodological inconsistencies and weaknesses in the current evidence base. On the whole, the designs and size of the included studies are inadequate for determining causal effects. Few studies addressed potential sources of bias, and even basic tests of statistical significance were often not reported. The majority based their conclusions on before-and-after assessments. Several studies used self-report data with only a few verifying retrospective information in records. Most of the studies were relatively small-scale. Where impact assessments were carried out on a sample of programme beneficiaries, convenience sampling was often used.
Our assessment shows that the current evidence base to support programmes aiming at increased participation of people with disabilities in the labour market is scarce. There is some limited evidence to suggest that therapeutic interventions, such as cataract surgery, and occupational rehabilitation programmes can be effective in increasing rates of employment, self-employment and higher income for people with disabilities. Likewise, the use of assistive devices, such as prostheses and manual wheelchairs may lead to higher chances of work (re)entry and higher income. Therapeutic techniques and social skills programmes may increase disabled people's motivation to work and improve their professional social skills. Community-based rehabilitation programmes may improve employment participation, while disabled people's loan schemes may positively affect employment, self-employment, working hours and incomes. However, while consistency in the direction of effects provides some evidence of an improvement in labour market outcomes, this needs to be treated with extreme caution. The overall paucity of research in this area, together with specific gaps and methodological limitations, mean that drawing strong inferences from the findings of this body of literature is not recommended.
A further objective was to explore the extent to which there are important differences in the results of these studies, and likely explanatory factors for such differences. Ideally we want to be able to discuss the effectiveness of an intervention within specific target groups, defined by age, gender, type and severity of impairment and so forth. In addition, we set out to explore participants' observations, experiences and views about why the intervention they received had or had not worked for them. However, as our review of the literature identified only a limited number of low quality studies addressing these questions, this limited any meaningful synthesis of study findings.
This is an area of study where rigorous impact evaluation does not exist, and even those using less credible methodologies are scarce. Our findings support earlier claims about the dearth of literature examining the impacts of labour market supports for people with disabilities in LMICs (Andrysek, 2010; Borg et al., 2011; Iemmi et al., 2012; Mitra & Sambamoorthi, 2006; Velema et al., 2008). Where improvements in outcomes were observed in individual studies it was extremely difficult to assess the extent to which these were directly attributable to the interventions. We cannot say with any certainly whether persons with disabilities can improve their labour market situation as a result of the interventions reviewed, nor who is most likely to benefit and who will not. The overall conclusion of the review is that the existing body of evidence about the impact of labour markets supports for people with disabilities is inconclusive.
7.3 STRENGTHS AND LIMITATIONS OF THIS REVIEW
A major strength of this study is its application of systematic review principles to improve upon prior work. The involvement of representatives from Sightsavers at all stages of the review process was invaluable for ensuring the relevance of the review. A major limitation is the scarcity of high quality research evidence to inform decision-making in this area.
This systematic review had additional limitations, as indeed any broad review of complex interventions is likely to have. Although steps were taken to minimise publication and study selection bias, there may be studies missing from the review.
First, although eligibility was not limited to studies written in English, language bias was not fully avoided, as the literature search involved searching only a limited range of non-English language databases and we did not include search terms in other languages. Second, the very broad scope of this review may have resulted in missing studies. Broadening review scope has advantages in allowing policymakers to select the most effective intervention relative to their context, and enabling generalisability to be assessed across a wider range of contexts, study populations and behaviours (Shadish et al., 2002; Waddington et al., 2012). However, broad reviews place demands on, and may even compromise, the search process. In this review, we did not set the question around a single type of intervention, nor impairment category, and so a large number of terms was required for the search query. Particular problems arose over the term ‘disabled’ and the diverse nature of health conditions leading to disability. It was challenging employing broad search terms because the number of references returned became unmanageable. The searches were both time-consuming and cumbersome to manage, and eventually it was necessary to request support from ProQuest staff as the searches timed out before they were fully executed. Despite our best efforts, it is possible that, due to the review's broad scope, the full coverage of relevant search terms were not identified and/or used, leading to missed studies.
7.4 IMPLICATIONS
The overarching aim of this review was to provide an evidence base for policy development. Given the limitations of the existing evidence base, however, drawing out the implications for policy-makers and other stakeholders is challenging. The available evidence comes from a small number of studies implemented in a few settings, at a small scale, over a relatively short period of time and from evaluations using methods open to a high degree of bias. Based on this evidence we cannot definitively conclude what interventions are likely to work, for whom, and where. There is an urgent need for investment in high quality impact evaluations of interventions to support participation of people with disabilities in the labour market in low- and middle-income countries.
The overall paucity of research in this area, together with specific gaps and methodological limitations, affirm the need for strengthening the evidence base. There is an urgent need to invest in research which rigorously evaluates a broader range of interventions, in particular specific legislations and policies, a spectrum of educational and skills development programmes, and employer sensitisation and awareness raising campaigns. There is a need for studies from a broader range of countries and settings and targeting different sub-groups of people with disabilities, in particular adults with hearing impairments. Reviews of the effectiveness of interventions are available for high-income countries and more analytical work is needed to examine both the extent to which these interventions are transferrable to LMICs and the characteristics of the labour markets that determine the differences between high-income countries and LMICs. There is a need to develop scales to measure the effects that are appropriate for LMICs and for longer-term outcome measurements. Future analyses should include issues of impairment type and severity, otherwise they risk under-estimating the complexity of factors involved. Acting on these suggestions will require the various stakeholders, including national governments, academic institutions, development donors, and implementing NGOs, taking a critical look at the opportunities and barriers affecting research production and dissemination in this area.
8 Acknowledgments
The authors would like to acknowledge Sightsavers International and the International Initiative for Impact Evaluation (3ie) for providing financial support for this study. Special thanks are due to Sandra Jo Wilson, editor of the Education Coordination Group (ECG), for her guidance throughout the project. We would also like to thank the anonymous reviewers for their valuable comments on earlier drafts of the reports. The funding agency informed the scope and development of the review; however, the opinions expressed in this report are those of the authors and do not necessarily reflect those of the funding agency.
Footnotes
10 Appendix I: Additional Tables
1
Each year, the World Bank revises the classification of the world's economies based on estimates of gross national income (GNI) per capita for the previous year. For the fiscal year starting 1 July 2013, these are: low income ($1,035 or less), middle income ($1,036 to $12,615).
2
As such, the terms ‘impairment’ and ‘health condition’ are often used interchangeably (a practice adopted in this review).
3
In the study protocol HIV/AIDS was included in our definition. However, we subsequently took the decision that this group have different rehabilitation needs, and therefore studies evaluating intervention to improve the labour market situation of persons living with HIV/AIDS are not included in this review.
4
As there is no consistent terminology used for different types of designs used for evaluating the effects of interventions, and the labels in common use are interpreted in different ways, the main focus here is on describing the key differences between designs. It is recognised that not everyone classifies the less rigorous designs as quasi-experimental.
5
For example, our search includes the LILACS database, an underused source of trials that indexes journals mainly from Latin American and Caribbean.
6
Zimbabwe (Lagerkvist, 1992a) and Philippines (Lagerkvist, 1992b)
7
Biggeri et al. (2012) amalgamated data from two related programmes. Therefore, we treat this as a single intervention in this review.
8
Contains two studies, and referred to as Lagerkvist (1992a) and (1992b) in the text.