
Abstract
We examined the effect that long-handled shoehorn (LHSH) length and body mass index (BMI) have on hip range of motion (ROM) in female adults. Thirty-eight female participants were asked to don a shoe using 18-, 24-, and 30-in. LHSHs. Significant differences in hip flexion were found between the 18- and the 24-in. shoehorns and between the 18- and the 30-in. shoehorns. A significant positive relationship was found between BMI and internal rotation for each of the LHSHs. The results suggest that healthy women with low BMIs using a 24- or 30-in. LHSH have the greatest chance of not violating hip flexion or hip internal rotation ROM precautions. Implications suggest that therapists consider individual BMI and available hip ROM before prescribing an LHSH. A follow-up study is needed involving populations who would likely benefit from using LHSHs.
According to the Agency for Healthcare Research and Quality (AHRQ; 2010a), 306,525 people were admitted to the hospital for hip fractures in 2007. Almost 90% of hip fractures occurred in people > age 65, and 70% of admissions were women (AHRQ, 2010a). One-third of the cases resulted in hip replacement surgery (AHRQ, 2010b). In addition, people with degenerative diseases, such as arthritis of the hip joint, sometimes choose to have hip replacement surgery to decrease pain. Whether hip replacement surgery is used to correct a hip fracture or to mediate pain because of degenerative processes, the intended outcome of surgery is to increase functional mobility and independence in completing activities of daily living (ADLs).
For recovery to go as smoothly as possible, patients must follow standard hip precautions after surgery to reduce the chance of hip dislocation (Rapuri, Klein, & Hozack, 2004). It has been reported that hip dislocations are a complication in approximately 0.5% to 4% of all total hip arthroplasty procedures (Smith, Berend, Lombardi, Emerson, & Mallory, 2005). Dislocation often destroys part of the hip prosthesis, which then requires surgical repair and continued postdislocation care, including rehabilitation (Callaghan & O’Rourke, 2004; Masaoka et al., 2006; Sanchez-Sotelo, Haidukewych, & Boberg, 2006). Although patient factors associated with dislocations include gender, age, level of cognition, and neurological impairment, flexing or rotating the hip beyond the recommended range of motion (ROM) has been indicated in unstable total hip arthroplasties (Smith et al., 2005). Although no documentation in the literature has been found regarding total hip arthroplasty dislocations because of shoe donning without the use of a long-handled shoehorn (LHSH), it follows that using an LHSH would decrease the likelihood of breaching the hip ROM precautions.
Adherence to hip precautions is especially critical during the first 3 mo after surgery to reduce the chance of dislocation (Seeger & Fisher, 1982). The most common type of hip replacement is completed by accessing the hip by means of a posterior approach (ActiveJoints, 2008). Generally accepted hip precautions for the posterior approach are as follows: no hip flexion beyond 90°, no hip internal rotation, no crossing the legs, and no adduction at the hip (Bear-Lehman, 2002). Some patients may also have restrictions on weight bearing (Goldstein, 1999).
The goal of the rehabilitation team when working with patients with hip replacement is to increase the person’s functioning as quickly as possible (Access Medicine, 2007). The role of the occupational therapist involves determining the need for equipment to facilitate independence in ADL performance. If equipment is needed, the occupational therapist is responsible for providing the necessary training to the patient, as appropriate, and to the patient’s caregiver (Moffa-Trotter & Anemaet, 1996; Sandell, 2008). The typical delivery of required equipment (e.g., LHSH, sock aid, tub or shower bench, and raised toilet seat) generally occurs a few days before discharge of the patient, with the possibility that the education could occur either pre- or postoperatively. The reasoning for this timing is to allow time for the patient to practice with the devices under the supervision of the occupational therapist before the patient’s hospital discharge (Daniel & Strickland, 1992, Lawson, 2005; Maher & Bear-Lehman, 2008; Poole, 2009; Sandell, 2008).
Correct use of assistive devices enables increased independence in ADLs. Common assistive devices used by post–hip replacement patients include reachers, long-handled sponges, LHSHs, and sock aids. Collectively, these items are often referred to as “hip kits” in home health magazines and medical supply stores. Proper use of these devices may help patients increase their independence at home and achieve rehabilitation goals (Bear-Lehman, 2002; Schemm & Gitlin, 1998).
As suggested by Occupational Therapy Protocol Management in Adult Physical Dysfunction (Daniel & Strickland, 1992), the treatment technique for donning a shoe for patients who recently have had hip arthroscopy is having the patient use an LHSH. Specifically in this population, shoehorn usage is encouraged so patients do not need to flex their hips past 90°.
Depending on hospital procedures, patients may be given the assistive device at the facility or buy it on their own from a magazine or medical supply store or online. Schemm and Gitlin (1998) reported that 64 of 86 patients with cerebrovascular accident, orthopedic deficit, or lower limb amputation received a shoehorn before discharge. In addition, Neville-Smith, Trujillo, and Ammundson (2000) performed a survey that investigated the consistency of postoperative education after total hip replacement among rehabilitation facilities throughout the United States. Of the 35 surveys mailed to rehabilitation facilities, 19 were returned, for a response rate of 54%. Among the questions on the survey was the frequency at which various pieces of assistive devices were issued or recommended to patients. LHSHs were grouped with stocking aids; that is, both devices were included in the same question and were therefore not queried separately. Seventy-nine percent of the respondents indicated that these items were “always” recommended, whereas 21% of the respondents indicated these items were “sometimes” recommended.
Similarly, Davidson (1999) surveyed 74 postoperative patients who underwent a total hip replacement regarding the provision and use of equipment issued to each patient. The surveys were sent out to patients discharged from the Perth and Kinroth areas of the United Kingdom. Data were calculated from 63 respondents, for a response rate of 85%. Of particular interest, 86% of the respondents were issued LHSHs, and most of those respondents (87%) indicated that the LHSHs were useful. In addition, slightly more than half of the respondents (51%) indicated that at 6 mo after surgery, they were still using the device.
Although the literature suggests that LHSHs are typically recommended to patients with total hip replacements, many LHSH lengths are available. One retailer offers four different lengths of shoehorns: 12 in., 18 in., 24 in., and 30 in. (Sammons Preston, 2007). We were not successful in locating a protocol for determining which type or size of LHSHs to issue. This finding raises the question of how to choose the appropriate shoehorn for patients.
The use of anthropometric principles may help health care professionals make recommendations about the assistive devices people should receive (Baker, 1999; Fairley, 2006). Anthropometry involves the measurement of the human body and is used to design objects and environments used by humans (Baker, 1999). Through anthropometrics, a designer can ascertain the most efficient way to design an environment or object to fit most of the population (Baker, 1999). It has been suggested that anthropometric techniques can play a significant role in the design of industrial workspace, ergonomic tools, and assistive devices (Baker, 1999; Fairley, 2006). Occupational therapists have used anthropometry to evaluate the effectiveness of ergonomic design on hand tools to reduce wrist ROM (Tebben & Thomas, 2004), the impact of wrist orthoses on wrist ROM while performing stacking and pouring tasks (King, Thomas, & Rice, 2003), and the effects of computer keyboard design on hand and wrist ROM (Baker & Cidboy, 2006).
Body mass index (BMI) is a calculated measure (i.e., weight in kilograms divided by height in meters squared, or kg/m2) that is important to consider when designing human working environments and investigating human movement. A study by Gilleard and Smith (2007) found that hip ROM increased in people with higher BMIs compared with participants with normal BMIs when engaged in a simulated work task. These authors concluded that because participants were engaged in a work task, they were forced to interact with other objects and their environment. The contributing factors of body size and interaction with the environment forced participants with higher BMIs to use internal compensation methods (e.g., more ROM at the hip) to complete a task. The same concept may also be true when people don shoes with LHSHs.
Few studies have been completed in the area of assistive device fitting and anthropometric techniques, although the idea of merging the two concepts has been suggested in the literature (Baker, 1999; Fairley, 2006). Studies that have examined assistive devices often examine the device in relation to specific biomechanical aspects of human movement. Kumar, Roe, & Scremin (1995) examined methods of estimating proper cane length by applying anthropometric principles and found that improperly fitted canes can lead to poor body mechanics; increased demand on the triceps; and an increased moment arm at the elbow, which increases the amount muscles must work. The study also revealed an improved way of fitting a cane (Kumar et al., 1995). Sevey and Rice (2002) found that a bent long-handled sponge in typical populations may help people with ROM limitations in the shoulder and wrist, whereas people with elbow limitations may benefit more with a straight long-handled sponge.
Because most assistive devices are mass produced, Sevey and Rice (2002) suggested that an important feature of many devices should be their adjustability. A product search of several medical supply companies did not reveal any adjustable shoehorns available on the market. The use of static anthropometry techniques may provide a way for health care professionals to determine what length LHSH to provide or to recommend to their patients. Static anthropometry is “the science of measuring length, breadth, and width of the human population” (Baker, 1999, p. 51). These measurements and principles may also provide valuable information for design of assistive devices on the basis of individual body size.
The purpose of this study was to examine the influence of three different lengths of LHSH—specifically, 18, 24, and 30 in.—on hip ROM (i.e., flexion and internal rotation) in a healthy adult female population. Because this particular assistive device is frequently recommended, research is needed to determine whether there is a difference in the degrees of hip ROM when using different lengths of shoehorns. We hypothesized that there would be less hip flexion and hip internal rotation when study participants used the longer LHSHs when donning a shoe. We also hypothesized that there would be a positive relationship between BMI and hip ROM when using LHSHs to don a shoe.
Method
Participants
A convenience sample of 40 female volunteers was recruited by recruitment flyers at colleges in the midwestern United States (mean age = 26 yr, standard deviation [SD] = 6.9, range = 21–47). Participants self-reported that at the time of the study, they were experiencing no orthopedic or neurological health problems that may have adversely affected their ability to participate. Two participants were African-American, and 36 participants were White. All but 2 participants stated that they were right handed.
Apparatus
Three stainless-steel LHSHs measuring 18, 24, and 30 in. long were purchased (item nos. 2061, 2064, and 2062, respectively; Sammons Preston, Bolingbrook, IL). Nontying, black canvas shoes in sizes 6 through 12 were also purchased (Walmart White Stag brand, item no. 2572575, Little Rock, AR). Data were gathered using a four-camera Qualisys three-dimensional kinematic system with Qualisys Track Manager software, Version 1.10.282 (Qualisys, Gothenburg, Sweden), which collected data through reflective markers placed on the body. Movement data were collected at 240 Hz. The three-dimensional system was connected to a Pentium IV desktop computer running Windows 2000 operating system software.
Procedure
This study was approved by the biomedical institutional review board at the University of Toledo. Informed consent was obtained from each participant before participation in the study. The study used a counterbalanced, repeated-measures design, in which participants served as their own control and were randomly assigned to one of three order groups. The groups all donned a right-foot canvas slip-on shoe 3 times with the aid of an LHSH in one of the following orders: 18–24–30 in., 24–30–18 in., or 30–18–24 in. To ensure similarity among participants, the canvas slip-on shoes were purchased in a variety of sizes before the study. Data were collected from the time participants picked up the LHSH from the start–stop area to the time they replaced the LHSH in the start–stop area. Data collection for each participant was completed in 1 day, took approximately 20 min, and occurred in a research laboratory setting where privacy and anonymity of data collection was protected by assigning identification numbers to all data.
Using anthropometric principles, the investigator measured and recorded the height, sitting height, weight, and waist circumference of each participant. BMI was also calculated. Participants were asked to sit comfortably in a straight-backed chair. They were then asked to remove their right shoe. A canvas shoe was placed for them just lateral to their right foot. They were instructed to place their feet flat on the floor so that their knees were flexed at a 90° angle. Platforms on which to rest the feet were available to accommodate participants’ varying heights. Participants were asked to sit with their back straight, so that a 90° angle was made at the hips. The following instructions were given:
One practice session will be provided for each type of device.
Pick up the long-handled shoehorn and use it to put the right-foot canvas shoe on your right foot. Once your foot is flat in the shoe, please wait until I tell you before you take the shoe off.
Go ahead and practice it once.
Okay, great.
Now do the same thing when I say, “Go.”
After the participant successfully placed her right foot in the shoe with the first length of shoehorn she was assigned, she took off the canvas shoe. The investigator then supplied the participant with the second length of shoehorn, and the process was repeated. After completion of the task with the second length of shoehorn, the same process occurred with the third length of shoehorn.
Reflective markers were placed on the right lower extremity at the lateral epicondyle of the femur, the greater trochanter, and the distal anterior border of the tibia. Markers placed on the upper extremity were placed at the head and lateral epicondyle of the humerus. Successfully donning the canvas shoe was determined when the sensor placed inside the bottom of the shoe was depressed by the heel. Depression of the sensor signaled the data collection computer by means of an analog-to-digital board marking the time at which the heel made contact with the sensor.
Data Reduction and Statistical Analyses
The hip ROM was analyzed for each participant. Movement data were smoothed using a second-degree curve using a 25-frame window (data smoothing is a method used to reduce error in motion data; Winter, 1990). Hip flexion was calculated from the markers placed on the head of the humerus, the greater trochanter of the femur, and the lateral epicondyle of the femur. Data from the markers were analyzed to determine the most acute angle made for each trial. Hip internal rotation was calculated by performing trigonometric calculations with the data collected from the marker placed on the distal anterior border of the tibia and the lateral epicondyle of the femur. The angle made from the starting point of the distal anterior border marker (i.e., the lateral epicondyle of the femur) to the maximum height of the distal anterior border marker made in the same plane was determined for each sampling of each trial using custom software written in Microsoft’s Visual Basic development software (Version 6.0). This custom software program automated the data reduction process. Figures 1 and 2 illustrate the marker placement and the flexion and rotation angles, respectively.
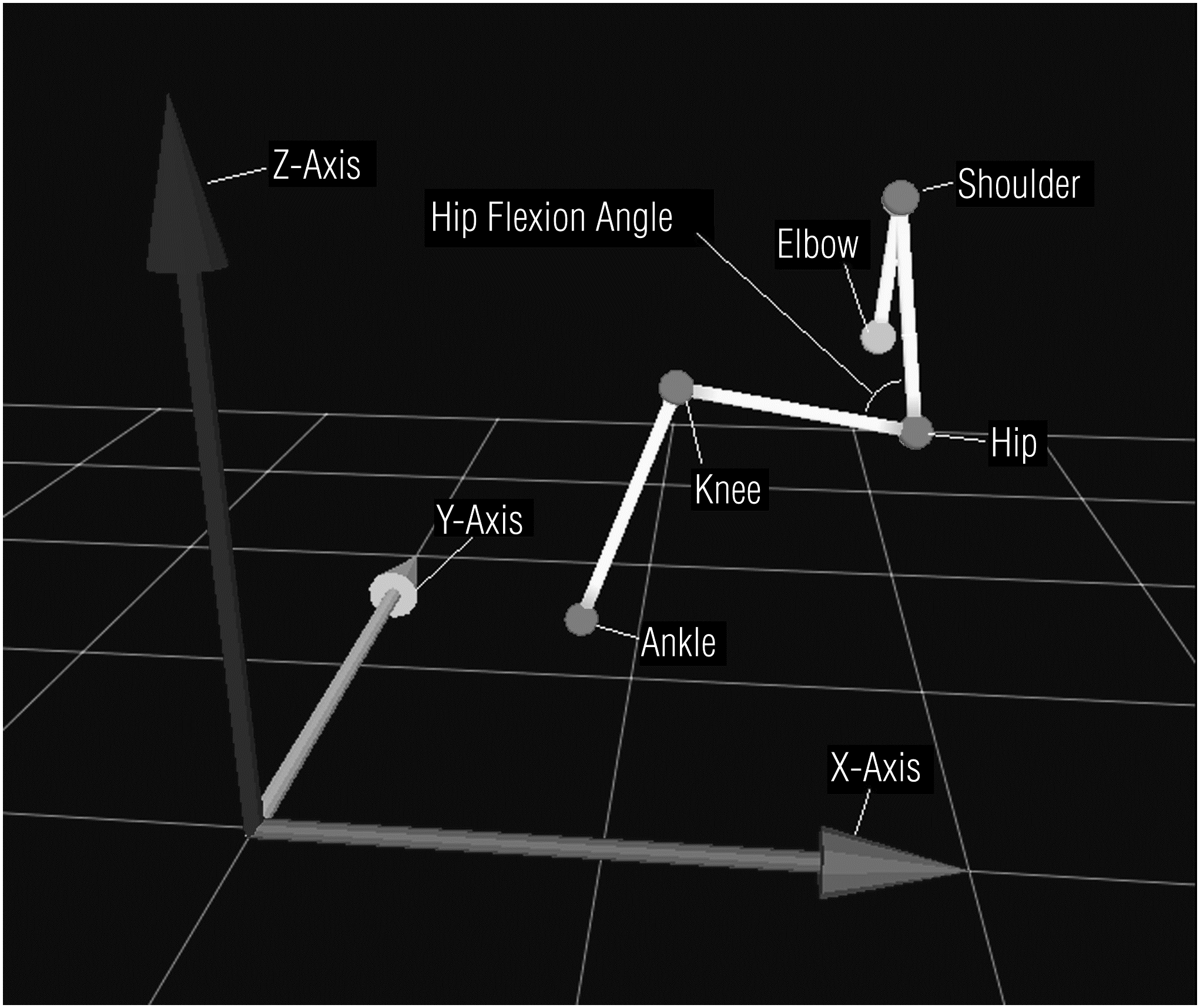
Schematic of markers and axes of orientation for hip flexion.
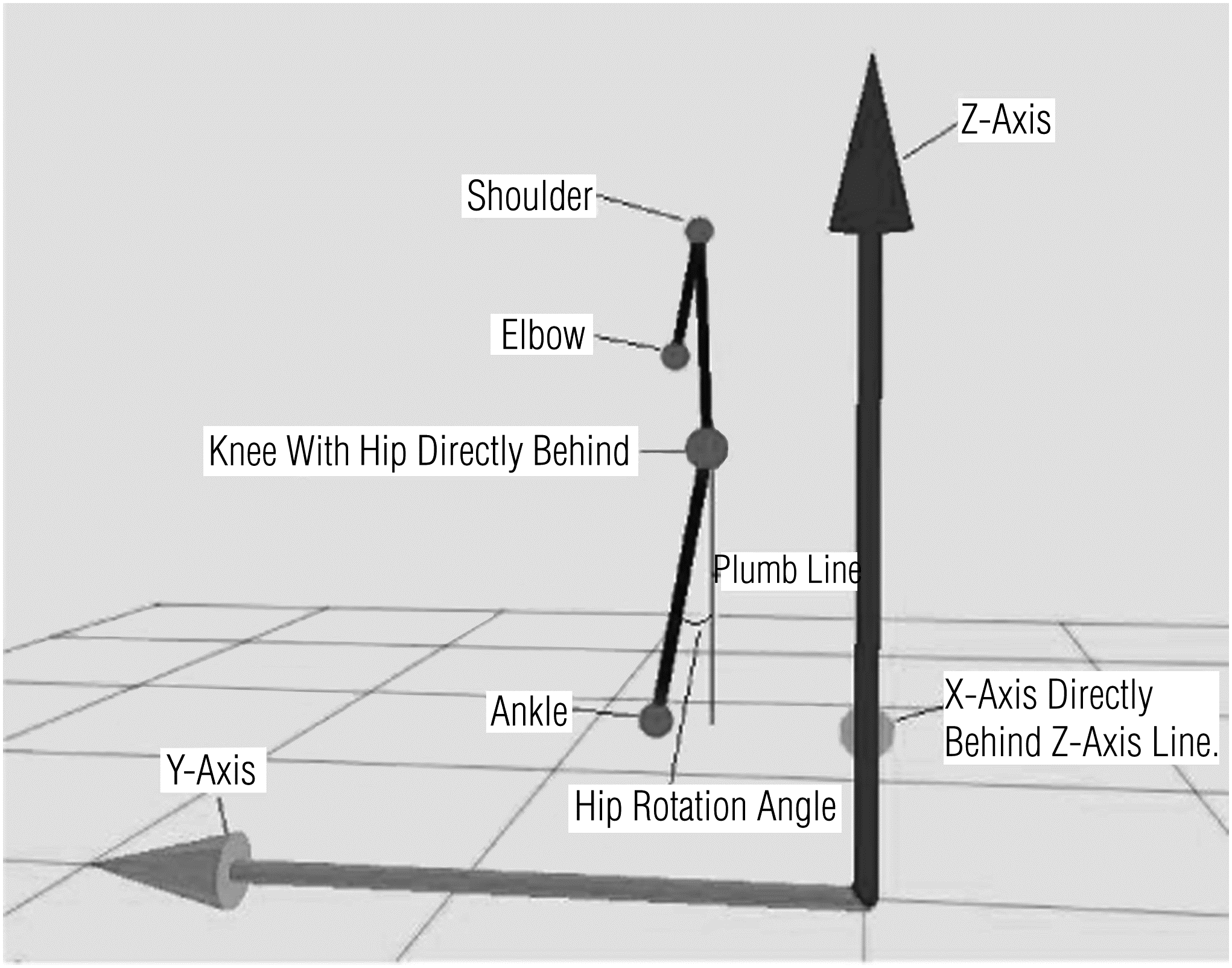
Schematic of markers and axes of orientation for hip rotation.
For the first hypothesis, repeated-measures contrasts were used to test whether length of shoehorn influenced hip flexion and rotation. For the second hypothesis, linear regression was used to test whether there was a relationship between BMI and the amount of hip flexion and rotation. SPSS statistical software Version 17.01 (SPSS Inc., Chicago) was used for all statistical analyses.
Results
Because of investigator error and technical difficulties, data from 2 participants were discarded. Therefore, 38 participants were included in the data analyses. All participants were able to successfully don the right shoe in each of the three conditions. All participants were required to complete the donning task with their right hand. Mean waist measurement, height, and sitting height are presented in Table 1. Mean weight was 158.0 lb (SD ± 37.6 lb). Mean BMI was 25.7 (SD ± 6.3). The mean ROM for hip flexion and hip internal rotation for all three conditions are displayed in Table 2.
Mean and Standard Deviation (SD) of Waist, Standing Height, and Sitting Height Measurements
Mean and Standard Deviation (SD) of Hip Flexion and Hip Internal Rotation for Each of the Long-Handled Shoehorns
The first hypothesis was partially supported in that the within-subjects repeated-measures contrasts revealed a significant difference in hip flexion performance between the 18- and the 24-in. LHSH (F[1, 37] = 16.11, p < .000) and between the 18- and the 30-in. LHSH (F[1, 37] = 16.96, p < .000) but not between the 24- and the 30-in. LHSH (F[1, 37] = 0.18, p = .678). For hip rotation, the within-subjects repeated-measures contrasts revealed no significant difference between any of the LHSH lengths, specifically, the 18- and the 24-in. LHSH comparison (F[1, 37] = 0.34, p = .567), the 24- and 30-in. comparison (F[1, 37] = 0.15, p = .699) and, finally, the 18- and 30-in. LHSH comparison (F[1, 37] = 0.53, p = .471).
Likewise, the second hypothesis was partially supported in that the linear regression analyses testing the relationship between BMI and hip flexion for each LHSH length were not statistically significant; however, the relationship between BMI and hip rotation for all three LHSH lengths was statistically significant. Specifically, for hip flexion, the result for the 18-in. length was F(1, 37) = 2.77, p = .105; for the 24-in. length, F(1, 37) = 1.00, p = .324; and for the 30-in. length, F(1, 37) = 0.19, p = .664. For hip rotation, the result for the 18-in. length was F(1, 37) = 9.03, p = .005; for the 24-in. length, F(1, 37) = 4.90, p = .033; and for the 30-in. length, F(1, 37) = 9.39, p = .04. Figure 3 is a scatterplot of hip rotation and BMI for each of the three LHSHs illustrating the positive relationship between the two factors.
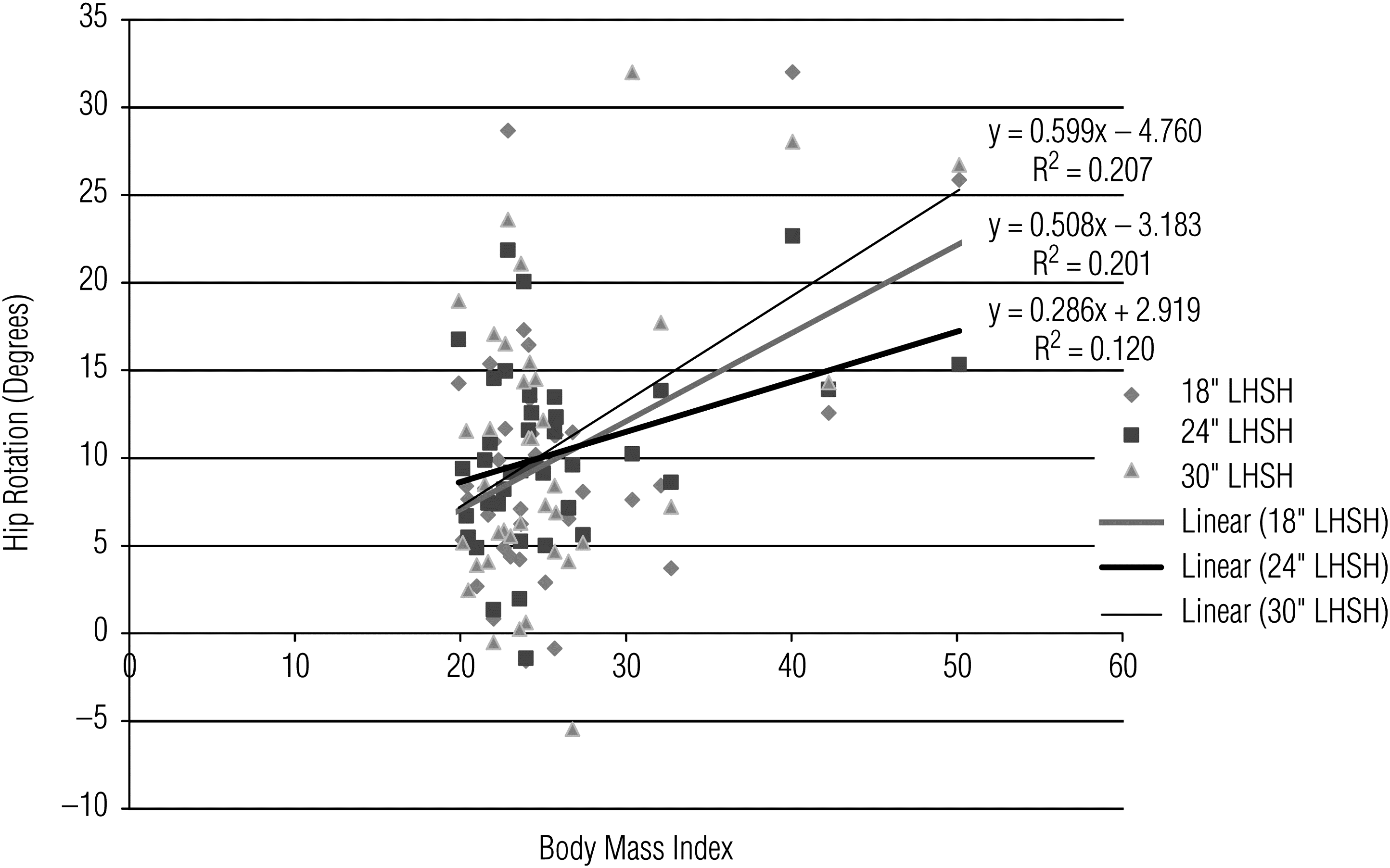
Scatter plot of body mass index (BMI) and hip rotation with trend lines for 18-in., 24-in., and 30-in. shoehorns.
Discussion
The results of this study partially supported the hypothesis that the length of LHSHs elicited differences in hip ROM while donning a shoe. Specifically, when using 30-in. LHSHs, participants tended to use less active hip flexion than when using the 18-in. LHSH; however, this difference was not exhibited for hip rotation. The results of this study also partially supported the second hypothesis in that no statistically significant relationship was found between hip flexion and BMI for participants using any of the three LHSHs. However, a significant positive relationship was found for hip rotation and BMI for each of the three LHSHs.
One interesting result is that we found statistically significant differences in hip flexion but not in hip rotation among the three LHSH lengths. Comparatively, no relationship was found between BMI and hip flexion, but a relationship was found between BMI and hip rotation. The findings speak largely to the strategy that participants used when donning the shoe using the various LHSHs. Participants tended to flex their hip joint more when using the smaller shoehorns. Although no significant difference was found between hip flexion with the 24- and 30-in. LHSHs, the trend was for more hip flexion with the 24-in. than with the 30-in. shoehorn (i.e., as the length of the shoehorn increases, the elicited hip flexion decreases). As a result, it is possible that a Type 2 error occurred in the comparison between the 24-in. and the 30-in. shoehorns for hip flexion. This trend was not seen with hip rotation across the three LHSHs (i.e., there was <1° difference of internal hip rotation between the three LHSHs). This finding suggests that two separate strategies were used when moving the hip joint while donning the shoe.
Regardless of BMI, hip flexion tended to increase as the length of the shoehorn decreased. BMI, however, did appear to influence hip internal rotation ROM. As BMI increased, there tended to be a greater elicitation of internal rotation. Of the three regression lines, the steepest slope is associated with the 30-in. shoehorn.
Another observation regarding the BMI–hip rotation relationship is that there appears to be a clumping of data between BMI scores of 20 and 30. Participants with a BMI ≤35 appeared to use a strategy that involved internal or external hip rotation. It appears that the strategy for using hip rotation was more prescribed for participants with BMI >35, who without exception elicited internal hip rotation >12°. The reason may be a matter of biomechanics. People with a large BMI tend to have more mass about their midriff. For someone with a larger BMI to see his or her feet when the knees are flexed at 90°, he or she may need to internally rotate the hip to move the foot into a position where the person can gain a line of sight to the foot. In particular, the back of the shoe and the back of the foot need to be seen. With a large midriff, flexing at the hip may not enable a view of the back of the foot and shoe. Therefore, a more successful strategy for this group may involve internally rotating at the hip, which appears to be the strategy adopted by this subgroup of participants in the study.
The relationship among BMI, hip flexion, and internal rotation found in this study contrasts with findings in other studies on BMI and ROM. Other studies have indicated that a higher BMI is significantly related to less ROM at elbow, trunk, hip, and knee joints than in healthy control participants when simply measuring joint ROM (Brown, 2008; Kotani, Yonekura, & Bourne, 2005). In the current study, however, participants with higher BMIs exhibited more movement at the hip to complete the donning task than did participants with lower BMIs.
Although BMI can be used as a factor in determining which length of shoehorn to prescribe, clinical reasoning should be based on more than just BMI when deciding the appropriate-length LHSH a patient should receive. It has been suggested that BMI is not an appropriate predictor of health or fitness because a high BMI may be the result of being very muscular (Gallagher et al., 1996). It is likely that someone who is very fit and muscular would have no problem seeing around his or her body to don a shoe or compensating in some other manner. Therapists can consider BMI when deciding on an LHSH length; however, the available ROM at other joints in the body should also be considered. Generally, the 30-in. shoehorn would be expected to elicit less hip flexion, regardless of the person’s BMI. However, people with BMI >30 or so should be highly cautioned in that they may have a predisposition to internally rotate their hip as their only strategy for performing ADLs involving the heel of the foot.
In light of the results of this study, the decision regarding the appropriate length of an LHSH should be considered carefully. Although LHSHs are widely available to the public in a variety of styles through catalogs and the Internet, proper selection and training in their use is an important, if not essential, service provided by occupational therapists. The cliché “one size fits all” should not be part of the necessary clinical reasoning process when determining the proper LHSH. Although the longer shoehorn tended to elicit less hip flexion, BMI influenced the degree of hip rotation. Hence, it is important for occupational therapists to be involved in the selection process and to consider the patient’s anthropometry and pertinent medical history when determining the appropriate LHSH.
Limitations and Future Research
This study has several limitations. First, participants needed to don a canvas shoe that was not their own. Because it was a nontying canvas shoe, participants may have had little familiarity with this style of shoe. However, the shoes were selected in advance to ensure similarities among participants. Interestingly, when viewing the method by which participants flexed their hips, the strategy often involved a two-pronged approach involving both bending forward at the hip or raising their thigh off of the chair. It would be interesting to determine whether patients with hip arthroplasty commonly raise their thigh or whether they rely more on bending forward at the hip. Last, it is possible that the placement of the markers could have influenced the motions of the participants as they donned the respective shoes.
In conclusion, this study found that 18-in. LHSHs elicited greater hip flexion than 30-in. LHSH in a population of healthy women. In addition, a positive relationship was found between BMI and hip rotation. Although this study provides evidence to help guide clinical reasoning pertinent to prescribing LHSHs to people with hip precautions, the results of this study are based on a group of healthy adult women. Therefore, the findings of this study cannot be generalized to all populations. Follow-up studies should be conducted with participants who may more frequently use LHSHs. To establish clinical significance in people who have diagnoses that typically require use of LHSHs, a comparison study should be carried out. Participants who have recently undergone arthroplastic hip surgery or who have arthritis may be good candidates for future studies. People with these two conditions may move differently from healthy people when donning a shoe with a LHSH. Last, the findings in this study provide foundational evidence on which to base clinical reasoning when prescribing LHSHs to patients with hip precautions.
Footnotes
Acknowledgments
This research was completed as a partial requirement for the degree of occupational therapy doctorate for Rachel Wehrkamp. We wish to thank the University of Toledo Graduate School and the School of Nursing for awarding a grant to help finance this study.