
Abstract
This publication is a Campbell Systematic Review of the effect of Multidimensional Family Therapy (MDFT) for treating abuse of cannabis, amphetamine, ecstasy or cocaine (referred to here as non-opioid drugs) among young people aged 11-21 years. The misuse of prescription drugs and the use of ketamine, nitrous oxide and inhalants such as glue and petrol are not considered in this review.
After a rigorous search of the literature, five randomized controlled studies with samples of 83-450 participants were identified. Three studies were conducted by MDFT program developers, one study was conducted by an independent investigator with the program developer as a co-author, and one study was conducted by independent investigators. Four studies were performed in the US, while the other was performed across five European countries.
There is evidence that MDFT is slightly more effective in treating young people's drug abuse than other treatments; however, the difference is small. Furthermore, none of the five included studies could be characterised as a robust randomised controlled trial with a low risk of bias on all assessed domains. One study provided insufficient information on core issues for the risk of bias to be assessed and therefore we find reason to question the validity of this study. Well-designed, randomized controlled trials within this population are needed. More research is also required to identify factors which modify the effect of MDFT and to identify which particular youth subgroups may be most likely to respond.
Key messages
PLAIN LANGUAGE SUMMARY
This publication is a Campbell Systematic Review of the effect of Multidimensional Family Therapy (MDFT) for treating abuse of cannabis, amphetamine, ecstasy or cocaine (referred to here as non-opioid drugs) among young people aged 11-21 years. The misuse of prescription drugs and the use of ketamine, nitrous oxide and inhalants such as glue and petrol are not considered in this review.
Youth drug abuse is a severe problem worldwide and recent reports describe ominous trends of youth drug abuse and a lack of effective treatment. This review is concerned with drug abuse that is severe enough to warrant treatment. It focuses on young people who are receiving MDFT specifically for non-opioid drug abuse.
MDFT is a manual-based, family-oriented treatment, designed to eliminate drug abuse and associated problems in young people's lives. MDFT takes a number of risk and protective factors into account; the approach acknowledges that young people's drug abuse is linked to dimensions such as home life, friends, school and community (Liddle et al., 2004). MDFT aims to modify multiple domains of functioning by intervening with the young person, family members, and other members of the young person's support network (Austin et al., 2005). MDFT is thus based on a number of therapeutic alliances, with the young drug abuser, his or her parents and other family members, and sometimes with school and juvenile justice officials.
After a rigorous search of the literature, five randomized controlled studies with samples of 83-450 participants were identified. Three studies were conducted by MDFT program developers, one study was conducted by an independent investigator with the program developer as a co-author, and one study was conducted by independent investigators. Four studies were performed in the US, while the other was performed across five European countries.
We used meta-analytic procedures to summarise the available evidence on the effects of MDFT in comparison with other interventions on drug abuse, education, family functioning, risk behavior and retention in treatment. In this review, we interpret a value of the standardised mean difference, SMD=0.20 as a small effect size, in line with the general practice (Cohen, 1988). We note, however, the possibility that such a value might actually represent a larger effect if it is equivalent to a large reduction in the percentage of days a youth uses drugs, but we cannot comment further as we were unable to analyse the absolute effect of MDFT given that no studies comparing MDFT to no other treatment were available. The findings are as follows: On drug abuse: Based on the available evidence we conclude that MDFT has an effect on drug abuse reduction compared to other treatments, although the difference is small. On education: There is insufficient evidence to conclude whether MDFT has an effect on education compared to other treatments. On family functioning: There is no available evidence to conclude whether MDFT has an effect on family functioning compared to other treatments. On risk behavior and other adverse effects: There is no available evidence to conclude whether MDFT has an effect on risk behavior and other adverse effects compared to other treatments. On treatment retention: MDFT may result in improved treatment retention in young drug abusers compared to other interventions
The evidence found was limited as only five studies were included, and two studies had significant amounts of missing data. The evidence was very limited in terms of the outcomes reported on education, family functioning and risk behavior, and was insufficient for firm conclusions to be drawn on the effectiveness of the treatment with regard to such outcomes.
There is evidence that MDFT is slightly more effective in treating young people's drug abuse than other treatments; however, the difference is small. Furthermore, none of the five included studies could be characterised as a robust RCT with a low risk of bias on all assessed domains. One study provided insufficient information on core issues for the risk of bias to be assessed and therefore we find reason to question the validity of this study.
Well-designed, randomized controlled trials within this population are needed. More research is also required to identify factors which modify the effect of MDFT and to identify which particular youth subgroups may be most likely to respond.
Executive summary/Abstract
BACKGROUND
Youth drug abuse is a severe problem worldwide, and the use of cannabis, amphetamine, ecstasy and cocaine (referred to here as non-opioid drugs) is strongly associated with a range of health and social problems. This review focuses on drug abuse that is severe enough to warrant treatment. The population of interest is young people who are receiving MDFT specifically for non-opioid drug abuse.
MDFT is a manual-based family therapy approach that focuses on individual characteristics of the young person, the parents, and other key individuals in the young person's life, as well as on the relational patterns contributing to the drug abuse and other problem behaviors. A variety of therapeutic techniques are used to improve the young person and the family's behaviors, attitudes, and functioning across the variety of domains. MDFT aims to reorient the young person and his/her family towards a more functional developmental trajectory based on key principles that include: 1) Individual biological, social, cognitive, personality, interpersonal, familial, developmental, and social ecological aspects can all contribute to the development, continuation, worsening and chronicity of drug problems; 2) The relationships with parent(s), siblings and other family members are fundamental domains of assessment and change; 3) Change is multifaceted, multi-determined and relates to the youths' cognitive and psychosocial developmental stages; 4) Motivation is not assumed, but is malleable; and motivating the young person and his or her family members about treatment participation and change is a fundamental therapeutic task; 5) Multiple therapeutic alliances are required to create a foundation for change; and 6) Therapist responsibility and attitude is fundamental to success (Liddle, 2010).
OBJECTIVES
The main objectives of this review are to evaluate the current evidence on the effects of MDFT on drug abuse reduction for young people (aged 11-21 years) in treatment for non-opioid drug abuse, and if possible to examine moderators of drug abuse reduction effects, specifically analysing whether MDFT works better for particular types of participants.
SEARCH STRATEGY
An extensive search strategy was used to identify qualifying studies. Searches were run in October 2014. A wide range of electronic bibliographic databases were searched along with government and policy databanks, grey literature databases, citations in other reviews and the included primary studies, hand searching in relevant journals, and Internet searches using Google. We also maintained correspondence with researchers in the field of MDFT. No language or date restrictions were applied to the searches.
SELECTION CRITERIA
To be eligible for inclusion, studies must: have involved a manual-based outpatient MDFT drug treatment for young people aged 11-21 years enrolled for non-opioid drug abuse; have used experimental, quasi-experimental or non-randomized controlled designs; have reported at least one of the following eligible outcome variables: abstinence, reduction of drug abuse, family functioning, education or vocational involvement, retention, risk behavior or any other adverse effect; not have focused exclusively on treating mental disorders; and have had MDFT as the primary intervention.
DATA COLLECTION AND ANALYSIS
The literature search yielded a total of 6,519 references, of which 170 studies were deemed potentially relevant and retrieved for eligibility determination. Of these, 16 papers describing five unique studies were included in the final review. Metaanalysis was used to examine the effects of MDFT on drug usage (measured by both frequency and problem severity), on education and on treatment retention.
It was not possible to perform a meta-analysis on family functioning, risk behavior or other adverse effects, nor was it possible to assess moderators of drug abuse reduction effects, or whether MDFT works better for particular types of participants.
RESULTS
Not all the studies provided data that enabled the calculation of comparable effect sizes on the different outcomes. Two studies had two comparison groups with different individuals, and we performed separate analyses including the different control groups where these two studies provided relevant outcome measures. The most conservative effects for the different outcomes are reported in the following. All outcomes are measured as decreases; hence a negative effect size favours MDFT.
Meta-analysis of the five included studies showed a small effect (around 30 percent of a standard deviation for the different control combinations) of MDFT for reduction in youth drug abuse problem severity at 6 months post-intake (SMD=-0.30 (95% CI -0.53 to -0.07, p=0.01 compared to Cognitive Behavioral Therapy (CBT), peer group, treatment as usual (TAU), multifamily educational therapy (MEI) and Adolescent Community Reinforcement Approach (ACRA)).
At 12 months post-intake meta-analysis of the five included studies showed a small effect (around 20 percent of a standard deviation for the different control combinations) of MDFT for reduction in youth drug abuse problem severity (SMD=-0.23 95% CI -0.39 to -0.06, p=0.007 compared to CBT, peer group, TAU, adolescent group therapy (AGT) and ACRA).
Pooled results of the four studies providing data on drug abuse frequency reduction favoured MDFT. The effect of MDFT for youth drug abuse frequency reduction was small at 6 months post-intake (overall around 20 percent of a standard deviation for the different control combinations) (SMD = -0.24; 95% CI -0.43 to -0.06; p=0.01 compared to CBT, peer group, TAU and MET/CBT5). It was not statistically significant at 12 month follow-up compared to CBT, peer group, TAU and MET/CBT5/ACRA.
Two studies reported on school grades as an outcome, providing data at 6 months post-intake only. Meta-analysis favored MDFT when the controls used in the analysis were peer group and MEI (SMD = -0.47; 95% CI -0.92, -0.01; p=0.05). It was not statistically significant when the comparisons used in the analysis were peer group and AGT.
We extracted data on retention from all five included studies. Meta-analysis favoured MDFT for retention of participants for all the different control combinations (OR = 0.44; 95% CI 0.21 to 0.94; p=0.03 compared to CBT, peer group, TAU, AGT and MET/CBT5). Overall the results indicated that retention may be positively affected by structured MDFT treatment compared to less structured control conditions.
AUTHORS' CONCLUSIONS
The available data support the hypothesis that, compared with certain other active treatments, MDFT reduces the severity of drug abuse among youth. The treatments MDFT was compared against in the included studies were Cognitive Behavioral Therapy (CBT), peer group, treatment as usual (TAU), adolescent group therapy (AGT)/multifamily educational therapy (MEI) and Motivational Enhancement Therapy/Cognitive Behavioral Therapy (MET/CBT5)/Adolescent Community reinforcement approach (ACRA). Furthermore, the available data support the hypothesis that there is a reduction in the frequency of drug abuse when treating young drug abusers with MDFT compared to CBT, peer group, TAU and MET/CBT5/ACRA at 6 months post-intake, but the effect is not statistically significant 12 months after intake.
The number of studies providing data that allowed calculation of an effect size for drug abuse reduction was limited, however, and this should be considered when interpreting these results. The conclusions that can be drawn about MDFT as an effective treatment for young drug abusers compared to other treatments would be more convincing if more studies were available. The pooled effect sizes are small and confidence intervals are often close to zero. The statistically significance of the pooled results on severity of drug abuse among youth 6 months post-intake is sensitive to the removal of studies with methodological weaknesses.
Overall, the results also indicate that retention may be positively affected by structured MDFT treatment compared to CBT, peer group, TAU, AGT/MEI and MET/CBT5/ ACRA which are all less-structured control conditions. However, the results must be interpreted with caution as two studies stand out from the others; here the effect sizes are large, confidence intervals are wide, and the estimated between study variation is relatively large.
The main conclusion of this review is that there is insufficient firm evidence of the effectiveness of MDFT, especially with regard to moderators of drug abuse reduction effects, and whether MDFT works better for particular types of participants. While additional research is needed, the review does, however, offer support that MDFT treatment to young non-opioid drug abusers reduce their drug abuse somewhat more than CBT, peer group, TAU, AGT/MEI and MET/CBT5/ACRA.
1 Background
1.1 DESCRIPTION OF THE CONDITION
Youth drug abuse 1 of the kind that persists beyond the experimentation phase is a severe problem worldwide (United Nations Office on Drugs and Crime (UNODC), 2010). Abuse of drugs such as cannabis, amphetamine, and cocaine, referred to in this review as non-opioids, are strongly associated with a broad range of negative health implications such as traffic accidents, sexually transmitted diseases, mental problems and suicide as well as social problems including poor academic achievement, delinquency and violent behavior (Bonner & van den Bree, 2009; Deas & Thomas, 2001; Essau, 2006; Lynskey & Hall, 2000; Office of National Drug Control Policy (ONDCP), 2000; Rowe & Liddle, 2006; Shelton, Taylor, Nordstrom & Levin, 2007).
While cannabis, amphetamine, cocaine and other non-opioid drugs remain illegal in most countries, surveys indicate widespread prevalence. In the US, 25.5 percent of 12th-grade students report having used an illicit drug (any kind) within the last month (Johnston, O'Malley, Miech, Bachman & Schulenberg, 2014). In Canada, 21 percent of 15-24 year olds report having used of some kind of illicit drug within the last year (Health Canada, 2011). In Australia, seven percent 12-17 year olds report using some kind of drug within the last month (White & Smith, 2009). The European Monitoring Centre for Drugs and Drug Addiction has found that within Europe prevalence differs significantly from country to country but that overall around a quarter of Europeans report having used some kind of illicit drug in their lifetime (European Monitoring Centre for Drugs and Drug Addiction (EMCDDA), 2013).
The prevalence of specific kinds of illicit drug abuse varies significantly, with cannabis generally being the most commonly used drug. In the US, 22.7 percent of 12th-grade students report having used marijuana/hashish (types of cannabis), 4.1 percent amphetamine, and 1.1 percent cocaine during the last 30 days before the National Survey on Drug Use conducted in 2013 (Johnston et al., 2014). The European Drug Report of 2013 indicates that 11.7 percent of the 15 to 34 year-olds in Europe has used cannabis, 1.3 percent amphetamine, and 1.9 percent used cocaine during the last year (EMCDDA, 2013).
Although not all drug users progress to severe drug abuse and dependence, some do and therefore warrant treatment (see e.g. Crowley, Macdonald, Whitmore & Mikulich, 1998). Individuals that warrant drug treatment are described variously as abusers, misusers or as dependent. These specific categorizations are used in the Diagnostic and Statistical Manual of Mental Disorders (DSM) (American Psychiatric Association, 1994, 2000). While DSM-IV is widely used, the International Statistical Classification of Diseases and Related Health problems (ICD, now ICD-10) developed by the World Health Organisation (WHO) is also in wide use. Differences between these rubrics concern both terminology and categorization criteria. For example, DSM-IV includes the category ‘abuse’, while ICD-10 explicitly avoids this term on the grounds of its ambiguity; harmful use and hazardous use are the equivalent terms in WHO usage, but the categories are not identical; and while ICD-10 uses only physical and mental criteria, DSM-IV also includes social criteria (WHO, 2011; Nordegren, 2002).
Research draws attention to the significant gap between the number of young people classified as in need of treatment and the number of young people who actually receive such treatment (SAMHSA, 2010; National Survey on Drug Use and Health (NSDUH), 2007). In the US, for example, 7.2 million young people are classified as needing treatment for illicit drug abuse, but only 1.4 million of these actually receive treatment at a specialty facility for an illicit drug abuse problem (SAMHSA, 2011). The treatment usually provided to young people is delivered in outpatient settings. Accordingly, 90 percent of the 89,521 clients under age 18 registered in substance abuse treatment in 2012 by SAMHSA were in outpatient treatment, which is the same proportion as the total treatment population (SAMHSA, 2013). Equal proportions of the clients under age 18 were enrolled in facilities with a primary focus on substance abuse treatment and in facilities whose primary focus were provision of a mix of mental health and substance abuse treatment services; this differs from the total treatment population as youth tend to be treated in dual focus facilities more often than adults (SAMHSA, 2013). Cognitive-behavioral therapy and motivational interviewing are specific therapeutic approaches that are used to some extent by most (respectively 91 and 87 percent) treatment facilities (SAMHSA, 2013).
There is growing public concern about the effectiveness and high cost of available treatments for young people, and the high rates of treatment dropout and post-treatment relapse to drug abuse (Austin, Macgowan & Wagner, 2005; Najavits & Weiss, 1994; Stanton & Shadish, 1997). While relapse must be acknowledged as an expected part of any treatment process targeting individual drug abuse, efforts should be made to make treatment as attractive, accessible and relevant as possible for young people in order to minimize the risk of unwarranted dropout and continuous relapse (Simmons et al., 2008; National Institute on Drug Abuse (NIDA), 2009). Furthermore, the services provided should be empirically supported to increase the likelihood that (a) treatment will be successful, and (b) public spending supports the interventions that are the most effective.
Researchers point to the fact that many research projects claim to have empirically validated different kinds of treatment approaches for young drug abusers (e.g. Austin et al., 2005; Rowe & Liddle, 2006; Waldron, Turner & Ozechowski, 2006; Williams, Chang & Addiction Centre Adolescent Research Group, 2000). The current dilemma in the field of youth substance use treatment is that it is not clear what works best and for whom as the research suggests that a number of interventions lead to reduced drug abuse (Waldron & Turner, 2008). Treatments identified as promising are individually based cognitive and motivational therapies including Cognitive Behavioral Therapy, Multisystemic Therapy, and Family therapies (Deas & Thomas, 2001; Galanter & Kleber, 2008; Kaminer, 2008; Waldron & Turner, 2008).
Family therapy covers a range of different interventions, and is based on different manuals and varying theoretical sources such as behavioral and cognitive behavioral theory, structural and strategic family theory, and family systems theory (Williams et al., 2000; Austin et al., 2005). Family-based interventions for the treatment of young drug abusers include Multidimensional Family Therapy, Brief Strategic Family Therapy, Functional Family Therapy and Family Behavior Therapy (Waldron & Turner, 2008; Austin et al., 2005; Rowe & Liddle, 2006; Alexander & Sexton, 2002; Waldron et al., 2006; Williams et al., 2000). Some reviews suggest that these family-based therapies are superior to individual-based programs in reducing youth drug abuse (Williams et al., 2000; Lipsey et al., 2010; Waldron, 1997).
Young people who abuse drugs persistently and to an extent that warrants treatment have unique needs due to their particular cognitive and psychosocial developmental stage. Recognizing that young people are particularly sensitive to social influences, families and peer groups being highly influential, authorities such as the U.S.
National Institute on Drug Abuse recommends that youth drug treatments facilitate positive parental and peer involvement (Institute on Drug Abuse (NIDA), 2009: 22). Moreover, they recommend that other systems in which the youth participates (such as schools and athletics) are also integrated into a comprehensive treatment approach to meet the unique needs of young drug abusers (ibid. 23). A number of studies and reviews show positive results for family therapies in general, but there is a need to synthesize individual study results for specific family therapies to determine whether and to what extent specific family therapy interventions work for young drug abusers (Williams et al., 2000; Austin et al., 2005; Waldron & Turner, 2008; Kaminer, 2008; Deas & Thomas, 2001).
This review has explored the specific family-based intervention of Multidimensional Family Therapy (MDFT) (Liddle, 2002; Liddle et al., 2001; Liddle, Rowe, Dakof, Henderson & Greenbaum, 2009) as aggregated evidence for MDFT's effects is needed. The review has attempted to clarify the effects of the MDFT program for relevant groups of young people aged 11-21 living with their families, and has focused on young people enrolled in treatment for drug abuse, independent of how their problem was labeled. Enrolment in drug treatment indicates that the severity of the young person's drug abuse has caused the young person or a significant adult close to the young person (such as teacher, parent, social services worker, school counselor) to seek treatment. The review focused on MDFT delivered as outpatient treatment 2 and primarily on non-opioid drug abuse 3 ; it is one in a series of reviews on different manual-based family therapy interventions for young people in treatment for drug abuse 4 .
1.2 DESCRIPTION OF THE INTERVENTION
Multidimensional Family Therapy (MDFT) has evolved over the last twenty years and is a manual-based, family-oriented treatment designed to eliminate drug abuse and associated problems in young people's lives (Liddle, 1999; Liddle, 2002; Liddle et al., 2009). MDFT is one of several family therapy forms that meet the general characteristics of manual-based family therapies in that it deals with young people and their families as a system throughout treatment, and thereby recognizes the important role of the family in the development and treatment of young people's drug abuse problems (Liddle et al., 2001; Muck et al., 2001).
MDFT is designed to take into account a number of risk and protective factors, and it acknowledges that young people's drug abuse is linked to multiple dimensions: home life, friends, school and community (Liddle et al., 2004). As such it advocates that a multi-dimensional approach is needed to resolve the young person's problematic drug abuse, and therefore aims to modify multiple domains of functioning by intervening with the young person, family members, and other members of the young person's support network (Austin et al., 2005). This also means that MDFT is based on multiple therapeutic alliances; with the young drug-user, his or her parents and other family members, and perhaps school and juvenile justice officials. While some young people have only a single parent and few significant others relevant to therapy, others might have two sets of parents and many significant others relevant to therapy, and the therapist must organize the treatment accordingly.
Treatment focuses on individual characteristics of the young person, their parents, and other key individuals in the young person's life, as well as on the relational patterns contributing to the drug abuse and other problem behaviors. A variety of therapeutic techniques are used to accomplish this and to improve the young person and the family's behaviors, attitudes, and functioning across the variety of domains (Liddle, 1999). MDFT aims to reorient the young person and family toward a more functional developmental trajectory on the basis a variety of key principles, including: 1) Individual biological, social, cognitive, personality, interpersonal, familial, developmental, and social ecological aspects can all contribute to the development, continuation, worsening and chronicity of drug problems; 2) The relationships with parent(s), siblings and other family members are fundamental domains of assessment and change; 3) Change is multifaceted, multi-determined and relates to the youths' cognitive and psychosocial developmental stages; 4) Motivation is not assumed, but is malleable and motivating the young person and family members about treatment participation and change is a fundamental therapeutic task; 5) Multiple therapeutic alliances are required to create a foundation for change; and 6) Therapist responsibility and attitude is fundamental to success (Liddle, 2010).
MDFT's theory of change hypothesizes that changing the family system constructively will produce changes in youths' drug abuse (reduction or elimination) as well as improvements in relation to other emotional and behavioral problems (Hogue, Liddle, Dauber, & Samoulis, 2004, Liddle et al, 2005). Specifically, MDFT process studies have emphasized the importance of addressing cultural themes and increasing youths' participation in treatment (Jackson-Gilford, Liddle, Tejeda & Dakof, 2001) and improving parents' skills (Schmidt, Liddle & Dakof, 1996). Moreover, the quality of therapeutic alliances between both the therapist and the youth, and the therapist and parent(s) are emphasized as decisive for the production of change (Robbins et al. 2006).
1.2.1 Theoretical background
MDFT combines elements of several theoretical frameworks, including family systems theory and developmental psychology (Bronfenbrenner, 1979; Minuchin, 1985; Stroufe & Rutter, 1984), ecosystems theory and the risk and protective model of adolescent substance abuse (Austin et al., 2005; Hogue & Liddle, 1999; Liddle & Hogue, 2000). The influence of ecological and developmental theory in MDFT is evident as the intervention takes into account the changing environments and multidimensional systems in which young drug abusers reside (Liddle, 2002; Liddle et al., 2001).
Like other family system-based therapies, MDFT builds upon the assumption that families can be viewed as systems with structures, hierarchies and patterns of interaction that influence each individual family members' actions (Poulsen, 2006). MDFT views any system of interrelated and interdependent family members as both unique and changeable. Problem behavior is understood in relation to the family context, and youth deviance (including drug abuse) is associated with maladaptive social interaction patterns in the family. Accordingly, MDFT theorizes that interventions should be directed at families rather than at individuals. The family, however, is itself part of a larger social system, and just as young people are influenced by their families, the family is influenced by the larger social (and cultural) systems in which they exist (Austin et al., 2005; Doherty & McDaniel, 2010; Kaminer & Slesnick, 2005; O'Farrell & Fals-Steward, 2008; Poulsen, 2006). Family therapies are thus also concerned with the wider social context in which the individual and the family are embedded.
The focal areas of MDFT (family, peers, and networks) are each considered to be a ‘holon’, i.e. they are at the same time viewed as systems on their own and as subcomponents of a larger unity (Bertalaffny, 1976, Bronfenbrenner, 1979). This means that a family is viewed as simultaneously a whole (composed by individual family members) as well as a “part” of other systems (such as communities) (Liddle, 2002; Minuchin & Fishman, 1981; Koestler, 1978). A therapist's job is to understand the workings of each system or ecology as both a whole and a part, and to devise interventions that fit the individual and the systems he/she is part of. For example, relationships with parents and/or peers must be included in therapy as part of changing problem behavior such as drug abuse. Approaching systems as simultaneously wholes and parts is identified as a core element in the MDFT-intervention (Liddle, 2002).
To produce change, MDFT proposes that therapists should focus on parenting skills and family interaction. However, MDFT stresses that this is not necessarily sufficient for a change in the young person's drug abuse. A key idea is that therapists, in addition to working with both internal family factors (such as family patterns and rituals, perceptions of each other and oneself), also need to address external systemic factors (such as peer relations, school and other pro-social institutions). Thus, MDFT aims at reducing symptoms and enhancing pro-social and normative developmental functions in problem youths, by targeting the family as the foundation for intervention and simultaneously facilitating curative processes in several domains (systems) of the young persons' lives. Particular behaviors, emotions and thinking patterns related to problem formation and continuation are replaced by new behaviors, emotions, and thinking patterns associated with appropriate intrapersonal and familial development (Liddle, 2002; Liddle, Cecero, Hogue, Dauber & Stambaugh, 2006).
The emphasis on therapists working simultaneously with several systems to produce change in young people's problem behavior is not unique to MDFT. Rather, this is generally emphasized in family therapy approaches (Dakof, Godley & Smith 2011). Likewise, these approaches in general also instruct therapists to be highly nonpunitive and non-judgmental toward youth and parents and stress that therapists should collaborate with youth and parents to develop meaningful, client-driven goals (ibid, p. 264). The distinctiveness in MDFT derives from the assembly of theories, methods and techniques into specific therapeutic principles that guide the intervention step-by-step as outlined in the following section.
1.2.2 MDFT components
MDFT is manual-based but is flexible with regards to its duration, settings and, to some extent, therapeutic methods (Liddle, 2002). It has been developed over time and has been used by both experienced family therapists and clinicians with no family therapy experience, but ideally (according to the MDFT manual; Liddle, 2002), both therapists and supervisors should have a background in family therapy and/or child development.
The MDFT approach has been developed and tested since 1985. Since 1991, this work has been performed through the Center for Treatment Research on Adolescent Drug Abuse, Miami USA. The latest version of the MDFT manual was published in 2002 (Liddle, 2002).
The comprehensive multidimensional assessment is hypothesized as a key feature in the success of MDFT for young people experiencing multiple problems. Assessment in MDFT provides a therapeutic map, directing therapists where to intervene in the multiple domains of the young person's life. The process involves not only the identification of different problem areas, symptoms, and co-occurring disorders, but also risk and protective factors in all relevant domains, so that these factors can be targeted for change. Through a series of individual and family interviews, meetings with school, court, and other mental health professionals, and observations of family interactions, the therapist seeks to answer critical questions about functioning in each area. First, assessment is an ongoing process throughout therapy, continually integrated with interventions to calibrate treatment planning and solving. Second, guided by this multidimensional assessment, the model addresses common root factors underlying a range of emotional and behavioral symptoms that co-occur with young persons' drug abuse.
MDFT is organized into phases, based upon knowledge of what is considered to be normal cognitive and emotional development for young people. Each phase represents one of several targets for assessment, intervention, and change, and the therapist will not progress to the next phase until the therapy has completed the current phase.
Each phase is implemented through four types of treatment sessions (Liddle, Dakof, Turner, Henderson & Greenbaum, 2008; Liddle et al., 2006, Liddle, 2002): individual sessions with the young person, sessions with the parent(s), sessions with other family members and systems external to the family 5 , and sessions to change the parent(s)-young persons-interaction(s).
The three phases structuring the MDFT intervention aim to: form therapeutic alliances and build the foundation for therapy; take action and make changes; and seal the changes and guide the family members toward creating a healthy internal relationship.
Phase 1: Therapeutic alliances
Engaging both the young person and his or her family in the process of change is the main objective in the first phase of MDFT (Liddle et al., 2001). Engagement strategies include the formulation of therapeutic alliances with the youth, family members, and other extra familial support systems. Liddle (2002) concludes in the MDFT manual that the first phase is important and includes presenting therapy as a collaborative process, defining therapeutic goals that are meaningful to each participant, generating hope and attending to each participant's experience. The focus is on individualizing treatment for each of the family members involved through the development of personal and individualized treatment objectives for each participant. The use of culturally specific themes is also cited as a useful tool for engaging diverse youths and families (Liddle, 1999).
The first phase will typically last for three weeks and is oriented at motivating and preparing the family for therapy, explaining the therapy to the family, and creating expectations. During this phase, the therapist will meet people relevant to the family. In some cases, it will be relevant to include siblings and relatives, while in other cases friends or perhaps a social worker are relevant depending on whom the young drug abuser spends most of their time with. The beginning of the first phase is crucial and it can be a challenging task to engage the family positively; especially as the young person can be resistant, often denies his/her drug abuse, and may lack cooperation. The first phase in forming therapeutic alliances allows for the MDFT program to be flexible and adaptable to different social settings, family structures and cultures (for example, single parents, different ethnic groups) and co-occurring conditions (for example, juvenile justice system issues, or co-morbid mental health conditions).
Phase 2: Make changes
In the second phase, the therapist will take action by mobilizing the young person and his/her family network, by working with the different systems (school, peers, family, community workers), and by the practice and training of the family members' stress and communication handling skills, as well as by preventing or preparing for detours.
The second phase is more behaviorally focused and includes efforts to increase the young person's pro-social behaviors, positive social networks, and antidrug behaviors and attitudes. There is also an emphasis on developmental issues, including a focus on increasing developmentally appropriate family interactions. Teaching problem-solving and decision-making skills and modifying defeating parenting beliefs and behaviors through a process called enactment are the primary techniques used by MDFT clinicians during phase two.
The therapist will work with the young person and the parents, both individually and together as a family, to observe how they communicate and treat each other. The therapist assesses different aspects of the young person's life and then starts the process of change by asking, ‘what are the missing aspects of the young person's and family's lives? What set of circumstances and what specific day-to-day activities and intrapersonal and interpersonal processes could reverse the current development-threatening circumstances?’ (Liddle, 2002)
Phase 3: Seal the changes and end of therapy
In the third phase, the therapist will seek to maintain the changes in the behaviors, emotions and thinking patterns of the family members. This is also the phase where the therapist will prepare for the MDFT sessions to end and works with the young person and family to generalize the newly acquired skills and behaviors for future situations to maintain the positive changes. MDFT does not include an aftercare component.
1.2.3 Duration and setting
Within the overall frame of MDFT, the components can be practiced in slightly different ways according to the clinical needs of the young person and his or her family (Rowe & Liddle, 2003; Liddle, 2002). MDFT has been developed and tested in different forms or versions, making it a flexible intervention. For example, an intensive outpatient version consists of 25 sessions over six months, and a less intensive version consists of 12 sessions over three months (Liddle, 2002). The frequency of sessions will depend on the needs of the family. Sessions can take place in clinical or home settings.
1.3 HOW THE INTERVENTION MIGHT WORK
Overall, MDFT proposes to produce positive changes through working simultaneously with different systems -- inside and outside the family -- to end drug abuse and related problems (Liddle, 2002; Rowe, 2010). MDFT outlines a three-phase model that explicates how the intervention is to be administered. Stage 2 is highlighted as the working phase of treatment, where significant change attempts are made within and across systems (Liddle et al., 2005).
The working phase of MDFT includes an adolescent module, a parent module and a family interaction module. In the adolescent module (Liddle et al., 2005, p. 140-141), the therapy seeks to produce change through a range of techniques such as helping the youth examine positives and negatives about their drug abuse as well as helping the youth articulate hopes and dreams for the immediate and long term. Overall, the module aims to help the youth see that they will have difficulties in achieving the things they say they want as long as current problem behavior continues, and the therapist helps the youth create concrete pathways toward a change of lifestyle.
In the parent module (Liddle et al., 2005, p. 141-142), the therapy seeks to produce change by, for example, clarifying and responding to parents' needs (e.g. for extra psychiatric service), instilling hope that change is possible (e.g. through bringing small signs of change to their attention), and advising parents -- respectfully, but in direct terms - on how to handle challenging situations. Overall, the module aims to improve parents' skills, such as their abilities to practice age-proportionate limit-setting and to enforce house rules, including defining both sanctions and rewards for adherence.
In the family interaction module (Liddle et al., 2005, p. 143), to the therapy seeks to produce change through helping families to establish more positive patterns of interaction, e.g. improving their communication and conflict resolution skills and their understanding of the importance of establishing positive, supportive relationships.
1.4 WHY IT IS IMPORTANT TO DO THIS REVIEW
Persistent drug abuse among young people is a problem worldwide as it causes a range of health problems and social problems. Drug treatment targeting young drug abusers is challenging and costly as interventions are often plagued by high dropout rates and post-treatment relapse into drug abuse. Research suggests that almost half of the young drug abusers who receive drug treatment do not complete that treatment (Substance Abuse and Mental Health Services Administration, 2008). While relapse must be acknowledged as an expected part of any treatment process targeting individual drug abuse, there is a need to identify effective treatments for addressing young people's drug abuse problems in order to minimize unwarranted treatment dropout and continuous post-treatment relapse (Simmons et al. 2008, NIDA 2009). Furthermore, the growing interest among policy makers in increasing funding for evidence-based interventions is a strong motivation to add to the evidence base with a systematic review on a promising treatment for young drug abusers.
Previous reviews (Vaughn & Howard, 2004; Waldron & Turner, 2008; Becker & Curry, 2008) indicate that MDFT is a promising treatment for young drug abusers. However, the only meta-analysis thus far conducted (Waldron & Turner, 2008) included MDFT as part of a broad category of family therapy rather than including MDFT as a distinct treatment model. In contrast, this review examines the effect of MDFT and by aggregating individual studies' results on MDFT, and so contributes to the knowledge about treatment of young drug abusers and their families.
The review informs practice by exploring whether results indicate that MDFT works better for some client groups than others based on characteristics such as age, gender, minority background, family composition (e.g., single parents), and co-occurring conditions. As previous reviews (e.g. Waldron & Turner 2008) indicate that individual treatment outcomes vary widely within intervention models, it is important to investigate who might benefit the most from MDFT. The hypothesis is that MDFT is not similarly efficacious for all client groups and the review investigates whether it is possible to identify subgroups that benefit more than others.
2 Objective of the review
The aim of this review was to evaluate current evidence about the effects of MDFT on drug abuse reduction for young people (aged 11-21 years) in treatment for non-opioid drug abuse. Further objectives of this review were, if possible, to examine the moderators of drug abuse reduction effects and to examine if MDFT works better for particular groups.
3 Methods
3.1 TITLE REGISTRATION AND REVIEW PROTOCOL
The title for this systematic review was registered in The Campbell Collaboration on 28.07.2011. The review protocol was registered on 01.09.2012. Both the title registration and the protocol are available at:
3.2 CRITERIA FOR CONSIDERING STUDIES FOR THIS REVIEW
3.2.1 Types of studies
The study designs eligible for inclusion in the review were: Controlled trials (in which all parts of the study are prospective, i.e. recruitment of participants, assessment of baseline, allocation to intervention, selection of outcomes and generation of hypotheses, see Higgins & Green, 2008) randomized controlled trials (RCTs); QRCTs - quasi-randomized controlled trials (QRCTs), where participants are allocated by means such as alternate allocation, person's birth date, the date of the week or month, case number or alphabetical order; NRCTs - non-randomized controlled trials (NRCTs), where participants are allocated by other actions controlled by the researcher such as location difference or time difference.
3.2.2 Types of participants
The population included in this review was young people aged 11-21 years enrolled in manual based MDFT drug treatment for non-opioid drug abuse (e.g., cannabis, amphetamine, ecstasy or cocaine).
Definitions of young people, and the age at which a person is considered a young person and may be entitled to special services such as drug treatment, varies internationally (United Nations, 2011). Age group distinctions for young people are unclear as the boundaries are fluid and culturally specific (Weller, 2006). Furthermore, young people start experimenting with illegal drugs at different ages in different countries (Hibell et al., 2009) and the pattern of movement from dependence on parents to independent living vary internationally. In order to capture international differences, we have set the age range from 11 to 21 years (Danish Youth Council, 2011; Hibell et al., 2009; United Nations, 2011; SAMHSA, 2010).
We included only interventions delivered in an outpatient setting in order to evaluate the effects of MDFT on youths living with their families, since family interactions are fundamental to MDFT.
We defined the population as young people referred to or in treatment for using non-opioid drugs. No universal international consensus exists on categories which should be used when classifying drug abusers, and different assessment tools and ways of classifying the severity of drug abuse are applied in different research studies (American Psychiatric Association, 2000; World Health Organization (WHO), 2011; Nordegren, 2002). We included all participants, regardless of any formal drug abuse diagnosis. The main criterion for inclusion was that the young person was enrolled to participate in the treatment (i.e. the intervention or a comparison condition). Referral to and enrolment in drug abuse treatment suggests a level of drug abuse such that a significant other or authority (or the young person themselves) has found it necessary to seek treatment.
3.2.3 Types of interventions
The review included outpatient manual-based MDFT interventions of any duration delivered to young people and their family (see 1.2, Description of the intervention). The MDFT interventions were required to be interventions that did not include overnight stays in a hospital or other treatment facility.
We did not include any studies where the young drug abuser had been placed outside the family home (e.g. inpatient treatment or incarceration in a locked facility); this is because MDFT is a family intervention requiring the active participation of the young drug abuser and his or her family with the aim of improving family functioning, and the core condition of the program would be seriously compromised if the young person was not residing within the family home.
Eligible control and comparison conditions included no intervention, waitlist controls and alternative interventions, as we were interested in both absolute and relative effects. Due to ethical considerations and the nature of the problem (i.e., young peoples' drug abuse), we anticipated the likelihood of finding a no treatment control group to be small.
3.2.4 Types of outcomes
The primary outcome of interest to this review was abstinence or reduction of drug abuse, as the overall review question is to evaluate current evidence on MDFT's effects on drug abuse reduction for young people in treatment for drug abuse. We sought evidence on how to best to reduce or eliminate drug abuse, as here it is drug abuse that is understood as the young person's primary problem.
Primary outcome(s)
Abstinence or reduction of drug abuse as measured by, for example: biochemical test (e.g. urine screen measures for drug abuse), self-reported estimates on drug abuse (e.g. Time-line Follow Back interview; Sobell & Sobell, 1992), or psychometric scales (e.g. Addiction Severity Index; McLellan, Luborsky, Woody & O'Brien, 1980).
In addition to the primary outcome of interest, we looked for the following secondary outcomes, but did not exclude studies on the basis of whether they reported any of these outcomes.
Secondary outcomes
Family functioning (e.g. measured by the Beavers Interactional Competence Scale; Beavers & Hampson, 2000). Education or vocational involvement (e.g. measured by grade point average, attendance, self-reported or reported by authorities, files, registers, or employment record.) Retention (e.g. measured by days in treatment, completion rates and/or attrition rates) Risk behavior, such as crime rates, prostitution (e.g. measured by self-reports or reports by authorities, administrative files, registers) Other adverse effects (e.g. measured by rates of hospitalization, suicide and over-doses).
3.3 SEARCH METHODS FOR IDENTIFICATION OF STUDIES
3.3.1 Electronic searches
The following bibliographic databases were searched: Medline, searched to October, 2014 Embase, searched to October, 2014 CINAHL, searched to October, 2014 Social Science Citation Abstracts, searched to October, 2014 Science Citation Abstracts, searched to October, 2014 SocINDEX, searched to October, 2014 PsycINFO, searched to October, 2014 Cochrane library, searched to October, 2014 Bibliotek.dk, searched to October, 2014 LIBRIS, searched to October, 2014 BIBSYS, searched to October, 2014 Social Care Online, searched to October, 2014 ERIC, searched to October, 2014 SweMed+, searched to October, 2014 Criminal Justice Abstracts, searched to October, 2014 Bibliography of Nordic Criminology, searched to December, 2008
3.3.2 Search terms
An example of the search strategy for MEDLINE (Ovid platform) is listed below. This strategy was modified for each of the databases searched (see appendix). MDFT .af. Multi-dimens* adj1 Famil*.af. Multidimens* adj1 Famil*.af. Multi adj1 dimens* adj1 Famil*.af. 1-4/or
3.3.3 Searching other resources
We checked the reference lists of relevant reviews and of reports of the five included primary studies for new leads. We also contacted ten international experts (Gayle Dakof, Lori Whitten, Minda Lynch, Kathleen Carroll, Debra Davis, Bernadette Christensen, Patricia Chamberlain, Brenna Bry, Henk Rigter and Bethany Kleine) in attempt to identify unpublished and on-going studies. Two studies were suggested but were rejected because they failed to meet the inclusion criteria.
3.3.4 Hand search
The following international journals were hand searched from 2011 to the time of review submission: Addiction Journal of Consulting and Clinical Psychology Journal of Substance Abuse Treatment Journal of Clinical and Adolescent Psychology Research on Social Work Practice
3.3.5 Grey literature
We made additional searches of Google and Google Scholar and checked the first 150 hits. European grey literature was searched using OpenGrey (http://www.opengrey.eu/). We made copies of relevant documents and recorded the exact URL and date of access. We also searched the following sites: The National Institute on Drug Abuse (NIDA)
3.4 DATA COLLECTION AND ANALYSIS
3.4.1 Selection of studies
One reviewer (MS) and one member of the review team (SLO) independently read titles and available abstracts of reports and articles identified in the search to exclude reports that were clearly irrelevant. Citations considered relevant by at least one reviewer were retrieved in full text versions. If there was insufficient information in the title and abstract to judge relevance, the full text was retrieved. One review author (PSR) and one member of the review team (SLO) read the full text versions to ascertain eligibility based on the selection criteria. Any disagreements about eligibility were resolved by discussion and consultation with a third reviewer (KK). Reasons for exclusion have been documented for each study retrieved in full text, and stored electronically. The study inclusion screening sheet was piloted and adjusted as required by the review authors and used throughout screening. The overall search and screening process is illustrated in a flow-diagram, see section 11.
3.4.2 Data extraction and management
One review author (PSR) coded the included studies, and a second reviewer (KK) checked the coding. The coding sheet was piloted on several studies (see the review protocol; Rasmussen et al., 2012). Numeric data extraction was carried out by one review author (TF) and checked by a member of the review team (ADK). Data and information were extracted on: characteristics of participants (e.g. age, gender, and drug abuse history), intervention characteristics and control conditions, research design, sample size, outcomes and results. Extracted data was stored electronically.
3.4.3 Assessment of risk of bias in included studies
We assessed the methodological quality of studies using a risk of bias model developed by Prof. Barnaby Reeves in association with the Cochrane Non-Randomized Studies Methods Group (Reeves, Deeks, Higgins, & Wells, 2011) 6 . This model, an unpublished extension of the existing Cochrane Collaboration's risk of bias tool (Higgins & Green, 2008), covers both risk of bias in RCTs and in NRCTs that have a well-defined control group.
The extended model is organized and follows the same steps as the existing Risk of Bias model according to the Cochrane Hand book, chapter 8 (Higgins & Green, 2008). The extension to the model is explained in the three following points: The existing Cochrane risk of bias tool needs elaboration when assessing non-randomized studies because, for non-randomized studies, particular attention must be paid to selection bias/risk of confounding. The extended model therefore specifically incorporates a formalized and structured approach for the assessment of selection bias in non-randomized studies
7
by adding an explicit item about confounding (Reeves, Deeks, Higgins & Wells, 2011). Another feature of non-randomized studies that make them at greater risk of bias compared to RCTs is that RCTs must have a protocol in advance of starting to recruit, whereas the protocol requirements for non-randomized studies are less consistent. The item concerning selective reporting therefore also requires assessment of the extent to which analyses (and potentially other choices) could have been manipulated to bias the findings reported, e.g. choice of method of model fitting, potential confounders considered/included. In addition the model includes two separate yes/no items asking reviewers whether they think the researchers had a pre-specified protocol and analysis plan. Finally the risk of bias assessment is refined, making it possible to discriminate between studies with varying degrees of risk. This refinement is achieved with the addition of a 5-point scale for certain items (see the following section Risk of bias judgment for details).
The refined assessment is pertinent when thinking of data synthesis as it operationalizes the identification of studies (especially in relation to non-randomized studies) with a very high risk of bias. The refinement increases transparency in assessment judgments and provides justification for not including a study with a very high risk of bias in the meta-analysis.
Risk of bias judgment items and assessment
The risk of bias model used in this review is based on 9 items:
The assessment was based on pre-specified questions (see section 9.3). “Yes” indicates a low risk, “No” indicates a high risk of bias, and “Unclear” indicates an unclear or unknown risk of bias. In the 5 point scale, 1 corresponds to No/Low risk of bias (e.g. 1 = a high quality RCT) and 5 corresponds to Yes/High risk of bias (e.g. 5= too risky, too much bias, i.e. a poor quality study). A judgment of 5 points on any of the items assessed translates to a risk of bias so high that the findings would not be considered in the data synthesis (because they are more likely to mislead than inform). None of the included studies were judged 5 on the risk of bias scale 8 .
Assessment
Reviewers (PSR,KK) independently assessed the risk of bias for each included study as described in the previous sections. Disagreements were resolved by discussion and consultation with a third reviewer with content and statistical expertise (TF). We reported the risk of bias assessment in risk of bias tables for each included study, see section 9.3.
3.4.4 Measures of treatment effect
Standardized mean differences (SMD) were used as the effect size metric for school grades, family functioning, drug abuse problem severity, and drug abuse frequency. Hedges g was used for estimating SMDs and the data used for these calculations were means, standard deviations and sample size.
Odds ratios were used as the effect size metric for retention, and the data used for these calculations were number of events and sample size. Computations were carried out with the natural logarithm of the odds ratio. Software used for statistical analyses was RevMan 5.0.
3.4.5 Unit of analysis issues
Multiple interventions per individual
We did not find any studies in which individuals received multiple interventions.
Multiple time points
Data from all follow-up durations reported in the primary studies were recorded. We used the time points 6 months post-intake and 12 months post-intake and performed separate analyses for these time points. We used the treatment termination and 6 month follow up outcome measure in two studies (Liddle, 2001, and Liddle, 2008b) as equivalents to the 6 and 12 months post-randomization time points.
Multiple intervention groups
Two studies (Liddle, 2001; Dennis, 2004) had two comparison groups with different individuals. As stated in the protocol, multiple control groups were not pooled. We performed separate analyses including the different control groups where these two studies provided relevant outcome measures.
Cluster randomized trials
No cluster randomized trials were included in this review.
3.4.6 Dealing with missing data and incomplete data
We assessed missing data and recorded attrition rates in the included studies. We were able to discern reasons for attrition from two of the studies (Liddle, 2009; Rigter 2011). None of the studies reported an intention-to-treat analysis, although Dennis 2004 provided data for all but two of the participants.
3.4.7 Assessment of heterogeneity
Heterogeneity among primary outcome studies was assessed with Chi-squared (Q) test, and the I-squared, and τ-squared statistics (Higgins, Thompson, Deeks, & Altman, 2003). Any interpretation of the Chi-squared test was made cautiously on account of its low statistical power.
3.4.8 Assessment of publication bias
Reporting bias refers to both publication bias and selective reporting of outcome data and results. We were unable to comment on the possibility of publication bias because there were insufficient studies for the construction of funnel plots. Selective reporting has been considered in the risk of bias assessment and any concerns reported in section 4.3.4.
3.5 DATA SYNTHESIS
None of the included studies were coded with 5 on the Risk of Bias 5 point scale (described in section 3.4.3), and no study was excluded from the data synthesis on this basis.
We did not find any studies comparing MDFT to no treatment or to untreated wait list controls, and so were unable to examine the absolute effects of MDFT. Our analysis of the relative effects of MDFT was conducted on studies that compared MDFT to other interventions and/or to treatment as usual (TAU). All follow-up durations reported in the primary studies were recorded. We performed separate analyses at 6 months and at 12 moths post intake.
All analyses were inverse variance weighted using random effects statistical models that incorporate both the sampling variance and between study variance components into the study level weights. Random effects weighted mean effect sizes were calculated using 95 percent confidence intervals. Graphical displays of effect sizes (forest plots) are provided in section 4.4.
3.5.1 Subgroup analysis, moderator analysis and investigation of heterogeneity
We did not identify sufficient studies to allow any moderator analysis to be conducted.
3.5.2 Sensitivity analysis
Sensitivity analysis was used to evaluate whether the pooled effect sizes were robust across components of risk of bias. We conducted a sensitivity analysis for the incomplete outcome data and other bias components of the risk of bias checklists by removing studies scoring 4 (see section 3.4.3 for a definition).
4 Results
4.1 RESULTS OF THE SEARCH
We ran the searches in June 2011 and October 2014. The results are summarised in the flow chart on page 107.
We identified 6,519 potential relevant records after excluding duplicates (database search, 1,425; grey search, 898; hand search, snowballing and other resources, 4,196).
All 6,519 records were screened based on title and abstract. Of these, 170 were retrieved and screened in full text. One hundred and fifty four records did not fulfil the screening criteria and were excluded. One paper from the snowball search was included. A total of five unique studies, reported in 16 papers, was included in the review. Further details of the included and excluded studies are provided in section 9.
4.2 DESCRIPTION OF THE STUDIES
4.2.1 Included studies
Five studies published in 16 articles between 2001 and 2014 met our inclusion criteria. Four were conducted in the US.
Design
All included studies were described by investigators as randomized controlled trials. Three employed a block randomized design (Dennis 2004; Liddle 2008; Rigter 2011), one study allocated participants using an urn procedure (Liddle 2009); and one study did not report the randomization procedure (Liddle 2001). Dennis 2004 used block randomization stratified on site (random allocation rule equivalent to one block). Dennis 2004 did not specify allocation ratio but it was probably 1:1 and did not specify the block size (s). Liddle 2008 used block size of 4 with allocation ratio 1:1. Rigter 2011 stratified on three or four variables (age, gender, level of drug abuse, ethnicity) and used block randomisation with randomly permuted blocks of 2 or 4 cases and an allocation ratio of 1:1. Liddle 2009 conducted random assignment using a balancing procedure to ensure equivalence of the groups on four key variables: gender, age, ethnicity and family income. No further details of the urn procedure were reported.
Two studies involved three arms (Dennis 2004 and Liddle 2001); the remaining three were, for the purpose of this review, two-armed intervention studies (Dennis 2004 described two trials, but only one trial dealing with three arms was relevant for this review).
Sample size
Overall, sample sizes were relatively large, with the number of participants randomised ranging from 83 (Liddle 2009) to 450 (Rigter 2011). The remaining studies comprised 182 (Liddle 2001), 224 (Liddle 2008), and 300 participants (Dennis 2004).
Participants
All five studies focused on the effects of manual-based MDFT for young people with substance abuse or dependence, mainly cannabis. Participants included in the review ranged from 11 to 18 year, with mean ages ranging from 13.7 to 16.3 years of age.
All investigators supplied data on gender and, with the exception of Rigter 2011, on family position. Three studies stated explicitly that an inclusion criterion was participants living with at least one parent (Liddle 2009, Liddle 2008, and Rigter 2011). Most participants included within the review were male, comprising between 73 to 83 per cent of the study populations in the primary studies. Approximately half of the participants were living in single parent households; these ranged from 48 to 58 percent of the study populations in the primary studies.
Participant characteristics
Intervention characteristics
All studies included outpatient manual-based MDFT intervention. The average duration ranged from 3-4 months (Dennis 2004 and Liddle 2009) to 6 months (Rigter 2011). The average number of sessions was 12-15 in Dennis 2004, 16-24 in Liddle 2001 and Liddle 2008, 24-32 in Liddle 2009 and 48 in Rigter 2011.
Comparison conditions
The three two-armed intervention studies (Liddle 2009, Liddle 2008 and Rigter 2011) all compared MDFT to CBT or CBT-informed interventions that were either individual or group-based. In Rigter 2011 the comparison treatments varied between the five participating countries, but had elements in common: predominantly CBT in Belgium and the Netherlands, psychodynamic approaches were included in France and Switzerland, and elements of both these pairs in Germany.
Duration and number of sessions was the same as for the MDFT in Liddle 2009 and Liddle 2008. In Rigter 2011 duration was the same as for MDFT, but the number of sessions was less than MDFT in all countries except Germany. In Dennis 2004, one comparison intervention was CBT-informed individual therapy but with a duration and number of sessions that was less than MDFT. The duration and number of sessions of the second comparison, Adolescent Community Reinforcement Approach (ACRA), was the same as MDFT, and four of the sessions included parents. In Liddle 2001, both comparison interventions were of the same duration as MDFT, involved the same number of sessions as MDFT and had a varying number of sessions including parents. The two comparison interventions were multifamily educational therapy (MEI) and adolescent group therapy (AGT).
Outcome measures
Outcomes measures included self-reported drug abuse and drug problem severity assessed via standardized measures: the Global Appraisal of Individual Needs, the Personal Experience Inventory and the Problem Oriented Screening Instrument for Teenagers.
One study, Liddle 2001, reported using a drug abuse classification scheme as the only measure of drug abuse reduction. Adolescent self-report, collateral reports (from parents), and urinalysis data were gathered for each adolescent. Information from these three data sources were assessed by three experienced clinician-raters and used to classify drug abuse consumption on a 15-point scale by the clinician-raters.
Two studies (Dennis 2004 and Liddle 2001) reported utilizing objective (urine samples) and collateral verification (parent report), of drug abuse.
Few secondary outcomes were reported. Education, measured by grade point averages and family functioning assessed via self-report and research assistant reports were provided in Liddle 2001 and Liddle 2009. Rigter 2011 reported adolescent self-reported family conflict and cohesion assessed via standardized measures. Delinquency data were provided by Liddle 2009, which were not included in the analysis for the reasons explained below. Rigter 2011, provided data on both self-reported and parent-reported externalizing symptoms assessed via standardized measures.
Regarding retention rates, the studies differed in the types of data they reported (completion rates and/or attrition rates, see section 9.1). We used the information reported in the five studies that came closest to the proportion of cases with fully completed treatment. As not all studies reported proportion of cases with 100% completion, the retention rate used for the individual studies varies between 50% and full completion. It is therefore possible to interpret only the difference between treatment and control groups; the level of retention could not be compared between studies. The numbers used for calculating retention rates are given in table 4.2.2.
Note 1: Completion varies across the individual studies with some reporting 50% completion of the planned dose of treatment and others reporting 100% completion of the planned dose of treatment.
Duration of follow-up observations
The outcomes were reported at varying time points. In three of the studies, termination, 6 month follow-up and 12 month follow-up data were available (Liddle 2001, Liddle 2008, and Liddle 2009). Dennis 2004 and Rigter 2011 provided 3, 6, 9 and 12 months post-intake data.
Independence
Three studies were conducted by MDFT program developers (Liddle 2001, Liddle 2008 and Liddle 2009); one study was ‘semi-independent’ (conducted by an independent investigator with the program developer as co-author, Dennis 2004); and one study was conducted by independent investigators (Rigter 2011).
4.2.2 Excluded studies
Many studies which appeared (by title or abstract) to be eligible did not ultimately meet our inclusion criteria. Some studies were excluded for more than one reason. Primary reasons for exclusion are listed below.
Reasons for exclusion
One study (Becker & Liddle, 2001) was a case study, focusing on single mothers. Diamond, Liddle, Hogue, & Dakof, 1999, was a process study focusing on alliance -- building. The outcomes of a prevention study were reported in Hogue et al, 2002. In Hogue et al, 1998, the focus was on treatment adherence; and the analysis was extended in Hogue et al, 2004. A multicomponent, multi-level technology transfer intervention developed to train staff was tested in Liddle, Rowe, Gonzalez, Henderson, Dakof & Greenbaum, 2001.
For further details on excluded studies, please see section 9.2, Characteristics of excluded studies.
4.3 RISK OF BIAS IN INCLUDED STUDIES
Overall, the included studies varied on risk of bias judgments and no single study could be characterised as a robust RCT with low risk of bias on all assessed risk of bias items.
The ratings of each study in relation to the nine domains in the Risk of Bias tool are listed below and summarized in Table 4.3 (see also section 3.4.3). The risk of bias judgments are based on pre-specified questions and a 5 point scale with ratings of 1=low risk and 5=high risk. Further details on risk of bias are provided in section 9.3, Risk of bias for individual included studies.
4.3.1 Allocation
All five included studies were randomized controlled trials. The methods of randomization were described in four studies (Rigter 2011, Liddle 2008, Dennis 2004 and Liddle 2009) and the method used for sequence generation was judged adequate in each case. Concerning allocation concealment, only one study mentioned the method used to achieve this (Dennis 2004), and one study simply stated that the allocation was concealed (Rigter 2011). It was not possible to judge whether concealment of allocation was adequate in the three remaining studies.
4.3.2 Blinding
As is common in social intervention, it is generally impossible to blind participants or those delivering the interventions. Only two studies clearly stated that outcome assessors were blinded to allocation status (Liddle 2001 and Liddle 2009).
4.3.3 Incomplete outcome data
Two studies had very low levels of missing data (Dennis 2004 and Liddle 2009), and two studies had relatively high levels (Liddle 2001 and Liddle 2008). All except one study (Liddle 2001) dealt with missing data, typically using latent growth curve modelling (however, the estimates of the latent growth curve models are not included in the meta-analyses in this review). Only one study (Dennis 2004) imputed missing data (see section 9.3).
4.3.4 Selective reporting
All studies reported data on the primary outcome reduction of substance abuse. Although Liddle 2009 did not provide data that enabled the calculation of effect sizes because only means and standard deviations of the natural log transformed variables were provided, the non-transformed data were kindly provided by Professor Howard Liddle. Two studies did not report all the secondary outcomes as planned in the protocol (Dennis 2004 and Rigter 2011). We could not locate a protocol for the remaining three studies.
4.3.5 A priori protocol and analysis plan
We were able to locate a protocol and an a priori analysis plan for two studies (Dennis 2004 and Rigter 2011).
4.3.6 Other potential sources of bias
The predictability of treatment assignment is an issue for all constrained randomization algorithms. This is particularly the case when blocked randomization or an urn procedure is used, and when the assignments are revealed subsequent to the person recruiting into the trial, it is sometimes possible to predict a future assignment, which implies a risk of bias 10 (Higgins & Green, 2008; Lachin, Matts & Wei, 1988; Berger, 2005). Consequently, none of the studies were rated 1 (low risk of bias) on this domain; Dennis 2004, Liddle 2008 and Rigter 2011 because block randomization was used, Liddle 2009 because an urn procedure was used, and Liddle 2001 because the randomisation procedure was not described. Confounding was not relevant in the review since we did not find any NRCTs meeting the inclusion criteria.
Risk of bias assessment
The RoB tool is provided in Section 12.3 and the detailed RoB assessment is given in Section 9.3. In the 5 point scale, 1 corresponds to Low risk of bias and 5 corresponds to High risk of bias.
4.4 EFFECTS OF THE INTERVENTIONS
MDFT was compared to other interventions in all the included studies, and so we were only able to analyse the relative effects of MDFT. Two studies, Liddle 2001, and Dennis 2004, had two comparison groups with different individuals, and we performed separate analyses including the different control groups where these two studies provided relevant outcome measures.
In Dennis 2004 one comparison intervention was CBT-informed individual therapy (MET/CBT5) and the second comparison was Adolescent Community Reinforcement Approach (ACRA). In Liddle 2001, the two comparison interventions were multifamily educational therapy (MEI) and adolescent group therapy (AGT).
Throughout this review, we have labelled the analyses (where relevant) as follows: 1A: 1 refers to AGT used as comparison in Liddle 2001 and A refers to MET/CBT5 used as comparison in Dennis 2004 1B: 1 refers to AGT used as comparison in Liddle 2001 and B refers to ACRA used as comparison in Dennis 2004 2A: 2 refers to MEI used as comparison in Liddle 2001 and A refers to MET/CBT5 used as comparison in Dennis 2004 2B: 2 refers to MEI used as comparison in Liddle 2001 and B refers to ACRA used as comparison in Dennis 2004
Liddle 2001 provided data that enabled the calculation of effect sizes for drug abuse problem severity, school grades, and retention. Dennis 2004 provided data that enabled the calculation of effects sizes for drug abuse problem severity, drug abuse frequency and retention.
The outcomes were reported at varying time points. We grouped the outcomes at 6 and 12 months post-randomization, using the termination and 6 month follow up outcome measure time point in Liddle 2001 and Liddle 2008 as equivalent to the 6 and 12 months post-randomization time points.
A summary of results is presented in the Table of comparisons, section 10.1, and forest plots are displayed in figures 4.1–4.22. The captions below the figures show whether results favour MDFT or the control group, and we will concentrate on the direction of effects in the text below.
4.4.1 Primary outcome results
It was possible to measure reduction of drug abuse by drug abuse frequency reduction as well as by reduction in drug abuse problem severity. One study, Liddle 2001, provided a drug abuse classification scheme as the only measure of drug abuse reduction. We judged that the drug abuse classification scheme compared best with the measures of drug abuse problem severity provided in the other studies.
All five studies thus provided data that enabled the calculation of comparable effect sizes on drug abuse problem severity reduction, while four studies provided data that enabled the calculation of comparable effect sizes on drug abuse frequency reduction. Drug abuse frequency and problem severity reduction are measured as decreases; hence a negative effect size favours MDFT.
Drug use problem severity 6 months post-intake
Three studies found statistically significant differences between treatments, all favouring MDFT (Liddle 2001, Liddle 2008 and Liddle 2009). In two studies there was no evidence of a statistically significant difference between treatments (Rigter 2011, and Dennis 2004). Pooled results showed a statistically significant effect of MDFT for drug abuse problem severity reduction. The random effects weighted standardised mean difference (SMD) for analysis 1A was -0.35 (95% CI -0.59 to -0.11, p=0.004), for analysis 1B SMD=-0.33 (95% CI -0.59 to -0.08, p=0.01), for analysis 2A SMD=-0.31 (95% CI -0.53 to -0.10, p=0.004) and for analysis 2B SMD=-0.30 (95% CI -0.53 to -0.07, p=0.01). There was a statistically significant heterogeneity of effects between studies in analysis 1A (τ2=0.04, Q= 10.12, df=4, p=0.04), analysis 1B (τ2=0.05, Q= 11.67, df=4, p=0.02) and analysis 2B (τ2=0.04, Q= 9.64, df=4, p=0.05). In analysis 2A there was no statistical significant heterogeneity (τ2=0.03, Q= 8.18, df=4, p=0.09). The forest plots are displayed in Figure 4.1–Figure 4.4.
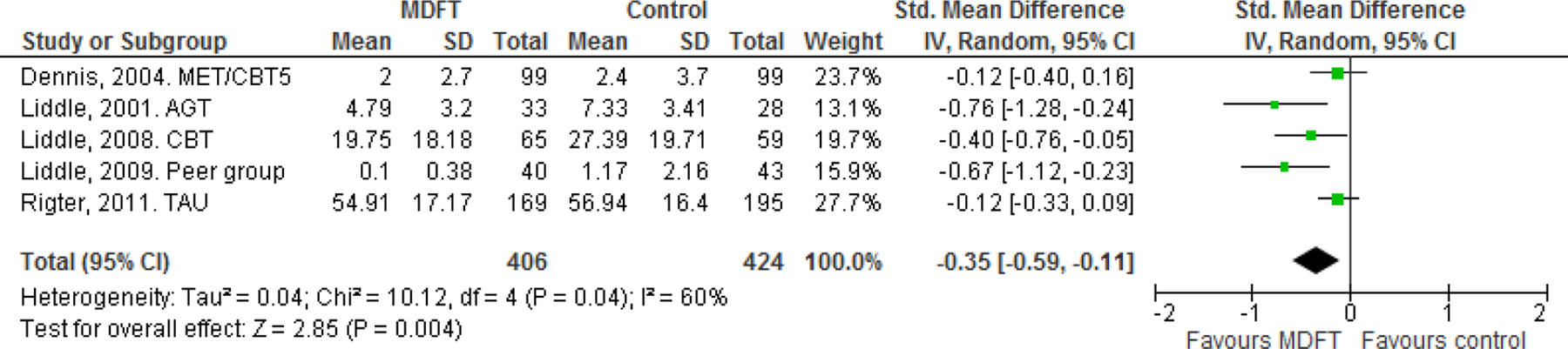
Drug abuse problem severity. 6 months post-intake 1A
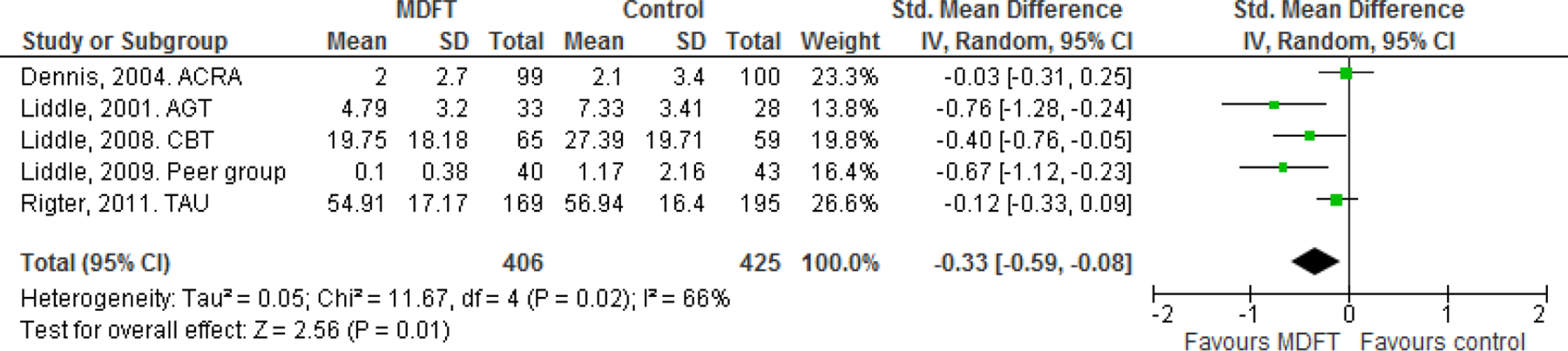
Drug abuse problem severity. 6 months post-intake 1B
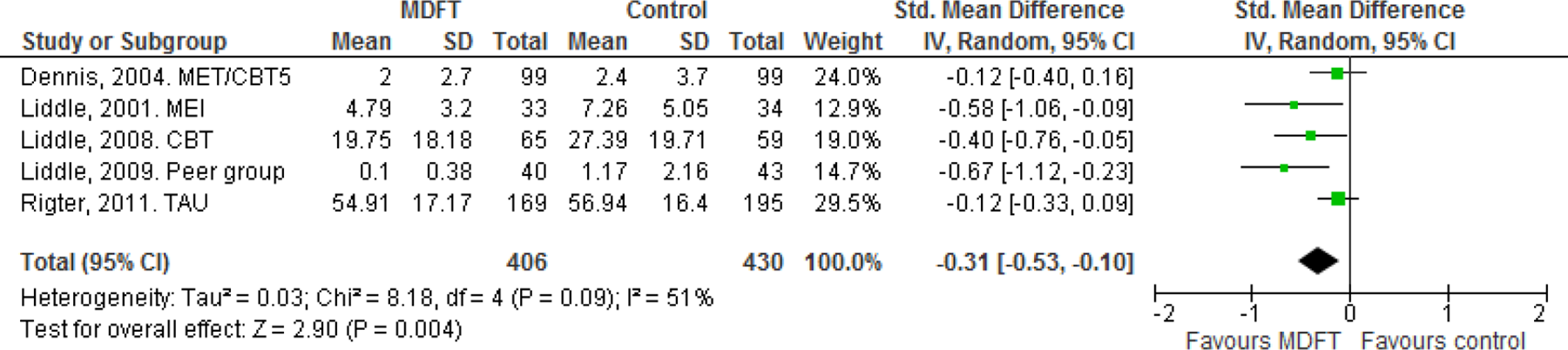
Drug abuse problem severity. 6 months post-intake 2A
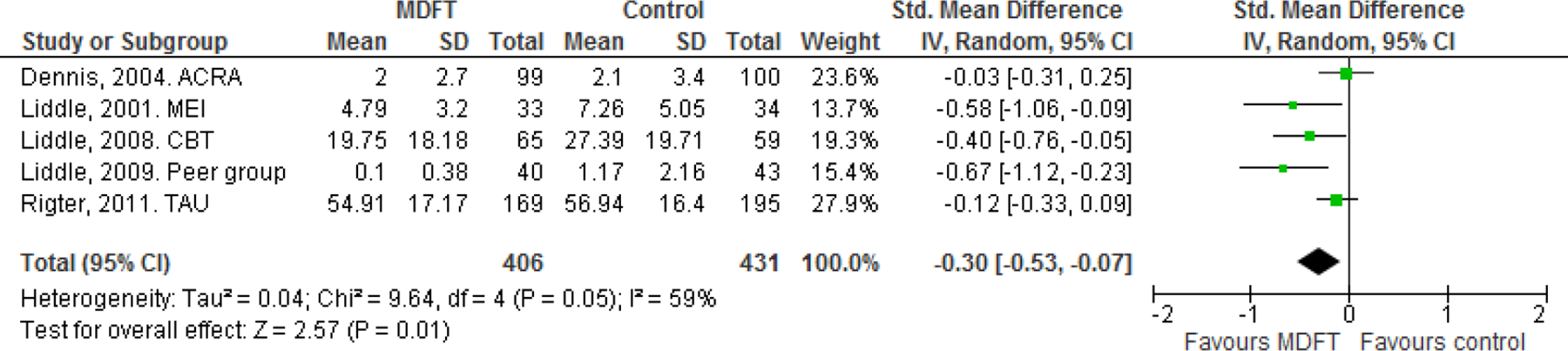
Drug abuse problem severity. 6 months post-intake 2B
Drug abuse problem severity 12 months post-intake
Two studies, Rigter 2011 and Liddle 2009, found a statistically significant difference between treatments, favouring MDFT, whereas in Dennis 2004, Liddle 2001, and Liddle 2008, the effect was not statistically significant. Rigter 2011 found an effect on drug abuse problem severity at 12 months, but not at 6 months; we have no explanation for this anomalous result.
Pooled results showed a statistically significant effect of MDFT for drug abuse problem severity reduction. The random effects weighted standardised mean difference (SMD) for analysis 1A was -0.25 (95% CI -0.39 to -0.10, p=0.0007), for analysis 1B SMD=-0.23 (95% CI -0.39 to -0.06, p=0.007), for analysis 2A SMD=-0.27 (95% CI -0.43 to -0.11, p=0.001) and for analysis 2B SMD=-0.25 (95% CI -0.43 to -0.07, p=0.007). Heterogeneity of effects among studies was not statistically significant in analysis 1A (τ2=0.00, Q= 4.19, df=4, p=0.38), analysis 1B (τ2=0.01, Q= 5.26, df=4, p=0.26), analysis 2A (τ2=0.01, Q= 4.97, df=4, p=0.29) and analysis 2B (τ2=0.01, Q= 6.17, df=4, p=0.19). The forest plots are displayed in Figure 4.5–Figure 4.8.

Drug abuse problem severity. 12 months post-intake 1A
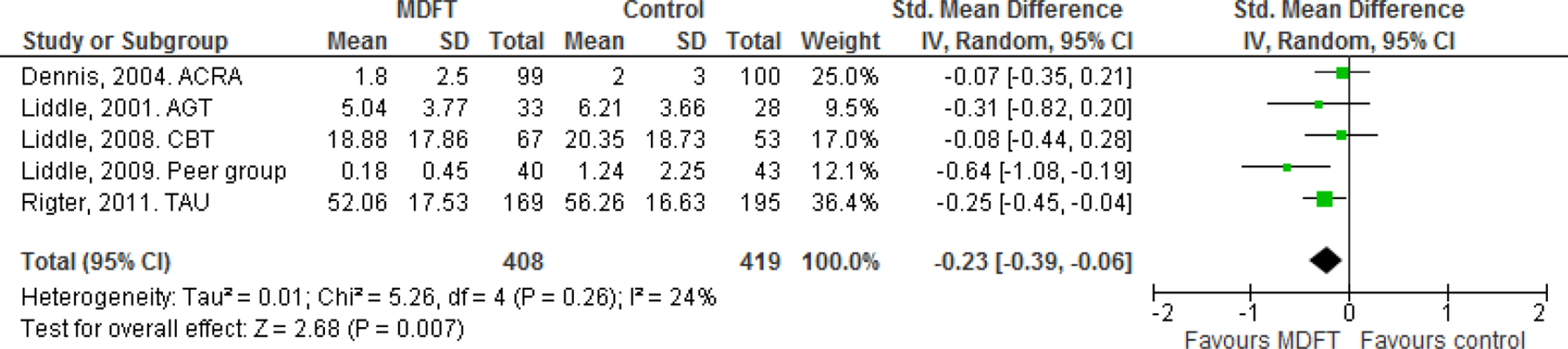
Drug abuse problem severity. 12 months post-intake 1B
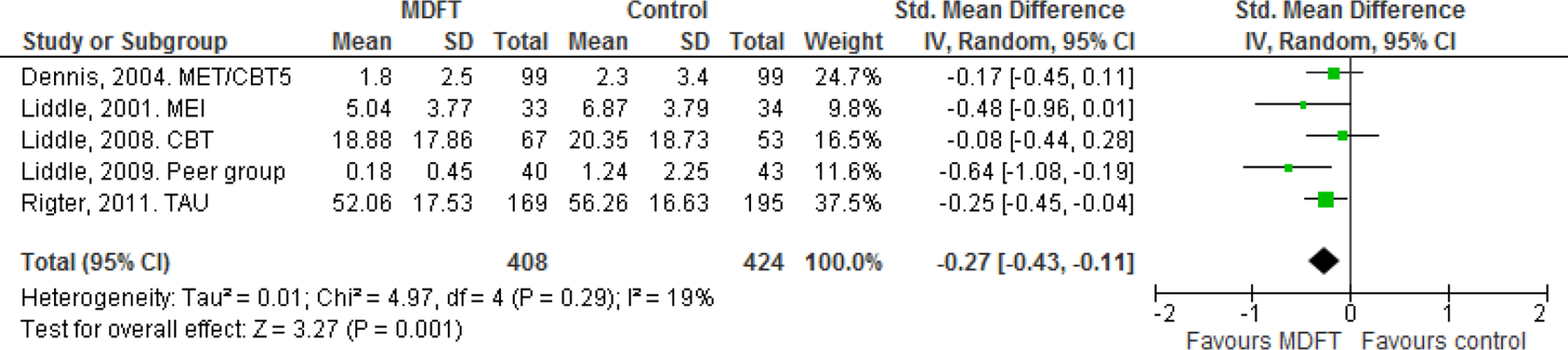
Drug abuse problem severity. 12 months post-intake 2A
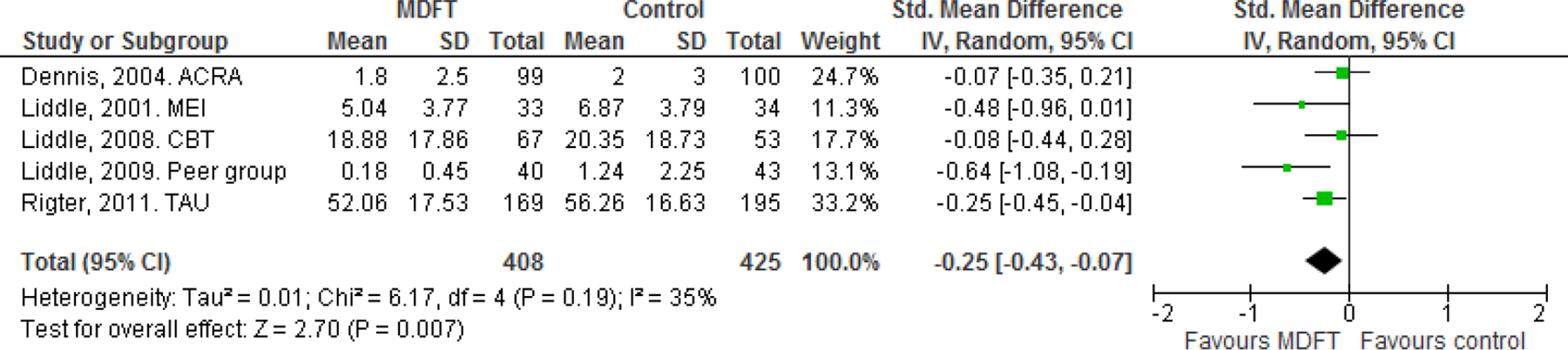
Drug abuse problem severity. 12 months post-intake 2B
Drug abuse frequency 6 months post-intake
Four studies reported data on the drug abuse frequency reduction. Three studies found a statistically significant effect that favoured MDFT (Liddle 2009, Rigter 2011 and Liddle 2008). In Dennis 2004, MDFT was not significantly different from the MET/CBT5 treatment or from ACRA treatment. Pooled results showed a statistically significant effect of MDFT for drug abuse frequency reduction. The random effects weighted standardised mean difference (SMD) for analysis A was -0.24 (95% CI -0.43 to -0.06, p=0.01), and for analysis B SMD=-0.25 (95% CI -0.40 to -0.11, p=0.0007). Heterogeneity of effects among studies was not statistically significant in analysis A (τ2=0.01, Q= 4.63, df=3, p=0.2) and analysis B (τ2=0.00, Q= 3.11, df=3, p=0.37). The forest plots are displayed in Figure 9 and Figure 4.10.
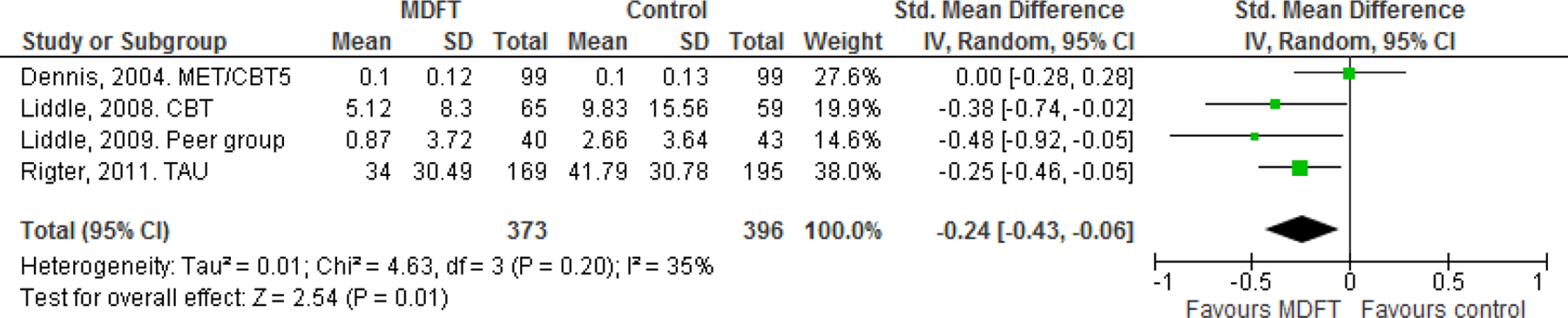
Drug abuse frequency. 6 months post-intake A
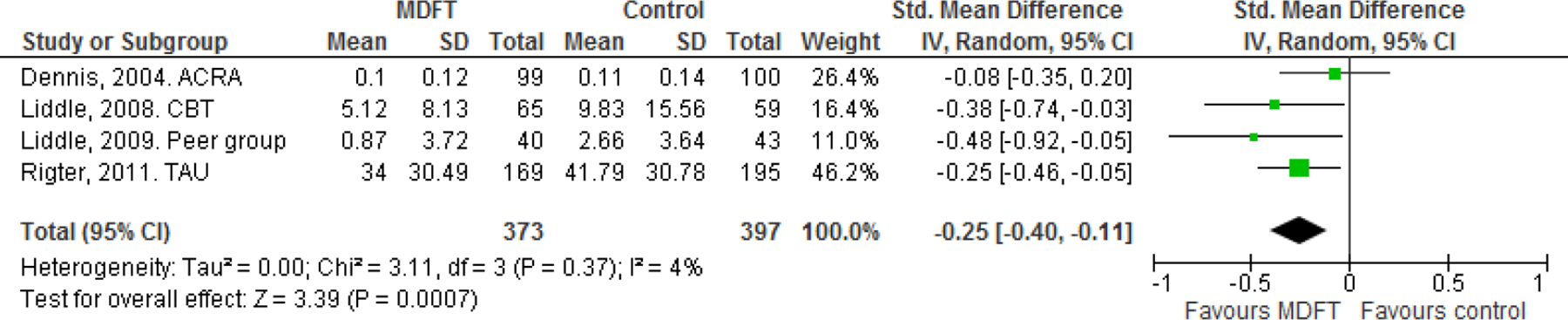
Drug abuse frequency. 6 months post-intake B
Drug abuse frequency 12 months post-intake
Two studies (Rigter 2011 and Liddle 2009) found a statistically significant effect that favoured MDFT, whereas the differences between treatments in Liddle 2008 and in Dennis 2004 were not statistically significant. Pooled results showed no statistically significant effect of MDFT for drug abuse frequency reduction. The random effects weighted standardised mean difference (SMD) for analysis A was -0.28 (95% CI -0.63 to 0.07, p=0.11), and for analysis B SMD=-0.28 (95% CI -0.63 to 0.07, p=0.11). There was a statistically significant heterogeneity of effects among studies in analysis A (τ2=0.10, Q= 15.43, df=3, p=0.001) and analysis B (τ2=0.10, Q= 15.45, df=3, p=0.001). The forest plots are displayed in Figure 4.11 and Figure 4.12.
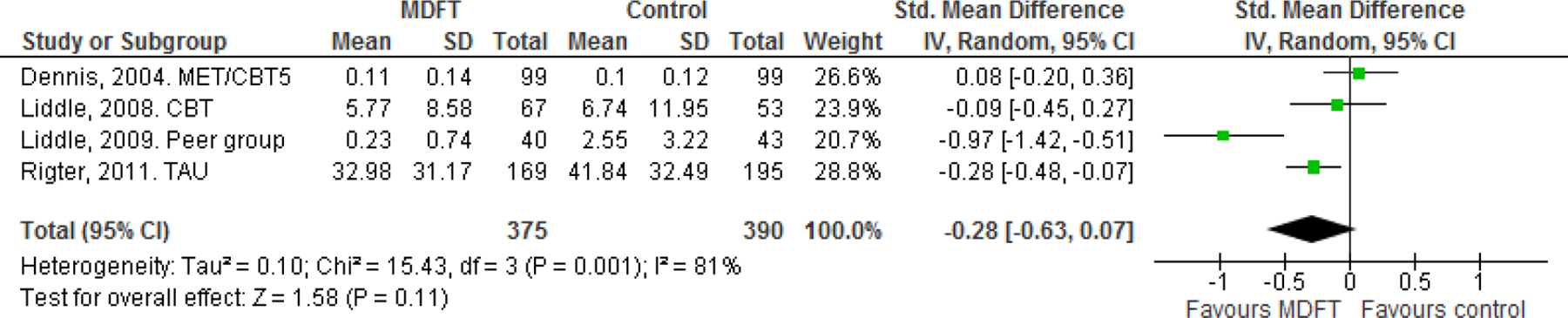
Drug abuse frequency. 12 months post-intake A
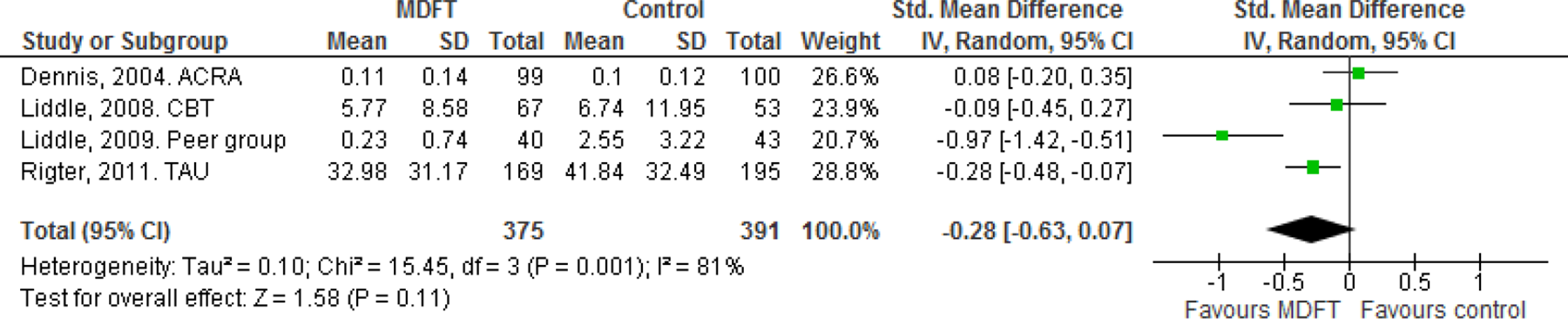
Drug abuse frequency. 12 months post-intake B
4.4.2 Secondary outcome results
Family functioning
It was not possible to perform a meta-analysis on family functioning. One study, Liddle 2001, used a rating scale that assessed the degree of family functioning from 1 (optimal functioning) to 10 (severely dysfunctional). Family functioning was measured as a decrease; hence a negative effect size favours MDFT. Results showed no significant differences between MDFT and the MEI treatment either at 6 months post-intake, SMD =0.25 (95% CI -0.23, 0.73), or at 12 months post-intake, SMD =-0.34 (95% CI -0.82, 0.15). Results showed no significant differences between MDFT and the AGT treatment at 6 months post-intake but a significant difference which favored MDFT at 12 months post-intake; SMD =-0.30 (95% CI -0.80, 0.21) at 6 months post-intake and SMD =-1.26 (95% CI -1.81, -0.70) at 12 months post-intake, respectively.
Liddle 2009 measured family functioning in terms of family interactions, measuring them separately as positive and as negative family interactions respectively. Results showed no significant differences between MDFT and the peer group comparison; SMD =-0.09 (95% CI -0.52, 0.34) at 6 months post-intake, SMD =0.13 (95% CI -0.30, 0.56) at 12 months post-intake for positive family interactions, and SMD = -0.26 (95% CI -0.69, 0.17) at 6 months post-intake, and SMD =-0.25 (95% CI -0.69, 0.18) at 12 months post-intake for negative family interactions.
Rigter (2011) reported on family functioning measured in terms of conflict and cohesion 11 . Results showed no significant differences between MDFT and the TAU comparison; SMD =0.14 (95% CI -0.07, 0.35) at 6 months post-intake, SMD =0.19 (95% CI -0.01, 0.41) at 12 months post-intake for family conflict, SMD =-0.15 (95% CI -0.36, 0.06) at 6 months post-intake, and SMD =-0.16 (95% CI -0.36, 0.05) at 12 months post-intake for family cohesion.
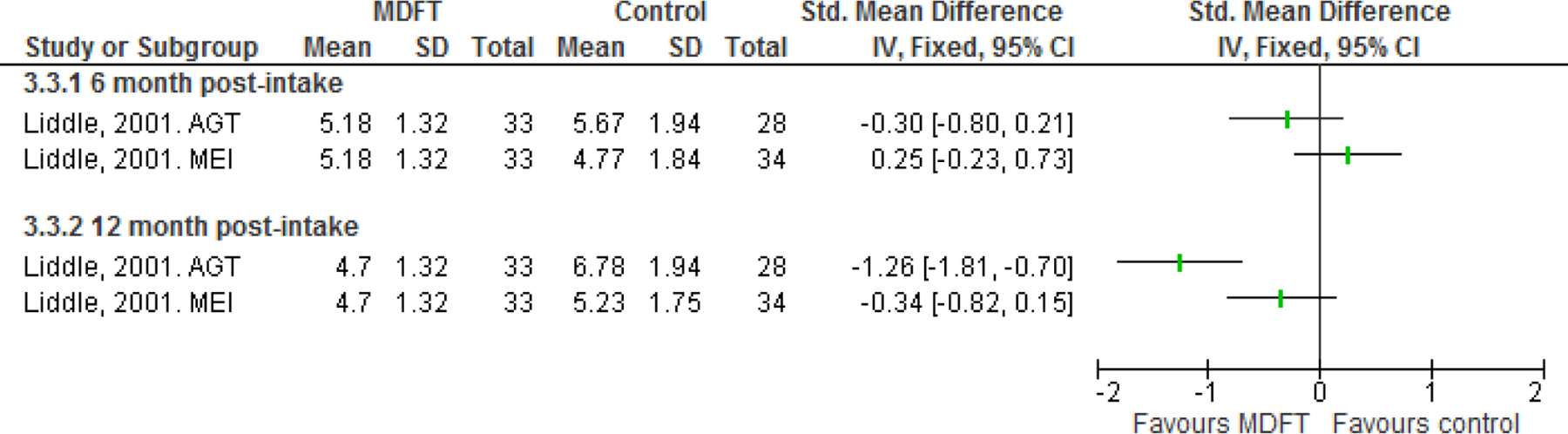
Family functioning.
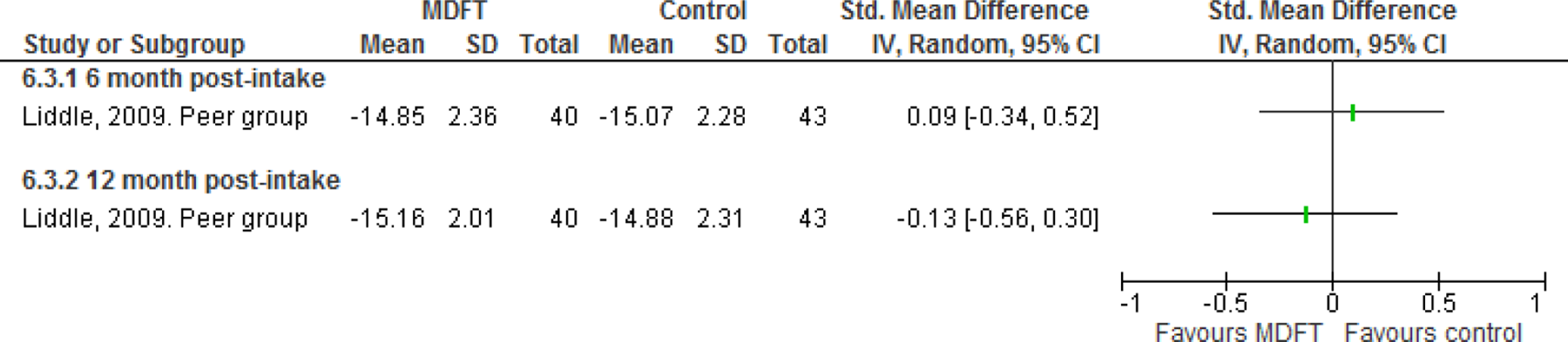
Positive family interaction.
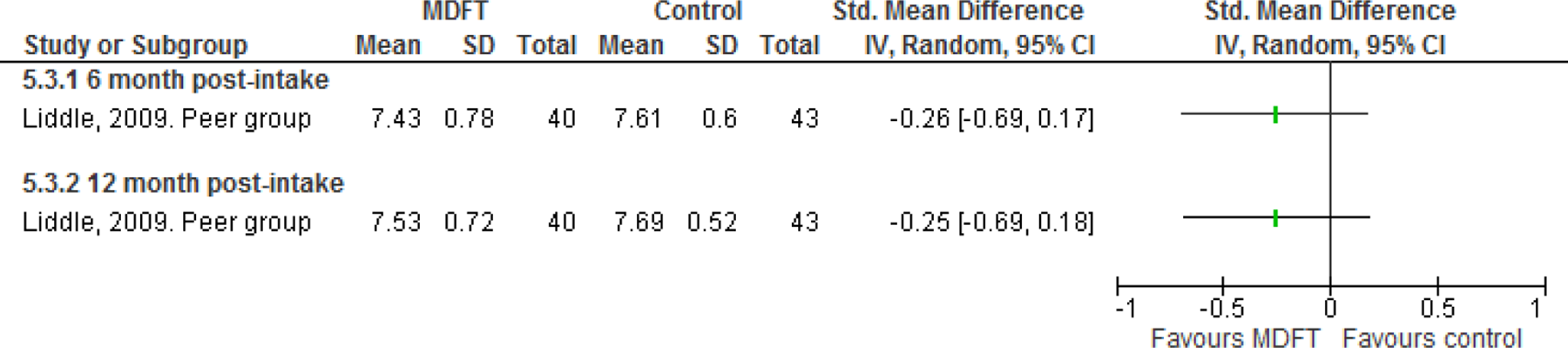
Negative family interaction.
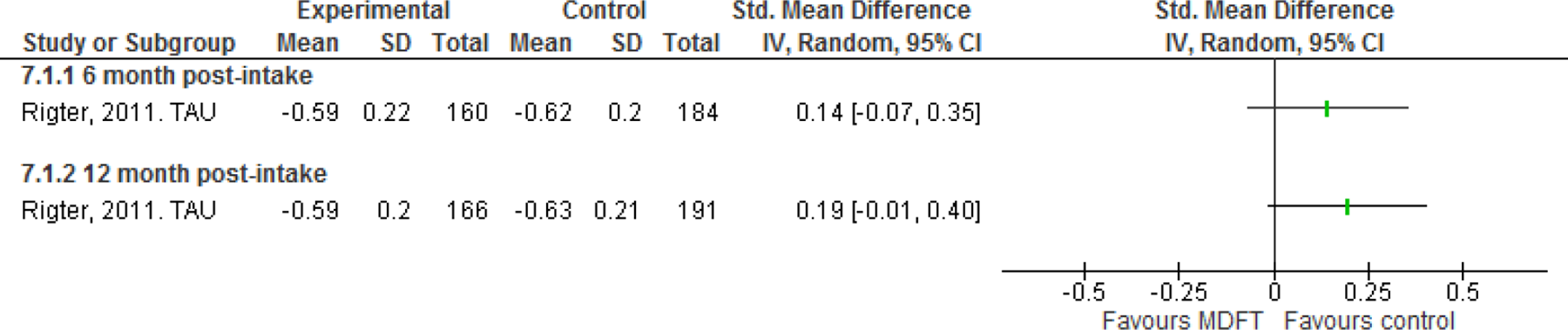
Family conflict.
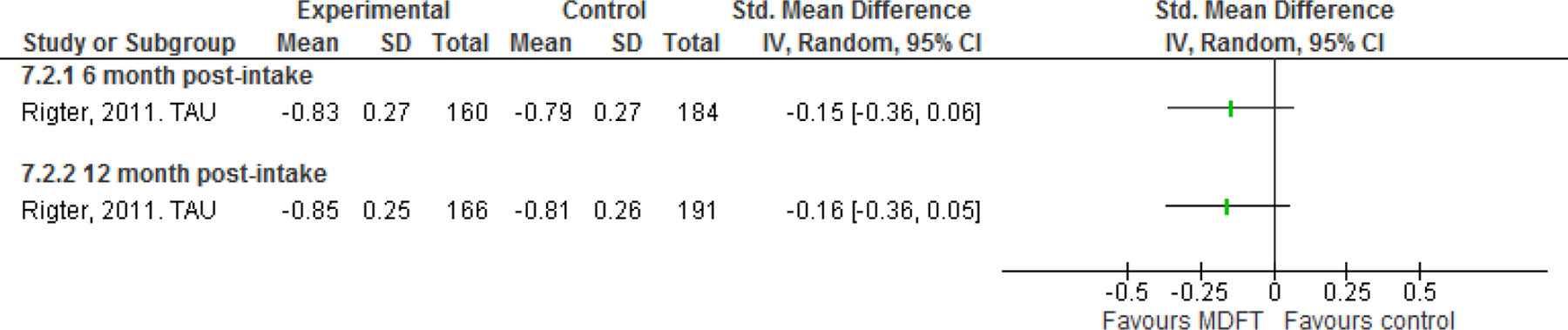
Family cohesion.
Education or vocational involvement
Two studies (Liddle 2001, and Liddle 2009) provided data that enabled the calculation of an effect size for the education outcome as measured by grade point average.
Grade point average 6 months post-intake
Grade point is measured as a decrease; hence a negative effect size favours MDFT. One study (Liddle 2009) found statistically significant differences that favored MDFT, whereas the differences in Liddle 2001 study were not statistically significant. Pooled results did not show a statistically significant effect of MDFT for school grade improvement when using the AGT comparison in the Liddle 2001 and a marginal statistically significant effect when using the MEI comparison in Liddle 2001. The pooled estimate were SMD =0.38 (95% CI -0.25, 1.01) and SMD =0.47 (95% CI 0.01, 0.92). There was no statistically significant heterogeneity between studies in any of the analyses (τ2=0.15, Q= 3.54, df=1, p=0.06 and τ2=0.05, Q= 1.96, df=1, p=0.05). However, effect sizes differ markedly and with only two studies the power to detect heterogeneity is very low.

Grade point average. 6 months post-intake 1

Grade point average. 6 months post-intake 2
Grade point average 12 months post-intake
No data were provided.
Retention
We used the information reported in all five studies that came closest to the proportion of cases with full completed treatment. Results were measured as odds ratio (OR) non-event, implying that an OR of less than one favours MDFT.
Three studies (Liddle 2008, Liddle 2001 and Dennis 2004) found no difference between retention rates. In the remaining two studies, the difference between retention rates between treatments favored MDFT (Rigter 2011 and Liddle 2009) and was statistically significant. Note that the magnitudes of the effect sizes of these two studies and the width of the confidence intervals were quite distinct from the three other studies (Liddle 2001, Liddle 2008 and Dennis 2004).
Pooled results showed a statistically significant effect of MDFT for retention when using the AGT comparison in Liddle 2001, but the effect was not statistically significant when using the MEI comparison in Liddle 2001.
The random effects weighted odds ratio (OR) for analysis 1A was 0.44 (95% CI 0.21 to 0.94, p=0.03), for analysis 1B OR=0.45 (95% CI 0.21 to 0.95, p=0.04), for analysis 2A OR=0.48 (95% CI 0.22 to 1.05, p=0.07) and for analysis 2B OR=0.49 (95% CI 0.22 to 1.07, p=0.07). There was statistically significant heterogeneity of effects among studies in analysis 1A (τ2=0.54, Q= 21.92, df=4, p=0.0002), analysis 1B (τ2=0.55, Q= 22.15, df=4, p=0.0002), analysis 2A (τ2=0.60, Q= 23.80, df=4, p<0.0001) and analysis 2B (τ2=0.60, Q= 23.97, df=4, p<0.0001). The forest plots are displayed in Figure 4.18–Figure 4.21.
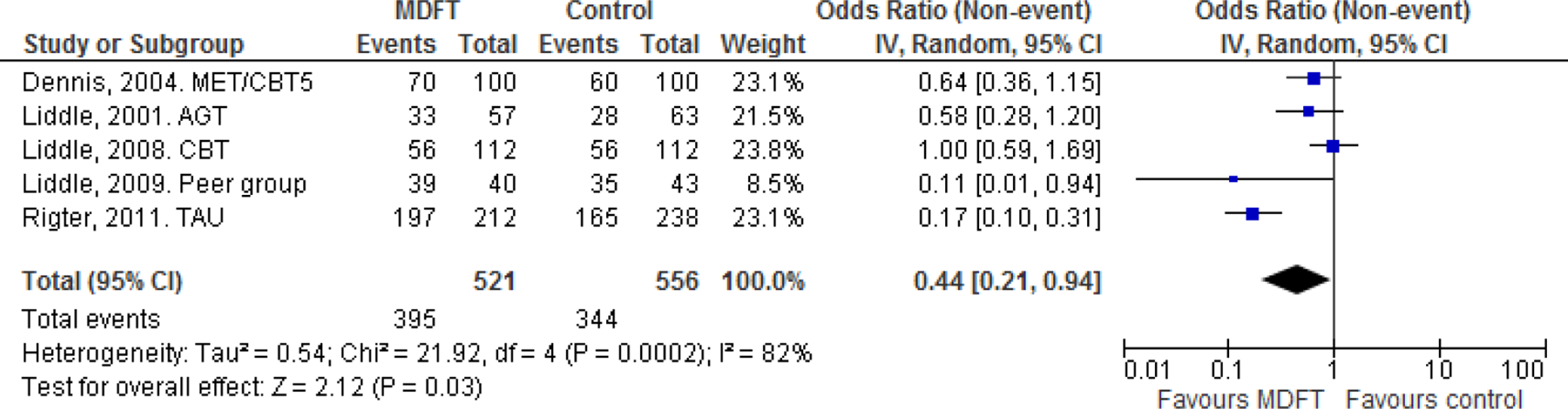
Retention.1A
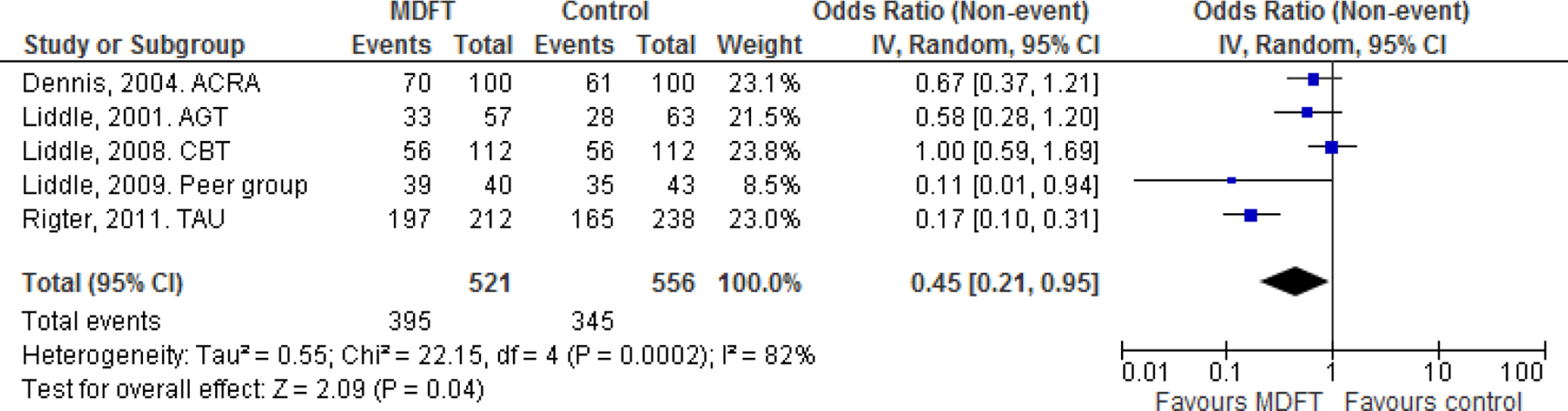
Retention.1B
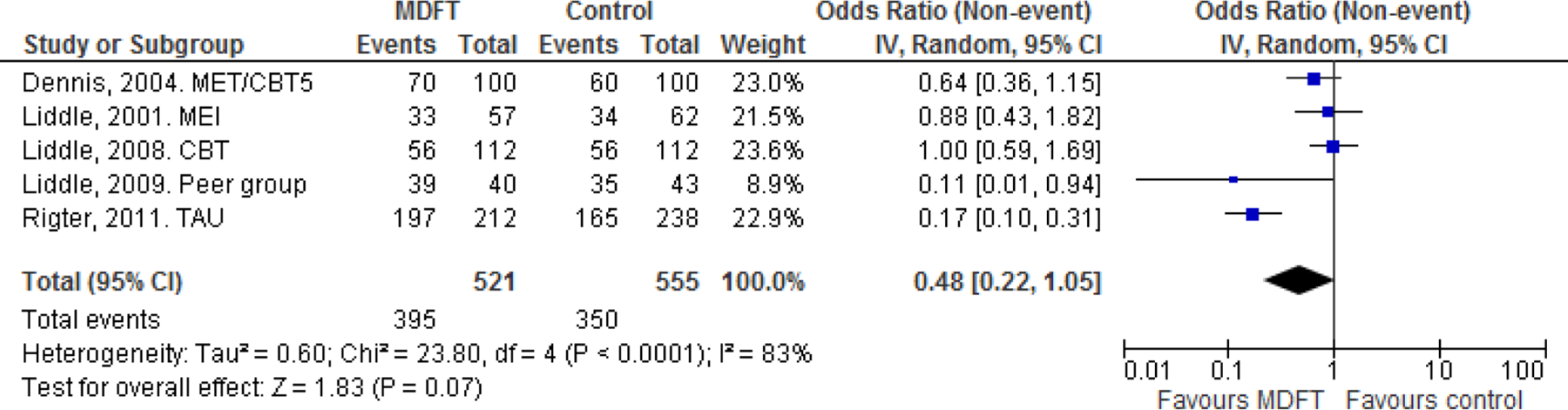
Retention.2A
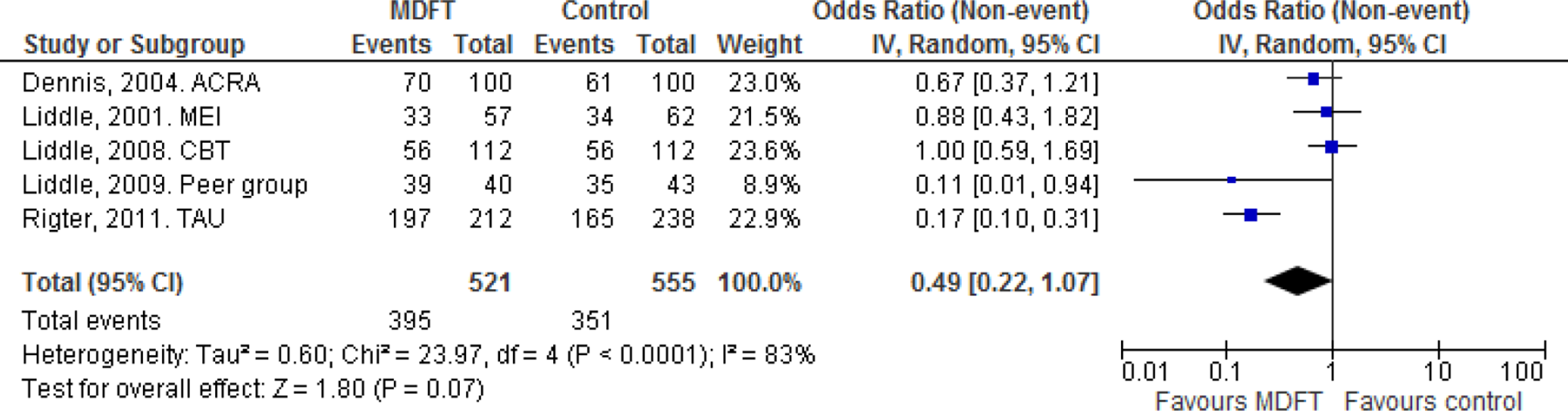
Retention.2B
Risk behavior
One study, Rigter 2011, provided data on externalizing disorders/symptoms (e.g. aggression and delinquency) measured by the Youth Self-report and the Child Behavior Checklist. Results showed no significant differences between MDFT and TAU on either of the scales; SMD =-0.02 (95% CI -0.23, 0.18) at 6 months post-intake and, SMD =-0.02 (95% CI -0.22, 0.19) at 12 months post-intake for the YSR scale; SMD =-0.01 (95% CI -0.20, 0.22) at 6 months post-intake and SMD =-0.02 (95% CI -0.23, 0.19) at 12 months post-intake for the CBCL scale.
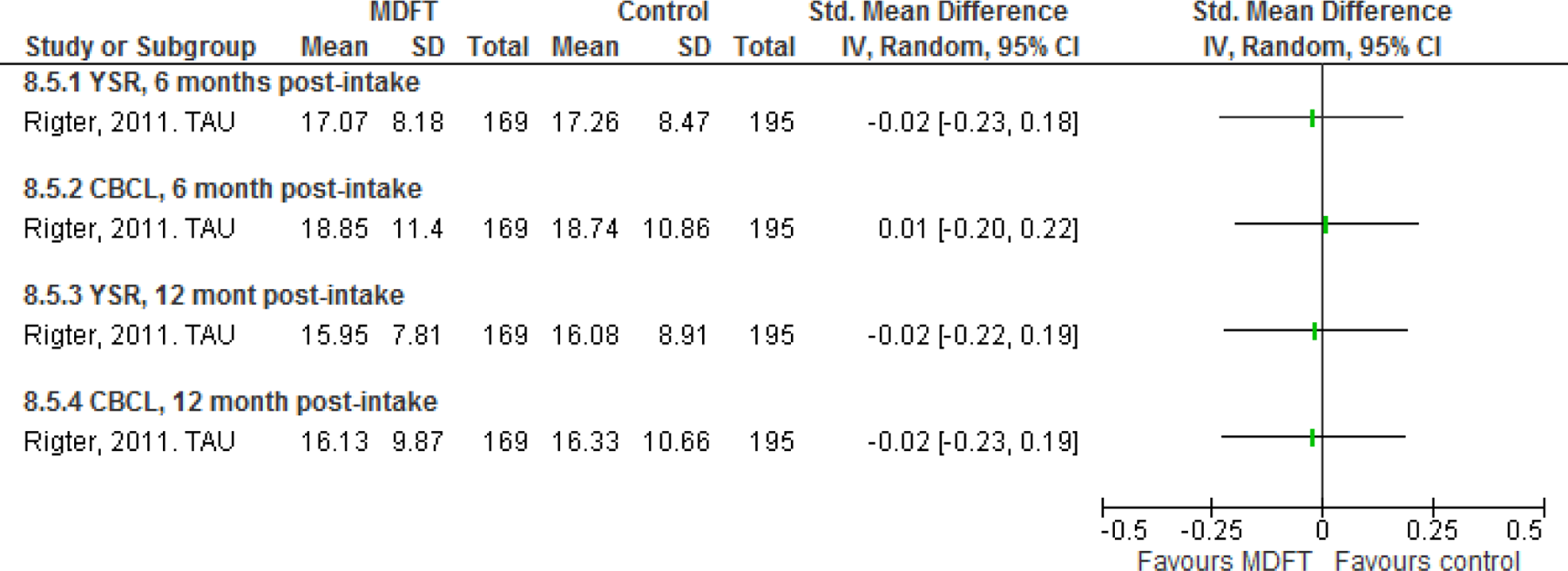
Externalizing symptoms.
One other study, Liddle 2009, provided delinquency measures. No significant differences between MDFT and peer group were found at either at 6 months post-intake, SMD =-0.28 (95% CI -0.71, 0.16), or at 12 months post-intake, SMD =-0.33 (95% CI -0.76, 0.10).
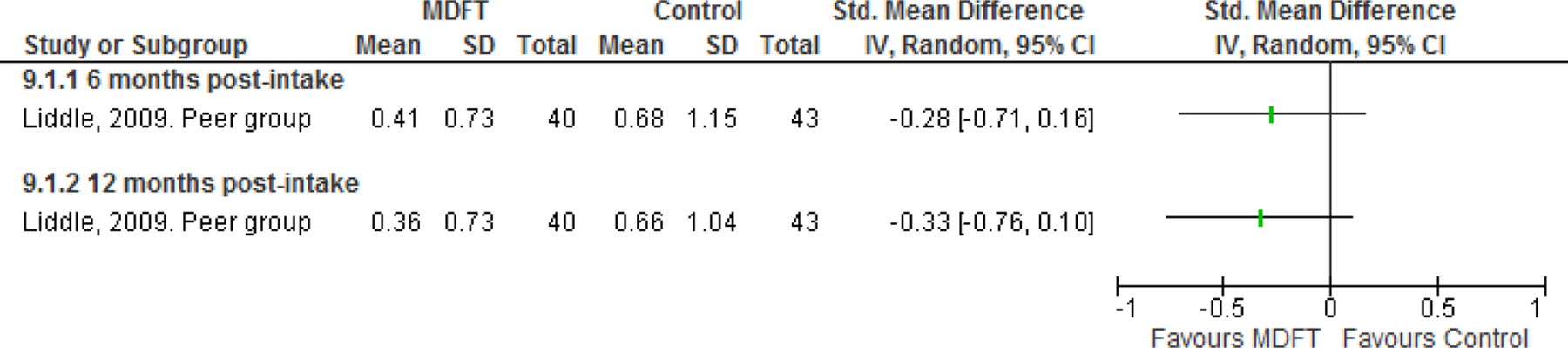
Delinquency
Other adverse effects
No other adverse effects (such as rates of hospitalization, suicide or over-doses) were provided in any of the five studies.
4.4.3 Sensitivity analysis
Sensitivity analyses were performed for the primary outcomes; drug abuse problem severity and drug abuse frequency. We examined the robustness of conclusions when the studies scoring 4 on the incomplete outcome data item (Liddle 2001 and Liddle 2008) and the other bias item (Liddle 2008 and Rigter 2011) respectively were removed from the analyses. The results are displayed in table 4.4.1 and 4.4.2.
Sensitivity analyses, drug abuse problem severity.
For drug abuse problem severity, the SMD remains statistically significant and still favours MDFT for most of the comparisons at the 12 post-intake when the studies scoring 4 are removed. However, the effect becomes no longer significant at 6 months post-intake when studies scoring 4 on the incomplete outcome data item are removed. The relative reduction remains significant and becomes larger for two of the contrasts (1A & 2A) at 6 months post-intake when studies scoring 4 on the other bias item are removed.
In both cases the relative reduction becomes marginally smaller at 12 months post-intake. As expected, when studies are removed from the analysis the confidence intervals become wider; there is however considerably overlap between confidence intervals (a graphical display is given in section 11). At 6 months post-intake, the results (with one exception 12 ) are no longer statistically significant whereas they are still statistically significant at the 12 post-intake (with two exceptions 13 ).
Sensitivity analyses, drug use frequency.
For drug use frequency, the SMD ceases to be statistically significant for most of the comparisons when studies scoring 4 are removed.
At 6 months post-intake, the results are no longer statistically significant when the comparison used in Dennis 2004 is MET/CBT5 whereas they are still statistically significant when the comparison used in Dennis 2004 is ACRA.
5 Discussion
5.1 SUMMARY OF THE MAIN RESULTS
Our main objective was to evaluate the current evidence on the effect of MDFT on drug abuse reduction for young people in treatment for non-opioid drug abuse. Further objectives of this review were to examine the moderators of drug abuse reduction effects and to examine whether MDFT works better for particular groups. Unfortunately it was not possible to assess this second review objective because of the limited number of studies.
Five randomized controlled trials of MDFT met the inclusion criteria for this review. All five studies compared MDFT to other treatments, mainly CBT or ‘CBT-informed’ interventions, thus it was not possible to analyze the absolute effect of MDFT. Two studies, Liddle 2001, and Dennis 2004, had two comparison groups with different individuals, and the Rigter 2011 study was carried out in five different countries with treatment as usual as the comparison condition, which varied across countries. The comparison treatments in the five studies were: Cognitive Behavioral Therapy (CBT), peer group, treatment as usual (TAU), adolescent group therapy (AGT)/multifamily educational therapy (MEI) and Motivational Enhancement Therapy/Cognitive Behavioral Therapy (MET/CBT5)/Adolescent Community reinforcement approach (ACRA).
The outcomes were reported at varying time points. We grouped the outcomes at 6 and 12 months post-intake. As duration of treatment in two studies was 3-4 months and in three studies was 4-6 months, these time points were approximately equivalent to termination and 6 month follow-up respectively.
In summarising these results, we have chosen to interpret a value of the standardised mean difference, SMD=0.20 as a small effect size, as is the general practice (Cohen, 1988).
Abstinence or reduction of drug abuse
Meta-analysis of the five included studies show a small but statistically significant effect of MDFT for youth drug abuse problem severity reduction at 6 months post-intake and 12 months post-intake compared to CBT, TAU, MET/CBT5 and ACRA. The pooled effect sizes are however small and confidence intervals are often close to zero. The statistically significance of the pooled results are sensitive to the removal of studies with methodological weaknesses at 6 months post-intake but not at 12 months post-intake. The available data thus supports the hypothesis that there is an effect on drug abuse problem severity reduction of giving MDFT to young drug abusers compared to other treatments.
Pooled results of the four studies providing data on drug abuse frequency reduction favours MDFT compared to CBT, TAU, MET/CBT5 and ACRA. The effect of MDFT for youth drug abuse frequency reduction is small and statistically significant at 6 months post-intake but there is no statistically significant effect at 12 months post-intake. The statistically significance of the pooled results are sensitive to removal of studies with methodological weaknesses at 6 months post-intake in one of two analyses (when the comparison used in Dennis 2004 is MET/CBT5).
The available data supports the hypothesis that there is a small drug abuse frequency reduction effect of giving MDFT to young drug abusers compared to other treatments at 6 months post-intake, but the effect appears to vanish 12 months after intake.
When interpreting these results, however, consideration should be given to the limited number of studies providing data that enables a calculation of an effect size regarding drug abuse reduction. The conclusions that can be drawn from giving MDFT to young drug abusers compared to other treatments 14 would be more convincing if more studies were available. The pooled effect sizes are small and confidence intervals are often close to zero.
Family functioning
It was not possible to perform a meta-analysis on family functioning as only three studies provided data and the measures used were not comparable.
School grades
Two studies reported school grades; however, only data at 6 months post-intake were provided. Meta-analysis favors MDFT compared to peer group and AGT/MEI; however confidence intervals are wide. The effect of MDFT for improving school grades is not statistically significant when using the AGT comparison in Liddle 2001 but is statistically significant when using the MEI comparison in Liddle 2001.
Retention
We extracted data on retention from all five included studies; meta-analysis favoured MDFT. Overall the results indicate that retention may be positively affected by structured MDFT treatment compared to the less structured control conditions of CBT, TAU, MET/CBT5 and ACRA.
However the pooled results must be interpreted with caution as two studies stand out from the others with large effect sizes and very wide confidence intervals (Liddle 2009 comparing MDFT to peer group, and Rigter 2011 comparing MDFT to TAU), and the estimated between study variation is quite large.
Risk behavior and other adverse effects
Opportunities for meta-analysis were limited for risk behavior as only one study (Rigter 2011) reported relevant data. No other adverse effects such as rates of hospitalization, suicide and over-doses were provided in any of the five studies.
5.2 OVERALL COMPLETENESS AND APPLICABILITY OF EVIDENCE
The number of included studies in this systematic review is small; only five trials met the inclusion criteria and examined whether MDFT reduced youth drug use. Three of these were conducted by MDFT program developers, one was conducted by an independent investigator with a program developer as a co-author and one study was conducted by independent investigators.
It was not possible to analyze the absolute effect of MDFT. All five studies compared MDFT to other interventions, mainly CBT or ‘CBT-informed’ treatments. Two studies had two comparison groups with different individuals and different treatments, while the study which was carried out in five different European countries had variations in comparison treatments across countries.
The five trials were reported in 16 papers, and we looked for and extracted relevant outcome data in all 16 papers. Studies of secondary analyses of the included trials (Hogue, Dauber, Samuolis, & Liddle, 2006; Hogue et al. 1998; Henderson, Dakof, Greenbaum, & Liddle, 2010; Henderson, Rowe, Dakof, Hawes, & Liddle, 2009; Shelef, Diamond, Diamond, & Liddle, 2005) did not provide any additional data for this review because they analysed subgroups of participants and/or explored for factors which moderate treatment effects.
It was possible to analyse outcomes at 6 and 12 month post-randomization (approximately equivalent to 6 and 12 months post-intake), although not all studies provided data at the longer follow up which would have allowed for documentation of accumulated or longer-term effects.
Whilst it was possible to include all studies in the analysis of the primary outcome reduction of substance abuse, reporting of secondary outcome data was very limited.
Four of the five studies originated from North America. This may limit the applicability of the evidence to a specific social and cultural setting, which in turn may be difficult to translate to other settings. This indicates a need for more well-conducted studies of CBT interventions in countries other than the USA.
5.3 QUALITY OF THE EVIDENCE
All five included studies were randomized controlled trials but none can be characterised as a robust RCT with low risk of bias on all assessed risk of bias items. One of the five included studies provided insufficient information on core issues to allow us to assess the risk of bias and had a significant level of missing data, making us question its validity.
Where effects were statistically significant, there was overall consistency in the direction of treatment effects regarding primary outcome (drug problem severity and drug abuse frequency) with all treatment effects favouring MDFT. Similarly, where effects on retention were statistically significant, MDFT was the favoured treatment. However the overall result must be interpreted with caution as two studies stand out from the others, with large effect sizes and very wide confidence intervals, and the estimated between study variation is quite large.
5.4 POTENTIAL BIASES IN THE REVIEW PROCESS
The narrow search strategy performed in this review may limit the likelihood of finding all relevant studies. However, we attempted to minimize the risk of missing relevant studies by conducting an extensive search for grey literature, an extensive hand searching and by contacting international experts within the field of MDFT; indeed, the large number of grey literature and hand searched literature that has been assessed for relevance attests to this effort.
5.5 AGREEMENTS AND DISAGREEMENTS WITH OTHER STUDIES OR REVIEWS
We identified five narrative reviews and three quantitative reviews on MDFT treatment for drug-using youth.
The identified narrative reviews (Thompson, Pomeroy, & Gober, 2005; Austin, Macgowan, & Wagner, 2005; Szapocznik, Lopez, Prado, Schwartz, & Pantin, 2006; Liddle, 2010; and Rowe, 2010) report a general pattern of a positive effect for MDFT treatment for drug-using youth. Thompson et al., 2005; Austin et al., 2005, and Szapocznik et al., 2006 review several interventions for drug-using youth, and with the exception of Thompson et al., 2005, their conclusions concerning MDFT are based on one study (Liddle 2001). In contrast, Liddle, 2010 and Rowe, 2010, focus on MDFT and base their conclusions on a greater number of studies.
We identified three quantitative reviews (Bender, Tripodi, Sarteschi, & Vaughn, 2011; Waldron & Turner, 2008; Vaughn et al., 2004). Vaughn et al., 2004, examined several interventions for drug-using youth and the conclusions concerning MDFT were based solely on Liddle 2001 with the authors reporting “evidence of clinically meaningful effect (Evidence Summary [ES] > .20) with at least 1 year follow-up or replication and using relatively strong designs”.
Waldron & Turner, 2008, used meta-analysis to evaluate family therapy, CBT (individual and group), and ‘minimal treatment control conditions' for drug-using youth. They concluded that “MDFT, FFT and group CBT emerged as well-established models for substance abuse treatment.” based on the studies by Liddle 2001, Liddle 2008, Liddle 2009 and Dennis 2004.
Bender et al., 2011 used meta-analysis to evaluate family therapy and individual therapy for drug-using youth. The authors reported that “Interventions with large effect sizes (>.80) included several family-based or multisystem approaches (Integrated Family, CBT, MDFT, Teaching family).” based on the studies by Liddle 2001, Liddle 2008 and Liddle 2009.
Consistent with our expectations, the apparent feedback from the three reviews is that more research is needed, not least with regard to moderators and identification of which particular subgroups of youth may be more likely to respond to specific interventions, as well as how treatments can be adapted or tailored to the individual needs of a young person to improve drug abuse outcomes. These are similar issues to those we planned to assess in our review. However, the lack of empirical evidence obscured the possibility of assessing moderators of effect and effects on subgroups.
6 Authors' Conclusion
6.1 IMPLICATIONS FOR PRACTICE
Although most of the few available studies on effectiveness are characterized by methodological problems, the results of this review suggest that MDFT seems to ‘work’ in the sense that the intervention results in a slightly higher reduction of drug abuse for the average individual compared to the average individual receiving other active treatments. Besides knowledge of whether a certain intervention ‘works’, in the sense that it is effective for the average individual, practitioners need knowledge about potential differential effects on treatment of highly relevant participant characteristics such as age, gender, minority background, family composition (e.g., single parents), and co-occurring conditions.
However, the participant characteristics listed above are potential predictors of treatment outcome, and practitioners need to be able to tailor the program to particular types of young drug abusers. It is not possible to identify which particular subgroups of youth may be more likely to respond to specific interventions, and subsequently how treatments could be adapted or tailored to the individual needs of a young person until results of additional MDFT outcome studies are available.
Programmes for drug using youth are costly, and it is also possible that such initiatives have potential cause damage to some individuals. The available evidence points to small effect sizes of MDFT in comparison to other treatments. Taking the individual variation in treatment effects into consideration, we cannot rule out the possibility that MDFT may be counterproductive for some individuals. It is therefore crucial to know more about its effectiveness in order to determine where money is best allocated as well as to understand which form of support would benefit young drug abusers most.
6.2 IMPLICATIONS FOR RESEARCH
It is important to address the need for more research in the field. A small body of evidence exists in relation to the treatment of young drug abusers, with only a very modest number of controlled evaluations of treatments for this group. Most of the few available studies of effectiveness have methodological problems, such as small sample size and varied methods of assessing drug abuse; such problems make definitive conclusions difficult, if not impossible. Well-designed, randomized controlled trials within this population are needed and should be reported clearly in accordance with the principles of the CONSORT 2010 statement. In addition, longer follow up data should be available in future studies.
It is also important to consider the possibility of any adverse effects these interventions might have. The popular belief is that MDFT, as well as other family therapy approaches, is harmless, but very little research has been conducted that focuses on the potential harm of such family therapy approaches.
7 Acknowledgements
The review authors would like to thank Professor Barnaby Reeves from the Cochrane Non-randomised Studies Methods Group for materials and training regarding the assessment of the risk of bias in NRCTs, the Campbell methods peer-referees; Dr. William Turner and Dr. Terry Pigott, Karianne Thune Hammerstrøm, and external content and methods peer-referees for valuable and insightful comments on methods and content, during the stage of writing the protocol and the final review report. We are grateful to external experts; Lori Whitten, RTI International and Prof. Gayle Dakof, University of Miami Miller School of Medicine, for their kind response and help in order to capture potential studies that were not part of our own literature search.
Thanks to Head of SFI Campbell, Ph.D. Mette Deding, for continued support and efforts to realize this review. Last but not least, thanks to the review team for their huge work morale, excellent collaboration and perseverance throughout the entire review process.
The review authors take full responsibility for the content in this publication.
Footnotes
9 Characteristics of studies
10 Additional tables
11 Figures
12 Differences between review and protocol
In the protocol it was stated in section 3.4.7 that statistically significant heterogeneity among primary outcome studies will be been assessed with Chi-squared (Q) test and I-squared (Higgins, Thompson, Deeks, & Altman, 2003). A significant Q (P<.05) and I-squared of at least 50 per cent will be considered as statistical heterogeneity. The assessment of heterogeneity has been changed to: Heterogeneity among primary outcome studies was assessed with Chi-squared (Q) test, and the I-squared, and τ-squared statistics (Higgins, Thompson, Deeks, & Altman, 2003). Any interpretation of the Chi-squared test was made cautiously on account of its low statistical power.
Appendix
12.2 CODE BOOK FOR DATA EXTRACTION
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Name the intervention | |
| How is the intervention delivered? | |
| If Family, Other or Combination, describe the way it is delivered | |
| Describe any practical circumstances relevant to the intervention | |
| If deviation from manual, describe/list the components given in the intervention | |
| Describe any co-interventions given with the intervention | |
| Frequency of the intervention | |
| Intensity | |
| Duration of the intervention | |
| Who delivered the intervention? | |
| List program delivers qualifications. | |
| List program delivers characteristics. | |
| Describe methods used to ensure adherence to the intervention (specific to the intervention) | |
|
What did the investigators do to check/measure treatment fidelity? Other important information |
|
|
|
| Name the control/comparison condition intervention | |
| How is the control intervention delivered? | |
| If Family, Other or Combination, describe the way it is delivered | |
| Describe any practical circumstances relevant to the intervention | |
| If deviation from manual, describe/list the components given in the intervention | |
| Describe any co-interventions given with the comparison intervention | |
| Frequency of the intervention | |
| Intensity | |
| Duration of the intervention | |
| Who delivered the intervention? | |
| List program delivers qualifications | |
| List program delivers characteristics | |
| Describe methods used to ensure adherence to the intervention | |
| What did the investigators do to check/measure treatment fidelity? | |
| Did they measure session attendance? | |
| Other important information |
| Baseline time - describe how baseline is defined | |
| End of treatment (from baseline time) to… | |
| …1st follow-up | |
| …2nd follow-up | |
| …3rd follow-up | |
| …Other | |
| Author's main conclusion | |
| Limitations of the study, as reported by the study authors | |
| Researcher's affiliation with program (if any) | |
| Your own concerns and notes | |
| Question(s) for review authors |
| OUTCOMES | |
| Outcome measurement | |
| What does it measure? | |
| Reliability & Validity | |
| Outcome measurement format (continous or binary) | |
| Direction | |
| Mode | |
| If other, describe | |
| Source | |
| If other, describe | |
| NOTES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12.3 ASSESSMENT OF RISK OF BIAS IN INCLUDED STUDIES: GUIDELINES
1
In this review, we use the term abuse to refer to the consumption of drugs beyond experimentation and into addiction.
2
A Cochrane review has evaluated psychosocial interventions for substance abuse and misuse in young offenders in locked facilities (Townsend et al., 2009).
3
A Cochrane review has evaluated psychosocial treatments for treatment of opioid dependence (Amato et al., 2009).
4
Please see the following Title Registrations in the Campbell Library for further information: Lindstrøm et al (2011). Family Behavior Therapy (FBT) for young people in treatment for illicit non-opioid drug use; Kowalski et al (2011). Functional Family Therapy (FFT) for young people in treatment for illicit non-opioid drug use; Lindstrøm et al (2011). Brief Strategic Family Therapy (BSFT) for young people in treatment for illicit non-opioid drug use
5
Sometimes the assessment of component three is split into two: a) a component concerning other family members and b) a component concerning systems external to the family, and thereby five components are presented in some MDFT studies (Liddle, 2002).
6
This risk of bias model was introduced by Prof. Reeves at a workshop on risk of bias in non-randomized studies at SFI Campbell, February 2011. The model is developed by the Cochrane Non-Randomized Studies Method Group (NRSMG).
7
The extended model was developed to ensure standardization of guidelines and procedures in the Risk of Bias assessment of NRS.
8
Although one study scored 5 on the item selective outcome reporting for three out of nine outcomes (drug use problem severity, drug use frequency and delinquency as only log transformed means and standard deviations were reported for these outcomes). These three outcomes are not included in the meta analyses.
9
The study refers to four different sites, due to there being two trials in the study, but only one of the trials concerns MDFT; it is this that is reported here and concerns two different sites in Philadelphia.
10
There is a risk of first-order selection bias when participants or others select the treatment assignment which is eliminated with randomization. There is a risk of second-order selection bias when upcoming assignments can be observed which is eliminated/minimized by allocation concealment. There is risk of third-order selection bias if upcoming assignments can be predicted or even determined, if some of the previous allocations are known, and if restrictions are placed on the randomization. The third-order selection bias can be controlled by perfect masking.
11
Reported in Schaub et al., 2014.
12
Analysis 1A when removing studies scoring 4 on the other bias item.
13
Analysis 1B and 2B when removing studies scoring 4 on the other bias item.
14
The comparison treatments were: Cognitive Behavioral Therapy (CBT), peer group, treatment as usual (TAU), adolescent group therapy (AGT)/multifamily educational therapy (MEI) and Motivational Enhancement Therapy/Cognitive Behavioral Therapy (MET/CBT5)/Adolescent Community reinforcement approach (ACRA).
15
This risk of bias model was introduced by Prof. Reeves at a workshop on risk of bias in non-randomized studies at SFI Campbell, February 2011. The model is a further development of work carried out in the Cochrane Non-Randomized Studies Method Group (NRSMG).