
Abstract
This Campbell Systematic Review examines the effectiveness of different approaches for promoting handwashing and sanitation behaviour change, and factors affecting implementation, in low and middle-income countries. The review summarises evidence from 42 impact evaluations, and from 28 qualitative studies.
Community-based approaches which include a sanitation component can increase handwashing with soap at key times; use of latrines and safe disposal of faeces; and reduce the frequency of open defecation. Social marketing seems less effective. The approach mainly shows an effect on sanitation outcomes when interventions combine handwashing and sanitation components.
Sanitation and hygiene messaging with a focus on handwashing with soap has an effect after the intervention has ended, but there is little impact on sanitation outcomes. However, these effects are not sustainable in the long term. Using elements of psychosocial theory in a small-scale handwashing promotion intervention, or adding theory-based elements such as infrastructure promotion or public commitment to an existing promotional approach, seem promising for handwashing with soap.
None of the approaches described have consistent effects on behavioural factors such as knowledge, skills and attitude. There are no consistent effects on health.
Plain language summary
Community-based approaches are most effective in promoting changes in hygiene practices, but sustainability is a challenge
Community-based approaches to promote handwashing and sanitation efforts seem to work better than social marketing, messaging and interventions based on psychosocial theory. Programs combining hygiene and sanitation measures appears to have a larger impact than either one alone.
What is this review about?
Diarrhoeal diseases are very common causes of death in low and middle-income countries. Improved sanitation and hygiene reduce diarrhoea, but adoption remains a challenge.
This review assesses the evidence for two questions: (1) how effective are different approaches to promote handwashing and sanitation behaviour change; and (2) what factors influence the implementation of these approaches?
What is the aim of this review?
This Campbell Systematic Review examines the effectiveness of different approaches for promoting handwashing and sanitation behaviour change, and factors affecting implementation, in low and middle-income countries. The review summarises evidence from 42 impact evaluations, and from 28 qualitative studies.
What studies are included?
Studies of effectiveness had to be impact evaluations using an experimental or quasi-experimental design and analytical observational studies. Implementation studies used qualitative designs.
Forty-two quantitative studies and 28 qualitative studies met the inclusion criteria. The quantitative studies were conducted in LMICs worldwide, with the majority of the studies in South Asia and Sub-Saharan Africa.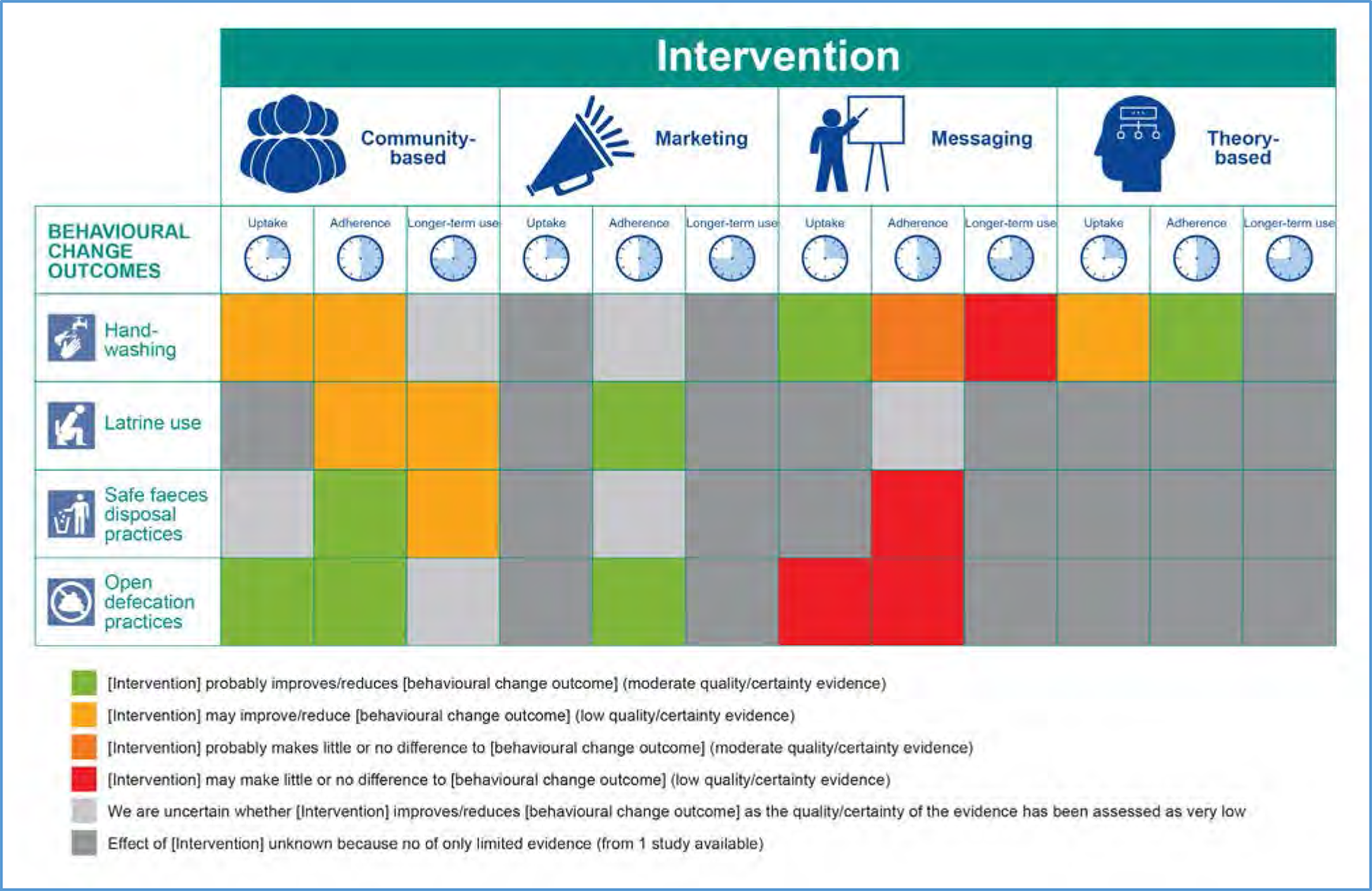
What are the main findings of this review?
None of the approaches described have consistent effects on behavioural factors such as knowledge, skills and attitude. There are no consistent effects on health.
What factors affect implementation?
Implementation is affected by length of the intervention; visit frequency; use of short communication messages; availability of training materials; kindness, respect, status and accessibility of the implementer; recipient awareness about costs and benefits and their access to infrastructure and social capital.
For
For
What do the findings of this review mean?
Promotional approaches aimed at handwashing and sanitation behaviour change can be effective in terms of handwashing with soap, latrine use, safe faeces disposal and open defecation. A combination of different promotional elements is probably the most effective strategy. Identifying and tackling the different barriers and facilitators that influence the implementation of these promotional approaches can increase effectiveness.
An important implication for research is that there is a need for a more uniform method of measuring and reporting on handwashing, latrine use, safe faeces disposal, and open defecation.
How up-to-date is this review?
The review authors searched for studies published until March 2016; this Campbell Systematic Review was published in May 2017.
Executive summary/Abstract
BACKGROUND
Water and sanitation are at the very core of sustainable development, critical to the survival of people and the planet. The Sustainable Development Goal 6 (i.e. ‘ensure availability and sustainable management of water and sanitation for all’) addresses the issues relating to drinking water, sanitation and hygiene. It is unclear which Water, Sanitation and Hygiene (WASH) promotional approach is the most effective for sanitation and hygiene behaviour change, and other outcomes leading to behaviour change (e.g. learning outcomes) or longer term outcomes that follow from behaviour change (e.g. mortality, morbidity).
OBJECTIVES
The overall goal of this systematic review is to show which promotional approaches are effective in changing handwashing and sanitation behaviour, and which implementation factors affect the success or failure of such interventions. This goal is achieved by answering two different review questions.
SEARCH METHODS
A comprehensive search was conducted to identify both published and unpublished studies. Using a sensitive search strategy, we searched the following databases from 1980 to March 2016: Medline (PubMed), Cochrane CENTRAL Issue 2, Applied Social Sciences index and abstracts (ASSIA, ProQuest), Global Health (CABI), EMBASE (OVID), PsycInfo (EBSCOHost), ERIC (EBSCOHost), Global Index Medicus, 3ie Impact Evaluation Database, International bibliography of the Social Sciences (IBSS, ProQuest), Sociological abstracts (ProQuest) and Social Sciences citation index (SSCI, Web of Science). To find unpublished material and relevant programme documents, we contacted various research groups and organizations and/or checked the relevant websites.
SELECTION CRITERIA
Participants included both children and adults from low- and middle-income countries (LMICs), as defined by the World Bank, at the time the intervention was implemented. Studies performed at an individual, household, school or community level were included, whereas studies conducted in institutional settings (e.g. hospitals) were excluded. The following promotional approaches or elements to promote handwashing, latrine use, safe faeces disposal, and to discourage open defecation (primary outcomes), were included: community-based approaches, social marketing approaches, sanitation and hygiene messaging and elements of psychosocial theory. Secondary outcomes of interest were behavioural factors (knowledge, skills, attitude, norms, self-regulation) and health outcomes (morbidity, mortality).
For
DATA COLLECTION AND ANALYSIS
Study selection and data extraction (including risk of bias assessment) were performed independently by two reviewers, using EPPI-Reviewer software. Study authors of all included papers were contacted by email (in July 2016) to ask for any relevant information, related to the population, intervention or outcomes, that was missing or not reported in the paper. Any disagreements between the two data extractors were resolved through discussion, or by consulting another review co-author. The GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach was used to assess the overall quality/certainty of evidence from quantitative studies included in this review. The qualitative studies were assessed using the CASP (Critical Appraisal Skills Program) checklist. Evidence relating to Question 1 (effectiveness of promotional approaches) was synthesized in a quantitative way (meta-analysis), where possible.
RESULTS
Forty-two quantitative studies and 28 qualitative studies met the inclusion criteria. The quantitative studies were conducted in LMICs worldwide, with the majority of the studies in South Asia and Sub-Saharan Africa. Most quantitative studies (69%) were performed in a rural setting and only 14% of the studies took place in an urban setting (with an additional 10% in an “informal-rural setting”). The effect of a promotional approach versus not using a promotional approach on sanitation and handwashing behaviour change, behavioural factors (knowledge, skills, attitude, norms and self-regulation) and health-related outcomes (morbidity and mortality), was studied in 34 different studies. In addition, 7 studies compared specific promotional approaches versus other promotional approaches, and one study compared two different communication strategies. All studies showed substantial variability in programme content, study types, outcome types, methods of outcome measurement and timing of measurement.
Risk of bias assessments of included studies were influenced by unclear reporting or lack of reporting of key methodological aspects of the study design and process. Five percent of the experimental studies (n=2) had a high risk of selection bias, 40% had a high risk of detection bias (n=17), 28% had a high risk of attrition bias (n=12) and 48% had a high risk of reporting bias (n=20). Most quasi-experimental and observational studies had bias in the selection of participants, some were at high risk of confounding, methods of outcome assessment were not comparable across intervention groups, and outcome assessors were aware of the interventions that the groups received. For the body of evidence, in most assessments, the certainty of evidence was considered as ‘low’ and in some cases ‘moderate’ or ‘very low’. For the qualitative studies, an overall CASP score was given to the studies, and only 21% of the studies had a score less than 8/10. In studies with a lower score the relationship between researcher and participants was not adequately considered or ethical issues were not explicitly reported.
We categorised the studies into 4 categories of promotional approaches or elements:
(1)
(2)
(3)
(4)
The most consistent results were obtained within the category of
The use of
Using
Finally, the methods used for communicating the content of a certain promotional approach, also play a role, and use of interpersonal communication was shown to be effective in certain circumstances.
We only found a limited number of studies that incorporated a range of incentives (from soap bars to food or subsidies) into the promotional approach. One study reported promising results when using subsidies as part of the community-based approach, but more research on the use of subsidies and incentives would be valuable.
None of the promotional approaches described in the review showed consistent effects on behavioural factors such as knowledge, skills and attitude. Also no consistent effects on health were demonstrated.
Facilitators which were relevant across different promotional approaches were: length of the approach, visit frequency, using short communication messages, availability of training materials, funding/resources and partnerships, kindness and respect of the implementer, accessibility of the implementer, and the implementer's authority/status; as well as, on the side of the recipient, awareness about costs and benefits, social capital, access to infrastructure and availability of space, and others showing the behaviour.
AUTHORS’ CONCLUSIONS
1 Background
1.1 THE PROBLEM, CONDITION OR ISSUE
Diarrhoeal diseases are the second highest cause of death in low income countries and the fifth highest cause of death in the world (WHO, 2011). In an update of the Global Burden of Disease study it was shown that unsafe water, sanitation and handwashing caused nearly 5% of DALYs (Disability-Adjusted Life Years) for males and females in poor communities (GBD Risk Factor Collaborators, 2015).
Water, Sanitation and Hygiene (WASH) interventions consist of (1) water supply (water quantity) and water treatment (water quality), including operation and maintenance of the water source (“Water”), (2) latrine construction, latrine use, latrine hygiene, faeces disposal practices, discouraging the practice of open defecation, disposal of solid waste and wastewater, and vector control (“Sanitation”), and (3) promotional activities around personal hygiene (e.g. handwashing, facial washing, showering/bathing practices, menstrual hygiene) and domestic hygiene (“Hygiene”) (DFID, 2013). The actual construction of WASH interventions, such as construction of a water source or latrine, is called the “hardware” element of the intervention. On the other hand, implementation of participatory approaches to promote safe hygiene practices, establish community-based management systems for the WASH facilities, create up-front demand and encourage community participation and ownership is called the “software” element of the intervention (Peal et al., 2010). The latter is particularly important to ensure long term sustainability of behaviours and technical durability of facilities since it was shown that the impact of WASH interventions on the burden of disease falls over time (Cairncross et al., 2010; Waddington et al., 2009).
One of the targets of the Millennium Development Goals was to halve the number of people without sustainable access to safe water and sanitation by 2015. In 2012 it was published that the target for water supply had been met, however, 780 million people still do not have access to safe water, with rural populations having five times less access than urban populations. The target for sanitation has not been met at all, and it is estimated that 2.5 billion people have no access to improved sanitation, with Sub-Saharan Africa having 30% access and South Asia having 41% access. Moreover, 1.1 billion people still practice open defecation (WHO/UNICEF, 2010; DFID, 2013).
1.2 THE INTERVENTION
1.2.1 Approaches to promote behaviour change
To improve effectiveness of WASH interventions, increasing attention is currently being focused on the design of programmes and the selection of approaches to promote WASH behaviour change. Several approaches have been developed over the last two decades, and are currently being applied in practice to promote uptake of WASH interventions and to achieve WASH behaviour change (Peal et al., 2010). The approaches can be grouped in the following categories:
Any combination of the promotional approaches or promotional elements mentioned above (Multichannel approach).
A promotional approach can contain different promotional elements, depending on the context for which the programme was developed. Based on the main focus or major element of the promotional approach, we classified the promotional approaches/promotional elements for the purpose of this review in 4 groups: community-based approaches, social marketing approaches, sanitation and hygiene messaging, and elements of psychosocial theory (detailed explanation below).
Any of the approaches above can be delivered using one or more different communication strategies: Interpersonal communication: peer to peer, home visits, focus group; either of these approaches could work with change/transformation agents such as hygiene promotors, WASH Committees, champions/natural leaders who are not part of community leadership system, community leaders (chefs, elected village/ appointed village leaders, councillors, etc.), religious leaders, teachers, Village Health Workers, Local Government Staff (dealing with WASH, Social Services, Health, etc.), volunteers (e.g. Red Cross volunteers), lecture, workshops, games, material provision with demonstration, quiz. Mass media communication: poster, TV, radio spot, radio programme, billboards, newspapers, outdoor/transit advertising, megaphones, hygiene day, stickers, paintings. Traditional communication: songs, folk drama and theatre, concerts, rallies, parades, cinema show.
It is not always clear which of these approaches is the most effective in relation to sanitation and hygiene behaviour change, and other outcomes leading to behaviour change (e.g. learning outcomes) or longer term outcomes that follow from behaviour change (e.g. mortality, morbidity). In the WASH sector, the evaluation of programmes tends to focus on intended outcomes and impacts (whether the intervention worked and what effect it had on outcomes) but not on appraising the process of implementation and establishing how the use of a specific approach leads to changes in outcomes. However, decision makers need to know the critical factors in the process of implementation that ensure that impacts are achieved and sustained, and how scaling up is best achieved.
For the purpose of this review we focused on approaches to promote handwashing and sanitation interventions, with behaviour change as the main outcome. To be able to make this choice we developed a review of existing systematic reviews (see below, 1.4). Since adherence to water, sanitation and hygiene programmes is known to be highly associated with factors such as gender, socioeconomic status, education and occupation, equity factors are also considered in this systematic review (DFID, 2013). Since the effect of WASH interventions on health outcomes (such as diarrhoea, cholera, trachoma, helminth infections) has been shown in many existing individual studies and systematic reviews (Cairncross et al., 2010; Dangour et al., 2013; Fewtrell et al., 2005; Peletz et al., 2013; Stocks et al., 2014; Strunz et al., 2014; Taylor et al., 2015; Waddington, 2009), and practicing/showing the right behaviour is a pre-requisite for health impacts, health outcomes are also looked at in those studies that measured behaviour change. Although it would be relevant to include studies that measured cost-effectiveness, this is outside the review scope.
1.2.2 Definitions
In the context of this review, we used the following definitions:
1.3 HOW THE INTERVENTION MIGHT WORK
We have built a theory of change (ToC) framework illustrating the hypothesized causal links, explaining how (elements of) handwashing and sanitation promotional approaches are expected to lead to the intended short-term, intermediate and longer-term outcomes, and how different factors could influence the implementation of the promotional approaches (see Figure 1). The following sources were used to inform the ToC: a systematic review of WASH behavioural models (Dreibelbis et al., 2013), 6 systematic reviews that were included in the scoping phase (overview of existing systematic reviews, see below), the PROGRESS framework (O'Neill et al., 2014), the Checklist for implementation (“Ch-IMP”) (Cargo et al., 2015), and the SURE framework (The SURE Collaboration, 2011). We also incorporated the input of our team and Advisory Group members. A more detailed list of the different sources of information is provided in Appendix 1. In addition, a more detailed description of how stakeholder engagement resulted in an improved version of the ToC will be published in a separate peer-reviewed publication.
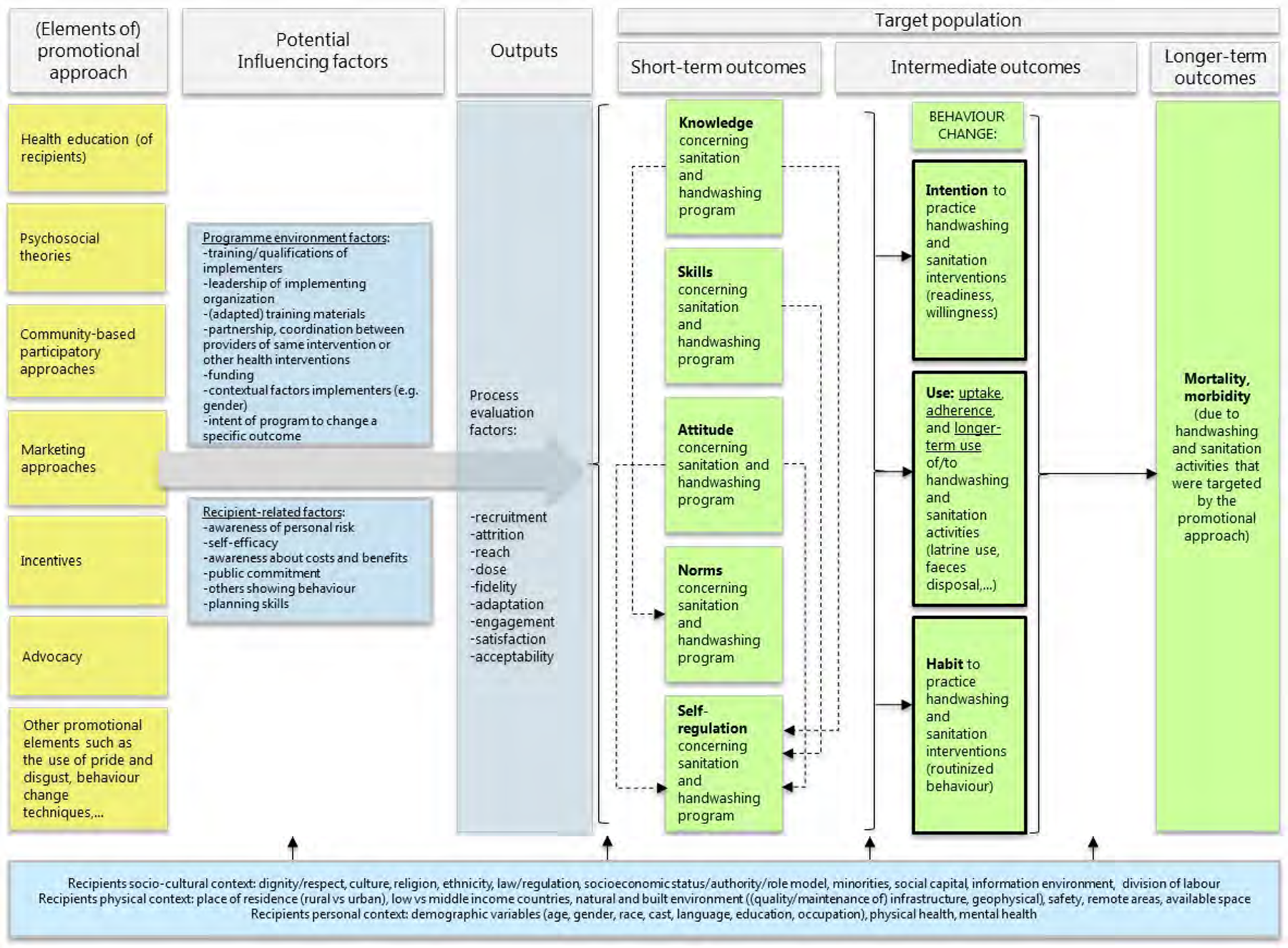
Initial theory of change framework concerning the effect of promotional approaches intended to improve handwashing and sanitation behavioural factors (short-term outcomes), handwashing and sanitation behaviour change (intermediate outcomes) and reduce morbidity and mortality (longer-term outcomes)
The ToC contains 6 different (elements of) promotional approaches aimed at inducing handwashing and sanitation behaviour change. Furthermore, it contains (1) short-term outcomes, consisting of 5 “behavioural factors” (knowledge, skills and attitude, norms, self-regulation), (2) intermediate outcomes, consisting of the different elements that compose “behaviour change”: intention, use and habit, and (3) longer term outcomes, including health outcomes such as mortality and morbidity due to agents with faecal-oral transmission. Health outcomes were included since these are the final intended outcomes for which behaviour change is a pre-requisite. However, data on health outcomes were only included from studies that also report behavioural outcomes, which ensures that these outcomes are linked (and considering confounding factors such as other causes of morbidity or mortality). The “behaviour change” outcomes are the primary outcomes in this review, while the other outcomes are included as secondary outcomes. These outcomes were measured in quantitative research.
In addition to the “core structure” of the ToC, three types of factors that are able to influence the implementation of the promotional approaches were added to the model: (1) programme environment factors and recipient-related moderators, (2) process evaluation factors (such as recruitment, attrition, reach, dose, fidelity, adaptation, engagement, satisfaction and acceptability), and (3) recipient-related contextual factors (including socio-cultural, physical and personal contextual factors of the recipients). These factors were looked at in qualitative studies. An example of such factors are equity factors such as gender.
1.4 WHY IT IS IMPORTANT TO DO THE REVIEW
1.4.1 Key debates in current policy
As part of its 2030 Agenda, the United Nations (UN) set as Goal 6 of the 17 Sustainable Development Goals (SDGs) the ambition to “Ensure access to water and sanitation for all”, including the target to “achieve access to adequate and equitable sanitation and hygiene for all and end open defecation, paying special attention to the needs of women and girls and those in vulnerable situations.” The importance of influencing behavior in order to achieve these goals is widely recognized.
In the eighties and nineties health promotion was based mainly on cognitive psychology (Aunger and Curtis, 2015). Behavior change policies in the WASH sector were predominantly influenced by different theory models such as the ‘Health Belief Model’ or ‘Theory of planned behavior’ among others (Rosenstock, 1974). When translated into policies, these theories shared a major commonality in assuming that people make rational decisions about protecting their health based on knowledge, skills and facilities. This is the era of participatory methodologies like PHAST 1 (Participatory Hygiene and Sanitation Transformation) which aimed at increasing collective understanding about health risks and promoting preventive actions. This is also the time of extensive health and/or hygiene campaigns which would aim at educating the public by raising awareness and public understanding about risk behavior.
With the spread of social marketing theories in the early 2000's, the ‘education campaign’ approach in WASH policies have shifted into new emerging approaches such as Communication for Behavioral Impact (COMBI) 2 or Change for Development (C4D) 3 . The incorporation of social marketing principles in behavior change approaches has led to the massive production of Information, Education and Communication (IEC) materials, often without considering the relevance of these materials to the desired behavioral outcome. Little attention was given on how to sustain these campaign approaches within targeted populations.
The last 10 years new developments on behavior change models were introduced, with emphasis on non-cognitive models and psychosocial theory, shaping again policies and resulting in approaches such as the current widely spread ‘Community Led Total Sanitation’ (CLTS) 4 or ‘Behaviour Centered Design’ 5 . This new vision emphasized the importance of attitudes and beliefs that influence certain behavior and social choices that shape what people think. Many variations of these approaches currently exist and it is still questionable if there is any added value of subsidies or incentives to this type of behaviour change approaches.
In summary, different behavioral theories and models have informed (and still inform) policy makers, donors and implementers about the issues to consider and the likely success of initiatives and interventions. Despite the efforts by the WASH sector in developing approaches to influence WASH behaviors, there still is no guidance on which are the most succesful techniques.
1.4.2 Overview of existing systematic reviews
In a first scoping phase (September 2015 – January 2016) an extensive overview of
We identified systematic reviews on the following WASH interventions : water quality (Fiebelkorn et al., 2012), hygiene hand sanitizers (Mah et al., 2008; Ejemot-Nwadiaro et al., 2015) and multiple WASH interventions (water, sanitation, hygiene) (Evans et al., 2014; Hulland et al., 2015;Joshi & Amadi, 2013). No systematic review focused on water supply or sanitation promotion programmes only.
The (multiple) WASH interventions were promoted using different approaches as follows: via social marketing principles (Mah et al., 2008; Evans et al., 2014), via community-led total sanitation (Hulland et al., 2015), via educational and/or communication channels (Ejemot-Nwadiaro et al., 2015; Hulland et al., 2015; Joshi & Amadi, 2013) or via multiple promotional approaches (community mobilization, health education, motivational interviewing, role modeling, and social marketing: Fiebelkorn et al., 2012). No systematic reviews on the use of financial incentives or other approaches to promote WASH interventions were found.
There was a paucity of information on promotional approaches of interventions in the systematic reviews, which prevented us from making any further conclusions. Population heterogeneity, type of intervention and outcome measurement were some of the reasons why meta-analyses were not performed in systematic reviews.
Only one systematic review reported data on implementation factors that could influence WASH behaviour (sustained adoption) (Hulland et al., 2015). Systematic reviews concerning other factors influencing implementation were not identified. Evidence from the systematic review by Hulland et al. (2015) suggests that the most influential programme factors associated with sustained adoption include frequent, personal contact with a health promoter over a period. While the Hulland review investigated factors that affect sustained adoption of WASH technologies (e.g. promotion via frequent, personal contact), this review focuses on factors that influence the implementation of approaches to promote WASH behaviour (e.g. culture as a barrier to use a financial incentive).
More details on the methodology used in this scoping phase can be found in Appendix 2, and detailed information about the methodology, results, and conclusions will be published in a separate peer-reviewed publication.
Based on our scoping review, we concluded that in the context of our two research questions, there is still an evidence gap. For example, no systematic collection of evidence is available regarding specific promotional approaches (e.g.community-based approaches) or specific WASH components (e.g. sanitation), in relation to behaviour change as an outcome. In addition, systematic reviews lack qualitative information about factors that can influence implementation of WASH promotional approaches. Therefore, we concluded that the systematic collection, extraction and analysis of qualitative/quantitative data on the effectiveness of promotional approaches aiming to promote handwashing and sanitation behaviour change outcomes was relevant and timely.
The objective of this systematic review is to identify promotional elements and those factors in the implementation process that influence behaviour change. This study objective is answered by a mixed-methods systematic review: findings from quantitative studies that identify effective promotional approaches (quantitative arm) were enriched with insights from qualitative studies that explore factors that hinder or facilitate the implementation of these promotional approaches (qualitative arm), focusing on people's lived experiences and perceptions. The findings of this review will provide guidance to governments and international bodies in selecting promotion strategies that positively influence behaviour change.
2 Objectives
This review is a “Mixed methods research synthesis”, consisting of a strand of quantitative, and a strand of qualitative evidence. In this way, we aim not only to answer the question “what works”, but we will also inform policy makers on “why, for whom, and under which circumstances,” a programme will work.
The overall goal for this systematic review is to show which promotional approaches are effective to change handwashing and sanitation behaviour, and which implementation factors affect the success or failure of such an intervention.
This goal is achieved by answering two different review questions, in a quantitative and qualitative arm of the review:
3 Methods
The protocol for this review was published in the Campbell Library on 2 May 2016 (De Buck et al. 2016). For reasons of completeness, the majority of the information in the protocol is included in the Methods section below. Deviations from the initial protocol are described in paragraph 3.5.
3.1 MIXED METHODS RESEARCH SYNTHESIS DESIGN (MMRS)
A segregated concurrent type of MMRS design was used for this review (Heyvaert et al., 2016). In this type of design, the quantitative and qualitative studies are analyzed separately (Figure 2).
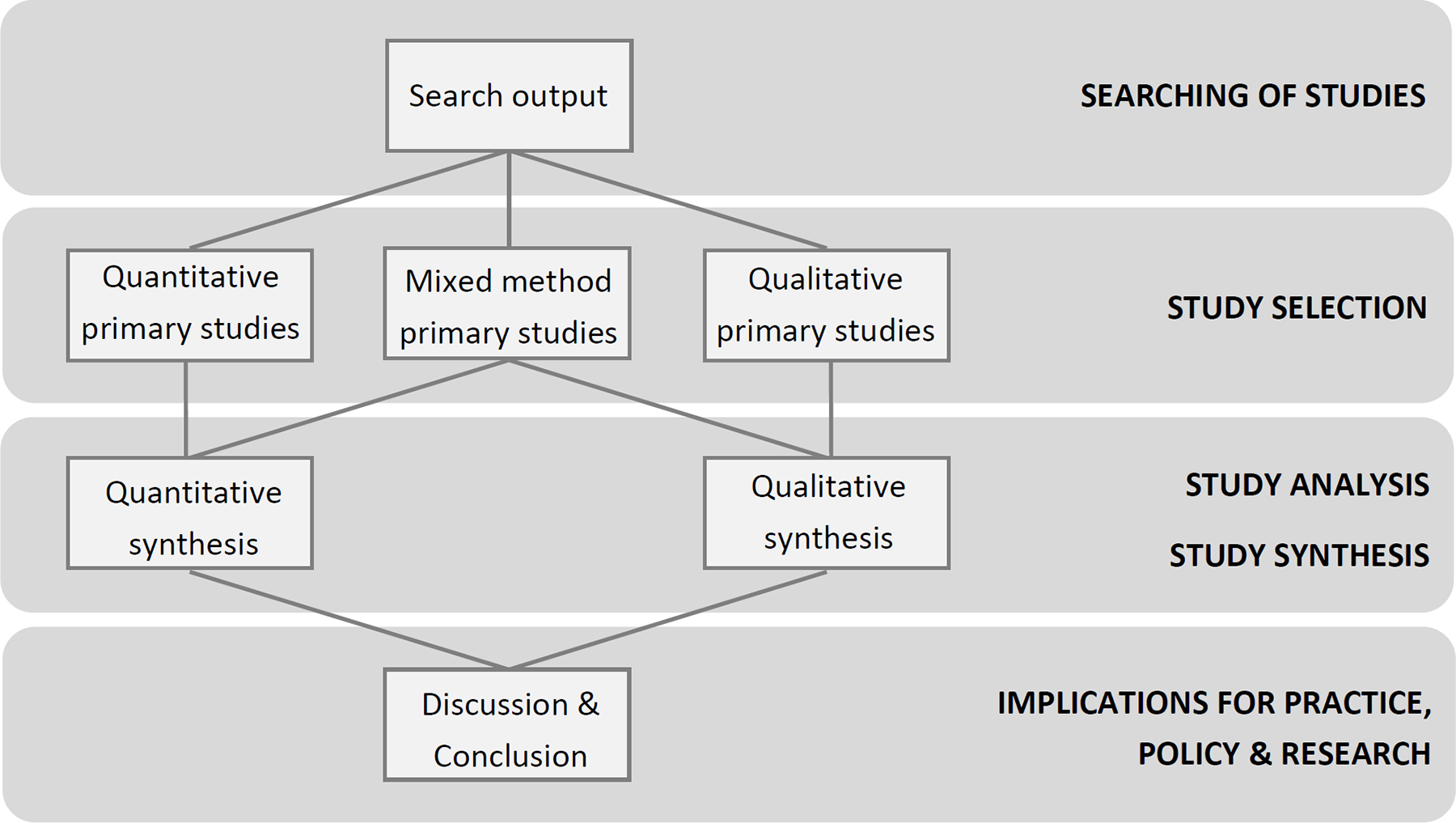
Schematic overview of the segregated concurrent type of Mixed Methods Research Synthesis design that is used in this review
We used a comprehensive search to identify relevant literature. Quantitative and qualitative study designs were separated in the screening phase. Primary mixed method studies (i.e. studies answering both Research Question 1 and 2) were considered for inclusion when quantitative and qualitative results/findings could be separated. Design specific critical appraisal instruments were used to assess the quality of each study type. Quantitative evidence was analysed using statistical pooling techniques (if possible). The qualitative evidence was synthesized using a “Best fit framework synthesis” approach (Booth & Carroll, 2015; Carroll, 2013).
The analysis of both strands of evidence feeds into an overall discussion and conclusion section.
3.2 CRITERIA FOR CONSIDERING STUDIES FOR THIS REVIEW
3.2.1 Types of studies
The type of study design is different for the quantitative and qualitative component of the review.
To answer Impact evaluations using an experimental design (Randomised Controlled Trials (RCTs) with assignment at individual or household/community (cluster) level; Quasi-randomised controlled trials, using a quasi-random method of allocation (e.g. alternation)) Impact evaluations using a quasi-experimental design (non-randomised controlled studies (e.g. self-selection of participants), taking into account confounding variables at the design or analysis stage) Observational analytic studies such as cohort studies and case-control studies.
Quasi-experimental and observational analytic studies were included since these were prevalent in the WASH literature, because randomised assignment is not always feasible or ethical.
Uncontrolled studies, case series, research methodology reports/manuscripts, editorials and economic analyses were excluded.
To answer
3.2.2 Types of participants
Participants included both children and adults from low- and middle-income countries (LMIC), as defined by the World Bank, at the time the intervention was conducted. Studies performed at an individual, household, school or community level were included, whereas studies conducted in institutional settings (e.g. hospitals) were excluded.
3.2.3 Types of interventions
Programmes conducted to promote uptake and use of handwashing, and the following sanitation interventions were included: latrine/toilet use, safe faeces disposal practices, and discouraging the practice of open defecation. Any combination of the interventions listed above were included. The following programmes were excluded: programmes conducted to promote water treatment, water supply for drinking only, menstrual hygiene, food hygiene, animal waste disposal, facial cleansing. Any combination of the interventions listed above with water treatment, drinking water supply or other hygiene interventions were included if individual outcomes, as listed below, were present.
The programme contained a direct promotional approach related to one of the following categories: community-based approaches, social marketing approaches, sanitation and hygiene messaging, elements of psychosocial theory, incentives, advocacy, or any combination of the promotional approaches or promotional elements mentioned above (multichannel approach) (details on these approaches can be found in paragraph 1.2.1).
Programmes using no promotional approaches were excluded.
3.2.4 Comparison
For
3.2.5 Types of outcome/evaluation measures
To answer
Primary outcomes
The primary outcome is behaviour change, operationalized in the following way: (a)
Secondary outcomes
The secondary outcomes are: behavioural factors (knowledge, skills, attitude, norms, and self-regulation concerning the practice of handwashing and sanitation interventions); morbidity and mortality due to agents associated with faecal-oral transmission. Indirect outcomes, such as “pupil absence”, were not considered. Symptom-based health outcomes, such as cough, general illness, fever and congestions were not included. Studies reporting data on morbidity and mortality were only included if data on primary outcomes (behaviour change) were also available. Studies reporting only behavioural factors, and no primary outcomes, were included. We included outcomes that were measured via direct observation/demonstration (where a participant is asked to show how a behaviour is practiced), as well as self-reported, parent-reported or teacher-reported outcomes. To answer the
3.2.6 Duration of follow-up
No restrictions in timing of outcome measurement were used. Outcomes measured during the implementation of the programme were categorised as “uptake”, outcomes measured within 12 months after the programme implementation were categorised as “adherence”, and outcomes measured >12 months after the end of the programme implementation were categorised as “longer-term” outcomes.
3.2.7 Language
No language restrictions were used.
3.2.8 Publication date
Studies from 1980 to March 2016 were included. This date is based on the introduction of the Millennium Development Goals in 1990 (MDG7: “To ensure access to drinking water and sanitation for all”), which was followed by the development of evidence-based interventions for hygiene promotion (DFID, 2013). We also checked the publication dates of the included studies in the identified systematic reviews (scoping phase), but since one study was published in 1985, we chose 1980 as cut-off date (Stanton & Clemens, 1985).
3.3 SEARCH METHODS FOR IDENTIFICATION OF STUDIES
Searching for studies was done according to the principles stated by Hammerstrøm et al. (2010). One search strategy per database was developed to search for quantitative and qualitative studies.
3.3.1 Electronic databases
We searched the following databases from 1980 to March 2016: 3ie Impact Evaluation Database Applied Social Sciences Index and Abstracts (ASSIA, ProQuest) Cochrane CENTRAL issue 2 of 12, February 2016 EMBASE (OVID) ERIC (EBSCOHost) Global Health (CABI) Global Index Medicus International bibliography of the Social Sciences (IBSS, ProQuest) MEDLINE (PubMed) PsycINFO (EBSCOHost) Social Sciences Citation Index (SSCI, Web of Science) Sociological Abstracts (ProQuest)
A sensitive search strategy based on existing search strategies from existing WASH systematic reviews, our ToC and our selection criteria, was developed by an information specialist and tested in an iterative way for each database separately. A combination of index terms (where relevant) and free text words (in title/abstract) was used, with attention to possible synonyms and words used in key papers. De-duplication of the references was done by the information specialist using Reference Manager 12. All searches, search dates, and number of references found per database are documented in Appendix 3 (search strategies) and 4 (search report).
3.3.2 Searching other resources (grey literature)
To find unpublished material and relevant programme documents, we contacted the following research groups and organizations and/or checked the following websites (March 2016): CLTS Foundation (www.cltsfoundation.org) Development Media International (DMI) (http://www.developmentmedia.net/) Government of India website (https://India.gov.in) iDE Global WASH Initiative (http://www.ideorg.org/WhatWeDo/WASH.aspx) International Centre for Diarrhoeal Disease Research, Bangladesh (ICDDR,B) (http://www.icddrb.org/) International Water Centre – Australia (www.watercentre.org/) IRC International Water and Sanitation Centre (http://www.irc.nl/) Oxfam International (https://www.oxfam.org/en/tags/water-and-sanitation) R4D (Research for Development) UK DFID http://r4d.dfid.gov.uk/Default.aspx
SHARE (Sanitation and Hygiene Applied Research for Equity) consortium (www.SHAREresearch.org#sthash.DsqhxgDC.dpuf) Social Science Research Network Electronic Library Susana project database (http://www.susana.org/en/resources/projects) United Nations Children's Fund (UNICEF) (http://www.unicef.org.uk/) Water and Sanitation for the Urban Poor (WSUP) (http://www.wsup.com/) Water, Engineering and Development Centre, UK (www.lboro.ac.uk/wedc/) WaterAid (
www.wateraid.org/) WaterSHED (http://www.watershedasia.org/) WHO: Department of Child and Adolescent Health and Development (WHO) http://www.who.int/maternal_child_ adolescent/en/) Water, Sanitation and Health Program (WHO) (http://www.who.int/water_sanitation_health/en/) World Health Organization (WHO) (http://www.who.int/en/) World Bank: World Bank (http://www.worldbank.org/) World Bank Water and Sanitation Program (http://water.worldbank.org/related-topics/water-and-sanitation-program, http://water.worldbank.org/shw-resource-guide/promotion/hygiene-promotion-approaches)
This list of sources was based on the advice and network of our team members and Advisory Group members. Content experts (including the Advisory Group) were consulted for missing studies.
3.4 DATA COLLECTION AND ANALYSIS
Statistical support was provided by the statistician who is part of the review team.
3.4.1 Selection of studies
Study selection was performed independently and in parallel by two evidence reviewers, using EPPI-Reviewer software. In the first phase, titles and abstracts of the references identified during the search were scanned. Full text versions of relevant articles were retrieved, and references that met the selection criteria were included for further analysis. The references resulting from grey literature sources were screened, based on title and abstract, by only one reviewer. Full text assessment of the grey literature was done by 2 reviewers. Any discrepancies between the two reviewers were resolved by consensus, and in case of disagreement, a third reviewer was involved. A PRISMA study selection flowchart was developed (Moher et al., 2009), and a list of excluded studies with the reasons for exclusion was provided. References were labelled as “unavailable”, when it was not obtainable through the libraries of the institutions involved (Stellenbosch University (South Africa), KU Leuven (Belgium)).
3.4.2 Data extraction and management
Data extraction (including quality assessment) was performed by two reviewers independently.
3.4.3 Quality assessment of included studies and determination of certainty of evidence
3.4.4 Measures of treatment effect
Binary outcomes were used to calculate risk ratios (RR) (+ 95% confidence intervals (CI)). For continuous data, (weighted) mean differences (MD) (+ 95% CI) were calculated. We only used the (unadjusted/adjusted) effect measures calculated by the study authors in case the binary/continuous data were not available. If outcome measures were opposite to the intervention categories we defined (e.g. “no latrine use” instead of “latrine use”), binary data were reversed. This was indicated on the forest plots with an asterisk. Unit of analysis issues were carefully considered in order to adjust for the clustering effect (in case of cluster RCTs) and/or for multiple testing (in case of multi-arm trials). For cluster RCTs a cluster adjustment on the raw data (binary/continuous outcomes) was made. For the binary outcomes, the raw data (e.g. number of handwashing at key times events) were divided by the calculated design effect. For the continuous outcomes, the raw data (e.g. mean number of people washing their hands at key times) was multiplied by square root of the calculated design effect. The design effect was calculated by the formula: design effect = 1 + ((average cluster size -1) x ICC (intra-cluster correlation coefficient)), as detailed in the Cochrane Handbook of Systematic Reviews Chapter 16.3 (Higgins and Green, 2011). We used the ICC as reported by the original study. In cases where the ICC was not reported, we estimated the ICCs using the following strategy: within each category of promotional approaches we used the mean of the ICCs of studies for which an ICC was reported; in two categories of promotional approaches (i.e. sanitation and hygiene messaging and social marketing approach) none of the studies had reported ICCs, in which case the most conservative ICC value of the other categories was used. We calculated synthetic effects for any instances of dependent effects (e.g. shared control groups in multi-arm trials), according to the method described in the Cochrane handbook chapter 16.5.4 (Higgins and Green, 2011): for dichotomous outcomes both the sample sizes and the numbers of people with events were summed across groups.
3.4.5 Data synthesis
Evidence relating to Question 1 (effectiveness of promotional approaches) was synthesized in a quantitative way (meta-analysis), where possible. Meta-analyses were performed for 13 different outcomes across promotional approaches and timing of measurement of outcomes, to be able to make conclusions about the effect of “any promotional approach versus no promotional approach”. As soon as an outcome was present more than once, but within the same study type, it was included in a meta-analysis. Meta-analyses were conducted using Stata version 14 software. Meta-analysis results are displayed using forest plots. We used random-effects meta-analysis to produce an overall summary, if an average treatment effect across trials was considered meaningful. Fixed effect meta-analysis was not applied because its homogeneity assumption was not applicable in this systematic review. Included experimental studies were categorised and analysed according to the different promotional approaches. Experimental and quasi-experimental/observational studies were analysed separately. Mantel-Haenszel (M-H) methods were used for binary outcomes in the random-effects meta-analysis, and for calculating the effect measures, and the Inverse-Variance (I-V) method was used for continuous outcomes. Effect measures of binary outcomes were expressed as RRs (as described in 3.4.4), however a sensitivity analysis using risk differences (RD) was also made and tabulated. Forest plots reporting RDs are available upon request. Where meta-analysis was not possible, we reported results from individual studies separately. The data were grouped in separate forest plots according to the promotional approach and outcome. Data were included in forest plots if possible, or reported narratively otherwise. Evidence conclusions were formulated in a narrative way, but mentioning where possible the effect sizes (and CI), and considering risk of bias. Where possible, differences in results are explained by describing likely explanatory factors. A statistically non-significant p-value was interpreted as a finding of uncertainty (“no evidence of effect”) unless confidence intervals were sufficiently narrow (no imprecision according to the GRADE approach) to rule out an important magnitude of effect (“evidence of no effect”). Accuracy of numeric data in the review were checked against the data as available from the original study.
3.4.6 Assessment of statistical heterogeneity
The measures I2and τ2 were used as a measure of presence of heterogeneity, which was then further explored. An I2 value of greater than 50% was considered as a substantial measure of heterogeneity.
3.4.7 Subgroup analysis
Subgroup analyses were performed according to the type of promotional approach (community-based approaches, social marketing approaches, sanitation and hygiene messaging, psychosocial theory). Because of an insufficient number of studies per meta-analysis, no other subgroup analyses were made. The following factors were used in a descriptive way as likely explanatory factors for differences in results: (1) different types of promotional approaches,(2) the targets of the study (individual, household, community), (3) the setting where the approach has been applied (rural, urban, informal-urban; see Peal et al., 2010)(Fiebelkorn et al.(2012) reported differential behaviour change near the city and among the rural population; see also DFID, 2013), (4) the scale at which the approach has been applied (small scale (one village, several villages) vs larger scale (sub-district, district, province or region, national); see Hulland et al., 2015), and (5) other equity factors such as socioeconomic status, occupation and education (O'Neill et al., 2014) (adherence to water, sanitation and hygiene programmes is known to be highly associated with these confounding factors; see DFID, 2013).
3.4.8 Sensitivity analysis
No sensitivity analyses were performed due to insufficient number of studies per meta-analysis, however the risk of bias of the individual studies was considered when interpreting results.
3.4.9 Synthesis of qualitative research
For the qualitative evidence synthesis, we used the “Best fit framework synthesis” approach (Booth, 2015; Carroll, 2013). The first step of this approach was to identify an existing model for a particular health behaviour, in this case “WASH behaviour”. In the scoping phase of this project existing models for WASH behaviour change were identified, including the RANAS model and IBM-WASH model (Mosler, 2012; Dreibelbis et al., 2013). These models, that were included in our ToC, were used as an “a priori framework”. In addition to the information from the WASH behaviour change models, elements from the “Checklist for implementation” (Cargo et al., 2015), the SURE framework for implementation of a policy option (The SURE Collaboration 2011), and the PROGRESS framework to consider equity issues (O'Neill et al., 2014), were used to inform the a priori framework. In the second step of this approach, we coded data from individual qualitative studies against the a priori themes of our ToC model, representing factors that can influence the implementation of the promotional approaches ToC model (i.e. programme environment factors and recipient-related moderators, process evaluation factors and recipient-related contextual factors). Inductive, thematic analysis techniques were used if data could not be accommodated within these themes. Information from the critical appraisal items (CASP tool) was not used a-priori to exclude low-quality or high-quality studies. A sensitivity analysis was conducted by excluding low-quality studies and to test the impact of these exclusions on the overall synthesis of findings (Carroll et al., 2012). The conclusions of both strands of evidence were integrated at the end of the review process in the conclusion and discussion section. In addition, the conclusions were coupled back to the ToC. Conclusions were based only on findings from the synthesis (quantitative or narrative) of studies included in the review. In the discussion section of the review, policy implications of the findings are discussed, taking into account local considerations. In addition to the policy messages, implications for research are formulated.
3.5 DEVIATIONS FROM THE PROTOCOL
In the protocol, it was stated that for study selection we would use the text mining features of EPPI-Reviewer. However, since this feature was not ready to use at the time of study selection, this was removed from the Methods section. In the phase of study identification, we were not able to obtain the full text for some relevant references. We added to the Methods section that we labeled such papers as “unavailable” if both university libraries involved were not able to retrieve the full text articles. During the phase of data extraction, we further operationalized the definitions for the promotional approaches “sanitation and hygiene messaging”, “elements of psychosocial theory” and “community-based approach”, and for the outcomes “uptake”, “adherence” and “longer-term use”. We added to the Methods section that a promotional programme would be categorised as “community-based” when one of the above-mentioned community-based programmes is reported or where it is clearly indicated that “community members should be invited to share decision-making authority with all other persons involved”. For “uptake” we defined that this should take place during the implementation of the programme. For “adherence” we defined that this outcome should take place until 12 months after the end of the programme's implementation, while “longer-term use” takes place at least 12 months following the project period. We added to the Methods section that we classified the promotional approaches/promotional elements in 4 main groups, based on the major component of each approach: community-based, social marketing, sanitation and hygiene messaging, or elements of psychosocial theory. Concerning the primary outcomes, it was clarified that outcomes concerning animal faeces were not included; if the type of faeces was not mentioned, the outcome was included. The outcome “safe disposal of child faeces”, as mentioned in the protocol earlier, was changed into “safe faeces disposal”, to be more inclusive. For “handwashing at key times” we added “other key times” to the methods section, as compared to the protocol, to allow other key times measured in the studies. In the protocol, it was mentioned that no further data extraction would be carried out if a substantial amount of information concerning the promotional approach was missing. We now removed this from the Methods section, since there was no study for which data extraction was not carried out. In addition, it was mentioned that when information on the content of the programme was missing, related programme reports would be checked; this was removed from the Methods section since we did not encounter this situation. Because of heterogeneity across the studies for several aspects (interventions, having a WASH component and promotional approach component; outcome measures; timing of measurement of outcomes; method of outcome assessment), it was difficult to perform meta-analyses, and meta-analyses were only performed to a limited extent. In addition, since only a limited number of studies was included in each meta-analysis, subgroup analyses for several factors, adjusting for missing data and the assessment of publication bias were not made as originally planned. In the methods section we now specified how we determined ICC values for cluster RCTs and how these were used to calculate the design effect and to adjust for clustering. It was also decided post hoc to express effect measures based on binary data as RRs (risk ratios), as well as RDs (risk differences) to show absolute effects. In the protocol, it was mentioned that the certainty of evidence for the “body of evidence” resulting from the quantitative studies would be assigned according to the GRADE approach. We now added to the Methods section that this happened for each type of promotional approach, and each type of outcome. It was also included in the protocol that we would use the CerQual approach to assess the overall confidence in the qualitative evidence synthesis. Since almost all codes that were identified were based on a single study, it was decided not to make the CerQual assessment. The quality assessment using the CASP checklist was performed for each qualitative study. The research team used the first 6 months of the project (September 2015-February 2016) to perform the overview of reviews, to develop the ToC and to organize a stakeholders meeting to discuss these results and to fine-tune our initial protocol. Therefore, due to the restricted time available from March 2016 onwards, we needed to deviate from the initial protocol for the following steps: We did not search citation and reference lists of included studies and we did not check retraction statements and errata. In addition, the “Related Articles” feature of the databases was not used. As a backup for identification of missing studies we consulted our Advisory Group and a bigger group of stakeholders (including practitioners, policy makers, funders, and content experts). In addition, references from grey literature sources were only screened by one reviewer based on title and abstract. Full text assessment of the grey literature was done by 2 reviewers. In the initial protocol, a broader set of primary sanitation outcomes (including more indirect behaviour change outcomes such as latrine construction, latrine hygiene, buying of latrines, latrine maintenance) were included compared to the primary handwashing outcomes (only direct outcomes: handwashing (at key times) with or without soap). In order to be consistent and due to the availability of direct primary sanitation outcomes (i.e. open defecation practices, latrine use or safe faeces disposal practices), we decided to exclude the indirect sanitation outcomes. Concerning health outcomes, we excluded symptom-based outcomes such as cough, general illness, fever and congestion. Since it was not mentioned in the protocol if indirect outcomes would be included, we now added to the Methods section that indirect outcomes such as “presence of soap” and “pupil absence” were not considered. In addition, we added to the Methods section that outcomes that could not clearly be categorised under one of the outcome measures listed were excluded. We now mention in the Methods section for which outcomes the certainty of evidence was determined according the GRADE approach. We decided not to determine levels of evidence for secondary outcomes, for individual outcomes and for pooled outcomes with heterogeneity > 50%. For the data extraction of the qualitative studies it was indicated in the protocol that this would be done by 2 reviewers in parallel. However, initial data extraction was only done by one reviewer, and a double check of the extracted data was performed by the second reviewer. A pilot trial of the codebook was not performed beforehand, however, changes were made iteratively during the process. For the quantitative studies, the following codes, related to the quality appraisal of quasi-experimental/observational study designs, were developed post hoc: bias in selection of participants into the study (4 questions + risk of bias judgement), bias due to confounding (3 questions + risk of bias judgement), bias in measurement of interventions (3 questions + risk of bias judgement), bias in measurement of outcomes (3 questions + risk of bias judgement), bias due to departures from intended interventions (3 questions + risk of bias judgement) and reporting bias (2 questions). For the qualitative studies, it was part of the process of data extraction that additional themes were added to the ones that were already identified in the ToC model.
4 Results: Effectiveness of different approaches
4.1 DESCRIPTION OF STUDIES
4.1.1 Results of the search
We identified 23,435 records through database searching. In addition, 2,132 references were identified through grey literature searching. Following title and abstract screening, 522 records were selected for full text screening, including 401 references from database searching and 121 records via screening of the grey literature. The full texts of these references were read in detail, and after applying the pre-specified selection criteria, 342 database papers and 111 grey literature reports were excluded. This finally resulted in 35 quantitative, 19 qualitative and 5 mixed-methods studies from databases, and 6 quantitative and 4 qualitative studies from grey literature. A mixed-methods study was defined as a study fulfilling the criteria of our first and second research question. Taken together, we identified 46 references to quantitative studies (individual quantitative and mixed-methods studies), and 28 references to qualitative studies (individual qualitative and mixed-methods studies). For the quantitative papers published by Contzen et al. (2015a and 2015b), Galiani et al. (2012 and 2015), Hoque et al. (1994 and 1996) and Patil et al. (2013 and 2015), two separate references (with complementary information) for each study were included resulting in a total number of 41 quantitative studies (from 45 references). The study selection flowchart can be found in Figure 3.
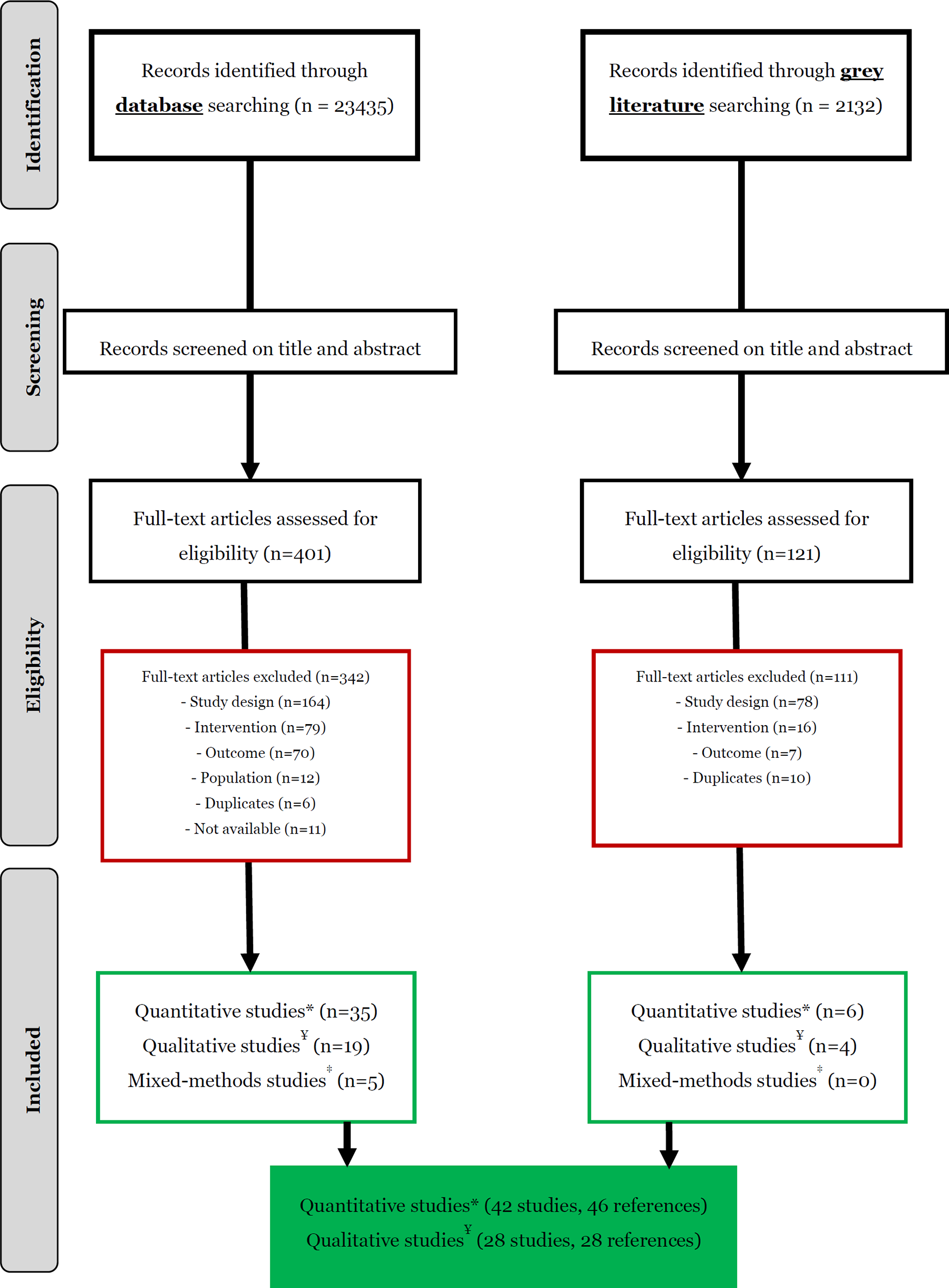
Study selection flowchart
4.1.2 Included quantitative studies (n=42)
An overview of the characteristics of the included quantitative studies can be found in Table 1. The majority of the studies was published in the last 10 years, with only 5 studies published between 1987 and 2006. Study type
Characteristics of included studies
Scale: small scale: programme enrolled in one/several villages; large scale: programme enrolled on a sub-district, district, province, region or national level; Setting: rural/urban setting: as mentioned by the paper; informal-rural setting: all relatively dense, unplanned, informal settlements within the boundaries of towns or cities. It encompasses: slums (unplanned housing illegally constructed on land with no security of tenure, sometimes referred to as ‘squatter settlements’); unplanned settlements where land tenure is formalised; growth areas on the edges of cities and towns where housing may be unplanned and growth rates high (often referred to as ‘periurban’ or the ‘peri-urban interface’) and all other densely settled areas which lie outside the formal planned definition of a city or town.
Self-reported outcome
Outcome measured through observation
We included 32 experimental studies, which are studies using random allocation methods. Among the 32 experimental studies are 26 RCTs, of which 22 are cluster RCTs, and 6 quasi-RCTs, the latter being prospective studies using a quasi-random method of allocation (e.g. alternation). In addition to the 32 experimental studies we included 8quasi-experimental studies (non-randomised controlled trials), which by definition use non-random allocation methods (e.g. self-selection of participants) alongside statistical analysis to address confounding. Finally we also included 2 observational studies(i.e. cohort studies). Countries (see Figure 4)
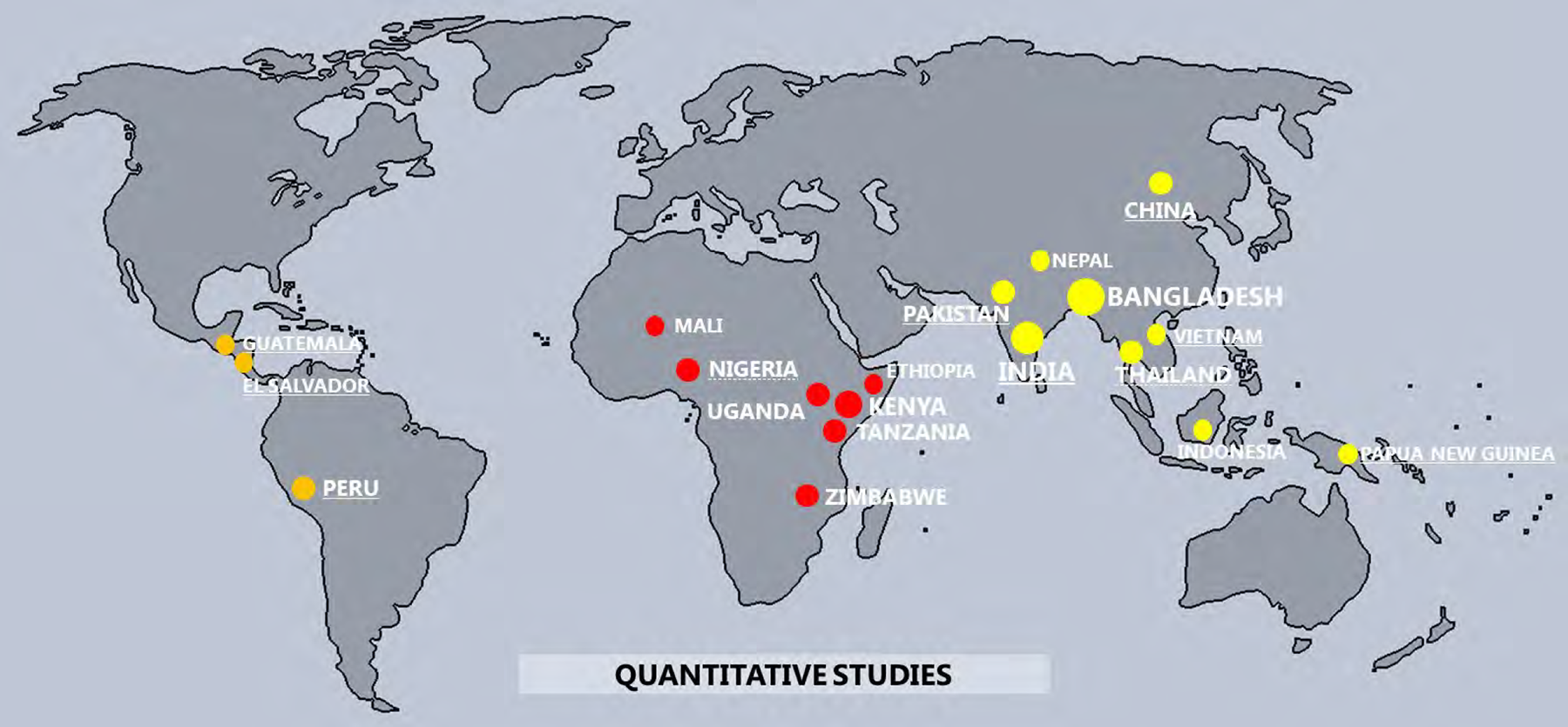
World map indicating in which countries the included quantitative studies were performed
Most of the studies (n=25, 59%) were performed in Asia: 17 studies in South Asia (Bangladesh (n=8), India (n=7), Pakistan (n=2) and Nepal (n=1)), 5 in South-East Asia and Oceania (Thailand (n=2), Indonesia (n=1), Papua New Guinea (n=1), Vietnam (n=1) and 2 in East Asia (China (n=2)). Thirteen studies were performed in Sub-Saharan Africa (Kenya (n=3), Zimbabwe (n=2), Uganda (n=2), Tanzania (n=2), Nigeria (n=2), Ethiopia (n=1) and Mali (n=1)), and only 4 in Central America (Guatemala (n=1) and El Salvador (n=1)) or Latin America (Peru (n=2)).
Considering country income at the time the studies were performed, 22 studies (52%) were conducted in low-income countries (Bangladesh, Ethiopia, Kenya, Mali, Nepal, Nigeria (until 2007), Tanzania, Thailand, Uganda and Zimbabwe), 18 studies (43%) in lower middle-income countries (China (until 2010), El Salvador, Guatemala, India, Nigeria (from 2007), Pakistan, Papua New Guinea, Peru (until 2008), Thailand and Vietnam) and 2(5%) in upper middle-income countries (China (from 2010) and Peru (from 2008)). Setting and target level
Most (69%) of the studies were executed in a rural setting (n=29), 6 studies (14%) were performed in an urban setting, and 4 studies (10%) were performed in an informal-rural setting (i.e. slums, settlements). Three studies (7%) had no information about the setting in which the studies were conducted. The intervention was targeted at a a household level in 14 studies, a village level in 6 studies, a household/village level in 2 studies, a community level in 5 studies, a household/community level in 1 study, an individual level in 2 studies, a neighborhood level in 1 study, on a compound level in 2 studies and at a school level in 8 studies. One study investigated interventions on both a community level and a school level. WASH intervention
Thirty-threestudies compared one WASH intervention to either no intervention (n=23), or another intervention (n=10). The intervention programmes comprised different combinations of WASH components: sanitation only (n=5), handwashing only (n=10), handwashing+sanitation (n=3), handwashing or sanitation with other WASH components (other hygiene (n=3), water supply (n=4), other hygiene+water supply (n=1), water quality (n=1)), and general WASH (n=6).
Six studies compared two WASH interventions to no intervention. The WASH components of the two intervention groups were: sanitation+handwashing versus handwashing (n=1), handwashing+water supply versus handwashing (n=1), sanitation versus sanitation+other hygiene (n=1) and handwashing in both intervention groups (but different promotional approaches used) (n=3).
Two studies compared three WASH interventions to no intervention (n=1) or another intervention with general WASH components (n=1). The WASH components of the 3 intervention groups were: sanitation versus handwashing versus sanitation+handwashing (n=1), and handwashing only in the 3 intervention groups (but different promotional approaches used) (n=1).
One study compared four WASH interventions to no intervention. The WASH component of the four intervention groups was sanitation (but different promotional approaches used). Promotional approach
The promotional approaches differed considerably across the studies. For each study, we indicated if elements of sanitation and hygiene messaging, psychosocial theory, community-based working, social marketing, incentives or advocacy were used, leading to 27 different combinations of elements and thus 27 different promotional approaches (see Figure 5). Based on the main promotional element in each approach we classified the promotional approaches/promotional elements in 4 groups. This was done independently by 4 team members (methodological and content experts), followed by discussion to resolve disagreements. In addition, we also discussed this with a large group of stakeholders who agreed with the classification approach
Based on the major component of the promotional approach used in each study, we distinguished these 4 major approaches: Community-based approaches: in this category we included the studies that used a formal community-based approach or those approaches that contained elements of community-based working as the major strategy. Other elements that could be part of these approaches were: education, incentives, and/or theory-based elements. Social marketing approaches: all studies that used a formal social marketing approach or where marketing was the main element of the promotional approach were grouped in this category; other elements that could be part of these approaches were: community-based aspects, incentives, advocacy, and/or theory-based elements. Sanitation and hygiene messaging: since educational elements were present in almost all promotional approaches we only included those approaches that used a directive way of education, making use of one-way communication; other elements that were part of the approach were incentives, public commitment, and/or theory-based elements. Elements of psychosocial theory: in this category we included those approaches that used psychosocial theory, social cognitive elements or theoretical elements of behaviour change to design the intervention and as the main focus of the approach. Interventions designed this way were typically small-scale and used formative research.
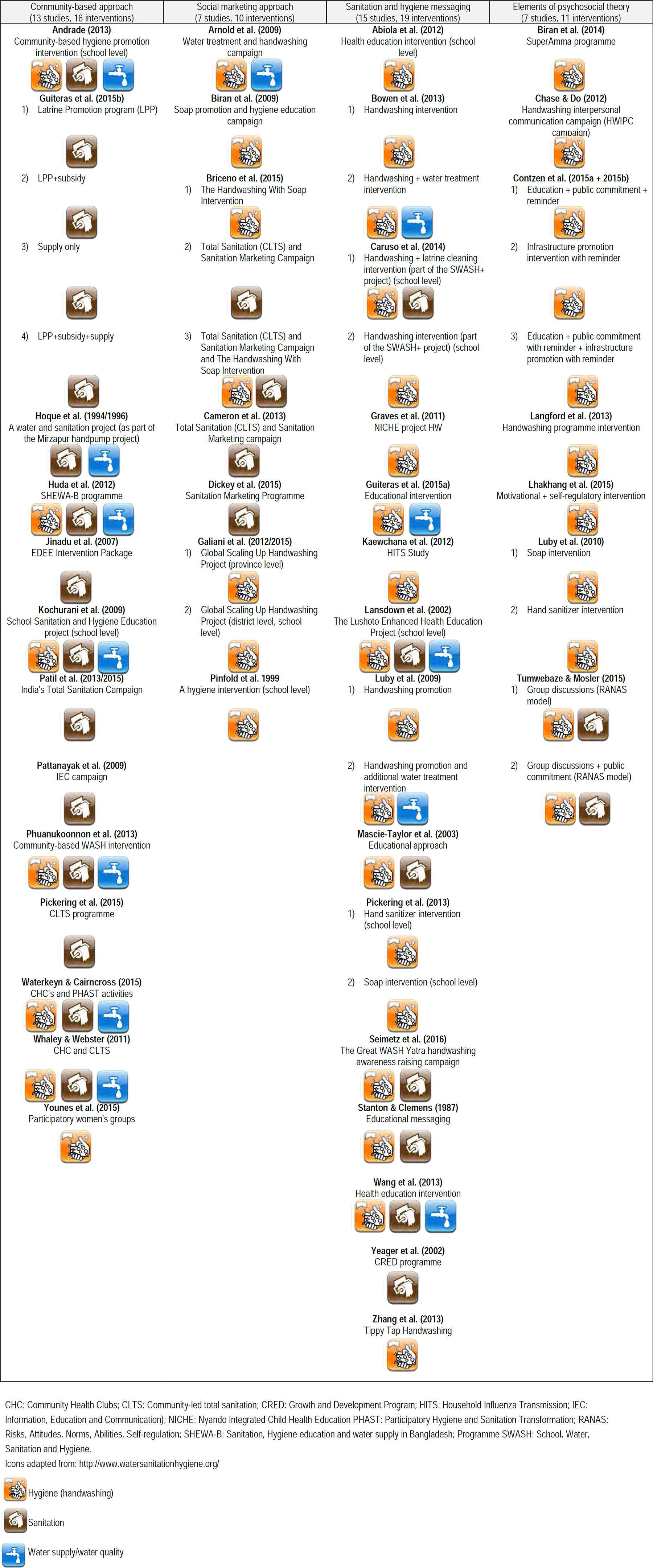
According to these criteria we classified the promotional approach as a community-based approach in 13 studies, a social marketing approach in 7 studies, and sanitation and hygiene messaging in 15 studies. Elements of psychosocial theory were investigated in 6 studies. Table 2 gives an overview of which studies were grouped under each category.
List of included quantitative studies in each of the 4 categories of promotional approaches
Figure 6 also lists the specific approach in each study and the WASH component for each study. Community-based approaches all contained at least a sanitation component (except for one study with a handwashing-only intervention), social marketing approaches and sanitation and hygiene messaging interventions focused in the majority of the cases at least on handwashing, and the approaches based on elements of psychosocial theory almost in all cases only had a handwashing component.
Seven studies only looked at the relative effectiveness of a promotional approach versus another promotional approach and 1 study compared programmes with a similar promotional approach (i.e. sanitation and hygiene messaging) but with different communication channels (interpersonal+mass media communication versus mass media only).
Since (non-) financial incentives were always part of a broader promotional approach listed above, we did not create a separate category for this type of promotional elements. However, in Table 3 an overview of the types of incentives is provided, and in the results section below, incentives are dealt with as a possible moderating factor. Financial incentives included a modest salary and subsidies, and non-financial incentives included a motorcycle, lunch, food, gifts and soap. We make the distinction between incentives given to the secondary implementer (community-member involved in the implementation) and the recipients (villagers/household members, receiving the promotional approach).
Overview of studies describing the use of financial or non-financial incentives
Communication strategies
All intervention programmes (n=55) used (at least) interpersonal communication channels: 22 interventions (40%) used interpersonal communication only, 16 interventions (29%) used interpersonal+mass media communication, 7 interventions (13%) used interpersonal+traditional communication and 10 interventions (18%) used interpersonal+mass media+tradional communication.
The programmes with a promotional approach in the control group (n=10) were promoted via interpersonal communication only (n=5), via mass media communication only (n=1), via traditional communication only (n=1), via interpersonal+mass media communication (n=1) or via interpersonal+mass media+traditional communication channels (n=2). Implementers (see Figure 7)
Almost all studies (n=40, 95%) reported who the implementers of the programme were. Information about training/qualification of the implementers (n=24, 57%), the role of the evaluator (n=18, 43%) and gender of the implementers (n=11, 26%) was less frequently reported. Information about ethnicity (n=4, 9%), age (n=4, 9%) and socio-economic status (n=4, 9%) of the implementers was rarely reported. Implementing organization (see Figure 8)
In general, information about the implementing organization was not frequently reported: about 30% of the studies provided information about leadership (n=15), the quality of the training materials (n=14), technical support or supervisory guidance (n=14). Funding information (about the programme (not the study)) was provided in 10 studies (24%) and only 2 studies (5%) provided information on partnership/coordination between providers. Process evaluation factors (see Figure 9)
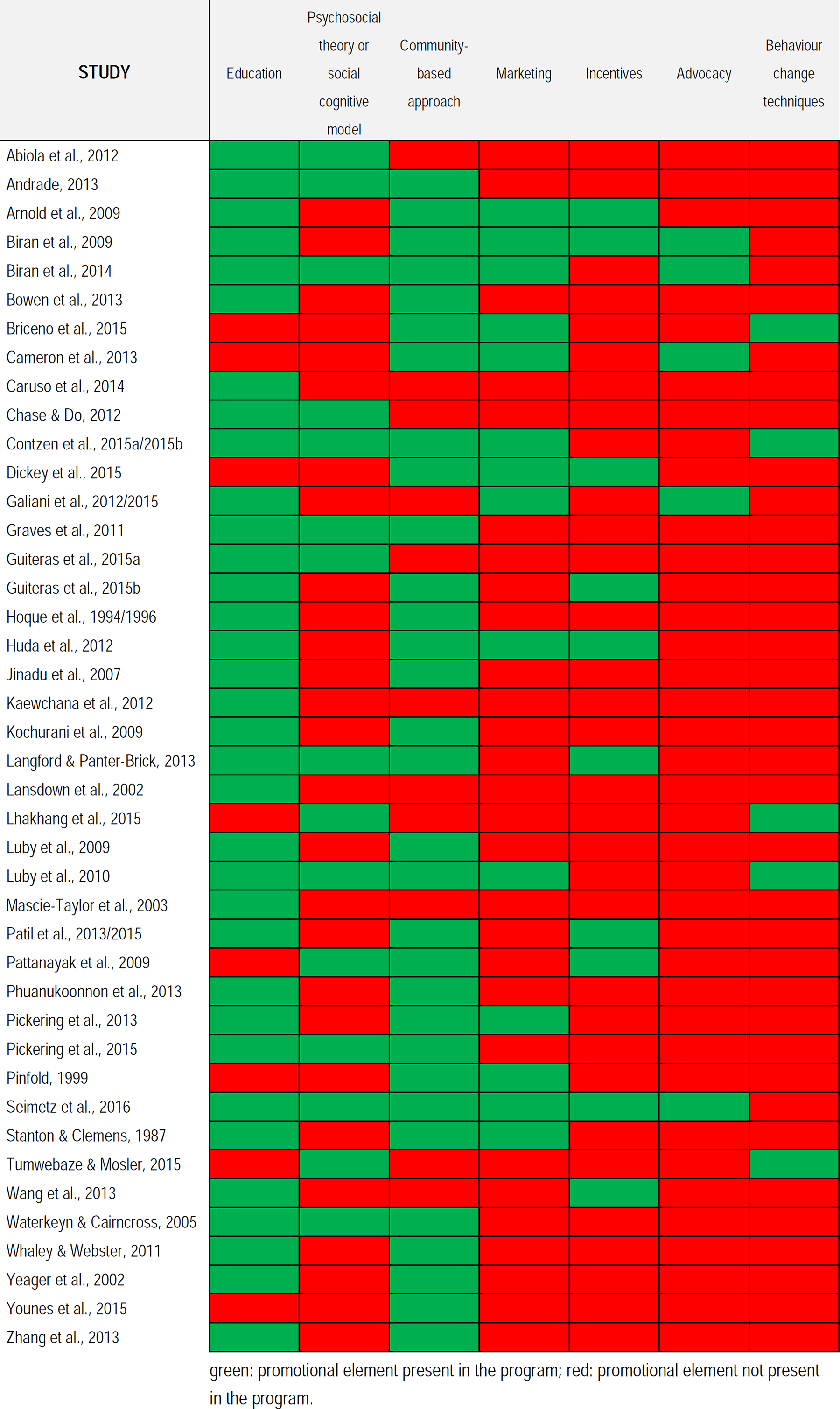
Promotional elements present in the interventions of the 41 included quantitative studies
Main categories of promotional approaches with detailed indication of WASH component and specific promotional approach for each included quantitative study
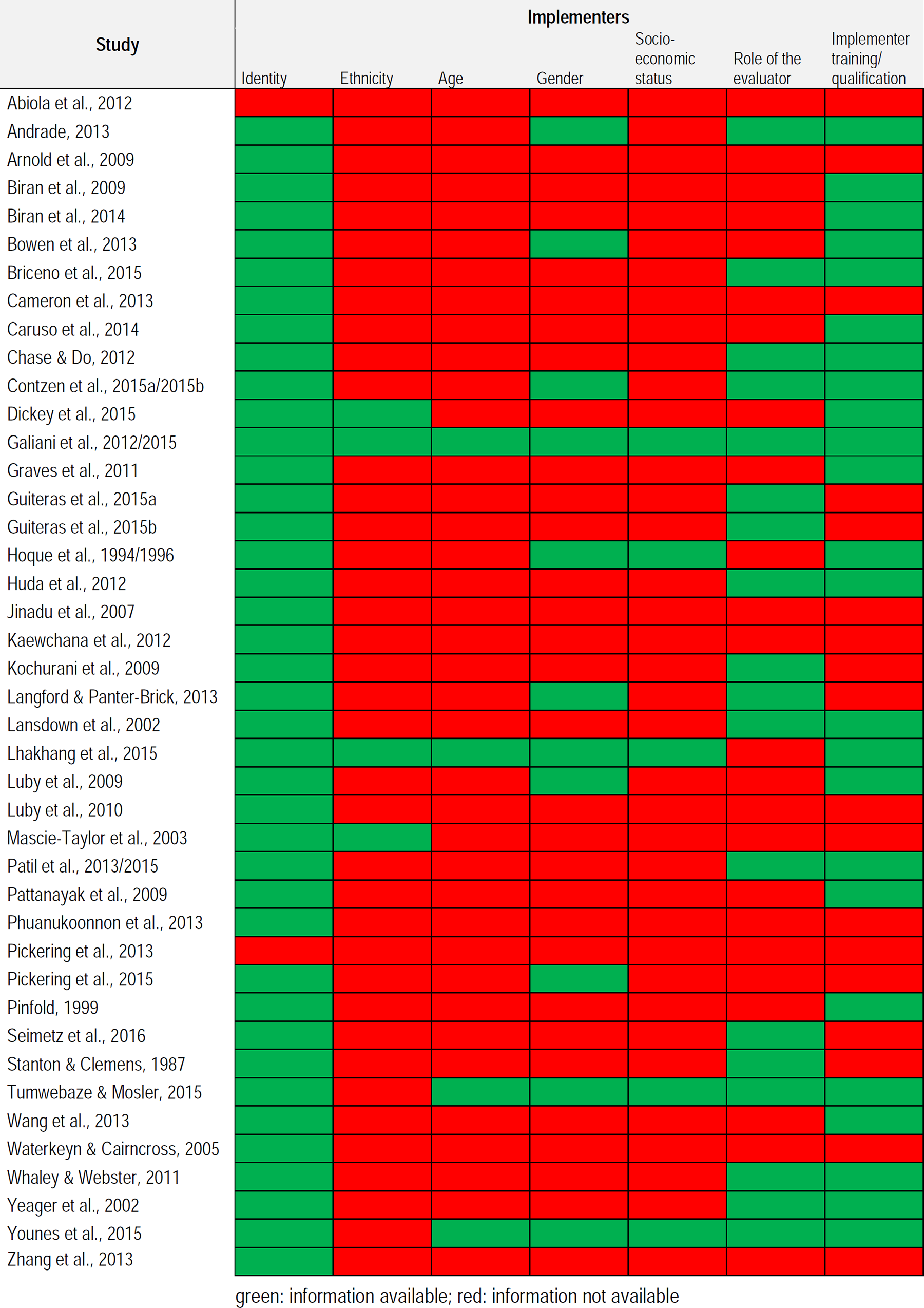
Reported information about the implementers
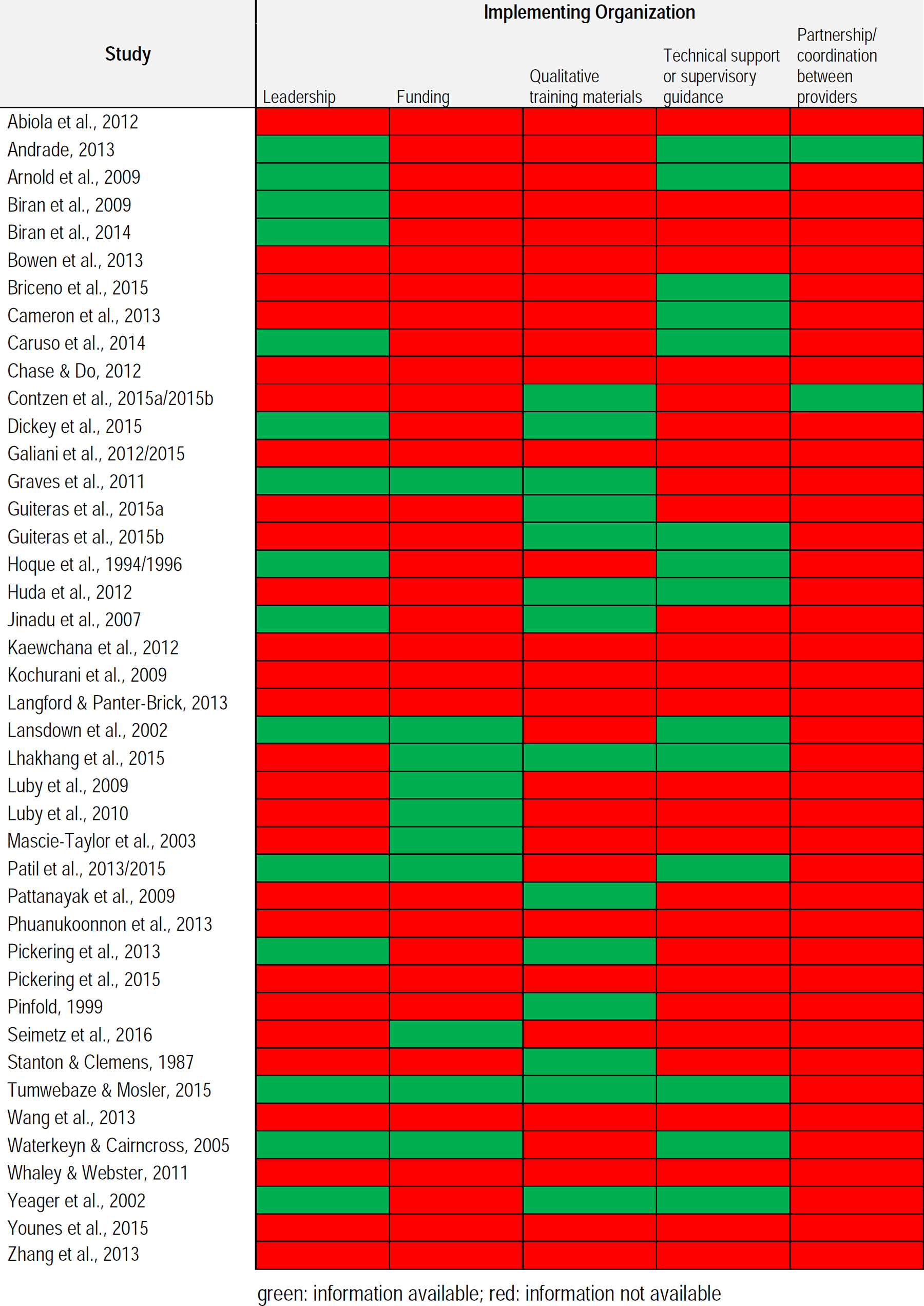
Reported information about the implementing organization
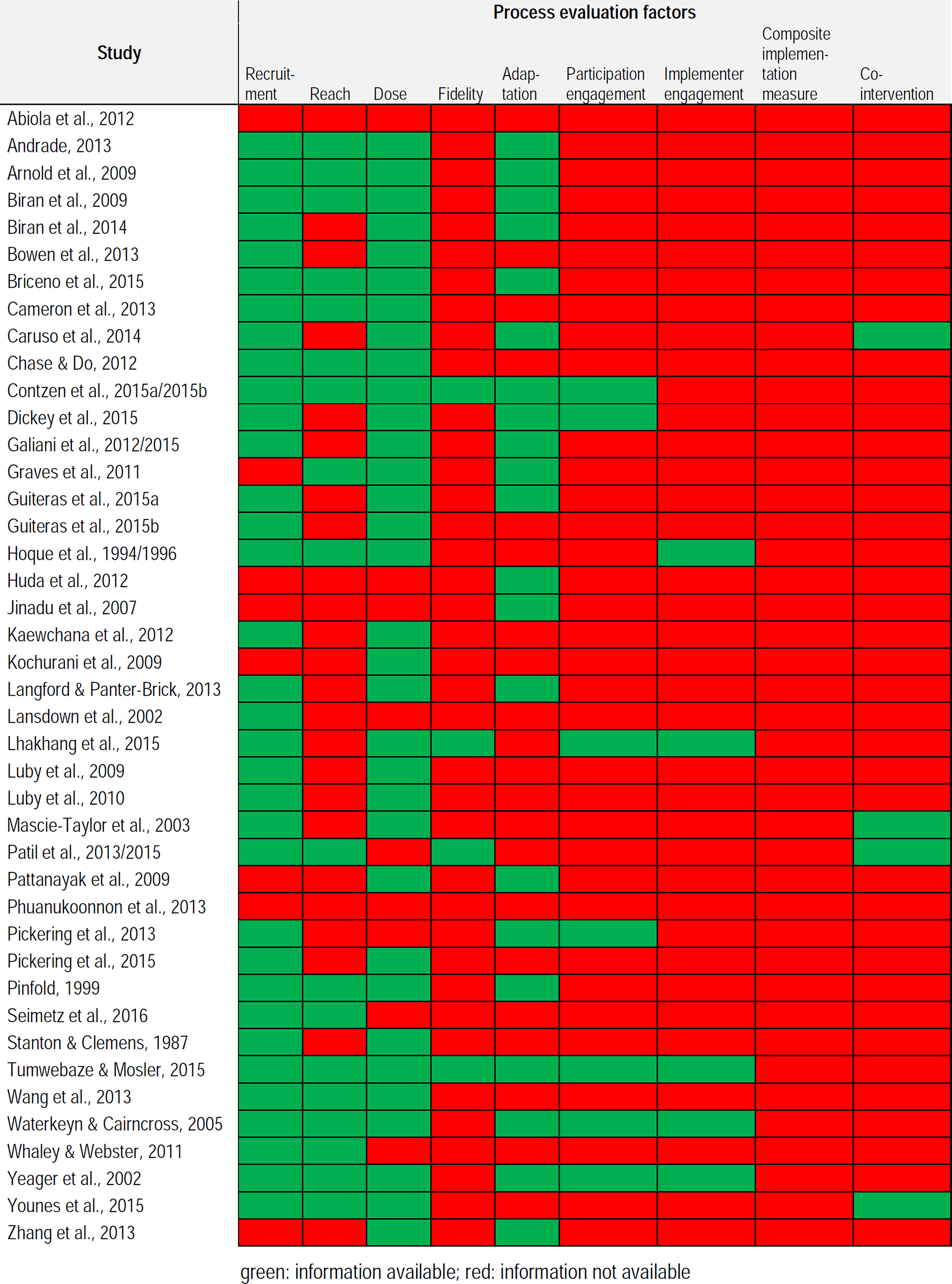
Reported information about the process evaluation factors
Recruitment (n=34, 81%) and dose (n=33, 78%) were frequently reported. Forty-three percent of the studies provided information on reach (n=18) or adaptation (n=21, 50%) whereas information on fidelity (n=5), implementer engagement (n=5), participation engagement (n=7) or co-intervention (n=4) was only reported in 10-20% of the studies. No studies had information on composite implementation measures. Outcomes
In total, 559 different outcomes (i.e. different outcome descriptions, timing of measurement, method of assessment, and reported statistics) were measured across all studies.
Raw data were available in most of the studies (n=39, 93%): binary data (n=18), continuous data (n=12), binary+continuous data (n=7), continuous+correlation data (n=1) and binary data+calculated effect sizes (n=1). Three studies (7%) only reported calculated effect size measures.
Primary (behaviour change) outcomes were reported in 39 studies: intention in 2 studies, handwashing (with or without soap) in 12 studies, handwashing at key times in 21 studies, latrine use in 9 studies, faeces disposal practices in 9 studies and open defecation in 9 studies. The following behavioural factors (secondary outcomes) were assessed: knowledge in 12 studies, skills in 6 studies, attitude in 5 studies, and self-regulation in 4 studies. Morbidity and mortality (secondary outcomes) were measured in 11 studies and 1 study, respectively.
Outcomes were assessed via self-reported measures in 27 studies (64%), via direct observation in 10 studies (24%), or via self-reported measures plus direct observation in 5 studies (13%).
The timing of outcome assessment was different across studies: 18 studies assessed the outcomes during the programme implementation (i.e. uptake), 16 studies assessed the outcomes within 12 months after the end of the implementation (i.e. adherence) and only 5 studies measured the outcomes more than 12 months after the end of the implementation (i.e. longer-term use). Three studies assessed outcomes at two different time points: 1 study at uptake+adherence, 1 study at uptake+longer-term use and 1 study at adherence+longer-term use.
4.1.3 Excluded studies
After title and abstract screening, 522 full texts (401 from databases and 121 from grey literature) were screened for eligibility. The majority of these full-texts were excluded (n=461, 88%) for different reasons: study design (n=242, 52%), intervention (n=95, 21%), outcome (n=77, 16%), population (n=12, 3%), duplicates (n=24, 5%), not available (n=11, 2%). Detailed information can be found in Appendix 9 (List of excluded database studies) and 6 (List of excluded grey literature studies), and the reference list of excluded studies.
4.2 RISK OF BIAS IN INCLUDED STUDIES
4.2.1 Experimental studies (n=32)
A visual overview of the risk of bias of the experimental studies can be found in Figure 10. Random sequence generation
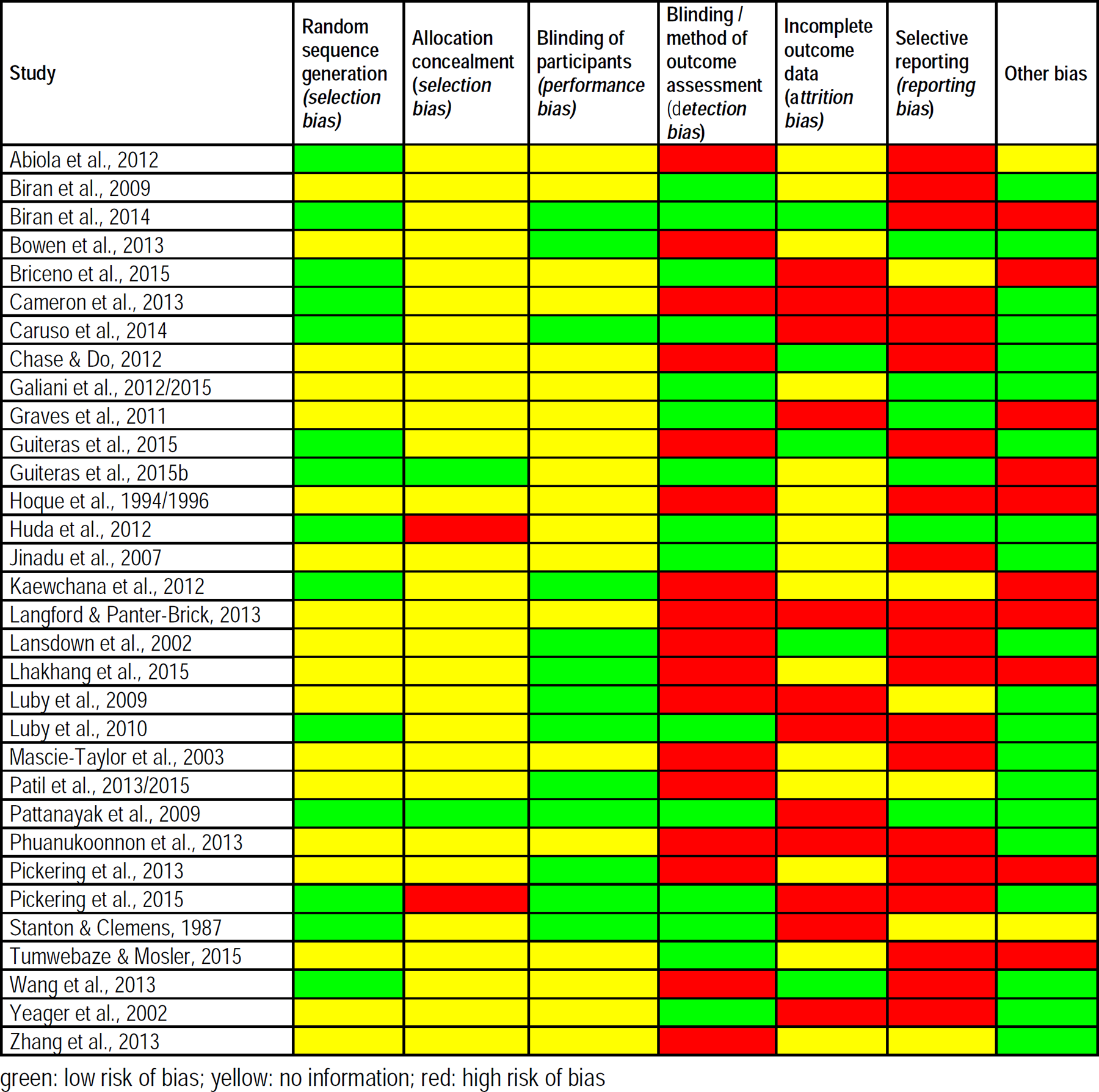
Risk of bias in the experimental studies
Many studies did not provide clear information on the way the randomization sequence was generated. In 14 of the 32 studies (44%) the randomization sequence was clearly described, and assigned as being at low risk of selection bias. In 18 of the 32 studies (56%), not enough information was provided to determine if the method of random sequence generation was adequate. Allocation concealment
In two studies (6%), Guiteras et al. (2015b) and Pattanayak et al.(2009), allocation concealment was described, and was assessed to be a low risk of bias. In two studies (6%), Pickering et al.(2015) and Huda et al.(2012), allocation concealment was not conducted and thus assessed as high risk of bias. The majority of studies (n=28, 88%) did not provide any information to assess risk of bias and were thus assigned as unclear. Blinding of participants
Blinding of participants to a treatment group was not easy for this type of intervention, and only one study (2%), Biran et al.(2014), reported on blinding of participants. In 18 studies (56%), there was a lack of information about blinding, and these studies were rated as unclear. Thirteen studies (42%) reported no blinding of participants. Blinding of outcome assessors
No information on blinding of outcome assessors was given in 12 of the studies (37%), with 11 studies (34%) reporting no blinding and 9 studies clearly indicating that outcome assessors were blinded (28%). Self-reported outcomes were assessed in 18 studies (56%) whereas 14 studies (44%) measured outcomes via direct observation techniques. Incomplete outcome data
Incomplete outcome data was clearly dealt with in 5 studies (16%), with the many studies (n=13, 40%) having not dealt with this issue. In the remaining 14 studies (44%), there was no information on how incomplete outcome data was dealt with. Selective reporting
Selective reporting bias was found to be present in many studies (20/32, 62%), with only 5 studies (16%) reporting having dealt adequately with this bias. No information was present in 7studies, and these were rated as unclear. Other risks of bias
There were no other risks of bias in the majority of the studies (20/32, 62%). There were other risks of bias in 10 studies (high risk, 31%) and two studies (6%) did not provide any information regarding other risks of bias. No intra-cluster correlations (ICC) were reported in 15 of the 22 cluster RCTs.
4.2.2 Quasi-experimental (n=8) and observational studies (n=2)
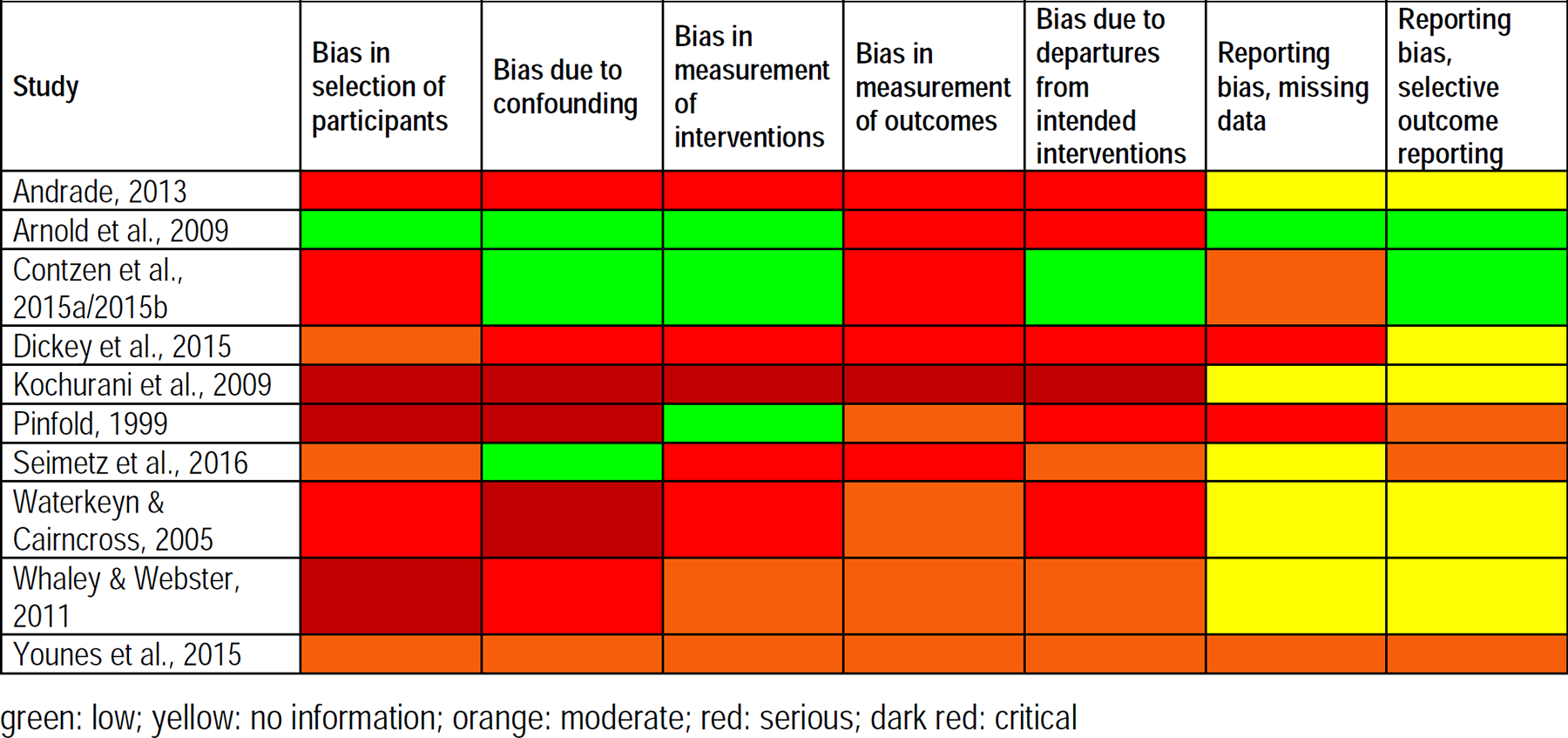
A visual overview of the risk of bias of the quasi-experimental and observational studies can be found in Figure 11. The observational studies both were cohort studies (Arnold et al., 2009, Seimetz et al., 2016). Bias in selection of participants
Risk of bias in the quasi-experimental and observational studies
Three studies (30%) were assessed to be at a critical level for this category. Three studies (30%) were judged to have serious bias and three were moderate. Only the Arnold et al. (2009) study was judged to be of low bias, as the selection into the study (or into the analysis) was unrelated to intervention or unrelated to outcome. The start of follow-up and start of intervention coincided for most participants, and there were adjustment techniques used that were likely to correct for the presence of selection biases. The allocation mechanism was also appropriate to generate equivalent groups. Bias due to confounding
There were 4 studies (40%) judged to have critical level of bias due to confounding. An equal number had a low risk of bias, as the authors used an appropriate analysis method that controlled for all the important confounding areas (baseline confounding). The authors also used an appropriate analysis method that controlled for time-varying confounding, if present, and confounding areas that were controlled for measured validly and reliably by the variables available in this study. The remaining studies were judged to be of moderate (1) and serious (3) bias. Bias in measurement of interventions
Three studies (30%) had a low bias in measurement of interventions, with 3 studies (30%) being judged as moderate and 4 studies (40%) being judged as serious. One study, Kochurani et al. (2009), was evaluated to have critical bias as the intervention was not well defined, the information used to define intervention groups was not recorded at the start of the intervention, and information on intervention status was affected by knowledge of the outcome or risk of the outcome. Bias in measurement of outcomes
Four studies (40%) showed moderate bias in this category and 5 studies (50%) were judged as serious. One study, Kochurani et al. (2009), was deemed to show critical bias as this study did not have an objective outcome measure. The methods of outcome assessment were not comparable across intervention groups, and outcome assessors were aware of the interventions that the groups received. Bias due to departures from intended intervention
The Contzen et al. (2015a/2015b) study had a low risk of bias and three other studies were of moderate bias. Five studies (50%) were shown to have serious bias, and the Kochurani et al. (2009) study was assessed to have critical levels of bias as the important co-interventions were not balanced across intervention groups, the study participants did not adhere to the assigned intervention regimen, and the intervention was not implemented successfully for most participants. Reporting bias (missing data + selective outcome reporting)
The reporting biases as discussed here incorporate biases because of missing data and selective outcome reporting. The Arnold et al. (2009) study showed low bias for both aspects of reporting bias. Contzen et al. (2015a/2015b) showed low bias in the selective outcome reporting category, but moderate for the missing data category. Andrade (2013), Dickey et al. (2015), Kochurani et al. (2009), Seimetz et al. (2016), Waterkeyn & Cairncross (2005) and Whaley & Webster (2011) provided no information on reporting bias and were assessed as unclear. Both Pinfold (1999), and Seimetz et al. (2016) were assessed as moderate for the selective outcome reporting category.
4.3 SYNTHESIS OF RESULTS
Studies were very heterogenous (various promotional approaches and different outcomes), which made it difficult to present the study findings. In the first part of the results (4.3.1) we first compared any promotional approach versus no promotional approach. We pooled similar outcomes across promotional approaches, and created meta-analyses for the following outcomes: Handwashing after toilet use Handwashing before cooking Handwashing after cleaning a child's anus Handwashing before eating Handwashing before feeding a child Latrine use Safe faeces disposal Safe child faeces disposal Open defecation Skills: using soap for handwashing Skills: rubbing hands together at least 3 times Skills: lathering hands more than 10 seconds Skills: drying hands with a clean towel
In addition to the outcomes captured in the meta-analyses, many individual outcomes were reported that could not be pooled because of variation in study designs, outcome measures, or timing of measurement. Therefore, all data were also presented individually, and grouped in separate forest plots according to the promotional approach, outcome and timing of measurement (uptake, adherence or longer-term use). This is the second part of the results section, comparing a certain promotional approach versus no promotional approach. For this purpose, we grouped the outcomes in six major groups (according to our ToC): Behaviour change (primary outcomes): handwashing (handwashing with soap, handwashing without soap, handwashing at key times). Behaviour change (primary outcomes): latrine use. Behaviour change (primary outcomes): safe faeces disposal. Behaviour change (primary outcomes): open defecation. Behavioural factors (secondary outcomes); outcomes were grouped under “knowledge”, “skills”, “attitude”, “norms” and “self-regulation”. Health outcomes (secondary outcomes); outcomes were grouped under “morbidity” and “mortality”.
In a next section (4.3.2), different types of promotional approaches are compared. Finally, we looked at the effect of different communication strategies to the same promotional approach (4.3.3).
4.3.1 Promotional approach versus no promotional approach
In 34 studies the effect of using a promotional approach was compared with not using a promotional approach. Of these studies, 12 studies described a community-based approach, 6 studies described a social marketing approach, 12 studies described sanitation and hygiene messaging, and 4 studies described a small-scale intervention based on elements of psychosocial theory. An overview of the studies included in each category of promotional approaches (compared to not using a promotional approach) can be found in Table 4.
Overview of the studies comparing a promotional approach versus no promotional approach (control group), divided into the 4 categories of promotional approaches
4.3.1.1 Any promotional approach
For the list of predefined outcomes (see above) meta-analyses were performed across the different promotional approaches and different times of measurement. For each meta-analysis, subgroup analyses according to the promotional approach were performed, and where possible according to timing of measurement. However, for 11 of the 13 outcomes there was too much heterogeneity to be able to make conclusions across the different types of promotional approaches. The pooled value per promotional approach is reported below in case no statistical heterogeneity was present. Below we describe the results for the 1 different outcomes: Behaviour change: handwashing after toilet use (Analysis 1). Since there was too much heterogeneity it was not possible to pool the outcomes across promotional approaches. Only for the community-based approaches, a level of heterogeneity < 50% was found. A community-based approach may make little or now difference in handwashing after toilet use (RR 1.06, 95 %CI [0.99, 1.14]; level of certainty: low, Table 5) (Huda et al., 2012; Phuanokoonnon et al., 2013). Behaviour change: handwashing before cooking (Analysis 2). There was no significant increase in handwashing for the community-based approach (RR 0.94, 95% CI [0.31, 2.91]) (Huda et al., 2012). Sanitation and hygiene messaging may improve handwashing before cooking (RR 1.23, 95% CI [1.09, 1.39]; level of certainty: low (Table 6)) (Bowen et al., 2013; Stanton & Clemens, 1987). The effect of elements of psychosocial theory on handwashing before cooking is uncertain(RR 33.06, 95% CI [6.72, 162.69]; level of certainty: very low (Table 7)) (Langford & Panter-Brick, 2013; Luby et al., 2010). Behaviour change: handwashing after cleaning a child's anus (Analysis 3). There was no A significant increase in handwashing for the community-based approach (RR 1.34, 95% CI [0.85, 2.12]) (Huda et al., 2012). For the other approaches and “overall promotional approach” there was too much heterogeneity to be able to make overarching conclusions. Behaviour change: handwashing before eating (Analysis 4). A community-based approach may lead to slightly improved handwashing before eating (RR 1.12, 95% CI [1.02, 1.22]; level of certainty: low (Table 8)) (Huda et al., 2012; Phuanukoonnon et al., 2013), while elements of psychosocial theory may improve it (RR 34.73, 95% CI [4.90, 246.39]; level of certainty: low (Table 9)) (Langford & Panter-Brick, 2013; Luby et al., 2010). In case of sanitation and hygiene messaging, there was too much heterogeneity to be able to make overall conclusions. Behaviour change: handwashing before feeding a child (Analysis 5). The effect of a community-based approach is uncertain (RR 1.04, 95% CI [0.94, 1.15]; level of certainty: very low (Table 10)) (Huda et al., 2012, Phuanukoonnon et al., 2013). A theory-based approach may improve handwashing before feeding a child (RR 3.63, 95% CI [1.91, 6.88]; level of certainty: low (Table 11)) (Langford & Panter-Brick, 2013; Luby et al., 2010). Behaviour change: latrine use (Analysis 6). High heterogeneity across the studies (all using a community-based approach) did not make it possible to pool the outcomes. Therefore, we were not able to make any overall conclusions for this outcome. However, when a subgroup analysis was performed according to timing of measurement (adherence and longer-term use), a community-based approach may improve latrine use less than 12 months after the end of programme implementation (adherence) (RR 2.63, 95% CI [1.62, 4.29]; level of certainty: low (Table 12)) (Jinadu et al., 2007; Pattanayak et al., 2009). Behaviour change: safe faeces disposal practices and safe child faeces disposal practices (Analysis 7 and 8). Since there was too much heterogeneity it was not possible to pool the outcomes across and within the promotional approaches. For sanitation and hygiene messaging, only one study was included, showing statistically significant increased safe faeces disposal practices(RR 1.68, 95% CI [1.21, 2.32]), however a significant effect on safe child faeces disposal practices could not be demonstrated (RR 1.07, 95% CI [0.70, 1.65]) (Yeager et al., 2002). Behaviour change: open defecation (Analysis 9). A community-based approach resulted in a statistically significantly decrease in open defecation (RR 0.40, 95% CI [0.37, 0.44]) (Pickering et al., 2015). Sanitation and hygiene messaging may make little or no difference in open defecation (RR 0.99, 95% CI [0.72, 1.37]; level of certainty: low (Table 13)) (Lansdown et al., 2002; Stanton & Clemens, 1987; Wang et al., 2013). Behavioural factors: skills: using soap for handwashing (Analysis 10). Sanitation and hygiene messaging probably slightly improves using soap for handwashing (handwashing technique) (RR 1.05, 95% CI [1.02, 1.08]; level of certainty: moderate (Table 14)) (Bowen et al., 2013; Luby et al., 2009). No studies on other approaches measured this outcome. Behavioural factors: skills: rubbing hands together at least 3 times (Analysis 11). Only studies using sanitation and hygiene messaging measured if there was an improvement in rubbing the hands together at least 3 times (Bowen et al., 2013; Luby et al., 2009). Since there was too much heterogeneity it was not possible to pool the data, and it was not possible to make any overall conclusions for this outcome. Behavioural factors: skills: lathering hands > 10 seconds (Analysis 12). Only studies using sanitation and hygiene messaging measured if lathering hands for more than 10 seconds (handwashing technique) had increased (Bowen et al., 2013; Luby et al., 2009). Since there was too much heterogeneity it was not possible to pool the data, and it was not possible to make any overall conclusions for this outcome. Behavioural factors: skills: drying hands with a clean towel (Analysis 13). Only studies using sanitation and hygiene messaging measured if drying hands with a clean towel (handwashing technique) had resulted in an increase (Bowen et al., 2013; Luby et al., 2009). Since there was too much heterogeneity it was not possible to pool the data, and it is not possible to make any overarching conclusions for this outcome.
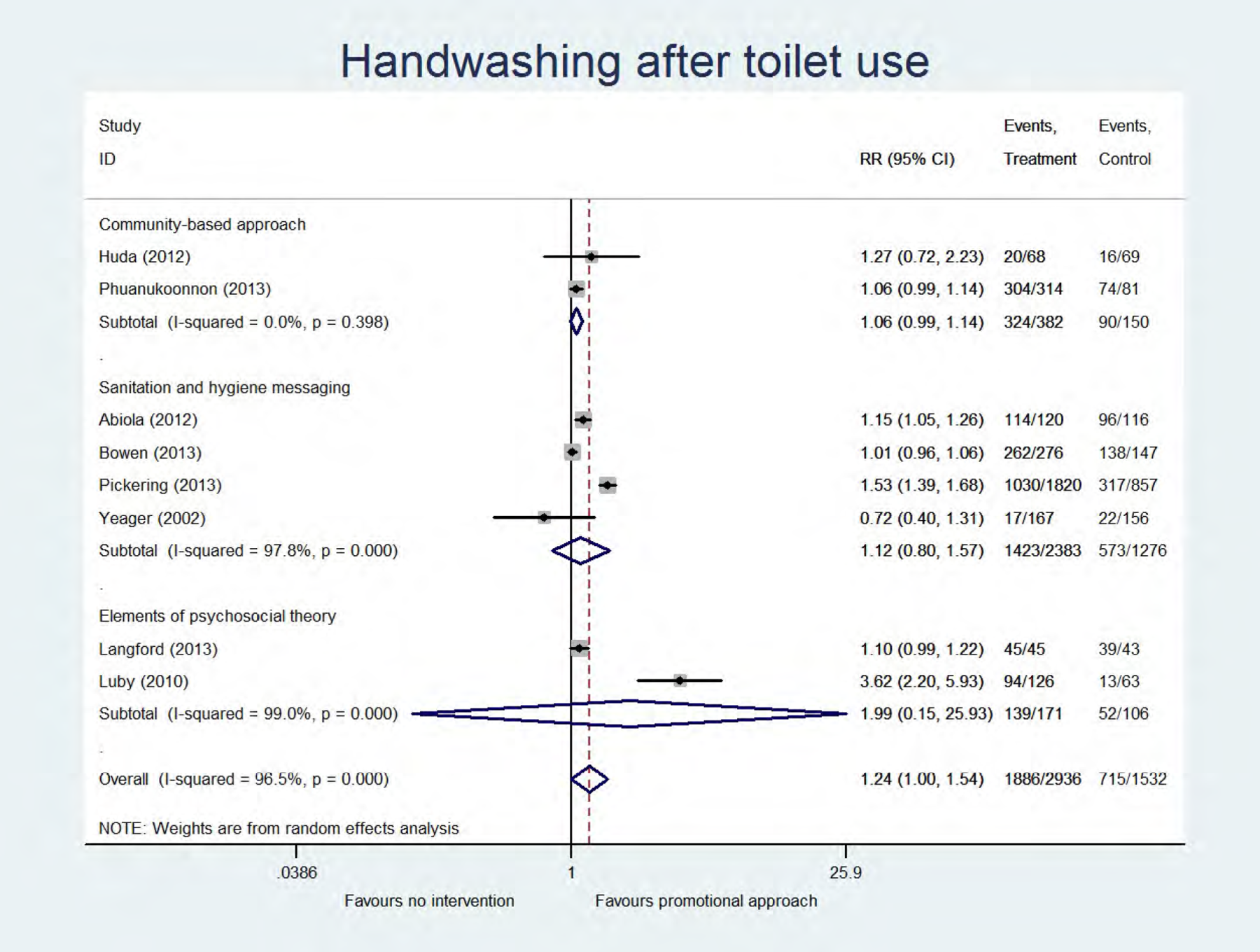
Analysis
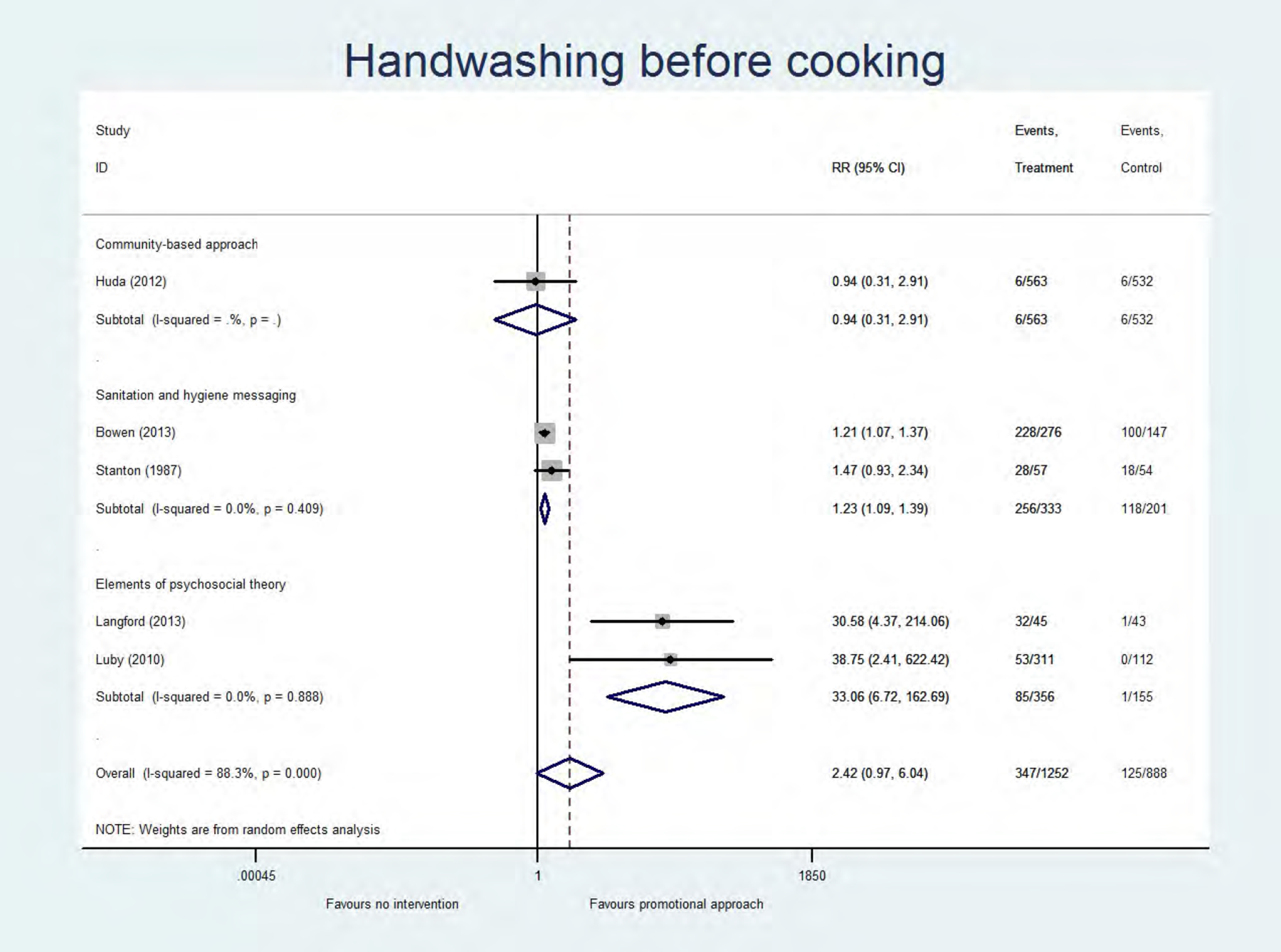
Analysis
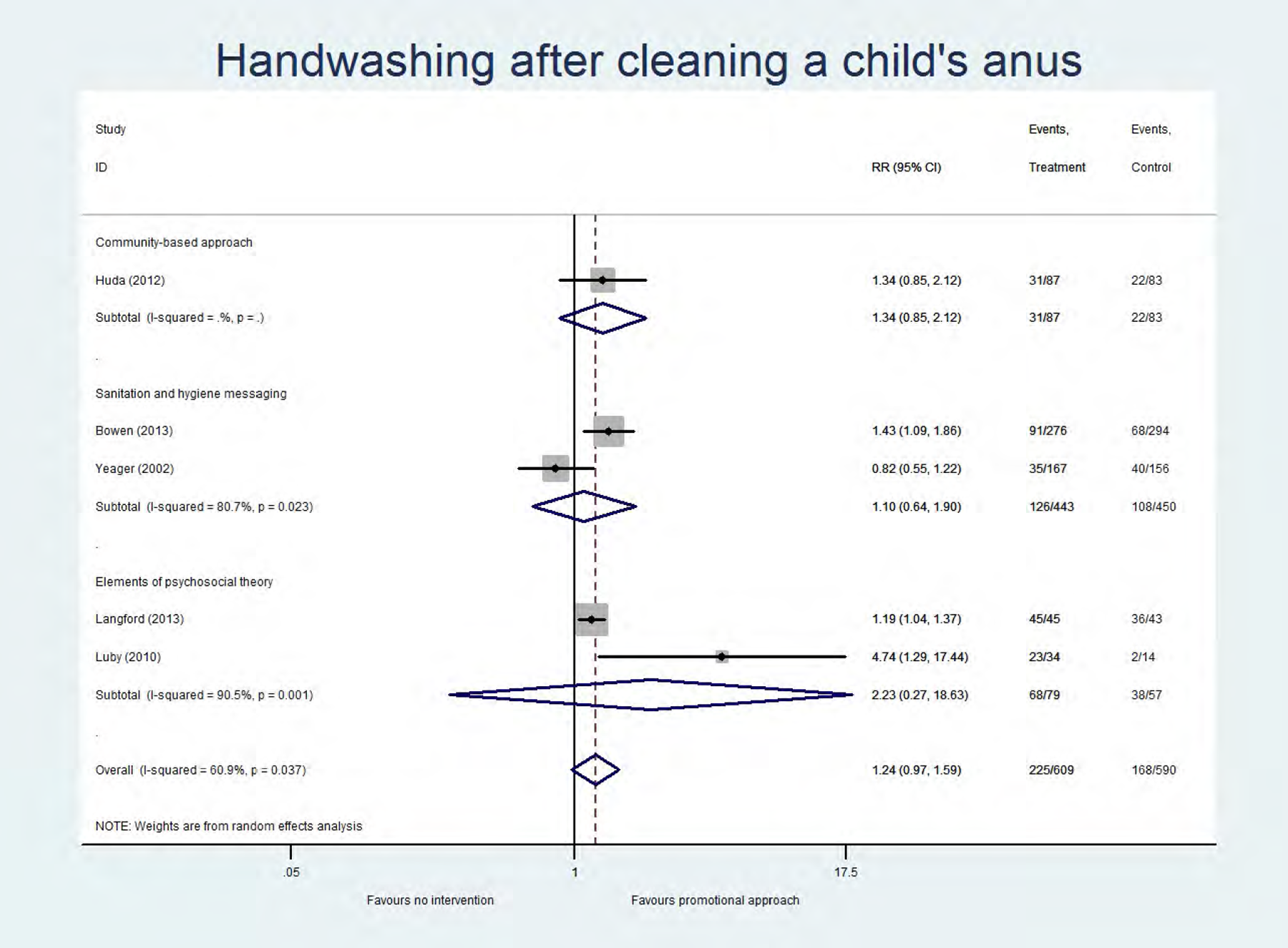
Analysis
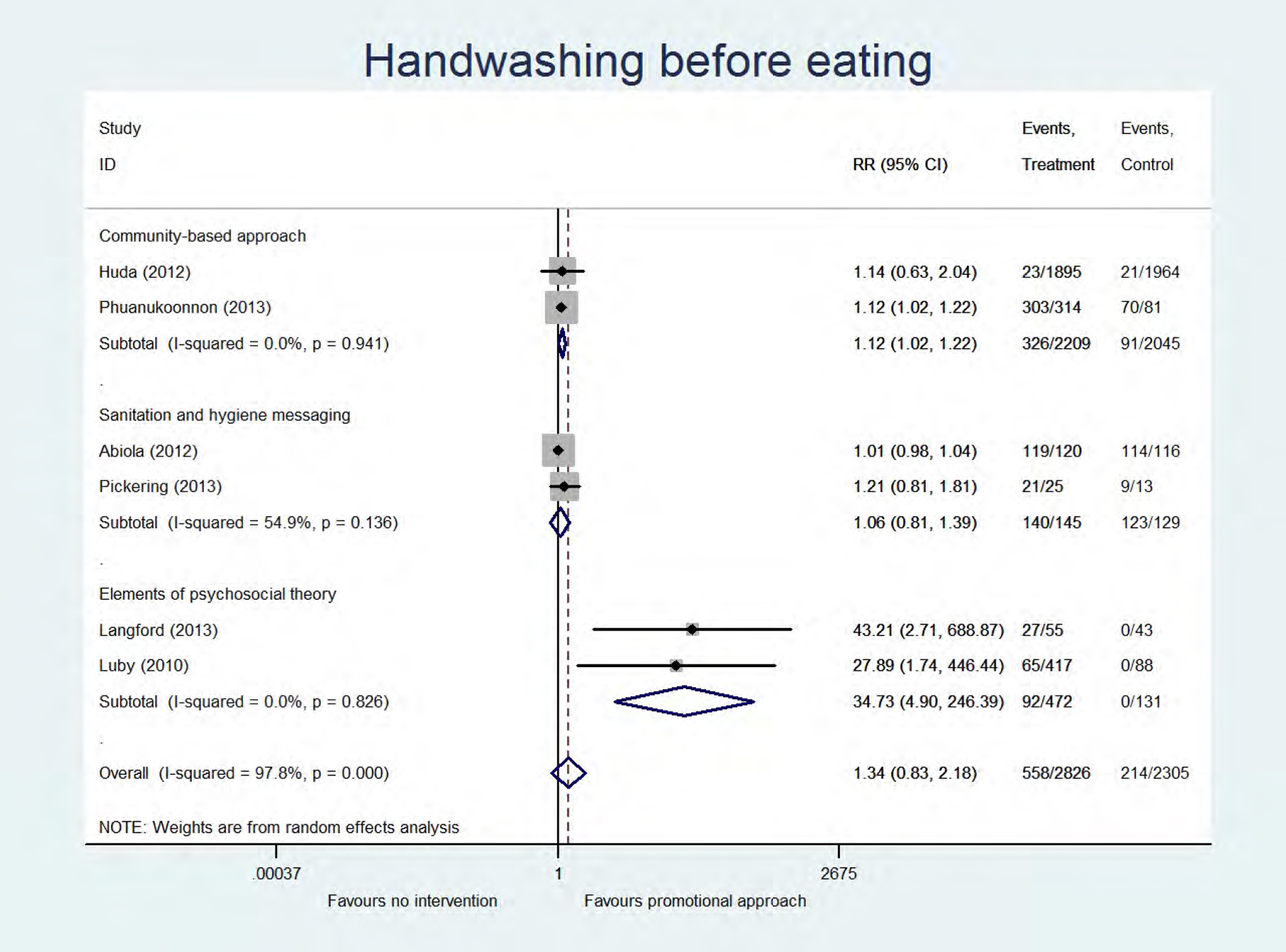
Analysis
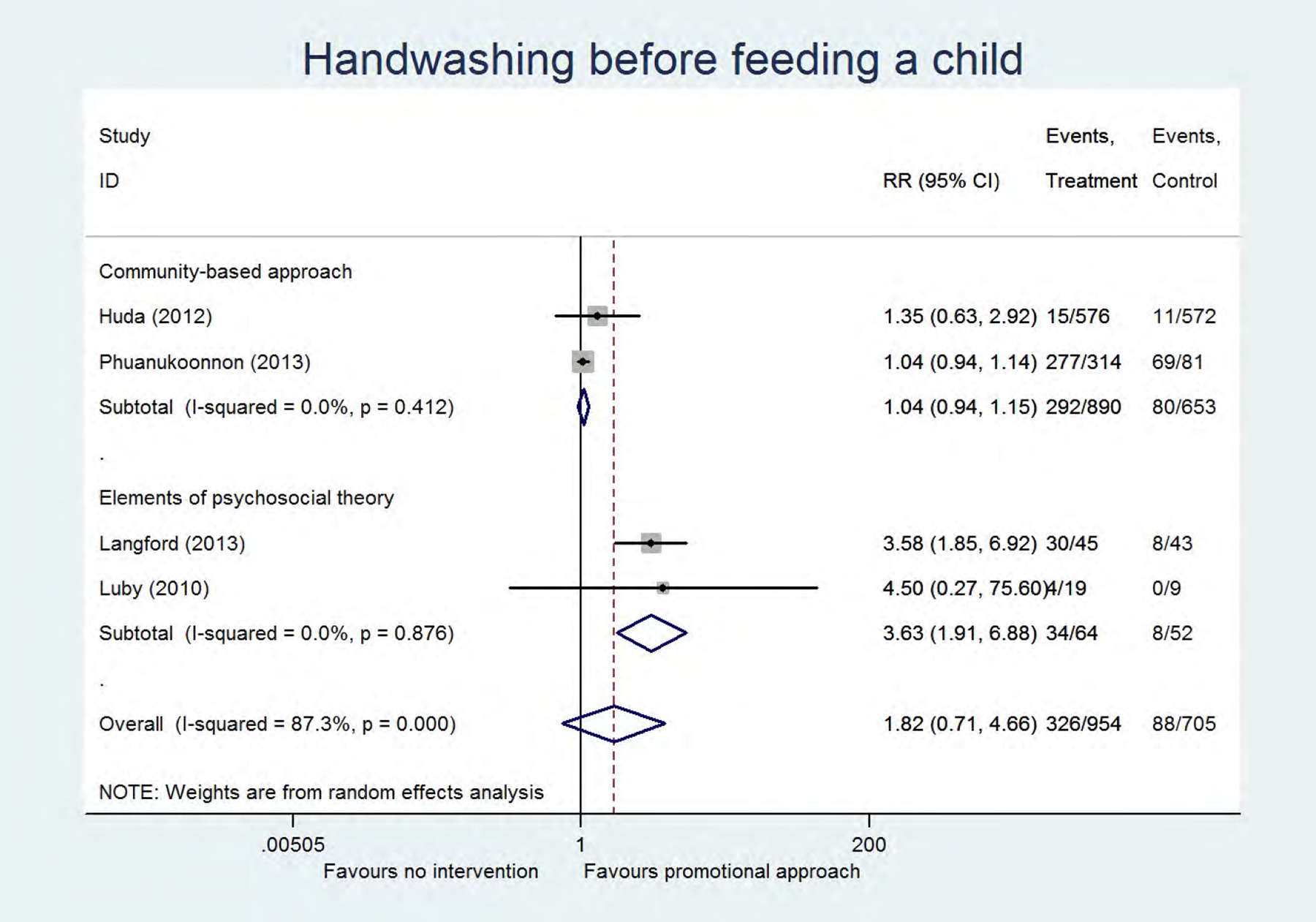
Analysis
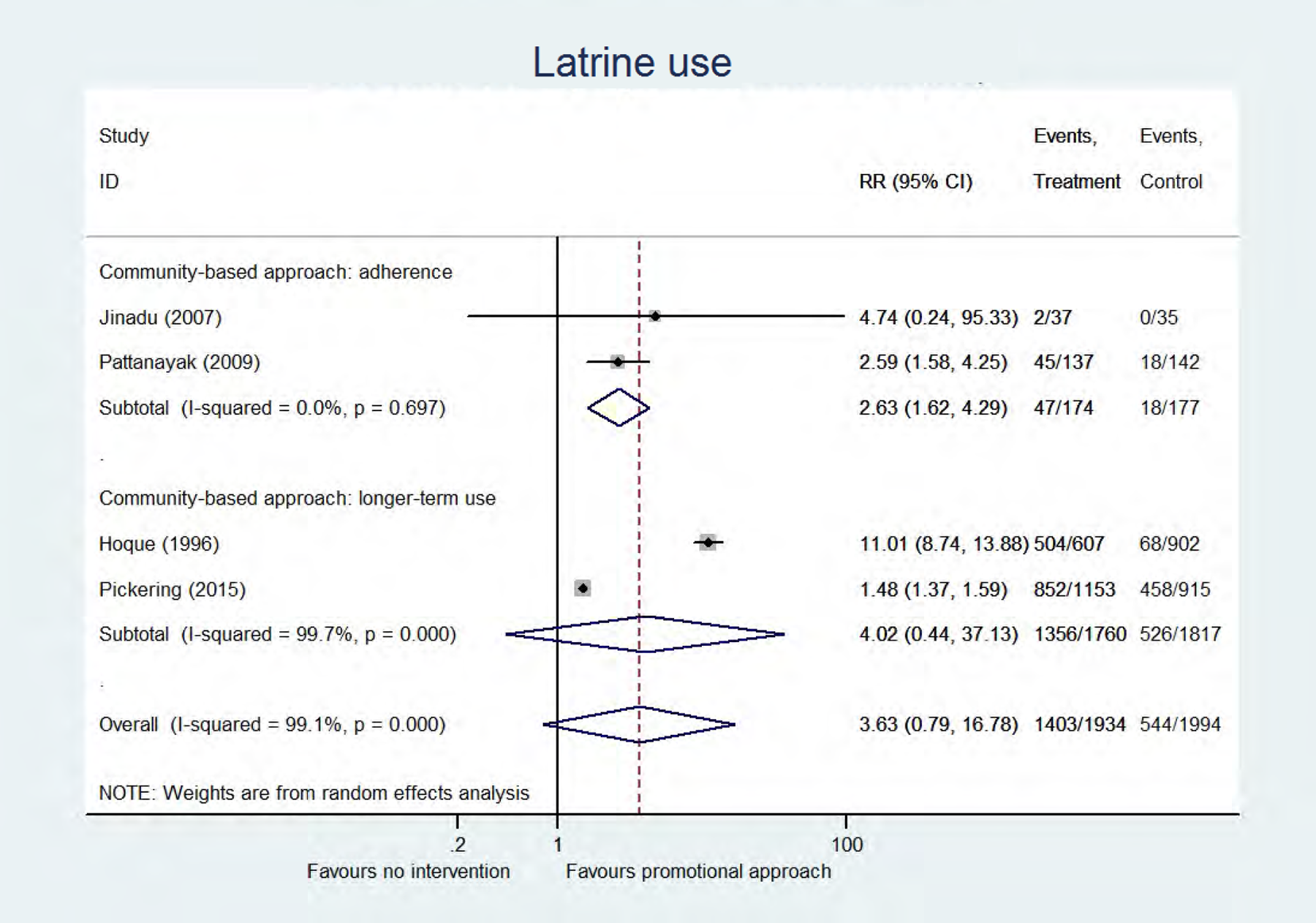
Analysis
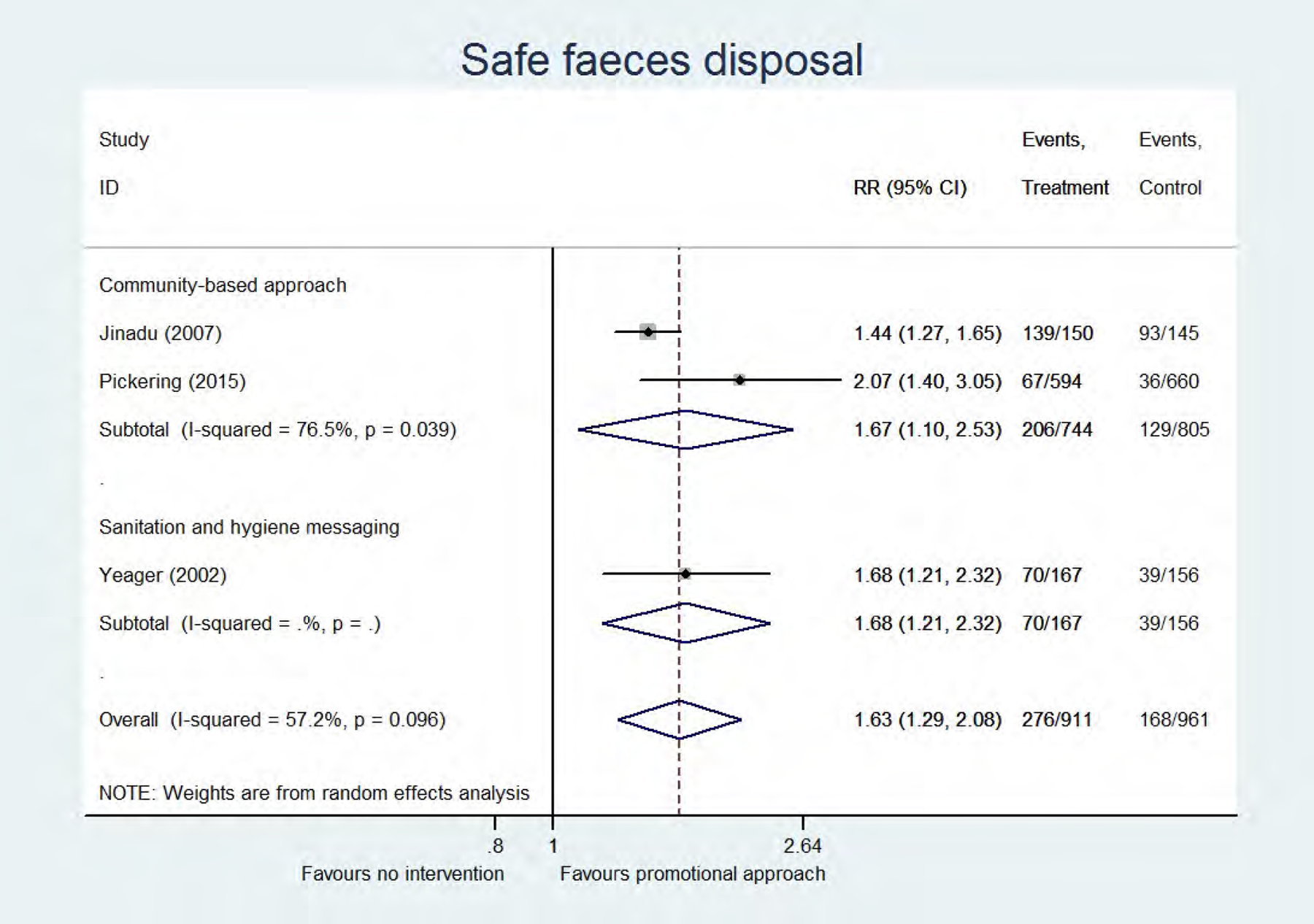
Analysis
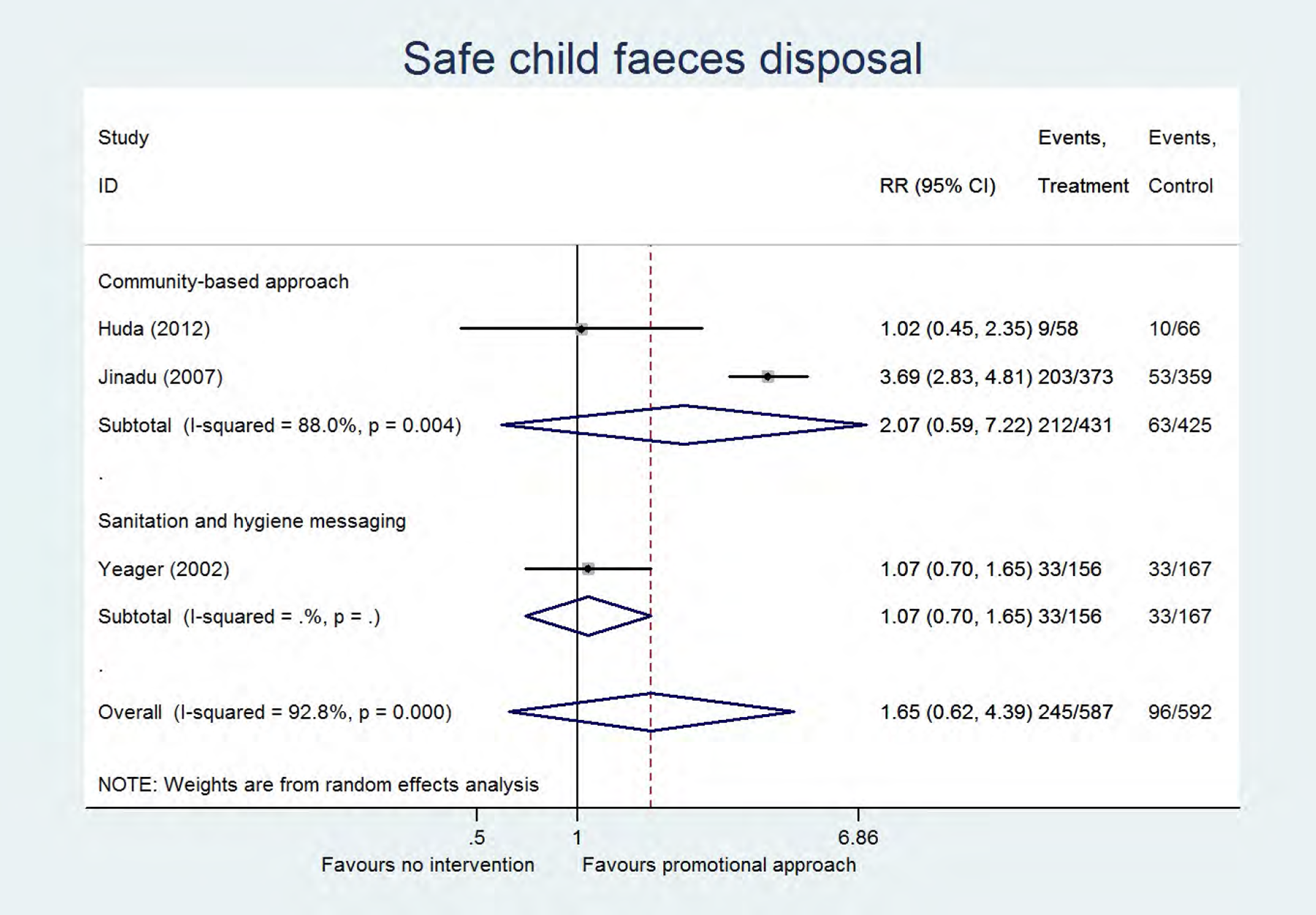
Analysis
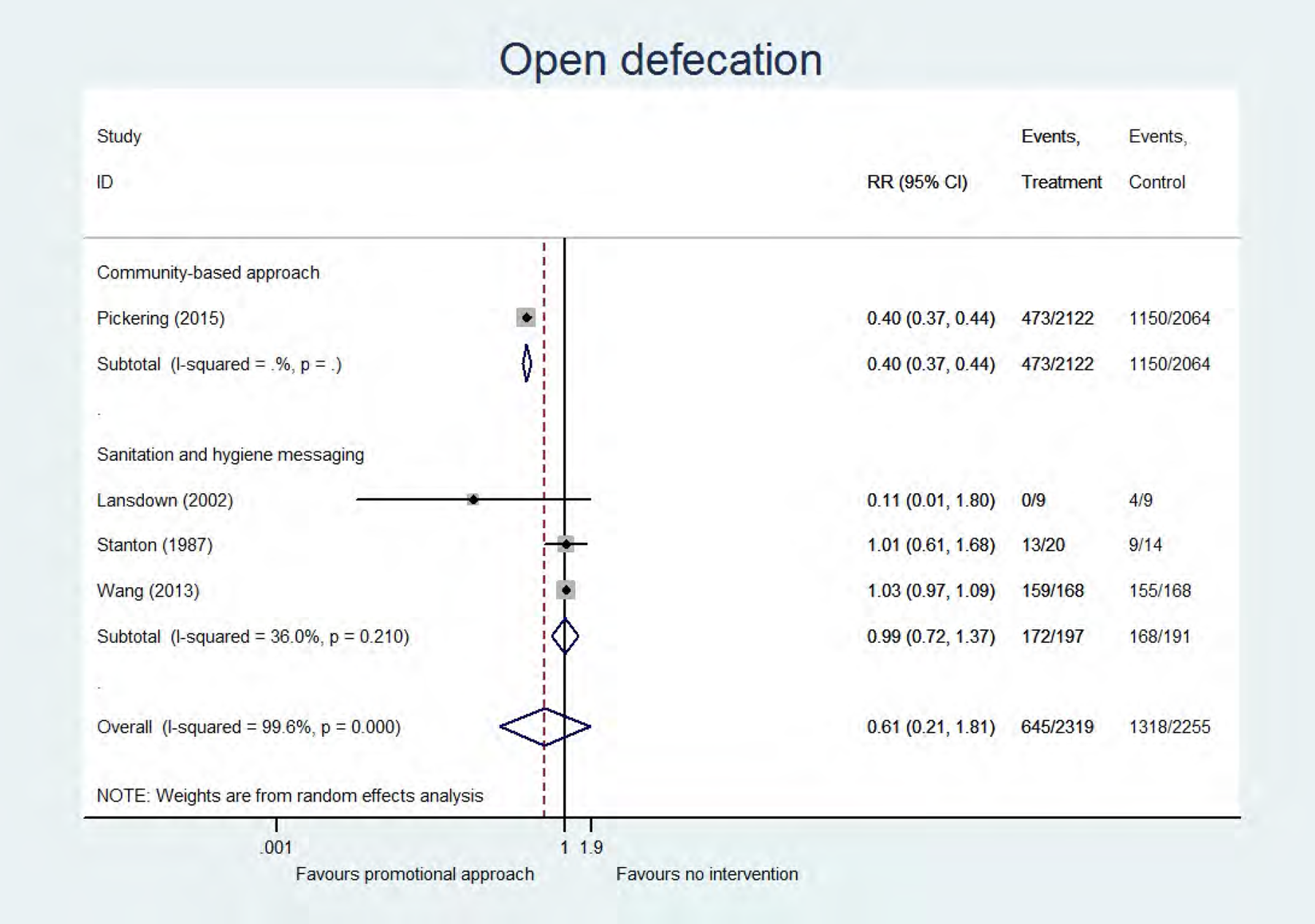
Analysis
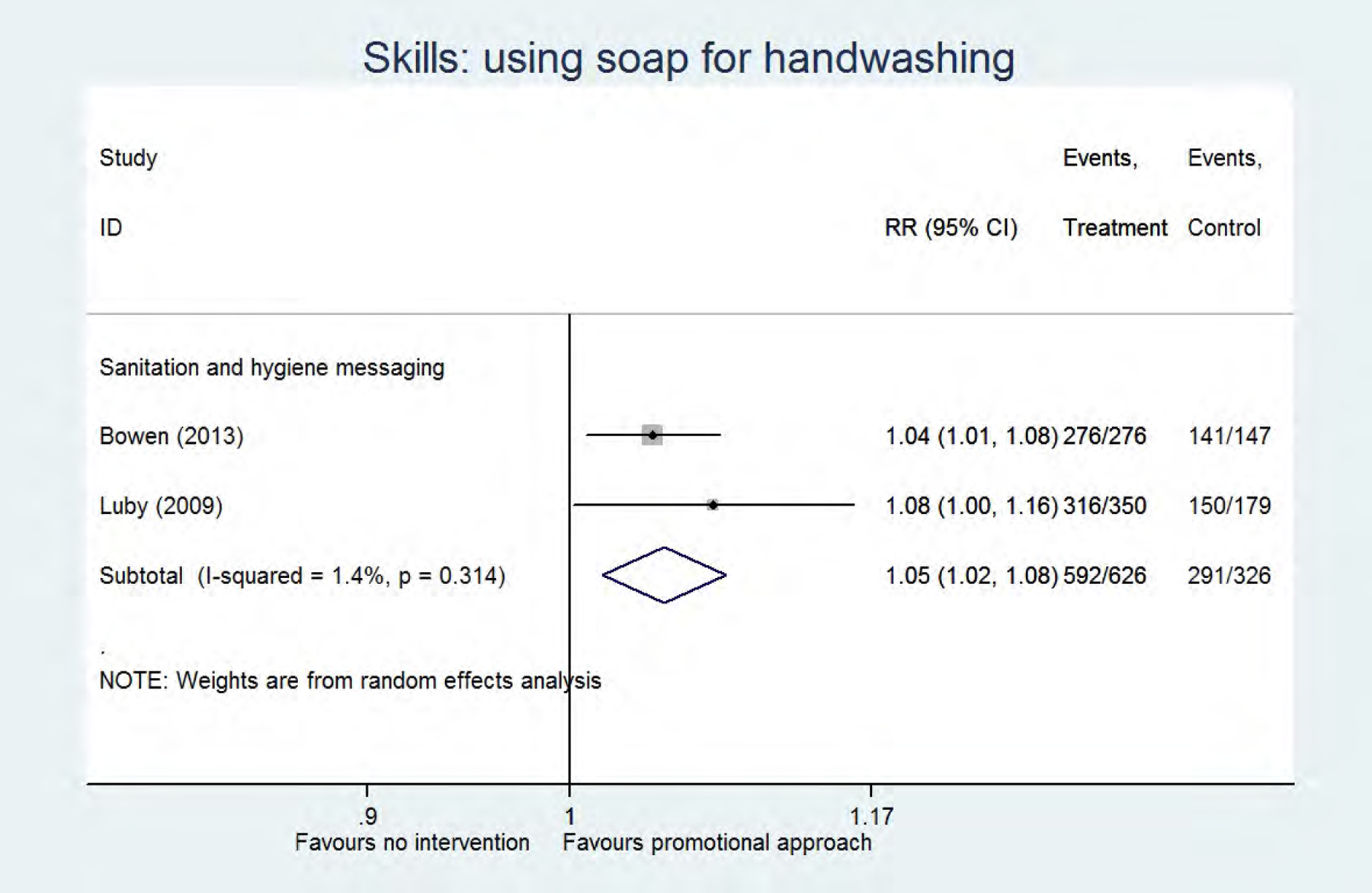
Analysis
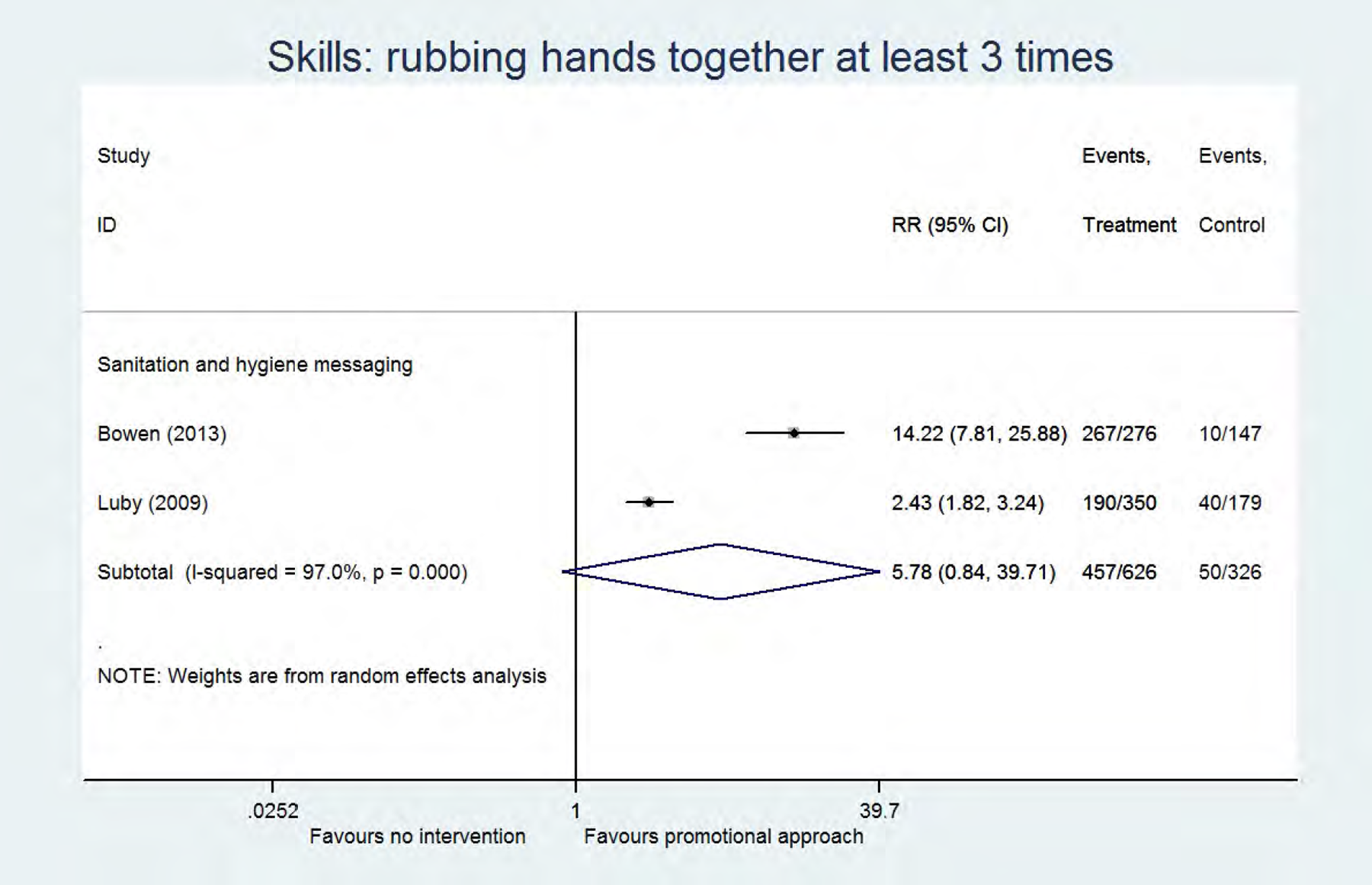
Analysis
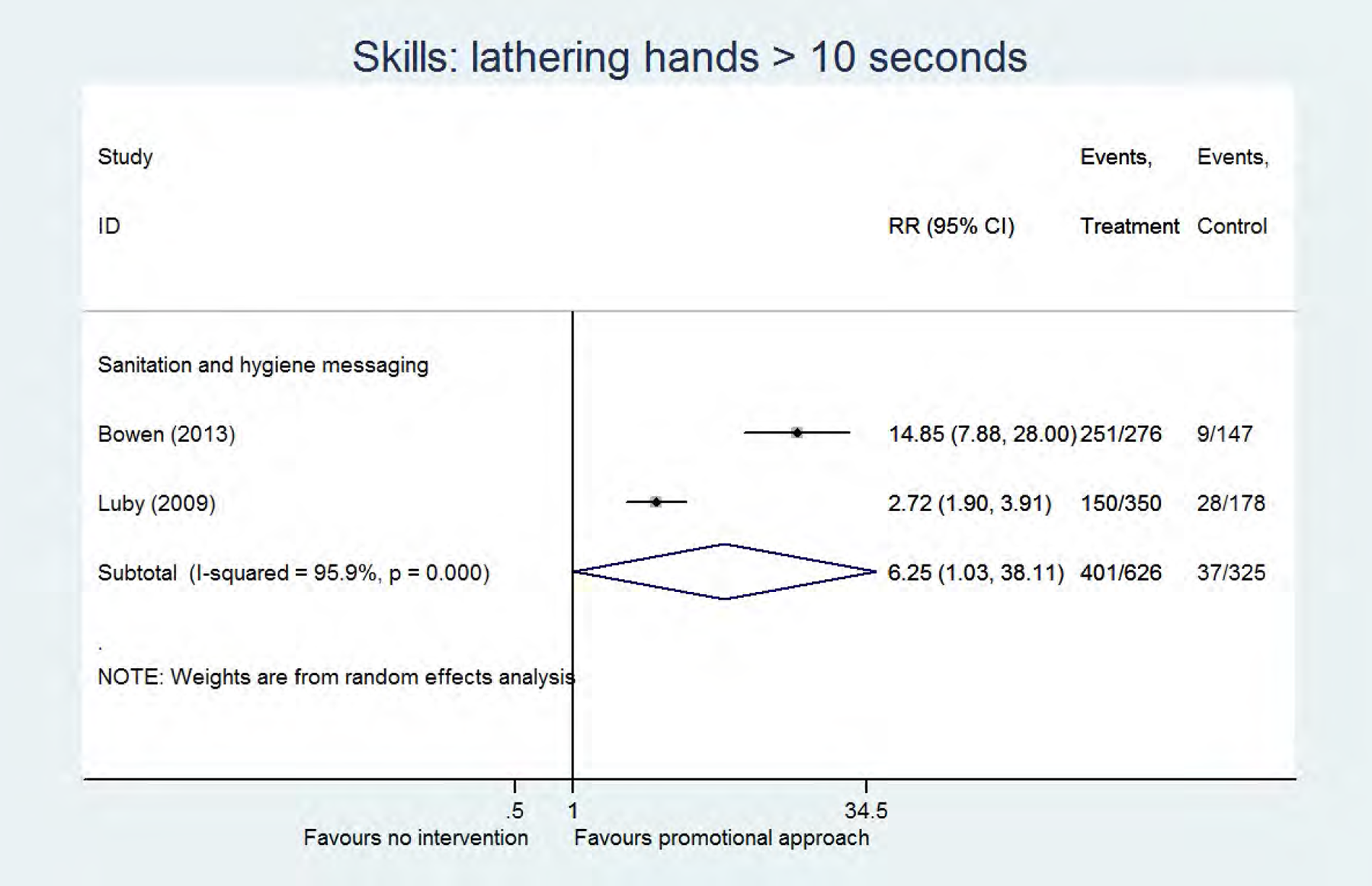
Analysis
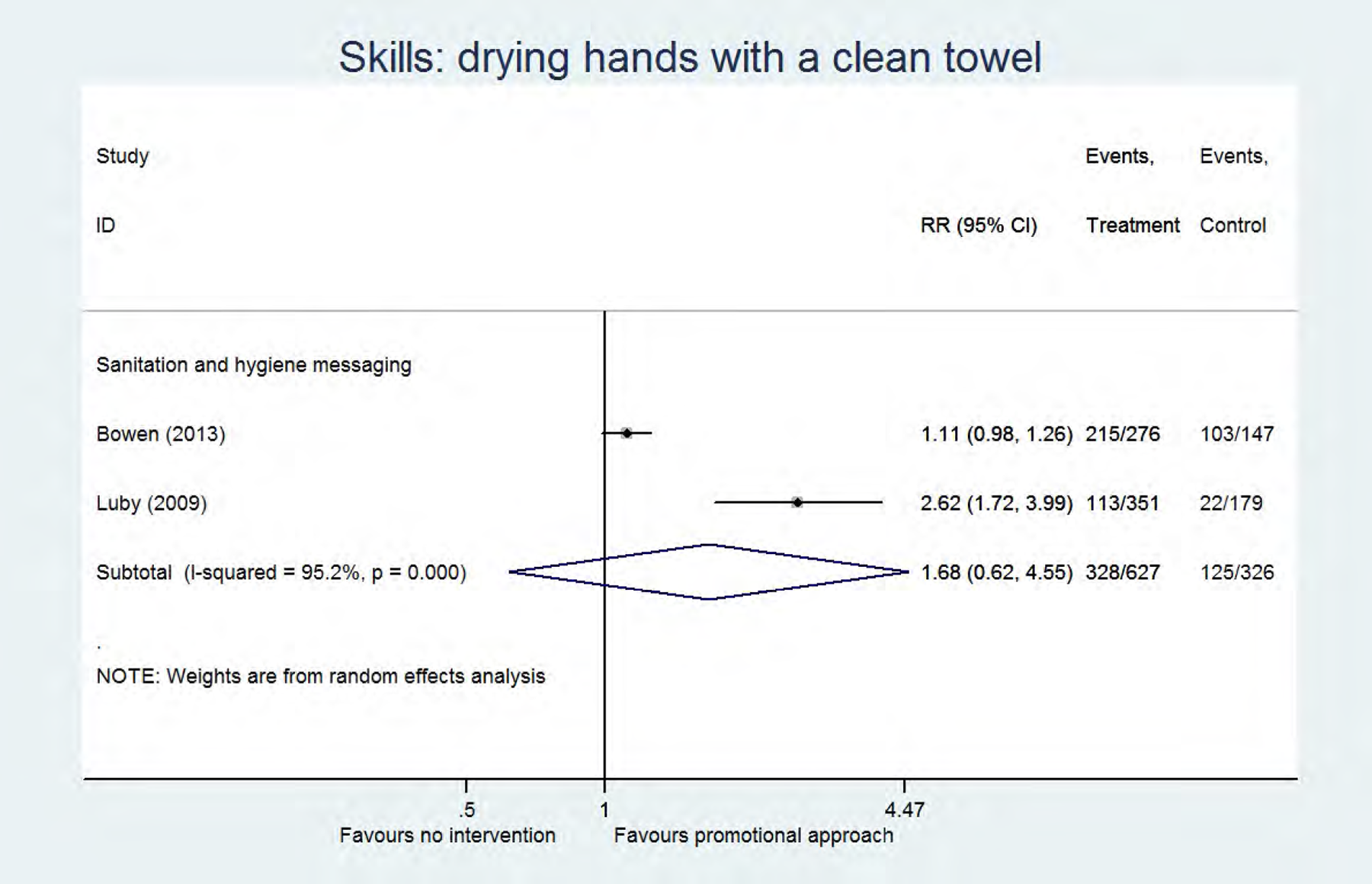
Analysis
Assessment of the certainty of evidence for handwashing after toilet use (pooled data), community-based approach vs no promotional approach
1 cluster RCT (Huda 2012) and 1 quasi-RCT (Phuanukoonnon 2013)
Selection bias (Huda 2012), attrition, detection and reporting bias (Phuanukoonnon 2013)
Assessment of the certainty of evidence for handwashing before cooking (pooled data), sanitation and hygiene messaging vs no promotional approach
2 cluster RCTs
detection bias (Bowen 2013) and attrition bias (Stanton 1987)
low number of events
Assessment of the certainty of evidence for handwashing before cooking (pooled data), elements of psychosocial theory vs no promotional approach
1 cluster RCT (Luby 2010) and 1 quasi-RCT (Langford 2013)
Detection bias (Langford 2013), attrition bias (Langford 2013 and Luby 2010), reporting bias (Langford 2013 and Luby 2010) and other bias (Langford 2013)
Low number of events
Assessment of the certainty of evidence for handwashing before eating (pooled data), community-based approach vs no promotional approach
1 cluster RCT (Huda 2012) and 1 quasi-RCT (Phuanukoonnon 2013)
Selection bias (Huda 2012), attrition, detection and reporting bias (Phuanukoonnon 2013)
Assessment of the certainty of evidence for handwashing before eating (pooled data), elements of psychosocial theory vs no promotional approach
1 cluster RCT (Luby 2010) and 1 quasi-RCT (Langford 2013)
Attrition and reporting bias (Langford 2013 and Luby 2010) and detection and other bias (Langford 2013)
Low number of events
Assessment of the certainty of evidence for handwashing before feeding a child (pooled data), community-based approach vs no promotional approach
1 cluster RCT (Huda 2012) and 1 quasi-RCT (Phuanukoonnon 2013)
Selection bias (Huda 2012), attrition, detection and reporting bias (Phuanukoonnon 2013)
Low number of events
Assessment of the certainty of evidence for handwashing before feeding a child (pooled data), elements of psychosocial theory vs no promotional approach
1 cluster RCT (Luby 2010) and 1 quasi-RCT (Langford 2013)
Attrition and reporting bias (Langford 2013 and Luby 2010) and detection and other bias (Langford 2013)
Low number of events
Assessment of the certainty of evidence for latrine use (adherence) (pooled data), community-based approach vs no promotional approach
1 RCT (Jinadu 2007) and 1 cluster RCT (Pattanayak 2009)
Reporting bias (Jinadu 2007) and attrition bias (Pattanayak 2009)
Low number of events
Assessment of the certainty of evidence for open defecation (pooled data), sanitation and hygiene messaging vs no promotional approach
1 RCT (Lansdown 2002) and 2 cluster RCT's (Stanton 1987 and Wang 2013)
Detection bias (Lansdown 2002), attrition bias (Stanton 1987) and reporting bias (Lansdown 2002 and Wang 2013)
Low number of events
Assessment of the certainty of evidence for skills, using soap for handwashing (pooled data), sanitation and hygiene messaging vs no promotional approach
2 cluster RCT's
Detection bias (Bowen 2013) and attrition bias (Luby 2009)
We also expressed the effect measures as Risk Differences (RD), showing the absolute effect, instead of Risk Ratios (RR) (Table 15).
Risk ratio and risk difference
All risk ratios and risk differences are presented as Cochran-Mantel-Haenszel Estimate, [95% CI]. RR: Risk Ratio; CI: Confidence Interval; RD: Risk Difference; I2: heterogeneity; *p≤0.05
We performed a sensitivity analysis for the use of incentives as part of the promotional approach (see Table 16, forest plots available upon request). Three studies made use of financial or non-financial incentives, including providing a modest salary to the secondary implementer as part of a community-based approach (Huda et al., 2012), providing small subsidies to the households as part of a community-based approach (Pattanayak et al., 2009), and providing a bar of soap as part of a theory-based approach (Langford & Panter-Brick, 2013).
Risk ratios in studies describing programmes including incentives versus programmes without use of incentives
All risk ratios are presented as Cochran-Mantel-Haenszel Estimate, [95% CI]. RR: Risk Ratio; CI: Confidence Interval; I2: heterogeneity; *p≤0.05
In Table 16 we present the findings of the studies describing programmes with incentives versus studies where no incentives were used. Focussing on findings from studies with low heterogeneity (< 50%), we found: (1) statistically significant improvement in handwashing after toilet use (RR 3.62, 95% CI [2.20, 5.93], elements of psychosocial theory), handwashing before eating (RR 1.12, 95% CI [1.02, 1.22], community-based approach) and safe child faeces disposal (RR 1.44, 95% CI [1.27, 1.65], community-based approach) when using programmes without incentives, while this was not the case for similar programmes using incentives; (2) for handwashing before cooking, handwashing after cleaning a child's anus and handwashing before eating, both programmes (based on elements of psychosocial theory) with and without incentives had statistically significant positive effects, but the RR was larger for the programmes without incentives; (3) programmes that used elements of psychosocial theory: statistically significant improvement in handwashing before feeding a child (RR 3.58, 95% CI [1.85, 6.92]), and in latrine use (RR 2.59, 95% CI [1.58, 4.25]) was found when using programmes making use of incentives, while this was not the case for programmes not using incentives; (4) no positive effects on handwashing after toilet use or before feeding a child were present in community-based interventions with or without incentives. Overall, the number of studies is too limited, and the type of incentives is too variable, to be able to make any firm conclusions based on these data.
In summary, because of a high degree of heterogeneity it was very difficult to make overall conclusions about the effectiveness of using any promotional approach versus no promotional approach, and about the effectiveness of a specific promotional approach. Since many other specific outcomes were measured that were not included in the meta-analyses because these were unique outcomes, we provide a more complete overview below, however without statistically pooling these.
4.3.1.2 Community-based approaches
From the 12 studies that we categorised as describing a community-based approach, 8 clearly described the approach as a formal community-based approach, and the following formal approaches were identified: community-led total sanitation (Guiteras et al., 2015b; Patil et al., 2013/2015; Pattanayak et al., 2009; Pickering et al., 2015), community-based interventions (Andrade, 2013; Jinadu et al., 2007) and community health clubs or women's groups (Waterkeyn & Cairncross, 2005; Younes et al., 2015). The other studies did not formally describe their approach as community-based approach, but clear elements of community involvement and engagement were described (Hoque et al., 1994/1996; Huda et al., 2012; Kochurani et al., 2009; Phuanokoonnon et al., 2013). One study was a school-based study (Kochurani et al., 2009), and Andrade (2013) worked at household, community and school level at the same time. All but one study had a sanitation component in the intervention: four studies only focused on sanitation, 7 studies looked at a mixed intervention (all WASH components in 6 cases, water supply/water quality and sanitation in one case) component, and only one study contained a handwashing only programme (see Figure 6).
Below we narratively describe the findings for the different outcome types. We specifically mention when the programme only consisted of a sanitation intervention, or handwashing intervention. In all other cases the programme contained all WASH elements. Behaviour change: handwashing (Analysis 14). One study, implementing a handwashing only intervention, measured handwashing at key times during the intervention period (“uptake”) (Younes 2015). A significant increase in handwashing with soap before food preparations (RR 4.31, 95% CI [3.40, 5.45]), or before feeding a child was measured (RR 2.83, 95% CI [2.50, 3.20]) (certainty of evidence: low (Table 17)) (Younes et al., 2015). In two studies adherence outcomes were measured. In a sanitation only study with a moderate risk of bias a statistically significant increase in handwashing after cleaning children's faeces, and after defecation was found (RR 2.23, 95% CI [1.21, 4.10]) (Jinadu et al., 2007). A significant increase in “handwashing before eating” was shown (RR 1.12, 95% CI [1.02, 1.22]) in a smaller experimental study with serious risk of bias, however a significant change could not be shown for 5 other key times (Phuanokoonnon et al., 2013). The certainty of evidence for the adherence outcomes was found to be low (Table 18). In addition, three studies measured longer-term use outcomes (Huda et al., 2012; Pickering et al., 2015; Kochurani et al., 2009). The community-based intervention, only containing a sanitation component, significantly improved handwashing with soap (MD 0.50, 95% CI [0.33, 0.67]) (Pickering et al., 2015). Kochurani et al. (2009), a school level study, found that the community-based intervention significantly increased the frequency of handwashing before eating (96% versus 61%, n=7,835; p<0.0001). However, a significant effect in handwashing at 7 different key times (including handwashing before eating) could not be demonstrated in an experimental study with serious risk of bias (Huda et al., 2012). The level of evidence for handwashing at longer term was found to be very low (Table 19). Behaviour change: latrine use (Analysis 15). A statistically significant increase in latrine use during the intervention period (“uptake”) was measured (RR 1.88, 95% CI [1.39, 2.55]) (Waterkeyn & Cairncross, 2005). In Hoque et al. (1994/1996) it was shown that latrine use after the intervention increased by 89%, however no standard deviations were provided, so it was not possible to calculate confidence intervals. Adherence outcomes were measured in two different experimental studies, describing a sanitation only intervention, and a significant increase in overall latrine use (RR 2.59, 95% CI [1.58, 4.25]), and latrine use in children up to 24 months (RR 7.95, 95% CI [4.72, 13.40]) was shown (Pattanayak et al., 2009; Jinadu et al., 2007), however no difference in latrine use in children between 25 and 60 months could be shown (RR 4.74, 95% CI [0.24, 95.33]) (Jinadu et al., 2007). The adherence outcomes had a low certainty of evidence (Table 20). In the longer term statistically significantly increased overall latrine use (RR 1.48, 95% CI [1.37, 1.59]), latrine use by males (RR 10.40, 95% CI [7.59, 14.26]), latrine use by females (RR 11.70, 95% CI [8.36, 16.37]), and potty use by children (RR 3.28, 95% CI [2.90, 3.71]) was shown (Hoque et al., 1994/1996; Pickering et al., 2015). The certainty of evidence for the longer-term outcomes was found to be low (Table 21). The study by Pickering et al. (2015) was a sanitation-only intervention, while Hoque et al. (1994/1996) combined sanitation with a water supply/water quality intervention. Behaviour change: safe faeces disposal (Analysis 16). Two studies measured outcomes during the study period (“uptake”) (Waterkeyn & Cairncross, 2005; Patil et al., 2013/2015). A statistically significant increase of “not disposing faeces in the open” (RR 2.41, 95% CI [1.99, 2.90]) was demonstrated in a quasi-experimental study (Waterkeyn & Cairncross, 2005). No difference in the presence of child faeces in the yard was shown (Waterkeyn & Cairncross, 2005). Patil et al. (2013/2015), describing a sanitation-only intervention, reported this outcome result as means, but no standard deviations were given. From the paper, the ITT adjusted difference between intervention and control was 0.075, 95% CI [0.036, 0.113] for child faeces disposal (in favour of the community-based intervention) and 0.019, 95% CI [-0.026, 0.065] for “no faeces observed in living area”, the latter being non-significant. The certainty of evidence for the uptake outcomes was assessed as very low (Table 22). Significant outcomes were also shown in the period less than 12 months after the programme period (“adherence”): child faeces disposal (RR 2.16, 95% CI [1.60, 2.91]) and no faeces lying around (RR 1.44, 95% CI [1.27, 1.65]), in a study implementing a sanitation-only intervention (Jinadu et al., 2007). The certainty of evidence for the adherence outcomes was assessed as moderate (Table 23). In the longer term a significant increase in not leaving human faeces in the compound was shown in an experimental study (sanitation-only) with moderate risk of bias (RR 2.07, 95% CI [1.40, 3.05]) (Pickering et al., 2015), but a significant effect on child faeces disposal could not be demonstrated in an experimental study with serious risk of bias (RR 1.02, 95% CI [0.45, 2.35]) (Huda et al., 2012). The certainty of evidence for longer-term outcomes was found to be low (Table 24). Behaviour change: open defecation (Analysis 17). One experimental study, describing a sanitation-only programme, measured outcomes during the study period (“uptake”) (Patil et al., 2013/2015). The study reported this outcome result as means, but no standard deviations were given. The ITT adjusted difference between intervention and control was -0.087, 95% CI [-0.135, -0.038] for men, -0.091, 95% CI [-0.141, -0.041] for women and -0.054, 95% CI [-0.088, -0.020] for children, thus the community-based intervention significantly reduced open defecation in men, women and children. The certainty of evidence for the uptake outcomes was moderate (Table 25). One study, implementing a sanitation-only intervention, measured adherence outcomes, and found a statistically significant decrease of open defecation in case of a latrine promotion program combined with use of subsidies (MD -9.00, 95% CI [-13.70, -4.30]) or a combination of subsidies and a supply intervention (MD -9.00, 95% CI [-14.10, -3.90]). No significant effect was shown in case of the supply intervention alone (MD -2.50, 95% CI [-10.73, 5.73]) (Guiteras et al., 2015b). The certainty of evidence for the adherence outcomes was found to be moderate (Table 26). Three studies measured open defecation in the longer term (Guiteras et al., 2015b; Pickering et al., 2015; Kochurani et al., 2009). A statistically significant decrease in open defecation on the longer term was shown in adult women, adult men, and children younger and older than 5 years in one study with a sanitation-only intervention (Pickering et al., 2015), however this could not be shown in case of a latrine promotion program in the study by Guiteras et al. (2015b) (MD -2.10, 95% CI [-7.20, 3.00]). Kochurani et al. (2009) found that the community-based intervention in schools significantly reduced the number of girls practicing open defecation (1% versus 9%, n=7,835; p=0.004), however for boys no significant difference was found (30% versus 23%; p=0.12). Open defecation at the longer term had a certainty of evidence of very low (Table 27). Behavioural factors (Analysis 18). Three studies measured knowledge (Andrade, 2013; Kochurani et al., 2009; Phuanukoonnon et al., 2013). Andrade (2013) showed statistically significantly increased disease transmission knowledge and knowledge of key handwashing times at 1 and 2 years following the implementation of the intervention (see forest plot). For Kochurani et al. (2009), a quasi-experimental study with critical risk of bias, there was no difference in knowledge of handwashing before eating, in a group of school boys and girls. However, the community-based intervention significantly increased knowledge of handwashing after using the toilet (girls: 100% vs 93%, p=0.001; boys: 100% vs 85%, p<0.001) and knowledge on the health advantages of handwashing (girls: 98% vs 88%, p=0.002; boys: 100% vs 77%, p<0.001). For Phuanukoonnon et al. (2013) significantly higher mean knowledge scores were observed in the community-based intervention compared to the control group, concerning the fact that diarrhoea can cause weight loss among children (3.66 versus 3.47 (out of 4), n=395, p<0.05). No effect was shown for 6 other outcomes concerning knowledge about causes and consequences of diarrhoea (Phuanukoonnon et al. 2013). Health outcomes (Analysis 19-20). A significant decrease in diarrhoea in children over 5 years old (RR 0.45, 95% CI [0.31, 0.64]) (Hoque et al., 1994/1996), and in acute respiratory tract illness (RR 0.58, 95% CI [0.45, 0.75]) (Younes et al., 2015) was shown. However, a significant effect on overall diarrhoea, and diarrhoea in children under 5 years old, could not be demonstrated in three studies (Hoque et al., 1994/1996; Pickering et al., 2015; Huda et al., 2012). In addition, using the ITT adjusted mean difference for the mean number of cases reported in the previous 7 days, Patil et al. (2013/2015) found no difference in cases of diarrhoea (-0.002, 95% CI [20.019, 0.015]) and high credible gastrointestinal illness (-0.002, 95% CI [20.024, 0.020]), but found that there were more cases of acute lower respiratory tract illness in the control group than in the intervention group (0.049, 95% CI [0.009, 0.089]) (Patil et al., 2013/2015). One experimental study with moderate risk of bias measured mortality outcomes (Pickering et al., 2015). A significant decrease of all-cause mortality and diarrhoea-related mortality was not found (Pickering et al., 2015). Influence of incentives in programs. From the 12 studies describing community-based approaches, 5 studies described the use of incentives (see Table 3), including a modest salary to the hygiene promotors (Huda et al., 2012), a motorcycle and lunch to the health technicians (Waterkeyn & Cairncross, 2005), and subsidies to households (Guiteras et al., 2015b; Patil et al., 2013, 2015; Pattanayak et al., 2009). For these studies: (1) when providing additional incentives to the secondary implementers, there was a significant improvement of latrine use and safe faeces disposal on the short term (uptake) (Waterkeyn & Cairncross, 2005), but no significant effects on handwashing and safe faeces disposal on the longer term (Huda et al., 2012, serious risk of bias); (2) when providing incentives to the recipients of the programme, a significant improvement of safe faeces disposal and open defecation (uptake, adherence), and latrine use (adherence) was found. When comparing absolute effect measures of the individual outcomes between the studies with or without use of incentives, no major differences were found. However, Guiteras (2015b) compared a community-based intervention with and without use of subsidies (i.e. latrine vouchers), and found significant better results for open defecation when subsidies were given as an additional incentive.
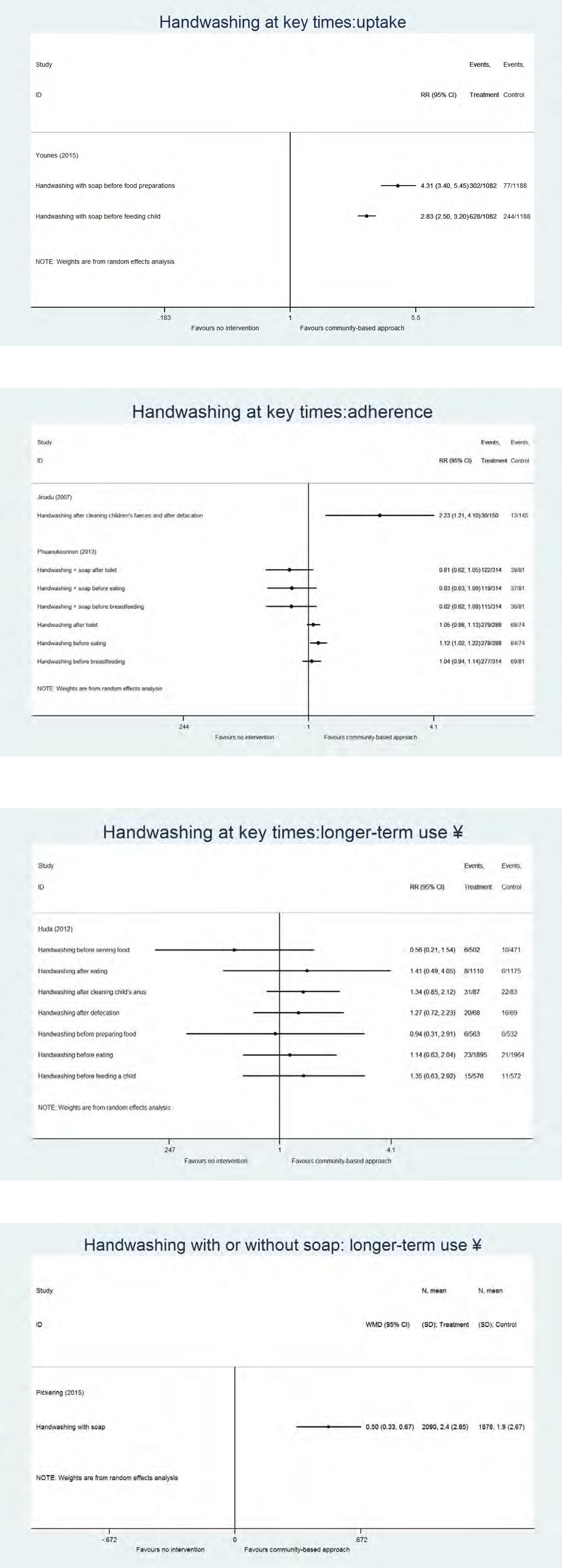
Analysis
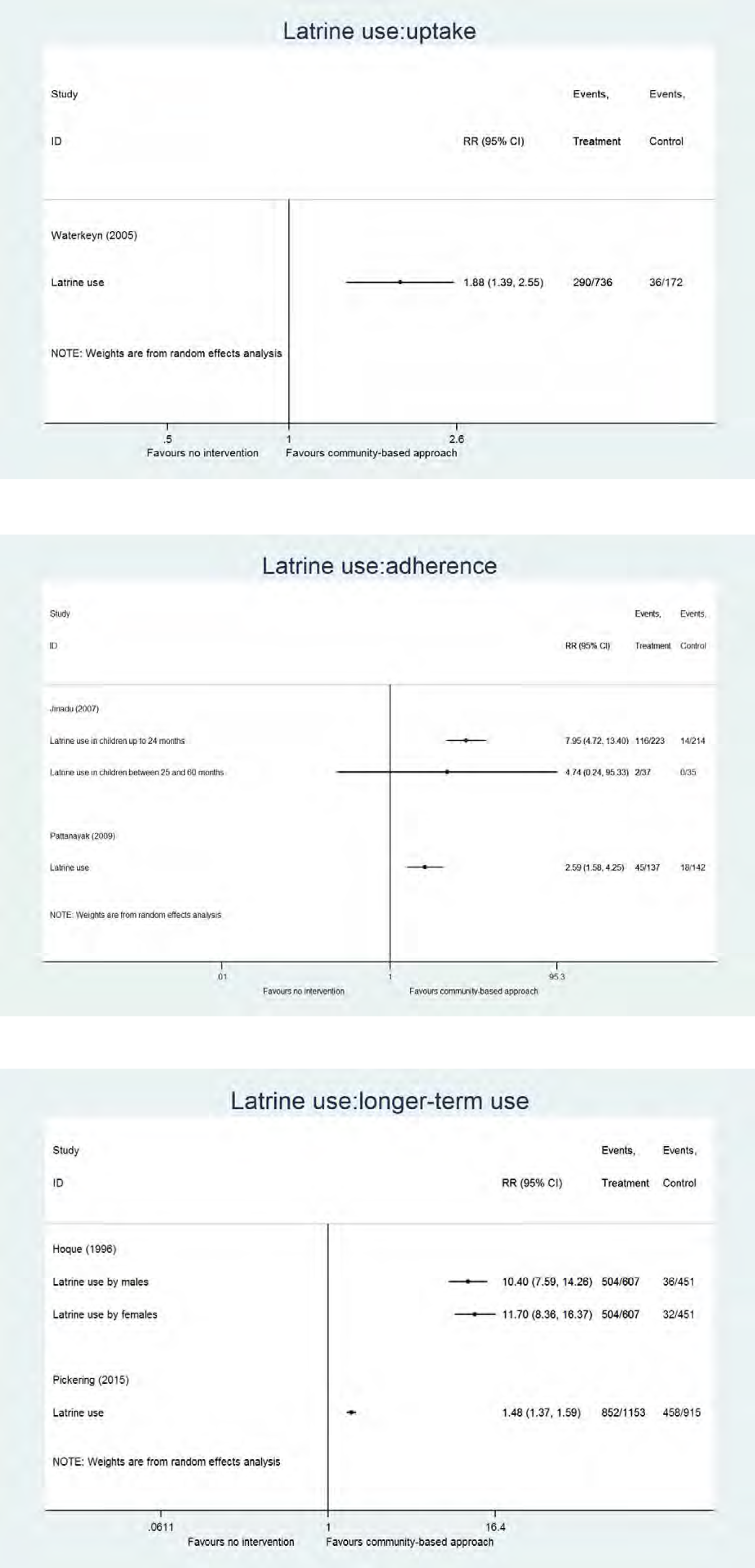
Analysis

Analysis
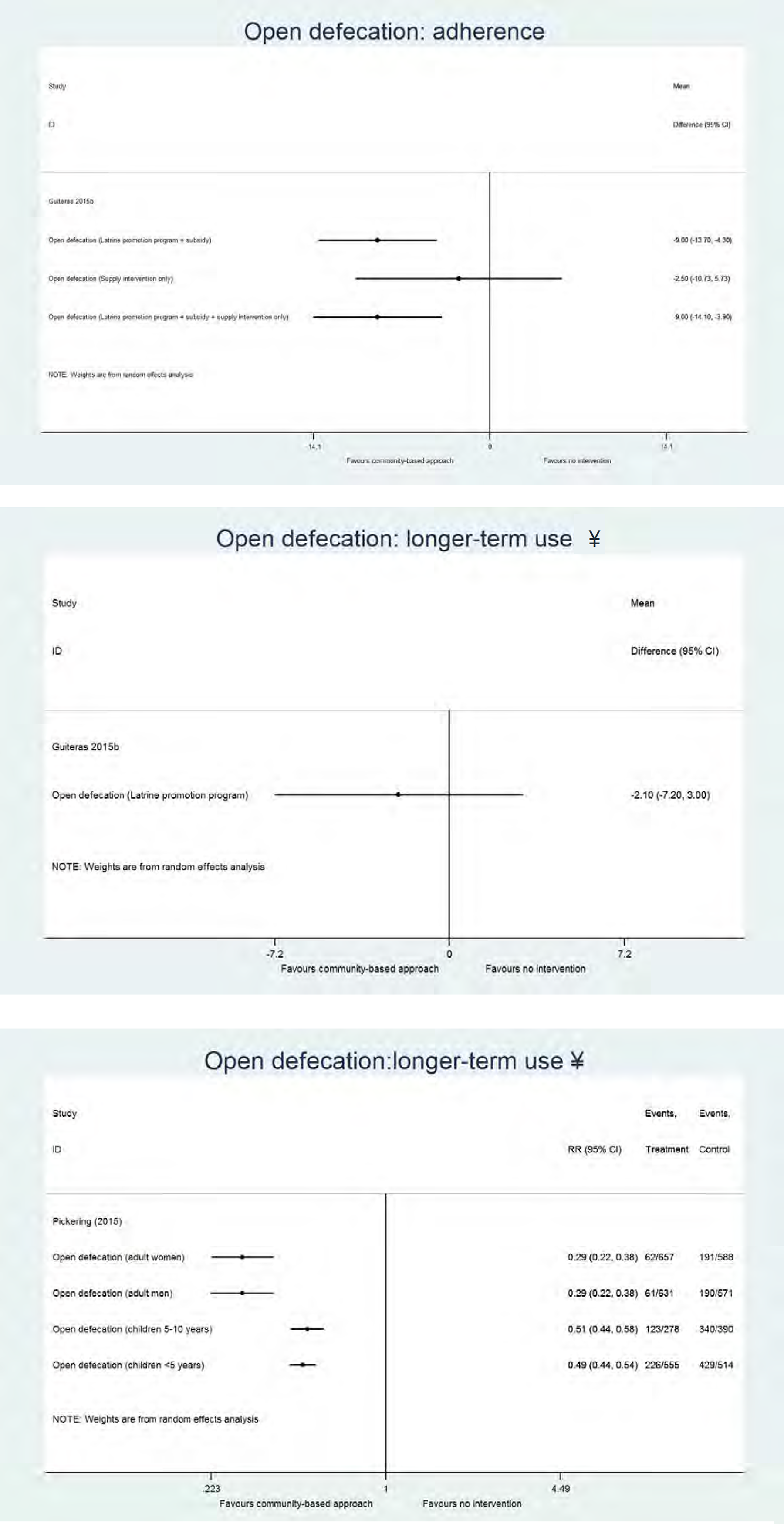
Analysis
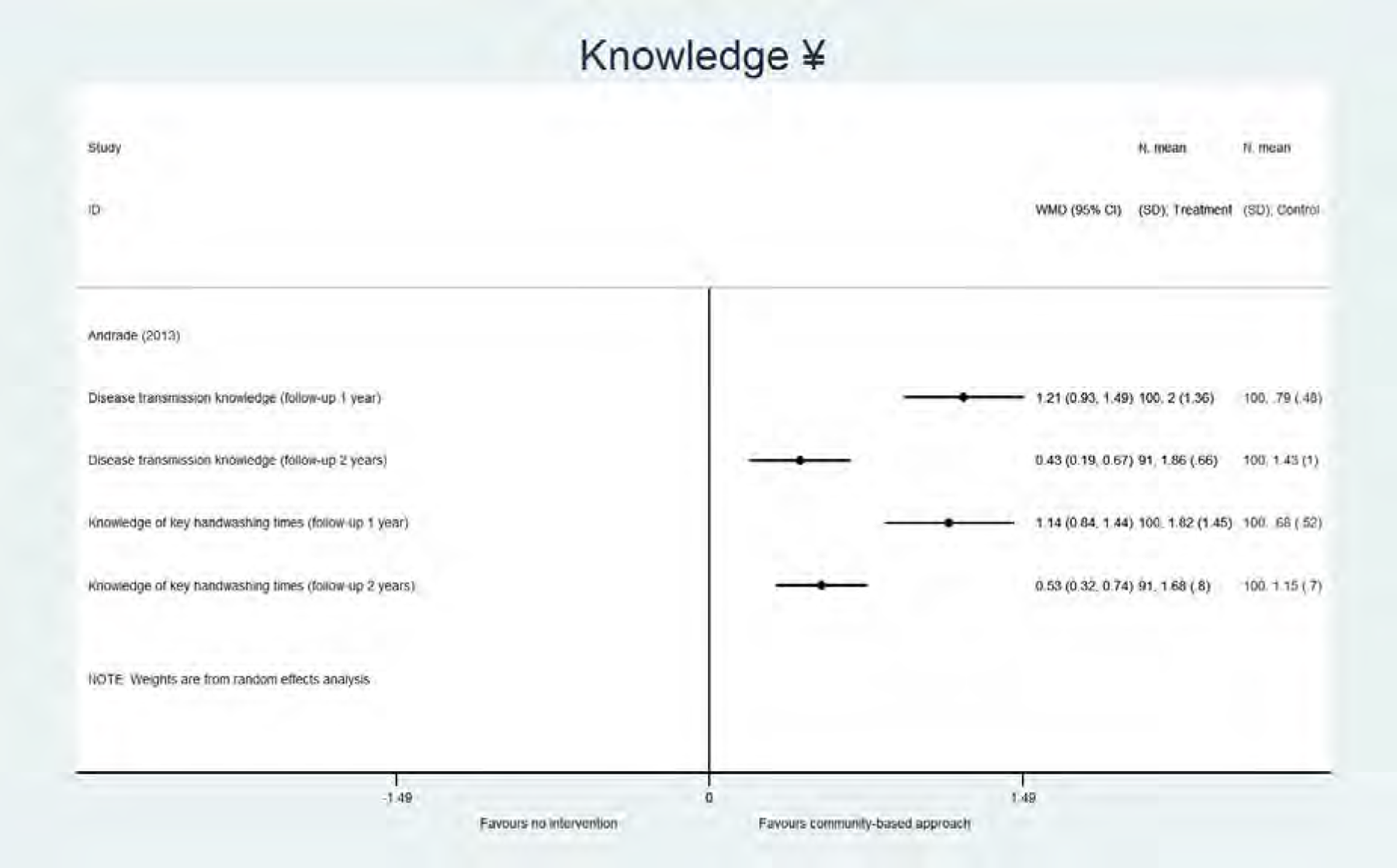
Analysis
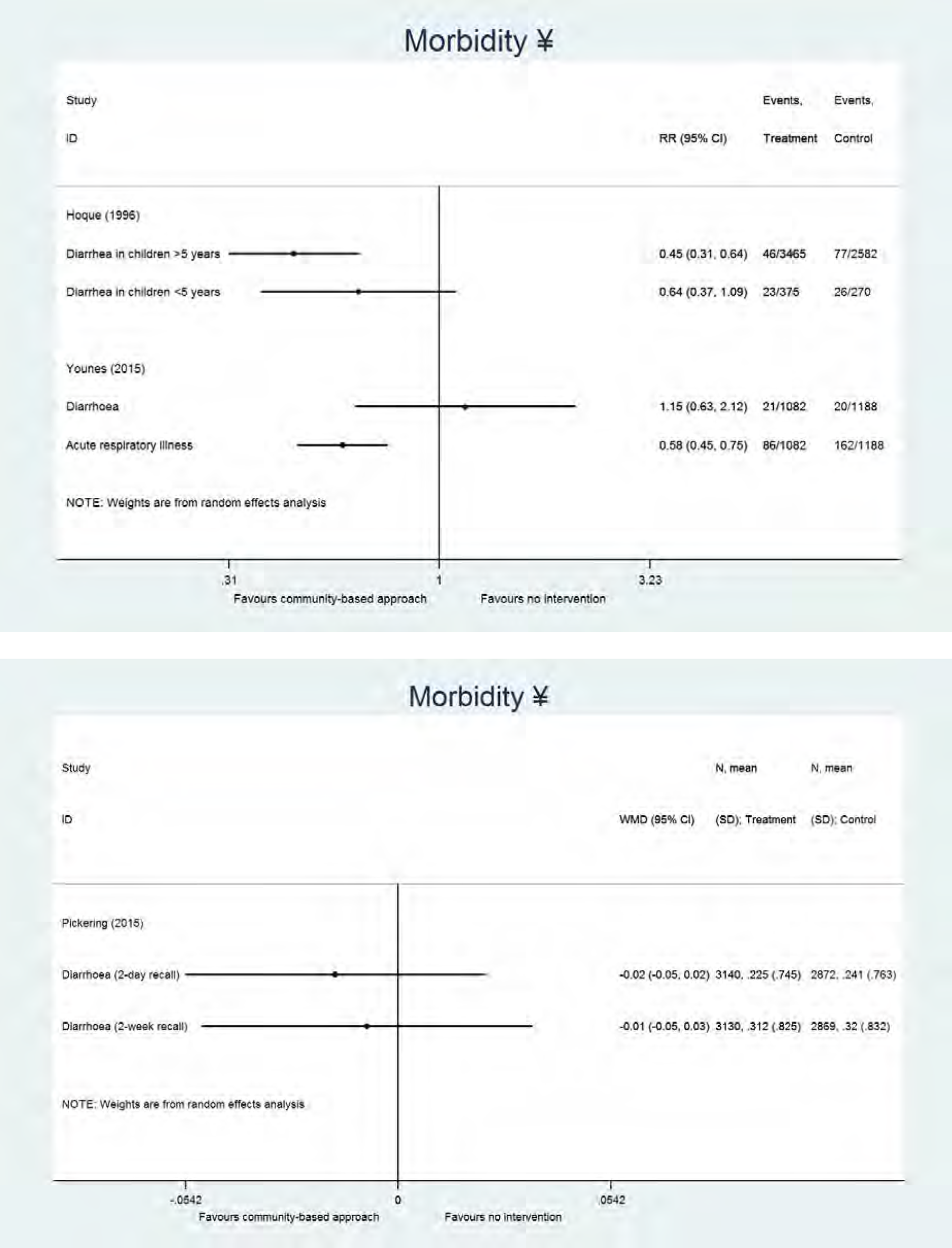
Analysis
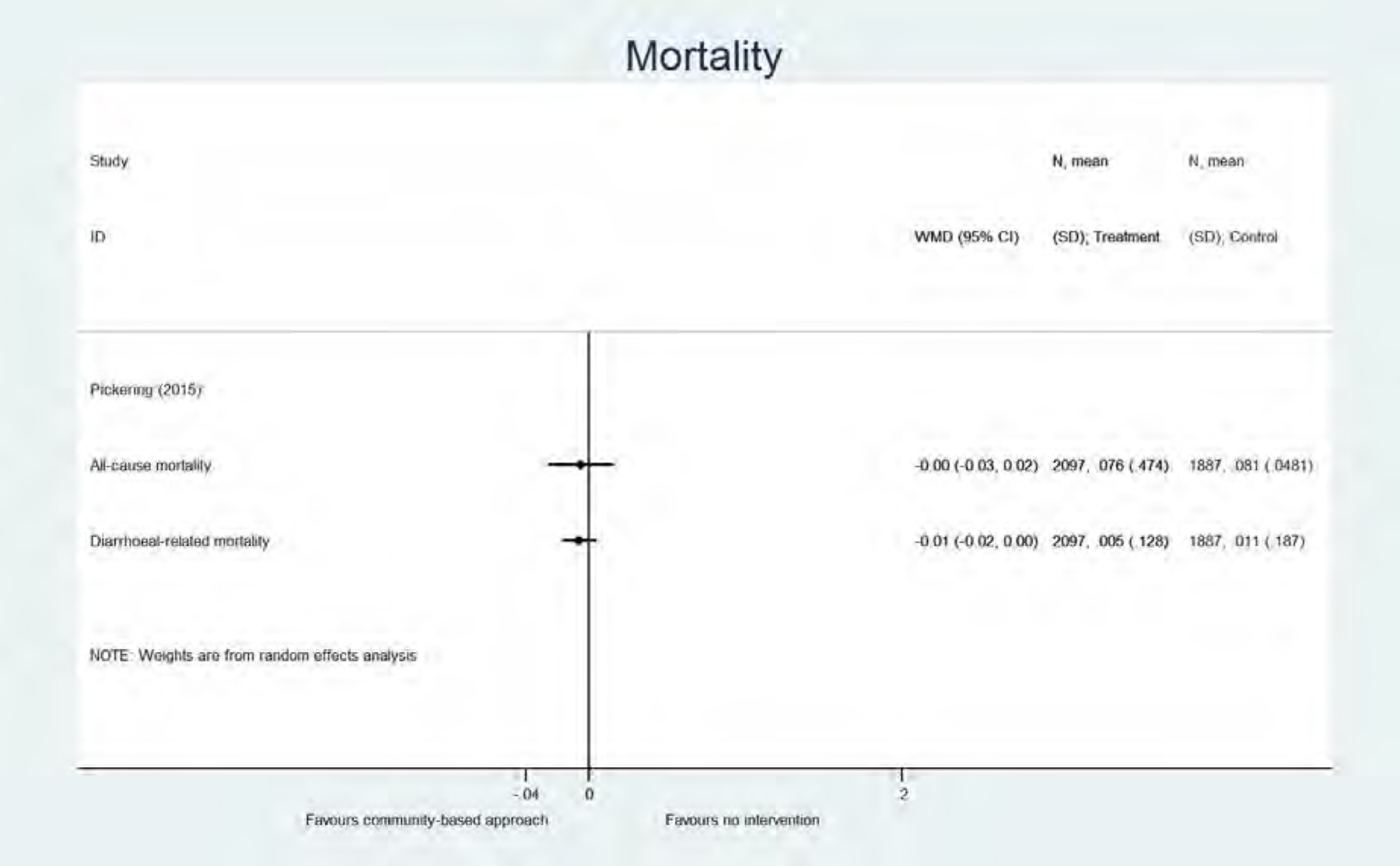
Analysis
Assessment of the certainty of evidence for handwashing at key times (uptake) (unpooled data), community-based approach vs no promotional approach
1 non-randomised controlled trial
Assessment of the certainty of evidence for handwashing at key times (adherence) (unpooled data), community-based approach vs no promotional approach
1 RCT (Jinadu 2007) and 1 quasi-RCT (Phuanukoonnon 2013)
Attrition bias (Phuanukoonnon 2013) and detection bias (Phuanukoonnon 2013)
Assessment of the certainty of evidence for handwashing at key times (longer-term use) (unpooled data), community-based approach vs no promotional approach
2 cluster RCT's (Huda 2012 and Pickering 2015)
1 non-randomised controlled trial (Kochurani 2009)
Selection bias (Huda 2012, Kochurani 2009 and Pickering 2015), attrition/reporting bias (Pickering 2015), bias due to confounding/bias in measurement of outcomes/interventions/bias due to departures from intended interventions (Kochurani 2009)
Lack of data
Assessment of the certainty of evidence for latrine use (adherence) (unpooled data), community-based approach vs no promotional approach
1 RCT (Jinadu 2007) and 1 cluster RCT (Pattanayak 2009)
Reporting bias (Jinadu 2007) and attrition bias (Pattanayak 2009)
Low number of events
Assessment of the certainty of evidence for latrine use (longer-term use) (unpooled data), community-based approach vs no promotional approach
1 RCT (Hoque 1994/1996) and 1 cluster-RCT (Pickering 2015)
Selection bias (Huda 2012/Pickering 2015) and attrition/reporting bias (Pickering 2015)
Assessment of the certainty of evidence for safe faeces disposal (uptake) (unpooled data), community-based approach vs no promotional approach
1 cluster RCT (Patil 2013/2015)
1 non-randomised controlled trial (Waterkeyn 2005)
Detection bias (Patil 2013/2015), selection bias/bias due to confounding/bias in measurement of interventions/outcomes/bias due to departures from intended interventions (Waterkeyn 2005)
Lack of data
Assessment of the certainty of evidence for safe faeces disposal (adherence) (unpooled data), community-based approach vs no promotional approach
1 RCT
Reporting bias
Assessment of the certainty of evidence for safe faeces disposal (longer-term use) (unpooled data), community-based approach vs no promotional approach
2 cluster RCTs
Selection bias (Huda 2012 and Pickering 2015) and attrition/reporting bias (Pickering 2015)
Low number of events
Assessment of the certainty of evidence for open defecation (uptake) (unpooled data), community-based approach vs no promotional approach
1 cluster RCT
Detection bias
Assessment of the certainty of evidence for open defecation (adherence) (unpooled data), community-based approach vs no promotional approach
1 cluster RCT
Other bias
Assessment of the certainty of evidence for open defecation (longer-term use) (unpooled data), community-based approach vs no promotional approach
2 cluster RCT's (Guiteras 2015b and Pickering 2015)
1 non-randomised controlled trial (Kochurani 2009)
Selection bias (Kochurani 2009 and Pickering 2015), attrition/reporting bias (Pickering 2015), bias due to confounding/bias in measurement of outcomes/interventions/bias due to departures from intended interventions (Kochurani 2009) and other bias (Guiteras 2015b)
Lack of data
4.3.1.3 Social marketing approaches
From the 6 studies that we grouped in the category “social marketing approaches”, 5 studies formally described that they used a marketing campaign or social marketing techniques or interventions (Biran et al., 2009; Briceno et al., 2015; Cameron et al., 2013; Galiani et al., 2012/2015; Pinfold, 1999). Two of these studies implemented their intervention at school level (Galiani et al., 2012/2015; Pinfold, 1999). One study did not describe their approach as a formal social marketing approach, but used several elements that are generally part of a social marketing approach (infrastructure promotion, use of incentives) (Arnold et al., 2009). Since for the study of Galiani et al. (2012/2015) no raw data were available, the data represented are adjusted for confounding factors (gender and education of household head, children's age and gender, mother living in the home, rainfall and geographical region). All but one study had a handwashing component in the intervention (in contrast to the community-based approaches, where the focus was a sanitation intervention): four studies described a handwashing-only intervention, with one of these also studying an intervention arm with sanitation-only and a combined intervention, one study combined the handwashing intervention with a water supply/water quality component, and two studies included a sanitation-only intervention (see Figure 6).
Below we narratively describe the findings for the different outcome types. Since the majority of the studies had a handwashing-only intervention, we only mention the intervention specifically in case of a sanitation or combined programme. Behaviour change: handwashing (Analysis 21). Ony study, implementing a sanitation-only intervention, measured outcomes during the study period (“uptake”) (Cameron et al., 2013). Handwashing after toilet use was measured, but no significant increase in handwashing could be demonstrated (Cameron et al., 20132013). Two experimental studies (Galiani et al., 2012/2015; Briceno et al., 2015), and one observational study, with a combined handwashing and water supply/quality intervention (Arnold et al., 2009), measured outcomes less than 12 months after the programme period (“adherence”), and some differences across these studies were found. In a study with moderate risk of bias (Briceno et al., 2015), for the outcome “handwashing before food handling” a significant effect was shown when implementing a handwashing intervention (MD 7.70, 95% CI [3.78, 11.62]), or a combined handwashing and sanitation intervention (MD 1.60, 95% CI [0.03, 3.17]), however results were not consistent when measured by observation or in a self-reported way (Briceno et al., 2015). In addition, this effect could not be shown in a second study with moderate risk of bias, implementing a community level or school level intervention (Galiani et al., 2012/2015). For “handwashing with water and soap prior to eating” a significant effect was shown in the case of a school level intervention (self-reported: MD 0.09, 95% CI [0.01, 0.18]; observation: MD 0.12, 95% CI [0.02, 0.21]) (Galiani et al., 2012/2015), but not for the community level intervention (Galiani et al., 2012/2015) or in the observational study (Arnold et al., 2009). Finally, no significant effect could be demonstrated for handwashing with soap during the period “the last 24 hours” (Briceno et al., 2015), or handwashing at other key times (before feeding a child, after faecal contact, before cooking, before eating, after changing baby) (Arnold et al., 2009; Briceno et al., 2015; Galiani et al., 2012/2015). The certainty of evidence was very low for the adherence outcomes (Table 28). No longer term outcomes were found in studies using social marketing approaches. Behaviour change: latrine use (Analysis 22). In one experimental study latrine use adherence was measured (Briceno et al., 2015). A significant effect on shared latrine use could not be demonstrated in the case of a handwashing intervention only (MD -3.1, 95% CI [-8.98, 2.78]), however in the case of a sanitation intervention, or a combined handwashing and sanitation intervention, a significant decrease of shared latrine use (indicating more private latrine use) was shown (MD -9.2, 95% CI [-14.49, -3.91] and MD -7.6, 95% CI [-70.90, -81.10] respectively) (Briceno et al., 2015). The certainty of evidence for this outcome was moderate (Table 29). Behaviour change: safe faeces disposal (Analysis 23). Only outcomes for the period “less than 12 months after the end of the implementation period” were measured (“adherence”). In an experimental study with moderate risk of bias, a positive effect was seen for the observation of faeces outside the latrine in the case of a combined handwashing and sanitation intervention (MD -4.3, 95% CI [-8.42, -0.18]), but not for the handwashing or sanitation intervention alone. A significant increase of safe child faeces disposal was seen in the case of a sanitation or combined intervention (MD 11.7, 95% CI [5.04, 18.36] and MD 8.4, 95% CI [1.93, 14.87] respectively)), but not for the handwashing intervention alone (MD 4.3, 95% CI [-2.76, 11,36]) (Briceno et al., 2015). No significant increase in safe faeces disposal could be demonstrated in an observational study with serious risk of bias where a handwashing and water supply/quality programme was implemented (RR 0.91, 95% CI [0.83, 1.01]) (Arnold et al., 2009). The certainty of evidence for these outcomes was very low (Table 30). Behaviour change: open defecation (Analysis 24). No statistically significant decrease of open defecation could be shown during the progam period (“uptake”) in an experimental study with low risk of bias, describing a sanitation-only intervention (RR 0.92, 95% CI [0.80, 1.05]) (Cameron et al., 2013). In case of a sanitation, or combined sanitation and handwashing intervention, a statistically significant decrease of people that always or regularly practice open defecation, and that usually defecate in fields, bushes or rivers, could be shown for the period less than 12 months after the end of the implementation (“adherence”), but not for the handwashing intervention alone (Briceno et al., 2015). The certainty of evidence for this outcome was found to be moderate (Table 31). Behavioural factors (Analysis 25). Three experimental (Cameron et al., 2013; Briceno et al., 2015; Galiani et al., 2012/2015), and one quasi-experimental study performed in schools (Pinfold, 1999), measured the effect of social marketing approaches on knowledge. In a study with low risk of bias (Cameron et al., 2013), no effect could be demonstrated concerning knowledge about causes of diarrhoea, and building of a latrine. In a study with a moderate risk of bias, a significant increase in the knowledge that “not washing hands with water and soap is the main cause of diarrhoea”, was seen for the community level intervention (Galiani et al., 2012/2015). A statistically significant increase in handwashing knowledge was reported in 3 studies (Pinfold, 1999; Briceno et al., 2015; Galiani et al., 2012/2015). In Briceno et al. (2015), only the combined handwashing and sanitation intervention led to improved knowledge concerning the best method to wash hands and when to wash hands. In Galiani et al. (2012/2015), this result was only seen in the school level intervention. In one study, the knowledge of the key events when handwashing was required, was tested, but no effect on this knowledge could be demonstrated as a result of the intervention (Galiani et al., 2012/2015). One study looked at skills, and more specifically at the practice of handwashing with one or both hands (Biran et al., 2009). An effect on washing one hand or both hands could not be demonstrated (RR 1.01, 95% CI [0.62, 1.64] and RR 0.70, 95% CI [0.48, 1.02] respectively) (Biran et al., 2009). A third behavioural factor, attitudes, was investigated in one experimental study with a low risk of bias (Cameron et al., 2013), but no effect on the attitude to open defecation could be demonstrated. The outcome “norms” was measured in one experimental study (Briceno et al., 2015); the combined sanitation and handwashing intervention resulted in a significant decrease in the number of households that were aware of community members practicing open defecation (MD -6.6, 95% CI [-12.87, -0.033]), but this was not the case for the sanitation (MD -5.50, 95% CI [-11.18, 0.18]) or handwashing (MD -5.20, 95% CI [-10.88, 0.48]) intervention alone (Briceno et al., 2015). Health outcomes (Analysis 26). Morbidity outcomes were studied in three experimental (Cameron et al., 2013; Briceno et al., 2015; Galiani et al., 2012/2015) and one observational study (Arnold et al., 2009). An effect of the social marketing approach could not be shown for any diarrhoeal, and acute respiratory tract infection outcomes (Cameron et al., 2013; Briceno et al., 2015; Arnold et al., 2009; Galiani et al., 2012/2015). Influence of incentives in programs. From the 6 studies describing social marketing approaches, 2 studies described the use of incentives (see Table 3), including food (Arnold et al., 2009), and gifts (Biran et al., 2009) to the progam recipients. A third study compared two different promotional approaches, both with use of incentives, and is described below (Dickey et al., 2015). When focusing on these studies we found no significant effects on handwashing (adherence) and safe faeces disposal. When comparing the studies with or without use of incentives, there were no major differences.
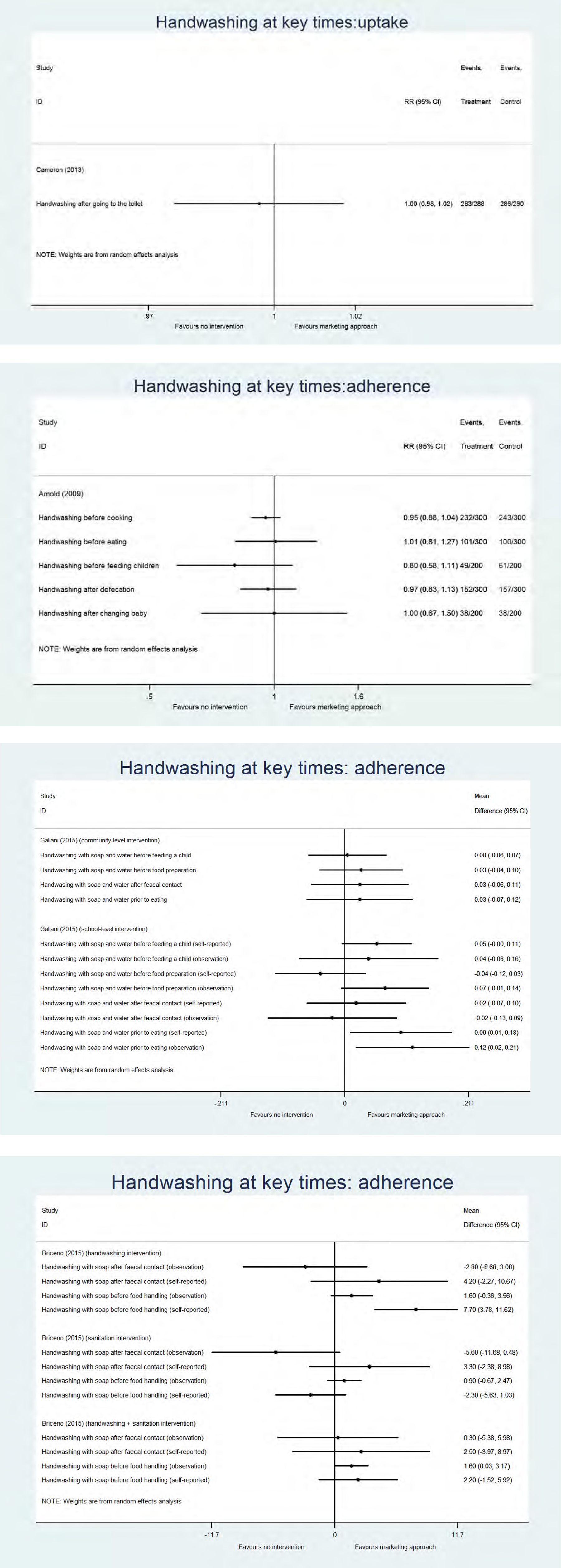
Analysis
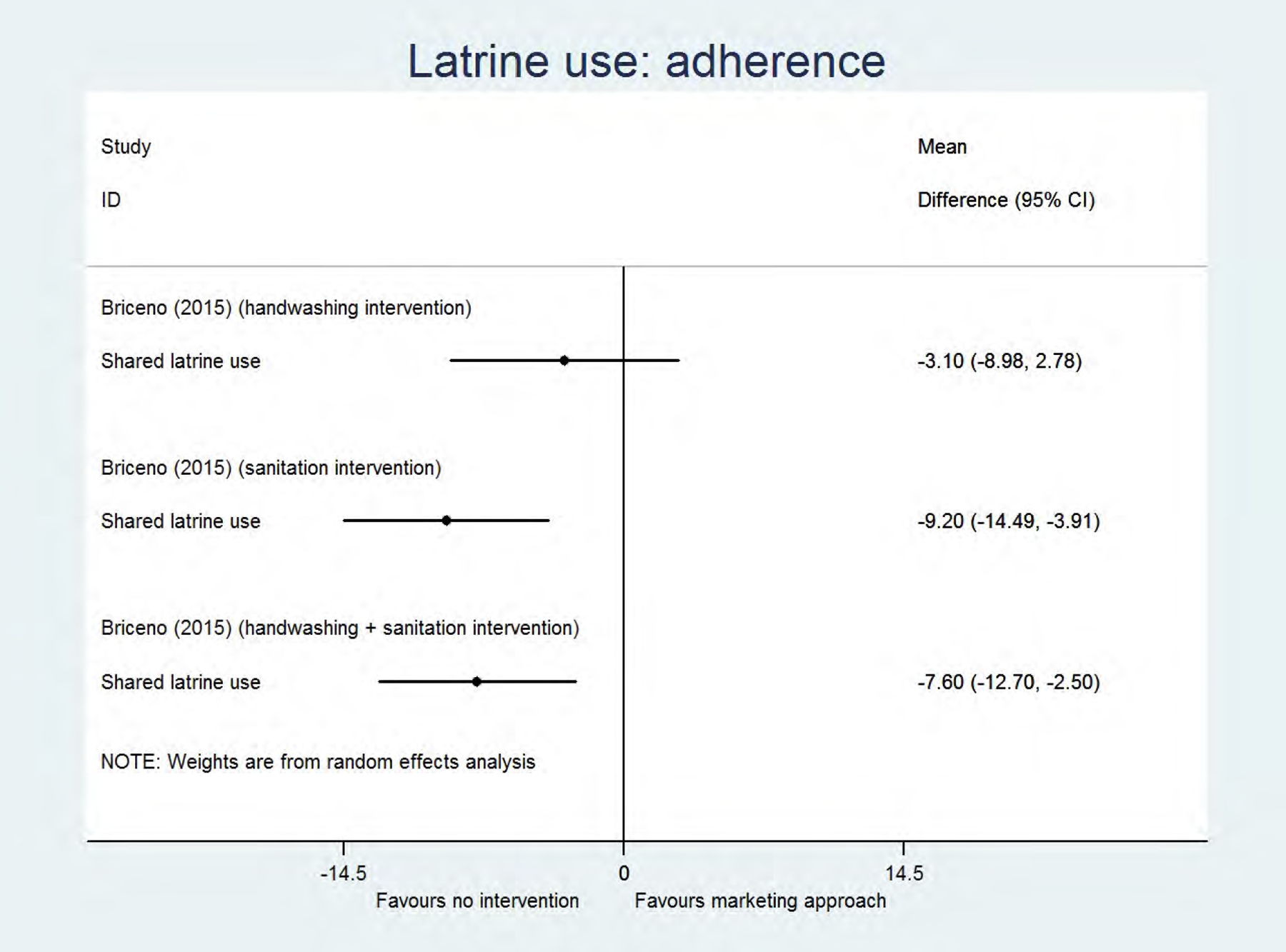
Analysis
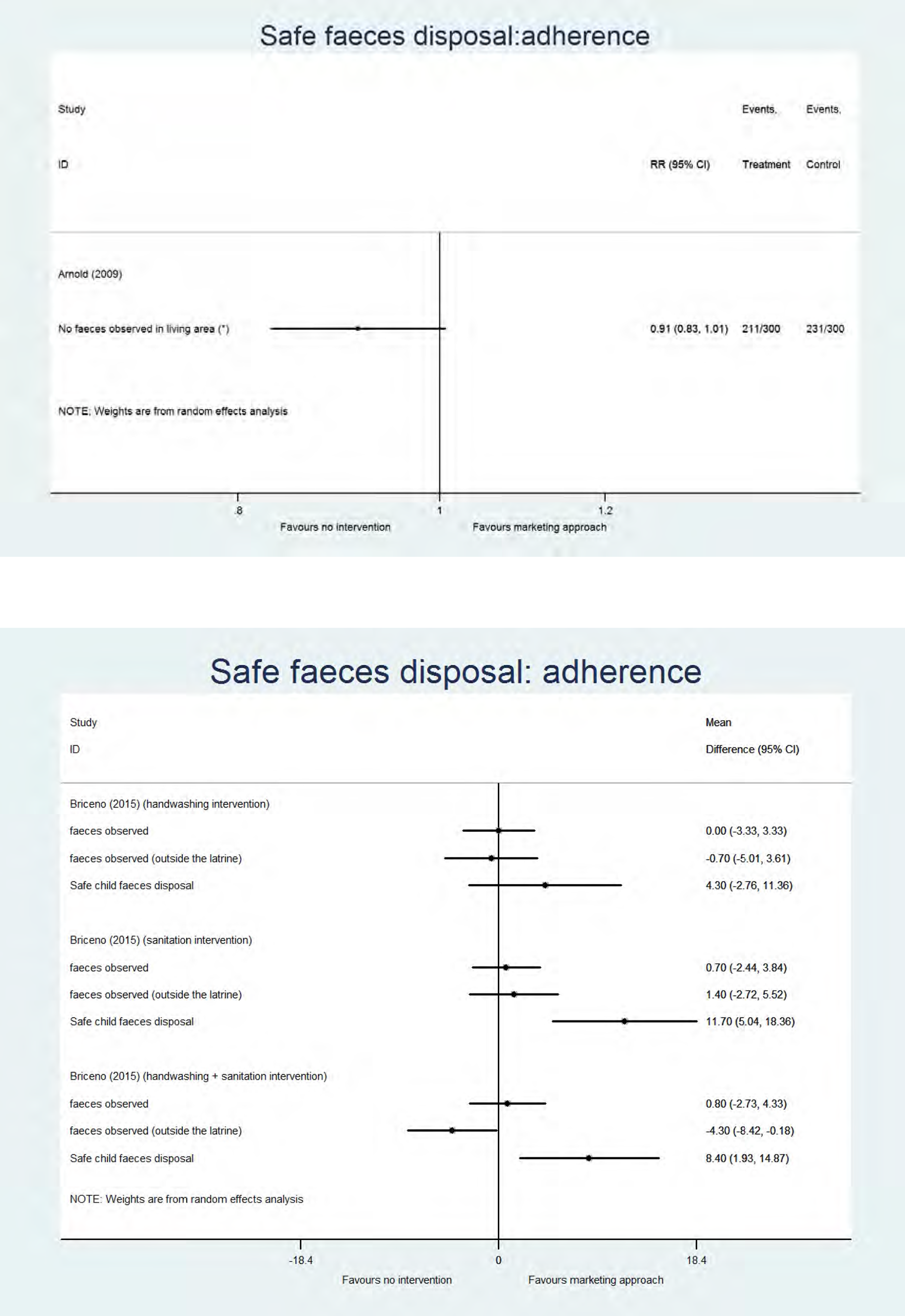
Analysis
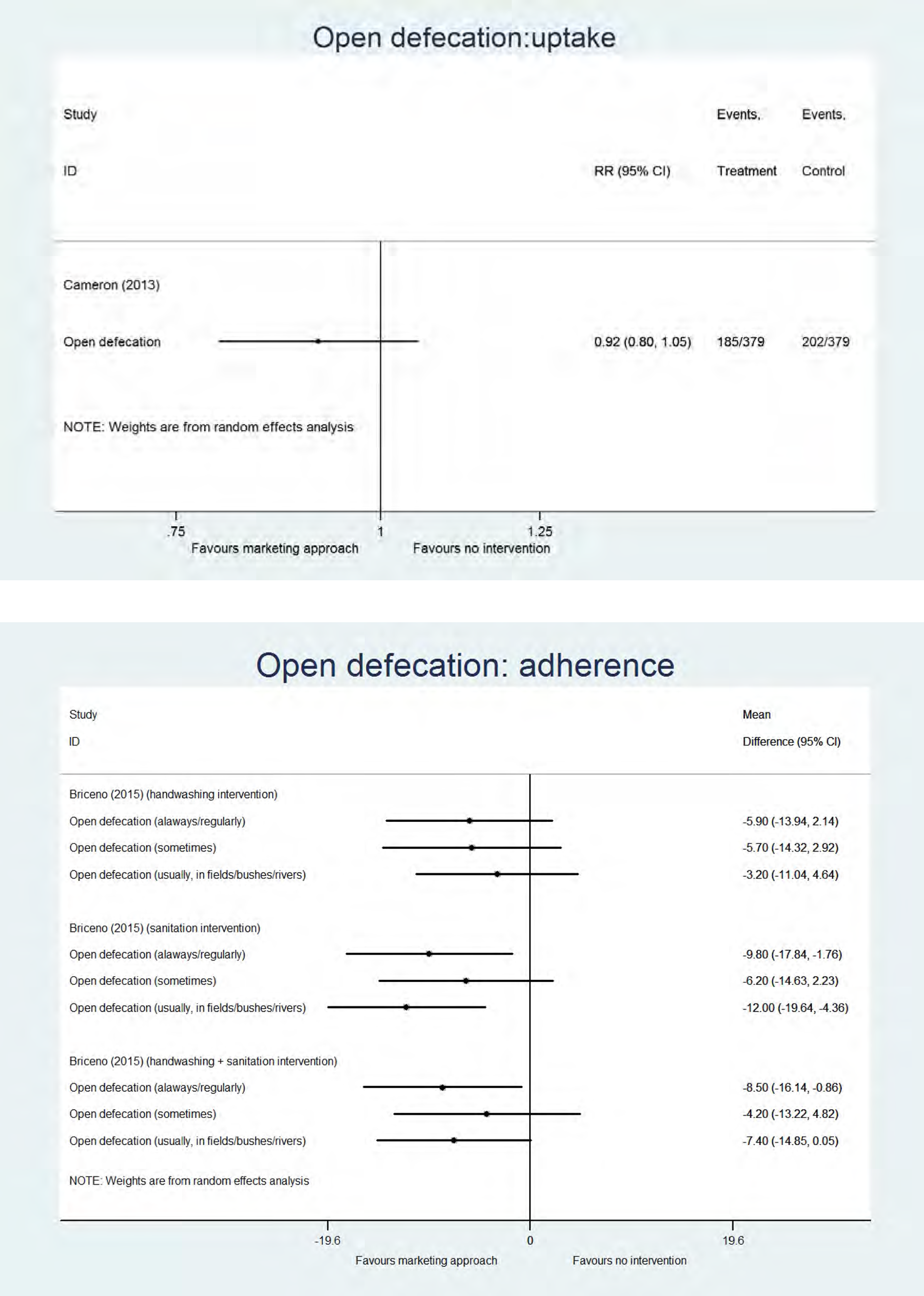
Analysis
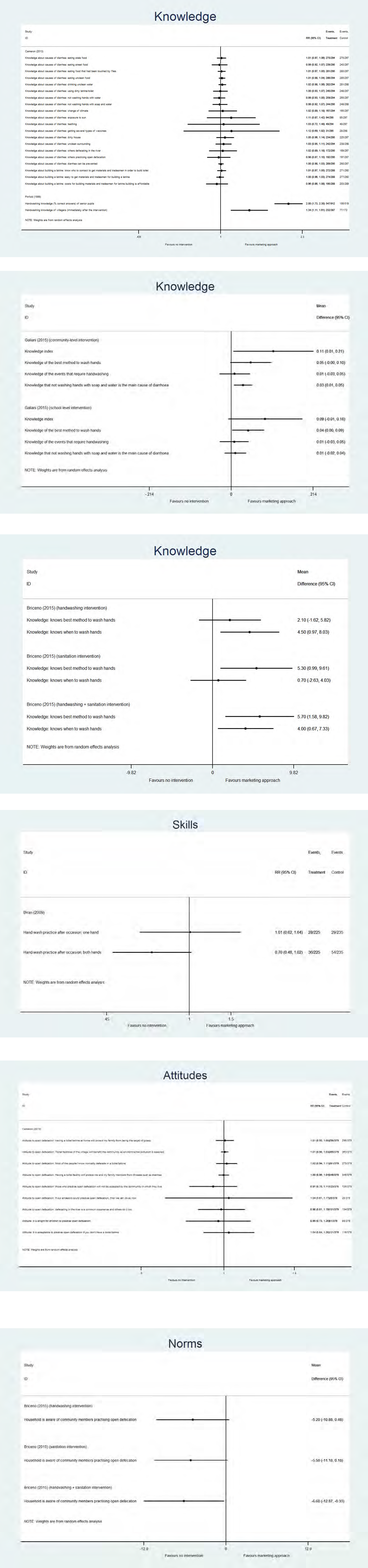
Analysis
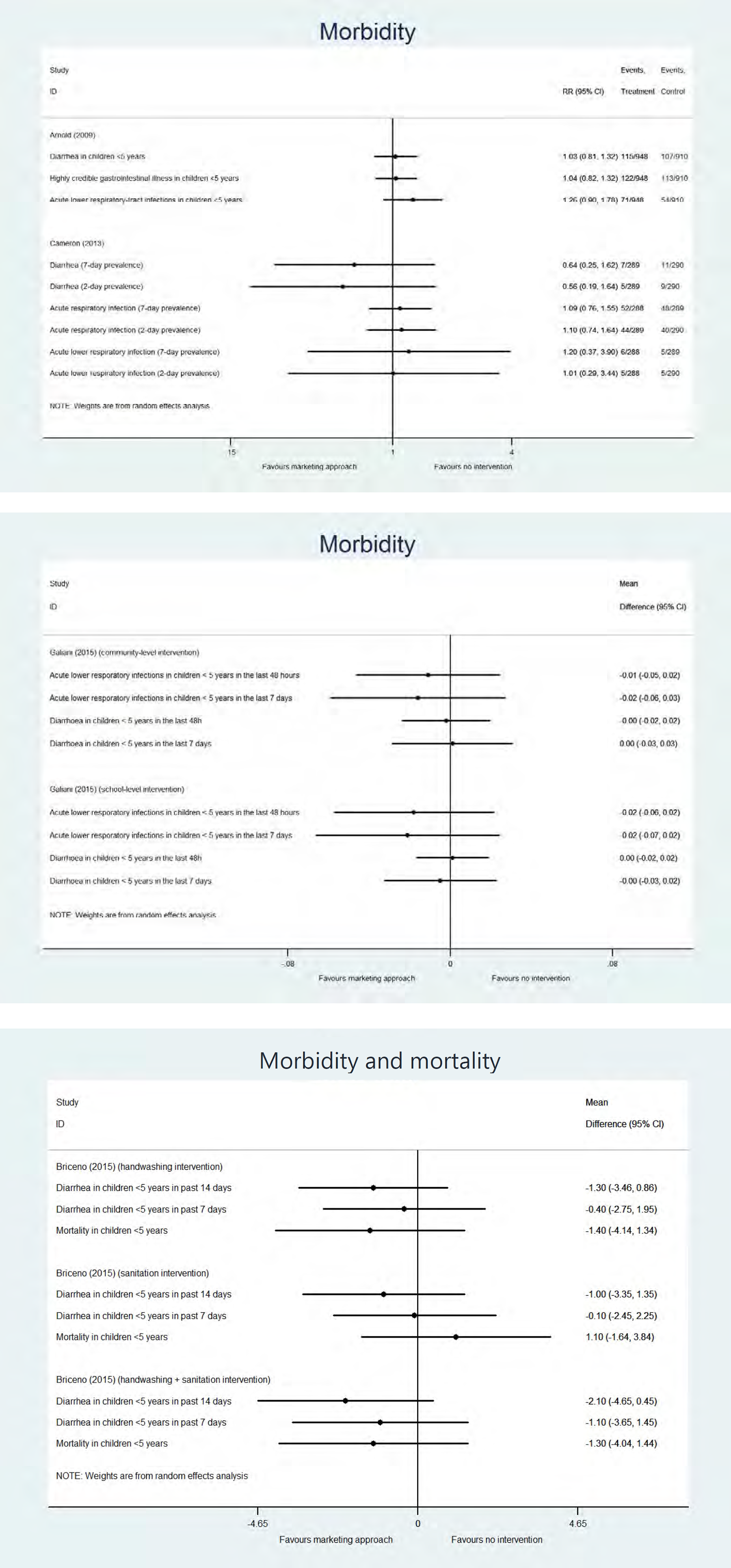
Analysis
Assessment of the certainty of evidence for handwashing at key times (adherence) (unpooled data), social marketing approach vs no promotional approach
2 cluster RCTs (Briceno 2015 and Galiani 2012/2015)
1 cohort study (Arnold 2009)
Attrition/other bias (Briceno 2015), bias in measurement of outcomes/bias due to departures from intended interventions (Arnold 2009)
Assessment of the certainty of evidence for latrine use (adherence) (unpooled data), social marketing approach vs no promotional approach
1 cluster RCT
Attrition/other bias
Assessment of the certainty of evidence for safe faeces disposal (adherence) (unpooled data), social marketing approach vs no promotional approach
1 cluster RCTs (Briceno 2015)
1 cohort study (Arnold 2009)
Attrition/other bias (Briceno 2015), bias in measurement of outcomes/bias due to departures from intended interventions (Arnold 2009)
Assessment of the certainty of evidence for open defecation (adherence) (unpooled data), social marketing approach vs no promotional approach
1 cluster RCT
Attrition/other bias
4.3.1.4 Sanitation and hygiene messaging
Sanitation and hygiene messaging is a predominantly directive educational approach, consisting mainly of one-way communication, designed to help individuals and communities improve their health, by increasing their knowledge and/or skills. We identified an approach using sanitation and hygiene messaging as the major element of the promotional approach in 12 studies, of which 4 studies described school-based interventions (Abiola et al., 2012; Caruso et al., 2014; Lansdown et al., 2002; Pickering et al., 2013). All but one study had a handwashing component in the intervention (comparable to the social marketing approaches): eight studies described a handwashing-only intervention, with three of these also studying an intervention arm where handwashing was combined with either a water supply/quality or sanitation component. Six studies described a combined intervention (either handwashing with water supply/quality, handwashing with sanitation, or all three WASH components). One study included a sanitation-only intervention (see Figure 6).
Below we narratively describe the findings for the different outcome types. We specified the intervention if it was not focused on handwashing alone. Behaviour change: handwashing (Analysis 27-28). A significantly improved frequency of handwashing (MD 18.00, 95% CI [17.31, 18.69]) during the programme period (“uptake”) was shown in an experimental study (Kaewchana et al., 2012). In another experimental study, with a combined handwashing and sanitation intervention, a significant decrease was seen in washing hands only with water (MD -11.6%, p<0.001) (Mascie-Taylor et al., 2003). In addition, a statistically significant increase in handwashing with product after toilet use and before lunch was shown in the case of an educational intervention with hand sanitizer provision in schools (Pickering et al., 2013). In the case of an educational intervention with soap in schools, a significant increase in “handwashing with soap” after toilet use (RR 18.66, 95% CI [11.58, 30.08]) was shown, but not in “any type of handwashing” (Pickering et al., 2013), meaning that handwashing already regularly occurred before the handwashing with soap intervention was implemented. A significant increase in “handwashing with soap” before lunch was also shown in the case of the soap intervention, but again not in “any type of handwashing” (RR 19.00, 95% CI [1.22, 295.91]) (Pickering et al., 2013). For “handwashing after toilet use” at less than 12 months after the programme period (“adherence”) results were inconsistent (RR 1.15, 95% CI [1.05, 1.26]) (Abiola et al., 2012); RR 0.72, 95% CI [0.40, 1.31] (Yeager et al., 2002 (sanitation-only))), and for none of the other adherence outcomes a significant effect was demonstrated (Stanton & Clemens, 1987; Yeager et al., 2002; Abiola et al., 2012). For the uptake outcomes the certainty of evidence was found to be moderate and for the adherence outcomes it was low (Tables 32 and 33). Finally, two experimental studies, both with moderate risk of bias, measured longer-term outcomes (Bowen et al., 2013; Luby et al., 2009); in one study (Bowen et al., 2013) the handwashing intervention was combined with a water supply/quality component. No significant difference in handwashing with or with soap was shown in the first study (RR 1.00, 95% CI [0.97, 1.04]; RR 1.02, 95% CI [0.99, 1.06]) (Luby et al., 2009). However, in the second study the promotional approach had a positive effect on 9 out of 14 “handwashing at key times” outcomes (Bowen et al., 2013). The certainty of evidence for the longer-term outcomes was low (Table 34). Behaviour change: latrine use (Analysis 29). Latrine use was measured in one experimental study, less than 12 months following the end of the study period (“adherence”) (Caruso et al., 2014). No statistically significant difference in latrine use was shown in this study (handwashing intervention: MD 1.80, 95% CI [-0.17, 3.77], latrine cleaning + handwashing intervention: MD -1.00, 95% CI [-2.91, 0.91]) (Caruso et al., 2014). The certainty of evidence for this outcome was found to be very low (Table 35). Behaviour change: safe faeces disposal (Analysis 30). In one experimental study, with a moderate risk of bias, describing a sanitation-only intervention, a statistically significant increase in “no child faeces on the ground” was shown (RR 1.68, 95% CI [1.21, 2.32]), but an effect on “safe child faeces disposal” could not be demonstrated, in the period less than 12 months after the end of the study period (“adherence”) (RR 1.07, 95% CI [0.70, 1.65]) (Yeager et al., 2002). The certainty of evidence for this outcome was assessed to be low (Table 36). Behaviour change: open defecation (Analysis 31). A significant effect of an education approach on open defecation in a short term (“uptake”) and less than 12 months after project implementation (“adherence”) could not be demonstrated in 3 experimental studies, all with moderate risk of bias (Lansdown et al., 2002; Wang et al., 2013; Stanton & Clemens, 1987). All studies had an intervention with a handwashing and sanitation component, and in 2 of the 3 also a water supply/quality component was included. The certainty of evidence for both the uptake and adherence outcomes was assessed as low (Tables 37 and 38). Behavioural factors (Analysis 32). Knowledge was measured in 3 experimental (Lansdown et al., 2002; Mascie-Taylor et al., 2003; Abiola et al., 2012) and one observational study (Seimetz et al., 2016). In one study an effect of the school-based educational intervention on knowledge could not be demonstrated 9 months after the start of the intervention, however a statistically significant increase in knowledge (health causation and prevention) was measured 15 months after the end of the implementation (MD 2.71, 95% CI [0.36, 5.06]) (Lansdown et al., 2002). In a second study, no effect on perceived vulnerability, severity, or health knowledge was shown (Seimetz 2016). In Mascie-Taylor et al. (2003), the percent difference in knowledge from baseline to 18 months between intervention and control was calculated. The promotional intervention improved the level of health knowledge regarding whether worms are good for health (MD 31.1%, p<0.001), whether defecation in the courtyard is associated with worms (MD 68.2%, p<0.001), whether defecation in the bushes is associated with worms (MD 58.1%, p<0.001), and whether removal of all worms is good for a person (MD 54.7%, p<0.001). In Abiola et al. (2012) a significant increase in knowledge about the meaning of personal hygiene (RR 1.16, 95% CI [1.06, 1.27]), and eating with unclean hands as the cause of diarrhoea (RR 1.65, 95% CI [1.31, 2.08]) was shown after implementing a school-based intervention, but not for 2 other outcomes on personal hygiene knowledge. Next, three studies also measured skills (Bowen et al., 2013; Luby et al., 2009; Seimetz et al., 2016). In two of the studies (Bowen et al., 2013; Luby 2009) a statistically significant increase in using soap for handwashing (handwashing skills) was shown (RR 1.05, 95% CI [1.02, 1.08], see pooled value in Analysis 10). Also a significant increase in “rubbing hands together at least 3 times” (skills) and “lathering hands for at least 10 seconds” was shown. For “drying hands with a clean towel” a significant effect could not be shown in 2 of the 4 intervention arms (Bowen et al., 2013; Luby et al., 2009). In Seimetz et al. (2016), no difference in maintenance self-efficacy (confidence in abilities to maintain the behaviour) and recovery self-efficacy (confidence in abilities to successfully return to the behaviour) could be demonstrated, and, surprisingly, a decrease in action self-efficacy, which is the confidence in the abilities to successfully perform the behaviour, was shown (MD -0.20, 95% CI [-0.31, -0.09]). Finally, attitude outcomes were measured in two studies (Seimetz et al., 2016; Abiola et al., 2012), however the effect of sanitation and hygiene messaging on the majority of the outcomes could not be demonstrated (beliefs about costs, belief that the behaviour will lead to the outcome (response), feelings of liking washing hands, feelings of dirtiness when not washing hands, necessity to wash hands after going to the toilet, willingness to recommend practice of personal hygiene to friends), except for feelings of attractiveness when using soap to wash hands, which was significantly decreased (MD -0.27, 95% CI [-0.48, -0.06]). Seimetz et al. (2016) also measured “norms” and “self-regulation”, but no significant effects were demonstrated except a significant decrease in action control (“self-regulation”), the determination to execute and control the behaviour, was shown. Health outcomes. Health outcomes were not measured in studies using sanitation and hygiene messaging approaches. Influence of incentives in programs. From the 12 studies describing sanitation and hygiene messaging, only one study described the use of incentives (see Table 3), which was the provision of soap bars to the programme recipients (Seimetz et al., 2016). This study only reported outcomes such as skills, attitude and self-regulation and could not show any improvement of these outcomes. No difference were shown in these outcomes when in- or excluding this study making use of soap bars as incentives.
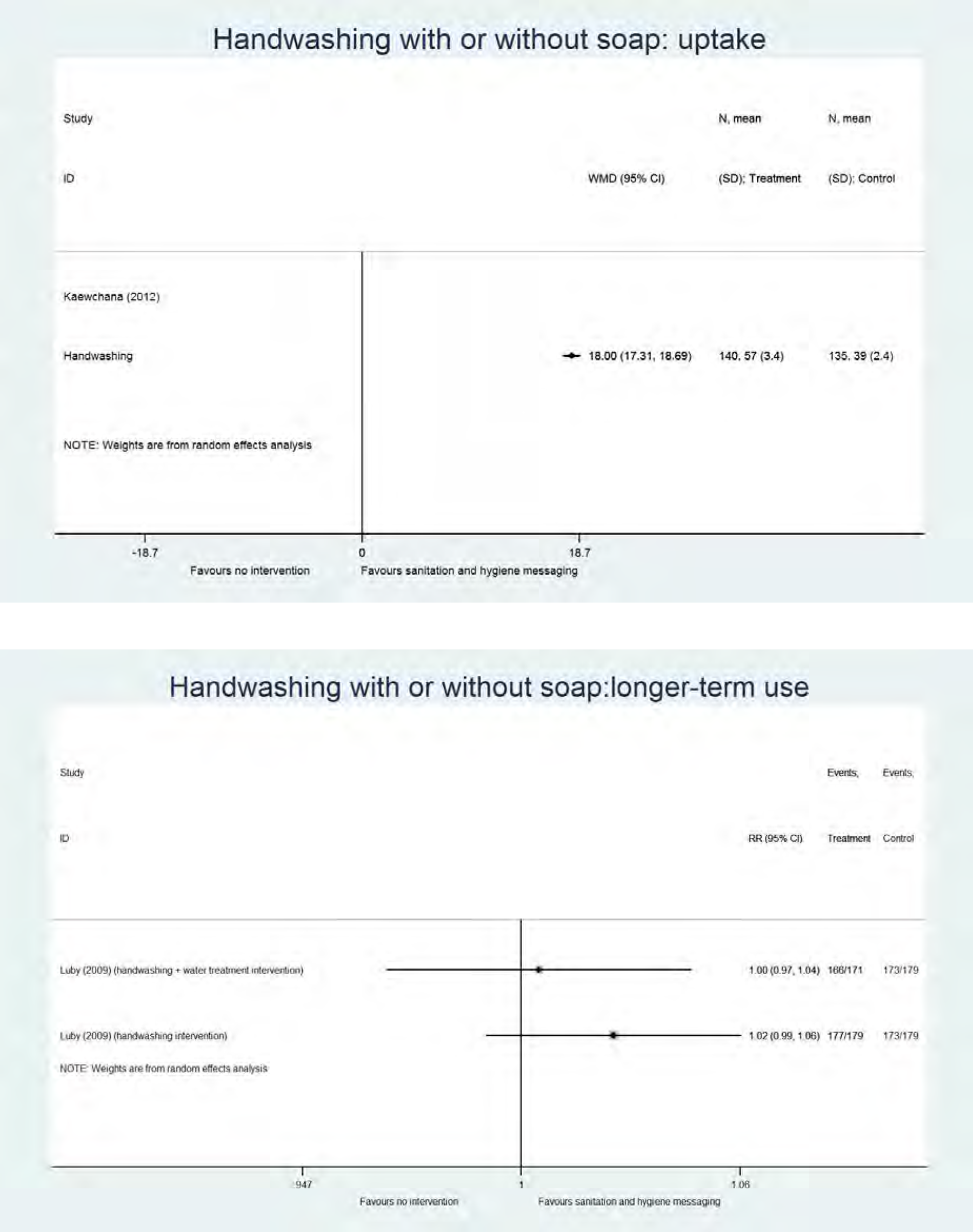
Analysis
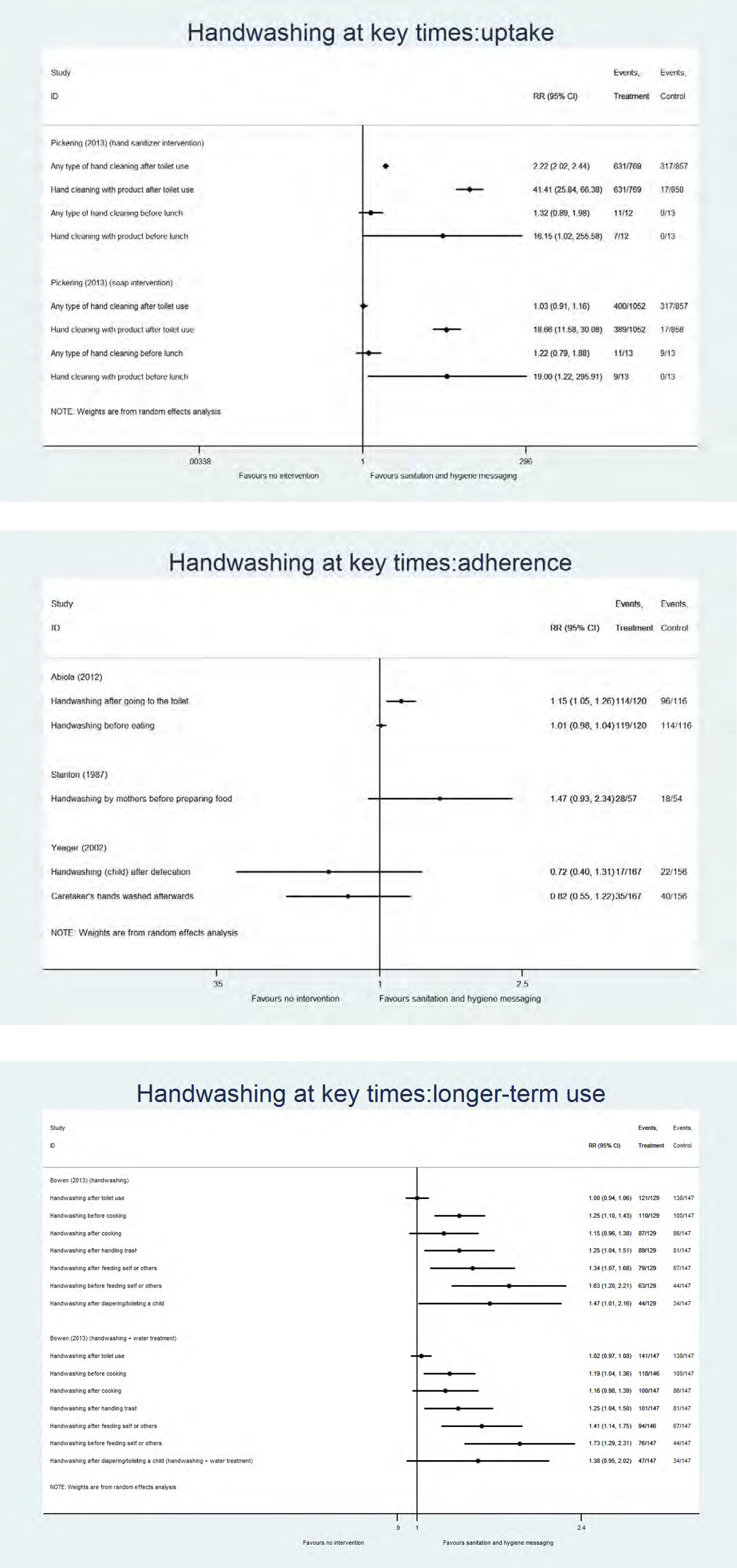
Analysis
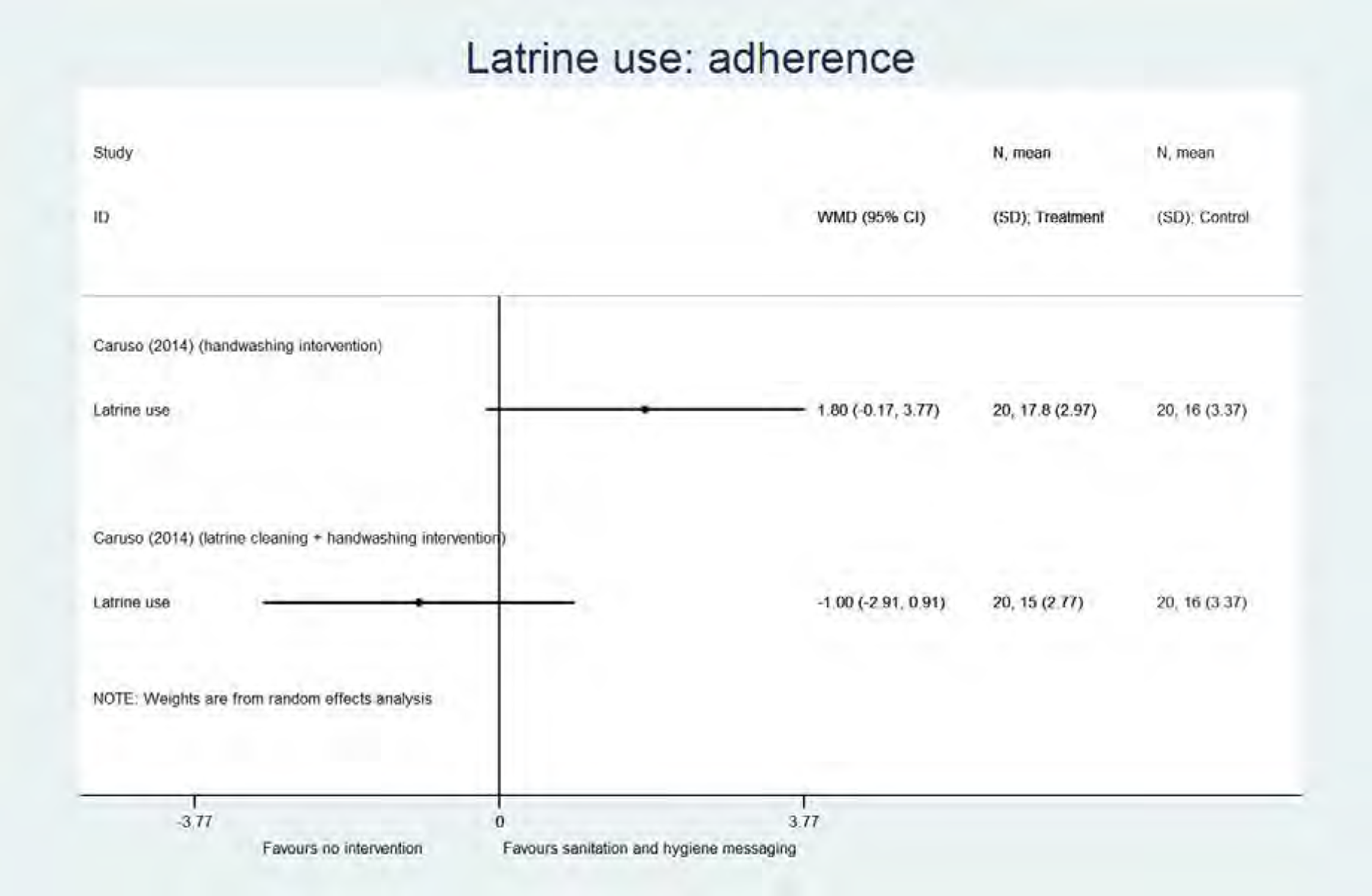
Analysis
Analysis

Analysis
Analysis
Assessment of the certainty of evidence for handwashing at key times (uptake) (unpooled data), sanitation and hygiene messaging vs no promotional approach
1 cluster RCT
Reporting, detection and other bias
Assessment of the certainty of evidence for handwashing at key times (adherence) (unpooled data), sanitation and hygiene messaging vs no promotional approach
2 quasi-RCTs (Abiola 2012 and Yeager 2002) and 1 cluster RCT (Stanton 1987)
Reporting bias (Abiola 2012 and Yeager 2002), attrition bias (Stanton 1987 and Yeager 2002) and detection bias (Abiola 2012)
Assessment of the certainty of evidence for handwashing at key times (longer-term use) (unpooled data), sanitation and hygiene messaging vs no promotional approach
2 cluster RCTs
Detection bias (Bowen 2013 and Luby 2009) and attrition bias (Luby 2009)
Assessment of the certainty of evidence for latrine use (adherence) (unpooled data), sanitation and hygiene messaging vs no promotional approach
1 quasi-RCT
Attrition/reporting bias
Large variability in results
Assessment of the certainty of evidence for safe faeces disposal (adherence) (unpooled data), sanitation and hygiene messaging vs no promotional approach
1 quasi-RCT
Reporting/attrition bias
Low number of events
Assessment of the certainty of evidence for open defecation (uptake) (unpooled data), sanitation and hygiene messaging vs no promotional approach
1 RCT (Lansdown 2002) and 1 cluster RCT (Wang 2013)
Reporting and detection bias (Lansdown 2002 and Wang 2013)
Low number of events
Assessment of the certainty of evidence for open defecation (adherence) (unpooled data), sanitation and hygiene messaging vs no promotional approach
2 cluster RCTs
Attrition bias (Stanton 1987) and reporting/detection bias (Wang 2013)
Low number of events
4.3.1.5 Elements of psychosocial theory
The 4 studies that we included in this category all described theoretical elements or a formal psychosocial theory as the basis of the intervention. One study used the Theory of Planned Behaviour (Langford et al., 2013) and one study the RANAS model (Tumwebaze & Mosler, 2015). Biran et al. (2014) describes the SuperAmma approach, based on emotional drivers of behaviour, and Luby et al. (2010) describes an approach based on the stages of change theory. It should be noted that all these studies were conducted at small scale, and that elements of psychosocial theory should be incorporated in a larger promotional approach for a programme at scale. All studies implemented a handwashing-only intervention (see Figure 6).
Below we narratively describe the findings for the different outcome types. Behaviour change: handwashing (Analysis 33). Two different experimental studies describing interventions based on elements of psychosocial theory, measured handwashing at key times during the study period (“uptake”) (Langford & Panter-Brick, 2013; Luby et al., 2010). The study by Luby et al. (2010) had two different intervention arms, one with a theory-based intervention with soap, and one with a theory-based intervention with hand sanitizer. A significant effect on handwashing at different key times could be shown for 7 of the 9 outcomes (excluding the programme with hand sanitizer) (Langford & Panter-Brick, 2013; Luby et al., 2010). For the hand sanitizer intervention, a significant effect for handwashing in 3 out of 10 key times was shown (Luby et al., 2010). The certainty of evidence for the uptake outcomes was found to be low (Table 39). In one experimental study, with a low risk of bias, adherence outcomes were measured (Biran et al., 2014). Handwashing at key times was significantly improved, both at 6 weeks (MD 15.00, 95% CI [10.71, 19.29]) and 6 months (MD 31.00, 95% CI [29.45, 32.55]). For the adherence outcomes, the certainty of evidence was moderate (Table 40). Behavioural factors (Analysis 34). One experimental study with moderate risk of bias measured knowledge, skills and attitudes (Tumwebaze & Mosler, 2015). An effect on knowledge about disease severity (MD 0.09, 95% CI [-0.06, 0.24]) and knowledge about disease vulnerability (MD 0.02, 95% CI [-0.05, 0.09]) could not be demonstrated. An additional public commitment element in the promotional approach also did not result in any significantly improved outcomes. An intervention based on elements of psychosocial theory improved skills in cooperation confidence in both treatment arms (MD 0.44, 95% CI [0.06, 0.82]; MD 0.42, 95% CI [0.06, 0.78]), but improved skills in cleaning ease (confidence in the ability to participate in cleaning a shared sanitation facility) and using a cleaning roster (planning showing who is responsible for cleaning at a certain time point) could not be demonstrated. Finally, no differences in attitudes regarding time cost, cleaning affect and cleaning effort could be shown in any of the treatment arms (Tumwebaze & Mosler, 2015). Health outcomes. Langford et al. (2013) measured morbidity outcomes. The intervention based on elements of psychosocial theory significantly reduced the “median days of diarrhoea” from 16.3 to 9.7 (intervention vs controls, n=88, p=0.023). Influence of incentives in programs. From the4 studies describing elements of psychosocial theory, only one study described the use of incentives (see Table 3), which was the provision of soap bars to the programme recipients (Langford & Panter-Brick, 2013). This study found a significant increase in handwashing at the short term, however absolute effects were similar as with the studies not using incentives.
Analysis
Analysis
Assessment of the certainty of evidence for handwashing at key times (uptake) (unpooled data), elements of psychosocial theory vs no promotional approach
1 quasi-RCT (Langford 2013) and 1 cluster RCT (Luby 2010)
Attrition/reporting bias (Langford 2013 and Luby 2010) and detection and other bias (Langford 2013)
Assessment of the certainty of evidence for handwashing at key times (adherence) (unpooled data), elements of psychosocial theory vs no promotional approach
1 cluster RCT
Reporting bias
4.3.2 Comparison of different promotional approaches
In 7 studies, certain promotional approaches were compared with one another. In this way, the effect of specific additional elements to a promotional approach could be studied. We discuss the different comparisons below (Contzen et al., 2015a/2015b; Dickey et al., 2015;Graves et al., 2011; Guiteras et al., 2015a; Lhakhang et al., 2015;Whaley & Webster, 2011; Zhang et al., 2013).
An overview of the findings on studies comparing different communication strategies is given in Table 41 and described in detail below.
Overview of the findings on studies comparing different promotional approaches
All mean differences and risk ratios are presented as Cochran-Mantel-Haenszel estimate, [95% CI]. MD: Mean difference; RR: risk ratio; CI: Confidence interval. *p<0.05
4.3.2.1 Hygiene messaging and elements of psychosocial theory versus hygiene messaging alone
In Contzen et al.(2015a/2015b) three intervention arms were compared (Analysis 35). A health education approach (hygiene messaging) based on psychosocial theories (elements of infrastructure promotion, public commitment, reminders) was compared with health education (hygiene messaging) alone, and only handwashing was included in the intervention. In one intervention arm, education was combined with infrastructure promotion and reminder, in another intervention arm, education was combined with a focus on public commitment and reminder, and in a third arm, both elements were included. These 3 intervention arms were compared with a control arm, consisting of health education alone. A statistically significant increase of stool-related and food-related handwashing were shown in case of using the infrastructure promotion (stool-related: MD 0.20, 95% CI [0.04, 0.36]; food-related: MD 0.21, 95%CI [0.06, 0.36]) or the combined infrastructure promotion and public commitment (stool-related: MD 0.27, 95% CI [0.11, 0.43]; food-related: MD 0.32, 95% CI [0.17, 0.47]) interventions, however in case of a programme only using public commitment this could not be demonstrated (stool-related: MD 0.09, 95% CI -0.07, 0.25]; food-related: MD 0.08, 95% CI [-0.07, 0.23]).
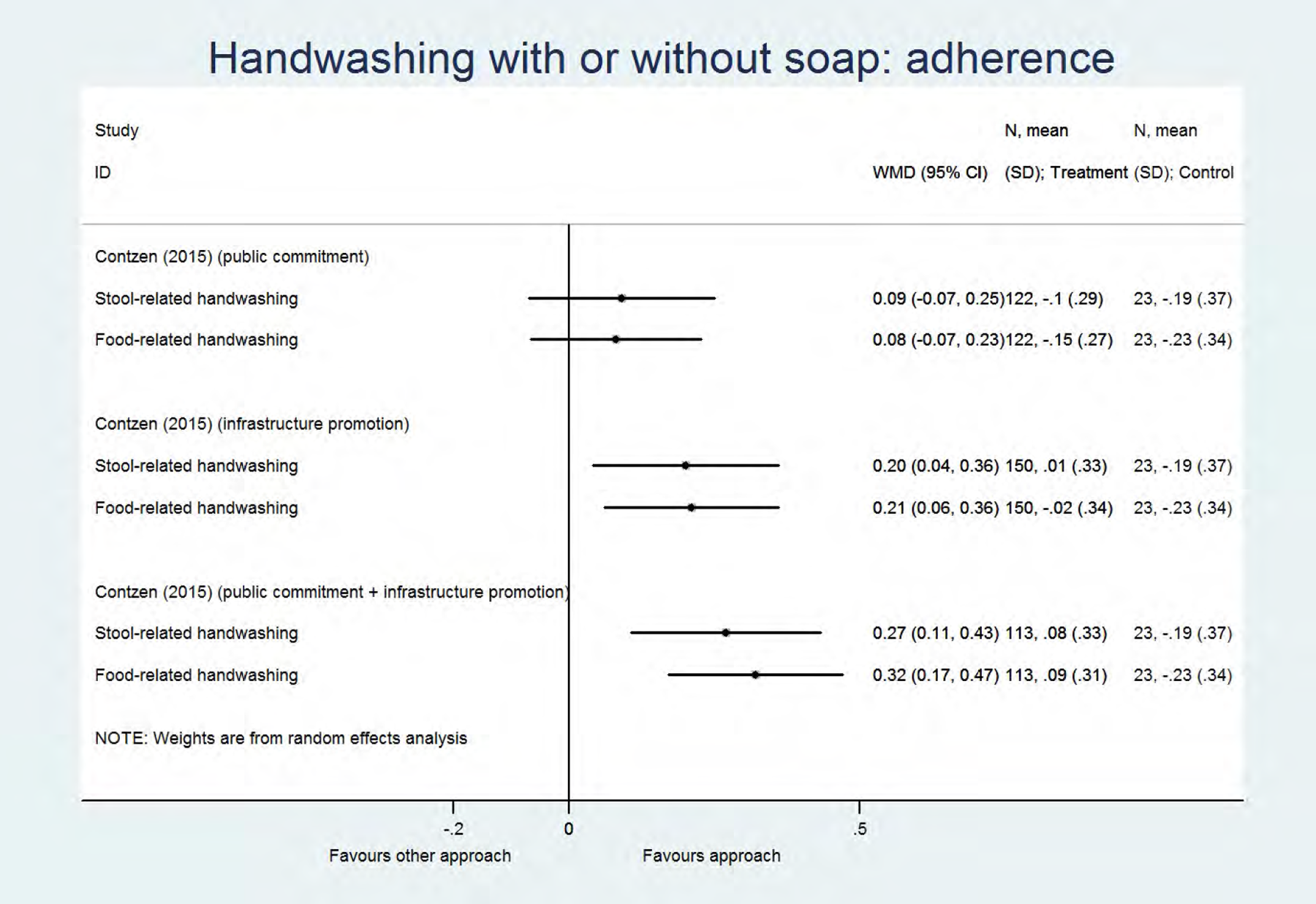
Analysis
In addition, several behavioural factors were also measured in this study. A statistically significant correlation was shown between the educational approach together with infrastructure promotion, public commitment and reminder, and the following behavioural factors, regarding changes in food- and stool-related handwashing: descriptive norm (correlation coefficient food-related handwashing: 0.87; stool-related handwashing: 1.05), injunctive norm (correlation coefficient food-related handwashing: 0.65; stool-related handwashing: 0.60), commitment strength (correlation coefficient food-related handwashing: 0.53), forgetting (correlation coefficient food-related handwashing: -0.66; stool-related handwashing: -0.66), motivational self-efficacy (belief in ability to initiate and execute the behaviour) (correlation coefficient food-related handwashing: 0.47; stool-related handwashing: 0.54), volitional self-efficacy (belief in ability to maintain the behaviour) (correlation coefficient food-related handwashing: 0.44; stool-related handwashing: 0.44) and impediments (anticipated barriers and distractions to a behaviour) (correlation coefficient food-related handwashing: -0.49; stool-related handwashing: -0.49). For the educational intervention with infrastructure promotion, a significant correlation was found for most of the behavioural factors, while for the educational intervention with public commitment, significant correlations could only be found for less than half of the factors studied.
4.3.2.2 Local-builder social marketing approach versus outside-expert building team approach
The comparison between a local-builder social marketing approach versus an outside-expert building team approach was made in a study published in 2015, implementing a sanitation intervention (Dickey et al., 2015). The local-builder social marketing approach resulted in a statistically significant decrease in the number of households refusing to use the new toilet(RR 0.02, 95% CI [0.00, 0.31]).
4.3.2.3 Hygiene messaging with poster contest versus hygiene messaging alone
In the study by Graves et al. (2011), the effect of an additional communication strategy (poster contest), in addition to an existing educational intervention (hygiene messaging), was tested in Kenyan primary schools where a handwashing intervention was implemented. A statistically significant increase in handwashing after 4 months (MD 0.08, 95% CI [-0.19, 0.35]), and a significant change after 4 months (MD 0.06, 95% CI [-0.36, 0.48]) when the additional poster contest was organized, could not be demonstrated.
4.3.2.4 Hygiene messaging with elements of disgust versus hygiene messaging alone
Guiteras et al. (2015a) measured the effect of focusing on “disgust” in an educational intervention (hygiene messaging) in urban Dhaka, Bangladesh, implementing a handwashing and water supply/quality intervention (Analyses 36-37). The educational intervention was embedded in a broader intervention consisting of infrastructure promotion, a free trial of water treatment and handwashing hardware (chlorine dispenser), reminder visits, sales coaching and a sales offer (giving the opportunity to purchase hardware for a fee). Using additional elements of disgust in an educational approach did not result in an increase of handwashing after last defecation at 3.5 and 7 months (RR 1.00, 95% CI [0.95, 1.07]; RR 0.98, 95% CI [0.92, 1.05]), and at all 3 key times at 3.5 and 7 months (RR 1.39, 95%CI [0.89, 2.15); RR 1.27, 95% CI [0.86, 1.88]). No significant effect on the feeling of disgust when hands are not washed with soap could be demonstrated at 3,5 (RR 0.99, 95% CI [0.96, 1.01]), and 7 months (RR 1.00, 95% CI [0.99, 1.01]). This study also measured knowledge concerning “usual times to wash hands with soap”: a significant increase of knowing all 3 key times for handwashing with soap was shown at 3.5 months (RR 1.38, 95% CI [1.01, 1.68]) and 7 months (RR 3.38, 95% CI [2.24, 5.11]) follow-up. At 7 months, the knowledge about “other key times” also significantly increased (RR 3.09, 95% CI [1.42, 6.76]), however an effect on knowledge about “after defecation” as usual time to wash hands with soap could not be demonstrated (Guiteras et al., 2015a).
4.3.2.5 Elements of psychosocial theory: motivational intervention followed by self-regulatory intervention versus self-regulatory intervention followed by motivational intervention
Lhakhang et al. (2015) implemented a handwashing intervention, and compared a group that received a motivational intervention followed by a self-regulatory intervention 17 days later, with a group that received the same two intervention modules in the opposite order. No statistically significant overall difference in handwashing was found between the 2 different programmes (MD 0.09, 95% CI [-0.18, 0.37]). However, when only the first intervention was implemented, a statistically significantly higher degree of handwashing was shown in the group that received the self-regulatory intervention compared with the group that received the motivational intervention (MD -0.78, 95% CI [-1.07, -0.5]). For “intention”, after introducing both programme elements, a statistically significantly higher degree of intention was measured for the group that first received self-regulatory elements followed by motivational elements (MD -0.80, 95% CI [-1.09, -0.52]). For “self-efficacy”, a higher degree of self-efficacy was found after receiving only the self-regulatory intervention, compared to the group that only received the motivational intervention (MD -0.83, 95% CI [-1.12, -0.55]), but after receiving both elements the significant difference disappeared (MD -0.16, 95% CI [-0.44, 0.11]). For “planning”, again the group only receiving the self-regulatory intervention showed significantly better results (MD -1.71, 95% CI [-2.03, -1.39]), but after receiving both elements of the intervention, the group that first received motivational and then self-regulatory elements scored significantly better (MD 0.31, 95% CI [0.03, 0.59]).
4.3.2.6 Community Health Clubs versus Community-Based Total Sanitation
Whaley & Webster (2011) compared two different types of community-based approaches, Community Health Clubs versus Community-Based Total Sanitation. Both interventions contained all WASH components. No significant difference in latrine use could be demonstrated between the two approaches, 6 months and 2 years after the start of the programme(RR 0.96,95% CI [0.74, 1.25] and RR 2.20,95% CI [0.97, 5.01]). In addition, no difference in open faecal disposal could be shown, 6 months and 2 years after the start of the programme(RR 1.19,95% CI [1.00, 1.42] and RR 1.04,95% CI [0.96, 1.12]).
4.3.2.7 Hygiene messaging and infrastructure promotion versus hygiene messaging alone
Zhang et al. (2013), measured the effect of adding an infrastructure promotional component to a school-based educational intervention focused on handwashing (hygiene messaging). A statistically significant improvement in handwashing (RR 8.48,95% CI [5.31, 13.55]), handwashing when using the toilet (RR 4.19,95% CI [3.08, 5.71]), and handwashing with soap (RR 6.50,95% CI [4.15, 10.19]) could be demonstrated, as a result of implementing an infrastructure promotional component.
4.3.3 Effect of different communication strategies
An overview of the findings on studies comparing different communication strategies is given in Table 42 and described in detail below.
Overview of the findings on studies comparing different communication strategies
All mean differences are presented as Cochran-Mantel-Haenszel estimate, [95% CI]. MD: Mean difference; CI: Confidence interval; yrs: years. *p<0.05
4.3.3.1 Mass media and interpersonal communication versus mass media alone
Only in one experimental study, with a moderate risk of bias, two types of communication strategies were compared (Chase & Do, 2012). The programme in the study focused on handwashing and was based on psychosocial theory (based on the FOAM framework), and a combination of mass media and interpersonal communication activities was compared with mass media alone.
The additional component of interpersonal communication resulted in a statistically significant increase in handwashing, less than 12 months after the programme period (“adherence”) (MD 0.01, 95% CI [0.01, 0.01]) (Analysis 38). In addition, an increase in handwashing at different key times (after faecal contact, before food preparation, before (breast) feeding a child, when hands look or feel dirty) was measured. An increase in “handwashing while doing laundry” could not be demonstrated, and, surprisingly, a significant decrease in “handwashing before eating” was measured (Chase & Do, 2012) (Analysis 39). Finally, a significant decrease in diarrhoea (MD -0.02, 95% CI [-0.02, -0.02]), and acute respiratory tract infection (MD -0.04, 95% CI [-0.05, -0.04]) was shown when using additional interpersonal communication activities (Chase & Do, 2012) (Analysis 40).
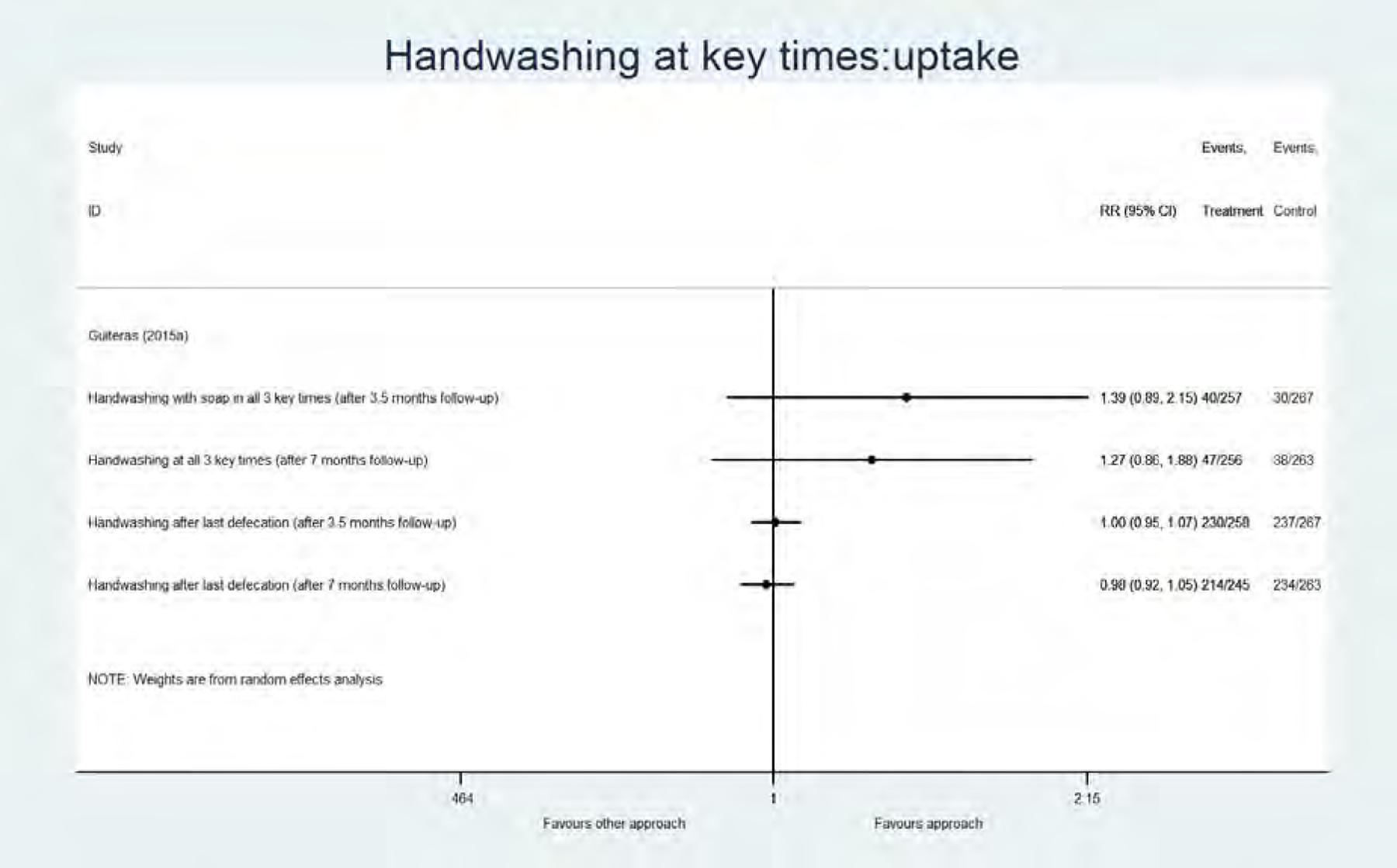
Analysis
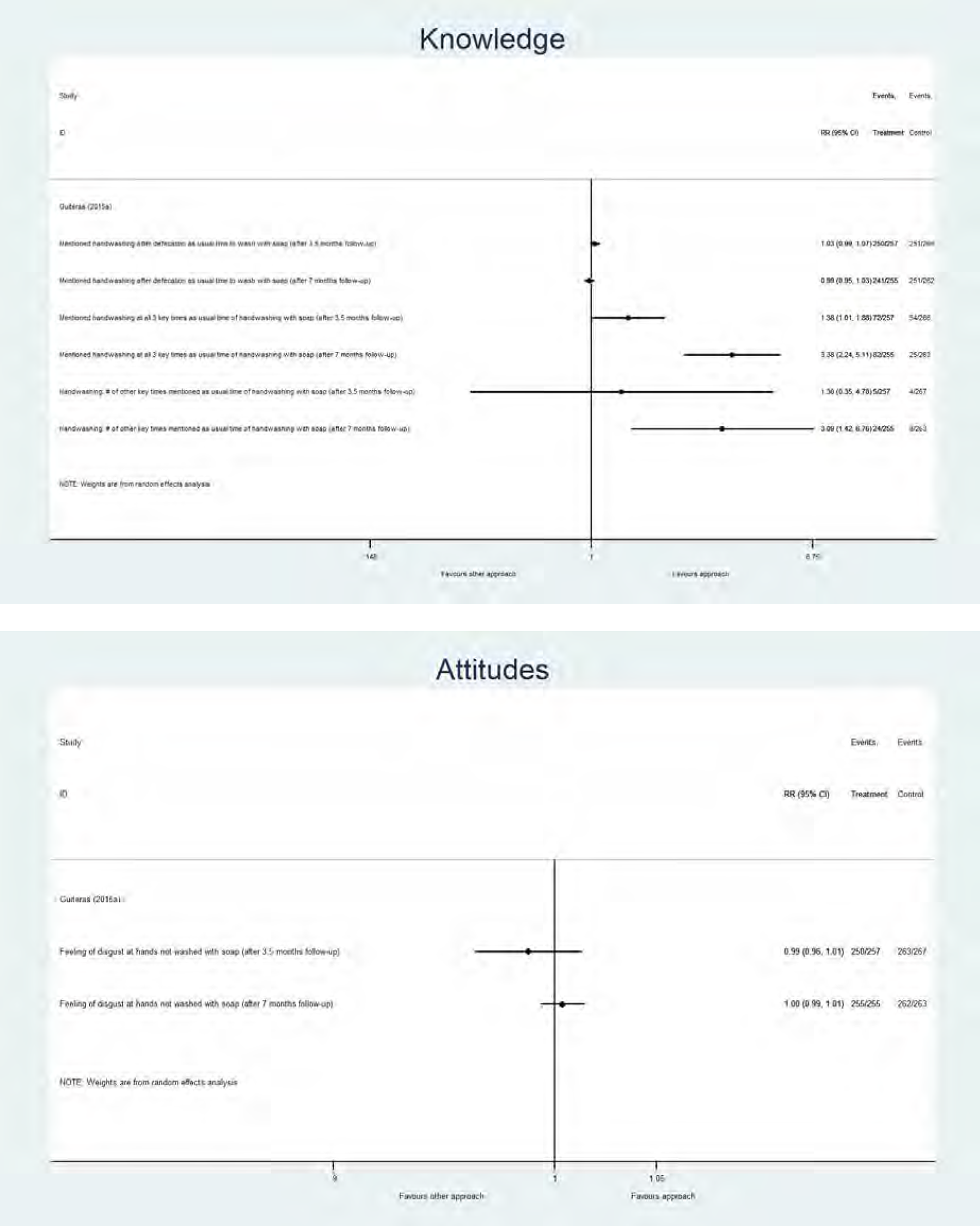
Analysis
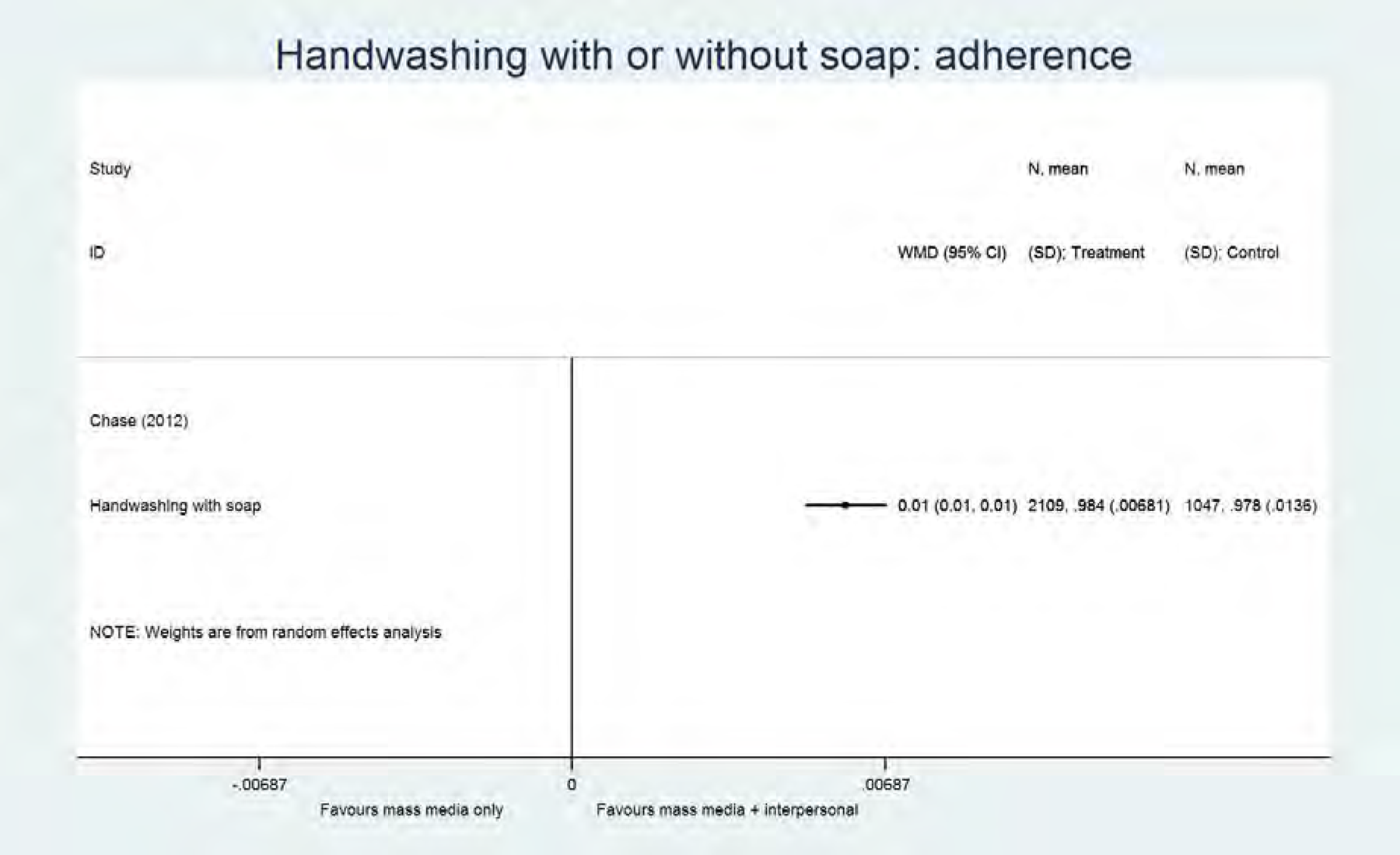
Analysis
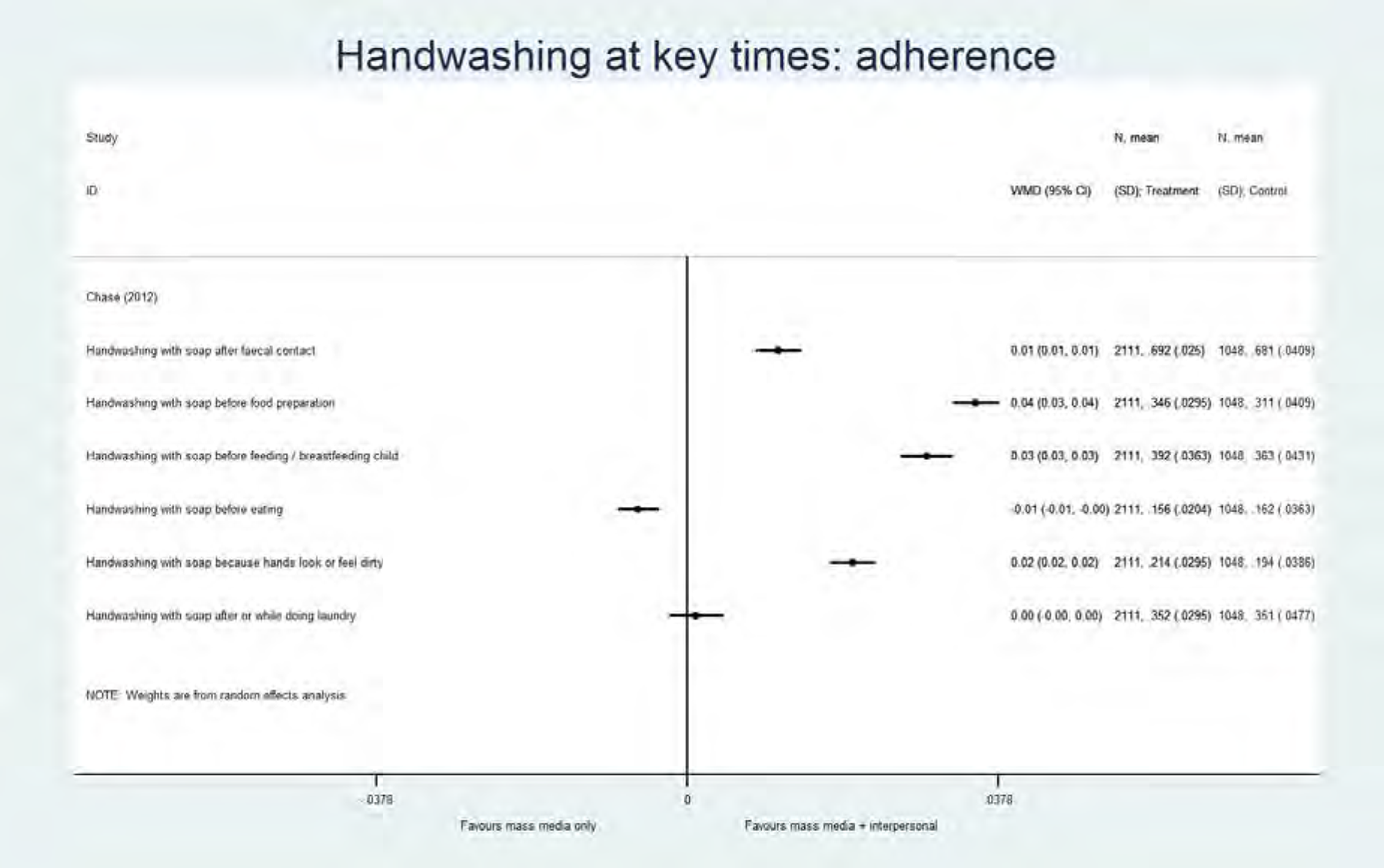
Analysis
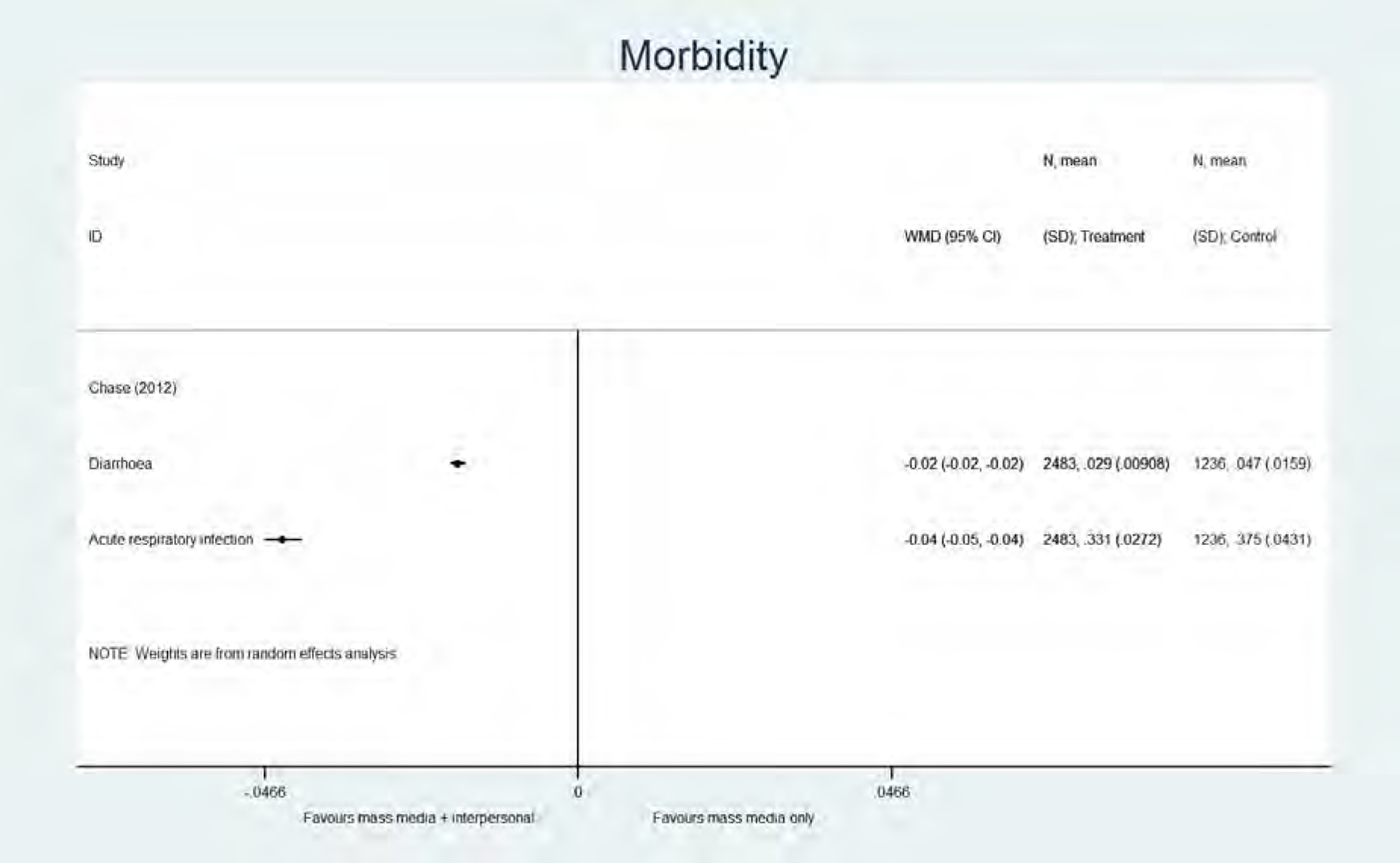
Analysis
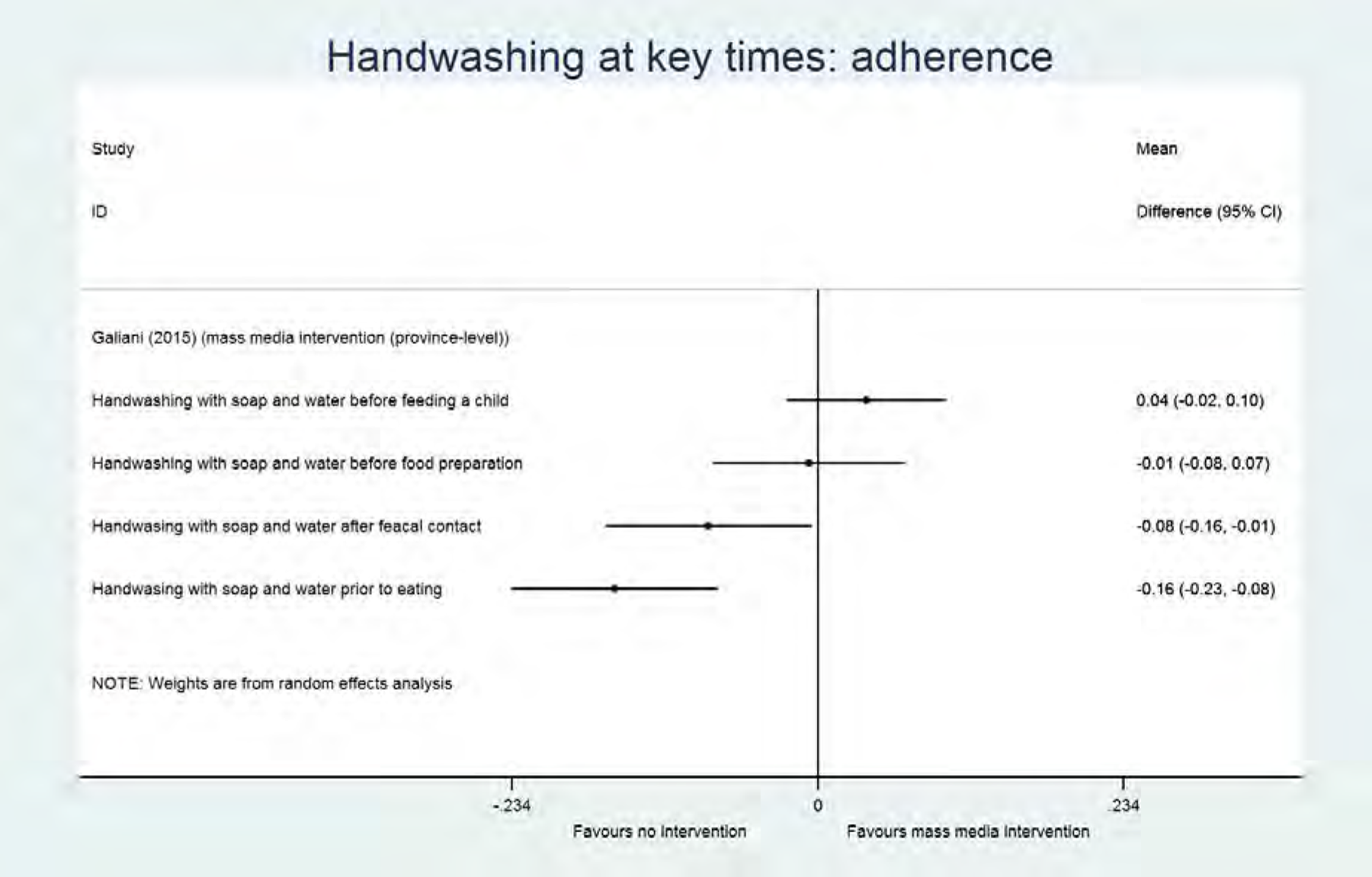
Analysis
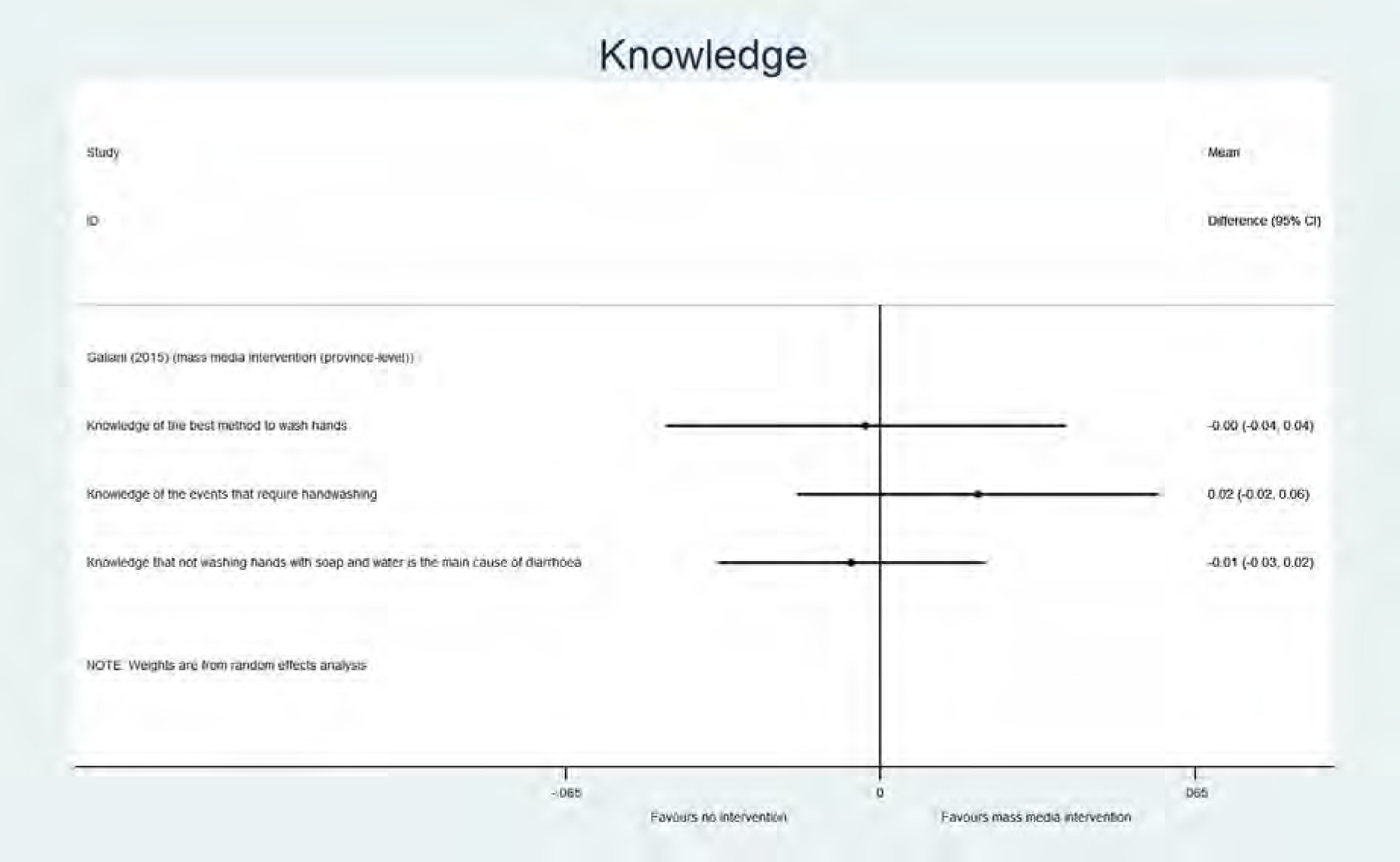
Analysis
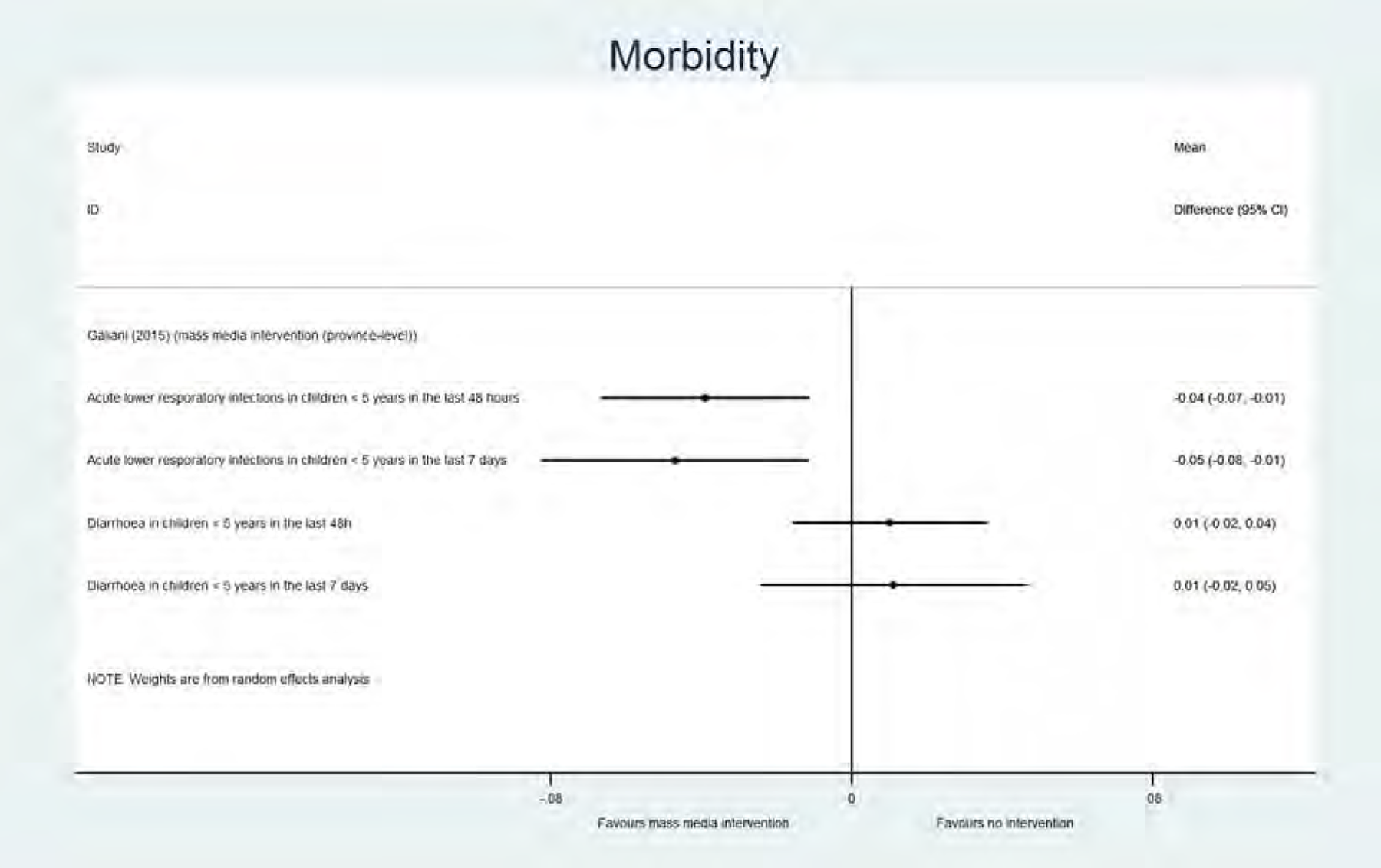
Analysis
4.3.3.2 Mass media and direct consumer contact versus no promotional approach
One study, using a social marketing approach to implement a handwashing intervention, compared a mass media campaign with direct consumer contact (province level intervention) to not using a promotional approach (Galiani et al., 2012/2015). In the intervention arm with only the mass media and direct consumer contact results were mixed (Analyses 41-43): surprisingly a significant decrease in handwashing at two different key times, in the period less than 12 months after the end of the implementation (“adherence”) (after faecal contact: MD -0.08, 95% CI [-0.16, -0.01]; prior to eating: MD -0.16, 95% CI [-0.23, -0.08]) was shown, and an effect in handwashing at two other key times could not be demonstrated (before feeding a child: MD 0.037, 95% CI [-0.02, 0.1]; before food preparation: MD -0.007, 95%CI [-0.08, 0.07]). In addition, an effect on knowledge of the best method to wash hands (MD -0.003, 95% CI [-0.04, 0.04]), of the events that require handwashing (MD 0.02, 95% CI [-0.02, 0.06]) and about not washing hands as the cause of diarrhoea (MD -0.006, 95% CI [-0.03, 0.02]) could also not be demonstrated. Finally, an effect on diarrhoea in children under five years was not shown (recall period 2 days: MD 0.01, 95% CI [-0.02, 0.04]; recall period 7 days: MD 0.011, 95% CI [-0.02, 0.05]), however a significant decrease of acute lower respiratory infections in children under five years was found (recall period 2 days: MD -0.039, 95% CI [-0.07, -0.01]; recall period 7 days: MD -0.047, 95% CI [-0.08, -0.01]) (Galiani et al., 2012/2015).
In a second intervention arm, elements of community involvement were added to the mass media intervention. Results are described in paragraph 4.3.1.3. It can be concluded that for handwashing (only at school level) and knowledge more effect was reached when the community was involved.
5 Results: Factors influencing implementation
5.1 DESCRIPTION OF STUDIES
5.1.1 Results of the search
The identification of qualitative studies was performed in parallel with the identification of quantitative studies, since the same search strategy was used. Therefore, full text screening of 400 records, as described in 4.1.1, also resulted in a number of qualitative studies. We finally identified 28 qualitative studies, of which 24 were found through database searching (19 qualitative studies and 5 mixed-methods studies) and 4 from the grey literature. In addition, 5 mixed-methods studies were identified, as described above. The study selection flowchart is depicted in Figure 3 (see 4.1.1).
5.1.2 Included studies (n=28)
An overview of the characteristics of the included qualitative studies can be found in Table 43. The majority of the studies (n=19, 68%) was published in the last 5 years, with only 9 studies published between 2002 and 2011. Countries (see Figure 12)
Most of the studies (n=15, 53%) were performed in Sub-Saharan Africa (Kenya (n=3), Tanzania (n=3), Zimbabwe (n=2), Nigeria (n=1), Ethiopia (n=1), Malawi (n=1), Uganda (n=1), Zambia (n=1), Somalia (n=1) and South Africa (n=1)). Ten studies (36%) were performed in Asia:7 studies in South Asia (Bangladesh (n=3), India (n=3) and Nepal (n=1) and 3 studies in South-East Asia (Vietnam (n=2) and Cambodia (n=1)). Only 4 studies (11%) were conducted in Latin America and the Caribbean (El Salvador (n=1), Haiti (n=1) and Peru (n=1)).
Considering country income at the time the studies were performed, 19 studies (68%) were conducted in low-income countries (Bangladesh, Cambodia, Ethiopia, Haïti, Kenya, Malawi, Nepal, Somalia, Tanzania, Uganda, Vietnam (until 2008) and Zimbabwe) and 9 studies (34%) in lower middle-income countries (El Salvador, India, Nigeria, Peru, South Africa, Vietnam (from 2009) and Zambia). Setting and target level

World map indicating in which countries the included qualitative studies were performed
Most (68%) of the studies were executed in a rural setting (n=19), 3 studies (11%) were performed in an urban setting, 2 studies (7%) were executed in both a rural and urban setting and 3 studies (11%) were performed in an informal-rural setting (i.e. slums, settlements). One study (3%) did not provide any information about the setting in which the study was conducted. The intervention was targeted at a community level in 22 studies (12 on a community level, 4 on a (sub-) district level, 2 on a household level, 2 on a village level, 1 on a compound level and 1 on a county level) and at a school level in 3 studies. Two studies investigated interventions on both a school level and a community level (n=1) or village level (n=1). One study did not provide any information about the target level in which the study was conducted. WASH components
The following (combination of) WASH components were present in the interventions: WASH (general) in 11 studies, sanitation only in 9 studies, handwashing only in 4 studies, handwashing/sanitation in 1 study, handwashing/sanitation/water supply in 1 study, and handwashing/sanitation/hygiene/water quality in 1 study. Promotional approach
We classified the promotional approaches in 4 main groups according to the same criteria used for the quantitative studies (see 4.1.2: promotional approach). The approach in 18 studies (64%) was considered as a community-based approach, a social marketing approach in 2 studies, sanitation and hygiene messaging in 5 studies, and the intervention was based on elements of psychosocial theory in 3 studies.Table 44 shows which studies were grouped under each category, and Figure 13 in addition also provides the WASH component of each study.
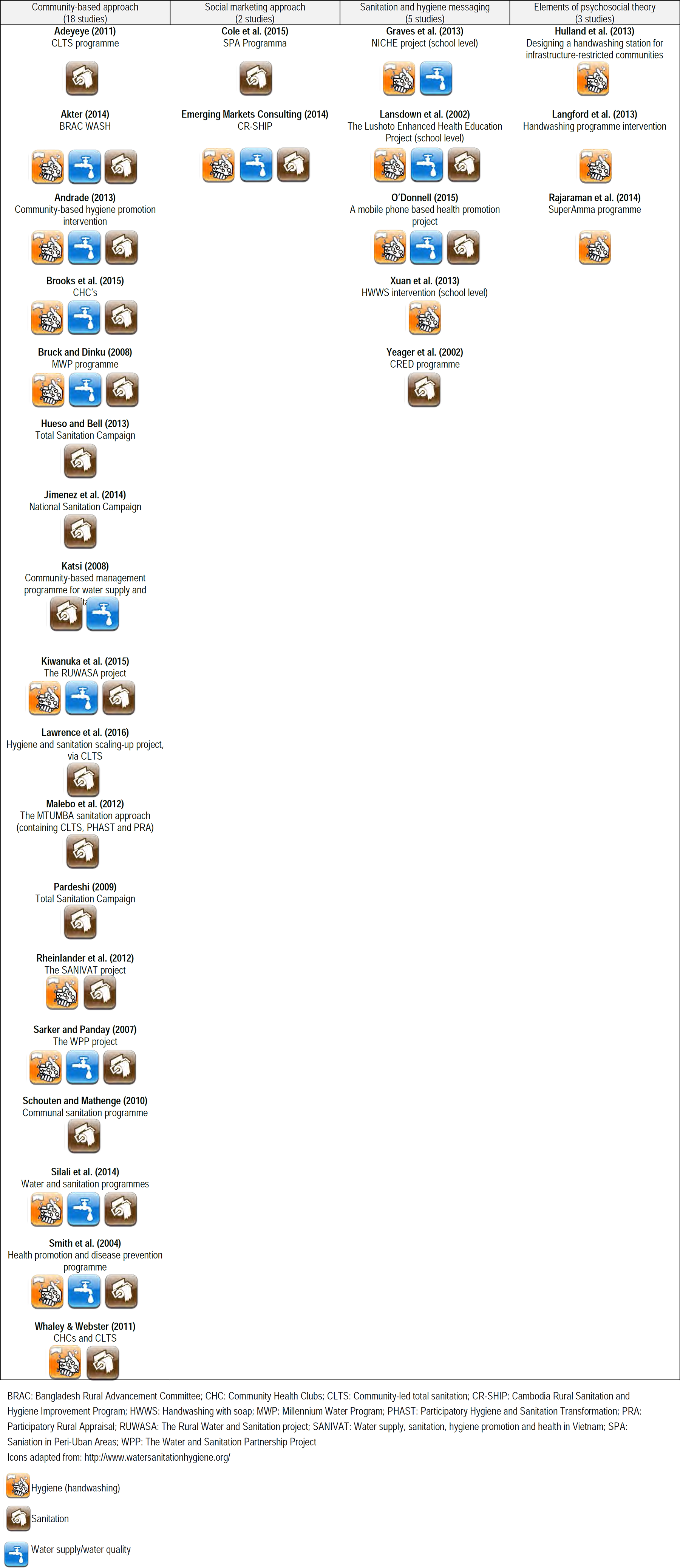
Main categories of promotional approaches with detailed indication of WASH component and specific promotional approach for each included qualitative study
Characteristics of the included qualitative studies
List of included qualitative studies in each of the 4 categories of promotional approaches
5.1.3 Excluded studies
Since study selection was performed in parallel for both the quantitative and qualitative studies, the main reason for exclusion of papers is described for both study types in paragraph 4.1.3. Detailed information can be found in Appendix 9 (List of excluded database studies) and 10 (List of excluded grey literature studies), and the reference list of excluded studies.
5.2 QUALITY ASSESSMENT OF INCLUDED STUDIES
We appraised the quality of each study according to the 10 items of the Critical Appraisal Skills Programme (CASP) tool (see Figure 14).
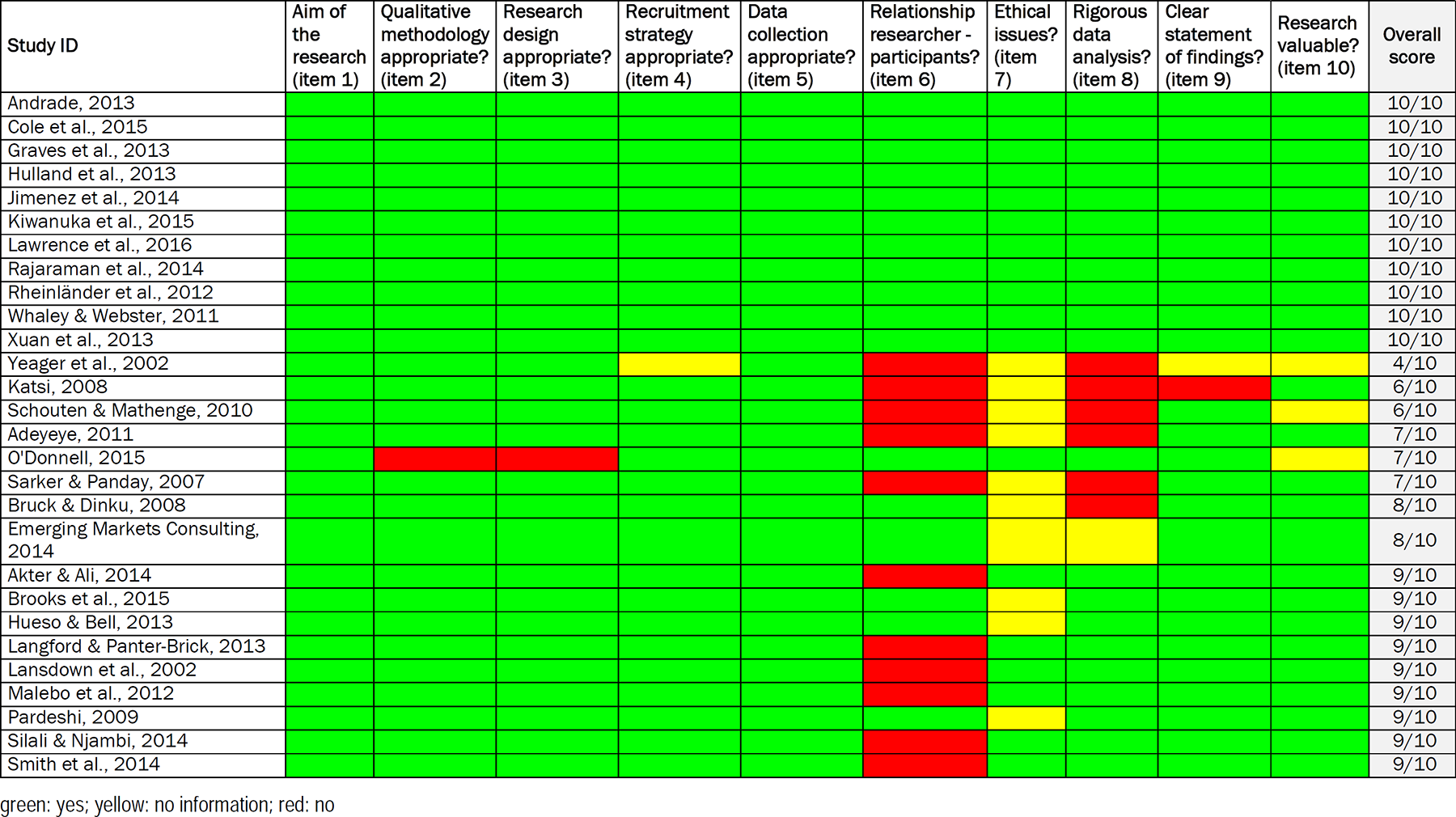
Quality assessment of qualitative studies using CASP checklist
All studies provided clear statements of the research aims (item 1). The use of qualitative methodology (item 2), the qualitative research design that was used (item 3), the recruitment strategy (item 4) and the data collection techniques (item 5) were considered as appropriate in almost all studies. A clear statement of findings (item 9) was present in 26 studies (93%) and the research was considered as a valuable contribution (item 10) in 25 studies (89%). The relationship between researcher and participants was adequately considered in 17 studies (61%), which was evidenced via member checking or matching demographic variables between interviewer and target group. Ethical issues were explicitly considered in 18 studies (64%) and the data analysis was sufficiently rigorous in 21 studies (75%).
5.3 SYNTHESIS OF RESULTS
The term ‘category’ was used as an umbrella term to define the overall process and implementation issues, namely the process evaluation factors, the programme environment factors and the recipient/implementer-related (contextual) factors. Specific factors in these categories (e.g. acceptability as a process evaluation factor or demographic variables as a personal contextual factor) were defined as ‘themes’ and barriers/facilitators related to these themes were called ‘factors’.
For many of the factors we describe below, we make the distinction between implementer-related factors and recipient-related factors. Because often community members are also involved in the implementation of a programme, they can be the implementer and recipient at the same time. For the description below we defined the implementer as: (1) the organization, NGO or funding body that is the primary implementer of the approach, or (2) a change agent, health promoter or member of the community involved in the implementation as a secondary implementer. A recipient is defined as a member of a household, a villager, or trainee, receiving the promotional approach.
5.3.1 Process evaluation factors
Barriers/facilitators related to almost all (7/9) pre-identified process evaluation themes (acceptability, dose, engagement, fidelity, reach and satisfaction) were extracted from the qualitative studies. No information was available for 2 factors: recruitment and attrition. An overview of all barriers and facilitators identified can be found in Table 45 and Appendix 11. Acceptability
Barriers and facilitators in the category “Process evaluation factors”
Acceptability refers to the quality or state of meeting one's needs adequately. Evidence from 3 studies identified recipients not willing to change their Dose
Dose refers to the content, frequency, duration and coverage of the programme. Several of the included studies identified the following barriers related to dose of the programme: the messages are Engagement
Engagement refers to the subjective attributes that define the recipient's participation in interaction with or receptivity to an intervention. It also refers to the subjective attributes of programme staff that can influence their capacity to deliver intervention strategies (Cargo et al., 2015). The following barriers at the level of the implementer and related to recipient engagement were found:
People from the interviews or focus group discussions also indicated several positive factors (facilitators) at the level of the implementer, including Fidelity
Fidelity reflects the extent to which an intervention is implemented as originally intended by programme developers (Cargo et al., 2015). One school-based study conducted in India suggested that Reach
Reach refers to the degree to which the intended audience participates in an intervention by ‘their presence’ (Cargo et al., 2015). In at least one study with a primarily social marketing approach, the Satisfaction
Satisfaction refers to the fulfilment of a need or want. Several of the included studies contained potential barriers related to the satisfaction of the recipients/implementers. The following barriers at the level of the implementer and related to the satisfaction of the recipient were found:
Other evidence identified 9 potential facilitators to keep recipients/implementers satisfied:
5.3.2 Programme environment factors
Barriers/facilitators related to all programme environment themes (training materials, funding/resources, intent of a programme to change a specific outcome, providing leadership to the implementing organization and partnerships) were extracted from the qualitative evidence. One additional theme was developed after coding the primary evidence/author statements: community capacity. An overview of all barriers and facilitators identified can be found in Table 46 and Appendix 12. Training materials
Barriers and facilitators in the category “Programme environment factors”
Evidence from five studies identified the following potential barriers related to training materials:
Two studies with a major community-based component and 1 study promoting water and sanitation via educational messaging identified sufficient Community capacity
Several of the included studies identified the following barriers:
In two school-based programmes focusing on sanitation (Lansdown et al., 2002) or sanitation, handwashing and water supply (Graves et al., 2013), teachers and mothers indicated that Funding/resources
The most frequent reported barrier, identified in different community-based approaches (such as the MTUMBA approach in Tanzania, RUWASA in Uganda, and CLTS in Zambia) and social marketing programmes, was the
From interviews and focus group discussions conducted during the CLTS approach in Tanzania, it was noted that Intent of a programme to change a specific outcome
Community Health Club facilitators indicated that changing their Providing leadership to the implementing organization
During the Total Sanitation Campaign in India, the Partnership, coordination between providers of the same intervention or other health interventions
Several community-based studies implemented in different continents (Sub-Saharan Africa, The Caribbean and South-East Asia) criticized the Training/qualification of the implementers
Evidence from 1 educational promotional programme and 1 community-based sanitation/water supply intervention, both conducted in Sub-Saharan Africa, suggested a
5.3.3 Implementer-related factors
In our initial ToC, we only defined recipient-related factors in addition to the programme environment factors and process evaluation factors. However, in community-based approaches the recipients are typically involved as (secondary) implementer, called for example a health promoter or community leader. However, at the same time they are also recipient of the approach. We therefore created a separate category “implementer-related factors”, containing the same factors as were predefined for the recipients. Barriers/facilitators related to most (4/6) pre-identified factors were extracted from the qualitative studies. No information was available for 2 factors: self-efficacy and awareness about personal risk. An overview of all barriers and facilitators identified can be found in Table 47 and Appendix 13. Awareness about costs and benefits
Barriers and facilitators in the category “Implementer-related factors”
For this factor, we only identified evidence from a study describing a social marketing approach and making use of a loan system (Emerging Markets Consulting, 2014). The Motivation
Motivation was a newly identified theme, compared to our initial ToC. A factor negatively influencing the motivation of sanitation teachers was Planning skills
Others showing behaviour
For the implementer it was important that people in the environment began to show the correct behaviour. In a study describing a school-based education approach, Public commitment
On the level of the implementer some evidence was found in a study describing a social marketing approach about the lack of commitment of the loan officers, which slowed down the loan process (Emerging Markets Consulting, 2014).
5.3.4 Recipient-related factors
In our initial ToC, we included 6 recipient-related factors (themes) that might influence implementation of promotional approaches: awareness about costs and benefits, planning skills, awareness of personal risk, others showing behaviour, public commitment and self-efficacy. For all these categories, barriers and facilitators were identified. In addition, two extra recipient-related themes were identified in the included studies, namely motivation and knowledge. An overview of all barriers and facilitators identified can be found in Table 48 and Appendix 14. Awareness about costs and benefits
Barriers and facilitators in the category “Recipient-related factors”
Several barriers were identified, related to the recipients’ awareness about costs and benefits of the implemented intervention. Recipients were reported by several studies to be concerned about their
Nevertheless, the Motivation
A barrier for implementation that was mentioned by studies on community-based and approaches containing elements of psychosocial theories was that recipients had
A potential motivational facilitator that was reported by two community-based approach studies, was the fact that interventions which required Planning skills
In one social marketing-based intervention study, the application of Awareness of personal risk
Being
Conversely, being Knowledge
A study on a social marketing-based promotional approach, where people could apply for micro-loans, suggested that recipient's
On the other hand, Norms
In one study on a community-based promotional approach, it was noticed that a
Conversely, if there was Others showing behaviour
A study on a community-based approach, using a model-home competition used to stimulate community members to compete with each other in hygienic behaviour, found that this
On the other hand, if done less explicitly, Public commitment
In a community-based promotional approach study, where people were invited to become part of a community health club, it was suggested that this type of Self-efficacy
A community-based approach study stated that
Therefore, keeping community-based interventions simple might be a facilitator for the implementation (Andrade, 2013). Furthermore, self-efficacy could also be a facilitator for implementation of community-based approaches (Lawrence et al., 2016).
5.3.5 Implementer-related contextual factors
In our initial ToC, we included a box with socio-cultural, physical and personal contextual themes of the recipients. However, since the contextual factors of the implementers were as important, we included a separate category of implementer-related contextual themes. An overview of all barriers and facilitators identified can be found in Table 49 and Appendix 15. Personal context
Barriers and facilitators in the category “Implementer-related contextual factors”
Barriers/facilitators of different Socio-cultural context
Barriers/facilitators of the following themes were identified: dignity and respect, information environment, law-legislation, socioeconomic status-role model-authority and social capital. No statements were linked to culture, religion, ethnicity, minorities or division of labour. Social-political environment was created as a new theme. In two studies, it was suggested that implementers being friendly, treating the villagers well, paying attention to language and attitude towards the villagers, and having a relationship of trust are facilitators of implementation (Andrade, 2013; Emerging Markets Consulting, 2014). Furthermore, the continued Physical context
Barriers of the following themes were identified: available space, natural and built environment, place of residence (rural vs urban) and remote areas (Schouten & Mathenge, 2010; Brooks et al., 2015; Lawrence et al., 2016; Rheinländer et al., 2012). More in detail, evidence suggested that
5.3.6 Recipient-related contextual factors
For almost all themes/sub-themes included in our initial ToC, at least one barrier or facilitator was found in the included studies. An overview of all barriers and facilitators identified can be found in Table 50 and Appendix 16. Personal context
Barriers and facilitators in the category “Recipient-related contextual factors”
Several
One study describing an approach containing elements of psychosocial theories suggested that
One study concerning an approach containing elements of psychosocial theories, using public pledging, suggested that Social-cultural context
Different sub-themes were included in our initial TOC: culture, division of labour, ethnicity, law/legislation, minorities, status/role model/authority, social capital, dignity/respect, religion, information environment. For all subthemes but dignity/respect and religion, at least one recipient-related contextual facilitators or barrier was identified.
Concerning cultural factors, one study using sanitation and hygiene messaging identified
One study on a community-based intervention suggested that taking into account the
With regard to law/legislation, a barrier towards the implementation of promotional approaches was
For the sub-theme minorities,
Concerning status/role model/authority,
Several facilitators with regard to social capital building were suggested. The improvement of Physical context
Several sub-themes were included in our initial ToC concerning recipient-related physical contextual factors: available space, low vs middle-income countries, natural and built environment, place of residence, remote areas and safety. For all these sub-themes, at least one facilitator or barrier was identified.
Living in
With regard to income, living in a
Concerning the natural/built environment sub-theme,
The place of residence also influenced programme implementation, as living in
Living in
One study describing a sanitation and hygiene messaging intervention showed that
5.3.7 Sensitivity analysis
A sensitivity analysis (excluding studies with a CAP-score < 8/10, i.e. 6 studies, see figure 14) was included to evaluate the magnitude of methodological flaws or the extent to which it has a small rather than a big impact on the findings and conclusions. Overall, the impact of excluding the 6 lower quality studies was considered as rather small. The robustness of the evidence around the barriers/facilitators of the
6 Discussion
6.1 SUMMARY OF MAIN RESULTS
6.1.1 Quantitative studies
In total, 42 quantitative studies were identified. The effect of a promotional approach versus not using a promotional approach on sanitation and handwashing behaviour change, behavioural factors (knowledge, skills, attitude, norms and self-regulation) and health-related outcomes (morbidity and mortality), was examined in 34 different studies. In addition, 7 studies compared specific promotional approaches versus other promotional approaches, and 2 studies compared two different communication strategies. Methodological heterogeneity across studies was present, i.e. difference in programme content (27 different combinations of promotional elements), study types (32 experimental, 8 quasi-experimental and 2 observational studies), outcome types (binary versus continuous versus (un) adjusted calculated effect sizes), methods of measurement (self-reported versus direct observation) and timing of measurement (during programme implementation versus ≤12/>12 months after implementation of the programme).
To find out the absolute effect of any promotional approach (versus not using a promotional approach), we pooled data across approaches in several meta-analyses. However, because of the above described heterogeneity, only a small proportion of the data could be pooled, and statistical heterogeneity (I2>50%) was found in most of the meta-analyses, making it difficult to formulate clear conclusions about which promotional approach is the most effective.
Subsequently, we looked at the individual (unpooled) outcomes across the 4 categories of promotional approaches/promotional elements (compared to not using a promotional approach). An overview of these outcomes, with an indication of their results and the certainty of the evidence according to the GRADE approach, is provided in Table 51. The promotional approach as well as the WASH component(s) of the intervention is also shown in this table. Based on this table and the additional information about the study characteristics, we were able to formulate the following conclusions: Community-based approaches (n=12). Community-based approaches involve community members in the implementation of the approach, and shared decision-making is typically part of the approach. All but one study in this category implemented a sanitation intervention, in some cases combined with a handwashing and/or water supply/water quality component. Community-based approaches may improve Social marketing approaches (n=6). Social marketing approaches are aimed at creating demand and make use of commercial enterprise techniques. All but one study in this category implemented a handwashing intervention, with one study of these also having a sanitation-only and a combined intervention group, one study that combined with a water supply/water quality component, and one sanitation-only study. No uniform positive effect was shown for Sanitation and hygiene messaging (n=12). Sanitation and hygiene messaging are educational approaches mainly using one-way communication and a directive way of educating. All but one study in this category implemented a handwashing intervention, in some cases combined with a sanitation and/or a water supply/water quality component. Sanitation and hygiene messagin gprobably improves Elements of psychosocial theory (n=4). In four studies a small-scale intervention was studied based on behavioural factors derived from a psychosocial theory, using formative research. All studies implemented a handwashing-only intervention. Elements of psychosocial theory may improve
Overview of quantitative studies comparing a promotional approach versus no promotional approach, with indication of results and certainty of evidence for primary outcomes (GRADE approach)
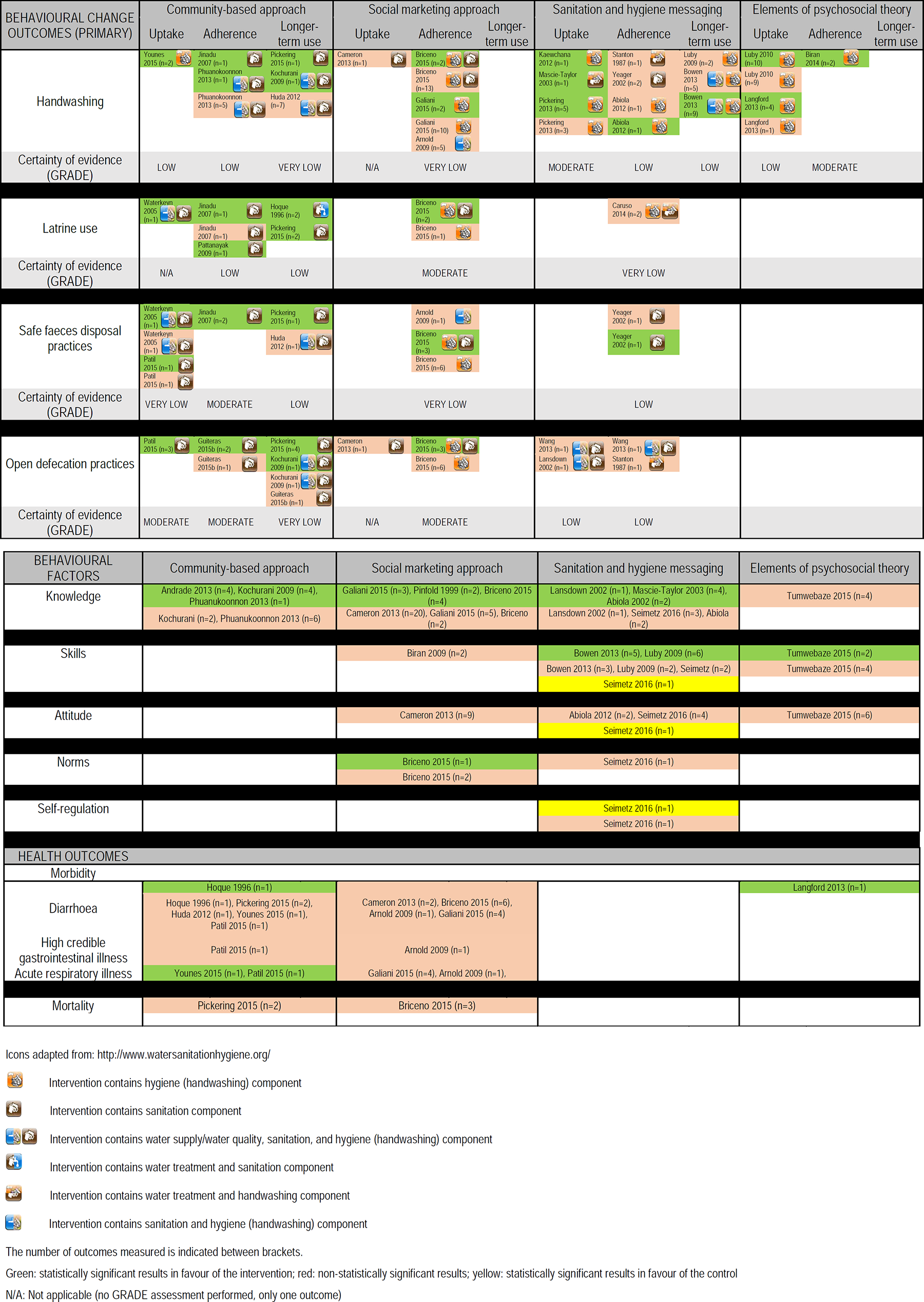
The addition of separate elements derived from psychosocial theory, to an existing educational (hygiene messaging) approach, was measured in 3 studies: Infrastructure promotion (and use of reminders). Statistically significantly improved handwashing was shown, when adding a component of infrastructure promotion to a school-based health education (hygiene messaging) intervention (Zhang et al., 2013). In a second study, use of infrastructure promotion and reminders also resulted in a significant increase in handwashing, and a significant correlation between the promotional approach and the majority of measured behavioural factors (Contzen et al., 2015a/2015b). Public commitment and use of reminders. A statistically significant increase in handwashing could not be demonstrated, and a significant correlation between the promotional approach and less than half of the measured behavioural factors was shown (Contzen et al. 2015a/2015b). Infrastructure promotion combined with public commitment and use of reminders. The addition of elements of infrastructure promotion, public commitment and the use of reminders, to a health education (hygiene messaging) intervention, resulted in a significant increase in handwashing and a significant correlation between the promotional approach and several behavioural factors (Contzen et al., 2015a/2015b). Elements of disgust. When the hygiene messaging approach appealed to feelings of “disgust” in an urban area in Bangladesh, this resulted in improved knowledge of handwashing key times, but an effect on handwashing and on the feeling of disgust could not be shown (Guiteras et al., 2015a).
In addition to studies comparing a promotional approach with not using a promotional approach, some studies also investigated the relative effectiveness (comparison of two different types of approaches) (4 studies): Community-based approach: Community Health Clubs versus Community-Based Total Sanitation. No difference in latrine use and open faeces disposal was shown for this comparison (Whaley & Webster, 2011). Social marketing approaches: local-builder social marketing versus outside-expert building team. The local-builder social marketing approach resulted in a significant decrease in the number of households refusing to use the new toilet (Dickey et al., 2015). Hygiene messaging in schools: education with poster contest versus education alone. Adding a poster contest to a school-based education intervention did not result in a significant increase in handwashing (Graves et al., 2011). Elements of psychosocial theory: motivational intervention followed by self-regulatory intervention versus self-regulatory intervention followed by motivational intervention. No difference in handwashing could be demonstrated between these two interventions (Lhakhang et al., 2015).
Two studies compared different communication strategies: Intervention based on psychosocial theory: interpersonal communication. A significant increase in handwashing and decrease in morbidity outcomes was shown when interpersonal communication was added to a mass media campaign (Chase & Do, 2012). Social marketing approach: mass media campaign. It was shown that a mass media campaign alone had no effect on behaviour (handwashing) and behavioural factors (knowledge), while a combination with community involvement had some effect on handwashing and knowledge (Galiani et al., 2012/2015).
Finally, we also focused on the use of incentives as part of the promotional approach, which was the case in 10 of the included studies. Financial incentives included a modest salary and subsidies, and non-financial incentives included a motorcycle, lunch, food, gifts and soap. Incentives were mostly used in studies describing a community-based approach, but were also included in the other approaches. When comparing the studies with or without use of incentives, no major differences were seen, and absolute effects were similar. However, one study compared programmes with and without use of subsidies, and found significant better results for open defecation when subsidies were included as part of the community-based programme (Guiteras et al., 2015b). Use of incentives could be promising and warrants more research.
In summary, since each study described a specific promotional approach, even within one category of approaches, it was difficult to generalise our findings. However, several promising promotional elements were identified. The most consistent results were obtained within the category of community-based approaches, where at least a sanitation component was part of the programme. It was concluded that working in a community-based way may be effective in terms of handwashing with soap, and sanitation outcomes (latrine use, safe faeces disposal, and open defecation). The use of social marketing approaches seems to be less uniformly applicable, and this approach mainly shows an effect on sanitation outcomes when sanitation is part of the intervention. When implementing a social marketing approach, working with the community, for example using local builders, and considering consumer preferences, could be crucial. Sanitation and hygiene messaging, with a focus on handwashing with soap, seem to have an effect on handwashing with soap immediately after the intervention has ended. However, these effects are not sustainable in the long term. The use of elements derived from psychosocial theory, such as infrastructure promotion, public commitment, or elements of disgust, seems promising and warrants further research. Finally, the methods used for communicating the content of a certain promotional approach, also play a role, and the use of interpersonal communication was shown to be effective in certain circumstances. None of the promotional approaches described in the review showed consistent effects on behavioural factors such as knowledge, skills and attitude. Also no consistent effects on health were demonstrated.
6.1.2 Qualitative studies
In total, 28 qualitative studies were identified. Below we give a summary of the 6 categories of influencing implementation factors for which barriers and facilitators were identified from qualitative research. First, we list influencing factors that were relevant across all promotional approaches. Process evaluation factors. In the initial ToC, nine process evaluation factors were identified. For 2 of these, recruitment and attrition, no barriers and facilitators from qualitative studies were identified. Barriers and facilitators that were relevant across different types of promotional approaches were: intervention duration, visit frequency, and communication methods, with use of long messages and lack of communication being barriers for implementation. Programme environment factors. In the initial ToC 6 process evaluation factors were included. For each factor, barriers and facilitators were identified in qualitative research, and one additional factor was identified, being “community capacity”. Barriers and facilitators that were relevant across different types of promotional approaches were: availability of training materials, sufficient funding/resources and partnerships with local government, NGOs and between community-members. Implementer-related factors. In the initial ToC 6 implementer-related factors were identified. For 2 of these, awareness of personal risk and self-efficacy, no barriers and facilitators from qualitative studies were identified. In addition, one new positive driver was identified: motivation. Time constraints seemed to be a barrier that was relevant across different types of promotional approaches. Implementer-related contextual factors. In the initial ToC 26 different contextual factors were identified, in the group of socio-cultural, physical or personal contextual factors. For 15 of these no evidence from qualitative studies was identified: culture, religion, ethnicity, minorities, division of labour, low- versus middle-income countries, safety, age, race, cast, language, education, occupation, physical health and mental health. In addition, one new factor was identified: social-political environment. Contextual factors that were relevant across promotional approaches were: kindness and respect of the implementer, accessibility of the implementer, and the implementer's authority/status. Recipient-related factors. In the initial ToC 6 implementer-related factors were identified. For each factor, barriers and facilitators were identified in qualitative research, and three additional factors were identified: motivation, knowledge and norms. Recipient-related facilitators that were relevant across promotional approaches were: awareness about costs, awareness about benefits, social control, and others showing the behaviour. Barriers across approaches were: having other priorities, time constraints and not being aware of spread of disease. Recipient-related contextual factors. The same 26 contextual factors were also included for the recipients, and for 10 of these no evidence was found in qualitative studies: dignity/respect, religion, information environment, age, race, cast, language, occupation, physical health and mental health. Contextual factors that were relevant across promotional approaches were: age, gender, available space, access to the infrastructure, poverty and social capital (solidarity, cooperation, social connection).
In addition to barriers and facilitators that are relevant across different promotional approaches, we also identified barriers and facilitators that are specifically relevant for one type of promotional approach: Community-based approach. The majority of qualitative studies described a community-based promotional approach (18 out of 28 studies). The following factors were influencing process evaluation factors relevant for community-based approaches: enthusiasm of community leaders, income generating activities at health clubs, and lack of implementer training in participatory development methods. Barriers and facilitators of programme environment factors were: involvement of communities, implementers accountability, responsibility and having a sense of ownership, lack of communication/information from the implementers to the recipients. Within the category of implementer-related contextual factors, the following factors were typically relevant for a community-based approach: the implementer being part of the community and being representative for the community, gender of the implementer (since villagers sometimes want to discuss private items with an implementer of the same sex), being able to trust the implementer, and developing a culture of cooperation. In the category of implementer-related factors, a typical facilitator for community-based approaches was the use of people showing the behaviour in real life as a teachable moment. A recipient-related factor that seemed to be a barrier was that villagers felt undervalued, since they were asked to perform voluntary work as part of the participatory process. The introduction of competition, and identity formation within a health club (e.g. using a club name and slogan) were found to be facilitators. Finally, gender was a recipient-related contextual factor relevant for the implementation of community-based approaches (e.g. men not having time to participate in community-based WASH activities; women not having the same decision-making power). Social marketing approach. Only one study reported on barriers and facilitators to process evaluation factors, specifically influencing the implementation of social marketing approaches. Barriers identified for this approach were mainly about the use of sanitation loans (lack of communication to latrine business owners about which area to cover, sanitation loans not reaching poor people, attitude of the loan officers, interest rate of loans, loan processing times). One qualitative study searched for barriers and facilitators to implementer-related factors. The bureaucratic application process for sanitation loans and costs for a loan were seen as a barrier. Two studies reported on barriers and facilitators related to recipient (contextual) factors. Lack of financial knowledge and poverty were found to be a barrier for the recipients, while additional income/resource generation and durability of the infrastructure were facilitators. Sanitation and hygiene messaging. Three studies reported on barriers and facilitators to process evaluation factors (two at school level, and one at community level with SMS messages). Barriers identified were (SMS) messages that were too long, passive teaching methods in schools, the need for longer intervention periods and frequent reminders with children, overlap of school level intervention with interventions in the community, and lack of interest from the family in case of a school intervention. One study reported on barriers and facilitators to programme environment factors, influencing a sanitation and hygiene messaging approach at school level. The study found that when using this approach, it was difficult to disseminate behaviour from children to parents because it was felt improper for children to teach parents. No barriers or facilitators for implementer-related contextual factors were identified. One study reported on barriers and facilitators to other implementer-related factors, and these concerned lack of involvement of the parents. Three studies reported on barriers and facilitators related to recipient (contextual) factors (two at school level, and one at community level with SMS messages). Time constraints, improper (SMS) messages (not culturally sensitive), poverty of communities, and illiteracy were seen as a barrier, while awareness of disease risk by parents was a facilitator. Elements of psychosocial theory. No barriers or facilitators specifically related to using elements of psychosocial theory were identified. However, two studies using a community-based approach reported the use of emotive factors, such as shame and disgust, as a facilitator for implementation.
6.1.3 Integrated synthesis
In order to make an integrated synthesis of both qualitative and quantitative findings, key summary points from both were integrated within the initial ToC, so the original ToC was refined (Figures 15 and 16). For the majority of pre-defined outcomes and factors, influencing implementation evidence was identified (see Figures 15 and 16).
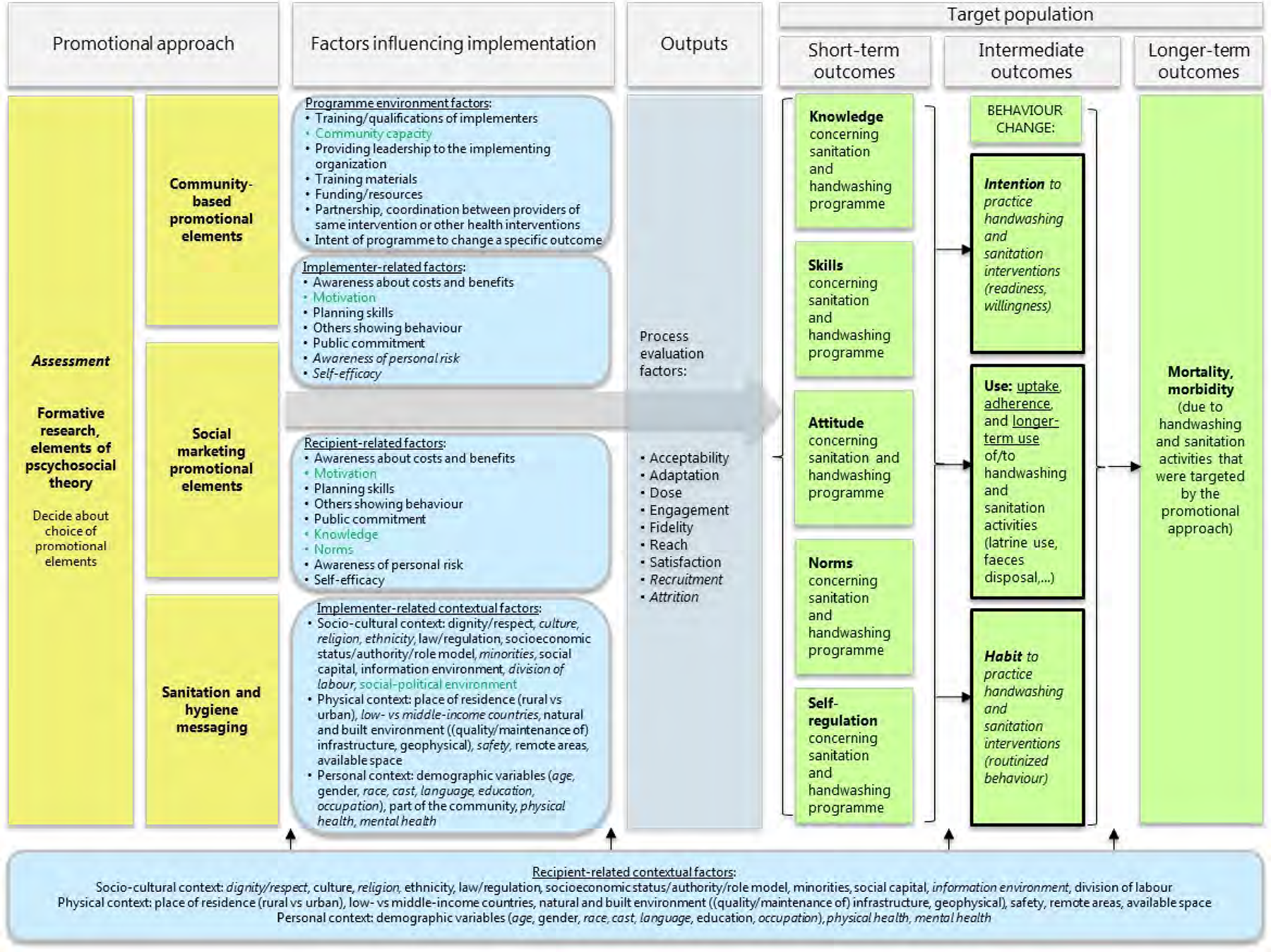
Integrated synthesis: results from quantitative and qualitative findings coupled back to ToC
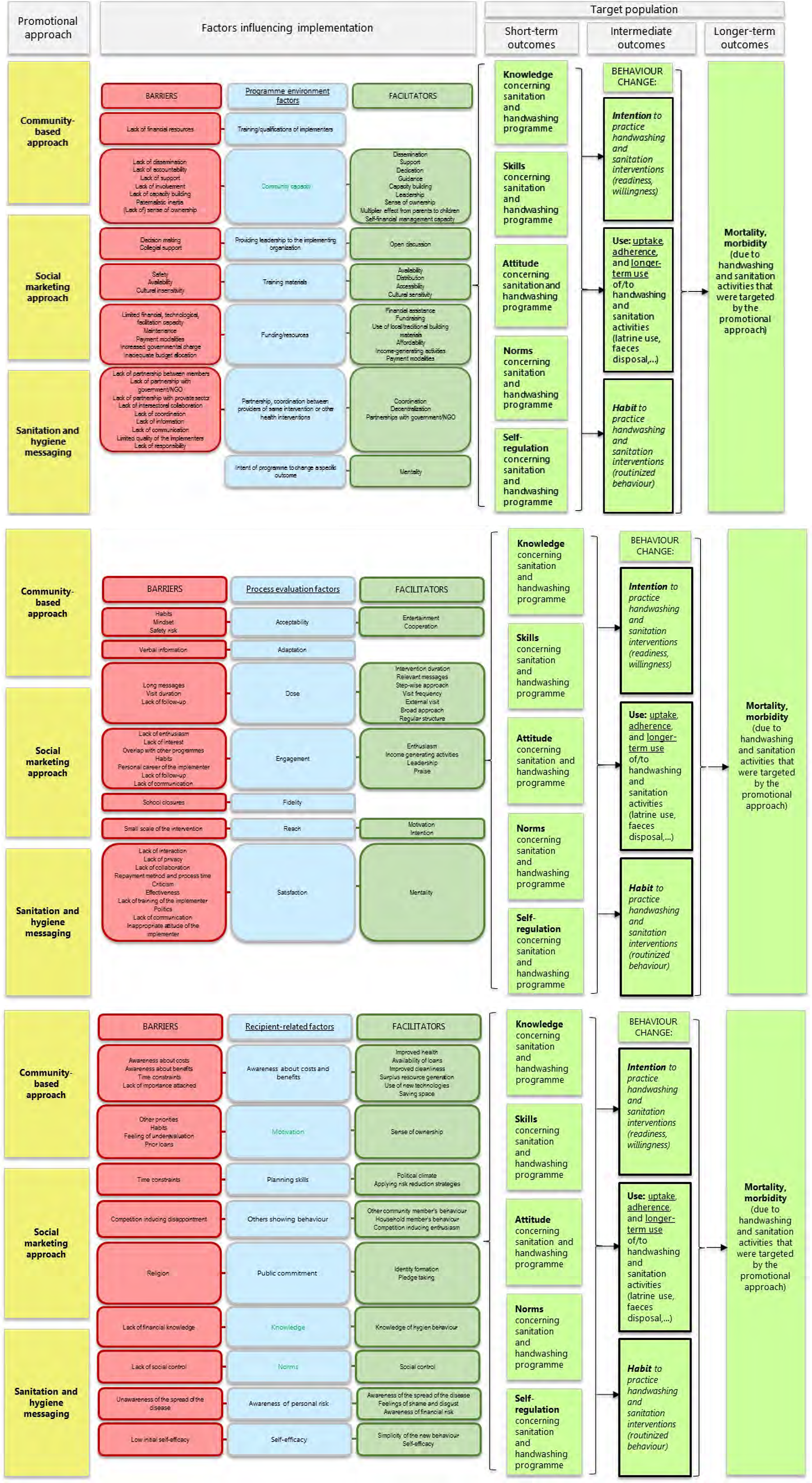
Legend: Green boxes contain short-term, intermediate or longer-term outcomes. Primary outcomes are indicated in boxes with a black border. Blue boxes contain factors that can influence the implementation of the promotional approaches. Factors indicated in green are newly identified compared to the original ToC. Items in italics are not supported with evidence from our systematic review.
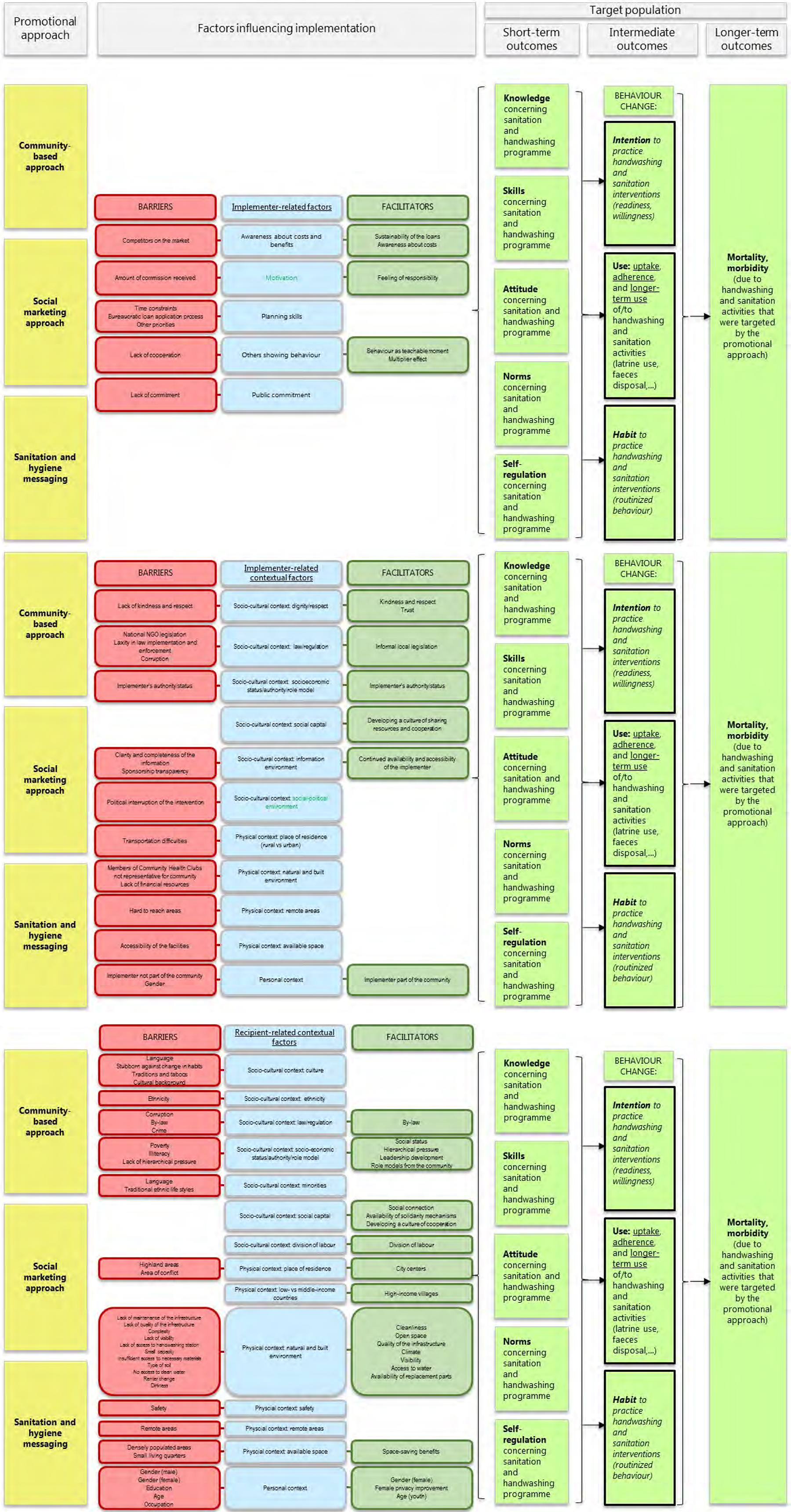
First of all, we describe whether key findings for the different groups of influencing factors were also reported in the quantitative studies. Secondly, we used the qualitative findings as possible explanatory factors for the conclusions we drew from the quantitative findings. Based on input from different stakeholders it seemed relevant to focus on: (1) why social marketing approaches had mixed effects, and (2) why sanitation and hygiene messaging, which is thought to be an ineffective approach for behaviour change because of its directive approach, was found to result in some effect on handwashing in the short term.
First we describe which of the influencing factors identified from qualitative research, were also reported in the quantitative studies:
Second, we used the qualitative findings as possible explanatory factors for the conclusions we drew from the quantitative findings.
It should be noted that these factors (partnerships, attitude of the implementer) were also identified with community-based approaches, and therefore it is not really clear if they can explain the effects of social marketing approaches on behaviour change.
Due to heterogeneity at different levels (WASH component, promotional approach, outcome measures, and timing of outcome measurement), we only performed a limited number of meta-analyses, and few studies per intervention and outcome category were included. As a consequence, no subgroup analyses were made. We also identified a serious number of barriers and facilitators from qualitative studies, and these were not always reported in the quantitative studies. Therefore, we were not able to use these barriers and facilitators in subgroup analyses and to confirm if they indeed influence implementation of handwashing and sanitation promotional approaches.
Based on the available evidence and the input collected during our stakeholder meeting, following changes to our initial ToC were made: Six categories of potential influencing implementation factors are now presented in the ToC, as described above. Since not one promotional approach was shown to be effective, and most probably elements of each approach should be combined in practice, we used “promotional elements” instead of “promotional approaches” in the ToC. We only included the categories of promotional elements that were identified in this review: community-based promotional elements, social marketing promotional elements, sanitation and hygiene messaging, and elements of psychosocial theory. Since elements of psychosocial theory were identified as a consequence of formative research on a small scale, and these elements should be incorporated in broader promotional approaches to scale, we added this type of promotional elements to an “assessment box”, which was introduced before the intervention boxes in the ToC. The assessment period when developing a programme is a preparatory phase in which the problem is identified and a decision about the choice of promotional elements is made. It is now indicated for which elements of the ToC evidence was lacking (italics), and which new influencing factors were identified from qualitative research (green).
6.2.1 Quantitative studies
We identified 42 quantitative studies (46 references) to answer the first review question “What is the effectiveness of different approaches to promote handwashing and sanitation behaviour change in communities in low- and middle-income countries?”.
The studies we identified were performed in LMICs worldwide, with the majority of the studies in South Asia and Sub-Saharan Africa. Most studies (68%) were performed in a rural setting and only 14% of the studies took place in an urban setting (with an additional 12% in an “informal-rural setting”). Since differential behaviour in rural versus urban settings has been noticed (Fiebelkorn et al., 2012), it would have been interesting to have more data from urban settings. No data from emergency settings were identified.
Concerning the intervention, studies were available on the major promotional approaches, including community-based approaches, social marketing approaches, sanitation and hygiene messaging and interventions based on psychosocial theory. However, we pre-specified in our protocol that “incentives” or “advocacy” would also be relevant elements of promotional approaches. Since these elements were most often used in combination with other promotional elements, it was not possible to draw conclusions about the additive value of these elements. In addition, we hypothesised that communication strategies would also be important in obtaining behaviour change; however, only one study specifically compared different communication strategies, by adding elements of interpersonal communication to a mass media approach. Elements of traditional communication (songs, theatre, parades) were sometimes part of one of the approaches in the studies, but the additional effect of these elements was not studied.
Our pre-defined primary outcomes were measured in almost all the studies (n=38, 93%). We defined behaviour change as “use”, “intention” and “habit”, but almost no information about intention and habit was measured (n=2, 5%). For the secondary outcomes, most studies measured knowledge and skills. In order to have a complete view on the hypotheses we made in our theory of change, more information about attitude, norms and self-regulation would be valuable. Health outcomes were measured in some, but not all of the studies.
Overall, the evidence we identified to answer the effectiveness question was relatively complete, i.e. evidence was identified for the majority of the interventions and outcomes that were predefined. Due to the large availability of studies in the WASH sector, we were able to exclude indirect populations (e.g. studies conducted in higher-income countries), indirect interventions (e.g. programmes without a clear promotional approach) or indirect outcomes (e.g. proxy-indicator for latrine use such as latrine construction or latrine hygiene). This means that the current evidence directly answers our review questions. The methodological and conceptual heterogeneity, however, prevent us from generalising our findings to different contexts. In addition, since we were not able to make sub-group analyses, the applicability of the evidence in rural versus urban contexts, middle-income versus low income countries, is difficult to determine. Also, 56% (n=23) of the studies were at small scale, meaning that the evidence is not necessarily applicable on a larger scale (or vice versa). Since no evidence from an emergency setting was found, it will be difficult to apply the evidence identified in such a context.
6.2.2 Qualitative studies
We identified 28 qualitative studies to answer the second review question “What factors influence the implementation of approaches to promote handwashing and sanitation behaviour change, in communities in low- and middle-income countries?”.
These studies were conducted in LMICs worldwide, with the majority of the studies in Sub-Saharan Africa and South Asia, as was the case for the quantitative studies. Again, most studies (68%) were performed in a rural setting and only 11% of the studies took place in an urban setting. In addition, 11% were performed in an “informal-rural setting” (i.e. slums, settlements) and 7% in both a rural and urban area.
Concerning the intervention, studies were available on the major promotional approaches, however the majority of the studies (71%) described a community-based approach. No studies were identified that looked at factors influencing implementation of a specific communication strategy.
The majority of the predefined factors (or barriers/facilitators of these factors), which were part of the initial ToC, were described in the qualitative studies. In addition to the factors that were initially described in the ToC, information on 7 additional factors was retrieved from the qualitative evidence. For 19 factors, including 15 contextual factors, no information was included in our studies. This can partly be explained by our particular focus on factors influencing implementation: process evaluation factors, programme environment factors and implementer- and recipient-related factors. The lack of information from qualitative studies on contextual factors such as religion, age, race, language, occupation and physical/mental health, does not mean that these are not relevant. It simply means that we have not opted for a systematic selection of articles addressing the broader contextual factors, nor for an extensive extraction of such information from the selected articles.
Overall, the evidence we identified to answer the question about implementation was relatively complete, i.e. evidence was identified for the majority of the factors that were predefined.
6.3 QUALITY OF THE EVIDENCE
6.3.1 Quantitative studies
The GRADE approach was used to assess the overall quality of evidence (certainty of evidence) included in this review. In most GRADE assessments, the certainty of evidence was considered as ‘low’ and in some cases ‘moderate’ or ‘very low’. The interventions assessed were complex. Included studies varied greatly – from the intervention studied to the outcomes measured – thus resulting in high levels of inconsistency. The majority of studies were experimental studies, including 22 cluster RCTs, 4 RCTs, and 6quasi-RCTs. No intra-cluster correlations (ICC) were reported in 15 of the cluster RCTs. Risk of bias assessments of included studies were influenced by unclear reporting or lack of reporting of key methodological aspects of the study design and process. Many included studies did not report how allocation sequence was generated. Due to the type of intervention, blinding of the participants (performance bias) and blinding of the outcome assessors (detection bias) were not considered. To assess detection bias, we rather considered whether the outcome was measured subjectively (self-reported) or objectively (direct observation). Most quasi-experimental and observational studies had bias in the selection of participants, some were at high risk of confounding, methods of outcome assessment were not comparable across intervention groups, and outcome assessors were aware of the interventions that the groups received.
6.3.2 Qualitative studies
The qualitative findings mainly explored and created an understanding of the impact of process and implementation factors on the causal chain developed in the ToC. We considered the use of the CerQual approach to assess the overall confidence in the findings from the qualitative evidence synthesis part. However, because it has not fully been tested yet on review projects that attempt to refine a predefined conceptual model, we decided to postpone this exercise to the next update. We are confident that the new guidance currently in development will allow us to include such an assessment in future updates of this review. It follows that in this review project we only assessed the quality of primary research studies currently included in the review.
A quality assessment using the CASP checklist was performed for each qualitative study. The use of qualitative methodology, qualitative research design, recruitment strategy and data collection techniques was considered appropriate in almost all studies. For some studies (n=11) the relationship between researcher and participants was not adequately considered or ethical issues were not explicitly reported (n=10). The data analysis was sufficiently rigorous in 21 studies. An overall CASP score was given to the studies, and only 6 studies had a score less than 8/10. These studies were considered as studies with a lower quality, which were excluded in our sensitivity analysis.
6.4 LIMITATIONS AND POTENTIAL BIASES IN THE REVIEW PROCESS
This review used comprehensive methods to minimise bias during the review process. A clear protocol (with both methodological and stakeholder input) was published. Additionally, a comprehensive search was conducted to identify both published and unpublished studies. Two reviewers worked independently to select studies using the predetermined eligibility criteria, to extract data and to perform risk of bias assessments using a standardised data extraction form.
At the level of study selection, only controlled studies were included in this systematic review. This implies that evaluations conducted by practitioners, which are typically done without control group (e.g. before-after evaluations), were not included in this project. The latter can be seen as a potential limitation from the perpective of the practictioners. However, from a methodological point of view, (quasi-) experimental studies with a control group are the gold standard to address the absolute/relative effectiveness (of promotional approaches). No studies were included describing older approaches such as SARAR or PRA. This could be due to the limitation in publication date (1980) that was applied to the search strategy.
We focused on direct outcomes and excluded indirect outcome measures (e.g. soap use for handwashing, absenteeism for morbidity). Because of a plethora of outcome measures reported in the papers, we decided to exclude behaviour change outcomes besides handwashing, latrine use, safe faeces disposal and open defecation (e.g. latrine maintenance, latrine hygiene, latrine construction, buying of latrines). Included studies assessed these outcomes as self-reported outcomes or via direct observation techniques. Self-reported outcomes are prone to reporting biases, which, as with this type of intervention, could often not be minimized in included studies by using blinding. In our risk of bias assessments of the included studies we considered how outcomes were assessed. There was significant heterogeneity between studies, which made it difficult to perform meta-analyses. In order to make overall conclusions, we classified all the approaches into 4 main categories, however there was still a lot of variation in the combinations of promotional elements. Furthermore, in most cases no formal promotional approach was named or identified in the study itself, so we decided a-posteriori which criteria should be fulfilled to be placed in a certain category (this was done by 4 team members independently, followed by internal discussion and formal agreement during our stakeholder meeting). In addition, because of the complexity of the interventions and outcome measures, we were not able to conduct subgroup analyses, and to draw conclusions about the role of the setting (urban versus rural), or equity factors such as gender, and socioeconomic status.
To enable data analysis across studies, we only used the raw data as reported in the studies, and only for one study we used the adjusted data from the paper since no raw data were available. Since the majority of the studies were experimental or quasi-experimental the issue of confounding factors is not problematic.
Of the 32 experimental studies included, 22 studies were cluster RCTs, which is a type of RCTs where groups of subjects are randomised instead of individuals. This type of design is not surprising for our intervention of interest, and is often used for logistical, feasibility or ethical reasons. However, participants within the same cluster may be more similar than participants from different clusters, possibly leading to correlation of observations within clusters. When this correlation is not accounted for, standard errors of the intervention effect will be too small (Donner & Clar, 2000). For 15 of the22cluster RCTs included in this review, the information to correct for the clustering effect (Intracluster Correlation Coefficient) was not available in the studies, and an ICC was estimated based on information from other studies (see Methods section).
Because of a high degree of heterogeneity we did not draw any conclusions about the effectiveness of using any promotional approach versus no promotional approach, and about the effectiveness of a specific promotional approach, based on the meta-analyses.
The long-term goal of a WASH promotion programme is to reduce morbidity and mortality. In our review, we only included morbidity/mortality data if studies assessed sanitation/handwashing behaviour (i.e. behaviour change outcomes or behavioural factors). Therefore, we need to emphasise that we only included a subset of data about the effectiveness of promotional approaches on morbidity/mortality which may be misleading and might result in incorrect/incomplete conclusions. However, the additional value of this selection criterion is that we could explore the relationship between behaviour and morbidity/mortality.
A final limitation of the quantitative review process concerns the use of process evaluation factors as a descriptive context or to explain differences between findings across the quantitative studies. Many process evaluation factors were not described in all studies (e.g. fidelity, implementer engagement, participation engagement, etc.), but information on recruitment and dose were present in about 80% of the studies. Because of the above-mentioned heterogeneity in the promotional approaches, even within one category of approaches, we decided not to link the findings to information on aspects of implementation such as recruitment and dose.
There are also some limitations for the qualitative analysis. The decision for conducting a deductive type of qualitative synthesis approach (i.e. refining an a-priori theoretical model) rather than an interpretative qualitative synthesis approach was based on the availability of resources in terms of man-power and expertise within the team (dominantly quantitatively oriented). In future updates a sufficient amount of time should be preserved to study all relevant contextual factors impacting on the short, mid- and long term outcome of the promotional programmes and to conduct an interpretive type of synthesis that allows us to configure the findings into new theory. The focus on process and implementation factors should best be elaborated to allow reviewers to provide more details about social-cultural, political, physical and other factors that hinder or facilitate the engagement of our target group.
Although we found evidence (i.e. barriers/facilitators) for most themes in our ToC model, barriers/facilitators of several themes were not identified in the included qualitative studies, e.g. recruitment, attrition, religion, race, physical and mental health. Since we did not actively engage with potential disconfirming cases (i.e. other studies that addressed barriers/facilitators of these themes), we cannot rule out that some of these themes will not apply to the promotion of WASH programmes in nearby future. Future updates of this review may shed some light on the relevance of the factors that were lost in the move from our general ToC to the refined ToC based on the findings of this review.
6.5 AGREEMENTS AND DISAGREEMENTS WITH OTHER STUDIES OR REVIEWS
In the scoping phase of this review, an extensive overview of existing systematic reviews on WASH promotional programmes was performed to be able to focus the research questions of the current systematic review.
Six systematic reviews, that met the criteria set out in the scoping phase, were identified in response to these questions (Fiebelkorn et al., 2012; Mah et al., 2008; Ejemot-Nwadiaro et al., 2015; Evans et al., 2014; Hulland et al., 2015; Joshi & Amadi, 2013). Compared to the current review, in the scoping phase we also included systematic reviews that did not exclusively select studies from LMICs. However, from these reviews we selected those studies that fulfilled our selection criteria. Another important difference is that in the scoping phase we included systematic reviews on all WASH aspects, and not only on sanitation and handwashing.
Two systematic reviews looked at education approaches (Ejemot-Nwadiaro et al., 2015, Joshi & Amadi, 2013). Three studies identified by Ejemot-Nwadiaro (2015) were also included in the current review (Luby et al., 2009; Pickering et al., 2013; Stanton & Clemens, 1985), under the category “sanitation and hygiene messaging”. Other studies in this review were either performed in high-income countries, or did not focus on handwashing or sanitation, or only measured health outcomes, and thus were excluded from the current review. This review concluded that hygiene education resulted in an increase in handwashing at key times in a school and community setting, and a reduction in diarrhoea. For handwashing, these conclusions correspond to the findings of the current review; however, we only found a significant increase in a short term. We were not able to draw conclusions about the effect of these approaches on health outcomes in the current review, since no evidence for these outcomes was identified. None of the studies included in the review by Joshi & Amadi (2013) were incorporated in our systematic review, since either only health outcomes were reported, or the intervention was not a handwashing or sanitation intervention. The review (Joshi & Amadi, 2013) concluded that more research is needed to assess the long-term impact of the interventions.
Two systematic reviews looked at social marketing strategies.
The systematic review by Evans et al. (2014) included two studies that were also incorporated in our review (Pinfold, 1999; Yeager et al., 2002), while the review by Mah et al. (2008) only included the study by Pinfold (1999). This study (Pinfold, 1999) was also categorised under “social marketing approach” in the current review, however the study by Yeager et al. (2002) was classified as “sanitation and hygiene messaging”, since the definition of social marketing used by Evans et al. (2014) was less strict (at least one the 4 P's should have been used). Other studies included in these reviews did not fulfil our selection criteria, and were therefore excluded from the current review. These reviews concluded that results concerning behaviour and behavioural factors were mixed, which corresponds with our findings. The systematic review by Fiebelkorn et al. (2012) included studies with various approaches, but focused on water treatment. One study included in this review (Arnold et al., 2009) was also included in the current review, since here a water treatment and handwashing intervention was implemented. The review concluded that there was first an increase in behaviour, and then a decline, and that differences between urban and rural settings were seen. This latter conclusion could not be verified in our systematic review, since subgroup analyses were not possible due to too much heterogeneity in interventions and outcomes.
A last systematic review was the review by Hulland et al. (2015), looking at factors influencing sustained adoption of WASH technologies. Four studies included in this review were also included in the current review (Bowen et al., 2013; Arnold et al., 2009;Whaley & Webster, 2011;Waterkeyn & Cairncross, 2005). The majority of the other studies did not study a specific promotional approach or did not fulfil our study type selection criteria. The review concluded that influential programme factors associated with sustained adoption include frequent, personal contact with a health promoter over a period of time. This corresponds with our current findings, since we also concluded that interpersonal communication is a relevant aspect.
Meta-analyses were not performed in any of the above mentioned systematic reviews. Similarly, in the current systematic review, due to the heterogeneity in population, programme content, study types, type of intervention, and outcome measurement, it was difficult to perform meta-analyses.
7 Authors’ conclusions
7.1 IMPLICATIONS FOR PRACTICE AND POLICY
Stakeholder engagement occurred throughout this project. Our stakeholders contributed in formulating implications for practice and policy, and a stakeholder specific dissemination strategy was discussed.
Promotional approaches targeting handwashing and sanitation behaviour are complex programmes based on several promotional elements, and adapted to the context of the environment where they are implemented. This could be confirmed in the studies included in this review. From the quantitative findings we conclude that there is not one promotional approach that is more effective than another. In other words, one size does not fit all.
However, several effective elements of behaviour promotion could be identified, including:
Concerning the use of incentives as part of the promotional approach, it is difficult to generalize findings, since we only found a limited number of studies that used a wide range of incentives (from soap bars, to food over subsidies). One study reported promising results when using subsidies as part of the community-based approach, but more research on the use of subsidies and incentives would be valuable. It should be noted that evidence concerning the use of elements derived from psychosocial theory was only found in small-scale studies implementing a handwashing programme, nevertheless such promotional elements could be added to a broader programme. Determining which theory-based elements are relevant in a certain context should be part of an assessment/pilot phase. Therefore, a more in-depth formative research during the assessment phase, leading to the right selection of promotional elements, seems to be a critical step for programmes aiming at behaviour change for sanitation and handwashing.
A combination of approaches, including several promotional elements as described above, is likely to be the most effective strategy. This is currently acknowledged as best practice in the WASH sector, as we learned from our Advisory Group and different stakeholders (practitioners, policy makers).
In addition to the characteristics of a certain promotional approach, a wide variety of influencing factors should be taken into account during implementation. Based on our findings from qualitative studies, key barriers and facilitators need to be well understood when planning an intervention and selecting the right combination of promotional approaches. Those barriers and facilitators are related to: the programme environment (e.g. funding, partnership, coordination, etc.) the implementation process (“process evaluation factors”) (e.g. acceptability, dose, reach, fidelity, etc.) implementer-related (contextual) factors (e.g. leadership, attitude, gender, etc.) recipient-related (contextual) factors (e.g. motivation, others showing behaviour, culture, education etc.)
Key barriers and facilitators for each of the four sections above were identified in this review, and revealed equally critical in terms of selecting successful promotional approaches. These influencing factors are likely to explain the success or failure of a promotional programme and are a real added value for practitioners.
For
In the case of
In case of
A prior assessment of the context and situation, by doing formative research, will provide more information on which influencing factors to take into account and which elements could be included in the promotional strategy.
An important implication for the future is that there is an urgent need to use a more uniform method of outcome measurement (type of outcomes, way of assessment, timing of assessment). This will facilitate making conclusions on the effects of promotional approaches in the future (see also 7.2). In addition, it is important to further test barriers and facilitators, identified in this review, alongside quantitative analyses of promotional approaches.
7.2 IMPLICATIONS FOR RESEARCH
Based on the review of the 41 quantitative studies we included, we can formulate some specificre commendations for future research.
Firstly, the analysis of the 41 quantitative studies resulted in the identification of the gaps in evidence that answers our primary review question. On the population level, only few studies were available from the Latin America and Caribbean region, and from French-speaking African countries. In addition, most studies were performed in a rural setting, and it would also be valuable to have evidence on the effect of handwashing and sanitation promotional approaches in urban settings. No studies were performed in a disaster setting, and more research in this specific context is warranted. Concerning interventions more research is needed on the effect of marketing approaches and the use of elements derived from psychosocial theory. From consultation with our stakeholders, we learned that the addition of incentives to existing approaches such as CLTS is currently being questioned, however we only found a limited number of studies that incorporated incentives into the promotional approach. One study reported promising results, but more research on the use of subsidies and incentives would be valuable. In addition, since we hypothesised that communication strategies would also play a role in the effect of promotional approaches, and we only identified one study that compared different communication strategies, more research on this subject is needed. On the outcome level, more outcome measurement in the longer term is needed, especially for the marketing approaches, in order to be able to draw conclusions about programme sustainability.
A second recommendation for researchers is based on how the outcomes were measured across the included studies. We established that there was a large variability in the way outcomes were measured across studies, using different assessment methods (e.g. self-reported versus observation methods), outcome measures (dichotomous, continuous, different outcome types) and different timings of measurement. This makes it very difficult to compare and synthesize outcomes across studies (e.g. in the format of a meta-analysis), and therefore there is an urgent need for research to use a more uniform method of outcome measurement (type of outcomes, way of assessment, timing of assessment). In addition to outcome assessment, outcome reporting is also important, e.g. good reporting practices for experimental studies are described in the CONSORT checklist.
A third recommendation for future research concerns the ability to identify effective promotional elements that could be part of a promotional approach. Because of the heterogeneity and complexity of the promotional approaches used in practice it is difficult to come to a conclusion about successful elements that could be part of the approach. Studies adding a specific element to an existing approach, such as some of the studies described in paragraph 4.3.2, could be an interesting way to approach this. Our systematic review could be a source of promising elements to be further investigated in future studies. In addition, the approaches that were shown to be promising from this review should be tested to see if they are replicable and viable at larger scale.
Fourthly, since the scope of our systematic review was limited to handwashing and sanitation promotional approaches, we would like to make some suggestions for future systematic reviews. To be able to draw conclusions for all the different aspects of WASH interventions, information is needed about 1) the effect of water treatment and water supply programmes, 2) the effect of sanitation programmes on other outcomes such as latrine construction, latrine hygiene and latrine maintenance, and 3) the effect of programmes that aim to improve hygiene in a broader way than handwashing alone (e.g. menstrual hygiene).
A final suggestion for quantitative studies concerns cost-effectiveness. In addition to evidence on the effectiveness of WASH promotional programmes, evidence on cost-effectiveness is an aspect of major importance. It is already known that hygiene promotion is a cost-effective strategy in LMIC (> 10 USD per DALY averted) (Laxminaryan et al., 2006), however not much information is available on how this measure was determined and whether it includes health effects in the longer term. In order to achieve more sustainable effects with WASH programmes, more complex programmes (such as the promotional approaches described in the studies included in this review) have been developed, but it is not known if these are still cost-effective. Therefore, more primary research (and a systematic review in a second phase) on this subject is warranted.
The qualitative studies included in this review identified many factors that may influence the successful implementation of a certain promotional approach. This information can be used and further tested in future quantitative research. The heterogeneity of barriers and facilitators to implementation, highlights the importance of conducting qualitative process evaluations alongside trials in order to understand the dynamics of programme implementation. In addition, quantitative researchers should be encouraged to measure and report factors concerning process evaluation and implementation. Programme developers of WASH promotion programmes may also benefit from the qualitative study results by adopting of or anticipating on specific barriers/facilitators when developing their programme. Moreover, the identification of these implementation factors will guide researchers in which circumstances their programme may work (or not) and which barriers/facilitators they probably will need to tackle. Finally, researchers in the domain of WASH promotion programmes can translate the information from the implementation factors to the specific context where the research will be conducted.
During this project active stakeholder engagement was part of the process and it was a real added value that researchers, practitioners, policy makers and donors were brought together at several moments. Therefore, we recommend stakeholder involvement both for the conduct of primary research (quantitative and qualitative studies), and the development of systematic reviews. In the context of this systematic review, stakeholders had an added value in: refining and approval of definitions (promotional approaches), fine-tuning the research questions and selection criteria, improving the ToC (increasing relevance to practitioners and policy makers), identifying relevant sources of grey literature, discussing about applicability of findings, formulating implications for practice, and thinking about dissemination and communication.