
Abstract
This Campbell systematic review examines the effectiveness of vocational rehabilitation interventions to help adults with traumatic brain injury (TBI) get competitive employment. Three randomized controlled trials are included: two of military populations in the United States and two of the civilian population in China (Hong Kong).
Studies are included which assess interventions focused on assisting helping workingaged adults with TBI return to competitive employment, including self-employment. Participants must have been between 18 and 65 years of age, experienced a nonpenetrating TBI, been engaged in either full-time or part-time employment at time of injury, and been unemployed or on medical leave at time of receipt of the intervention. The studies must have competitive employment as an outcome.
Three randomized controlled trials (RCT) are included in the analysis, two studying US military personnel and one of civilians in China (Hong Kong). All three studies compared alternative programmes. One compared an intensive in-hospital program versus an at-home program. The second study compared the CogSMART program plus supported employment with supported employment alone. And in the third study the control group received psycho-educational training with the treatment group receiving the same content via a virtual reality-based training platform.
Synopsis/Plain Language Summary
Programs for adults who have suffered traumatic brain injury may improve employment status. However, no programme was found to be more effective than its comparator programme.
The unemployment rate in the United States for people who have suffered traumatic brain injury (TBI) was around 60 percent for 2001-10, compared to a national average of around 7 percent. Post-acute rehabilitation services - such as residential community reintegration programs, comprehensive day treatment programs, and community re-entry programs - focus on helping individuals adjust to ongoing impairments and to re-enter their communities, workplaces, and education. This review assesses the most effective type of intervention for returning individuals with TBI to work.
This Campbell systematic review examines the effectiveness of vocational rehabilitation interventions to help adults with traumatic brain injury get competitive employment. Three randomized controlled trials are included: two of military populations in the United States and two of the civilian population in China (Hong Kong).
Studies are included which assess interventions focused on assisting helping working-aged adults with TBI return to competitive employment, including self-employment. Participants must have been between 18 and 65 years of age, experienced a nonpenetrating TBI, been engaged in either full-time or part-time employment at time of injury, and been unemployed or on medical leave at time of receipt of the intervention. The studies must have competitive employment as an outcome.
Three randomized controlled trials (RCT) are included in the analysis, two studying US military personnel and one of civilians in China (Hong Kong). All three studies compared alternative programmes. One compared an intensive in-hospital program versus an at-home program. The second study compared the CogSMART program plus supported employment with supported employment alone. And in the third study the control group received psycho-educational training with the treatment group receiving the same content via a virtual reality-based training platform.
None of the programs were better at improving employment outcomes than the comparator program to which it was compared. That is the intensive in-hospital program was no better than the at-home alternative, CogSMART added to no value to supported employment alone, and virtual reality-based training was no better than psycho-educational training. Comparison of employment before and after the interventions suggests that the interventions in the United States improved employment status, but not that in China
None of the studies reported secondary employment outcomes: hours worked and wages earned.
It was not possible to conduct analysis of the relative effectiveness of different types of programme because of the small number of included studies.
These three studies have limited implications for practice and policy. No intervention was found to be more effective than any other. In two of the studies the populations were limited to military subjects, who present with significantly different challenges such as posttraumatic stress disorder.
The comparator interventions of at-home training and supported employment appear promising.
There is a need for more RCTs on RTW interventions with adults with TBI, preferably separating competitive employment from school attendance. Military interventions should be conducted with civilian samples in order to determine their effectiveness in the civilian population, including on populations outside the United States. A broader range of employment outcomes should be studied, with regular follow up at standard intervals (e.g., six months, 12 months, 18 months, etc.).
The search was completed in 2015. This Campbell Systematic Review was published in July 2016.
The Campbell Collaboration is an international, voluntary, non-profit research network that publishes systematic reviews. We summarise and evaluate the quality of evidence about programmes in the social and behavioural sciences. Our aim is to help people make better choices and better policy decisions.
This summary was written by Howard White (Campbell Collaboration). This PLS is based on Campbell Systematic Review 2016:6 ‘Employment Interventions for Return to Work in Working Aged Adults Following Traumatic Brain Injury (TBI): A Systematic Review’ by Carolyn W. Graham, Michael D. West, Jessica L. Bourdon, Katherine J. Inge and Hannah E. Seward (DOI:10.4073/csr.2016.6). Anne Mellbye (RBUP, Norway) designed the summary, which was edited and produced by Tanya Kristiansen (Campbell Collaboration).
Executive Summary/Abstract
BACKGROUND
Individuals with traumatic brain injury (TBI) often struggle to obtain competitive employment after sustaining a TBI, commonly as a result of the post-injury difficulties they exhibit (Andelic, Stevens, Sigurdardottir, Arango-Lasprilla, & Roe, 2009; Mansfield et al., 2015). The currently reported unemployment rate for people with TBI is approximately 60% (Cuthbert et al., 2015). Hence, the unemployment for individuals with TBI is considerably higher than for individuals without disabilities.
Many adults with TBI seek assistance in gaining employment through post-acute rehabilitation. Post-acute rehabilitation services focus on helping individuals adjust to ongoing impairments and to re-enter their communities, workplaces, and education. Post-acute interventions are broadly classified into the following groups (Shames, Treger, Ring, & Giaquinto, 2007): residential community reintegration programs, comprehensive day treatment programs, and community re-entry programs that focus on vocational and social reintegration. This review focused on identifying the most effective type of intervention for returning individuals with TBI to work. The authors of this review drew on a wide range of databases, searched grey literature, included studies with a range of follow-up times, and focused on competitive employment outcomes among individuals with TBI regardless of the injury severity of the individuals.
OBJECTIVES
This review examined the effectiveness of vocational rehabilitation (VR) interventions to help adults with TBI attain competitive employment.
SEARCH METHODS
Studies for this review were identified by searching 16 databases, including the Australian Education Index, CIRRIE – the Center for International Rehabilitation Research Information and Exchange Databases, the Academic Complete collection, EBSCOhost Research Databases, MEDLINE/PubMed, ProQuest, and 11 other databases. Unpublished papers and grey literature were also searched. Reference lists of papers included in the analysis and previous systematic reviews were searched.
SELECTION CRITERIA
The following inclusion criteria were used for each potential study: (1) Studies are of interventions focused on assisting helping working-aged adults with TBI return to competitive employment, including self-employment. (2) Competitive employment had to be measured as an outcome. (3) Participants must have been between 18 and 65 years of age, experienced a non-penetrating TBI, been engaged in either full-time or part-time employment at time of injury, and been unemployed or on medical leave at time of receipt of the intervention. Studies that included individuals with other disabilities were included only if the results were provided for TBI participants separately from those with other disabilities. (4) Data had to be presented separately for competitively employed participants. (5) The design must be a randomized controlled trial (RCTs) or quasi-experimental design, with a treatment and a control/comparison group.
DATA COLLECTION AND ANALYSIS
Odds ratios and log odds ratios were computed and 95% confidence intervals were computed for each included study. Only datab for the primary outcome, competitive employment status, were used due to insufficient secondary outcome data.
RESULTS
The literature search resulted in 6,941 unduplicated documents. From these 6,941 documents, 414 documents were selected for full-text review. From these 414 documents, 67 intervention reports were found, with only three return-to-work RCTs meeting inclusion criteria for this systematic review. The last search was conducted November 7, 2015.
The three studies included in this review were RCTs with parallel interventions (Man et al., 2013; Salazar et al., 2000; Twamley et al., 2014, 2015). Man et al. (2013) compared two interventions, an artificial intelligent virtual reality-based training program (n = 17) and a psycho-educational vocational training system (n = 20) using a civilian population from China. Salazar et al. (2000) compared an in-hospital cognitive treatment (n = 67) to an in-home treatment (n = 53) for active U.S. military personnel. Twamley et al. (2014, 2015) compared a CogSMART Plus supported employment program (n = 21) to an enhanced supported employment program (n = 21) for U.S military veterans.
Salazar and colleagues (2000) used active military samples and Twamley et al. (2014, 2015) used U.S. military veterans. Man and colleagues (2013) used civilians in China. The sample in Salazar et al. (2000) was predominantly African American and White. There were more Hispanic/Latino and White participants in the Twamley et al. (2014, 2015) study. Man and colleagues (2013) RCT did not report the ethnicity or race of its sample from China. The Twamley et al. (2014, 2015) and Man et al. (2013) studies reported severity of injury as mild to moderate.
All studies were RCTs; however, blinding, incomplete data, and selective outcome reporting were of concern for all studies. Design, review status, publication type, and presence of control group were sufficient. Findings from this systematic review were inconclusive in that all odds ratios were not significant. Man et al. (2013) had the largest odds ratio (OR = 2.204, P = 0.264) but had the lowest employment rates (30%). Salazar et al. (2000) and Twamley et al. (2014, 2015) had odds ratios less than one. This indicated that the alternate interventions for Salazar et al. (OR = 0.514, p = 0.353) and Twamley et al. (OR = 0.817, p = 0.749) were more effective than the primary intervention. The employment rates for Salazar et al. and Twamley et al. ranged from 55% to 94%, which were rates higher than observed in Man et al. In sum, there were no significant odds ratios. Although all interventions evidenced positive average gains, no intervention was identified as more effective than another.
AUTHORS' CONCLUSIONS
All interventions showed positive average gains. However, we were unable to determine which intervention was most effective due to the small number of studies (n = 3). More experimental RCTs need to be conducted with interventions not included in this study. There are several recommendations for the direction of research concerning return-to-work for adults with TBI. First, studies of return-to-work VR interventions for adults with TBI must improve their quality of research by conducting RCTs. Second, separating competitive employment from education would provide a more accurate estimate of impact on return to work. Third, research is needed with other populations outside the United States and civilian samples. Last, future return-to-work VR studies should report time to employment, hours worked, separate rates of competitive employment, sheltered employment, educational training, and continued follow-ups at 12 months or more.
Linked article:
1 Background
1.1 THE PROBLEM, CONDITION, OR ISSUE
1.1.1 Incidence and Causes of Traumatic Brain Injury
Traumatic brain injury (TBI) occurs when an external force causes an alteration to brain function (e.g., loss of consciousness, memory loss, and neurologic defects). A TBI can occur from a blow to the head, blast waves from an explosion, swift acceleration or deceleration, or the penetration of a foreign object into the brain (Maas, Stocchetti, & Bullock, 2008; Menon, Schwab, Wright, & Maas, 2010). TBI is a major concern worldwide and affects 10 million people annually (Hyder, Wunderlich, Puvanachandra, Gururaj, & Kobsingye, 2007). The two most common worldwide causes of TBI are traffic accidents and falls, with traffic accidents declining in predominance and falls rising due to aging populations (Bražinova et al., 2015; Li et al., 2015; Majdan, Rusnák, Bražinová, & Mauritz, 2015; Peeters et al., 2015; Popescu, Anghelescu, Daia, & Onose, 2015; Scholten, Haagsma, Panneman, Beeck, & Polinder, 2014; Shekhar, Gupta, Premsagar, Sinha, & Kishore, 2015; Shivaji, Lee, Dougall, McMillan, & Stark, 2014).
1.1.2 Severity and Sequelae
Levels of TBI range from mild to severe and are determined by measures such as duration of coma or post-traumatic amnesia (PTA), Glasgow Coma Scale (GCS) scores, and the nature and extent of functional impairments following the injury. Individuals with TBI experience various combinations of physical, cognitive, sensory, and emotional symptoms, which are largely determined by the severity of the impact, the location of the impact, and whether the TBI is a penetrating (open) or non-penetrating (closed) injury (BrainandSpinalCord.org, 2013).
Brain injury severity is typically related to the degree and extent of impairment post-injury. Even individuals experiencing mild brain injuries can experience problems in one or more areas of functioning, though most individuals with a mild TBI will recover lost functioning. In most cases of moderate and severe TBI, individuals' recovery will plateau below pre-injury functioning levels.
1.1.3 Return to Work Following TBI
Individuals with TBI often struggle to either obtain or maintain competitive employment after sustaining a TBI, commonly as a result of the post-injury difficulties they exhibit (Andelic, Stevens, Sigurdardottir, Arango-Lasprilla, & Roe, 2009; Dikmen et al., 1994; Ezrachi, Ben-Yishay, Diller, & Rattock, 1991; Mansfield et al., 2015; Ruttan, Martin, Liu, Colella, & Green, 2008). Reported unemployment rates of people with TBI have ranged from 45% to 78% (Cuthbert et al., 2015; Doctor et al., 2005; Kendall, Muenchberger, & Gee, 2006; Yasuda, Wehman, Targett, Cifu, & West, 2001). This variation in return-to-work (RTW) rates is related to differences in sample characteristics, methodologies, and measures of employment. Nevertheless, unemployment for individuals with TBI is considerably higher than for individuals without disabilities.
TBI and its effects can be overwhelming, not only for individuals with this injury and their families (Cifu, Craig, & Rowland, 1996; Liu, Zhu, Liu, & Guo, 2015; Moriarty et al., 2015; Tarn, McKay, Sloan, & Ponsford, 2015), but also for other sectors of society. While individuals and families experience financial burdens due to the loss of jobs and wages, as well as medical and rehabilitation expenses (Costa, Dagher, Lamoureux, Guise, & Feyz, 2015; Fadyl & McPherson, 2009; Joseph et al., 2015; Ma, Chan, & Carruthers, 2014; Samuelsson, Tropp, & Lundqvist, 2014; Te Ao et al., 2014), communities and employers experience lost workdays and productivity (Te Ao et al., 2014; Andlin-Sobocki, Jonsson, Wittchen, & Olesen, 2005; Samuelsson et al., 2014). TBI can also impose substantial burdens on governments through publicly funded healthcare, rehabilitation service costs, and financial support for injured persons (Te Ao et al., 2014; Hyder et al., 2007; Samuelsson et al., 2014). The Centers for Disease Control and Prevention (CDC) in the United States, estimated that the medical and indirect costs of TBI (e.g., lost productivity) in 2010 were $76.5 billion in the United States (Coronado, McGuire, Faul, Sugerman, & Pearson, 2012; Finkelstein, Corso, & Miller, 2006), while the total annual cost in Europe was approximately ***386 billion (Andlin-Sobocki, Jonsson, Wittchen, & Olesenet al., 2005). Thus, the cost of TBI to both the individual and society is staggering. These costs can be ameliorated through rehabilitation and by returning individuals with TBI to work (Doctor et al., 2005; Kendall et al., 2006; Samuelsson et al., 2014; Yasuda et al., 2001).
Shames, Treger, Ring, and Giaquinto (2007) conducted a comprehensive review of the literature regarding factors associated with successful RTW following TBI and current rehabilitation strategies. They note that predicting a successful RTW involves a complex interaction of variables, including pre-morbid factors (e.g., age, education, and prior employment history), injury-related factors (type, severity, and location), post-injury impairments, and personal and environment factors (e.g., marital status, alternative income sources, and social support). Because of this complexity and the unique characteristics of each individual with a TBI, prediction of RTW is not feasible. They note, however, that the literature includes numerous examples of high-risk individuals who have been successful when given sufficient rehabilitation and support. In addition, the TBI employment research literature is international (e.g., Cancelliere et al., 2014; Fear et al., 2008; Li et al., 2015; Shekhar et al., 2015; Te Ao et al., 2014), which brings into consideration differences across economies, cultures, health care and rehabilitation systems, and national landscapes of public and social disability policies.
Despite the variety of factors related to poor employment outcomes for individuals with TBI, some factors are more frequently reported to contribute to poor employment outcomes (Shames et al., 2007): More severe injury (Cuthbert et al., 2015; Kreutzer et al., 2003; Trexler, Trexler, Malec, Klyce, & Parrott, 2010; Wagner, Hammond, Sasser, & Wiercisiewski, 2002), as measured by the GCS, PTA, duration of rehabilitation, or other means Higher age at injury (Cuthbert et al., 2015; Keyser-Marcus et al., 2002; Kreutzer et al., 2003) Gender (Female) (Cuthbert et al., 2015) Lower levels of pre-injury educational and/or occupational status (Cuthbert et al., 2015; Hart, Whyte, Polansky, Kersey-Matusiak, & Fidler-Sheppard, 2005; Keyser-Marcus et al., 2002; Walker, Marwitz, Kreutzer, Hart, & Novack, 2006) Limited social support from friends, family, neighbors, church, etc. (Yasuda et al., 2001) Significant physical, psychosocial, or cognitive impairments (Cuthbert et al., 2015; Keyser-Marcus et al., 2002; McCrimmon & Oddy, 2006; Wagner et al., 2002; Walker et al., 2006) Member of a minority group (Arango-Lasprilla et al., 2008; Cuthbert et al., 2015; Hart et al., 2005; Kreutzer et al., 2003) History of substance abuse (Bogner, Corrigan, Mysiw, Clinchot, & Fugate, 2001; Corrigan, 1995; Hollar, McAweeney, & Moore, 2008; McAweeney, Jones, & Moore, 2008; Wagner et al., 2002) Financial status and receipt of a settlement or public benefits following the injury (Cuthbert et al., 2015)
1.2 THE INTERVENTION
1.2.1 Post-Acute Return-to-Work Interventions
Following acute care, post-acute rehabilitation services focus on helping individuals adjust to ongoing impairments and re-enter their communities, workplaces, schools, etc. Post-acute interventions are broadly classified into the following groups (Shames et al., 2007): (1) Residential community reintegration programs that provide intensive behavioral interventions; (2) Comprehensive day treatment programs that emphasize training in self-awareness, social skills, daily living skills, and coping mechanisms; and (3) Community re-entry programs that focus on vocational and social reintegration.
Within these, RTW interventions are funded and delivered through multiple avenues. In the United States, the primary sources of RTW interventions are employee disability management programs and state vocational rehabilitation (VR) agencies. Many other countries have equivalent organizations (United Nations World Health Organization & The World Bank, 2011).
Brief descriptions of employee disability management and VR programs are presented in this section.
Employee Disability Management Programs, typically provided directly by employers or through their insurance programs, are a combination of many services (e.g., work injury prevention programs, early intervention, transitional work programs, and case management) to better address the physical and psychological needs of the worker (Ongori, 2012; Shrey, 1996). Job accommodations, support services, and determining the use of adaptive devices are all potential components of disability management (Ongori, 2012; Shrey, 1996). For example, gradual RTW would fall into this category. Additionally, some companies may offer on-site training as a disability management component. This may be similar to transitional programs, where the client receives physical, cognitive, and behavioral training while developing job skills in a practice work environment. This allows employers to see how and if they need to make accommodations, and helps the employee develop the skills they need to perform on the job (Ben-Yishay et al., 1985; Jacobs, 1997; Klonoff et al., 2007; Prigatano et al., 1994).
State VR Services are provided to individuals with various types of disabilities with the goal of increasing their independence and employment. Services include physical restoration (prosthetic devices), vocational training, counseling, and job development assistance. Supported employment is an increasingly utilized VR service option for clients with TBI, where a client obtains paid work that is integrated with people without disabilities while receiving ongoing support from an employment specialist or job coach (Wehman et al., 2003). An unique feature of the supported employment model is that individuals with TBI receive training on the job as opposed to pre-training.
An individual placement model of supported employment consists of an employment specialist or job coach who assists the individual with TBI in finding a job. This specialist then helps coordinate pre-employment supports (e.g., benefits counseling or transportation) and may provide on-the-job support and training (Wehman et al., 2003), in addition to other counseling or advocacy services that are needed (Wehman et al., 1993). These supports provided by the employment specialist vary from person to person and change over time. Eventually, the specialist's involvement reduces to periodic checks, as mandated by the Rehabilitation Act (U.S. Department of Education, 2004). These checks are critical to long-term support and the ongoing employment of individuals with TBI. Such long-term support is unique to the supported employment model (Wehman et al., 2003).
Job accommodations are common to the generally differing systems of Employee Disability management programs and state VR services. Title I of the Americans with Disabilities Act (ADA; Americans with Disabilities, 2008) requires employers with 15 or more employees to consider providing reasonable accommodation for employees who meet the ADA's definition of disability. Accommodations are negotiated between the employee and the employer and are determined on a case-by-case basis. Before becoming eligible for a reasonable accommodation, the applicant or employee with TBI must disclose his or her disability status to the employer and make a request for the accommodation.
Accommodations are alterations made for the employee that do not conflict with the responsibilities of the job, such as flexible scheduling to accommodate the person“s disabilities (e.g., epilepsy, chronic fatigue, or psychosocial disabilities). Environmental modifications are a type of job accommodation and include building ramps for wheelchair access, adding elevators, relocating an employee's office, and widening aisles. With the increasing use and availability of technology such as high-speed Internet, some businesses permit telework from home, allowing an employee to accomplish their daily tasks without having to leave their residence (West & Anderson, 2005). In addition, employers may also reassign non-essential job functions that the employee cannot perform due to his or her disability. Employers are not required to make accommodations for essential job functions by eliminating them from the job description. Essential functions are the fundamental, crucial job duties performed in a position.
Another accommodation strategy common to both systems is to provide assistive technology services and devices. These can include memory aids, touch-screen computers, adjustable mounts at desks, specialized computer software, or alternative input devices to allow a person with limited manual dexterity or fine motor skills to use a computer (Inge & Targett, 2007). With the advent of handheld devices such as Smartphones and tablet computers, individuals can use pre-installed programs to create schedules and set alarms (Gentry, Lau, Molinelli, Fallen, & Kriner, 2012). There are Applications (apps) for these devices that may be used to train employees with disabilities such as TBI by providing visual cues for how to complete tasks, ways to deal with interpersonal situations, and individualized task lists (Burke, Andersen, Bowen, Howard, & Allen, 2010; Chang, Chen, Chuang, 2011; Gentry et al., 2012; Tsai, 2012). Since Individuals with TBI often have memory deficits, the use of handheld devices with apps is an example of an accommodation that can facilitate skill acquisition and job retention.
Finally, both service systems can offer ancillary therapeutic services which, though not directly employment-focused, support the RTW process. These include physical therapy, occupational therapy, speech-language therapy, neuro-cognitive therapy, and peer or professional counseling. Utilizing these programs as part of a cohesive rehabilitation strategy emphasizes a holistic approach (Ben-Yishay et al., 1985; Prigatano et al., 1984, 1994).
1.3 HOW THE INTERVENTION MIGHT WORK
1.3.1 Supply-Side and Demand-Side Interventions
Employment barriers and interventions may be broadly grouped into either supply-side or demand-side sources (Chan et al., 2010). Supply-side barriers are those related to individuals with disabilities, such as skill deficits, interfering behaviors, functional limitations related to the disability, and accommodation needs. Vocational rehabilitation provides support to individuals with disabilities on the supply-side of the labor market by providing training and placement services to job seekers (Luecking, 2008). The intent of these services is to prepare individuals with disabilities for employment and then supply these trained workers to employers. Supply-side interventions typically include the assessment of skill deficits followed by skill training and the provision of accommodations (including assistive technology) to prepare the job seeker for employment. Supported employment is a supply-side intervention. However, this is a “place and then train” approach to provide a labor supply to employers (Wehman, Inge, Revell, & Brooke et al., 2007). Individuals with TBI are supported in identifying their preferences for employment, and then are presented to potential employers for meeting labor market needs (Wehman & Targett, 2006). An employment specialist or job coach provides training and support on the job until the worker with disabilities performs to the satisfaction of the workplace. VR counselors, employment specialists, therapists, and educators typically deliver supply-side interventions. The duration of these interventions can range from days to years depending on the nature of the services. For example, an individual receiving supported employment services should receive ongoing support throughout his or her work history.
Conversely, demand-side interventions are increasingly seen as important for assisting individuals with disabilities in becoming employed (Chan et al., 2010; Gilbride & Stensrud, 1999; Luecking, 2008; Wehman, Kregel, & Brooke, 2008). Examples of demand-side barriers include employers' limited experience with employees with disabilities, employer attitudes toward hiring individuals with disabilities, high turnover or absentee rates, high production demands, and high costs related to injured workers.
Demand-side interventions may include disability management practices such as gradual return to full duty following injury, employer training and technical assistance related to disability and accommodation, co-worker and supervisor support and assistance, and employer-provided internships, skills training, or support programs.
The Logic Model (see Figure 1) presents the supply-side and demand-side intervention activities, recipients of intervention activities, and short- and long-term outcomes. Both types of interventions for individuals with TBI are included.
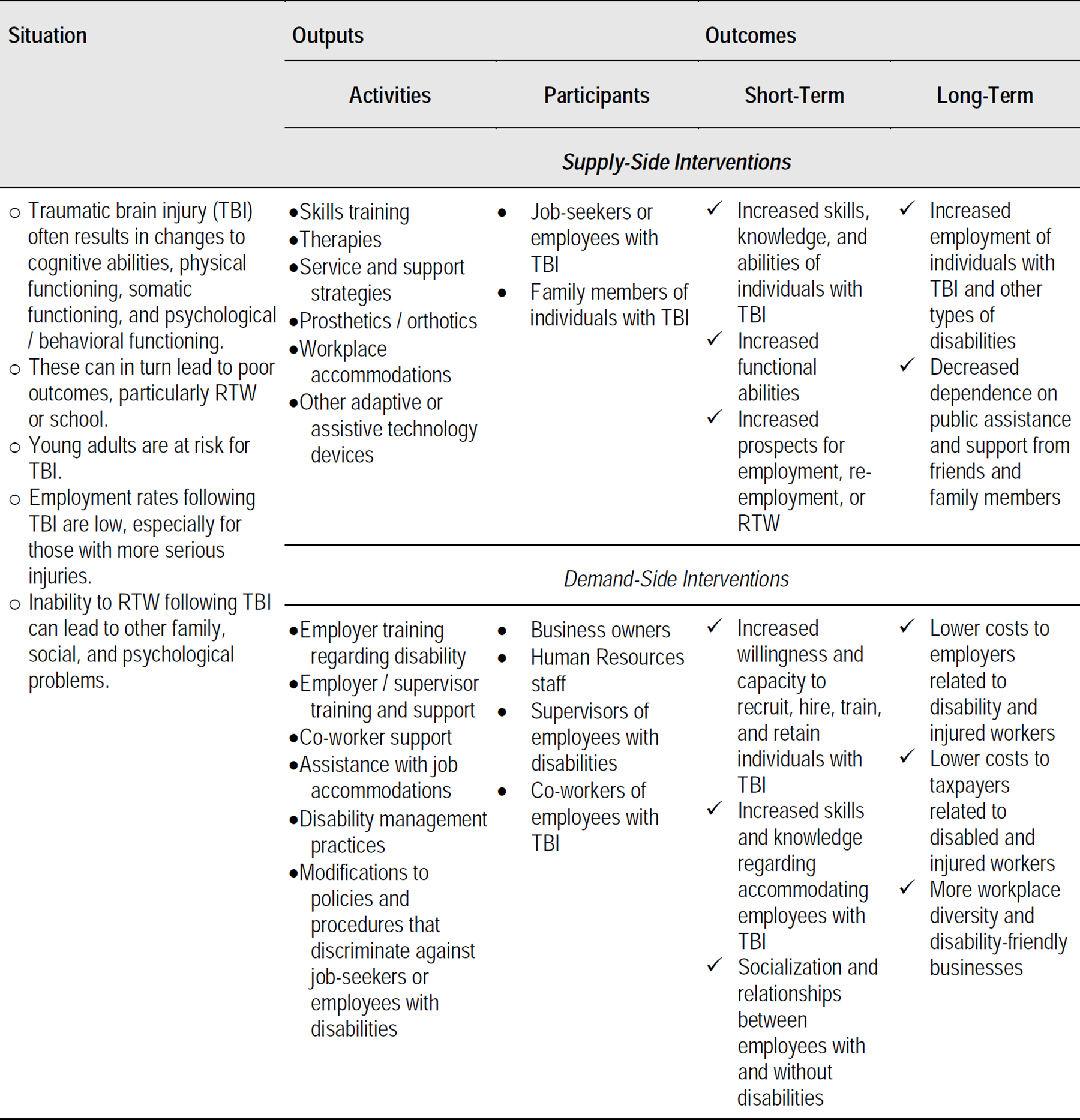
Logic Model, Employment Interventions for RTW in Working Aged Adults After TBI
1.4 WHY IT IS IMPORTANT TO DO THE REVIEW
Previous TBI systematic reviews have not compared the efficacy of different types of VR interventions on competitive employment. Instead, they have examined the effectiveness of specific interventions for individuals with TBI regarding their community integration (Kim & Colantonio, 2010); cognitive rehabilitation (Cicerone et al., 2011; Rohling, Faust, Beverly, & Demakis, 2009); quality of life (Berger, Leven, Pirente, Bouillon, & Neugebauer, 1999); functional independence (Willemse-van Son, Ribbers, Verhagen, & Stam, 2007); community participation (Cattelani, Zettin, & Zoccolotti, 2010; Evans & Brewis, 2008); and physical, psychological, and social functioning (Carney et al., 1999; Cattelani et al., 2010; Hellweg & Johannes, 2008; Kennedy et al., 2008).
There also have been systematic reviews that have examined the effectiveness of interventions at improving vocational outcomes for those with acquired brain injury (ABI) (Turner-Stokes, Nair, Sedki, Disler, & Wade, 2005). Specifically, Van Velzen, Van Bennekom, Edelarr, Sluiter, and Frings-Dresen (2009) examined the number of people with ABI—a diagnosis that includes brain injury from non-traumatic causes such as stroke, disease, and substance abuse—who returned to work over a 16-year period, but did not look at VR interventions. Similarly, Nightingale, Soo, and Tate (2007) conducted a systematic review that examined the prognostic factors related to people with TBI and RTW. Two of the outcome variables were productivity and competitive employment, but Nightingale et al. (2007) did not examine interventions. Additionally, a recent Campbell Collaboration title registration by Braathen and colleagues (2011) proposed to examine the effectiveness of comprehensive occupational rehabilitation programs for RTW among people on long-term sickness absence. Their review will include people with mental disorders and/or musculoskeletal disorders, but not those with TBI. While necessary, This further illustrates the need for the current systematic review. Saltychev, Eskola, Tenovuo, & Laimi (2013) conducted a review on predictive factors for employment after TBI, which included interventions. This review included studies that examined individuals that had worked or studied before injury.
Further, Fadyl and McPherson (2009) reviewed and evaluated the evidence for the effectiveness, strengths, and weaknesses of vocational interventions for individuals with TBI. Unlike the longer time period (1973 to 2015) and broad information retrieval (more databases and grey papers) of this proposed review, Fadyl and McPherson limited their search to articles available in English from January 1990 to July 2007. Further, their search was restricted to the Ovid Journals database, which includes MEDLINE, PsycInfo, CINAHL, AMED, health and psychosocial instruments, evidence-based medicine databases, and Web of Science. Geurtsen, Van Heugten, Martina, and Geurts (2010) conducted a systematic review of the effectiveness of comprehensive rehabilitation program interventions for a number of outcome variables, including employment. only PubMed, PsycINFO, and PsychLit databases and articles published from 1990 to 2008 were searched. Similarly, a recent systematic review protocol that addresses the effectiveness of multidisciplinary post-acute rehabilitation for adults with moderate to severe TBI (Agency for Healthcare Research Quality, 2011) limited its electronic database search to MEDLINE, the Cochrane Central Register of Controlled Trials, PEDro, and PsycINFO.
Unlike previous systematic reviews, this review focused on identifying the type of intervention that was most effective in returning individuals with TBI to work. This review searched a wider range of databases, searched and included grey literature, searched a broader length of time (1973 to 2011), and focused on competitive employment outcomes among persons with TBI regardless of injury severity. By including all competitive employment, supply- and demand-side interventions, and evidence-based research interventions for persons with TBI, this systematic review may provide some information concerning the effectiveness of these employment intervention programs that will guide practitioners and VR policymakers. Further, this review provides information concerning the direction for future research.
2 Objectives
This review examined the effectiveness of interventions on competitive employment outcomes for adults with TBI.
3 Methods
The methods for this systematic review are based on the protocol published by the Campbell Collaboration Library of Systematic Reviews (Graham & West, 2014). The protocol can be accessed at http://www.campbellcollaboration.org/lib/project/241/
3.1 CRITERIA FOR CONSIDERING STUDIES FOR THIS REVIEW
3.1.1 Types of Studies
A priori criteria were developed for the selection of studies to be included in this review. The following criteria were used. Each study must have: (1) explored interventions that assist working-aged adults with TBI to return to competitive employment (with competitive employment as the outcome), including self-employment; (2) at least included the primary outcome and employment status, and may also have included secondary outcomes, length of time employed, and mean hours worked; (3) participants who were between the ages of 18 and 65, with a non-penetrating TBI, engaged in either full-time or part-time employment at the time of injury, and unemployed or on medical leave at the time of receipt of intervention (participants could have been injured on or off the job); and (4) presented data separately for competitive (i.e., open or independent) employment and the non-competitively employed participants or students. Studies that included individuals with other disabilities were included only if the results were provided for TBI participants separate from those with other disabilities. The designs of the included studies could be randomized controlled trials (RCTs) or quasi-experimental designs, with a treatment group and a control/comparison group consisting of treatment as usual, other appropriate interventions, or no intervention.
Types of Participants
Participants were between the ages of 18 and 65 years of age, had a non-penetrating TBI, engaged in either full-time or part-time employment at the time of injury, were unemployed or on medical leave at the time of receipt of intervention, and were injured either on or off the job. All included studies consisted of only participants with TBI. No subsets of TBI participants were used. Penetrating TBI was not included because these injuries have a more complex sequelae and require more extensive rehabilitation than non-penetrating injuries.
Types of Interventions
To be included, studies must have used interventions that helped working-aged adults with TBI to return to competitive employment (including self-employment), with competitive employment as the outcome. The intensity of the intervention could vary. All intervention types—such as transitional, supported, and holistic strategies—were included.
Types of Outcome Measures
Primary Outcomes
The primary RTW outcome was a dichotomous variable, competitive employment status, in which individuals with TBI were either employed full-time or part-time for 45 days or more or not employed. The premise for using competitive employment as the one outcome variable is that competitive employment represents optimal real-world functioning. The definition of competitive employment was based on three criteria: Employed individuals with TBI perform employment-related tasks in an integrated setting (i.e., not a disability organization) and must interact with co-workers who are predominantly non-disabled. Employed individuals with TBI are hired and paid by the business where the work is performed, not by a disability organization (such as facility-based program or sheltered workshop). In this way, competitively employed individuals with TBI have the same risks of losing their position as non-disabled individuals. Employed individuals with TBI are also paid commensurate with that received by non-disabled co-workers who have similar qualifications and perform similar duties. When an individual with TBI is competitively employed, the individual vied for a position against individuals without disabilities, which is more difficult than sheltered employment or volunteer work, and, in most cases, more difficult than entering an educational program. In contrast, individuals who volunteer or are employed in facility-based programs typically work at lower performance or production standards than those required in competitive employment. Opportunities to re-do their performance through retaking exams or courses are not typically available in competitive work environments.
Secondary Outcomes
Based on the protocol (Graham & West, 2014), expected secondary outcomes were length of time to competitive employment and hours worked. However, none of the studies included reported this information. Thus, no secondary outcomes were analyzed.
3.2 SEARCH METHODS FOR IDENTIFICATION OF STUDIES
3.2.1 Language and Geographic Origin
The search was restricted to published or unpublished research written in English or Spanish and published between 1973 and 2015. To include reports in all languages would be untenable and fiscally burdensome to include in this report.
3.2.2 Electronic Searches
Two trained research assistants conducted the literature search, sixteen databases (with 125 sub-search engines within them) were divided between the two research assistants. Each research assistant searched one database at a time, using appropriate search terms (see Table 2) for the database, before moving on to the next assigned database. One research assistant was assigned to conduct grey literature searches not related to databases.
A spreadsheet was constructed and shared with authors and research assistants to maintain a record of searches. Each database had a separate tab in which the name of the searcher, date, database, search string, year, first author, journal/source, title, and DOI were entered. Each day, research assistants reviewed titles of documents located during the search that appeared to describe an employment intervention. If research assistants could not determine relevance from the title, they read the abstract. These relevant abstracts and all search results were saved as PDFs by the research assistants and uploaded to a shared electronic folder, as well as printed out for record-keeping. Two authors (Graham and West) reviewed each relevant abstract and requested the full article for those that appeared appropriate for the systematic review. If documents were not available online, research assistants acquired copies from the university library or submitted an interlibrary loan request. These documents were subsequently added to the shared online folder for review.
Studies for this review were identified by searching 16 databases: Australia Education Index/Australian Council for Educational Research, CIRRIE - Center for International Rehabilitation Research Information and Exchange Database, www.ClinicalTrials.gov, Cochrane Central Registry of Controlled Trials, Ebrary: Academic Complete Collection, EBSCOhost Research Database, First Search, Google Scholar, MEDLINE/PubMed, NARIC REHABDATA, ProQuest, PsycEXTRA, PsycINFO, Science Direct, Web of Knowledge, and Web of Science. Within First Search, nine sub-search engines were searched. Within ProQuest, 47 sub-search engines were searched. Within EBSCOhost, 69 sub-search engines were searched. Further, unpublished papers and grey literature were also searched. Reference lists of papers included in the analysis and previous systematic reviews concerning RTW employment and TBI were also searched.
Grey papers were also searched via 67 national and state websites, which included eight international websites: Great Britain
European Union Australia
European Union Grey Papers
3.3 DATA COLLECTION AND ANALYSIS
3.3.1 Selection of Studies
Three team members (Graham, West, & Inge) independently reviewed the amassed abstracts of articles and reports selected by the research assistants as potentially eligible for the systematic review. Articles were then screened by title and abstract. If the title and abstract suggested that the article might meet the inclusion criteria, the article was assigned to two of the three authors for review. Each author was assigned a set of articles to review, which included coding and determining whether the study should be included. Each reviewer used the approved coding template, in which characteristics of the study were coded, such as type and description of intervention, number of subjects, group and subject characteristics, and data needed for analysis. (See Appendix or Graham and West, 2014, for coding template.) reviews stopped if the reviewer determined that the article did not meet the inclusion criteria. After both assigned authors had reviewed the article, the authors met to discuss the article, coding, and inclusion decision. Each article was discussed concerning coding. If there was a difference in coding, the authors discussed the coding and came to a consensus, inclusion required both assigned reviewers to come to a consensus on coding and the inclusion decision. A consensus of included studies for this systematic review was reached without requiring a third reviewer to resolve selection conflicts. None of the authors were involved in any of the studies reviewed, and a third-party reviewer was not needed to minimize bias.
3.3.2 Data Extraction and Management
After coding included studies, inter-rater reliability was established above 85%. Using coded forms for each included study, the authors entered data into Comprehensive Meta-Analysis 2.2 software.
Assessment of Risk of Bias in Included Studies
Cochrane's risk of bias tool (i.e., sequence generation, allocation concealment, blinding, incomplete data, and selective outcome reporting; Higgins & Altman, 2008), along with study design, review status, type of publication, and control group, were used to assess the chance of bias. Each factor was coded as low risk, high risk, or unclear/unknown for each potential study to be included, “unclear” means insufficient detail was reported in the study, what was done in the study was unknown and the risk of bias is therefore unknown, or the risk of bias item was irrelevant to the study (Higgins & Altman, 2008). This latter point is especially relevant with regard to blinding and incomplete data on the outcome variable (Higgins & Altman, 2008). For more information concerning the high risk, low risk, or unclear ratings, see the coding form in the Appendix. In addition, design, review process, publication type, and presence of a control group (Higgins & Altman, 2008) were coded for quality. This was completed at the time of coding, included in the coding template, and discussed by the two assigned reviewers.
Data from the three identified random control studies were entered into Comprehensive Meta-Analysis 2.2 software (CMA) from coding sheets. All three studies compared two interventions. Each study was entered into the CMA program. As the protocol states (Graham & West, 2014), multiple time points for employment status (event) reported within a single study were averaged, and the average employment status was the datum used. No meta-analysis was performed (as stated in the protocol) because of the small number of studies. Odds ratios and standard error for log odds ratios were computed, and a forest plot of the effect sizes was constructed, as stated in the protocol (Graham & West, 2014).
Unit of Analysis Issues
The unit of analysis for this synthesis was at the group level, since each study had two viable and independent intervention groups.
Dealing With Missing Data
Attrition occurred in all groups. The total number used in the calculations was the total number in the intervention at the last time point. A description of missing data is provided in the results section.
Assessment of Heterogeneity
As stated in the protocol (Graham & West, 2014), we had planned to assess heterogeneity by interpreting the statistical significance of Qs and the value of I2. The criteria for determining heterogeneity were a statistically significant Q (p < 0.05) and a moderate I2 of 0.50 (Borenstein, Hedges, Higgins, & Rothstein, 2009). Due to the small number of studies identified, a meta-analysis was not performed and the assessment of heterogeneity was not needed.
Assessment of Reporting Biases
As stated in the protocol (Graham & West, 2014) we planned to use a funnel plot to assess publication bias (Biostat, 2005). This was not performed due to the small number of included studies.
Subgroup Analysis
As stated in the published protocol (Graham & West, 2014), we planned to conduct eight subgroup comparisons: (1) level of education pre-injury; (2) severity of TBI; (3) type of intervention; (4) provider (demand- or supply-side); (5) duration of intervention using six-month increments (six months or less, 6.1 months to 12 months, etc.) i ; (6) subject population (civilian or military); (7) where the injury occurred (fall, motor vehicle/traffic accident, colliding with an object, assault, combat/terror); and (8) type of comparison group (no intervention, treatment as usual, other intervention). These were not performed due to the small number of studies and lack of information.
Group Comparisons
Group comparisons were not performed due to the small number of studies.
Sensitivity Analysis
Sensitivity analysis was not performed, as mentioned in the protocol (Graham & West, 2014).
4 Results
4.1 DESCRIPTION OF STUDIES
4.1.1 Results of the Search
An extensive literature search was completed on VR and RTW of adults with TBI (see Figure 2).
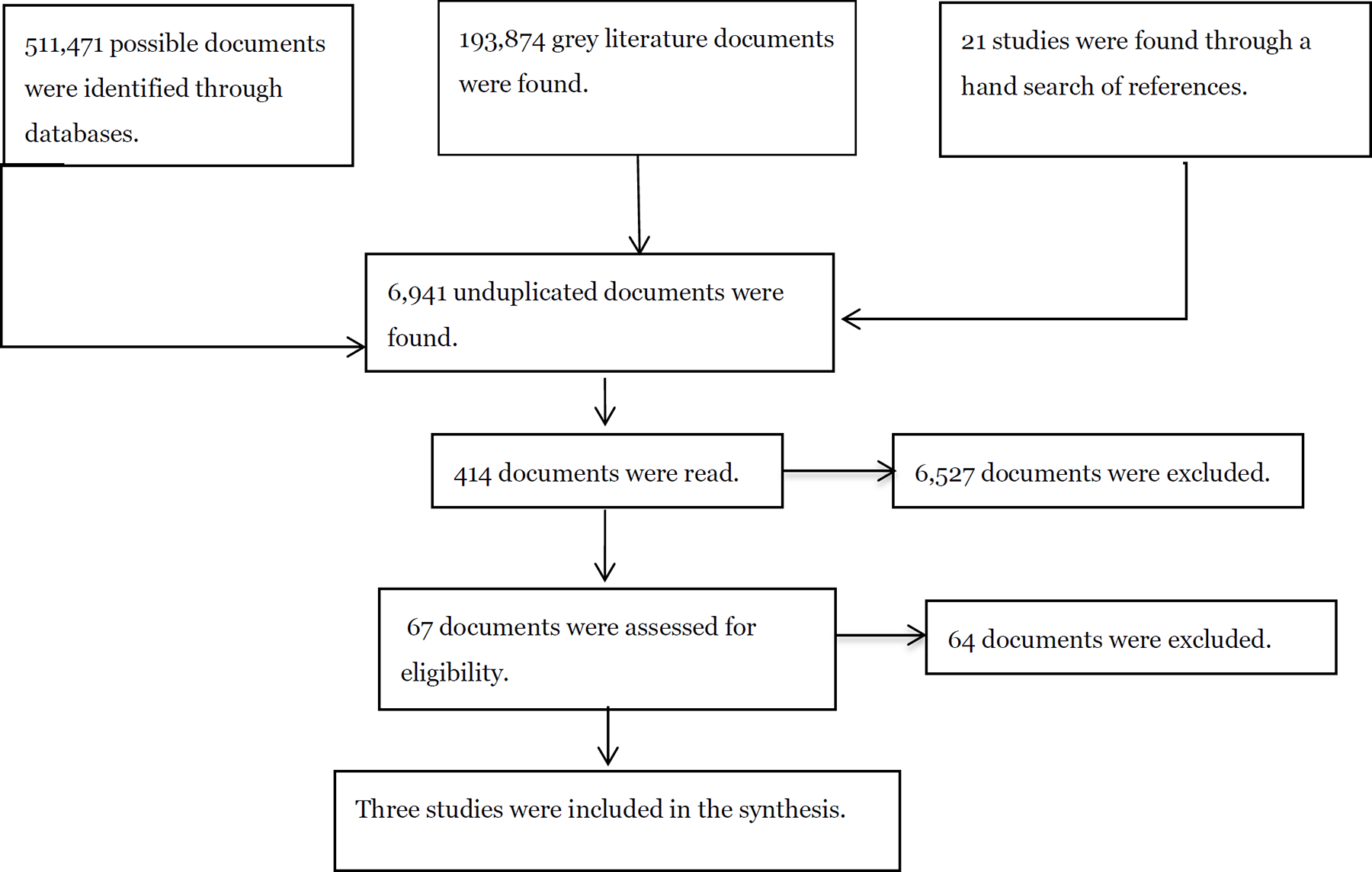
Specific overview of article selection.
The literature search utilized 16 search engines and 125 sub-search engines to search for published, peer-reviewed articles and grey literature. In addition, 67 websites were searched for grey literature. This yielded a total of 705,362 studies, which included duplicates (511,471 possible documents within the search engines 193,874 documents examined on Internet websites with grey literature and 21 additional articles found through hand searching past systematic reviews and primary study reference lists). In order To manage data, a series of Google Drive folders were constructed. The “All Search Documents” folder contained a folder for each search engine. Each of these search engine folders consisted ofcontained the actual search results for each term used research assistants who were assigned search engines kept track of the number of documents found in the “Unduplicated Results” folder. After each search term was run in a search engine, the research assistant would determine the overall number of hits, upload the search hits, screen each hit by article title of the article to determine whether further examination was needed by other team members, and determine whether there were duplicates from past searches. Of those 705,362 documents, 6,941 were unduplicated. The document title and abstract were read to determine whether documents were relevant to the systematic review. Unpublished articles with titles and abstracts that were considered potentially eligible were recorded in the “All GreyDocument” spreadsheet file. The record for a potential grey document consisted contained of name of the research assistant, date found, website address, year the document was published, author, title, type of document (e.g., dissertation, presentation, etc.), search string that located the document, and note (access status). When the document was available, a copy of the document was uploaded into the “Grey PDFs” folder. Once the document had been read by a researcher, the document would be either moved to the “Print Out” folder for further review or to the “Viewed” folder. Researchers discussed which studies should be examined further. The identified documents were then printed out for further review. If it was decided that the study might fit the criteria, researchers coded the document. Documents in the “Viewed” folder were those found not to meet the inclusion criteria. Peer-reviewed articles were processed similarly. From these 6,941 documents, the abstracts of 374 peer-reviewed articles and 40 grey literature documents were reviewed. Of the 414 peer-reviewed and grey documents examined, 67 presented findings on the effectiveness of interventions for RTW for working-aged adults with TBI and were assessed for eligibility. The last search was conducted on November 7, 2015.
4.1.2 Included Studies
Of the 67 intervention study reports identified, only three studies (Man, Poon, & Lam, 2013; Salazar et al., 2000; Twamley, Jak, Delis, Bondi, & Lohr 2014, and Twamley et al. 2015) fit all of the inclusion criteria. Note that Twamley reported outcomes in two articles. These two articles are being counted as one article, as both articles concern the same study. All three RCTs included in this review used other interventions that were suspected to be less effective than the “treatment” group. Below, both the primary treatment and alternate treatment groups are described.
The Man et al. (2013) study was a RCT study conducted in China with a civilian sample. This study was conducted with 50 individuals who had mild to moderate TBI and were recruited from Hong Kong hospitals and rehabilitation facilities. Man et al. did not report The cause of TBI. Inclusion criteria required participants to have a loss of consciousness of less than six hours. There was no report of mean length of loss of consciousness for either group. However, the Glasgow Coma Scale was used to assess the severity of TBI, and the mean score on this scale was 10.25 (SD = 1.51; Range = 9-14) for the artificial intelligent virtual reality-based training program (AIVTS; treatment group) and 10.05 (SD = 1.31; Range= 9-13) for the psycho-educational vocational training system (PEVTS; second intervention). No time since injury information was reported.
In the Man et al. study (2013), 50 participants were randomly assigned to either the first intervention group (AIVST) or the second intervention group (PEVTS) (Man et al., 2013). Each group began with 25 participants. Both groups had similar informational content but the training platform differed by group. The AIVST group received 12 sessions using a 3-D artificial intelligence reality-based training software program. The program begins the training by determining the skill level of the participants. As the participant progresses through training, the program can upgrade, maintain, or downgrade the training level to meet the training needs of the participant based on performance. Therefore, when participants performed well, the program would increase difficulty. If the participant's performance declined, the program would revert to previous levels of training.
The PEVTS group also received 12 training sessions with similar problem-solving tasks, content, and structure, given by a vocational trainer. The trainer provided instruction, time to practice skills, and games on problem solving specified by the manual. The fidelity of the administration of this intervention was assessed by four trained rehabilitation professionals. The fidelity agreement intra-class coefficient was 0.645, P = 0.021.
Although the study authors referred readers to a demographic table, no demographic table was published in the article. Forty participants (20 per group) provided three follow-up reports of employment outcome at one, three, and six months. Primary outcomes consisted of Tower of London assessment, Wisconsin Cord Sorting Test, Vocational Cognitive Rating Scale, and employment outcomes. Employment outcomes were measured by four categories: full-time employment, supported employment, sheltered employment, and unemployed/unable to return to work. No other employment measures were reported.
Of the 20 participants in the AIVTS group (treatment group) that were assessed at follow-ups, 17 (85%) were unemployed and three (15%) were employed at one month; 14 (70%) were unemployed and six (30%) were employed at three months; and 12 (60%) were unemployed and eight (40%) were employed at six months. Of the 20 participants in the PEVTS group that were assessed at follow-ups, 20 (100%) were unemployed and zero were employed at one month; 16 (80%) were unemployed and four (40%) were employed at three months; and 16 (80%) were unemployed and four (40%) were employed at six months. The odds ratio was 2.204 (95% confidence interval [CI] = 0.459, 10.573).
The Salazar et al. (2000) study was conducted on a United States military sample and is based on three articles that used the same dataset from one RCT with parallel group interventions: (1) an intensive in-hospital, cognitive treatment group, and (2) an in-home program without a VR group (Braverman et al., 1999; Salazar et al., 2000; Warden et al., 2000). The Salazar et al. (2000) article was the complete report that met all the inclusion criteria for this systematic review and was used in this review.
The Salazar et al. (2000) study was an RCT with parallel treatment groups, conducted with 120 active duty military service persons who had acquired a TBI. There is some discrepancy in the reporting of the severity of injury. Salazar et al. report that the injuries were “moderate to severe” (p. 3035), but state later that the injuries were “relatively severe” based on “the rates of axonal shear injury on MRI (92% and 95%), cerebral contusions (51% and 54%), posttraumatic amnesia of 7 days or more (41% to 42%), and traumatic unconsciousness for 24 hours or more (30% and 38%), respectively, in the hospital and home treatment groups” (p. 3077). Another article from this study reported “moderate to severe TBI” (p. 1100) based on “all patients reaching] the inclusion criteria of Rancho los Amigos level of 7” (Warden et al., 2000, p. 1097). Most participants obtained TBI through motor vehicle/traffic incident, assault, and alcohol-related accidents. The mean loss of consciousness was 35 hours. All participants were within 90 days of injury. Participants in the study were randomly assigned to one of the two treatment groups. Each group had a separate treatment team from the other, and the treatment teams worked independently. There were periodic reviews of the treatment teams in order to maintain fidelity to each treatment protocol.
The 67 active duty military participants assigned to the in-hospital, cognitive treatment group received eight weeks of intense cognitive rehabilitation program. Their mean age was 24.7, 93% were male, 69% were White, 24% were African American, and 7% were “other” or not specified. Participants had either moderate to severe TBI or severe TBI with a Glasgow Coma score of 9.4.
This in-hospital, cognitive treatment program consisted of a team of interdisciplinary practitioners, including a physiatrist, neuropsychologist, occupational therapist, speech pathologist, and rehabilitation assistants. The physical therapist and psychiatric and neurological experts were consulted when needed. The participants in the group were expected to follow military standards and a structured daily routine. The structured daily routine consisted of physical fitness training, and group and individual therapies. Therapies included cognitive, psychotherapy, pragmatic speech, community re-entry, and integrated work programs.
The 53 active duty military participants assigned to the in-home without VR intervention treatment group received a limited home rehabilitation program. Their mean age was 26, 96% were male, 70% were White, 17% were African American, 11% were Hispanic, and 2% were Native American. All had moderate to severe TBI or severe TBI with a mean Glasgow Coma score of 9.5.
The in-home rehabilitation program included TBI education and individual counseling by a psychiatric nurse, who made weekly 30-minute phone calls to each participant. Educational materials and strategies to improve cognitive and organizational skills were given to participants. Participants were also trained in card game exercises and were encouraged to watch the news and read. They were also expected to resume daily physical fitness training. No participants in this group received vocational or work rehabilitation.
The Salazar et al. study (2000) reported on the 12-month outcome evaluation. Sixty participants (90%) in the in-hospital, cognitive treatment group returned to work, whereas 50 of 53 participants (94%) in the in-home treatment group returned to work with an odds ratio of 0.514 (95% CI = 0.126, 2.093). See Table 3 for the characteristics of the included study.
Twamley et al. (2014, 2015) also conducted a RCT with parallel treatment groups. Fifty United States veterans with mild to moderate TBI from recent conflicts participated. Twenty-five were randomly assigned to the supported employment with CogSMART group (treatment group) and 25 were randomly assigned to the enhanced supported employment group. Only 42 participants completed the study, with 21 participants in each of the two groups. Time since most recent TBI was 4.08 years (SD=2.78) for the CogSMART group (treatment one group) and 5.04 years (SD=4.61) for the enhanced supported employment group (treatment two group) (p=0.377). The majority of participants in each group were men (96% in each group). The two groups were also similar in composition in terms of the number of participants who identified as Hispanic (36%). Twenty-four percent of the treatment one group and 48% of the treatment two group identified as White. The mean length of loss of consciousness across the last four traumatic brain injuries was six hours for the treatment one group and one hour for the treatment two group (p=0.274). There was a statistically significant difference between the two groups in terms of participants' age. The treatment one group had a mean age of 29.68 (SD=6.05), and the treatment two group had a mean age of 33.84 (SD=7.89) (p = 0.042). A statistically significant difference was also reported in education. The treatment one group had a mean of 12.88 years (SD=1.2.7), versus 14.00 years (SD=1.80) for the treatment two group (p=0.014). The odds ratio for this comparison was 0.881 (95% CI = 0.235, 2.844).
All participants in both groups received supported employment for one year. For the first three months of the intervention, the treatment one group received supported employment and CogSMART, while the treatment two group received additional supported employment sessions. CogSMART addressed post-concussive symptoms, prospective memory, attention and vigilance, learning and memory, and executive functioning (see cogsmart.com for more information). The treatment one group received one hour of CogSMART and one hour of supported employment per week for the first three months, and then one hour of supported employment for the rest of the year. The treatment two group received two hours of supported employment for the first three months, and then one hour of supported employment for the rest of the year. Separate employment specialists worked with each group.
Each group lost four participants during the course of the study or at follow-up, which left each group with 21 participants each. There was no difference in competitive employment at 12 months, with both groups having 13 participants (52%) in employment. Thus, CogSMART did not improve the odds of employment for the treatment one group. The supported employment sessions that both groups received may have contributed to this finding. Further research with three groups—CogSMART only, CogSMART and supported employment, and supported employment only—needs to be conducted.
Man et al. (2013) did not report on any demographic data such as gender, race/ethnicity, or education level. Twamley presented the demographic data previously mentioned, but the reporting across the two articles published on this study varied (Twamley et al., 2014, 2015).
For the Salazar et al. (2000) study, the primary outcome was employment status, and it was reported in binary form at twelve-month follow-up. None of the other articles concerning this study reported other time points (Braverman, 1999; Warden et al., 2000). The secondary outcome data—mean hourly wage and total days employed—were not reported in this study.
Man et al. (2013) used four categories to measure employment: (1) full-time employment, (2) full-time supported employment, (3) sheltered employment, and (4) unemployed or unable to work. For this review, full-time employment and full-time supported employment were summed to determine the number of competitively employed participants. Sheltered employment and unemployed/unable to be employed were summed for the unemployed group. Employment data were collected and reported at three time periods: one month, three months, and six months (See Table 1).
Twamley et al. (2014, 2015) reported that employment status was collected at three, six, and twelve months. Twamley et al. reported three-month employment data in one study (2014). The second article states that three-month, six-month, and twelve-month outcome data would be presented, but Twamley et al. (2015) only reported twelve-month results in this article. Six-month data were not reported in either article, and further literature searches did not yield any documents reporting the six-month data. Only the binary data of whether participants were employed or not was collected. No other employment-oriented outcomes were measured, such as those of interest to this study—total days employed and mean hourly wage.
studies reported employment status at different time periods ranging from one month to six months. Two studies (Man et al., 2013; Twamley et al., 2014) reported employment outcomes at three months. Salazar et al. (2000) and Twamley et al. (2015) reported employment outcomes at 12 months. Twamley et al. (2015) stated that three-month, six-month, and twelve-month outcome data would be reported, but only twelvemonth employment findings were reported in this article. The overall analysis was performed on the latest time period for each study, which was 12 months for the Salazar et al. (2000) and Twamley et al. (2015) studies, and six months for the Man et al. study (2013). Sensitivity analysis was conducted to determine whether this was problematic. (See Table 1.)
Lastly, none of the studies reported to be intent-to-treat studies. Two studies had attrition: Man et al. (2013) lost three participants in the artificial intelligence group and none of the participants in the psychoeducational group. Twamley et al. (2014, 2015) lost four in each of the two groups (CogSMART Plus group and enhanced supported employment group). Salazar et al. (2000) did not report attrition. This was an active military sample and the type of participants might have contributed to no attrition being reported. Data were used as reported. In the two studies where participants dropped out, the total number remaining in the sample was used. Thus, findings for the participants who remained are included in the Results section.
4.1.3 Excluded Studies
Sixty-four of the 67 study reports did not meet the inclusion criteria. The excluded studies included eight randomized controlled trials (RCT), 13 non-randomized pre-post two-group studies, one non-randomized pre-post three-group study, 22 pre-post one-group studies, 11 retrospective studies, five case studies, and one description of an intervention. Below, the RCT and non-randomized pre-post designs are summarized. The RCTs included cognitive rehabilitation (Cicerone et al., 2008; Vanderploeg et al., 2008), multidisciplinary rehabilitation programs (Powell, Heslin, & Greenwood, 2002; Zhu, Poon, Chan, & Chan, 2007), early intervention (Wade, Crawford, Wenden, King, & Moss, 1997), motivational interviewing by way of the telephone (Bell et al., 2005), resource facilitation (Trexler, Trexler, Malec, Klyce, & Parrott, 2010), and individualized tailored treatment (Andersson, Emanuelson, Björklund, & Stålhammar, 2007). Five used control groups (Andersson et al., 2007; Bell et al., 2005; Powell et al., 2002; Trexler et al., 2010; Wade et al., 1997), and three used comparison treatment groups (Cicerone et al., 2008; Vanderploeg et al., 2008; Zhu et al., 2007). All but one study used civilians in their study (Andersson et al., 2007; Bell et al., 2005; Cicerone et al., 2008; Powell et al., 2002; Wade et al., 1997; Trexler et al., 2010; Zhu et al., 2007). The other study used veterans (Vanderploeg et al., 2008). TBI severity ranged from mild to severe, with two studies not reporting severity. The sample size ranged from 68 to 483. These studies were conducted in China, Sweden, the United Kingdom, and the United States. Most RCTs were rejected because some of the participants were under 18 years of age (Andersson et al., 2007; Bell et al., 2005; Powell et al., 2002; Wade et al., 1997; Trexler et al., 2010; Zhu et al., 2007), or because some participants did not work at the time of injury (Andersson et al., 2007; Bell et al., 2005; Cicerone et al., 2008; Trexler et al., 2010; Wade et al., 1997; Zhu et al., 2007). One RCT was rejected because it combined RTW with school and did not present separate findings (Vanderploeg et al., 2008).
The 13 non-randomized pre-post two-group studies and the one non-randomized pre-post three-group study (High, Roebuck-Spencer, Sander, Struchen, & Sherer, 2006) will also be described. The interventions used in these studies included neuropsychologic interventions (Prigatano et al., 1984; Prigatano et al., 1994; Sarajuuri et al., 2005; Wilier, Button, & Rempel, 1999), community-based interventions (Heinemann, Corrigan, & Moore, 2004; High et al., 2006; O'Neill, Zugger, Fields, Fraser, & Pruce, 2004; Ponsford, Harrington, Olver, & Roper, 2006), cognitive interventions (Cicerone, Mott, Azulay, & Friel, 2004; Dawson, Binns, Hunt, Lemsky, & Polatajko, 2013), occupational interventions (Radford et al., 2013), work entry interventions (Haffey & Abrams, 1991), comprehensive day interventions (Hashimoto, Okamoto, Watanabe, & Ohashi, 2006), and an employment enhancing program with club houses (Niemeier et al., 2010). There was one non-randomized pre-post three-group study (High et al., 2006), which will also be described. Ten studies used control groups (Cicerone et al., 2004; Dawson et al., 2013; Hashimoto et al., 2006; Niemeier et al., 2010; O'Neill et al., 2004; Prigatano et al., 1984; Prigatano et al., 1994; Ponsford et al., 2006; Radford et al., 2013; Sarajuuri et al., 2005; Willler et al., 1999), and four compared treatments (Haffey & Abrams, 1991; Heinemann et al., 2004; High et al., 2006). All used civilians. TBI severity ranged from mild to severe. The sample size ranged from 13 to 319. These studies were conducted in Australia, Canada, Finland, Japan, the United Kingdom, and the United States. Most of these studies were rejected because not all participants were employed at the time of injury (Cicerone et al., 2004; Haffey & Abrams, 1991; Hashimoto et al., 2006; Heinemann et al., 2004; Ponsford et al., 2006; Prigatano et al., 1984; Prigatano et al., 1994; Radford et al., 2013; Sarajuuri et al., 2005). Other reasons for exclusion included the following: not all participants were over the age of 18 years (Radford et al., 2013; Sarajuuri et al., 2005); employment category was unclear, which made it difficult to determine whether competitive employment was assessed or not (O'Neill et al., 2004); some participants were employed at the beginning of the treatment (Dawson et al., 2013); and separate findings were not provided for TBI (Niemeier et al., 2010; Wilier et al., 1999).
Studies had to have a control or comparison group to be included in this systematic review. Thus, all of the pre-post only-group studies were excluded from the review. The interventions found among the 22 pre-post one-group studies included neurorehabilitation (Bjorkdahl, 2010; Ezrachi, Ben-Yishay, Kay, Diller, & Rattok, 1991; Geurtsen et al., 2011; Geurtsen et al., 2012; Klonoff, Lamb, & Henderson, 2000; Klonoff, Lamb, & Henderson, 2001; Perino, Zappala, Verne, & Rago, 2000); supported employment (Curl, Frasier, Cook, & Clemmons, 1996; Ellerd & Moore, 1992; Malec & Moessner, 2006; Wehman et al., 2003); club house (Vandiver & Christofero-Snider, 2000); cognitive therapy (Braverman et al., 1999; Walker, Onus, Doyle, Clare, & McCarthy, 2005); transitional job coaching (Preston & Ulicny, 1992); in-home rehabilitation (Warden et al., 2000); comprehensive outpatient rehabilitation (Ben-Yishay, Silver, Piasetsky, & Rattok, 1987); multidisciplinary interventions (Christensen, 1992); community-based interventions (Kolakowsky-Hayner, Wright, Shem, Medel, & Duong, 2012); interpersonal communication training; attention training; community training; and personal counseling (Rattok et al., 1992). The severity of TBI ranged from mild to severe, and sample sizes ranged from 9 to 603. Two studies were military (Braverman et al., 1999; Warden et al., 2000) and were one-group analyses of the Salazar et al. (2000) study included in this review. The other 20 studies were civilian. These studies were conducted in Australia, Denmark, Italy, the Netherlands, Sweden, the United Kingdom, and the United States. See Table 4 for more information concerning the characteristics of the excluded studies.
4.1.4 Location of Study
Two of the three included studies were conducted in the United States (Salazar et al., 2000; Twamley et al., 2014, 2015). The other study (Man et al., 2013) was conducted in China.
4.1.5 Participants
Sample sizes ranged from 40 to 120 participants, with a total sample size across the three included studies of 146. Two studies provided the proportion of males and mean age (Salazar et al., 2000; Twamley et al., 2014, 2015). The unweighted mean age for study participants was 28.56. The Salazar et al. and Twamley et al. samples were predominantly male, ranging from 93% to 96% male, with a mean of 95.25. Salazar and colleagues (2000) used active military samples from the United States, and Twamley et al. (2014, 2015) used U.S. military veterans. Man and colleagues (2013) used civilians in China. The Salazar et al. (2000) sample was predominantly African American and White, and there were more Hispanic/Latino and White participants in the Twamley et al. (2014, 2015) study. Man and colleagues (2013) did not report the ethnicity or race of their sample from China. The Twamley et al. (2014, 2015) and Man et al. (2013) studies reported severity of injury as mild to moderate. There were inconsistencies in the reporting of severity in the Salazar et al. (2000) study, with most places in the document reporting moderate to severe and one location in the Salazar et al. document reporting only severe injuries.
4.2 RISK OF BIAS IN INCLUDED STUDIES
A funnel plot was created, as stated in the protocol, to determine publication bias. (See Figures 3 and 5). too few articles were found to say that there was no publication bias because only three studies were included in the review. However, using log odds ratio on the horizontal axis and standard error on the vertical axis, the funnel plots were not symmetrical. Caution should be used in interpreting this funnel plot as an indication that there is no bias. The trim and fill analysis was performed and the point estimate for this analysis was 0.942 (df= 2) with 95% CI = 0.420, 2.183; Q = 2.188, p = 0.335 and the funnel plot was asymmetrical, which indicates bias (See Figure 4.).
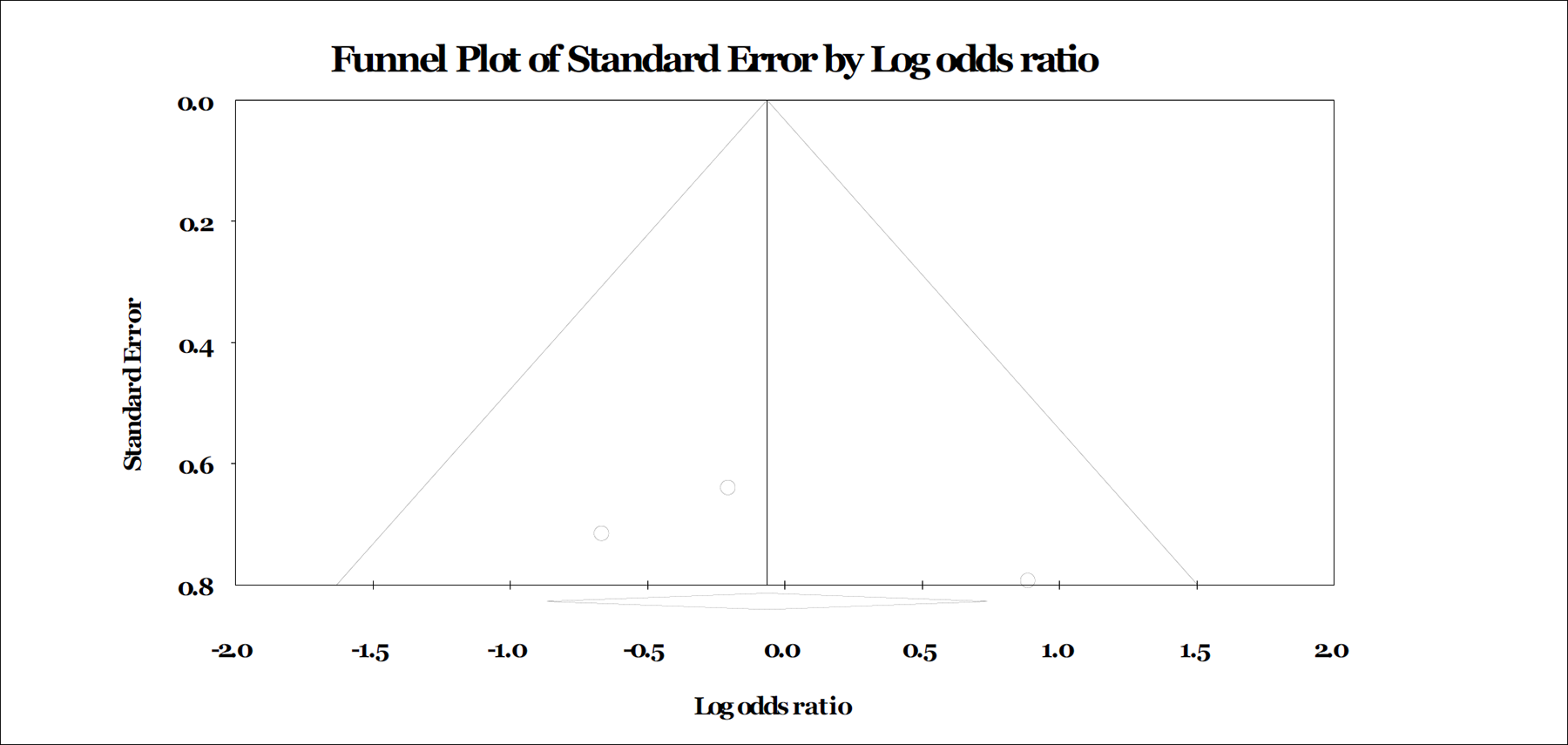
Standard Funnel Plot.
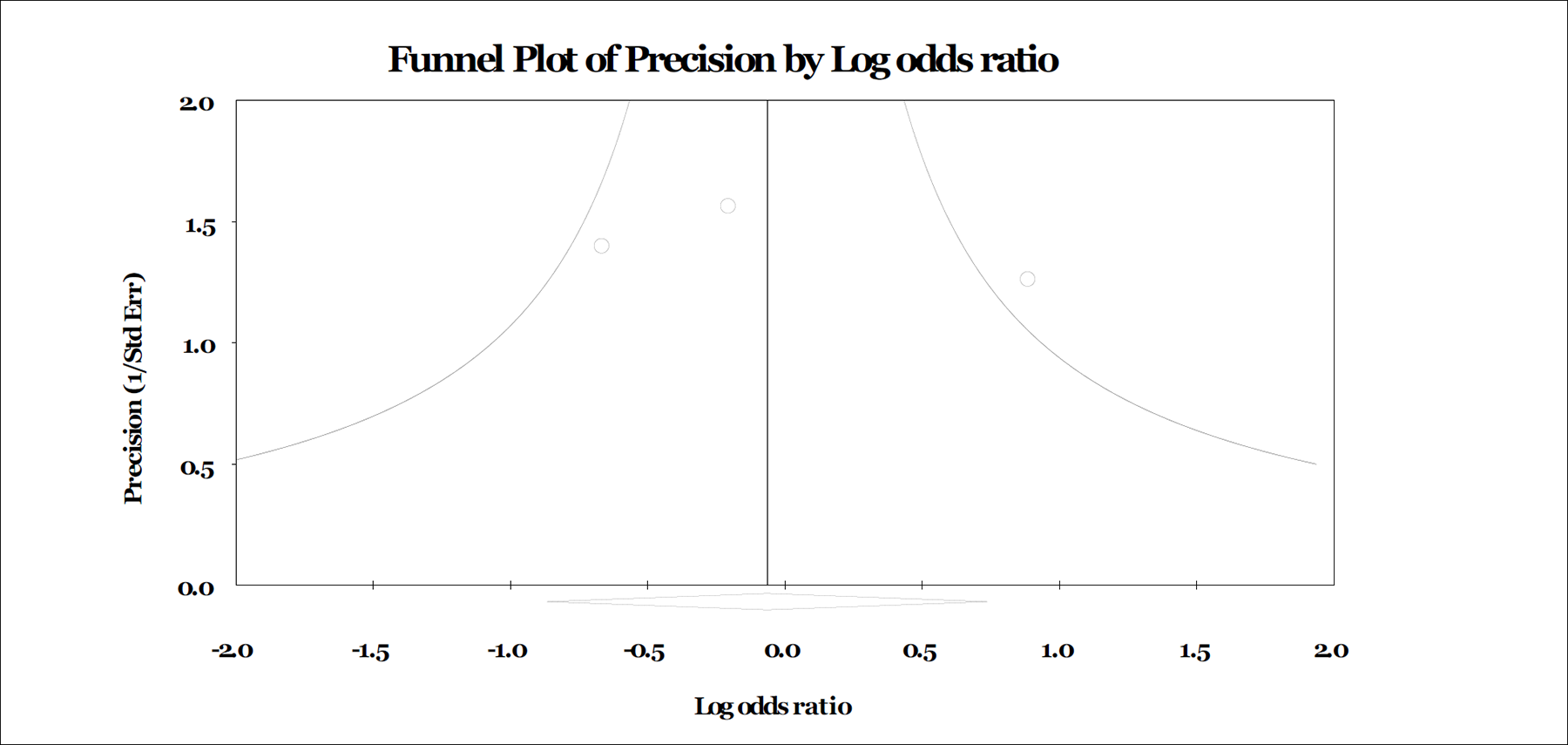
Precision Funnel Plot.
Each of the included studies was assessed on the following five factors of risk of bias: allocation concealment, blinding, sequence generation, incomplete outcome data, and selective outcome reporting. Studies were rated as low risk, high risk, or unclear/unknown on each of the five factors. Based on the findings in Table 4, it is clear that there is risk of bias, especially in allocation of concealment, blinding, and selective outcome reporting. All three studies had a high risk of bias for allocation concealment (Man et al., 2013; Salazar et al., 2000; Twamley et al., 2014, 2015). All three were at low risk for sequence generation because all three stated that they used randomized assignment. However, none of the studies discussed the process of randomization. All were at high risk of selective outcome reporting because Salazar et al. (2000) and Twamley et al. (2014, 2015) did not report the employment status of participants at all times the data were collected. Man et al. (2013) only collected and reported data during the first six months, not at 12 months. Further, none of the studies included additional employment information other than employment status. These studies did not report on hours worked, length of time worked, or wages paid, which would provide a better understanding of the success of the employment situations.
Design, review status, publication type, and the presence of a control group were also examined. All were experimental studies. The Man et al. (2013) and Salazar et al. (2000) studies used a parallel design, in which another intervention was used. In the Man et al. study, the PVETS was used as the comparison (second intervention) group. In the Salazar et al. study, an in-home intervention was used. Both of these interventions were less intense than the treatment groups. The Twamley et al. study said it used a control group that received less intense treatment. However, it could be argued that framing the use of enhanced supported employment as a control group may have been inappropriate, since supported employment is an intervention. Thus, we considered all three studies to have alternate treatment (second intervention) groups that had the possibility of being as effective as the primary treatment group, which biased this systematic review. See Table 4 for a summary of all risk of bias factors.
4.3 SYNTHESIS OF RESULTS
None of the odds ratios were statistically significant. A comparison of the odds ratios was not conducted due to the small number of studies. No one intervention can be identified as being the most effective. Below, the odds ratios of each study are discussed.
Man et al. (2013) hypothesized that participants in the virtual reality-based vocational training program would have better employment outcomes compared to participants in the conventional psychoeducational vocational training program. Four groups were used to organize employment status: unemployed, sheltered workshop, supported employment, and open (competitive) employment. No participants reported sheltered workshop involvement. The odds ratio above was computed with supported employment included in the competitive employment count, as stated in the methods section. The odds ratio indicated that participants in the virtual reality training were 2.204 times as likely to be competitively employed than participants in the psychoeducational training program. Although the odds ratio indicated that virtual reality training was more effective than psychoeducational training, the rate of employment for the virtual reality program was only 30%, compared with 15% for the psychoeducational training. Thus, the average unemployment rate was 70% for the virtual reality training, and 85% for the psychoeducational training program. Even though the statistically non-significant odds ratio indicated that the virtual reality training was twice as effective as the psychoeducational training, the employment rate was still low.
The Salazar et al. (2000) study hypothesized that of the two parallel groups, the intensive in-hospital rehabilitation program would have a greater number of participants returning to work than the at-home program. The statistically non-significant odds ratio indicated that participants in the in-hospital program were 0.514 times as likely to be employed as participants in the at-home program. In addition, the employment rates of both intervention groups were high, with the majority of the in-hospital (89%) and at-home (94%) participants returning to work.
Twamley et al. (2014) hypothesized that the supported employment plus CogSMART group would have better rates of job placement when compared to the enhanced supported employment group. The statistically non-significant odds ratio in this study indicated that participants in the supported employment plus CogSMART group were 0.815 as likely to be competitively employed as participants in the enhanced supported employment group. Further, the supported employment plus CogSMART group had an average job placement of 55% across the two time periods (3 months and 12 months), while the enhanced supported employment group had an average job placement of 60%.
In summary, all odds ratios were statistically non-significant. No comparisons of the three included studies were performed. No one intervention was more effective, although all interventions led to competitive employment for some of their participants.
4.3.2 Sensitivity Analysis
This review did not have an adequate number of studies to conduct a meta-analysis to determine group differences. A larger number of studies might have been included in this systematic review if inclusion criteria had included (1) a broader range of brain injuries, and (2) a broader definition of employment to include sheltered employment and/or employability (i.e., volunteerism and engaging in post-secondary education). Broadening the diagnosis to include acquired brain injury, including non-traumatic diagnoses such as cerebral anoxia, aneurysm, carbon monoxide poisoning, cardiac arrest, and brain tumour (Bergquist et al., 2012; Geurtsen et al., 2012; Malec & Moessner, 2006; Rattok et al., 1992; Sloan et al., 2009), had the potential to increase the number of studies included. However, all five of the excluded studies that included participants with acquired brain injury did not meet other inclusion criteria. A few studies were one-group, no-comparison-group studies (Bergquist et al., 2012; Geurtsen et al., 2012), and others studies did not use competitive employment as the outcome (Geurtsen et al., 2012; Malec & Moessner, 2006; Rattok et al., 1992; Sloan et al., 2009). Broadening employment to include sheltered employment, volunteerism, and educational achievement would also have provided a larger number of studies to include. However, it would not have provided information on how effective interventions were at returning people with TBI to work in a competitive setting with people without TBI. The ultimate goal of vocational research interventions is to help people with disabilities such as TBI find employment with people without disabilities, rather than segregating people with TBI into sheltered employment. Furthermore, sheltered employment, volunteer work, and school do not have the same high standards as competitive employment.
4.4 SUMMARY OF MAIN RESULTS
Three RCTs comparing two intervention groups were found. The three RCTs consisted of an active military sample (Salazar et al., 2000), a veteran sample (Twamley et al., 2014, 2015), and a civilian sample from China (Man et al., 2013). Interventions included an intensive in-hospital program versus an at-home program (Salazar et al., 2000); CogSMART plus supported employment versus enhanced supported employment (Twamley et al., 2014, 2015); and virtual reality-based training versus psycho-educational training (Man et al., 2013). Two studies involved U.S. military personnel: one used active military personnel (Salazar et al., 2000) and the other used a veteran population involved in recent conflicts (Twamley et al., 2014, 2015). The last study used a civilian sample located in China (Man et al., 2013). All odds ratios were statistically non-significant. A meta-analysis was not performed due to the small number of included studies. Although all study interventions led to competitive employment, no one intervention was identified as more effective than the rest. A larger sample of studies is needed to provide a conclusive determination. None of the studies reported secondary employment outcomes: hours worked and wages earned.
The Man et al. (2013) study trained individuals with TBI using two different methods to determine which intervention was more effective in assisting participants to gain employment. Most of the outcome variables measured were cognitive. One intervention consisted of a computer-based, 3-D, virtual-reality training program, and the other intervention was described as a conventional psycho-educational approach. The hypothesis was that individuals who were trained with the computer-based training program would have higher problem-solving skills and better employment outcomes than the group that received psycho-educational training. Employment outcomes were measured as competitive full-time employment, competitive part-time employment, supported employment, and sheltered employment. Competitive full-time and part-time employment and supported employment were considered competitive employment for the purposes of this review.
Both groups were tested using a number of cognitive tests and an “on-site, work performance test.” The work-performance test included clerical tasks similar to those used for the training interventions. Testing was not conducted to evaluate whether the participants generalized problem-solving skills to a workplace or job.
Neither group showed improvements in the on-site test, although there were differences in employment between the groups. This finding is important to consider, because teaching problem-solving skills that do not generalize to an actual work setting may be counter-productive and may expend valuable resources that should be used for other services, such as supported employment. Supported employment addresses a person's difficulty with generalizing by providing training in skills that an individual with TBI needs on the job and not in simulated settings.
Man and his colleagues (2013) reported that poor employment outcomes were related to participants' lack of interest in obtaining employment, a poor economy, supported employment as a new initiative in Hong Kong, and legal limitations. If these assertions are correct, additional research is needed that explores participant interest in obtaining employment after China has fully accepted supported employment, and with participants who are not involved in legal situations that may inhibit them from seeking employment. In addition, future research should include outcomes such as wages, access to benefits, increased hours worked, job tenure, and job satisfaction.
Twamley and her colleagues' description of supported employment and the manner in which they implemented the intervention are of concern (Twamley et al., 2014, 2015). Twamley reported that the CogSMART group received one hour of supported employment and one hour of the CogSMART intervention per week, for a total of two hours of intervention per week. The enhanced supported employment group received two hours of supported employment. Supported employment services for both groups was defined as one-hour sessions provided in a location of the individual's choice, such as the career center, home, coffee shop, library, or VA clinic.
Although supported employment can be provided away from the individual's job site, as defined in the Workforce Innovation and Opportunity Act, no other information was provided on the types of supports that were delivered during the intervention. In other words, there is no information on what the employment specialists did with the participants during these sessions. Supported employment supports can include assessment, assistance with the job search/job development, job placement, on-the-the job training, and ongoing supports throughout the person's job tenure. These supports are based on the needs of each individual and can be provided off as well as on the individual's job site. In addition, the intensity of the intervention or amount of time spent providing services varies based on an individual's needs and typically fades as the individual requires less assistance. Since no information was provided on the types of supported employment supports that the participants received, replication of the supported employment intervention is problematic.
While the authors concluded that the CogSMART intervention was associated with reductions in post-concussive symptoms, there is no evidence that this intervention was associated with improved employment outcomes. Using supported employment as a component of the intervention in the comparative group is also problematic. It is uncertain whether the supported employment intervention or the CogSMART intervention affected the employment outcomes reported by the researchers. In addition, no statistical difference was found for the employment outcomes achieved by either group. Clearly, additional research is needed to determine if the CogSMART intervention affects the competitive employment outcomes of individuals with TBI.
Salazar et al. (2000) evaluated the effectiveness of in-hospital cognitive rehabilitation versus an in-home rehabilitation program in returning veterans with TBI to employment. Patients were randomly assigned to the two interventions. The in-hospital group received physical fitness training, as well as group and individual cognitive, speech, occupation, and coping skills therapy. The afternoon sessions included integrated work therapy, including coordinated placement in various work settings similar to the individual's military specialty. Participants in the in-home intervention were given recommended strategies to improve their cognitive skills, including training in card game exercises, reading books, and watching news programs. This group also received weekly 30-minute telephone calls from a psychiatric nurse. The researchers hypothesized that the in-hospital group would experience greater RTW and fitness for military duty at a one-year follow-up. Results of the study found that there were no statistically significant differences in RTW for the two groups, with 90% of the hospital group and 94% of the in-home group returning to work at one-year post follow-up. Although this study reported high employment rates, the odds ratio of 0.514 was not significant (p = 0.353).
4.5 OVERALL COMPLETENESS AND APPLICABILITY OF EVIDENCE
4.5.1 Duration of Follow-Up
All of the studies (Man et al., 2013; Salazar et al., 2000; Twamley et al., 2014, 2015) followed Participants for six months (Man et al., 2013) and 12 months (Salazar et al. 2000; Twamley et al., 2014, 2015) after the end of the RTW intervention. Note that Twamley et al. (2014) stated that three-month, six-month, and twelve-month results were reported in the article, but only the twelve-month follow-up competitive employment status outcome data were reported in this article. In all of the studies, information is not provided on the latency between completion of the program and employment experiences during the follow-up period. It is unknown how long it took participants to obtain employment, or whether they were placed in a single or multiple employment positions within the 12 to 18 months. Future research should continue to follow participants for at least 12 months and should report the length of time taken to achieve employment, the number of placements, and the duration of each placement in order to assess the extent of engagement in the competitive workforce following treatment.
4.5.2 Coverage of Outcomes
This review focused on competitive employment as the primary outcome because it is the optimal level of real-world functioning and the most appropriate measure of the success of a RTW intervention. This diverges from much of the extant research, which tends to combine college student status, sheltered employment, and competitive employment. Some past studies have also used level of productivity as the outcome variable. Due to the number of ways in which RTW can be assessed, future research should report separate rates for all possible outcomes, rather than combining outcomes.
Neither of the secondary outcomes—time to employment and hours worked—were analyzed due to lack of data. In order to understand the effectiveness of RTW vocational interventions, future research should also report time until employment and hours worked per week.
4.5.3 Origin
Two of the three studies used military samples and were only applicable to military populations in the United States. Further, while the use of military samples is relevant today due to the Global War on Terror, it is unknown whether this intervention is effective with civilian samples. Although the Man et al. (2013) study used a Chinese sample, study samples need to be more diverse. Future research is needed with people from other countries, and with civilians.
4.6 QUALITY OF THE EVIDENCE
All the studies were RCTs with parallel treatment groups. However, there is some concern about the effectiveness of these interventions compared to a true control group. The three studies included in this systematic review used parallel groups that received an intervention. This is different from comparing a known inferior intervention or no intervention to an intervention. While this allows two effective interventions to be compared to determine which is best, it is not possible to determine the effect size of the interventions in the absence of a true control group. It would have been helpful to have control groups with no intervention as a point of comparison.
Other issues that impact the quality of the evidence concern blinding, incomplete data, and selective outcome reporting. Blinding was only attempted by Salazar et al. (2000); Man et al. (2013) and Twamley et al. (2014, 2015) did not blind. Incomplete data was also an issue for the studies as a result of attrition, lack of demographic data, inconsistent use of the same severity measure, and data collection at different time points. Having this information would have increased the sample size and provided more information on which to compare studies using demographic data. Not having data at the same time point is problematic. More subjects could have gained employment from six to twelve months in the Man et al. (2013) study. Collecting and reporting employment status more frequently (e.g., at three months and six months) would help to understand the efficacy of the interventions. Salazar et al. (2000) and Twamley et al. (2014, 2015) did not provide this information.
The studies were selective in their reporting of findings and data. All of the studies only reported on competitive employment status. No other employment data were reported. Employment status was the primary outcome, but this alone does not provide a clear understanding of RTW for persons with a TBI. number of hours worked and wages earned provide important information on effectiveness. An intervention that leads to employment in which a person is working 35 or more hours a week is important to note. Further, wage information is important to determine whether people with TBI will be able to earn enough money to live or lift themselves out of poverty. Thus, selective reporting of employment status only, and not hours worked and wages earned, impedes assessments of efficacy.
In sum, the strengths of these studies were that they were experimental, they randomly assigned participants to groups, they were peer reviewed, and they were published in academic research journals. The weaknesses of the studies include lack of blinding, incomplete data, selective reporting, and a lack of comparison groups.
4.7 LIMITATIONS AND POTENTIAL BIASES IN THE REVIEW PROCESS
4.7.1 Limitations
The limitations of this systematic review are the study quality and number of included studies. Findings from this review may have been different if more studies had been included, and if the studies were of a higher quality than the ones included.
4.7.2 Potential Biases in the Review Process
Four issues in the review process might have contributed to potential bias: (1) including studies that had all been published in peer-reviewed journals, (2) coding studies into type of interventions, (3) determining whether studies were supply-side or demand-side interventions, and (4) language bias.
An international grey literature search was conducted using internet databases that included or consisted only of grey literature, as well as an international search of peer-reviewed studies. The results of these searches were four studies published in peer-reviewed journals. Although studies were not limited to those published in English, a study that meets the criteria may not have been found because it was published in a language other than English or Spanish.
Coding studies into types of interventions was discussed among the authors and colleagues. It was determined that supported employment intervention would be used as a broad category that included support from rehabilitation professionals on the supply-side and co-workers or employers on the demand-side.
Language bias was evident in the review process. Only articles written in either English or Spanish were reviewed, and all databases were in English.
4.8 AGREEMENTS AND DISAGREEMENTS WITH OTHER STUDIES OR REVIEWS
Although this systematic review had fewer studies than other TBI systematic reviews, this review had higher quality studies compared to previous systematic reviews (Brasure et al., 2013; Cancelliere et al., 2014; Fadyl & McPherson, 2009; Geurtsen et al., 2010; Kendall, Muencherberger, & Gee, 2006; Rohling, Faust, Beverly, & Damakis, 2009; Van Velzen, Van Bennekom, Edelaar, Sluiter, & Frings-Dresen, 2009; Virk, Williams, Brunsdon, Suh, and Morrow, 2015). The one exception was Virk and associates (2015), which examined cognitive interventions for people with acquired brain injury with attention as the outcome. Both this study and the Virk et al. (2015) study used only random control trials (RCTs).
Productivity—which includes employment as well as other productivity activity, including education—was used as the outcome in the other RTW/productivity systematic reviews. Brasure et al. (2013) examined RCTs and cohort studies and used a more inclusive outcome variable—productivity. Kendall and colleagues (2006) also examined productivity and return to competitive employment in treatment and non-treatment studies. Fadyl and McPherson (2009) included RCTs, other quantitative studies, secondary analyses, and qualitative research, and examined a range of RTW outcomes including job retention and stability. The other systematic reviews examined intervention characteristics (Geurtsen et al., 2010), prognosis of return to work (Cancelliere et al., 2014), number of people with TBI who return to work (Van Velzen et al., 2009), and cognitive functioning (Rohling et al., 2009; Virk et al., 2015). Combining return to work and school attendance in productivity is problematic in these studies. Attending or completing school does mean a person with TBI will be able to obtain employment afterward. However, it would be helpful and more rigorous for TBI intervention studies to provide separate findings for those who obtain employment and those who are attending school.
The Findings from the systematic reviews that examined vocational interventions for RTW indicated that there are interventions that are effective in returning people with TBI to competitive employment, but there was no one intervention that was more effective (Brasure et al., 2013; Fadyl & McPherson, 2009; Kendall et al., 2006). The present systematic review concurs with these past systematic reviews. It is worth noting that Brasure and colleagues (2013) mentioned that intensive cognitive rehabilitation showed promise as being an effective intervention for return to work. However, Virk et al. (2015) reported in their systematic review that none of the cognitive treatments were currently effective at remediating any dimension of attention, which is an important piece of cognitive treatment.
The use of competitive employment as the sole outcome was unique to the present systematic review. Kendall et al. (2006) included a variety of RTW variables in their systematic review, including competitive employment. Kendall et al. found that studies with more inclusive definitions of RTW (such as productivity) reported higher employment rates than studies in which competitive employment was the outcome. However, those who were competitively employed were more likely to continue to be engaged in employment than people who were engaged in other productive activities (Kendall et al., 2006).
In sum, this systematic report offers tentative findings for military interventions and samples, but, as with other systematic reviews, offers no conclusive findings on the most effective intervention. This systematic review was different in that it included only RCTs and used a higher standard of employment outcome (i.e., competitive employment) than other studies.
5 Authors' Conclusions
5.1 IMPLICATIONS FOR PRACTICE AND POLICY
Implications for Practice and Policy
Job placement and vocational experts working in the field with clients who have TBI, especially moderate to severe TBI, are faced with a myriad of challenges. These include the obvious cognitive and social-emotional issues, but may also include self-awareness of TBI limitations, substance abuse, family and marital challenges, and service provider limitations in understanding how to place, train, and retain these individuals in employment. TBI is a lifelong disability, which requires (for the most part) ongoing support from the family and the service provider community, such as VR.
This systematic review does not provide conclusive findings regarding an effective intervention. Although the odds ratios of the Salazar et al. (2000) and Twamley et al. (2014, 2015) studies were below one—which means that the alternate interventions were more effective—the treatment and intervention employment rates were higher than the Man et al. (2013) study, with the employment rate ranging from 55% for the CogSMART plus supported employment intervention (Twamley et al.) to 94% for the at-home intervention in the Salazar et al. study. Hence, we conclude that all employment interventions lead to employment, though we cannot identify the most effective treatment. Each study used a different intervention and population.
The summary of excluded studies indicates that not all interventions currently in use were represented in this study. In addition, these three studies provide limited information to assist service providers provide ongoing supports (e.g., information about the intensity, frequency, or nature of these supports in the long term). Additional work is needed with standard follow-up times (such as three, six, 12, and 18 months) to effectively compare findings.
These three studies have limited implications for practice and policy. Although they were randomized control studies, the populations were substantially limited to military subjects, who present with significantly different comorbidities and unique challenges (such as posttraumatic stress disorder), which can often skew whether the population is actually brain injured. The previous competitive employment histories of many of the subjects were also unclear. A meta-analysis of all of the subject outcomes might be helpful in this regard.
5.2 IMPLICATIONS FOR RESEARCH
Some of the interventions used in this review—in-home (Salazar et al., 2000), in-hospital (Salazar et al., 2000), and supported employment (Twamley et al., 2014, 2015) interventions—are innovative and promising approaches to assist individuals who return to work. However, it remains difficult to find replication efforts or evidence that these approaches are being widely used by individuals with TBI. To improve access to this option, there is a need to establish mechanisms for educating and training individuals with TBI and their family members, as well as VR professionals and direct service staff. Individuals with TBI and family members need information about effective interventions (e.g., upon discharge from an outpatient or inpatient medical unit, and at follow-up at selected intervals, such as three months, six months, one year, and five years post-discharge). This may offer an opportunity to assist some individuals with returning to their preinjury employer in the same or a new position. Based on our previous research concerning VR professionals' beliefs, knowledge, and willingness to engage in evidence-based practices (Graham, Inge, Wehman, Murphy, Revell, & West, 2013; Inge, Graham, Erickson, Sima, West, Cimera, In Press), VR professionals, first and foremost, must understand and embrace the basic principles associated with effective interventions (e.g., power of workplace supports). They must become skilled at successfully individualizing services and supports that focus on the career goals and preferences of individuals.
There is a need for more evidence-based prospective studies that compare the efficacy of different interventions based on the work outcomes of persons with TBI. Studies that compared the outcomes of supported employment versus competitive employment that occurs without job coach supports would be helpful, as would studies comparing self-employment outcomes versus competitive employment outcomes. There is also a need for studies that examine whether the time of intervention makes a difference to the outcome. In addition, the use of peer mentors, the role of co-workers, and the role of the family-friend network all need to be investigated longitudinally. Further long-term follow-up, beyond the twelve months after intervention, is also needed to provide information on the use of follow-up employment services and employment outcomes.
There is a clear need for public funding sources and services for this population beyond the federal/state VR program. The lack of funding for work services is a major problem, given that many third-party insurance companies do not cover these services. From a policy perspective, this is an enormous obstacle that will need to be resolved.
More creative ways to measure employment services are also needed, besides the use of employment rate. Employment rates often skew our understanding of the person with TBI's learning trajectory. For example, a monthly employment ratio—total number of months the person could be employed versus actual months of employment—would allow for a more sensitive assessment.
There needs to be significantly more effort aimed at training rehabilitation counselors, special education teachers, transition specialists, case managers, and psychologists on the work capacity and potential of persons with TBI. The initial work performance of many individuals with TBI is likely to be a failure but eventually can grow into success, although not without knowledge of workplace supports. These supports involve understanding the government's role, the agency or clinical role, and the individual's role and perspectives.
There are several recommendations for the direction of research concerning RTW for adults with TBI. First, VR researchers must improve the quality of research by conducting randomized controlled trials (RCTs) on RTW interventions with adults with TBI. Second, separating competitive employment from school attendance would provide a more accurate estimate of RTW. Third, military interventions should be conducted with civilian samples in order to determine their effectiveness in the civilian population. Fourth, research is needed from other populations outside the United States. Fifth, studies need to include employment stability as an outcome. This can be measured by the amount of hours and days of post-employment services required by each participant, as well as the length of time in a job. Last, studies need to collect and report data at standard intervals (e.g., six months, 12 months, 18 months, etc.). This would allow reviews to provide a more accurate account of the effectiveness of the different interventions. Last, future RTW VR studies should report: Time to employment Hours worked Separate rates of competitive employment, sheltered employment, educational training, etc. Continued follow-ups at 12 months Employment outcome and employment characteristics, collected every six months for at least 18 months The number of employment experiences during the follow-up period, including the duration of each experience Employment stability, measured by length of time worked at each job and number of jobs since intervention at each follow-up.
Footnotes
7 Information About This Review
8 Tables
9 Data and Analyses
Appendix 3. Coding Form for Primary Research Characteristics for Employment Interventions for Return to Work in Working-Aged Adults Following Traumatic Brain Injury (TBI) Systematic Review
Appendix 4: Coding Form for Primary Research Characteristics for Employment Interventions for Return to Work in Working-Aged Adults Following Traumatic Brain Injury (TBI) Systematic Review
i
For supported employment that states a length of intervention duration, we will use this information. For those supported employment studies in which the supportive intervention is ongoing, we will use the data collection times, such as 12 months and 30 months in the 1992 Ellerd & Moore study.