
Abstract
This Campbell systematic review examines the effectiveness of e-learning in improving evidence-based health care (EBHC) knowledge and practice.
Compared to no learning, pure e-learning improves EBHC knowledge and skills but not attitudes and behaviour. Pure e-learning is no better than face-to-face learning in improving any of the primary outcomes.
Blended learning is better than no learning for improving EBHC knowledge, skills, attitude and behaviour; and is better than face-to-face learning in improving attitudes and behaviour.
Compared to pure e-learning, blended learning improves EBHC knowledge. It is not clear which elearning components are most effective in improving outcomes.
However, the included studies were of moderate to low quality, with a small number of studies included in each analysis, and imprecision and inconsistency of results in all comparisons.
These shortcomings need to be taken into consideration when interpreting the results
Plain language summary
Blended learning is most effective in increasing evidence-based health care competencies of health workers
E-learning is a useful strategy to increase EBHC knowledge and skills, and when combined with face-to-face learning, to increase EBHC attitude and behaviour.
The review in brief
Evidence-based health care (EBHC) is decision-making for health care, informed by the best research evidence. Doctors, nurses and allied health professionals need to have the necessary knowledge and skills to apply EBHC. The use of electronic learning (e-learning) for EBHC training is increasing.
E-learning, compared to no learning, improves EBHC knowledge and skills but not attitudes and behaviour. There is no difference in outcomes when comparing e-learning to face-to-face learning. Combining e-learning with face-to-face learning (blended learning) has a positive impact on EBHC knowledge, skills, attitude and behaviour.
What did the review study?
Evidence-based health care (EBHC) involves phrasing questions based on a knowledge gap, searching for research that can answer the question, critically appraising and interpreting the research, applying the results and auditing the process. Electronic learning (e-learning) has become an increasingly popular method of teaching EBHC.
This review assesses the effectiveness of e-learning of EBHC for increasing EBHC competencies in healthcare professionals. The primary outcomes are EBHC knowledge, skills, attitude and behaviour.
What is the aim of this review?
This Campbell systematic review examines the effectiveness of e-learning in improving evidence-based health care knowledge and practice.
What studies were included?
Eligible studies were randomised controlled trials (RCTs), cluster RCTs, non-RCTs, controlled before-after studies and interrupted time series of any healthcare professional evaluating any educational intervention on EBHC, and that was delivered fully (pure e-learning) or in part (blended learning) via an electronic platform compared to no learning, face-to-face learning or other forms of e-learning of EBHC.
The review included 24 trials, comprising 20 RCTs and four non-RCTs, with a total of 3,825 participants. Participants were medical doctors, nurses, physiotherapists, physician assistants, athletic trainers and a combination of professionals at all levels of education. The studies included a variety of interventions.
What are the main findings of this review?
Compared to no learning, pure e-learning improves EBHC knowledge and skills but not attitudes and behaviour. Pure e-learning is no better than face-to-face learning in improving any of the primary outcomes.
Blended learning is better than no learning for improving EBHC knowledge, skills, attitude and behaviour; and is better than face-to-face learning in improving attitudes and behaviour. Compared to pure e-learning, blended learning improves EBHC knowledge. It is not clear which e-learning components are most effective in improving outcomes.
However, the included studies were of moderate to low quality, with a small number of studies included in each analysis, and imprecision and inconsistency of results in all comparisons. These shortcomings need to be taken into consideration when interpreting the results.
What do the findings of this review mean?
E-learning of EBHC, whether pure or blended, compared to no learning, improves EBHC knowledge and skills. There is no difference in these outcomes when comparing e-learning to face-to-face learning. Blended learning, which typically comprises multiple interventions, appears more effective than other types of learning in improving EBHC knowledge, skills, attitude and behaviour.
Future research should focus on the different components of e-learning and should adequately report on all the intervention components, the educational context and implementation strategies.
How up-to-date is this review?
The review authors searched for studies published until May 2016. This Campbell Systematic Review was published in March 2017.
Executive summary
BACKGROUND
It is important that all healthcare professionals acquire the knowledge and skills necessary to make healthcare decisions which are informed by the current best research evidence. Evidence-based health care (EBHC) typically involves phrasing questions based on a knowledge gap, searching for research that can answer the question, critically appraising and interpreting the research, applying the results and auditing the process. Electronic learning (e-learning) has become an increasingly popular method of teaching EBHC but literature on the effectiveness there of has not been synthesized and it is not clear which e-learning strategies are most useful.
OBJECTIVES
The primary objective of this review was to assess the effectiveness of e-learning of EBHC on increasing EBHC competencies in healthcare professionals. Secondary objectives were to assess the effectiveness of specific dimensions of e-learning in increasing EBHC competencies, to assess how educational context influences the effectiveness of EBHC e-learning, and to assess how implementation approaches influence the effectiveness of EBHC e-learning.
SEARCH METHODS
We searched MEDLINE, EMBASE, ERIC, CINAHL, CENTRAL, SCOPUS, Best Evidence Medical Education (BEME), Web of Knowledge, PsycInfo and dissertation databases (ProQuest) for relevant studies (24 May 2016). We examined reference lists of included studies and contacted experts in the field. We did not apply any language restrictions.
SELECTION CRITERIA
We considered randomised controlled trials (RCTs), cluster RCTs, non-randomised controlled trials (non-RCTs), controlled before-after studies (CBAs) and interrupted time series (ITS) of any healthcare professional at any level of education, evaluating any educational intervention that included any or all of the five steps of EBHC and was delivered fully (pure e-learning) or in part (blended learning) via an electronic platform compared to no learning of EBHC, face-to-face learning of EBHC or other forms of e-learning of EBHC. The primary outcomes were EBHC knowledge, EBHC knowledge and skills, EBHC skills, EBHC attitude and EBHC behaviour.
DATA COLLECTION AND ANALYSIS
Two authors independently screened search results and assessed eligibility of potentially eligible studies, extracted data and made judgments about risk of bias. Discrepancies were resolved through discussion or consultation of a third author. We contacted study authors in case of missing data. Due to high levels of heterogeneity between studies, we pooled results using random-effects meta-analysis and reported on the standardized mean differences (SMD) and 95% confidence intervals for each outcome.
RESULTS
We included 24 studies (20 RCTs and four non-RCTs) with a total of 3825 participants in the review. Participants included medical doctors, nurses, physiotherapists, physician assistants, athletic trainers and a combination of professionals at all levels of education. E-learning interventions were heterogeneous with 17 different intervention components. The interventions of five studies included only one component while the remaining interventions comprised various components in combination and were considered to be multi-faceted.
Overall we judged studies to be at moderate to high risk of selection bias and high risk of attrition bias. Meta-analyses contained a small number of studies and participants. Results were mostly imprecise and inconsistent. Our confidence in the following results is therefore low.
Primary outcomes
Pure e-learning vs no learning (3 studies)
Pure e-learning compared to no learning improved EBHC knowledge (SMD 0.71; 95%CI 0.40 to 1.01; 1 study, n=175) and EBHC attitude (SMD 1.05; 95%CI 0.26 to 1.83; 1 study, n=29). There was no difference between groups for EBHC knowledge and skills (SMD 0.47; 95%CI -0.27 to 1.21; 1 study; n=29).
Blended learning vs no learning (5 studies)
Blended learning compared to no learning improved EBHC knowledge (SMD 0.20; 95%CI 0.13 to 0.86; 1 study; n=119), EBHC knowledge and skills measured at one month post-intervention (SMD 0.90; 95%CI 0.42 to 1.38; 2 studies; n=241) and 3+ months post-intervention (SMD 1.11; 95%CI 0.80 to 1.42; 2 studies; n=186) and EBHC behaviour measured at 3+ months post-intervention (SMD 0.61; 95%CI 0.21 to 1.01; 1 study; n=100). There was no difference between groups for EBHC knowledge and skills measured immediately post-intervention (SMD 1.40; 95%CI -0.06 to 2.85; 2 studies, n=241), EBHC attitude (SMD 0.17; 95%CI -0.09 to 0.43; 2 studies; n=226), EBHC attitude measured at 1 month post-intervention (SMD 0.05; 95%CI -0.34 to 0.44; 2 studies; n=241) and 3+ months post-intervention (SMD 0.32; 95%CI -0.02 to 0.67), and EBHC behaviour measured directly post-intervention (SMD 0.06; 95%CI -0.28 to 0.40; 2 studies; n=207) and 1 month post-intervention (SMD 0.19; 95%CI -0.19 to0.56; 1 study; n=109).
Pure e-learning vs face-to-face learning (6 studies)
We did not find a difference between groups for EBHC knowledge (SMD -0.03; 95%CI -0.26 to 0.20; 5 studies, n=632), EBHC skills (SMD -0.15; 95%CI -0.34 to 0.04; 2 studies; n=457) or EBHC attitude (SMD 0.11; 95%CI -0.27 to 0.48; 1 study; n=111).
Blended learning vs face-to-face learning (5 studies)
We did not find a difference between groups for EBHC knowledge (SMD 0.28; 95%CI -0.23 to 0.79; 1 study; n=146), EBHC knowledge and skills (SMD -0.22; 95%CI -0.49 to 0.05) and EBHC skills (SMD -0.21; 95%CI -0.68 to 0.26). Scores for participants in the blended learning group were higher for EBHC attitude (SMD 1.07; 95%CI 0.57 to 1.58; 1 study; n=69) and EBHC behaviour (SMD 2.34; 95%CI 1.72 to 2.96; 1 study; n=69).
Blended learning vs pure e-learning (3 studies)
Blended learning compared to pure e-learning improved EBHC knowledge (SMD 0.69; 95%CI 0.40 to 0.99; 2 studies, n=193). For EBHC skills, results favoured pure e-learning for the non-RCT and blended learning for the RCT. There was thus significant heterogeneity between studies and the pooled effect showed no difference between groups (SMD -0.53; 95%CI -2.31 to 2.25; 2 studies; n=218).
Pure e-learning vs pure e-learning (3 studies)
We found that the interventions improved EBHC skills (SMD 1.30; 95%CI 0.68 to 1.93; 2 studies; n=119). Interventions were heterogeneous. One study compared a DVD containing recorded PowerPoints and tutorials, as well as access to online learning material to a standard online distance learning programme. The other compared an online journal club with an asynchronous discussion list to receiving the articles via email and access to journal articles.
Secondary outcomes
Secondary outcomes were poorly reported. Attrition rates of learners were high, but did not differ between groups. Four studies reported on satisfaction of learning but results were not conclusive and both advantages and disadvantages of both methods of learning were identified.
We were unable to address the secondary objectives of our review, as included studies provided insufficient information on educational context and implementation strategies. Meta-analyses generally contained a small number of studies, which prevented us from doing subgroup analyses on different dimensions of e-learning.
AUTHORS’ CONCLUSIONS
Our findings suggest that e-learning of EBHC, whether pure or blended, compared to no learning, improves EBHC knowledge and skills. We did not find a difference in these outcomes when comparing e-learning to face-to-face learning, suggesting that both methods of learning can be beneficial. It appears that blended learning, which typically comprises multiple intervention components, could be more effective than other types of learning in improving EBHC knowledge, skills, attitude and behaviour. These findings need to be considered in light of the limited number of studies per outcome in each comparison, risk of bias across studies and heterogeneous interventions, as well as inconsistent and imprecise results.
Future research on EBHC e-learning should focus on the effectiveness of various e-learning components and should explicitly report on all the intervention components, educational context and implementation strategies.
1 Background
1.1 THE PROBLEM, CONDITION OR ISSUE
1.1.1 The need for evidence-based health care competencies
Evidence-based medicine (EBM), introduced in 1991, has its roots in the field of clinical epidemiology and was listed as “one of the 15 greatest medical milestones since 1840” in the British Medical Journal (Montori & Guyatt, 2008). The most commonly used definition of evidence-based medicine (EBM) describes it as “the conscientious, explicit and judicious use of the current best evidence in making decisions about the care of individual patients” (Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996). It thus requires practitioners to bring together external evidence that informs about the effects of new tests, treatments and interventions; clinical judgement and expertise of the clinician; and the patient's clinical state, values, preferences, needs and predicament.
These days, EBM is commonly referred to as evidence-based practice (EBP) or evidence-based health care (EBHC), as EBM is not limited to medical doctors, but should be adopted by all healthcare practitioners. Practicing EBHC typically involves five steps: i) Formulating an answerable question from a healthcare problem; ii) finding the best available evidence applicable to the question; iii) critically appraising the evidence for validity, clinical relevance and applicability; iv) applying the results of the evidence in the healthcare setting; and v) evaluating the performance (Dawes et al., 2005). An important aim of EBHC is that beneficial, effective health care practices are adopted and that harmful and ineffective ones are abandoned. Consequently, this requires healthcare professionals to recognise their deficiencies in knowledge and to adopt a philosophy of life-long learning, which is the backbone of practicing EBHC (Greenhalgh, 1997).
The importance of the knowledge, skills and attitude learnt through the principles of EBHC are also highlighted in the Lancet report on the health professional for the 21st century (Frenk et al., 2010), which proposes that healthcare professional training should become transformative. One of the fundamental shifts of transformative learning aligns almost perfectly with the steps of EBHC; the shift from memorization of facts to “critical reasoning that can guide the capacity to search, analyse, assess and synthesise information for decision-making” (Frenk et al., 2010).
In addition, Glasziouand colleagues (2011) have urged educational institutions to teach medical students skills which enable them to become life-long learners so that they are able to combine external evidence from research with their own expertise and their patients’ values and preferences. They emphasize that teaching EBHC skills should form an integral part of the medical curriculum and be re-iterated and practiced throughout undergraduate and postgraduate training (Glasziou, Burls, & Gilbert, 2008; Glasziou, Sawicki, Prasad, & Montori, 2011).
In an evaluation of an online module of EBM, we have proposed a set of EBHC competencies that all healthcare professionals should ideally possess once they graduate (Rohwer, Young, & van Schalkwyk, 2013). These competencies comprise five key competencies that mirrorthe five steps of EBHC; and enabling competencies which include basic knowledge of epidemiology and biostatistics. Figure 1 is a graphic representation of the EBHC competencies.
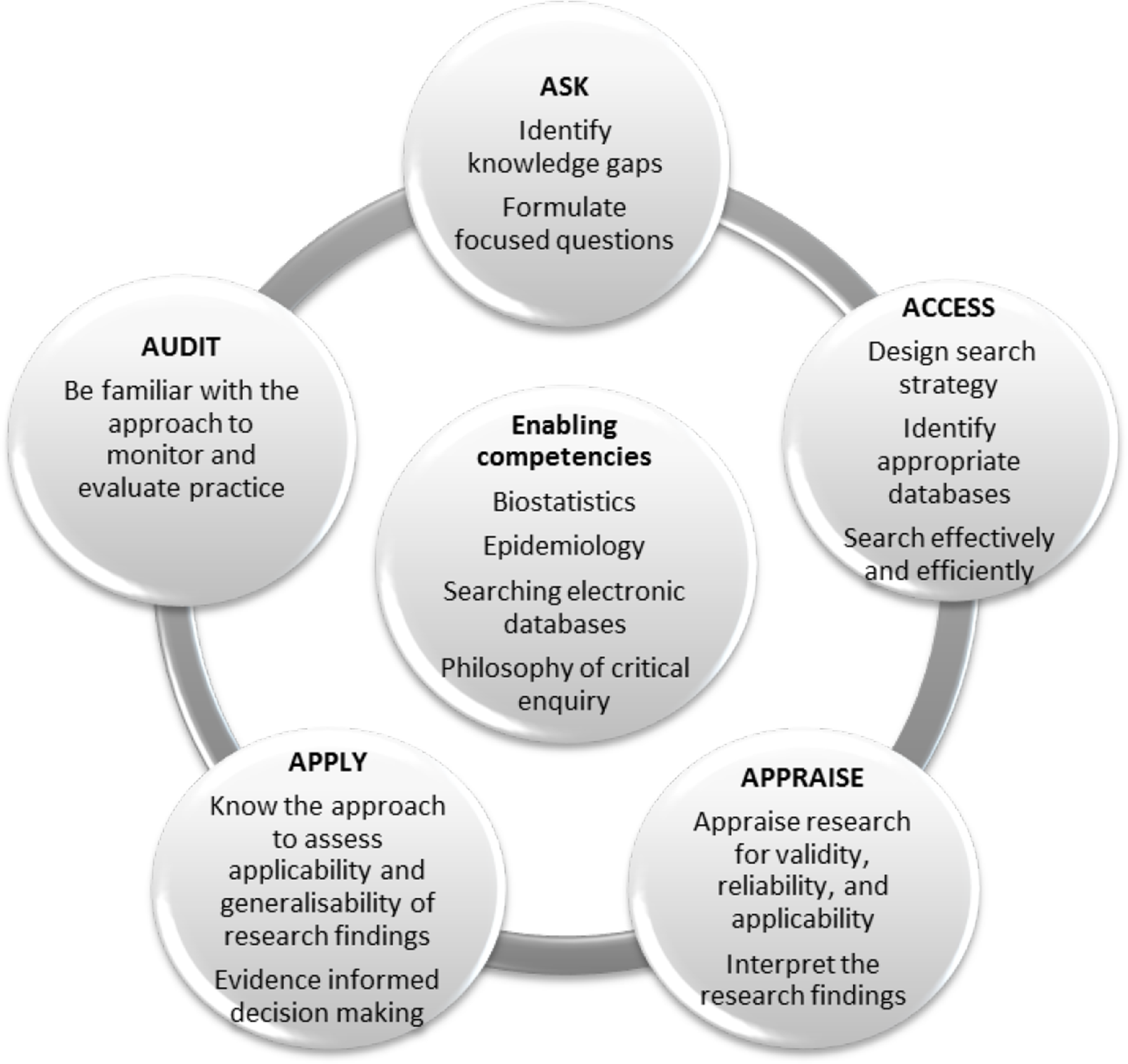
EBHC enabling and key competencies
A number of systematic reviews have explored the effects of teaching EBHC to healthcare professionals, both at an under- and postgraduate stage. From the results, it is evident that teaching EBHC to students and health care professionals leads to increased EBHC knowledge and skills (Young, Rohwer, Volmink, & Clarke, 2014). The question is therefore no longer whether we should be teaching EBHC; but rather how we should be teaching it. Khan and Coomarasamy (2006) have proposed a hierarchy of teaching EBHC, where integrated and interactive teaching is seen as the most effective way of teaching EBHC (Khan & Coomarasamy, 2006). This, however, only refers to traditional lecture-based or face to face teaching of EBHC and does not include the increasingly popular method of electronic learning.
1.2 THE INTERVENTION
1.2.1 Electronic learning (e-learning)
Electronic learning or e-learning (as the term is widely used) strategies have been widely adopted by educators around the world and it is not surprising that it has also become a buzz word amongst medical educators. E-learning, also called web-based learning, online learning, distributed learning, computer-assisted instruction and internet-based learning, can be defined as the delivery of training material via information and communication technology (ICT), including the internet, CD-ROM, DVD, smartphones and other media, both inside and outside of the classroom (Frehywot et al., 2013; Ruggeri, Farrington, & Brayne, 2013; Ruiz, 2006).
Pure e-learning refers to the use of e-learning materials only, without any face-to-face classroom methods. Although it seems to be synonymous to completely online learning, the difference between puree-learning and fully-online learning refers to the delivery platform. While online learning relies on a web-based delivery platform and requires internet access, pure e-learning can take place without internet access, for example, by using DVDs to deliver the educational content. Blended learning combines e-learning components with other traditional face-to-face, lecture-based learning in and outside of the classroom (Frehywot et al., 2013).
Advantages of e-learning include improved accessibility of educational materials at a time convenient to the learner; individualised or personalised learning, where the learner decides on the amount, pace and place, which allows personal tailoring of the learning experience and meeting of individual learner objectives; lower training costs; collaborative learning environments; the ability to track learner activity; and provision of consistent and standardized training to a larger number of learners all over the world (Clark, 2002; Ruggeri et al., 2013; Ruiz, 2006; Welsh, Wanberg, Brown, & Simmering, 2003).
Disadvantages of e-learning include costs related to the technologies as well as the staff needed, although most costs seem to occur at the development stage of e-learning courses; and social isolation or the lack of interaction among the participants of the e-learning activity or course. The lack of face-to-face networking and peer interaction can be seen as a huge drawback, making e-learning less attractive and less useful. Poor instructional design, technical problems and de-individualised instruction can also be regarded as disadvantages of e-learning (Cook, 2007; Welsh et al., 2003).
E-learning is a complex intervention with multiple components and dimensions that interact, in a linear or non-linear way, in a specific context (Wong, Greenhalgh, & Pawson, 2010). In the literature, different components, levels, dimensions and categories of e-learning have been described.
Ruiz et al. (2006) describe the components of e-learning as being i) the development of content ii) management of the content and iii) delivery of the content. Regarding development of content, digital learning objects, i.e. “any grouping of digital materials structured in a meaningful way and tied to an educational objective”, are the fundamental components of lessons, modules and curricula; created with the help of instructional design and pedagogical principles. Examples of digital learning objects include tutorials, case-based learning scenarios, hypermedia, simulations and game-based learning modules (Ruiz, 2006).
Management of content encompasses the administrative functions (storing, indexing, cataloguing) needed to make content available to learners through portals, repositories, digital libraries, learning management systems, search engines and e-Portfolios (Ruiz, 2006).
Content can be delivered in a synchronous or asynchronous way. Synchronous delivery of content refers to real time, instructor-led learning, where all learners receive information simultaneously and communicate and interact directly with other learners by logging onto platforms like virtual classrooms (e.g. teleconferencing, internet chat forums, instant messaging). Asynchronous delivery of content occurs when the transmission and receipt of information occurs at different time points. It can include pre-recorded presentations or podcasts, PowerPoint slides, or even more sophisticated applications like simulations. While asynchronous communication is done by means of email, online bulletin boards, listservs, newsgroups, wikis or weblogs, it enables learners to participate in the learning activity at any time of day, from any desired location (Ruiz, 2006; Welsh et al., 2003).
Ruggeri et al. (2013) describe the different dimensions and attributes of e-learning programmes under four headings: Synchronicity (asynchronous vs synchronous), location (same place vs distributed), independence (individual vs collaborative) and mode (electronic-only vs blended) (Ruggeri et al., 2013).
Cook (2005) describes four levels of instructional design in computer-based learning: Medium, which refers to the mode of delivery of instruction (e.g. textbook, face to face, computer-based, television); configuration, referring to the “big picture” differences within a given media format (e.g. computer: web-based discussion board, web-based or CD-ROM-based tutorial vs face to face: small-group discussion, lecture); instructional method, referring to teaching techniques that support learning processes (e.g. learning activities, self-assessment questions, clinical cases, simulations, group discussions); and presentation, referring to elements of the given medium that enhance the intervention, but do not qualify as instructional methods (e.g. hyperlinks, multimedia, font simulation fidelity etc.) Cook (2005).
We developed a system-based logic model of e-learning of EBHC, based on a template from Rohwer et al. (2016) depicting the different components, contextual factors and interactions that are needed to achieve the desired outcomes (Figure 2). In an effort to teaseout the characteristics and dimensions of e-learning interventions in order to be combined meaningfully, we have only listed the broad categories that we thought of as being most important.
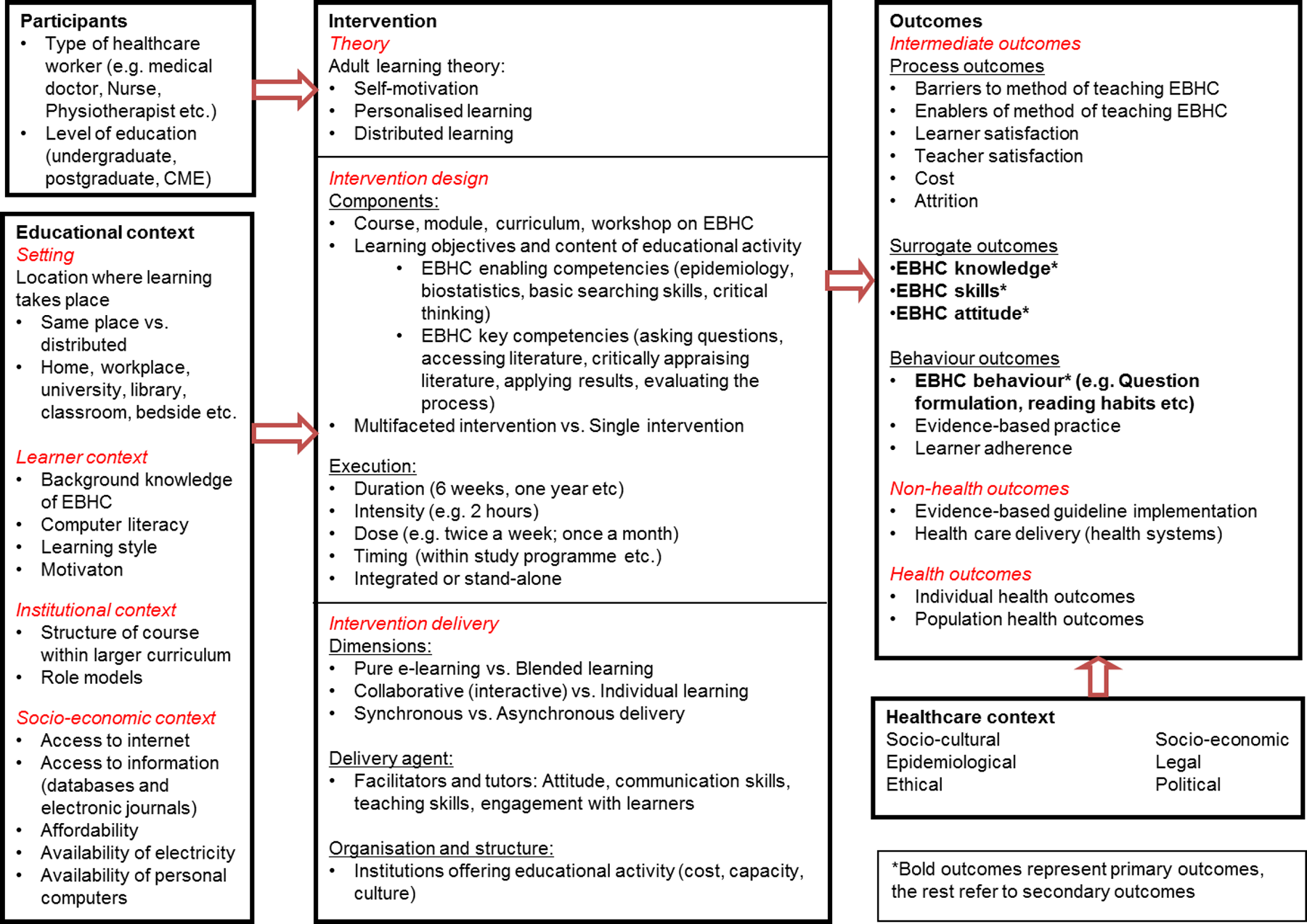
Systems-based logic model of e-learning of EBHC
1.3 HOW THE INTERVENTION MIGHT WORK
1.3.1 How e-learning may work
A number of systematic reviews have been conducted in various fields of medical and health science education, examining the effect of different types of e-learning on knowledge, skills and behaviour.
A systematic review conducted by the WHO evaluated the effectiveness of e-learning for undergraduate health professions education (Al-Shorbaji, Atun, Car, Majeed, & Wheeler, 2015). They included 209 studies and concluded that e-learning is similar to traditional face-to-face learning in terms of knowledge and skill acquisition. The majority of included studies were judged to be at high risk of bias.
Cook et al. (2008) conducted a systematic review to determine the effectiveness of internet-based learning for health professionals compared to no intervention or non-internet interventions. The authors pooled data in a random-effects meta-analysis and found significant results favoring internet-based learning for knowledge, skills, as well as behaviour and patient effects when compared to no learning. But when internet-based learning was compared to alternative methods of learning, there was no difference in results between groups. In a subsequent analysis on instructional design variations in internet-based learning, the authors concluded that interactivity, practice exercises, repetition and feedback appeared to be associated with improved learning outcomes (Cook et al., 2010). A review by Booth and colleagues (2009) found that presentation and design, flexibility, peer communication, support and knowledge validation were effective e-learning techniques for enhancing the learning experience of students.
Liu et al. (2016) conducted a systematic review on the effectiveness of blended learning compared to no or other learning amongst health professionals. They included 56 studies and results favored blended learning when compared to no learning and to other learning. However, authors caution that high levels of heterogeneity should be taken into account when interpreting results.
Another recent systematic review assessed the effectiveness of internet-based e-learning on health care professional behaviour and patient outcomes (Sinclair, Kable, Levett-Jones, & Booth, 2016). The authors found 7 studies that assessed behaviour of healthcare professionals and no studies that reported on patient outcomes. They were unable to pool results in meta-analysis due to substantial heterogeneity between studies. Although results from individual studies showed that e-learning was just as effective as face-to-face learning and better than no learning, authors concluded that there was currently insufficient evidence to answer their question.
Other studies have examined how e-learning works, focusing more on the essential components for successful learning, as well as certain contextual factors that influence learning. A realist review by Wong et al. (2010), looking at “what works, for whom and in what circumstances” when considering internet-based medical education, concluded that online courses need to engage the learners to use the technology, which is more likely to happen when the technology is perceived as being useful and easy to use; and that interactivity should be a key characteristic of an online course, since learners want to be able to enter a dialogue with tutors and peers (Wong et al., 2010).
E-learning technologies afford a new learner paradigm based on the adult learning theory, explaining that adults learn by relating new information to past experiences; tailoring learning to their unique needs (open learning); and applying learning in practice, resulting in more effective and efficient learning experiences. The attributes of accessibility and convenience (distributed learning) personalise the learning, because students decide when and where they are receptive to learning. Learning becomes an individual experience where adults learn because they want to learn – not because they are told to learn. This shift from “expert-led teaching to user-lead learning” results from intrinsic motivation and offers a much stronger learning stimulus. Some evidence suggests that learning by means of e-learning is more efficient and that learners gain knowledge faster, which in turn translates back to improved motivation and enhanced learning. (Clark, 2002; Dabbagh, 2005; Ruggeri et al., 2013; Ruiz, 2006).
When considering these attributes and pedagogical underpinnings of e-learning, one can argue that these fit perfectly within the EBHC paradigm. Enhanced learning occurs through internal motivation, rather than external drivers and requires acknowledgement of shortcomings (knowledge gaps) and adoption of a reflective approach towards one's own practice. This alignment between attributes of e-learning and EBHC foci suggests that making use of e-learning in this context could be of value.
The pathway from EBHC e-learning activities to the desired outcomes, i.e. increased knowledge, skill, attitude and behaviour, as well as health outcomes is depicted in Figure 3, a process-oriented logic model, based on the template by Rohwer et al. (2016).
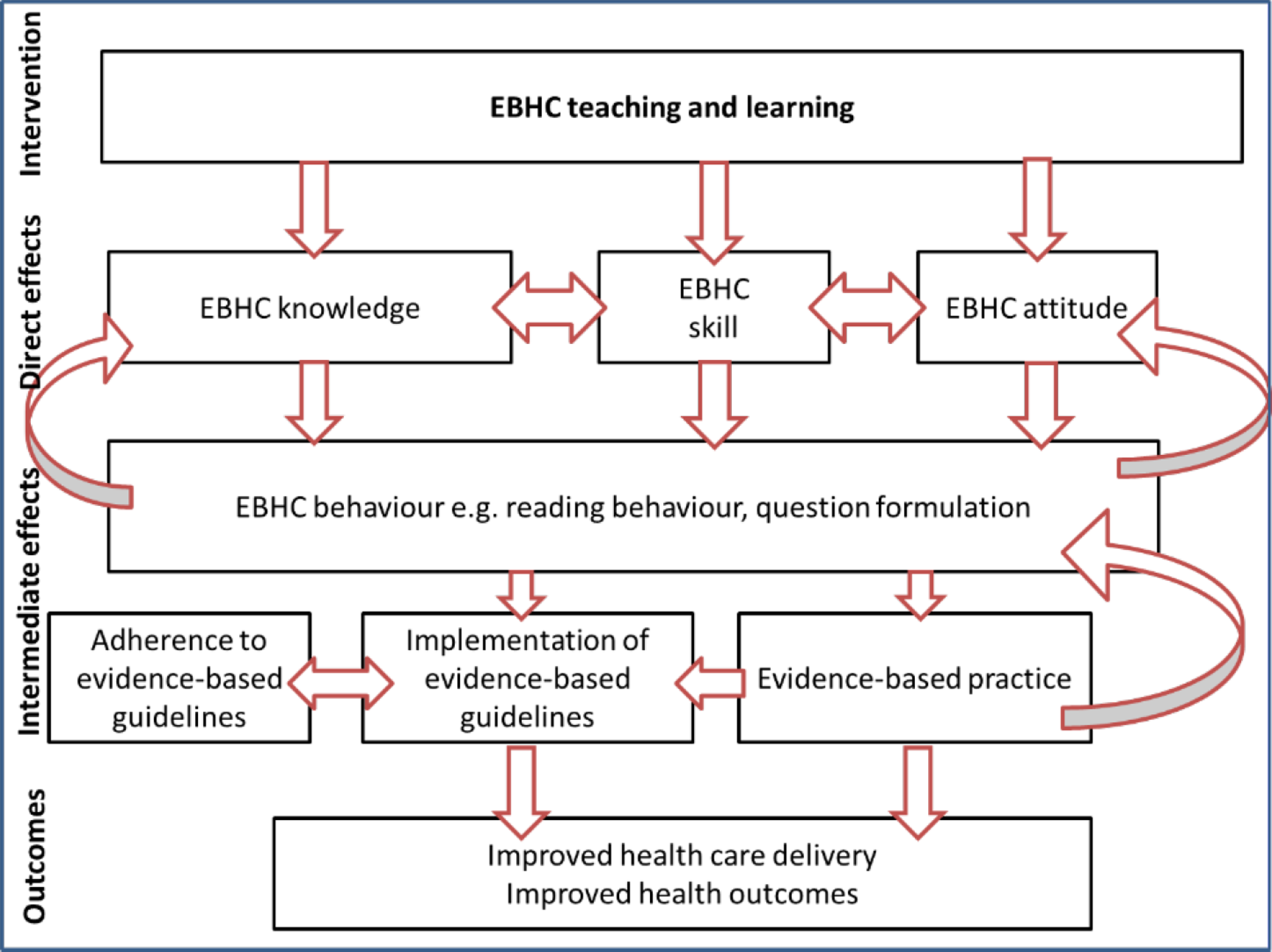
Process-oriented logic model showing the pathway from EBHC learning to desired outcomes
It is important to note that this pathway does not take place in a vacuum, but that ultimately, improved health care delivery and improved health outcomes do not only rely on evidence-based practice, but are influenced by a variety of other factors within the healthcare context e.g. socio-cultural, socio-economic, epidemiological, legal, ethical and political factors on a national and international level (See Figure 2).
1.4 WHY IT IS IMPORTANT TO DO THE REVIEW
A number of systematic reviews assessing the effectiveness of e-learning for healthcare professionals at various levels have been published in recent years. As described above, these reviews assessed e-learning of any content related to health professions education (Al-Shorbaji et al., 2015; Cook et al., 2008; Liu et al., 2016; Sinclair et al., 2016). Generally, systematic reviews concluded that e-learning was better than no learning, but neither superior nor inferior to other methods of learning. Although these reviews do not represent a comprehensive list of all published reviews in this area, they are an indication of the current interest in this field.
When examining the literature on EBHC learning, we also found a number of recently published studies. A recent overview of systematic reviews (Young et al., 2014) that included 16 systematic reviews examining the effects of educational activities on EBHC, found that when comparing single interventions (a workshop, journal club, lecture or e-learning) with multifaceted interventions (a combination of different strategies e.g. lectures, tutorials, e-learning, journal clubs, etc.) multifaceted clinically integrated educational activities were more likely to increase EBHC knowledge, skills, attitude and behaviour. Although some of the studies included in the systematic reviews related to e-learning activities, it is still unclear whether e-learning of EBHC leads to increased knowledge, skills, attitude and behaviour. The need to synthesise studies specifically evaluating the effect of EBHC e-learning was therefore identified.
Another recent systematic review (Ilic & Maloney, 2014) that aimed to determine what type of educational methods was most effective in increasing EBHC knowledge and skills found that there was no difference between the various educational methods for EBHC. It is therefore still unknown whether some e-learning strategies are more useful and effective than others.
This review considers e-learning of EBHC to be a complex intervention and aims to address the effectiveness of the interventions, as well as identify the implementation and contextual factors that are important in delivering the intervention. In teasing out these issues, we hope to be able to formulate evidence-based recommendations for EBHC teachers and program developers.
2 Objectives
Primary objective: To assess the effectiveness of e-learning of EBHC on increasing EBHC competencies in healthcare professionals
EBHC competencies include (Figure 1) Enabling competencies: biostatistics, epidemiology, basic searching skills, philosophy of critical enquiry Key competencies: asking clear questions, accessing the literature to find the best available evidence, critically appraising the evidence for validity and interpreting results, applying the results, and auditing the process
Secondary objectives: To assess the effectiveness of specific dimensions of e-learning in increasing EBHC competencies To assess how educational context influences the effectiveness of EBHC e-learning To assess how implementation approaches influence the effectiveness of EBHC e-learning
3 Methods
The protocol for this systematic review has been published in the Campbell Library (Rohwer, Rehfuess, & Young, 2014).
3.1 CRITERIA FOR CONSIDERING STUDIES FOR THIS REVIEW
3.1.1 Types of studies
We followed the guidance of the Effective Practice and Organisation of Care (EPOC) review group of Cochrane. We included randomised controlled trials (RCTs), cluster randomised controlled trials and non-randomised controlled trials (non-RCTs) in the review. In addition, we considered controlled before-after studies (CBAs) with at least two intervention and two control sites; and interrupted time series (ITS) with a clearly defined point in time when the intervention occurred with at least three data points before and three data points after the intervention.
In addition, we included studies supporting the included intervention studies that yielded information on the process of implementation. These studies were either quantitative (e.g. process evaluations, quantitative interview studies) or qualitative in nature (e.g. focus groups, qualitative interview studies). The information gathered was either reported within the above included intervention studies, or cited within these and published separately. We did not include these supporting studies in the data synthesis, but rather reported relevant results separately.
We excluded studies without a comparison group.
3.1.2 Types of participants
We included all healthcare professionals, including doctors, dentists, nurses, occupational therapists, physiotherapists, dieticians, audiologists, mental health professionals, psychologists, counsellors, social workers at undergraduate, postgraduate (e.g. residents) or continuing medical education (CME) level; working in primary, secondary or tertiary environments.
3.1.3 Types of interventions
3.1.3.1 Interventions
We included any educational intervention (a co-ordinated educational activity) that included any or all of the 5 steps of EBHC (asking questions, searching the literature, critically appraising the literature, applying the results, evaluating the process) and was delivered via an electronic platform (e-learning only), or made use of e-learning in a supplementary way (blended learning). E-learning (web-based learning, online learning, distributed learning, computer-assisted instruction) was regarded as: delivery of training material via any electronic media (internet, CD-ROM, DVD, smartphones and other media), independent of the delivery platform.
3.1.3.2 Comparisons
Comparisons included no educational intervention (no EBHC learning); any educational intervention that included any or all of the 5 steps of EBHC (asking questions, searching the literature, critically appraising the literature, applying the results, evaluating the process) that was delivered via an electronic platform, but with different components than the intervention (e.g. interactivity vs no interactivity; synchronicity vs asynchronicity); and any educational intervention that included any or all of the 5 steps of EBHC (asking questions, searching the literature, critically appraising the literature, applying the results, evaluating the process) and was delivered via face-to-face learning, with no e-learning components.
3.1.4 Types of outcome measures
Primary outcomes
EBHC knowledge (as measured by study authors, for example, evaluating knowledge scores with a validated pre-and post-training questionnaire such as Fresno test (Ramos, Schafer, & Tracz, 2003) or Berlin test (Fritsche, Greenhalgh, Falck-Ytter, Neumayer, & Kunz, 2002)) EBHC knowledge and skills measured as a composite outcome as measured by study authors EBHC skills (as measured by study authors, for example, evaluating skill scores with a validated pre-and post-training questionnaire such as Fresno test (Ramos et al., 2003) or Berlin test (Fritsche et al., 2002)) EBHC attitude (as measured by study authors, for example, with Likert-scale questions pre- and post-training) EBHC behaviour (as measured by study authors, for example, self-reported behaviour changes, amount of questions formulated, amount of searches done; or more objective measurements, for example, proportion of clinical cases where evidence was consulted)
Secondary outcomes
Process outcomes Satisfaction of students with method of learning (as measured by study authors, for example, Likert-scale questions post-training, or open-ended questions yielding qualitative data) Satisfaction of educators with method of learning (as measured by study authors, for example, with Likert-scale questions post-training, or open-ended questions yielding qualitative data) Enablers of the method of learning EBHC (as measured by study authors, for example, with Likert-scale questions post-training, or open-ended questions yielding qualitative data) Barriers to the method of learning EBHC (as measured by study authors, for example, with Likert-scale questions post-training, or open-ended questions yielding qualitative data) Cost (a sum of all the monetary cost involved in the training) Attrition of learners (measured quantitatively by looking at the proportion of learners that complete the training) Behaviour outcomes Learner adherence (measured either quantitatively by looking at the proportion of learners that adhere to the prescribed learning, or qualitatively by asking learners whether about their learning experience) Evidence-based practice (measured qualitatively through self-report of practitioners) Non-health outcomes Evidence-based guideline implementation (for example, measured quantitatively by looking at practice audits) Health care delivery (measured qualitatively through self-report of practitioners) Health outcomes Individual health outcomes (these refer to clinical patient-orientated outcomes, measured quantitatively) Population health outcomes (these refer to health outcomes of the community or the entire population measured quantitatively, for example, disease incidence rates)
3.2 SEARCH METHODS FOR IDENTIFICATION OF STUDIES
3.2.1 Electronic searches
We developed a comprehensive search strategy consisting of relevant terms (Table 9.1) and searched electronic databases (MEDLINE via PubMed, EMBASE via Ovid, ERIC, CINAHL, CENTRAL, SCOPUS, Best Evidence Medical Education (BEME), Web of Knowledge, PsycInfo) and dissertation databases (ProQuest) up to 24 May 2016 for relevant studies. We did not apply any language restrictions.
3.2.2 Searching other resources
We complemented our search with a thorough examination of reference lists of identified studies and contacted experts in the field to identify any on-going or unpublished studies. We also searched trial registries (ICTRP) for on-going studies (24 May 2016).
3.3 DATA COLLECTION AND ANALYSIS
3.3.1 Selection of studies
Two authors (AR and either TY, ER or NVM) independently screened the search outputs and abstracts for relevant studies. We retrieved full texts of studies with seemingly relevant abstracts and two authors (AR and TY, ER or NVM) independently assessed them for eligibility using the pre-specified inclusion criteria. We resolved discrepancies through discussions and consultations with a third author before classifying studies as included, excluded, or on-going.
3.3.2 Data extraction and management
Two authors (AR and either NVM, TY or ER) extracted data from relevant studies independently and in duplicate using piloted, electronic data extraction forms. Discrepancies were resolved through discussions and consultations with a third author. We contacted authors in case of missing data.
We extracted data related to study design (type of study, duration of study, country), participants (number of participants, type of health care professionals, level of education), interventions (learning theory, educational content, duration, intensity, dose and timing of intervention, delivery of interventions), outcomes (primary and secondary outcomes, measurement details and time point at which outcomes were measured), results (measures of effect with 95% confidence intervals, qualitative data) and educational context (setting, learner context, institutional context and socio-economic context). We considered the term “learning theory” in a broad way, to describe a body of implicit or explicit ideas about how learning works (May et al., 2007; Wells, Williams, Treweek, Coyle, & Taylor, 2012). We extracted theories, models or learning approaches, as defined by study authors.
We broadly categorised interventions and controls into pure e-learning, blended learning, face-to-face learning or no learning. In addition, we indicated whether interventions were single or multi-faceted interventions, whether EBHC learning was stand-alone or integrated, and for all e-learning interventions, whether they required individual or collaborative learning.
In addition, we compiled a matrix of the intervention components related to the included interventions and comparisons in order to compare the components across studies. The matrix was informed by components identified from the included studies and grouped according to mode of delivery, for example, e-learning components and face-to-face components.
3.3.3 Assessment of risk of bias in included studies
For each included study, two authors (AR and either NVM, TY, or ER) independently assessed the risk of bias according to the Cochrane Effective Practice and Organisation of Care's (EPOC) suggested risk of bias criteria (EPOC, 2015) for the following domains: selection bias, performance bias, detection bias, attrition bias, contamination (when participants in the comparison group are exposed to the intervention and vice versa), reporting bias, other bias (Table 9.2).
In addition, we assessed the possibility of additional biases for cluster RCTs according to the Cochrane handbook (Higgins & Green, 2008). Recruitment bias: We described whether participants were recruited before or after randomization of clusters. We regarded studies as having low risk of recruitment bias if participants were recruited before randomization of clusters; high risk of bias if they were recruited after randomization; and unclear risk of bias if information about the timing of recruitment is unclear. Baseline imbalance: We described any baseline imbalances between individuals and clusters Loss of clusters: We described the number of clusters lost as well as reasons for attrition Incorrect analysis: We described whether analysis was adjusted for clustering Compatibility with RCTs randomised by individuals: We described whether the intervention effects may be systematically different from individually randomised controlled trials i.e. whether it was likely that the effect size was over- or underestimated.
We resolved discrepancies through discussion and consultation with a third author if needed.
3.3.4 Measures of treatment effect
3.3.4.1 Dichotomous data
We presentedrates of attrition of learners as risk ratios (RR) with their respective 95% confidence intervals (CI).
3.3.4.2 Continuous data
Continuous outcomes included EBHC knowledge and skill scores; EBHC attitude scores and EBHC behaviour. We presented continuous data as the standardised mean difference (SMD) with 95% confidence intervals, to take into account differences related to various measurement tools. We interpreted the size of the effect as follows, based on Sawilowsky (2009): SMD 0.01-0.19: very small effect SMD 0.2-0.49: small effect SMD 0.5-0.79: medium effect SMD 0.8-1.19: large effect SMD 1.2-1.99: very large effect SMD 2.0 and above: huge effect
3.3.4.3 Other data
Outcomes not measured numerically were reported narratively. These outcomes included EBHC behaviour, satisfaction with the method of learning, and barriers and enablers to the method of learning EBHC.
3.3.5 Unit of analysis issues
In cluster RCTs, where authors had appropriately adjusted results for clustering, we included the adjusted effect estimates and standard errors using the generic inverse-variance method in RevMan. For outcomes where authors had not appropriately adjusted for clustering, we adjusted the data by calculating the ‘effective sample size’ of each intervention group in the cluster RCT. This was done by dividing the original sample size of an intervention group by the design effect (Higgins & Green, 2008). We then included the adjusted data in the meta-analysis.
For multi-arm studies, which contributed multiple comparisons to a particular meta-analysis, we split the ‘shared’ group (e.g. two intervention groups and one control group) as appropriate to avoid the inclusion of data from the same patient more than once in the same analysis.
3.3.6 Dealing with missing data
We contacted authors in case of missing data. Where authors did not respond, we calculated the means and standard deviations (SD) according to the methods described in the Cochrane Handbook (Higgins & Green, 2008). The mean difference (MD) and SD were then converted to a SMD, standard error (SE) and corresponding 95% confidence intervals (CIs) with RevMan software (RevMan, 2011).
For continuous outcomes, we only included participants for whom outcomes were measured, i.e., per-protocol analysis. For rates of attrition of learners, we used intention to treat analysis, i.e., we included all participants that were randomised to a specific group as the denominator in the analysis.
3.3.7 Assessment of heterogeneity
We assessed heterogeneity by describing variability among studies regarding participants, interventions and outcomes (educational heterogeneity), as well as variability in study design and risk of bias (methodological heterogeneity).
Educational heterogeneity was explored by clearly documenting the characteristics of participants; all components of the intervention relating to intervention design and delivery; as well as outcomes and measurement of outcomes in table format. In addition, the educational context (setting, learner context, institutional context, socio-economic context), in which the intervention was delivered, was explored and reported. See Figure 2.
Methodological heterogeneity was explored by clearly documenting study design as well as risk of bias for each study.
We assessed statistical heterogeneity by looking at the I2 statistic as well as the Chi2 test statistic. We considered an I2 value of more than 30%, and a p-value of less than 0.10 for the Chi2 test for heterogeneity to be an indicator of important heterogeneity. In case of considerable heterogeneity, we performed random-effects meta-analysis instead of fixed-effect meta-analysis or reported outcomes in tabular or narrative format.
3.3.8 Assessment of reporting biases
We did not assess reporting biases with funnel plots, since we had less than 10 included studies per outcome.
3.3.9 Data synthesis
Due to important heterogeneity related to the participants, interventions and outcome measurements, we used random-effects meta-analysis to pool results using RevMan. For continuous outcomes, we converted means and standard deviations reported at follow-up to SMD and SEs, and reported the pooled SMD with 95%CIs. For studies where outcomes were reported as mean change scores, we calculated follow-up means from baseline means and used baseline SDs for follow-up SDs before converting to SMDs (Higgins & Green, 2008). For dichotomous outcomes, we reported the pooled risk ratio (RR) with 95% CIs. Studies were grouped under six main comparisons: Pure e-learning vs no learning Blended learning vs no learning Pure e-learning vs face-to-face learning Blended learning vs face-to-face learning Blended learning vs pure e-learning Pure e-learning vs pure e-learning
3.3.10 Subgroup analysis and investigation of heterogeneity
We performed the following subgroup analysis on primary outcomes: Study design: Non-RCTs vs RCTs
3.3.11 Sensitivity analysis
We did not perform sensitivity analysis on primary outcomes, as the number of included studies per outcome was very small.
4 Results
4.1 DESCRIPTION OF STUDIES
4.1.1 Results of the search
Our search of the databases yielded 12980 citations (24 May 2016) and we identified three further citations from screening references of included studies and experts. After removal of duplicates, we screened 6175 titles and abstracts, of which we identified 55 as being potentially eligible. We assessed eligibility of these by obtaining and screening the full texts of the studies. We included 24 studies (Table 9.3), classified one study as ongoing (Table 9.4) and excluded 30 studies (Table 9.5) (Figure 4).
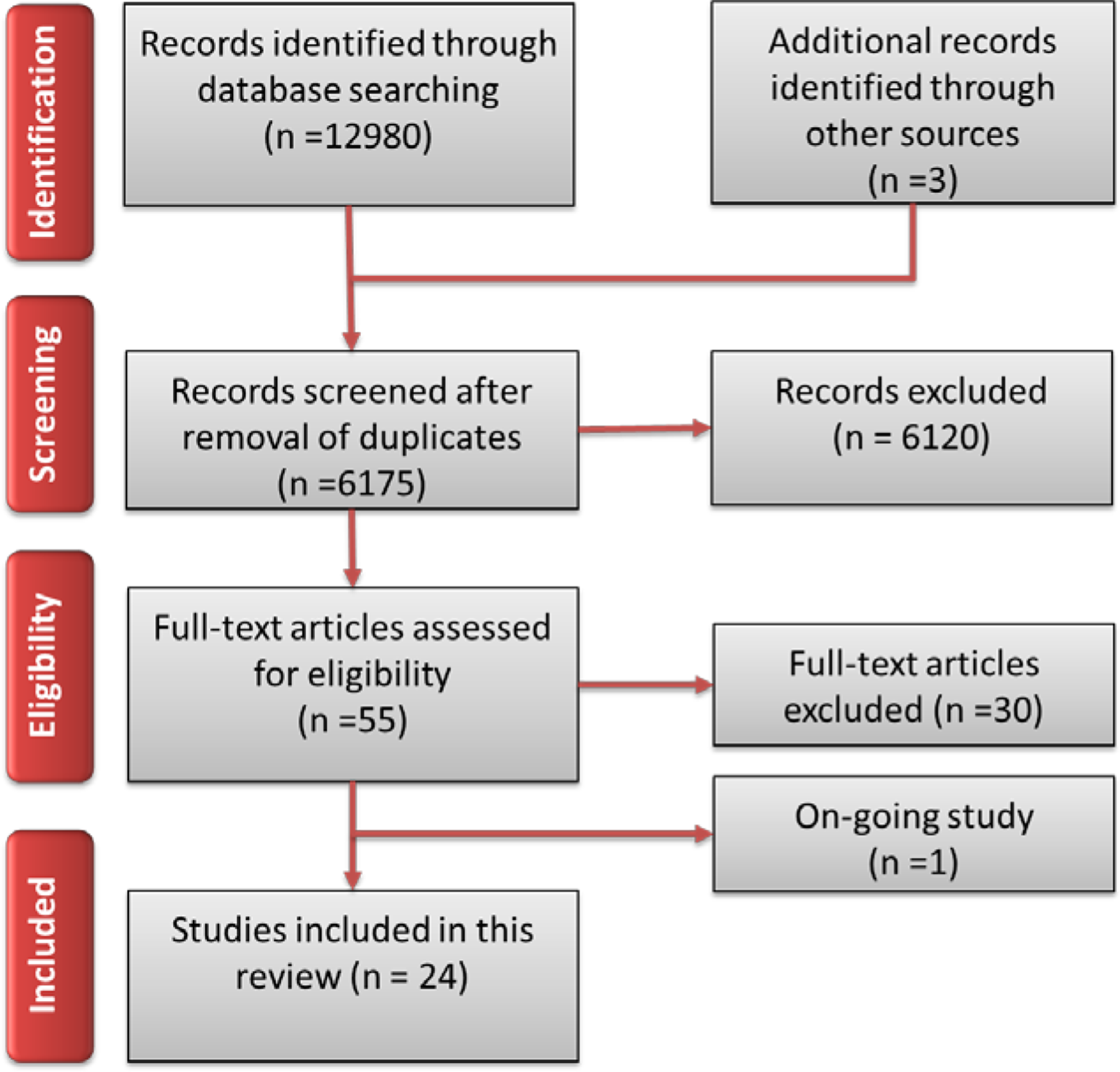
Flow diagram of included studies
4.1.2 Included studies
We included 24 studies with a total of 3825 participants in the review. Details of individual studies can be found in the table of characteristics of included studies (Table 9.3). Table 9.6 summarises the characteristics of included studies.
4.1.2.1 Study designs
Thirteen included studies were individually randomised controlled trials (Bergold et al., 2013; Bradley et al., 2005; Brettle & Raynor, 2013; Brouwers et al., 2011; Davis et al., 2007; Davis et al., 2008; Dizon et al., 2014; Forsetlund et al., 2003; Horiuchi et al., 2009; Kamin et al., 2001; Macrae et al., 2004; Saunders et al., 2016; Welch, Van Lunen, & Hankemeier, 2014), seven studies were cluster RCTs (Hadley et al., 2010; Ilic et al., 2015; Kok et al., 2013; Kulier et al., 2009; Kulier et al., 2012; Laibhen-Parkes, 2014; McLeod et al., 2010) and four were quasi-randomised trials (Fernandez et al., 2014; Ilic et al., 2013; Ramos-Morcillo et al., 2015; Schilling et al., 2006). We did not identify any eligible CBAs or ITS.
4.1.2.2 Participants
Participants of 14 included trials were medical doctors (Bergold et al., 2013; Bradley et al., 2005; Davis et al., 2007; Davis et al., 2008; Forsetlund et al., 2003; Hadley et al., 2010; Ilic et al., 2013; Ilic et al., 2015; Kok et al., 2013; Kulier et al., 2009; Kulier et al., 2012; Macrae et al., 2004; McLeod et al., 2010; Schilling et al., 2006). Of these, five trials included undergraduate students (Bradley et al., 2005; Davis et al., 2008; Ilic et al., 2013; Ilic et al., 2015; Schilling et al., 2006), six trials included qualified clinicians (Bergold et al., 2013; Davis et al., 2007; Forsetlund et al., 2003; Hadley et al., 2010; Kok et al., 2013; Macrae et al., 2004), and three trials included residents; that is, postgraduate students with a basic medical degree who are specialising (Kulier et al., 2009; Kulier et al., 2012; McLeod et al., 2010). Sixtrials included nurses (Brettle & Raynor, 2013; Fernandez et al., 2014; Horiuchi et al., 2009; Laibhen-Parkes, 2014; Ramos-Morcillo et al., 2015; Saunders et al., 2016), of which one study included undergraduate (Brettle & Raynor, 2013) and one postgraduate (Fernandez et al., 2014) students; and four trials included practicing nurses. The remaining four trials included practicing physiotherapists (Dizon et al., 2014), undergraduate physician assistants (Kamin et al., 2001), athletic trainers (Welch, Van Lunen, & Hankemeier, 2014) and a combination of healthcare professionals, clinicians, methodologists, policy makers and trainees (Brouwers et al., 2011).
4.1.2.3 Location of studies
Most studies were conducted in high-income countries, four in the UK (Brettle & Raynor, 2013; Davis et al., 2007; Davis et al., 2008; Hadley et al., 2010), four in the USA (Kamin et al., 2001; Laibhen-Parkes, 2014; McLeod et al., 2010; Schilling et al., 2006) two in Norway (Bradley et al., 2005; Forsetlund et al., 2003), two in Canada (Brouwers et al., 2011; Macrae et al., 2004), one each in Germany (Bergold et al., 2013), The Netherlands (Kok et al., 2013), Spain (Ramos-Morcillo et al., 2015), Finland (Saunders et al., 2016), Australia (Ilic et al., 2013) and Japan (Horiuchi et al., 2009). Three studies were conducted in more than one high-income country, one in the UK and The Netherlands (Kulier et al., 2009), one in Australia and Hong Kong (Fernandez et al., 2014), and one in Australia and Malaysia (Ilic et al., 2015). The remaining two studies were conducted in low-and middle-income countries, one in the Philippines (Dizon et al., 2014) and one had multiple study sites in Argentina, Brazil, Democratic Republic of Congo, India, Philippines, South Africa and Thailand (Kulier et al., 2012). One study did not report where participants were based, since they were members of the national athletics trainers’ association (NATA) which is a worldwide association (Welch, Van Lunen, & Hankemeier, 2014). Attempts to contact the authors for additional information were not successful.
4.1.2.4 Interventions
All but two studies had two study arms. One study had three arms (Brouwers et al., 2011) and one had four study arms (Fernandez et al., 2014). Interventions were heterogeneous and are described in detail in the table of characteristics of included studies (Table 9.3), with the intervention components summarised in Table 9.7.
Intervention components
Thirteen studies (Bradley et al., 2005; Brouwers et al., 2011; Davis et al., 2007; Davis et al., 2008; Fernandez et al., 2014; Hadley et al., 2010; Horiuchi et al., 2009; Kamin et al., 2001; Laibhen-Parkes, 2014; Macrae et al., 2004; McLeod et al., 2010; Schilling et al., 2006; Welch, Van Lunen, & Hankemeier, 2014) included interventions that were pure e-learning interventions, while eleven studies evaluated blended learning (Bergold et al., 2013; Brettle & Raynor, 2013; Dizon et al., 2014; Fernandez et al., 2014; Ilic et al., 2013; Ilic et al., 2015; Kok et al., 2013; Kulier et al., 2009; Kulier et al., 2012; Ramos-Morcillo et al., 2015; Saunders et al., 2016). Amongst the pure e-learning interventions, ten required individual learning only (Bradley et al., 2005; Brouwers et al., 2011; Davis et al., 2007; Davis et al., 2008; Fernandez et al., 2014; Hadley et al., 2010; Horiuchi et al., 2009; Laibhen-Parkes, 2014; Welch, Van Lunen, & Hankemeier, 2014) and four incorporated collaborative learning in the intervention (Kamin et al., 2001; Macrae et al., 2004; McLeod et al., 2010; Schilling et al., 2006). Amongst the blended learning interventions, six required individual learning (Bergold et al., 2013; Brettle & Raynor, 2013; Dizon et al., 2014; Kulier et al., 2009; Kulier et al., 2012; Saunders et al., 2016) and five included collaborative learning activities (Forsetlund et al., 2003; Ilic et al., 2013; Ilic et al., 2015; Kok et al., 2013; Ramos-Morcillo et al., 2015). Four of the pure e-learning interventions delivered the content via CD-ROM or DVD (Bradley et al., 2005; Davis et al., 2007; Davis et al., 2008; Fernandez et al., 2014), whereas all other interventions were delivered asynchronously via an online learning platform or email.
In eight studies the interventions were regarded as single-component interventions and delivered as stand-alone teaching (Bradley et al., 2005; Brettle & Raynor, 2013; Brouwers et al., 2011; Davis et al., 2007; Davis et al., 2008; Hadley et al., 2010; Horiuchi et al., 2009; Laibhen-Parkes, 2014; Welch, Van Lunen, & Hankemeier, 2014). The remaining interventions were multi-faceted, comprising more than one component. Of these, six were delivered as stand-alone teaching (Brouwers et al., 2011; Fernandez et al., 2014; Kamin et al., 2001; Macrae et al., 2004; McLeod et al., 2010; Ramos-Morcillo et al., 2015), while ten were integrated into clinical practice (Bergold et al., 2013; Dizon et al., 2014; Forsetlund et al., 2003; Ilic et al., 2013; Ilic et al., 2015; Kok et al., 2013; Kulier et al., 2009; Kulier et al., 2012; Saunders et al., 2016; Schilling et al., 2006).
Intervention components of included studies differed across studies (Table 9.7). The most common e-learning component was recorded PowerPoint presentations, which was included in twelve studies (Bergold et al., 2013; Bradley et al., 2005; Davis et al., 2007; Davis et al., 2008; Fernandez et al., 2014; Hadley et al., 2010; Horiuchi et al., 2009; Ilic et al., 2015; Kulier et al., 2009; Kulier et al., 2012; Laibhen-Parkes, 2014; Schilling et al., 2006), five of which had this as the only intervention component (Bradley et al., 2005; Davis et al., 2007; Davis et al., 2008; Hadley et al., 2010; Laibhen-Parkes, 2014). Eight studies included access to an online teaching site and learning materials (Brouwers et al., 2011; Dizon et al., 2014; Fernandez et al., 2014; Forsetlund et al., 2003; Ilic et al., 2013; Ilic et al., 2015; Kamin et al., 2001; Ramos-Morcillo et al., 2015), but they all had at least one other component. These other e-learning components included online tutorials (Brettle & Raynor, 2013; Brouwers et al., 2011; Fernandez et al., 2014; Saunders et al., 2016; Schilling et al., 2006), online exercises, assignments and clinical scenarios (Bergold et al., 2013; Horiuchi et al., 2009; Kamin et al., 2001; Kulier et al., 2009; McLeod et al., 2010; Ramos-Morcillo et al., 2015; Saunders et al., 2016), online support by a tutor and feedback (Brouwers et al., 2011; Dizon et al., 2014; Forsetlund et al., 2003; Ramos-Morcillo et al., 2015; Saunders et al., 2016), use of online tools such as checklists and calculators (Dizon et al., 2014; Schilling et al., 2006), asynchronous discussion lists (Forsetlund et al., 2003; Kamin et al., 2001; Macrae et al., 2004; McLeod et al., 2010; Ramos-Morcillo et al., 2015), and online journal clubs (Macrae et al., 2004; McLeod et al., 2010). Receiving an electronic newsletter (Forsetlund et al., 2003), access to databases (Forsetlund et al., 2003) and mobile learning at the bedside (Ilic et al., 2015) are intervention components that were each included in only one study. Two studies did not clearly describe the intervention components only referring to it as an “interactive online course” in Kok et al. (2013), and a “web-based module” in Welch, Van Lunen, and Hankemeier (2014).
Face-to-face intervention components that formed part of blended learning included classroom-based as well as clinical activities. The most commonly included classroom-based component was an interactive workshop, which was part of the intervention in five studies (Dizon et al., 2014; Forsetlund et al., 2003; Ilic et al., 2013; Ilic et al., 2015; Kok et al., 2013). Five studies included didactic lectures (Dizon et al., 2014; Forsetlund et al., 2003; Ilic et al., 2015; Ramos-Morcillo et al., 2015; Saunders et al., 2016), three included small group discussions (Ilic et al., 2013; Ilic et al., 2015; Kok et al., 2013) and two included hands-on computer-based training (Brettle & Raynor, 2013; Kok et al., 2013). Clinical activities and assignments formed part of the intervention in four studies (Bergold et al., 2013; Ilic et al., 2013; Kulier et al., 2009; Kulier et al., 2012), with three of these also including access to a tutor or facilitator in the clinical field (Bergold et al., 2013; Kulier et al., 2009; Kulier et al., 2012).
Content covered by interventions mostly related to EBHC key competencies (Table 9.8). Four studies focussed on asking questions and accessing the literature (Brettle & Raynor, 2013; Kamin et al., 2001; Ramos-Morcillo et al., 2015; Schilling et al., 2006), while the content of three others only related to critical appraisal (Brouwers et al., 2011; Macrae et al., 2004; McLeod et al., 2010). The learning content of one study related to the first three key competencies (asking questions, accessing the literature and critical appraisal) (Hadley et al., 2010), while the remaining studies included the four key competencies: asking questions, accessing the literature, critical appraisal and applying the results (Bergold et al., 2013; Bradley et al., 2005; Davis et al., 2007; Davis et al., 2008; Dizon et al., 2014; Fernandez et al., 2014; Forsetlund et al., 2003; Horiuchi et al., 2009; Ilic et al., 2013; Ilic et al., 2015; Kok et al., 2013; Kulier et al., 2009; Kulier et al., 2012; Laibhen-Parkes, 2014; Saunders et al., 2016 Welch, Van Lunen, & Hankemeier, 2014). Of these, five studies also included the fifth key competency, evaluating the process of EBHC (Bradley et al., 2005; Fernandez et al., 2014; Ilic et al., 2015; Saunders et al., 2016; Welch, Van Lunen, & Hankemeier, 2014), while another four (Dizon et al., 2014; Ilic et al., 2013; Ramos-Morcillo et al., 2015; Schilling et al., 2006) included certain enabling competencies (epidemiology, biostatistics and basic searching skills).
EBHC learning content of interventions
4.1.2.5 Duration of the interventions
Duration of interventions in included studies ranged from a single, one hour session in two studies (Davis et al., 2007; Davis et al., 2008) to a journal club addressing one article per month and running over eight months in two studies (Macrae et al., 2004; McLeod et al., 2010). In one study, the intervention period was two weeks, consisting of five half day sessions (Bradley et al., 2005), while in another, the intervention consisted of two one-hour sessions which were one month apart (Brettle & Raynor, 2013). In nine studies, interventions were delivered over a three to eight week period, with learners progressing according to their own needs (Bergold et al., 2013; Brouwers et al., 2011; Hadley et al., 2010; Horiuchi et al., 2009; Kulier et al., 2009; Kulier et al., 2012; Laibhen-Parkes, 2014; Ramos-Morcillo et al., 2015; Saunders et al., 2016; Schilling et al., 2006; Welch, Van Lunen, & Hankemeier, 2014). One study only specified that the intervention was delivered during the “fall quarter” and that participants accessed the learning material according to their own needs (Kamin et al., 2001). In one study with three intervention arms, the interventions were delivered over a period of 15 weeks, with 10 hours per week allocated to studying the content. In one of the intervention arms, participants received three additional workshops of two hours each (Fernandez et al., 2014). The interventions in two studies comprised ten two-hour sessions delivered over two periods of two months each (Ilic et al., 2013; Ilic et al., 2015), while the intervention of another consisted of five contact days spread over a period of six months (Kok et al., 2013). Two studies with blended learning interventions included an initial workshop followed by a period of online support, during which participants engaged with the content according to their own needs. In one of these, (Dizon et al., 2014) the one day workshop consisted of six lectures and four practical sessions, while the period of online support lasted three months. In the other, the duration of the workshops varied from one to five days, while the entire intervention period lasted 18 months (Forsetlund et al., 2003).
4.1.2.6 Learning theories
In ten studies, the intervention was explicitly based on a learning theory or on one or more learning approaches. Three studies referred to distributed learning (Bergold et al., 2013; Bradley et al., 2005; Horiuchi et al., 2009), another three based their intervention on the adult learning theory (Dizon et al., 2014; Macrae et al., 2004; Schilling et al., 2006), and two interventions made use of a learner centred approach (Bergold et al., 2013; Kulier et al., 2012). Other theories and learning approaches included the SPICES framework (Bergold et al., 2013), the constructivist model of learning (Fernandez et al., 2014), the innovation-diffusion process (Forsetlund et al., 2003), novice to expert theory and theory of planned behaviour (Laibhen-Parkes, 2014), just-in-time learning (Kulier et al., 2012), and the utility of reflective learning and collaborative learning (Schilling et al., 2006).
4.1.2.7 Comparisons
Comparisons included no EBHC learning, face-to-face learning of EBHC and e-learning of EBHC. Three studies compared pure e-learning to no learning (Laibhen-Parkes, 2014; Schilling et al., 2006; Welch, Van Lunen, & Hankemeier, 2014), while five studies compared blended learning to no learning (Bergold et al., 2013; Dizon et al., 2014; Forsetlund et al., 2003; Kok et al., 2013; Ramos-Morcillo et al., 2015). Seven studies compared pure e-learning to face-to-face learning (Bradley et al., 2005; Davis et al., 2007; Davis et al., 2008; Hadley et al., 2010; Horiuchi et al., 2009; Kamin et al., 2001; McLeod et al., 2010) and five studies compared blended learning to face-to-face learning (Brettle & Raynor, 2013; Ilic et al., 2013; Ilic et al., 2015; Kulier et al., 2009; Saunders et al., 2016). Three studies compared blended learning to pure e-learning (Fernandez et al., 2014; Kamin et al., 2001; Kulier et al., 2012) and two studies compared pure e-learning to other purely e-learning interventions (Brouwers et al., 2011; Macrae et al., 2004).
Amongst the sixteen trials that compared e-learning interventions to either face-to-face, blended or other e-learning interventions, there were nine single-component (Bradley et al., 2005; Brettle & Raynor, 2013; Brouwers et al., 2011; Davis et al., 2007; Davis et al., 2008; Fernandez et al., 2014; Hadley et al., 2010; Macrae et al., 2004; Saunders et al., 2016) and nine multi-faceted (Fernandez et al., 2014; Horiuchi et al., 2009; Ilic et al., 2013; Ilic et al., 2015; Kamin et al., 2001; Kulier et al., 2009; Kulier et al., 2012; McLeod et al., 2010) comparisons. Comparisons of all included studies were delivered via stand-alone teaching as opposed to integrated teaching. Four of the control interventions involved collaborative learning (Horiuchi et al., 2009; Ilic et al., 2013; Ilic et al., 2015; Kamin et al., 2001), while the rest relied on individual learning.
Amongst the face-to-face and blended learning interventions, didactic lectures were the most common intervention component (Brettle & Raynor, 2013; Davis et al., 2007; Davis et al., 2008; Fernandez et al., 2014; Hadley et al., 2010; Horiuchi et al., 2009; Ilic et al., 2013; Ilic et al., 2015; Kulier et al., 2009; Saunders et al., 2016). For four of these (Davis et al., 2007; Davis et al., 2008; Hadley et al., 2010; Saunders et al., 2016), it was the only intervention component. Other face-to-face components were small group discussions (Horiuchi et al., 2009; Ilic et al., 2013; Ilic et al., 2015; Kamin et al., 2001), an interactive workshop (Bradley et al., 2005; Ilic et al., 2015; Kulier et al., 2009), hands-on computer training (Brettle & Raynor, 2013; Fernandez et al., 2014) and a journal club (McLeod et al., 2010). The most common e-learning component of blended comparisons was access to the online teaching site and materials (Fernandez et al., 2014; Kamin et al., 2001). Other components included receiving teaching material via email (Brouwers et al., 2011; McLeod et al., 2010), access to databases and journals (Forsetlund et al., 2003; Macrae et al., 2004) access to a tutor on demand (Kulier et al., 2012) and recorded PowerPoint presentations (Kulier et al., 2012).
The content and duration of the control interventions was the same in both intervention and comparison groups.
4.1.2.8 Outcomes
Primary outcomes
Twelve trials reported on EBHC knowledge (Bergold et al., 2013; Bradley et al., 2005; Davis et al., 2007; Davis et al., 2008; Fernandez et al., 2014; Forsetlund et al., 2003; Hadley et al., 2010; Horiuchi et al., 2009; Kamin et al., 2001; Kulier et al., 2009; Kulier et al., 2012; Welch, Van Lunen, & Hankemeier, 2014). Six trials reported on EBHC knowledge and skills as a combined outcome (Dizon et al., 2014; Ilic et al., 2013; Ilic et al., 2015;Kok et al., 2013; Laibhen-Parkes, 2014; Ramos-Morcillo et al., 2015). Across studies, knowledge was measured with various validated tools or adaptations of these. The most commonly used tools were the Berlin questionnaire and the Fresno test. Four studies used a questionnaire based on both the Fresno test and the Berlin questionnaire (Davis et al., 2007; Davis et al., 2008; Kulier et al., 2009; Kulier et al., 2012), four studies used an adapted version of the Fresno test (Bergold et al., 2013; Dizon et al., 2014; Kok et al., 2013; Laibhen-Parkes, 2014), and two studies made use of the Berlin questionnaire or adaptations there of (Ilic et al., 2013; Ilic et al., 2015). Both these studies made use of additional assessments to measure EBHC knowledge, (Ilic et al., 2013) made use of two assignment tasks, while (Ilic et al., 2015) used the validated ACE tool. Two studies (Bradley et al., 2005; Hadley et al., 2010) made use of a questionnaire validated by Taylor et al. (Taylor et al., 2001). Ramos-Morcillo et al. (2015) used a Spanish version of the Evidence-based Practice Questionnaire (EBPQ) and Saunders et al., (2016) measured EBHC knowledge as part of the Evidence-based Readiness Inventory (ERI). Two studies measured knowledge with questionnaires developed by the study authors or working group (Kamin et al., 2001; Welch, Van Lunen, & Hankemeier, 2014), another (Forsetlund et al., 2003) measured self-reported knowledge on a Likert scale. In a further study knowledge scores were based on assignment marks (Fernandez et al., 2014).
Eight studies reported on EBHC skills (Bradley et al., 2005; Brettle & Raynor, 2013; Brouwers et al., 2011; Fernandez et al., 2014; Kulier et al., 2012; Macrae et al., 2004; McLeod et al., 2010; Schilling et al., 2006). In four studies participants had to critically appraise an article and were given scores for their appraisals (Bradley et al., 2005; Brouwers et al., 2011; Macrae et al., 2004; McLeod et al., 2010). Two studies scored the searches of participants (Brettle & Raynor, 2013; Schilling et al., 2006) and one study used an objective, structured clinical examination to measure EBHC skills (Kulier et al., 2012).
Thirteen studies reported attitude towards EBHC (Bradley et al., 2005; Brouwers et al., 2011; Davis et al., 2007; Davis et al., 2008; Dizon et al., 2014; Forsetlund et al., 2003; Ilic et al., 2013; Ilic et al., 2015; Kulier et al., 2009; Kulier et al., 2012; Laibhen-Parkes, 2014; Ramos-Morcillo et al., 2015; Schilling et al., 2006). All the studies made use of Likert scale questionnaires.
Five trials evaluated EBHC behaviour (Dizon et al., 2014; Forsetlund et al., 2003; Ilic et al., 2015; Kok et al., 2013; Ramos-Morcillo et al., 2015), of which two (Ilic et al., 2015; Ramos-Morcillo et al., 2015) measured behaviour with the Evidence-based Practice Questionnaire (EBPQ), requiring participants to rate their EBHC behaviour using a 7-point Likert scale.
Dizon et al. (2014) made use of activity diaries. EBHC behaviour of physiotherapists measured through activity diaries was categorized into evidence-based practice (EBP) behaviours (formulating PICO questions, logging PICO questions, searching research for evidence, appraising evidence and applying evidence) and non-EBP behaviours (asking colleagues, asking medical doctors and reading textbooks). This was reported for new or unique cases as well as for usual cases.
One study (Forsetlund et al., 2003) analysed the content of the local health service reports and asked participants to complete a hypothetical assignment and a questionnaire on self-reported behaviour. Scores (1-5) for the assignments were based on the extent to which the document reflected EBHC elements.
Kok et al. (2013) assessed the frequency of evidence of sufficient quality in disability evaluation reports through six indicators – presence of evidence; a discernible EBM question; search strategy; EBM source; and evaluation of quality.
Eight studies measured outcomes after the intervention only (Bradley et al., 2005; Brouwers et al., 2011; Fernandez et al., 2014; Ilic et al., 2013; Ilic et al., 2015; Laibhen-Parkes, 2014; Macrae et al., 2004; McLeod et al., 2010), while all other studies measured outcomes both before and after the intervention.
Secondary outcomes
Satisfaction with learning was reported in four studies (Bergold et al., 2013; Brouwers et al., 2011; Horiuchi et al., 2009; Ilic et al., 2015) and enablers and barriers of EBHC learning in one study (Ilic et al., 2015). Attrition of learners was reported in 17 trials (Bergold et al., 2013; Bradley et al., 2005; Brettle & Raynor, 2013; Brouwers et al., 2011; Davis et al., 2008; Dizon et al., 2014; Hadley et al., 2010; Horiuchi et al., 2009; Ilic et al., 2013; Ilic et al., 2015; Kok et al., 2013; Kulier et al., 2009; Kulier et al., 2012; Laibhen-Parkes, 2014; Macrae et al., 2004; McLeod et al., 2010; Saunders et al., 2016).
4.1.2.9 Educational context
Educational context in terms of learner context, institutional context and socio-economic context was not explicitly addressed, although for some studies, having access to a computer and internet was a pre-requisite to participating in the study.
4.1.3 Ongoing studies
We identified one study (Schneider et al., 2014) that is still on-going (Table 9.4).
4.1.4 Excluded studies
From those studies subjected to full-text screening we excluded 30 studies. Reasons for exclusion are listed in the table of excluded studies (Table 9.5).
4.2 RISK OF BIAS IN INCLUDED STUDIES
Overall, we judged risk of bias to be moderate. Details of our judgement of risk of bias are presented as part of the characteristics of included studies (Table 9.3). The risk of bias across studies is summarised in Figure 5 and Figure 6.
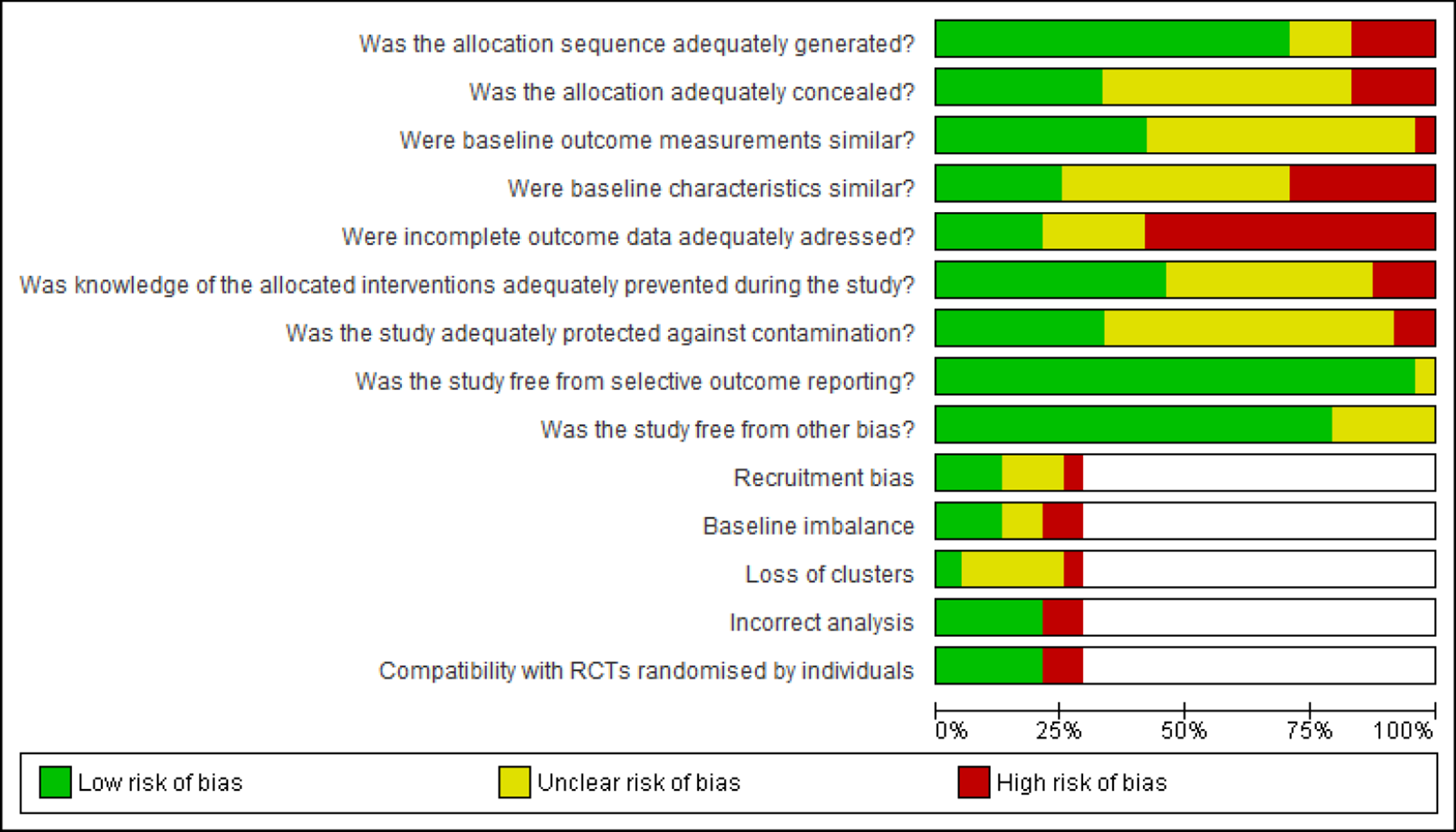
Summary of risk of bias across all included studies
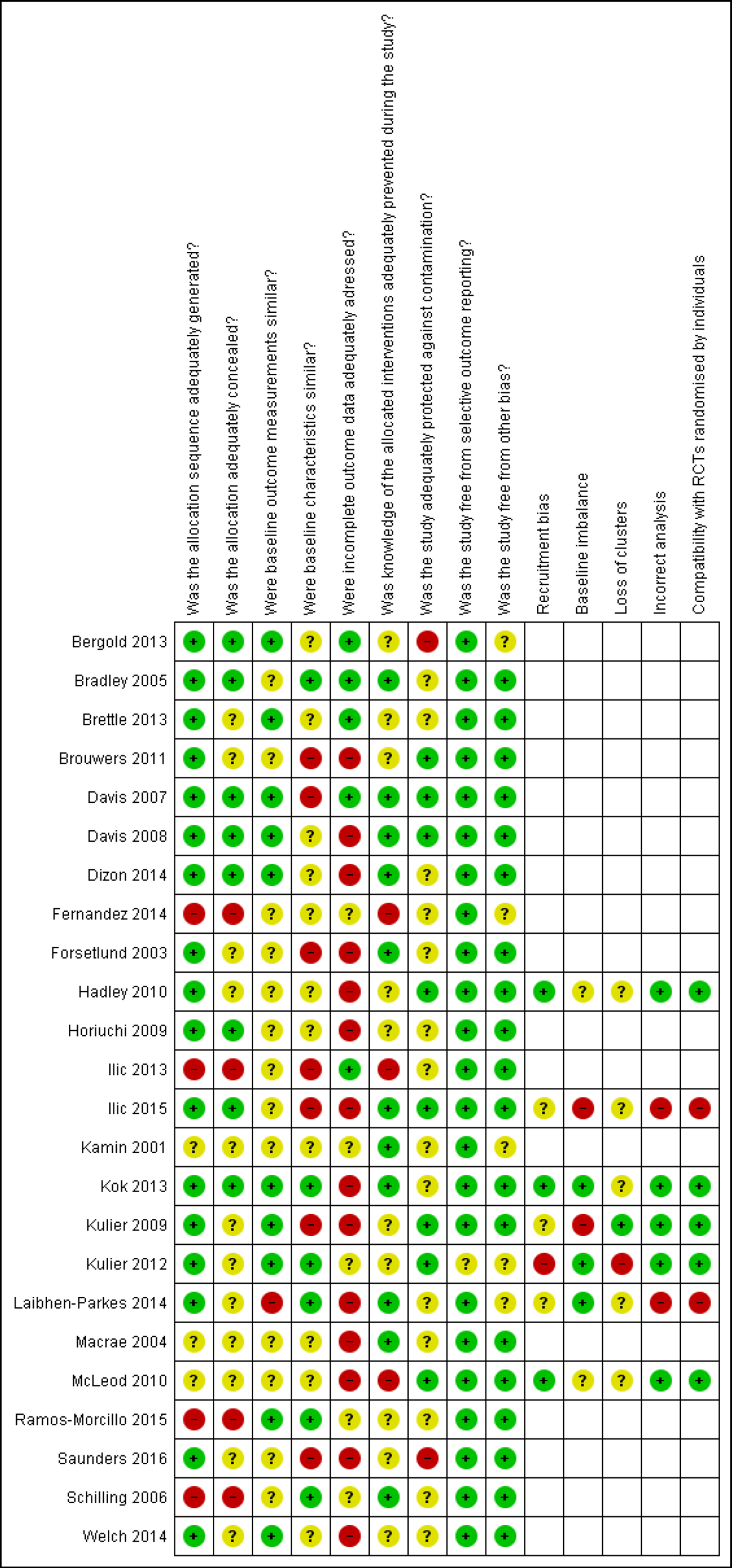
Risk of bias judgement per included study
4.2.1 Selection bias
In 17 RCTs the allocation sequence was adequately generated (Bergold et al., 2013; Bradley et al., 2005; Brettle & Raynor, 2013; Brouwers et al., 2011; Davis et al., 2007; Davis et al., 2008; Dizon et al., 2014; Forsetlund et al., 2003; Hadley et al., 2010; Horiuchi et al., 2009; Ilic et al., 2015; Kok et al., 2013; Kulier et al., 2009; Kulier et al., 2012; Laibhen-Parkes, 2014; Saunders et al., 2016; Welch, Van Lunen, & Hankemeier, 2014). Four non-RCTs did not make use of randomisation (Fernandez et al., 2014; Ilic et al., 2013; Ramos-Morcillo et al., 2015; Schilling et al., 2006) and three studies did not describe how the allocation sequence was generated so they were judged as having unclear risk of selection bias (Kamin et al., 2001; Macrae et al., 2004; McLeod et al., 2010). Allocation concealment was adequate in eight RCTs (Bergold et al., 2013; Bradley et al., 2005; Davis et al., 2007; Davis et al., 2008; Dizon et al., 2014; Kok et al., 2013; Kulier et al., 2009; Kulier et al., 2012), not done in the four non-RCTs (Fernandez et al., 2014; Ilic et al., 2013; Ramos-Morcillo et al., 2015; Schilling et al., 2006) and not described and thus judged as unclear in 12 studies (Brettle & Raynor, 2013; Brouwers et al., 2011; Forsetlund et al., 2003; Hadley et al., 2010; Kamin et al., 2001; Laibhen-Parkes, 2014; Macrae et al., 2004; McLeod et al., 2010; Saunders et al., 2016; Welch, Van Lunen, & Hankemeier, 2014).
Baseline outcome measurements were similar between groups in 10 trials (Bergold et al., 2013; Brettle & Raynor, 2013; Davis et al., 2007; Davis et al., 2008; Dizon et al., 2014; Kok et al., 2013; Kulier et al., 2009; Kulier et al., 2012; Ramos-Morcillo et al., 2015; Welch, Van Lunen, & Hankemeier, 2014) and not adequately reported in 13 studies (Bradley et al., 2005; Brouwers et al., 2011; Fernandez et al., 2014; Forsetlund et al., 2003; Hadley et al., 2010; Horiuchi et al., 2009; Ilic et al., 2013; Ilic et al., 2015; Kamin et al., 2001; Macrae et al., 2004; McLeod et al., 2010; Saunders et al., 2016; Schilling et al., 2006). In one study (Laibhen-Parkes, 2014) there was a significant difference in EBHC attitudes between groups at baseline.
Baseline characteristics were similar between groups in six studies (Bradley et al., 2005; Kok et al., 2013; Kulier et al., 2012; Laibhen-Parkes, 2014; Ramos-Morcillo et al., 2015; Schilling et al., 2006), not similar in four studies (Brouwers et al., 2011; Davis et al., 2007; Forsetlund et al., 2003; Saunders et al., 2016), not measured in three studies (Ilic et al., 2013; Ilic et al., 2015; Kulier et al., 2009) and unclear in 11 studies (Bergold et al., 2013; Brettle & Raynor, 2013; Davis et al., 2008; Dizon et al., 2014; Fernandez et al., 2014; Hadley et al., 2010; Horiuchi et al., 2009; Kamin et al., 2001; Macrae et al., 2004; McLeod et al., 2010; Welch, Van Lunen, & Hankemeier, 2014).
4.2.2 Attrition bias
Fourteen studies (Brouwers et al., 2011; Davis et al., 2008; Dizon et al., 2014; Forsetlund et al., 2003; Hadley et al., 2010; Horiuchi et al., 2009; Ilic et al., 2015; Kok et al., 2013; Kulier et al., 2009; Laibhen-Parkes, 2014; Macrae et al., 2004; McLeod et al., 2010; Saunders et al., 2016; Welch, Van Lunen, & Hankemeier, 2014) were judged as having high risk of attrition bias, due to significant loss to follow up. Five studies (Fernandez et al., 2014; Kamin et al., 2001; Kulier et al., 2012;Ramos-Morcillo et al., 2015; Schilling et al., 2006) did not adequately describe the flow of all participants and were judged as having unclear risk of attrition bias, whereas five studies (Bergold et al., 2013; Bradley et al., 2005; Brettle & Raynor, 2013; Davis et al., 2007; Ilic et al., 2013) were judged as having low risk of attrition bias.
4.2.3 Detection bias
Eleven studies (Bradley et al., 2005; Davis et al., 2007; Davis et al., 2008; Dizon et al., 2014; Forsetlund et al., 2003; Ilic et al., 2015; Kamin et al., 2001; Kok et al., 2013; Laibhen-Parkes, 2014; Macrae et al., 2004; Schilling et al., 2006) adequately blinded outcome assessors and were judged as having low risk of detection bias. We judged three studies (Fernandez et al., 2014; Ilic et al., 2013; McLeod et al., 2010) as having high risk of detection bias, since outcome assessors were not adequately blinded. The remaining 10 studies (Bergold et al., 2013; Brettle & Raynor, 2013; Brouwers et al., 2011; Hadley et al., 2010; Horiuchi et al., 2009; Kulier et al., 2009; Kulier et al., 2012; Ramos-Morcillo et al., 2015; Saunders et al., 2016; Welch, Van Lunen, & Hankemeier, 2014) did not adequately report on blinding and were judged as having unclear risk of detection bias.
4.2.4 Contamination
Eight trials (Brouwers et al., 2011; Davis et al., 2007; Davis et al., 2008; Hadley et al., 2010; Ilic et al., 2015; Kulier et al., 2009; Kulier et al., 2012; McLeod et al., 2010) were adequately protected against contamination. We judged two trials as having high risk of contamination (Bergold et al., 2013; Saunders et al., 2016;); in the remaining 14 trials (Bradley et al., 2005; Brettle & Raynor, 2013; Dizon et al., 2014; Fernandez et al., 2014; Forsetlund et al., 2003; Horiuchi et al., 2009; Kamin et al., 2001; Kok et al., 2013; Laibhen-Parkes, 2014; Macrae et al., 2004; Schilling et al., 2006; Welch, Van Lunen, & Hankemeier, 2014) the risk of contamination was unclear.
4.2.5 Reporting biases
We judged one study (Kulier et al., 2012) as having unclear risk of reporting bias, since the authors only reported the baseline measurements for one of the outcomes. The remaining studies all reported on pre-specified outcomes and were judged as having low risk of reporting bias.
4.2.6 Other bias
We judged five studies (Bergold et al., 2013; Fernandez et al., 2014; Kamin et al., 2001; Kulier et al., 2012; Laibhen-Parkes, 2014) as having unclear risk of other bias and the remaining studies as low risk of other bias.
4.2.7 Additional risk of bias in cluster RCTs
4.2.7.1 Recruitment bias
Three cluster randomised trials (Hadley et al., 2010; Kok et al., 2013; McLeod et al., 2010) had low risk of recruitment bias, since participants were recruited before randomisation of clusters. For three studies (Ilic et al., 2015; Kulier et al., 2009; Laibhen-Parkes, 2014) it was unclear whether participants were recruited before or after randomisation of clusters, and one trial (Kulier et al., 2012) was at high risk of recruitment bias, since participants were recruited after randomisation.
4.2.7.2 Baseline imbalance
In three studies (Kok et al., 2013; Kulier et al., 2012; Laibhen-Parkes, 2014), baseline characteristics were not significantly different between groups whereas in two other studies (Hadley et al., 2010; McLeod et al., 2010), it was unclear whether there were baseline imbalances between groups. Two studies (Ilic et al., 2015; Kulier et al., 2009) did not measure baseline characteristics and were judged as having high risk of baseline imbalances.
4.2.7.3 Loss of clusters
One study (Kulier et al., 2012) lost more than 20% of clusters and was judged as having high risk of bias. Five studies (Hadley et al., 2010; Ilic et al., 2015; Kok et al., 2013; Laibhen-Parkes, 2014; McLeod et al., 2010) had unclear risk of bias, since loss of clusters was not reported, and one study (Kulier et al., 2009) had low risk of bias.
4.2.7.4 Incorrect analysis
We judged five studies as having low risk of bias (Hadley et al., 2010; Kok et al., 2013; Kulier et al., 2009; Kulier et al., 2012; McLeod et al., 2010), since authors reported that adjustment for clustering was done. Two studies (Ilic et al., 2015; Laibhen-Parkes, 2014) did not adjust results for clustering and we judged them as having high risk of bias.
4.2.7.5 Compatibility with individually randomised controlled trials
Results from five cluster RCTs were compatible with the individually randomised trials and had low risk of bias. Two studies that did not adjust results for clustering were judged as not being compatible with individually randomised studies (Ilic et al., 2015; Laibhen-Parkes, 2014).
4.3 SYNTHESIS OF RESULTS
Twenty-three studies were included in the synthesis of results. One study (Bergold et al., 2013) was excluded from the synthesis because the timing of measurement of outcomes differed for the intervention and comparison group. EBHC knowledge and skills scores were measured at baseline and after the intervention in the intervention group. For the waitlist-control group, however, baseline scores were only measured at three months.
We pooled results using random-effects meta-analysis and report on the pooled standardised mean difference for each outcome. A summary of the results is presented in Table 9.9. Interventions differed considerably between studies, so the overall mean effect may not be an accurate reflection of the impacts for any particular intervention type.
4.3.1 Pure e-learning vs no learning
One non-randomised trial (Schilling et al., 2006) and two RCTs (Laibhen-Parkes, 2014; Welch et al., 2014) compared pure e-learning to no learning (Table 12.1). Overall, results favoured pure e-learning interventions.
4.3.1.1 Primary outcomes
4.3.1.1.1 EBHC knowledge
One RCT (Welch et al., 2014) reported on EBHC knowledge (Analysis 1.1). EBHC knowledge scores were higher for participants in the group that received pure e-learning compared to the group that received no learning (SMD 0.71 95%CI 0.40 to 1.01; 1 study, n=175). The SMD of 0.71 can be interpreted as a medium effect size.
4.3.1.1.2 EBHC knowledge and skills
One RCT (Laibhen-Parkes, 2014) reported on EBHC knowledge and skills. There was no significant difference between groups in post-intervention knowledge and skills scores (SMD 0.47 95%CI -0.27 to 1.21, 1 study, n=29) (Analysis 1.2).
4.3.1.1.3 EBHC skills
One non-RCT (Schilling et al., 2006) reported on EBHC skills. The mean MEDLINE searching score for the intervention group was 2.9 (n=74) compared to 2.1 (n=58) in the control group (p<0.05). The authors did not report standard deviations (SD) or 95%CI for the means. Participants in the intervention group had greater odds of calculating the number needed to treat (NNT) correctly, compared to the control group (OR 5.4 95%CI 2.7 to 11.0, n=179).
4.3.1.1.4 EBHC attitude
One non-RCT (Schilling et al., 2006) and one RCT (Laibhen-Parkes, 2014) reported on EBHC attitude. Post-intervention attitude scores, adjusted for pre-intervention scores, were higher for the intervention group compared to the control group (SMD 1.05 95% CI 0.26 to 1.83; 1 study, n=29) (Analysis 1.3). The SMD of 1.05 can be interpreted as a large effect size.
In Schilling et al. (2006), the MD in change of attitude scores from baseline to post-intervention, was significantly higher (p<0.05) in the intervention group for seven of the eight statements related to EBHC attitude.
4.3.1.1.5 EBHC behaviour
None of the studies comparing EBHC pure e-learning to no intervention reported on EBHC behaviour outcomes.
4.3.1.2 Secondary outcomes
4.3.1.2.1 Satisfaction of students with method of learning
No studies reported on this outcome.
4.3.1.2.2 Satisfaction of educator with method of learning
No studies reported on this outcome.
4.3.1.2.3 Enablers of the method of learning EBHC
No studies reported on this outcome.
4.3.1.2.4 Barriers to the method of learning EBHC
No studies reported on this outcome.
4.3.1.2.5 Cost
No studies reported on this outcome.
4.3.1.2.6 Attrition of learners
Two studies reported on attrition rates (Laibhen-Parkes, 2014; Welch, Van Lunen, & Hankemeier, 2014). There was no difference in attrition rates between the intervention and control group for this comparison (RR 1.03; 95% CI 0.9 to 1.18; Chi2=1.58, P=0.21; I2=37%; n=531) (Analysis 1.4).
4.3.1.2.7 Learner adherence
No studies reported on this outcome.
4.3.1.2.8 Evidence-based practice
No studies reported on this outcome.
4.3.1.2.9 Evidence-based guideline implementation
No studies reported on this outcome.
4.3.1.2.10 Health care delivery
No studies reported on this outcome.
4.3.1.2.11 Individual health outcomes
No studies reported on this outcome.
4.3.1.2.12 Population health outcomes
No studies reported on this outcome.
4.3.2 Blended learning vs no learning
One non-RCT (Ramos-Morcillo et al., 2015) and four RCTs (Bergold et al., 2013; Dizon et al., 2014; Forsetlund et al., 2003; Kok et al., 2013) compared blended learning with no learning (Table 12.2). Overall, results favoured blended learning interventions for EBHC knowledge and skills.
4.3.2.1 Primary outcomes
4.3.2.1.1 EBHC knowledge
One RCT (Forsetlund et al., 2003) reported on EBHC knowledge. Knowledge scores were higher in the blended learning group compared to the control group (SMD 0.50 95%CI 0.13 to 0.86; 1 study, n=119) (Analysis 2.1). The SMD of 0.5 can be interpreted as a medium effect size.
4.3.2.1.2 EBHC knowledge and skills
One non-RCT (Ramos-Morcillo et al., 2015) and two RCTs (Dizon et al., 2014; Kok et al., 2013) reported on EBHC knowledge and skills. These trials measured scores at multiple time points, i.e. directly post-intervention as well as one month (Kok et al., 2013; Ramos-Morcillo et al., 2015), 3 months (Dizon et al., 2014) and 6 months (Kok et al., 2013) after the intervention. We report on the short term as well as long term EBHC knowledge and skills scores separately.
For EBHC knowledge and skills scores measured immediately post-intervention we included two trials (Dizon et al., 2014; Ramos-Morcillo et al., 2015) in the random-effects meta-analysis (Analysis 2.2). Although results from both trials favoured blended learning, the pooled effect showed no difference in EBHC knowledge and skills scores (SMD 1.40 95%CI -0.06 to 2.85, 2 studies, n=163). Heterogeneity was high (Tau2=1.02; Chi2=13.80, P=0.0002; I2=93%) and the test for subgroup differences was significant (p=0.0002; I2=92%). The SMD of 1.4 can be interpreted as a very large effect size, although the results are not statistically significant.
For EBHC knowledge and skills scores measured one month after the intervention, we included two trials (Kok et al., 2013; Ramos-Morcillo et al., 2015) in the random-effects meta-analysis (Analysis 2.3). EBHC knowledge and skills scores were higher amongst participants in the blended learning group, compared to the group that received no learning (SMD 0.9 95%CI 0.42 to 1.38, 2 studies, n=141). Heterogeneity was high (Tau2 = 0.08; Chi2 = 3.25, P = 0.07; I2 = 69%) with a significant test for subgroup differences (p=0.07; I2=69.2%). The SMD of 0.9 can be interpreted as a large effect size.
For EBHC knowledge and skills scores measured more than 3 months after the intervention, we included two trials (Dizon et al., 2014; Kok et al., 2013) in the random-effects meta-analysis (Analysis 2.4). EBHC knowledge and skills scores remained higher in the blended learning group compared to the group that received no learning (SMD 1.11 95%CI 0.80 to 1.42, 2 studies, n=186). Heterogeneity was high (Chi2 = 5.33, P = 0.02; I2 = 81%). The SMD of 1.11 can be interpreted as a large effect size.
4.3.2.1.3 EBHC skills
No studies reported on EBHC skills.
4.3.2.1.4 EBHC attitude
One non-RCT (Ramos-Morcillo et al., 2015) and three RCTs (Dizon et al., 2014; Forsetlund et al., 2003; Kok et al., 2013; Ramos-Morcillo et al., 2015) reported on post-intervention attitude scores. Three trials measured scores at multiple time points i.e. directly post-intervention as well as one month (Kok et al., 2013; Ramos-Morcillo et al., 2015), 3 months (Dizon et al., 2014) and 6 months (Kok et al., 2013) after the intervention.
For EBHC attitudes measured directly post-intervention we included one non-RCT (Ramos-Morcillo et al., 2015) and one RCT (Forsetlund et al., 2003) in the random-effects meta-analysis (Analysis 2.5). There was no difference in EBHC attitude scores between groups (SMD 0.17 95%CI -0.09 to 0.48, 2 studies, n=226). Heterogeneity was absent (Tau2 = 0.00; Chi2 = 0.15, P = 0.70; I2 = 0%).
For EBHC attitude scores measured one month post-intervention, we included one non-RCT (Ramos-Morcillo et al., 2015) and one RCT (Kok et al., 2013) in the random-effects meta-analysis (Analysis 2.6). There was no difference in EBHC attitude scores between groups (SMD 0.05 95%CI -0.34 to 0.44). Heterogeneity was moderate but non-significant (Tau2 = 0.05; Chi2 = 2.36, P = 0.12; I2 = 58%).
One RCT (Kok et al., 2013) measured EBHC attitude six months post-intervention and found no difference between groups (SMD 0.32 95%CI -0.02 to 0.67, 1 study, n=132) (Analysis 2.7).
In Dizon et al. (2014), attitude scores (3-point Likert scale) in the blended learning group were significantly different compared to the wait-list control group for two of the six attitude statements (“I would lack confidence in undertaking a literature search” and “I would feel confident in undertaking a critical appraisal”) immediately post-intervention and three months post intervention. For the statement “I would find it difficult to change what I already do in clinical practice”, there was a significant difference between groups immediately post-intervention, but not at three months post-intervention.
4.3.2.1.5 EBHC behaviour
One non-RCT (Ramos-Morcillo et al., 2015) and three RCTs (Dizon et al., 2014; Forsetlund et al., 2003; Kok et al., 2013) reported on EBHC behaviour. Dizon et al. (2014) and Kok et al. (2013) measured behaviour 3 months after the intervention. Forsetlund et al. (2003) only measured behaviour directly after the intervention, while Ramos-Morcillo et al. (2015) measured EBHC behaviour directly after, as well as 40 days after the intervention.
For EBHC behaviour measured directly post intervention, we included one non-RCT (Ramos-Morcillo et al., 2015) and one RCT (Forsetlund et al., 2003) in the random-effects meta-analysis (Analysis 2.8). Overall, there was no difference between groups (SMD 0.06 95%CI -0.28 to 0.40, 2 studies, n=207). Heterogeneity was low (Tau2 = 0.02; Chi2 = 1.53, P = 0.22; I2 = 35%) and there was no difference between subgroups (p=0.22, I2=34.8%).
For EBHC behaviour measured one month post intervention, we included one non-RCT (Ramos-Morcillo et al., 2015) in the random-effects meta-analysis (Analysis 2.9). There was no significant difference between groups (SMD 0.19 95%CI -0.19 to 0.56, 1 study, n=109).
For EBHC behaviour measured 3+ months post-intervention, we included one RCT (Kok et al., 2013) in the random-effects meta-analysis (Analysis 2.10). Behaviour scores were greater for the blended learning compared to no learning results (SMD 0.61 95%CI 0.21 to 1.01, 1 study, n=100). The SMD can be interpreted as a medium effect size.
In Dizon et al. (2014), 18 participants in the intervention and 19 in the wait-list control group submitted activity diaries three months post-intervention. There was a significant difference in EBHC behaviour between groups for all categories when faced with a new or unique case (n=24), and significant differences for all but one category (logging PICO questions) when participants were faced with usual cases (n=19). For non-EBP behaviour, there was a significant difference between groups for two (asking medical doctors and reading textbooks) of the three categories when faced with a new case, but no significant difference between groups when faced with a usual case.
4.3.2.2 Secondary outcomes
4.3.2.2.1 Satisfaction of students with method of learning
No studies reported on this outcome.
4.3.2.2.2 Satisfaction of educator with method of learning
No studies reported on this outcome.
4.3.2.2.3 Enablers of the method of learning EBHC
No studies reported on this outcome.
4.3.2.2.4 Barriers to the method of learning EBHC
No studies reported on this outcome.
4.3.2.2.5 Cost
No studies reported on this outcome.
4.3.2.2.6 Attrition of learners
Three studies (Bergold et al., 2013; Dizon et al., 2014; Kok et al., 2013) reported on attrition rates. Random-effects meta-analysis (Analysis 2.11) showed no significant difference in attrition of learners between groups (RR 0.82 95%CI 0.55 to 1.20; n=306; Chi2=0.75, P=0.69; I2=0%).
4.3.2.2.7 Learner adherence
No studies reported on this outcome.
4.3.2.2.8 Evidence-based practice
No studies reported on this outcome.
4.3.2.2.9 Evidence-based guideline implementation
No studies reported on this outcome.
4.3.2.2.10 Health care delivery
No studies reported on this outcome.
4.3.2.2.11 Individual health outcomes
No studies reported on this outcome.
4.3.2.2.12 Population health outcomes
No studies reported on this outcome.
4.3.3 Pure e-learning vs face-to-face learning
SixRCTs (Bradley et al., 2005; Davis et al., 2007; Davis et al., 2008; Hadley et al., 2010; Horiuchi et al., 2009; McLeod et al., 2010) compared pure e-learning to face-to-face learning (Table 12.3). Overall, there was no difference between groups for any of the outcomes.
4.3.3.1 Primary outcomes
4.3.3.1.1 EBHC knowledge
Five RCTs reported on EBHC knowledge (Bradley et al., 2005; Davis et al., 2007; Davis et al., 2008; Hadley et al., 2010; Horiuchi et al., 2009) and were included in the random-effects meta-analysis (Analysis 3.1). There was no difference in knowledge scores between pure e-learning compared to face-to-face learning (SMD -0.03 95%CI -0.26 to 0.20; 5 studies, n=632). Heterogeneity was moderate (Tau2 = 0.03; Chi2 = 7.74, P = 0.10; I2 = 48%) and caused by one outlier (Davis et al., 2008). A possible reason for Davis et al. (2008) being the only study where results favoured face-to-face learning is the attrition rate amongst participants in the pure e-learning group (44/114; 39%) compared to the face-to-face learning group (6/115; 5%). When removing this trial from the analysis, the effect does not change (SMD 0.05 95%CI -0.14 to 0.25) and heterogeneity is reduced (Tau2 = 0.00; Chi2 = 3.24, P = 0.36; I2 = 7%).
4.3.3.1.2 EBHC knowledge and skills
No studies reported on this outcome.
4.3.3.1.3 EBHC skills
Two RCTs reported on EBHC skills (Bradley et al., 2005; McLeod et al., 2010) and were included in the random-effects meta-analysis (Analysis 3.2). There was no difference in EBHC skills scores between groups (SMD -0.15 95%CI -0.34 to 0.04; 2 studies, n=457), with no significant heterogeneity (Tau2 = 0.00; Chi2 = 1.04, P = 0.31; I2 = 4%).
4.3.3.1.4 EBHC attitude
Three RCTs (Bradley et al., 2005; Davis et al., 2007; Davis et al., 2008) reported on EBHC attitude. Data from one RCT (P. Bradley et al., 2005) showed no difference in EBHC attitude scores between groups (SMD 0.11 95%CI -0.27 to 0.48, 1 study, n=111) (Analysis 3.3). Change in EBHC attitude from baseline to post-intervention was similar between groups in Davis et al. (2007) and Davis et al. (2008). Authors did not report on means and SDs.
4.3.3.1.5 EBHC behaviour
No studies reported on this outcome.
4.3.3.2 Secondary outcomes
4.3.3.2.1 Satisfaction of students with method of learning
One study (Horiuchi et al., 2009) explored learners’ satisfaction with the learning modality and reported selected quotes from both groups. The intervention group felt that learning at their own pace and in their own time was very convenient, but some also felt that they at times lacked motivation to engage with the content. The face-to-face learning group enjoyed the interaction and small group discussions during the sessions but some could not fit the sessions into their schedule.
4.3.3.2.2 Satisfaction of educator with method of learning
No studies reported on this outcome.
4.3.3.2.3 Enablers of the method of learning EBHC
No studies reported on this outcome.
4.3.3.2.4 Barriers to the method of learning EBHC
No studies reported on this outcome.
4.3.3.2.5 Cost
No studies reported on this outcome.
4.3.3.2.6 Attrition of learners
Six studies reported on attrition rates (Bradley et al., 2005; Davis et al., 2007; Davis et al., 2008; Hadley et al., 2010; Horiuchi et al., 2009; McLeod et al., 2010). In Davis et al. (2007), no participants were lost to follow-up.
Random-effects meta-analysis (Analysis 3.4) of the attrition rates showed no difference for attrition rates between e-learning and face-to-face learning groups (RR1.24 95% CI 0.59 to 2.59; 5 studies n=1175; Tau2 = 0.55; Chi2 = 35.20, P<0.00001); I2 = 89%).
4.3.3.2.7 Learner adherence
No studies reported on this outcome.
4.3.3.2.8 Evidence-based practice
No studies reported on this outcome.
4.3.3.2.9 Evidence-based guideline implementation
No studies reported on this outcome.
4.3.3.2.10 Health care delivery
No studies reported on this outcome.
4.3.3.2.11 Individual health outcomes
No studies reported on this outcome.
4.3.3.2.12 Population health outcomes
No studies reported on this outcome.
4.3.4 Blended learning vs face-to-face learning
One non-RCT (Ilic et al., 2013) and four RCTs (Brettle & Raynor, 2013; Ilic et al., 2015; Kulier et al., 2009; Saunders et al., 2016) compared blended learning to face-to-face learning (Table 12.4). Overall, results were similar between groups for EBHC knowledge and skills, but favoured the blended learning approach for EBHC attitude and behaviour.
4.3.4.1 Primary outcomes
4.3.4.1.1 EBHC knowledge
Two RCTs reported on EBHC knowledge (Kulier et al., 2009; Saunders et al., 2016) and were included in the random-effects meta-analysis (Analysis 4.1). Results from Kulier et al. (2009) showed no difference in EBHC knowledge scores between groups (SMD 0.28 95%CI-0.23 to 0.79; 1 study, n=61).
Saunders et al. (2016) did not provide means and SDs and we were thus not able to include these in the meta-analysis. We contacted authors and are awaiting their response.
4.3.4.1.2 EBHC knowledge and skills
One non-RCT (Ilic et al., 2013) and one RCT (Ilic et al., 2015) reported on EBHC knowledge and skills and were included in the random-effects meta-analysis (Analysis 4.2). There was no difference in EBHC knowledge and skills scores between groups (SMD -0.23 95%CI -0.52 to 0.06; 2 studies; n=208). Heterogeneity was low (Tau2 = 0.00; Chi2 = 0.01, P = 0.93; I2 = 0%) and there was no significant difference between subgroups (p=0.93, I2=0%).
4.3.4.1.3 EBHC skills
One RCT reported on EBHC skills (Brettle & Raynor, 2013). Post-intervention searching scores were not significantly different between groups after the first session (SMD -0.21 95%CI -0.68 to 0.26; n=70) (Analysis 4.3).
4.3.4.1.4 EBHC attitude
One non-RCT (Ilic et al., 2013) and two RCTs (Ilic et al., 2015; Kulier et al., 2009) reported on EBHC attitude, but only Ilic et al. (2015) reported sufficient data to be included in a meta-analysis. EBHC attitude scores were significantly higher in the blended learning group compared to the face-to-face learning group (SMD 1.07 95%CI 0.57 to 1.58; 1 study, n=82) (Analysis 4.4). The SMD of 1.08 can be interpreted as a large effect size.
In Ilic et al. (2013) attitude scores in the blended learning group were significantly higher compared to the face-to-face group for the statement “I believe that I will use my EBM skills during my clinical career” (p=0.03), but not for the statement “I believe that practicing evidence based medicine is critical in being a good clinician”(p=0.08).
There was no statistically significant difference in attitudinal gain between blended learning and face-to-face learning groups in Kulier et al. (2009).
4.3.4.1.5 EBHC behaviour
One study (Ilic et al., 2015) reported on EBHC behaviour using the self-reported Evidence-based Practice Questionnaire, which contains six questions related to EBHC behaviour. Data was analysed for 17% (44/263) of participants from the blended learning group and 16% (38/234) of participants from the face-to-face learning group.
EBHC behaviour scores were significantly greater for participants in the blended learning group (SMD 2.3495%CI 1.72 to 2.96; 1 study, n=82) (Analysis 4.5). The SMD of 2.35 can be interpreted as a huge effect.
4.3.4.2 Secondary outcomes
4.3.4.2.1 Satisfaction of students with method of learning
One non-RCT (Ilic et al., 2013) and one RCT (Ilic et al., 2015) reported on satisfaction of participants with the method of learning.
Ilic et al. (2013) found that learners in the blended learning group were significantly more satisfied with the method of learning compared to the face-to-face learning group, with three of the five statements related to satisfaction being statistically significant. Learners preferred the blended learning approach.
Ilic et al. (2015) found that students preferred a blended learning approach. Learners felt that didactic lectures were useful for acquiring new knowledge, but that it did not matter whether these were delivered face-to-face or online. They also perceived small group activities to be useful in acquiring new skills, which also motivated them to apply these in the clinical context. Learners in the face-to-face learning group, however, found the content to be “dense and dry” and felt that the learning approach only supported superficial learning.
4.3.4.2.2 Satisfaction of educator with method of learning
No studies reported on this outcome.
4.3.4.2.3 Enablers of the method of learning EBHC
No studies reported on this outcome.
4.3.4.2.4 Barriers to the method of learning EBHC
One RCT reported on the enablers of the method of EBHC learning (Ilic et al., 2015). These included variations in methods of implementation of learning across study sites and the difficulty to apply the learned concepts in clinical practice. Learners also felt that EBHC teaching would have greater value in subsequent clinical years.
4.3.4.2.5 Cost
No studies reported on this outcome.
4.3.4.2.6 Attrition of learners
One non-RCT (Ilic et al., 2013) and four RCTs (Brettle & Raynor, 2013; Ilic et al., 2015; Kulier et al., 2009; Saunders et al., 2016) reported on attrition of learners. In Ilic et al. (2013) there was no loss to follow-up in either group. The four RCTs were included in the random-effects meta-analysis (Analysis 4.6) and showed similar attrition rates between blended learning and face-to-face learning groups (RR 1.50 95%CI 0.79 to 2.85; n=729; Tau2 = 0.17; Chi2 = 4.59, P=0.20; I2 = 35%).
4.3.4.2.7 Learner adherence
No studies reported on this outcome.
4.3.4.2.8 Evidence-based practice
No studies reported on this outcome.
4.3.4.2.9 Evidence-based guideline implementation
No studies reported on this outcome.
4.3.4.2.10 Health care delivery
No studies reported on this outcome.
4.3.4.2.11 Individual health outcomes
No studies reported on this outcome.
4.3.4.2.12 Population health outcomes
No studies reported on this outcome.
4.3.5 Blended learningvs pure e-learning
One non-RCT (Fernandez et al., 2014) and two RCTs (Kamin et al., 2001; Kulier et al., 2012) compared pure e-learning to blended learning (Table 12.5). In Fernandez et al. (2014), the pure e-learning intervention (DVD group) was compared to three control groups: the standard distance group (pure e-learning), the computer lab group (blended learning) and the didactic lectures group (blended learning). We included the two blended learning groups for this comparison. Overall, results favoured blended learning.
4.3.5.1 Primary outcomes
4.3.5.1.1 EBHC knowledge
Two RCTs (Kamin et al., 2001; Kulier et al., 2012) reported on EBHC knowledge and were included in the random-effects meta-analysis (Analysis 5.1). EBHC knowledge scores were significantly higher in the blended learning group compared to the pure e-learning group (SMD 0.69 95%CI 0.40 to 0.99; 2 studies, n=193). Results were consistent across the two studies with low levels of heterogeneity (Tau2 = 0.00; Chi2 = 0.97, P = 0.32; I2 = 0%). The SMD of 0.69 can be interpreted as a medium effect size.
4.3.5.1.2 EBHC knowledge and skills
No studies reported on this outcome.
4.3.5.1.3 EBHC skills
One non-RCT (Fernandez et al., 2014) and one RCT (Kulier et al., 2012) reported on EBHC skills. In Fernandez et al. (2014), participants had to submit two assignments. The first assignment measured EBHC skills related to formulating PICO questions, searching the literature and identifying the level of evidence, while the second assignment measured critical appraisal skills. We included critical appraisal scores in the random-effects meta-analysis (Analysis 5.2). Overall, there was no difference between blended learning and pure e-learning (SMD -0.53 95%CI -2.31 to1.25; 2 studies, n=218). There was a significant difference between subgroups (p<0.00001, I2=96.2%), with results for the non-RCT (Fernandez et al., 2014) favoring pure e-learning (SMD-1.46 95%CI -2.08 to -0.84) and results for the RCT (Kulier et al., 2012) favouring blended learning (SMD 0.36 95%CI 0.05 to 0.67).
We report the remaining results from Fernandez et al. (2014) related to PICO, searching and levels of evidence in Analysis 5.3. Overall, results favoured the pure e-learning group.
4.3.5.1.4 EBHC attitude
Although authors of one RCT (Kulier et al., 2012) stated that they measured EBHC attitude, they only reported baseline scores, and not those at follow-up.
4.3.5.1.5 EBHC behaviour
No studies reported on this outcome.
4.3.5.2 Secondary outcomes
4.3.5.2.1 Satisfaction of students with method of learning
No studies reported on this outcome.
4.3.5.2.2 Satisfaction of educator with method of learning
No studies reported on this outcome.
4.3.5.2.3 Enablers of the method of learning EBHC
No studies reported on this outcome.
4.3.5.2.4 Barriers to the method of learning EBHC
No studies reported on this outcome.
4.3.5.2.5 Cost
No studies reported on this outcome.
4.3.5.2.6 Attrition of learners
One RCT (Kulier et al., 2012) reported on attrition of learners. In the blended learning group, 25/123 (20.3%) of learners were lost to follow-up, compared to 13/81 (16%) in the pure e-learning group (RR 1.27, 95%CI 0.69 to 2.33, 1 study, n=204) (Analysis 5.4).
4.3.5.2.7 Learner adherence
No studies reported on this outcome.
4.3.5.2.8 Evidence-based practice
No studies reported on this outcome.
4.3.5.2.9 Evidence-based guideline implementation
No studies reported on this outcome.
4.3.5.2.10 Health care delivery
No studies reported on this outcome.
4.3.5.2.11 Individual health outcomes
No studies reported on this outcome.
4.3.5.2.12 Population health outcomes
No studies reported on this outcome.
4.3.6 Pure e-learning vs pure e-learning
One non-RCT (Fernandez et al., 2014) and two RCTs (Brouwers et al., 2011; Macrae et al., 2004) compared pure e-learning to another form of pure e-learning (Table 12.6). Brouwers et al. (2011) compared three intervention groups. The first group received an online tutorial on AGREE II and was granted access to a PDF copy of the AGREE II tool, the second group received the online tutorial plus a practical exercise and feedback, and the third group received the AGREE II manual. For Fernandez et al. (2014), we included the comparison between the DVD group and the standard distance group. In MacRae et al. (2004) the intervention group participated in an online journal club that included an asynchronous discussion list, while the control group only received the articles per email and had access to electronic journals.
4.3.6.1 Primary outcomes
4.3.6.1.1 EBHC knowledge
4.3.6.1.2 No studies reported on this outcome. EBHC knowledge and skills
No studies reported on this outcome.
4.3.6.1.3 EBHC skills
One non-RCT (Fernandez et al., 2014) and two RCTs (Brouwers et al., 2011; Macrae et al., 2004) reported on EBHC skills. We included critical appraisal skills for one non-RCT (Fernandez et al., 2014) and one RCT (Macrae et al., 2004) in the random-effects meta-analysis (Analysis 6.1). Results favoured the intervention (SMD 1.30 95%CI 0.68 to 1.98, 2 studies, n=119) with moderate levels of heterogeneity (Tau2 = 0.12; Chi2 = 2.45, P = 0.12; I2 = 59%). The test for subgroup differences was not significant (p=0.12, I2=59.2%). The SMD of 1.30 can be interpreted as a very large effect. Interventions comprised a DVD containing all the learning material compared to the standard distance learning programme in Ferndandez et al. (2014) and an online journal club with an asynchronous discussion list compared to receiving the journal arcitles via email in MacRae (2004).
Brouwers et al. (2011) calculated the distance function, which is the difference between participants and experts in scores for each domain of the AGREE II tool. There was no statistically significant difference in distance function between any of the three pure e-learning intervention groups.
EBHC skills related to PICO, searching the literature and levles of evidence are reported in Analysis 6.2. Overall, participants in the DVD group achieved higher scores compared to the standard distance learning group.
4.3.6.1.4 EBHC attitude
No studies reported on this outcome.
4.3.6.1.5 EBHC behaviour
4.3.6.2 No studies reported on this outcome. Secondary outcomes
4.3.6.2.1 Satisfaction of students with method of learning
One study (Brouwers et al., 2011) reported on satisfaction with the method of learning. There was no statistically significant difference in satisfaction scores between the three pure e-learning groups.
4.3.6.2.2 Satisfaction of educators with method of learning
No studies reported on this outcome.
4.3.6.2.3 Enablers of the method of learning EBHC
No studies reported on this outcome.
4.3.6.2.4 Barriers to the method of learning EBHC
No studies reported on this outcome.
4.3.6.2.5 Cost
No studies reported on this outcome.
4.3.6.2.6 Attrition of learners
Two studies (Brouwers et al., 2011; Macrae et al., 2004) reported on attrition rates. Random-effects meta-analysis showed that attrition rates were similar between groups (RR 1.43 95%CI 0.89 to 2.31; n=170; Chi2 = 0.89, P=0.64; I2=0%) (Analysis 6.3).
4.3.6.2.7 Learner adherence
No studies reported on this outcome.
4.3.6.2.8 Evidence-based practice
No studies reported on this outcome.
4.3.6.2.9 Evidence-based guideline implementation
No studies reported on this outcome.
4.3.6.2.10 Health care delivery
No studies reported on this outcome.
4.3.6.2.11 Individual health outcomes
No studies reported on this outcome.
4.3.6.2.12 Population health outcomes
No studies reported on this outcome.
5 Discussion
5.1 SUMMARY OF MAIN RESULTS
Twenty-four studies with a total of 3806 participants comprising 13 individually randomised trials, seven cluster RCTs and four non-RCTsmet the inclusion criteria for our systematic review.
Participants included under- and postgraduate students, as well as practicing health care professionals of various health professions with medicine being the most common profession (14/24 studies). Studies were mainly conducted in high-income countries including the USA, Australia and various countries in Europe with only two trials conducted in LMICs – one in the Philippines and one in multiple countries: Argentina, Brazil, Democratic Republic of Congo, India, Philippines, South Africa and Thailand.
E-learning interventions were heterogeneous. Although the content of the interventions generally covered the first four steps of EBHC (asking questions, accessing the literature, critically appraising the literature, and applying the results), we identified 17 different categories of intervention components. The interventions of five studies included only one component (single intervention), while the remaining interventions comprised various components in combination and were considered to be multi-faceted. Duration of interventions ranged from a single, one-hour session to a journal club addressing one article per month and running over eight months. Ten studies explicitly referred to educational theories or learning approaches underpinning the interventions but did not report results in light of these.
Studies mostly reported on EBHC knowledge and skills, with some reporting on EBHC attitude and only five assessing EBHC behaviour. Outcomes were measured at different time points and with various tools, including validated questionnaires, self-perceived knowledge scores, hypothetical assignments and critical appraisal of studies. Outcomes were typically measured and compared after the intervention. Most studies reported outcomes at follow-up, with only a few adjusting results for baseline outcome measurement. Secondary outcomes were rarely reported. Four studies reported on satisfaction of learning, while one study explored barriers to EBHC learning. Rates of the attrition of learners were reported in 16 studies and we were able to pool these results using meta-analysis.
Due to these variations in populations, interventions and measures of outcome assessments across included studies, heterogeneity was considered to be substantial. We therefore pooled results in a random-effects meta-analysis using the SMD for continuous outcomes. Due to the limited number of studies included per comparison, we were unable to explore remaining heterogeneity through subgroup analysis. Heterogeneity due to the different interventions needs to be taken into consideration when interpreting results. In an effort to tease out the differences and similarities between interventions, we compiled a matrix showing the different intervention components for all the included studies (Table 9.7). The EBHC content of each intervention is summarised in Table 9.8.
We summarised results for each comparison in Tables 12.1 to 12.6. We found that pure e-learning, compared to no learning, improved EBHC knowledge and attitude. However, studies in this comparison had high risk of selection and attrition bias, sample sizes were small and results imprecise. For each outcome, only one study provided data for the meta-analysis.
Blended learning compared to no learning improved EBHC knowledge, EBHC knowledge and skills one month post-intervention, and 3+ months post-intervention. We did not find significant differences between groups for EBHC attitude and EBHC behaviour. One study assessed EBHC behaviour 3 months after the intervention and found a significant difference in scores, favouring the blended learning group. There was high risk of selection and/or attrition bias across studies, inconsistency in results and imprecision for most outcomes.
There was no difference in results for pure e-learning compared to face-to-face learning for EBHC knowledge, skills and attitude. Results for outcomes in this comparison were more precise compared to other comparisons, there was high risk of attrition bias and moderate heterogeneity for the outcome EBHC knowledge, caused by one outlier.
There was no difference in EBHC knowledge and skills scores when comparing blended learning to face-to-face learning. We found a significant difference between groups for EBHC attitude and behaviour, although only one study with high risk of attrition bias was included in the analysis. In addition, authors did not adequately adjust for clustering.
Blended learning compared to pure e-learning improved EBHC knowledge. There was unclear risk of selection and attrition bias and high risk of recruitment bias and loss of clusters. For EBHC skills, the two studies included in the analysis had inconsistent results. While results for the non-RCT favoured pure e-learning, results for the cluster RCT favoured blended learning. Confidence intervals were thus very wide and the results imprecise.
When comparing various pure e-learning interventions, the pooled effect was imprecise and heterogeneity between studies was high. One study compared a DVD containing recorded PowerPoints and tutorials, as well as access to online learning material (intervention) to a standard online distance learning programme. The other compared an online journal club with an asynchronous discussion list (intervention) to receiving the articles via email and access to journal articles. Studies had high risk of selection, attrition and detection bias.
5.2 OVERALL COMPLETENESS AND APPLICABILITY OF EVIDENCE
We found substantial heterogeneity between interventions related both to intervention components and delivery of interventions, as has been shown in a previously conducted systematic review (Sinclair et al 2016). We were unable to perform planned subgroup analysis on the different dimensions of e-learning, due to the limited number of included studies per meta-analysis. Studies that reported significant differences between groups typically included multi-faceted interventions (interventions comprising more than one intervention component), intervention components that required participants to interact with one another (e.g. asynchronous discussion lists), and integration of learning with clinical practice by including e.g. mobile bedside learning, exercises related to clinical cases, and access to clinical facilitators. These findings are in line with international literature and recommendations on effective teaching of EBHC (Khan & Coomarasamy, 2006; Young et al., 2014). In addition, our results suggest that blended learning is a more effective strategy than pure e-learning, since it includes multiple components by definition and follows a “best of both worlds” approach.
These suggestions also resonate with other literature on e-learning. A systematic review on instructional design variations in internet-based learning, found that interactivity, practice exercises, repetition and feedback appeared to be associated with improved learning outcomes (Cook et al., 2010). A review by Booth and colleagues (2009) found that presentation and design, flexibility, peer communication, support and knowledge validation was effective e-learning techniques for enhancing the learning experience of students.
Educational context was poorly reported in all included studies. As learning does not occur in a vacuum, it is essential to take into consideration the context within which learning takes place (Figure 2). E-learning is a complex process where the learner, the technology and the context interact (Sandars & Lafferty, 2010). Factors such as learner motivation and the presence of role models in the clinical field can impact significantly on the acquisition of knowledge and skills, as well as learners’ attitude towards EBHC. Unfortunately, educational context was poorly reported in all included trials and we were therefore unable to take setting, learner, institution and socio-economic background into consideration in interpreting the results.
Although some studies did show significant differences in EBHC knowledge and skills scores between groups, the post-intervention scores for intervention groups were generally low, especially when measured with either the Fresno test or the Berlin test. Both these tools have been validated to measure all four steps of EBHC (Shaneyfelt et al., 2006) and are commonly used. In Dizon et al. (2014), for example, EBHC knowledge and skills were measured with an adapted Fresno test and the mean post-intervention score in the intervention group was 64.3/156 (41%). In Ilic et al. (2015), the Berlin test was used and the mean post-intervention score in the intervention group was 8.2/15 (57%). This raises questions about the actual effectiveness of the interventions in terms of knowledge gain and whether obtaining half (or less than half) of the maximum score is considered adequate when learning a new skill. In addition, knowledge and skills scores are the measurable, direct effects of the intervention. Increased knowledge and skills do not automatically translate to behaviour change and evidence-informed decision-making, which would be the ultimately desired outcome (Figure 3).
EBHC behaviour is a complex outcome and it is difficult to measure it objectively (Shaneyfelt et al., 2006; Strauss et al., 2004; Tilson et al., 2011). Only five of the included studies reported on this outcome. In two of these (Kok et al., 2012; Forsetlund et al., 2003), EBHC was measured objectively, while the other three (Ilic et al., 2015; Ramos-Morcillo et al., 2015; Dizon et al., 2014) used self-reported measures. Tilson et al. (2011), as part of the Classification Rubric for EBP Assessment Tools in Education (CREATE) Framework, propose that EBP behaviour should be assessed through activity monitoring. They highlight the lack of adequate tools to measure EBP behaviour and recommend that “valid, practicable methods are needed for monitoring learners’ EBP behaviours that can be used for both formative and summative purposes”. Indeed they also encourage researchers to use a common set of tools when assessing outcomes related to EBHC.
Satisfaction with learning was only addressed in four studies. Learner satisfaction is linked to learner motivation and drive and is thus an important factor to consider when developing EBHC modules. Our results were not conclusive regarding preferences of participants. In two studies, focus group discussions were held with some of the participants and reported on the results as part of the article (Ilic et al., 2013; Ilic et al., 2015), while two other studies (Bradley et al., 2005; Welch, Van Lunen, & Hankemeier, 2014) conducted qualitative interviews alongside the respective quantitative investigation, but published on these results in separate articles. Bradley and colleagues (2005) explored the experiences of students and tutors regarding directed and self-directed learning, but included data from 40% of students that did not participate in the trial. Welch and colleagues explored the perceived effectiveness of the e-learning module, but only included participants from the experimental group in the interviews (Welch, Van Lunen, Hankemeier, et al., 2014).
Attrition rates were high for most studies, even though they were similar between groups for all comparisons. Attrition of learners poses a significant threat to sustainability of e-learning programmes, since initial enthusiasm to learn decreases over time, especially in qualified professionals, who have limited free time to spend on e-learning. The benefits of e-learning in terms of learning at one's own convenience, time and place can become a disadvantage, especially if it is not linked to assessment or a formal certificate.
The studies included in this review were mostly undertaken in high income countries, with only two studies conducted in LMICs. One study was conducted in the Philippines, while the other was a multisite RCT conducted in various LMICs. Problems with internet connectivity, availability of PCs and access to databases are important challenges that will need to be addressed when implementing e-learning programmes in these countries. The studies conducted in LMICs did not assess these factors, on the contrary, in Kulier et al. (2012) adequate access to computers and databases was a part of the eligibility criteria for participation.
5.3 QUALITY OF THE EVIDENCE
We included 13 individually randomised controlled trials, seven cluster RCTs and four non-RCTs. Most comparisons only comprised one or two studies. We summarised results for each comparison in Tables 12.1 to 12.6 and commented on limitations related to the analyses. We made judgements about risk of bias according to the EPOC criteria and made additional judgements on risk of bias for cluster RCTs. Overall, the risk of bias in included studies was moderate. Only eight of the 24 included trials were judged as having low risk of selection bias, having used adequate methods for both random sequence generation and allocation concealment. In addition, baseline characteristics were either not reported or showed significant differences between groups for seven of the included studies. Fourteen studies were judged as having high risk of attrition bias, since loss to follow-up rates were very high. When making judgements about blinding, we only considered blinding of outcome assessors (detection bias), since blinding of participants and personnel (performance bias) is usually not possible for educational interventions. Three studies were judged as having high risk of detection bias, while ten studies did not report on blinding and were judged as having unclear risk of detection bias. We were unable to make a judgement regarding contamination for most individually randomised trials, since authors did not report how contamination was avoided. Of the cluster RCTs, two trials did not adjust results for clustering, limiting their compatibility with individually randomised trials. One study was judged as having high risk of recruitment bias, since participants were recruited after randomisation of clusters.
These limitations in quantity and quality of the evidence need to be taken into consideration when interpreting results.
5.4 LIMITATIONS AND POTENTIAL BIASES IN THE REVIEW PROCESS
We attempted to minimize bias in the review process. We conducted a comprehensive search across multiple medical and educational databases and did not apply any limits with regards to language or publication status. Two authors independently screened search results, selected studies for inclusion, extracted data and made risk of bias assessments. We also contacted authors in an attempt to obtain missing data. We were unable to produce funnel plots to assess reporting bias, since we did not include more than 10 studies per outcome in the meta-analysis.
The main limitation of our review is that we were unable to address our secondary objectives, because our included studies provided insufficient information on educational context and implementation strategies. In addition, we were unable to perform planned subgroup analysis on the effects of specific dimensions of e-learning. This was due to inadequate reporting of the included interventions and the small number of included trials per comparison. Phillips et al. (2016) recently published a guideline for reporting evidence-based practice educational interventions and teaching (GREET), in which they highlight the need to report details of the intervention. These include describing the educational theories or approaches, the learning objectives and EBHC content, learning materials and educational strategies, modes of delivery and educational environment. Indeed, we planned to extract data related to all these issues, but found that interventions were generally poorly described.
5.5 AGREEMENTS AND DISAGREEMENTS WITH OTHER STUDIES OR REVIEWS
EBHC e-learning is embedded in two domains, namely teaching EBHC and e-learning.
In terms of teaching EBHC, the findings of our review echo the results of an overview of systematic reviews on the effectiveness of EBHC teaching and learning, which included 16 systematic reviews (Young et al., 2014). This review recommends that teaching and learning strategies should be multi-faceted and clinically integrated and that they should incorporate assessment. We found that effective EBHC e-learning interventions were multi-faceted, contained interactive components and were integrated into clinical practice. Blended learning appeared to be more effective than pure e-learning.
The systematic review by Ilic & Maloney (2014) that aimed to determine which types of educational methods were most effective in increasing EBHC knowledge and skills included four of the studies included in our review (Bradley et al., 2005; Davis et al., 2007; Davis et al., 2008; Schilling et al., 2006) but compared a variety of educational methods (e.g. lectures, workshops, small group learning, problem-based learning, online learning, computer-assisted learning) and did not focus on e-learning compared to other types of learning. They found no difference in knowledge and skills between various educational methods.
In terms of e-learning, our review is also in accordance with the results of other relevant studies. When comparing e-learning (pure e-learning or blended learning) to no learning, our results were similar to those of other systematic reviews, favoring pure e-learning for knowledge and skills (Al-Shorbaji et al., 2015; Cook et al., 2008; Liu et al., 2016) and blended learning for EBHC behaviour (Sinclair et al., 2016).
When comparing e-learning (pure e-learning and blended learning) to other methods of learning (face-to-face learning or pure e-learning), our results were similar to those from other systematic reviews for pure e-learning compared to face-to-face learning, showing no difference in EBHC knowledge, skills, attitude (Al-Shorbaji et al., 2015; Cook et al., 2008; Liu et al., 2016) and behaviour (Sinclair et al., 2016). Our results favoured blended learning for EBHC attitude and behaviour when compared to face-to-face learning, and for EBHC knowledge when compared to pure e-learning.
6 Authors’ conclusions
6.1 IMPLICATIONS FOR PRACTICE AND POLICY
Our findings suggest that e-learning of EBHC, whether pure or blended, compared to no learning, improves EBHC knowledge and skills. We did not find a difference in these outcomes when comparing e-learning to face-to-face learning, suggesting that both methods of learning can be beneficial. It appears that blended learning, which typically comprises multiple intervention components, could be more effective than other types of learning in improving EBHC knowledge, skills, attitude and behaviour.
These findings need to be considered in light of the limited number of studies per outcome in each comparison, risk of bias across studies and heterogeneous interventions, as well as inconsistent and imprecise results.
Importantly, e-learning as such is not a panacea and the principles that apply to EBHC teaching in general (e.g. interactive, clinically integrated teaching) should be considered when developing e-learning training initiatives. Other factors such as resources, feasibility and preference of learners need to be taken into consideration when planning EBHC learning activities.
6.2 IMPLICATIONS FOR RESEARCH
Future research on EBHC e-learning should focus on the effectiveness of various e-learning components and should aim to identify a combination of minimum components for effective e-learning. Interventions should be based on suitable learning theories, and explicitly reported. In addition, studies should evaluate the educational context as part of the intervention, explore learners’ experience with learning and include outcomes related to short- and long term EBHC behaviour and cost of the intervention. Comprehensive reporting of these aspects in primary studies will be critical, if an updated systematic review is to provide more in-depth insights. There is a need to conduct studies on e-learning in LMICs in order to address the challenges unique to these settings.
Footnotes
8 Information about this review
9 Tables
10 Figures
Return to text
11 Data and analyses
Abbreviations related to type of healthcare professionals and level of education: AT: Athletic trainers CPD: Continuing Professional Development M: Medical doctors MIX: Mix of various healthcare professionals at different levels of education N: Nurses PG: Postgraduate PT: Physiotherapists UG: Undergraduate
11.1 PURE E-LEARNING VS NO LEARNING
11.2 BLENDED LEARNING VS NO LEARNING
11.3 PURE E-LEARNING VS FACE-TO-FACE LEARNING
11.4 BLENDED LEARNINGVS FACE-TO-FACE LEARNING
11.5 BLENDED LEARNING VS PURE E-LEARNING
11.6 PURE E-LEARNINGVS PURE E-LEARNING
12 Summary of findings
Abbreviations:
CPD: Continuing professional development
UG: Undergraduate
PG: Postgraduate