
Abstract
This Campbell systematic review reports the effects of psychosocial interventions on employment outcomes for cancer survivors. The review summarises findings from 12 studies covering 2,151 cancer survivors.
Interventions include education, training, psychological support, environmental adjustments or accommodations, flexible or job-sharing work conditions, or job search and placement assistance. Most interventions include more than one component to address barriers to employment.
Abstract
BACKGROUND
In the United States, an estimated 1.5 million people are diagnosed annually with some type of cancer (American Cancer Society, 2011). Work is an important stabilizing factor for cancer survivors (Arnold, 1999). De Boer and colleagues (2009) identified a rate of 33.8% unemployment among cancer survivors beyond the age of 18 compared to 15.2% among a healthy international control population. Greater awareness of the job-related and workplace issues that cancer survivors face can lead to more comprehensive rehabilitation plans and recovery (Centers for Disease Control, 2011; Nathan, Hayes-Lattin, Sisler, & Hudson, 2011). Although various recent interventions have been developed to address unemployment among cancer survivors, these have not yet been systematically evaluated.
OBJECTIVE
The objective of this systematic review is to examine experimental and quasi-experimental studies about interventions that (i) include one or more behavioral, psychological, educational, or vocational components, (ii) involve cancer survivors aged 18 years or older, and (iii) assess intervention outcomes on employment outcomes. The aims are both to describe the variety of interventions that have been studied using rigorous methods and to estimate intervention effects.
SEARCH STRATEGY
We used electronic search techniques of 27 computerized databases to conduct a comprehensive search. Keywords used were relevant terms from four categories: population, treatment, domain, and design. We identified grey literature through electronic searches of popular search engines, unpublished dissertations/theses, and cancer-related organizations and conferences. In addition, we searched reference lists from included individual studies for potential studies to consider. The dates of the last search for electronic databases and grey literature were November 2013 and October 2012, respectively.
SELECTION CRITERIA
We employed a two-stage process to determine inclusion or exclusion of studies: (1) title and abstract stage and (2) full text stage. Participants needed to be cancer survivors 18 years of age or older. Interventions were included if they measured gainful employment, return to work, wages, or hours worked as an outcome. Interventions were behavioral, psychological, educational, or vocational in nature, including workshops, training, or counseling targeted towards employment initiation, return-to-work, or decreasing absenteeism and use of work disability or sick leave. Interventions included an element apart from medical or physical treatment (e.g., exercise, surgery, pharmaceutical treatment). Studies with a research design of randomized controlled trial or quasi-experimental study were included.
DATA COLLECTION AND ANALYSIS
The combined electronic search, hand searches, and examination of the grey literature produced a total of 20,249 citations. Of these studies, a total of 70 citations were advanced for collection of a full text copy of the study when either one of the two independent reviewers agreed it appeared to meet the inclusion criteria. Twelve studies met the inclusion criteria.
The results of the studies were synthesized in a random-effects meta-analysis using odds ratio effect sizes.
RESULTS
We found 12 studies evaluating the effects of psychosocially-related interventions on the employment of cancer survivors (N = 2151). Our results provide promising evidence that the included interventions may improve employment status (OR = 1.71, 95% confidence interval (CI) = 1.26 to 2.32) for cancer survivors. For RCTs (k = 6), the weighted mean effect size for employment status was OR = 1.44 (CI = 0.99 to 2.09), favoring the intervention groups. The mean odds ratio of 1.44 translates to an employment rate of about 68% for intervention participants compared to a baseline 60% for comparison group participants. For QEDs (k = 6), the weighted mean effect size for employment status was OR = 2.18 (CI = 1.32 to 3.60), also favoring the intervention groups. The mean odds ratio of 2.18 for the quasi-experimental studies translates to an employment rate of about 77% for intervention participants, compared to the baseline rate of 60% for the comparison group participants. Although the mean effect size from QEDs was larger than that from the RCTs, there is no significant difference between the two types of experimental designs (p = 0.19).
There was no evidence of an effect on the number of hours worked (OR = 0.89, CI = 0.22 to 1.52) or number of sick leave days (OR = 1.18, CI = 0.81 to 1.71). Overall, the assessment of the risk of bias was high, and conclusions about the effectiveness of the included interventions should be interpreted with caution.
AUTHORS' CONCLUSIONS
This review highlights the positive effect psychosocial interventions may have on employment outcomes for cancer survivors. However, the methodological shortcomings of the included studies overall makes it likely that there is bias in the results and too few studies to provide sufficiently strong evidence to recommend particular practices. This review brings attention to the need for additional rigorous studies in this area, in particular, randomized controlled trials with more detailed reporting of data and study design and methodology.
1 Background
In the United States, an estimated 1.5 million people are diagnosed annually with some type of cancer (American Cancer Society, 2011). Today, survivorship after diagnosis is higher than it has ever been: as of January 2008, about 11.9 million individuals in the United States had a history of a cancer diagnosis (Howlander et al., 2011). Drawing on more recent estimates from the working-age population in particular, there are over 7 million cancer survivors in the United States between the ages of 15 and 69 years, and the number is expected to grow (American Cancer Society, 2012). The issues affecting cancer survivorship are complex, particularly when one considers the impact of this disability on employment specifically. De Boer and colleagues (2009) identified a rate of 33.8% unemployment among cancer survivors beyond the age of 18 compared to 15.2% among a healthy international control population. Work is an important stabilizing factor for cancer survivors (Arnold, 1999). Greater awareness of the workplace issues that cancer survivors face can lead to more comprehensive rehabilitation plans and recovery (Centers for Disease Control, 2011; Nathan, Hanes-Lattin, Sisler, & Hudson, 2011).
Cancer survivors face difficulties with activities of daily living, including employment, not only while their cancer is active, but for years afterwards. Mehnert, de Boer, and Feuerstein (2013) have developed a conceptual framework that summarizes various challenges to employment cancer survivors face. They divide these into three domains: individual and interpersonal factors; the short-, long-, and late-effects of cancer and treatments; and the work environment. The individual and interpersonal factors are described as “sociodemographics, socioeconomic status, educational professional training, life stage, personality, coping strategies, problem-solving skills, motivation, meaning of work, and social supports” (Mehnert et al., 2013, p. 2154). These factors affect the employment outcomes for any individual in the workplace, but cancer survivors have to rely more heavily on these various forms of individual-level resources to sustain employment. Blinder and colleagues (2011) noted that such challenges are even more difficult to overcome for people in low-income occupations.
Secondly, the effects of cancer specifically, whether short-, long-, or late-term, can be in the realm of “health status/comorbidity, continuity of care, quality of life, functional impairments, symptom burden, emotional and social well-being, change in identity and role functioning, social reintegration” (Mehnert et al., 2013, p. 2154). These barriers to employment all relate, in direct or indirect ways, to a person's health, both mental and physical, and well-being, and obviously can dramatically affect an individual's participation in the work setting. For example, treatment side effects such as alopecia (hair loss; Münstedt, Manthey, Sachsse, & Vahrson, 1997) or ‘chemo brain’ (cognitive functioning deficits; Staat & Segatore, 2007) may affect interpersonal relationships or workplace functioning.
A third domain constitutes work environment traits that can influence survivors' work outcomes. These traits range from the conditions, demands, and overall climate of the work setting to the accommodation and flexibility of the employer (Mehnert et al., 2013). Cancer symptoms and treatment can necessitate changes in work conditions, such as reducing demands or changing work hours to accommodate treatment. In 2008, Title I of the Americans with Disabilities Act (ADA) was amended to include “major bodily functions” that interfere with daily living in the definition of disability, underscoring the disability classification and associated job protections to cancer survivors that the law had always offered to them. Analysis of claims filed show that cancer survivors more often have issues with job termination and terms of employment than employees with other impairments (Feuerstein, Luff, Harrington, & Olsen, 2007).
1.1 THE INTERVENTION
This review focused on identifying interventions with behavioral, psychological, educational, or vocational content that aim to facilitate cancer survivors' employment outcomes, including a) employment status, b) return-to-work, c) absenteeism, and d) time spent on work disability or sick leave. Interventions of interest included education, training, psychological support, environmental adjustments or accommodations, flexible or job-sharing work conditions, or job search and placement assistance. We were also interested in interventions that did not target employment specifically, but included it as a related outcome among those measured. These studies give insight into what practices might be adapted and included in new interventions for the explicit purposes of promoting employment.
1.1.1 How the Intervention Might Work
It was anticipated that the literature would identify a broad set of interventions with behavioral, psychological, educational, or vocational components. Pathways of effects to the outcomes were expected to vary widely along with the setting, training of the facilitator, and whether delivered to individuals or groups by individuals or teams.
Approaches to addressing strain on individual and interpersonal resources---one of the domains Mehnert, de Boer, and Feuerstein (2013) identified---would include vocational components. Survivors are four times more likely to be employed when they receive employment assistance and support, such as job-hunting services or on-the-job training (Strauser et al., 2010). Basic components of interventions that United States-based vocational rehabilitation (VR) agencies use generally include diagnosis and vocational assessment, counseling, training, provision of accommodations, job placement, and post-employment services (Waddell, Burton, & Kendall, 2008). This review was designed to include studies of interventions that measured outcomes related to participants' search for new jobs but often dealt with issues of job retention. In an example of how VR, as a multi-component intervention, can be tailored to meet the needs of these two groups, Chiu and colleagues (2013) studied recipients of state VR services who had cancer, and their chief finding was that those who were employed used different VR services than those who were not employed: “While some services were indeed used by a large portion of all clients such as assessment, diagnosis and treatment of impairments and VR counseling and guidance, which were major needs by over half applicants in the current study---other services were contingent on the clients' employment status” (Chiu et al., 2013, p. 7). Employed clients needed services to support work adjustment and accommodation, such as diagnosis, treatment, “rehabilitation technology, disability-related augmentative skills training, technical assistance services, on-the-job supports and basic academic, remedial or literacy training” (Chiu et al., 2013, p. 7). Especially because there were significantly lower educational levels compared to the employed group, unemployed clients needed a wide variety of vocational rehabilitation services such as the search and placement process to obtain a job, and then job readiness training. A pilot randomized controlled trial of VR services among women with breast cancer following surgery is currently underway in the United Kingdom, though in these countries VR is more heavily oriented toward interventions that focus on health (Kyle et al., 2011) and psychological counseling.
Approaches to addressing health and well-being include components targeting behavioral change and/or alleviation of physical symptoms or emotional issues, with a focus on symptom reduction and improvement in related quality of life. A review of psycho-social interventions in oncology noted that treatment options for cancer patients vary due to the diversity among types of cancer and their treatment options, but that they included “counseling, cognitive-behavioral methods, information and educational treatments and complementary therapies” (Whatley & Milne, 1998, p. 1). Similar to the studies located in a meta-analysis of psychosocial interventions with adult cancer survivors conducted by Meyer and Mark (1995), these intervention studies did not measure employment. Another intervention targeting barriers in this domain is a tool currently being developed and evaluated at the University of Wisconsin-Madison called “Work ability Improvement through Symptom management and Ergonomic strategies” (WISE). The tool is a website that guides breast cancer survivors through questions that help determine how to address on-going symptoms, particularly shoulder pain, and improve ergonomics at their offices (Garrett, 2012; National Rehabilitation Information Center, 2012, p. I-37). Educational interventions also seek to overcome barriers in this domain, such as a group educational and discussion group intervention for men with prostate cancer (Lepore, Helgeson, Eton, & Schulz, 2003). Another example is the cancer-related fatigue intervention trial CAN-FIT, that sought to reduce severity of fatigue among survivors who have had radiotherapy by sharing a handbook, presentations, a goal-setting sheet, and progress diary that aimed to increase participants' knowledge about radiotherapy side effects and strategies to reduce fatigue (Purcell, Fleming, Burmeister, Bennett, & Haines, 2011).
Approaches to addressing barriers to employment that express themselves in work environments are primarily educational. Several organizations, for example including some that belong to the United States-based National Cancer Legal Services Network (www.nclsn.org), provide training and information to both employers and survivors. Publications and other information on various Web sites offer information about cancer-related employment issues and how to address them through greater awareness of cancer survivors' needs for accommodation. Examples of such informational resources are published by Cancer and Careers in the “At Work” section of their web site (see www.cancerandcareers.org/en/at-work) and Hoffman (2012). The American Cancer Society also has an employer-oriented publication (American Cancer Society, 2014). While increasingly common, to date the efficacy of this information provision has not been studied formally.
Given that the typical intervention includes more than one component targeting barriers to employment that straddle the domains outlined above, it is not surprising that a common approach to return-to-work interventions for cancer survivors (a) emphasizes the involvement of multidisciplinary teams (Fleischman, Retkin, Brandfield, & Braun, 2006; Retkin, Antoniadis, Pepitone, & Duval, 2013; Vonk Noordegraff et al., 2012) or (b) at least seeks to improve communication among employers, survivors, and medical providers (Nieuwenhuijsen, Bos-Ransdorp, Uitterhoeve, Sprangers, & Verbeek, 2006; Tamminga, de Boer, Verbeek, & Frings-Dresen, 2010). Many interventions seek to meet a diverse set of survivors' needs, using a variety of intersecting mechanisms.
1.2 CONTRIBUTION OF THE REVIEW
According to one systematic review of employment and work-related issues in cancer survivors, employer accommodation, flexible work, counseling, training and rehabilitation, educational levels, fewer physical symptoms, continuity of care, younger age, and male gender are associated with more positive work outcomes (Mehnert, 2011). However, little is known about how these factors relate to which interventions and how these might be most effective at helping cancer survivors to become employed. Gensby et al. (2012) led a systematic review of workplace disability management programs that focused on return-to-work, but consistent with Tamminga and colleagues' (2010) review, found none that focused on cancer. In addition, there are few published instruments relevant to evaluating interventions related to cancer survivorship and work (Ladehoff, Sturm, & Mehnert, 2013).
In 2011, de Boer and colleagues conducted a Cochrane review of medical, psychological, and physical interventions that targeted return-to-work outcomes with cancer survivors. Although they found a number of studies of interventions that enhanced return-to-work, none of the included studies were interventions that specifically targeted vocational rehabilitation, such as job-related skills, interviewing, etc. A contribution of our review is the inclusion of new literature after the de Boer (2011) review was published (e.g., Tamminga et al. 2013) and additional employment outcomes such as number of hours worked.
Understanding the impact on employment of interventions that include behavioral, psychological, educational, and/or vocational content, as compared to medical, pharmaceutical, or surgical treatments that a narrower range of providers are certified to deliver, could promote cancer survivors' employment and yield greater rewards for employees and employers alike (Centers for Disease Control, 2011; Kyle et al., 2011). Including interventions that measure, but do not necessarily target, employment will allow for the findings of this review to be applied to a broader set of theories of change. For example, Purcell et al. (2011) did not target employment as an outcome but did report employment status allowing the authors to include this study. Researchers designing impact evaluations of new interventions might choose to do longer-term follow-up, assume that the intervention intensity would need to be increased, or measure whether an intervention targeting an assumed barrier might inadvertently increase awareness of it and so contribute to its consequences (i.e., discussing fatigue might make people more concerned about it and more likely to avoid taxing their energies by employment until they feel energetic enough to return-to-work). This review demonstrates that employment outcomes can be included in data collection, beneficially allowing further understanding of the differences in successful employment outcomes across various disability conditions that differ by severity and range of limitations.
This review conducted a broader search that includes more databases and expanded employment-related outcomes (such as number of hours worked and wages) than those done on similar topics previously.
2 Objective
The objective of this review is to examine experimental and quasi-experimental studies about interventions that (i) include one or more behavioral, psychological, educational, or vocational components, (ii) involve cancer survivors aged 18 years or older, and (iii) assess intervention effects on employment outcomes. The aims are both to describe the variety of interventions that have been studied using rigorous methods and to estimate intervention effects.
3 Methods
3.1 TITLE REGISTRATION AND REVIEW PROTOCOL
The title for this systematic review was approved by the Campbell Collaboration on 20 October 2011. The review protocol was approved on 11 November 2013 (Fong, Murphy, Westbrook, & Markle, 2013). The title registration and protocol are available at:
Deviations from the protocol are described in the following sections and highlighted here: We expanded the inclusion criteria to encompass interventions not focused on developing employment-specific skills but contained behavioral, psychological, or social components necessary for gainful employment; We eliminated planned moderator/subgroup analyses due to the small number of included studies; and We modified the effect size metric to the odds ratio for all outcomes.
3.2 CRITERIA FOR INCLUSION AND EXCLUSION OF STUDIES IN THE REVIEW
3.2.1 Participants
The participant samples were required to be (a) adults aged 18 years or older and (b) cancer survivors (i.e., had a past or present cancer diagnosis which occurred while the individual was aged 18 years or older). Studies of populations that included, but were not limited to, cancer survivors were not excluded if the employment outcomes of the participants who were cancer survivors were reported independently from those of other participants. Studies of adults who were survivors of pediatric cancer were excluded, since these individuals may have participated in interventions as children, such as high school transition-to-work programs to which adult-onset populations could not have participated in, but which could affect employment outcomes. Study participants eligible for inclusion were individuals diagnosed with any type of cancer. Study participants with co-morbidities were not excluded.
Participants not employed at the time of the study intervention were the focus of this review as return-to-work and gainful employment were primary outcomes; however, employment maintenance is an important concern and individuals who were employed prior to an intervention study were not excluded in this review. Reviewers did not exclude studies in which the participant pool included both participants who had an employment history and those who did not.
3.2.2 Intervention
Included studies addressed the effectiveness of a behavioral, psychological, educational, or vocational intervention or component of an intervention for cancer survivors that facilitated their employment outcomes, including employment initiation, return-to-work, or decreasing absenteeism and use of work disability or sick leave.
Eligible interventions addressed social, behavioral, cognitive, or specific employment skills related to the acquisition and maintenance of employment among the study participants. Interventions could involve relatively specific and structured experiences of VR designed to support employment placement, for example, providing guidance in completion of applications, résumés, and engaging in interviews; shaping of work skills and appropriate employment setting social skills; or teaching of appropriate work-related communication skills. Furthermore, interventions could address more general psychological or behavioral aspects of functioning that can facilitate employment, such as coping skills. Examples are behavioral treatments such as self-care behaviors to reduce fatigue; behavioral therapies that help survivors cope with their scars or other issues associated post-surgery; psychological interventions through individual or telephone counseling that assist with adjusting to a cancer diagnosis; lecture-based educational interventions on cancer survivorship; and, vocational interventions through supported employment from a VR agency that provide job supports, interview training, etc.
Interventions could be multidisciplinary, incorporating physical and medical treatment and educational training. For example, an intervention could include multiple components such as a vocational training workshop, exercise, and yoga.
Interventions to be included in this review were often divergent in their scope and area of focus, e.g., including components that promoted psychological, physical, and work-oriented outcomes because of the particular needs of the subject group. This was expected due to the wide variation in health-related outcomes related to improving cancer survivors' overall well-being. To accommodate this need and appropriate variation in interventions, studies for inclusion addressed psychological, behavioral, medical and/or skill-oriented interventions with an employment outcome. Therefore, if there were two studies that evaluated the impact of VR, one with an employment outcome and the other with a quality of life outcome, only the first was included, and the latter excluded. Interventions must have included an element apart from medical or physical treatment (e.g., exercise, surgery, pharmaceutical treatment). One reason for excluding interventions with solely medical components is our focus on VR agencies as our primary audience and, as a result, focused on programs that rehabilitation organizations can feasibly implement. Interventions of any length or duration were included provided adequate description was given.
3.2.3 Research Design
Included studies used a randomized controlled trial (RCT) design, quasi-experimental equivalent and non-equivalent comparison design, or quasi-experimental design that employed regression discontinuity. Quasi-experimental designs with equivalent groups formed by matching or equating, or non-equivalent groups without matching or equating, involved, for example, comparing the employment rate of a treatment group compared with the employment rate of a general population of cancer survivors that did not receive the intervention.
3.2.4 Outcome Measures
Eligible studies provided evidence for the effect of the intervention on employment status and/or related outcomes such as disability onset; of time out-of-work (i.e., number of leave days taken, including sick, disability, or vacation); and/or differences in rates of employment between the intervention and comparison groups. Various other measures were used to estimate the rate of employment such as wage-earning or hours worked. These employment-related outcomes are commonly studied in the return-to-work literature and provide a more fine-grained understanding of the impact of cancer on employment (Murphy, Markle, Nguyen, & Wilkinson, 2013).
Consistent with many aspects of the definition that United States federal agencies such as the Bureau of Labor Statistics and United States Census use, this review considered study participants to be ‘employed’ if they have done at least one hour of work per week. This job could be as a paid employee or “in their own business, profession, or on their own farm.” Also considered ‘employed’ are those who were not working but who “had jobs or businesses from which they were temporarily absent because of vacation, illness, bad weather, childcare problems, maternity or paternity leave, labor-management dispute, job training, or other family or personal reasons, whether or not they were paid for the time off or were seeking other jobs” (Bureau of Labor Statistics, 2008). Because this definition includes a rather attainable threshold for “gainful” employment, the included studies operationalized employment in this regard.
3.2.5 Publication Status
Published and unpublished studies were included in the evidence pool.
3.2.6 Country of Origin and Language of Publication
Studies that were conducted in any country were eligible. We did not exclude studies reported in languages other than English, but we did not specifically search for non-English literature; however, we did search selected international databases. Non-English language studies that were retrieved or reviewed required the reviewers to obtain translation assistance from native speakers (e.g., Bottcher, 2013).
3.3 SEARCH STRATEGY FOR IDENTIFICATION OF RELEVANT STUDIES
The search strategy used for identification of relevant studies is described below. All databases search engines were last searched on November 2013. Conference programs and organizations were last searched on October 2012.
3.3.1 Electronic Searches
Studies were identified using electronic search techniques of 27 computerized databases (last search occurred in November 2013). We consulted database thesauri, where they were available, to assure that the universe of appropriate synonyms had been included in the intervention and outcome search term categories. Search terms and search strategies were modified to fit individual databases.
Databases searched included:
Academic One File Academic Search Complete Academic Source Complete Business Source Complete CINAHL Plus with Full Text CIRRIE (Center for International Rehabilitation Research Information and Exchange Database) Cochrane Central Registry of Controlled Trials Ed Line and Electronic Texts in Education and Training Education Full Text ERIC Professional Development Collection ProQuest ProQuest Dissertations & Theses PsycINFO Psychology and Behavioral Sciences Collection PubMed Science and Technology Collection Sociological Abstracts Web of Science World Cat [for monographs] MEDLINE EMBASE OSH-ROM (Occupational Safety and Health) Abstracts of Review of Effectiveness (DARE)
3.3.2 Search Terms
We included literature published between 1973 through August 2013. The rationale for the start date was that, during 1973, the United States Congress approved the Rehabilitation Services Act, catalyzing the development of VR programs and efforts to accommodate people with disabilities in the workplace. There has been some attention to occupational health internationally for over a century; for example, the International Commission on Occupation Health was founded in 1906. This date was well before scholarly work on disability management began to develop. For example, the first conference of the International Disability Management Standards Council was not held until 2002. Similarly, the field of cancer survivorship studies is relatively recent because the population of cancer survivors who had employment-related issues was small until medical advances of the late 20th century (Hewitt, Greenfield, & Stovall, 2006).
The search of databases used four sets of keywords that pertain to the population, intervention, outcomes, and study design. Search strings' keywords were customized to the particular thesaurus of each database. Keywords were connected with “and”/“or” when searching titles and abstracts. Search terms were truncated to include variations in word endings, spellings, and database indices.
The following is an example of the types of terms. Terms from the four categories were connected with “or” within each category and by “and” between categories.
Population: cancer, cancer survivor, neoplasm, leukemia
Intervention: intervention, model, program, practice, training, vocational rehabilitation, accommodation, occupational therapy
Outcomes: employment, return-to-work, job, wages, salary [Note: the terms ‘wages' and ‘salary’ are included since they might help to locate employment-related studies, but there are not intended to be included as measure of intervention effect.]
Study design: experiment, control group, random, effect
A sample search strategy is:
((cancer* OR “cancer survivor” OR neoplasm* OR leukemia*) AND (interven* OR model* OR program* OR practice* OR train* OR “vocational rehabilitation” OR accommodat* OR “occupational therapy”) AND (employ* OR “return-to-work” OR job OR wages OR salar*) AND (experiment* OR “control group*” OR random OR effect*))
For more information on the search strategy, see Appendix A: Documentation of Search Strategies for the Systematic Review.
3.3.3 International Contacts
Our efforts to find studies from outside the United States included searching in several non-United States and international databases. This yielded studies that were reviewed in Stage 1 of the title/abstract review procedures as well as one included study (Granstam-Bjorneklett et al., 2013).
3.3.4 Grey Literature
Grey literature that is identified through electronic searches was submitted to the same inclusion criteria as other studies. A time range for these types of studies was not specified in order to maximize consideration of all relevant grey literature. Reference lists from other systematic reviews and individual studies were searched for potential studies to consider for inclusion.
We inquired with two prominent researchers in the field of vocational rehabilitation of cancer survivors about any unpublished reports or completed research activity that may have a pending report. We searched the reference lists of identified articles (ancestry search), which might have been helpful, for example, in locating dissertations and theses not identified by our database searches. Also, a search of popular search engines was conducted. Using the search strategy described earlier, we used Google, Google Scholar, and Yahoo! to uncover any relevant web materials or unpublished studies not accessible through electronic databases. In addition, searching ProQuest Dissertations and Theses allowed for opportunities to uncover relevant unpublished doctoral dissertations and masters theses.
3.3.5 Cross-referencing of Bibliographies
The references in relevant journal articles, systematic reviews, and other reports of research results were reviewed for new additions to our study pool.
3.3.6 Conference Programs and Relevant Associations
Recent conference programs and conference syntheses from relevant associations and conferences were used to identify unpublished studies eligible for review inclusion. Programs and organizational resources were searched in 2012, using the most recent conference programs or those available online. Professional organizations/events that were reviewed included: American Cancer Society American Institute for Cancer Research American Public Health Association The Centers for Disease and Control and Prevention Dana-Farber Cancer Institute Livestrong Macmillan Cancer Support The National Cancer Institute National Cancer Research Institute National Cancer Legal Services Network National Coalition for Cancer Survivorship Organisation of European Cancer Institutes The University of Texas MD Anderson Cancer Center Work Disability Prevention and Integration The International Disability Management Standards Council
3.4 CODING PROCEDURES AND CATEGORIES
Studies were screened for inclusion/exclusion decisions at two stages, Stage 1: citation and abstract and Stage 2: full-text. The same two coders served as independent reviewers at both stages, reaching consensus on any coding discrepancies. A third party was not needed to resolve any coding difference.
3.4.1 Citation and Abstract Stage
At Stage 1, the decision for advancing the retrieved citations and abstracts to the full text stage retrieval was made independently two reviewers, discussing discrepancies to reach consensus. Decisions were based on meeting two criteria from the following questions (items a, b, c, or d) or a designation by a reviewer of ‘unsure’ (item e): Are the participants identified, described, and defined as cancer survivors? Are the participants adults who are employed or seeking employment? Is this abstract/citation about an intervention with behavioral, educational, or vocational content? Does the study report employment status or relevant time-to-event data? Unsure of meeting inclusion criteria?
3.4.2 Full-Text Level
At the Full-Text Stage 2 level, full texts of all citations advanced from Stage 1 were obtained and coded for an inclusion/exclusion decision. The decision for advancing the retrieved full-text studies to an inclusion status was made by two reviewers for each study, independently evaluating each study. An inclusion decision for advancement to the coding stage of the process required that a study met all the criteria presented earlier. Inter-rater reliability was established prior to initiating coding activities, minimizing coding disagreements. Coders demonstrated agreement in an initial set of 2 studies at a 95% rate of agreement. When differences did arise, resolution occurred through discussion and agreement of the two reviewers.
At the Full-Text Stage 2 level, the two reviewers also recorded all excluded studies and the reason for exclusion independently. For more information see Appendix B: Reasons Stage 2 Studies were Excluded from the Systematic Review.
When multiple studies used the same sample or outcome data, the study providing the most complete information focusing on our desired intervention outcome was selected for inclusion.
Other data for extraction and coding from the primary studies included: publication source, subject characteristics, sample source, employment setting, intervention characteristics, type of employment, and outcome measurement. See Appendix C for the coding form.
3.5 ASSESSMENT OF METHODOLOGICAL QUALITY
Included studies were coded by two independent reviewers for methodological quality on dimensions that included: Design type RCT Individual Randomized Design RCT Group Randomized Design Quasi-Experiment: Equivalent Comparison Design (individuals) Quasi-Experiment: Equivalent Comparison Design (groups) Quasi-Experiment: Nonequivalent Comparison Design (individuals) Quasi-Experiment: Nonequivalent Comparison Design (groups) Quasi-Experiment: Regression Discontinuity Unit of assignment (e.g., individual vs. group/class) Unit of analysis (e.g., Intention to Treat, Test only, Treated) Attrition from pretest to posttest Fidelity of implementation (e.g., following replicable program of intervention) Blinding of assessors/interventionists
In addition, an evaluation of the potential risk of bias of all included studies was conducted using procedures described by Higgins & Green (2011). The five sources of potential bias include (1) selection bias, (2) performance bias, (3) detection bias, (4) attrition bias, and (5) reporting bias. Potential selection bias was assessed via examination of a study's generation of a randomized sequence or concealment of allocations before assignment. Potential performance and detection biases were examined by recording the blinding of participants, personnel, and outcome measurement. Potential attrition bias resulting from incomplete outcome data was assessed by recording attrition, exclusions, reasons for exclusions, and any re-inclusions. Lastly, we assessed potential reporting bias, i.e., whether selective outcomes were reported.
3.6 CALCULATING EFFECT SIZES
We used Comprehensive Meta-analysis software (Borenstein, Hedges, Higgins, & Rothstein, 2005) for all statistical calculations. Only studies using an experimental or quasi-experimental design were included in the data synthesis.
3.6.1 Within-study Synthesis
The measures of effect were the rate of employment, mean number of leave days taken since disability onset, and mean number of hours worked. If these were not reported directly, they were calculated from the outcomes that were reported.
We employed a shifting unit of analysis approach (Cooper, 1998), which involves coding as many effect sizes from each study as exist as a result of variations in characteristics of the manipulation, sample, setting, and outcomes within the study. However, when calculating the overall effect size, the multiple effect sizes were averaged to create a single effect size for each study. The shifting unit of analysis approach maximizes the amount of data from each study without violating the assumption of independent data points.
3.6.2 Across-study Synthesis
The synthesis of effect sizes across conceptually similar constructs were conducted in order to determine the magnitude of the effect when combining similar outcome effects from several studies. However, all cross study synthesis utilized only one comparison effect size per study for any summary synthesis so that no single study outcome is represented more than one time in any analysis. For any group study (e.g., RCT, QED), any Cohen's d effect sizes or means and standard deviations were converted to a log odds ratio effect size so that all effect sizes for all group studies will be presented in the same metric. The following conversion formula was used:
The log odds ratio was synthesized in the final analysis (with results translated back into odd ratio for interpretability). We used a random-effects inverse variance weighting method to synthesize the effect sizes. Confidence intervals were calculated and reported as well.
The magnitude of the intervention effect was calculated using the commonly accepted statistical formulae and dedicated programs available.
3.6.3 Heterogeneity Analysis
For the analysis of dichotomous and continuous data, an assessment of heterogeneity was conducted using τ2 (tested against the null hypothesis of τ2 = 0) and I2 for ease of interpretability (see Higgins, Thompson, Deeks, & Altman, 2003). It is suggested that 50% is a moderate level of heterogeneity. We used a random effects model for heterogeneity analysis.
3.6.4 Sensitivity Analysis
A sensitivity analysis was conducted to assess the impact of a single study on the magnitude of an overall observed effect size. The sensitivity analysis was also to be conducted for the impact of moderating variables (e.g., attrition, type of treatment, missing data, sample size, study design). However, due to lack of data and reporting among the included studies, only study design was tested as a moderator.
3.6.5 Publication Bias
Publication bias was not assessed for published vs. unpublished included studies because there were no unpublished studies in this synthesis. However, we provide a funnel plot to assess the potential for small study bias (see Figure 4.1 and 4.2).
3.6.6 Incomplete Reporting of Study Data
For studies reporting incomplete outcome data (k = 3), we first contacted the senior author of the study and requested the missing information to include in the analysis. Study authors did not respond to our inquiries, so studies with incomplete data where imputation was not possible were excluded.
3.6.7 Subgroup and Moderator Analyses
Subgroup/moderator analyses were not conducted, except for study design (due to interest to a priori theoretical considerations). Since the approach to the moderator analyses were dependent on the available data, our included study sample did not allow us to conduct moderator or subgroup analyses given the small number of studies (<10) available within any category of moderator.
3.7 TREATMENT OF QUALITATIVE RESEARCH
Qualitative research was not included in the analysis of the intervention research. However, these studies were reviewed for potential background information and trends related to this review.
4 Results
4.1 INFORMATION RETRIEVAL
The combined electronic, hand searches, and examination of the grey literature produced a total of 20,249 citations at Stage 1 Abstract/Citation after removing any duplicate citations. All citations were saved in an Endnote® library.
Of these citations, 70 were advanced for collection of a full text copy of the study (Full-Text Stage 2) if either one of the two independent reviewers agreed it appeared to meet the inclusion criteria.
Upon review of the full-text for each of the 70 studies, 8 randomized controlled trials and 4 quasi-experimental studies met all inclusion criteria. A list of the 58 excluded studies and the reasons for exclusion are presented in Appendix C. Studies that did not describe or assess an intervention (n = 22), did not present outcomes related to gainful employment (n = 23), used solely a medical intervention (n = 6), did not provide a comparison/control group (n = 7), or did not have participants with a cancer diagnosis were excluded. See Figure 1 for a flow diagram of the information retrieval.
4.2 DESCRIPTION OF THE STUDIES
This section narratively summarizes the included studies and their characteristics such as research design, sample sizes, setting and recruitment, participants, interventions, and outcomes. Note that the studies will be referred by the last name of the first author and the year of the publication. See Table 9.1 entitled “Characteristics of included studies and assessment of risk of bias” for more details at the end of the report.
4.2.1 Research Design
Eight of the 12 included studies were randomized controlled trials (Berglund, 1994; Granstam-Bjorneklett, 2013; Hubbard, 2013; Lepore, 2003; Maguire, 1983; Maunsell, 1996; Purcell, 2011; Tamminga, 2013). The other four were quasi-experimental studies, (Bottcher, 2013; Capone, 1980; Gordon, 1980; Sachs, 1980) which compared the treatment groups to a non-equivalent yet comparable comparison group. No discussion of matching procedures was included in the quasi-experimental study reports.
All experimental studies allocated conditions at the level of the individual participant. Two studies used a form of stratification in the randomization process. One study stratified by adjuvant chemotherapy (Granstam-Bjorneklett, 2013) and another by age and cancer type (Tamminga, 2013). No included studies used wait-listed control groups. Five included studies reported data at multiple follow-up points (Berglund, 1994; Capone, 1980; Granstam-Bjorneklett, 2013; Hubbard, 2013; Maunsell, 1996).
4.2.2 Sample Sizes
The number of unique participants from both treatment and comparison groups within the 12 included studies was 2151. The average sample size per study was 139.5 participants (Treatment: 65.7 participants; Comparison: 73.8 participants).
4.2.3 Setting and Recruitment
All included studies recruited their participants through a hospital or clinic. Recruitment often occurred through referrals after chemotherapy or surgery.
A hospital or clinic was typically the primary treatment setting. The few exceptions were studies that incorporated treatments at the hospital as well as the home such as phone interviews/consultations or home visitations (Lepore, 2003; Maunsell, 1996). Another study incorporated the home setting with a vocational rehabilitation agency (Hubbard, 2013). One study administered treatment at a resort (Granstam-Bjorneklett, 2013). One study did not specify the treatment setting in the research report (Purcell, 2011).
4.2.4 Participants
4.2.4.1 Cancer type and treatment history
All participants had a cancer diagnosis as per the inclusion criteria. Six studies included only participants with breast cancer (Granstam-Bjoneklett, 2013; Hubbard, 2013; Maguire, 1983; Maunsell, 1996; Sachs, 1980). Two other studies had samples with varying diagnoses, but mainly breast cancer (Berglund, 1994; Purcell, 2011; Tamminga, 2013). One study included only prostate cancer patients (Lepore, 2003), and another included only gynecological cancer patients (Capone, 1980). The remaining studies included participants with a variety of cancer diagnoses ranging from breast cancer, genital cancer, lymphoma, thyroid cancer, airways cancer, stomach cancer, melanoma, and lung cancer (Bottcher, 2013; Gordon, 1980) Almost all participants had surgery or other treatment in the included studies. One study included participants without any prior medical treatment (e.g. surgery, radiation) for their present condition (Gordon, 1980). One study did not report whether their participants were post-operative or post-treatment (Capone, 1980).
4.2.4.2 Age and ethnicity
All studies reported age of the participants except for two (Maguire, 1983; Sachs, 1980). As expected, the majority of studies had participants over the age of 50. The average age of participants for studies that specified age was 54.32 years. Ethnicity was only reported for a few studies (Capone, Gordon, Lepore, 2003; Purcell, 2011), which included participants who would be classified by the United States Census categories as “White.”
4.2.4.3 Education level and socioeconomic status
Few studies reported the education level or socioeconomic status of the participants. If they did so, they reported a relatively even distribution of educational levels and socioeconomic statuses among the participants.
4.2.5 Interventions
Interventions varied widely in program components and duration. Three of the included interventions consisted solely of an educational or training component on topics ranging from physical information such as cancer biology, how to control side effects, and future health concerns, coping and stress, and goal setting. (Berglund, 1994; Lepore, 2003; Purcell, 2011). One study incorporated follow-up phone calls to reinforce the information (Purcell, 2011). Other interventions consisted of a therapeutic or counseling component on issues related to emotional support, behavioral change, holistic self-concept, and information-processing (Capone, 1980; Maguire, 1983). Two interventions paired education and counseling interventions together (Gordon, 1980; Maunsell, 1996). Two interventions combined physical components with education or counseling-related components such as integrating informational sessions with relaxation, qi-gong, and “liberating dance” (Granstam-Bjorneklett, 2013) or combining information, exercise, discussion, and group therapy (Sachs, 1980). In a similar way, another study evaluated a case-management intervention that tailored individual plans to integrate both physical and counseling components (Hubbard, 2013). Only two interventions directly addressed return-to-work or job-related issues by establishing return-to-work plans for cancer survivors combined with informational sessions (Tamminga, 2013) or therapy on job-related issues with physical therapy (Bottcher, 2013). See Figure 2 for a checklist of intervention components across studies.
4.2.6 Outcomes
Employment status or return-to-work was the primary outcome of the review, assessed by 10 studies (Berglund, 1994; Bottcher, 2013; Capone, 1980; Gordon, 1980; Lepore, 2003; Maguire, 1983; Maunsell, 1996; Purcell, 2011; Sachs, 1980; Tamminga, 2013). Two of these studies also included the hours worked as a secondary outcome (Purcell, 2011; Maunsell, 1996). A related primary outcome was the amount of sick leave taken by the participants. Two studies only included sick leave (Hubbard, 2013; Granstam-Bjorneklett, 2013), and two studies included sick leave as well as employment status (Berglund, 1994; Tamminga, 2013).
4.3 RISK OF BIAS
The potential risk of bias of included studies was assessed by evaluating the following: (1) selection bias, (2) performance bias, (3) detection bias, (4) attrition bias, and (5) reporting bias. See Figure 3 for a summary of the risk of bias assessment across studies.
4.3.1 Selection bias
The majority of randomized studies had relatively low risk of selection bias due to specifying a method of generating an allocation sequence including the use of a biased coin design (Berglund, 1994), envelope (Granstam-Bjorneklett, 2013; Lepore, 2003), Bernoulli probability distribution (Hubbard, 2013), random numbers table (Maguire, 1983), or random number generator (Purcell, 2011). Other randomized studies did not specify the generation of the allocation sequence (e.g., Maunsell, 1996). Other studies (e.g., Capone, 1983; Gordon, 1980) have high risk of selection bias due to lack of randomization.
4.3.2 Performance bias
Only one included study specified that the researcher was blinded to the allocation of subjects (Purcell, 2011). Many studies were judged to have unclear risk of performance bias due to lack of specification of researcher blinding.
4.3.3 Detection bias
Risk of detection bias was low for three studies that specified that assessors were blinded to participants' allocation (Hubbard, 2013; Lepore, 2003; Purcell, 2011). The remaining studies were judged to have unclear risk of detection bias.
4.3.4 Attrition bias
Attrition was generally well-reported (low risk of bias) in the included studies, which often explained attrition due to one or a combination of the following: cancer recurrence, misdiagnosis, decline, refusal to participate or death (Berglund, 1994; Gordon, 1980; Hubbard, 2013; Lepore, 2003; Maguire, 1983; Tamminga, 2013). Some studies acknowledged the presence of attrition in their studies but did not discuss reasons (Bottcher, 2013; Capone, 1983; Granstam-Bjorneklett, 2013). Lastly, two studies did not discuss any attrition (Purcell, 2011; Sachs, 1980), resulting in a rating of unclear risk of attrition bias.
4.3.5 Reporting bias
About half of the included studies had low risk of reporting bias and provided adequate information to derive effect sizes. Some studies did not include data on all follow-up time points such as all outcome data (Berglund, 1994) and sample sizes (Bottcher, 2013; Capone, 1980; Gordon, 1980; Lepore, 2003; Maguire, 1983; Sachs, 1980).
4.4 EFFECTS OF INTERVENTIONS
4.4.1 Employment status
Ten studies (Berglund, 1994; Bottcher, 2013; Capone, 1980; Gordon, 1980; Lepore, 2003; Maguire, 1983; Maunsell, 1996; Purcell, 2011; Sachs, 1980; Tamminga, 2013) measured employment status (employed vs. unemployed). Two main measures were used: employment status or return-to-work. Since studies that measured employment status did not distinguish whether participants had prior employment before cancer diagnosis or treatment, we combined these measurements as a single measure of gainful employment status. The results of the studies were synthesized in a random-effects meta-analysis using the odds ratio effect sizes. The weighted mean effect size for employment status was OR = 1.71 (95% confidence interval (CI) = 1.26 to 2.32); P = 0.001), favoring the intervention groups. To better interpret the odds ratio, we converted the mean odds ratio to percentages. We first calculated a baseline employment rate for all the comparison groups across studies, which was 60%. The adjusted odds ratio of 1.71 translates to an employment rate of about 71% for intervention participants, a non-trivial change. See Table 2 for a summary of intervention effects and Table 3 for effects on employment status. See Figure 5.1 for a forest plot. We assessed heterogeneity using the Q-statistic (Q(10) = 15.89, P = 0.10), I2 (37.06%), and τ2 (0.09). These statistics collectively indicate that the distribution of effect sizes is relatively homogeneous. This homogeneity and the small number of included studies suggest that the examination of moderators is not warranted.
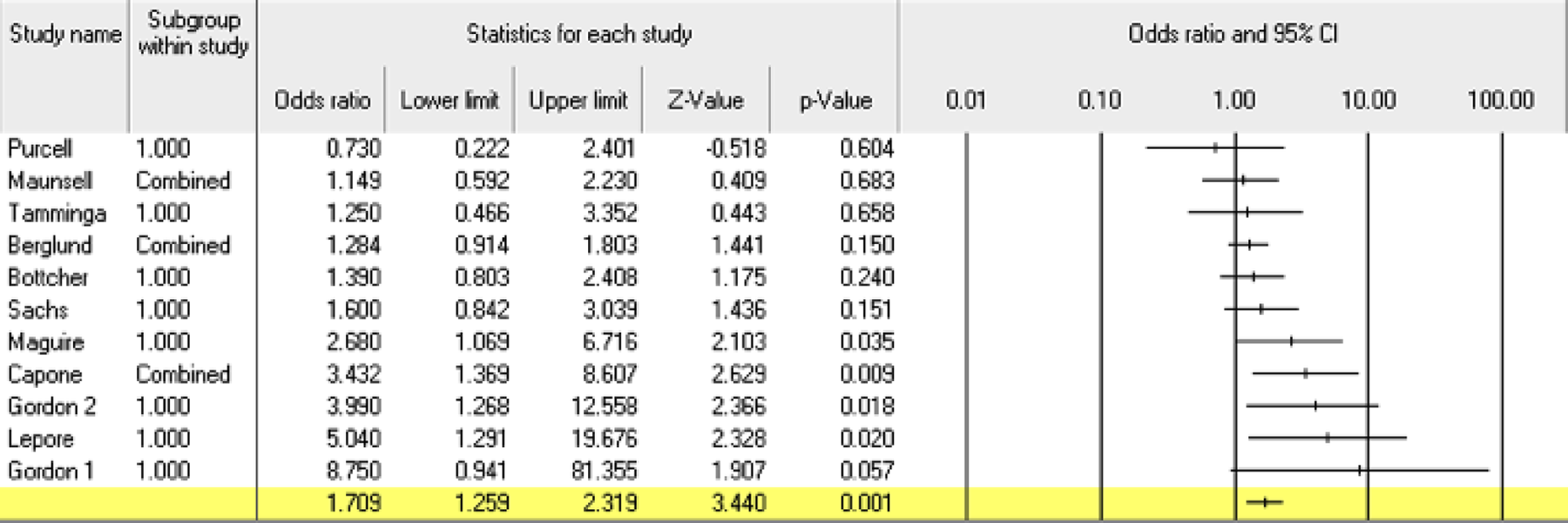
Forest Plot for Studies with Employment Outcome.
Although we did not locate a large enough number of eligible studies to conduct moderator analyses, we performed an exploratory analysis to distinguish effects of the randomized controlled trials from the quasi-experimental studies. For RCTs, the weighted mean effect size for employment status was OR = 1.44 (CI = 0.99 to 2.09); p = 0.058. The mean odds ratio of 1.44 translates to an employment rate of about 68% for intervention participants, compared to the baseline 60% for comparison group participants described previously. For QEDs, the weighted mean effect size for employment status was OR = 2.18 (CI = 1.32 to 3.60); p = 0.002. The mean odds ratio of 2.18 for the quasi-experimental studies translates to an employment rate of about 77% for intervention participants, compared to the baseline rate of 60% for the comparison group participants. See Figure 2 for a forest plot. Although the mean effect size from QEDs was larger than that from the RCTs, there is no significant difference between the two types of experimental designs (p = 0.19).
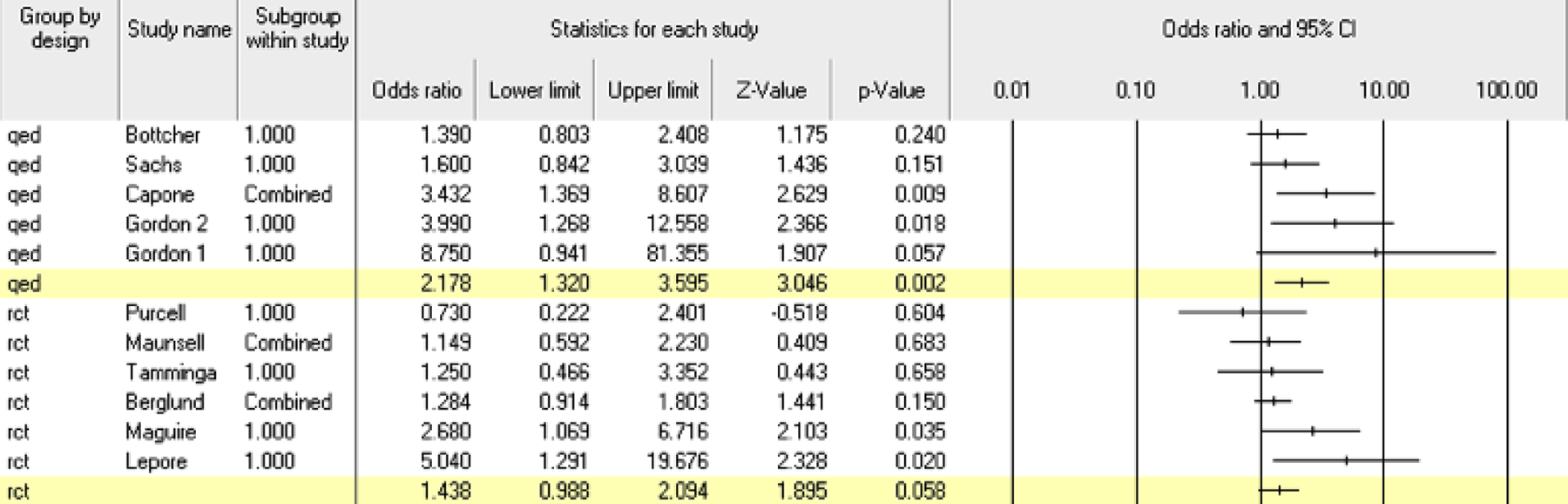
Forest Plot for Studies with Employment Outcome by Research Design (RCT and QED).
This result provides a potentially troubling indication that QED studies may be over-estimating intervention effects on employment whereas the RCT studies, when examined alone, result in a non-significant mean effect size. Therefore, caution needs to be exercised when interpreting the effectiveness of these interventions for increasing employment.
4.4.2 Hours worked
The number of hours worked was measured as an outcome in two studies (Maunsell, 1996; Purcell, 2011). Both studies were randomized controlled trials. The weighted mean effect size for hours worked was OR = 0.89 (CI = 0.22 to 1.52; p = 0.67), favoring the comparison groups. This non-significant result indicates there was no evidence of an effect of the interventions on working hours. See Table 4 for effects on number of hours worked.

Forest Plot for Studies with Hours Worked Outcome
4.4.3 Sick Leave
Four studies (Berglund, 1994; Granstam-Bjorneklett, 2013; Hubbard, 2013; Tamminga, 2013) measured sick leave. All four studies were randomized controlled trials. Sick leave was measured as the average number of days taken by cancer survivors. The weighted mean effect size for sick leave was OR = 1.18 (CI = 0.81 to 1.71; p = 0.39), favoring intervention participants. This non-significant result indicates there was no evidence of an effect of the interventions on sick leave. See Table 5 for effects on sick leave.

Forest Plot for Studies with Sick Leave Outcome
5 Discussion
5.1 SUMMARY OF THE MAIN RESULTS
We found 12 studies evaluating the effects of psychosocially-related interventions for the employment of cancer survivors. Our results provide promising evidence that the included interventions may improve employment status (OR = 1.71, p = 0.001) for cancer survivors. For RCTs, the weighted mean effect size for employment status was OR = 1.44 (CI = 0.99 to 2.09), favoring the intervention groups. The mean odds ratio of 1.44 translates to an employment rate of about 68% for intervention participants compared to a baseline 60% for comparison group participants. For QEDs, the weighted mean effect size for employment status was OR = 2.18 (CI = 1.32 to 3.60), also favoring the intervention groups. The mean odds ratio of 2.18 for the quasi-experimental studies translates to an employment rate of about 77% for intervention participants, compared to the baseline rate of 60% for the comparison group participants. Although the mean effect size from QEDs was larger than that from the RCTs, there is no significant difference between the two types of experimental designs. There was no evidence of an effect on the number of hours worked (OR = 0.89, p = .67) or for number of sick leave days (OR = 1.18, p = 0.39).
5.2 OVERALL COMPLETENESS AND APPLICABILITY OF EVIDENCE
The number of included studies was small given our inclusion criteria, producing a much larger pool of studies that were excluded. Moreover, the wide range of the types of interventions that were included most likely decreases the precision of the results of this review. Lastly, the included studies demonstrated a narrow age range, in particular, older age participants. The nature of our population, cancer survivors, tends to be older due to the late timing of when cancer occurs. Nine of the 10 studies that reported participant age had individuals of an average age of over 50 years. Additional research on these particular interventions and younger participants is needed before more specific generalizations and recommendations for the effectiveness of these programs can be put forth.
5.3 QUALITY OF THE EVIDENCE
This systematic review found limited evidence of sufficient methodological rigor confidently assess the effects of interventions for employment of cancer survivors. Overall, the number of RCTs was few in number, and even with quasi-experimental studies, sample sizes were relatively small (ranging from treatment groups of 7 to 172 participants). Moreover, the majority of studies lacked information about the study elements needed to assess risk of bias or evidenced high risk of bias. One particular study characteristic that was consistently missing from study reports was an assessment of treatment fidelity, a useful aspect for interpreting particularly conspicuous findings and to aid in broadening generalizability. Although some studies report dosage of the intervention and contamination of the control group (e.g., Tamminga, 2013), discussion of whether the intervention was implemented as intended was lacking. Overall, the internal and external validity of the included studies were limited.
5.4 POTENTIAL BIASES IN THE REVIEW PROCESS
The greatest bias in our review arises from interpretation of the intervention programs due to the multi-dimensional nature of our included studies. Although we limited our criteria to interventions that were psychosocial in nature, the broad range of interventions was unexpected and may be a source of additional weakness in interpreting the findings. The nature of many interventions targeted at cancer survivors tend to be multidisciplinary in nature, incorporating aspects from psychiatry, education, and physical exercise/medicine. This type of multi-component interventions obfuscates a clear “what works” picture for particular facets of a program, but at the same time, may be a potentially effective approach in facilitating employment for cancer survivors.
5.5 AGREEMENTS AND DISAGREEMENTS WITH OTHER STUDIES OR REVIEWS
This review presents the first meta-analysis of psychosocial interventions for improving employment for cancer survivors. Previous reviews (e.g., de Boer et al. 2011) did not average effects of interventions, omitted particular studies that measured employment-related outcomes, or were premature, precluding the development of more recent evaluations of interventions. De Boer et al. (2011) found relatively large effects for psychological interventions but did not locate any studies of vocational interventions in the field. Our review includes vocationally-oriented interventions and finds more modest support for the overall impact of psychosocial interventions for improving employment status among cancer survivors. In addition, our review includes other employment-related outcomes such as number of hours worked and sick leave.
The authors will examine the review every three years after publication for update as per C2 policy.
6 Conclusion
6.1 IMPLICATIONS FOR PRACTICE
This review highlights the positive effect psychosocial interventions may have on employment outcomes for cancer survivors. The multi-dimensional nature of the included interventions makes it difficult to isolate effective individual components. However, results suggest that multi-component interventions that incorporate information or educational training, counseling or coping skills sessions, and also physical exercise components may be the best way to target the generally multi-dimensional nature of employment for cancer survivors. In addition, some methodological shortcomings of the studies overall make it likely that there is bias in the results and too few studies to provide sufficiently strong evidence to recommend particular practices.
6.2 IMPLICATIONS FOR RESEARCH
This review highlights the need for additional rigorous studies in this area, in particular, randomized controlled trials with more detailed reporting of data and components of study design. Studies also need to report the fidelity with which the program was implemented and describe in more detail an intervention's particular features and duration. New trials need to collect information on employment status and not solely self-reported measures of quality of life. Many otherwise rigorous studies were excluded for this reason. Simple additions to interview protocols or questionnaires can provide valuable insight on whether interventions affect employment outcomes. In addition, perhaps more interventions that focus specifically on VR such as on-the-job supports, interview-training, strategies to cope with symptoms while working are needed to assess whether these programs influence return-to-work and employment (e.g., Tamminga et al., 2013).
7 Acknowledgements
This is a product developed by the Center on Knowledge Translation for Employment Research through grant H133A100026 to SEDL from the National Institute on Disability and Rehabilitation Research (NIDRR) in the United States Department of Education's Office of Special Education and Rehabilitative Services. However, these contents do not necessarily represent the policy of the United States Department of Education, and you should not assume endorsement by the Federal Government.
Footnotes
9 Characteristics of Included Studies and Assessment of Risk of Bias Table 9.1:
|
|
Randomly allocated | Valid sample size used in data synthesis |
|---|---|---|
| Dennis et al., 2004 | 300 | 300 (MET/CBT5: 100, MDFT: 100, ACRA: 100) |
| Godley et al., 2010 | 320 | 320 (MET/CBT7: 79, MET/CBT7+ACC: 81, CBOP: 80, CBOP+ACC: 80) |
| Hendriks et al., 2011 | 109 | 109 (CBT: 54, MDFT: 55) |
| Kaminer et al., 1998a & 1999 | 32 | 23 (CBT: 13, IT: 10) |
| Kaminer et al., 2002 | 88 | 88 (CBT: 51, PET: 37) |
| Latimer et al., 2003 | 43 | 42 (IFCBT: 21, DHPE: 21) |
| Waldron et al., 20011 | 61 | 61 (MET/CBT: 31, FFT: 30) |
|
|
|
|
10 Data and Analyses
11 Figures