
Abstract
We explored personal factors that can predict health-related lifestyles of community-dwelling older adults. A convenience sample of 253 older adults was recruited to complete the Health Enhancement Lifestyle Profile (HELP), a comprehensive measure of health-promoting behaviors. Data were analyzed through univariate correlational/comparative statistics followed by stepwise multiple regression analysis to determine significant predictor variables for different aspects of health-related lifestyle. Personal health conditions, including the number of chronic diseases or impairments and self-rated health, were two strong predictors for the HELP (R 2 = .571, p < .0001). Demographic characteristics, including age, gender, race, education, and employment status, also demonstrated varied degrees of capability for predicting the different HELP scales (e.g., Exercise, Diet, Leisure). When developing individualized plans for older adults in community settings, occupational therapists should consider the clients’ strengths and vulnerabilities potentially derived from personal health factors and demographic attributes to yield more effective lifestyle interventions.
Lifestyle choices play an important role in determining the health and vitality of older adults (Rowe & Kahn, 1997). A habitual pattern of health-promoting behaviors, such as routine exercise, healthy diet, leisure participation, spiritual growth, interpersonal relationships, stress management, and health responsibility, has been recognized as the core of a healthy lifestyle (Pender, 1996). The overarching statement of the Occupational Therapy Practice Framework: Domain and Process (2nd ed.; American Occupational Therapy Association, 2008), “supporting health and participation in life through engagement in occupation” (p. 626), suggests the responsibility of occupational therapists to help people shape their lifestyles through those health-enhancing occupations. An ample body of literature in occupational therapy and other disciplines has also identified lifestyle as a modifiable factor and has integrated it into the framework of successful aging to promote health and prevent or delay the deteriorating effects of chronic illness among older adults (e.g., Clark et al., 2001, 1997; Depp & Jeste, 2006; Rowe & Kahn, 1997). Therefore, occupational therapists working with older adults in community settings should evaluate and monitor factors associated with lifestyle choices as the first line of defense for reducing the risks of chronic diseases or disabling conditions in the elderly population.
Lifestyle is a complex health dimension that dynamically involves personal, environmental, behavioral, and occupational factors (Mandel, Jackson, Zemke, Nelson, & Clark, 1999). Although some researchers have attempted to conceptualize lifestyle as a matter of personal choice and individual responsibility, many others have argued for the existence of predetermined personal, cultural, environmental, and health factors that intertwine with various aspects of lifestyle (Lhussier & Carr, 2008). The evaluation of health-related lifestyle should take on a holistic approach that incorporates a range of personal and contextual factors to allow for an appraisal of its complexity and multidimensionality.
According to Pender’s (1996) Health Promotion Model, personal factors such as age, gender, education, socioeconomic status, marital status, living arrangements, and chronic health problems can serve as modifying factors that influence people’s health-related lifestyle. However, aging research that specifically investigates the relationships between these demographic characteristics and the health-related lifestyle of community-dwelling older adults has been limited (Cockerham, 2001; Schuster, Dobson, Jauregui, & Blanks, 2004).
We conducted a literature review and found that in many studies, these potential demographic correlations were presented as only a small part of a broad picture in the research findings and were often covariates of other major study variables (e.g., physical function, quality of life, risk behaviors). Second, most studies concluding that such relationships existed were based exclusively on subgroups of older adults with certain diagnostic characteristics (e.g., diabetes, arthritis, cancer, depression) rather than samples of typical community-residing older adults. Moreover, a lack of comprehensive and valid lifestyle measures was found in several population-based studies that investigated variables associated with lifestyles in older adults; that is, in these large-scale surveys, health-promoting behaviors and lifestyles were examined simply by asking a few questions that focused mostly on the habits of exercise, diet, or smoking (Koertge et al., 2003; Toft et al., 2008).
The purpose of this study was to determine personal factors that might predict health-related lifestyles in a sample of community-dwelling older adults. The specific factors examined were age, gender, race, marital status, education, employment status, the number of chronic diseases and impairments, and self-rated health status. A comprehensive measure of health-related lifestyle was completed, the Health Enhancement Lifestyle Profile (HELP; Hwang, 2010b), a Rasch-based instrument that assesses various aspects of health-promoting lifestyle behaviors.
Method
Design
This descriptive study explored the personal factors that can be used to predict the various aspects of health-related lifestyle of community-dwelling older adults. Data were derived from the development of HELP (Hwang, 2010b).
Participants
The study sample consisted of older adults residing in southern California. Each participant met the following criteria: age ≥55 yr, community dwelling, and adequate cognitive and English-language capabilities for responding to questionnaires. Convenience sampling and snowball sampling methods were used to recruit participants from a diversity of community sites, including senior citizen centers, senior residential communities, independent living facilities, adult day health care centers, local senior social and activities groups, and religious groups and organizations. Despite the use of nonprobability sampling methods, we attempted to ensure that the study sample would demonstrate an adequate distribution in various racial categories, age ranges, and residential locations.
Instrumentation
The measurement of personal factors and health-related lifestyle was completed through HELP (Hwang, 2010b). HELP can be administered as a self-report questionnaire or as an interview in which the interviewer reads aloud the questions and records the respondent’s answers. It consists of two sections. The first section assesses three categories of personal factors:
Demographics, such as age, gender, ethnicity, marital status, and education
Fifteen chronic illnesses or impairments (i.e., arthritis; back or neck problems; eye or vision problems; diabetes; heart problems; depression, anxiety, or emotional problems; walking problems) derived from the Centers for Disease Control and Prevention (CDC) Health-Related Quality-of-Life 14-Item Measure (CDC, 2000), assessed in a checklist
Self-rated heath, assessed in a single question that was modified from the RAND 36-Item Health Survey (i.e., “How do you rate your overall health status: excellent, good, fair, or poor?”; Hays & Morales, 2001).
The second section of HELP comprises seven scales measuring different aspects of health-related lifestyle: (1) Exercise, (2) Diet, (3) Productive and Social Activities, (4) Leisure, (5) Activities of Daily Living (ADLs), (6) Stress Management and Spiritual Participation, and (7) Other Health Promotion and Risk Behaviors. Each scale consists of eight items that examine the frequency of the respondent’s engagement in the previously mentioned areas of health-related occupations (see Figure 1 for sample items). Respondents are asked to answer each question according to their typical or routine performance during the past 3-mo period. Response categories generally include never, 1 to 2 days, 3 to 4 days, 5 to 6 days, and 7 days (per week).
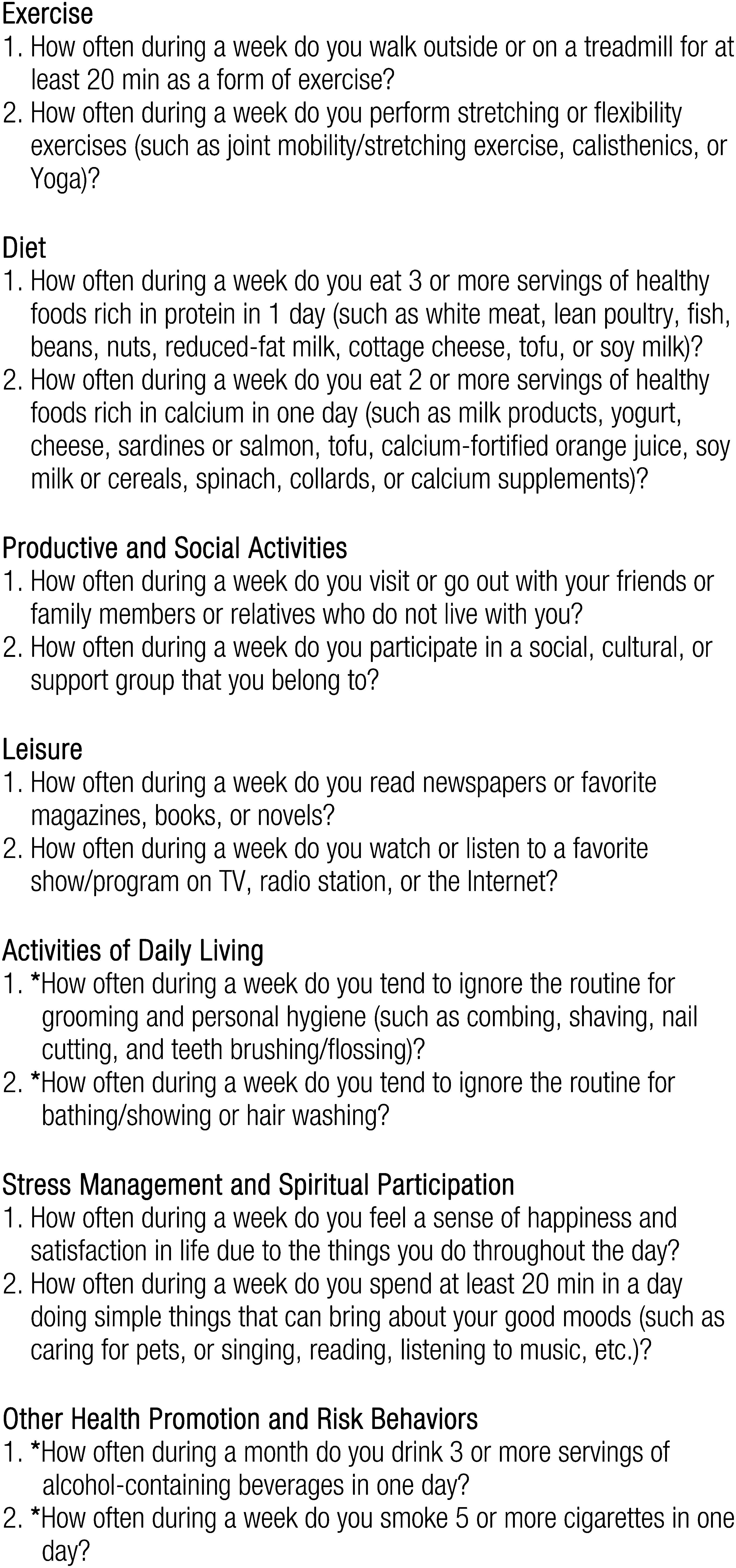
Sample Items of the Health Enhancement Lifestyle Profile Scales
As suggested by participants in the field pretesting study (see Hwang, 2010b), we added an additional category, 1 to 2 days a month. In addition, it was also suggested that monthly frequency (i.e., never, 1 day, 2 days, 3 days, 4 days, 5 days or more per month) be used for a few items assessing activities that may not be performed on a daily or weekly basis (e.g., carpentering, auto/boat/house fixing) and those assessing noticeable health risk behaviors (e.g., “drink three or more servings of alcohol-containing beverages in 1 day”).
For scoring, each response is given a numerical value reflective of the relative frequency. The result is a 0- to 5-point rating scale (0 = never; 5 = 7 days a week). Responses from negatively worded items (see sample items marked with an asterisk in Figure 1) are reversed for scoring. For each HELP scale, a subtotal score ranging from 0 to 40 can be computed; a higher score indicates a higher frequency of health-promoting behaviors. The total HELP score ranges from 0 to 280. The approximate time needed for completing and administering HELP is 20–40 min.
Psychometric properties of HELP have been supported through multiple procedures and studies. Piloting of HELP was completed through focus group and field pretesting to ensure the relevance and clarity of the measure (see Hwang, 2010b). The Rasch measurement model was used to establish the unidimensionality of each HELP scale through the analyses of principal components of residuals, goodness-of-fit statistics, local dependence, and differential item functioning. Items in each scale form a difficulty hierarchy that provides an expected pattern of health lifestyle behaviors in older adults. Acceptable to good person separation and reliability statistics substantiated the clinical applicability and consistency of HELP scores. In addition, analysis of the rating scale structure confirmed the functioning of the response categories (i.e., 0- to 5-point scale) used in the HELP scales (Hwang, 2010b).
Additional evidence of reliability and validity of HELP was provided through classical test theory: The α coefficients ranged from .75 to .92 among the HELP scales, indicating acceptable to good internal reliability (Hwang, 2010c). Construct validity was supported by the method of hypothesis testing that examined (1) the patterns of interrelationship and interdependence among the seven HELP scales (Pearson rs = .37–.62, p < .0001) and (2) the correlations between the HELP results and the global health status (Pearson rs = .42–.71, p < .0001; Hwang, 2010c). Finally, the stepwise multiple regression models revealed that five of the seven HELP scales (i.e., Exercise, Diet, ADLs, Stress Management and Spiritual Participation, and Other Health Promotion and Risk Behaviors) served as significant predictors for health-related quality of life of older adults (Hwang, 2010a).
Procedures
Approval from the institutional review board at California State University, Dominguez Hills, was received before data collection. HELP was completed by each participant either (1) in a direct interview, in which a graduate student or a staff member read aloud the questions and recorded responses for the participant or (2) by means of paper and pen, administered onsite to an individual or a group of participants. In a few cases, the instruments were delivered to potential participants by postal or electronic mail with instructions enclosed.
Data Analysis
Data were analyzed separately for each of the seven HELP scales as well as the total HELP (the total of the seven scales) to yield the distinct sets of personal factors that can serve as predictors of different aspects of the lifestyle measure. First, a series of univariate correlational and comparative analyses, including Pearson correlation coefficient (r), independent t test, and one-way analysis of variance (ANOVA), was conducted to screen factors that may have an effect (prediction potential) on the dependent variables (i.e., seven HELP scales and the total). A probability level (p) of .25 was adopted as the selection criterion for the entry of the predictor variables (factors) into the subsequent regression analyses. The use of the p range of ≤.25 was to avoid the exclusion of potentially important factors from the analyses (Hosmer & Lemeshow, 1989; Tabachnick & Fidell, 2007).
Before running the regression analysis, factors that were of a categorical variable were dummy coded. These factors included gender (reference group: female), race (reference group: White), marital status (reference group: married), and employment status (reference group: unemployed/retired). In addition, the possibility of muiticollinearity between predictor variables was investigated through collinearity diagnostics. The resultant tolerance values ranged from 0.82 to 0.99 (i.e., >0.40), and variance inflation factors ranged from 1.12 to 1.64 (i.e., <10), indicating an absence of muiticollinearity (Tabachnick & Fidell, 2007).
Finally, given the exploratory nature of the analysis, the stepwise option of variable entry was used, with a probability level of p < .05 to enter and p ≥ .10 to remove. An optimal regression model solution was developed for each HELP scale and the total HELP to identify significant predictor variables. With the eight potential predictor variables in this study, to achieve power of .80 and a medium effect size (effect size = .15, α = .05), a sample size of 108 was required to detect a significant model (Tabachnick & Fidell, 2007). Our sample size of 253 was thus considered adequate. All the previously mentioned statistical analyses were performed using SPSS/PC+ Version 17.0 software (SPSS Inc., Chicago).
Results
A total of 253 older adults (148 women and 105 men) were recruited for this study. Participants’ ages ranged from 55 to 92 yr (mean [M] = 71.4, standard deviation [SD] = 10.5). Table 1 provides a summary of participants’ demographics and health-related information. Most participants were unemployed or retired. The most commonly reported health problems or impairments among the participants included hypertension, arthritis, visual impairment, back or neck pain, and diabetes. The total number of chronic diseases and impairments reported by each participant ranged from 0 to 10 (M = 2.77; SD = 2.03). Slightly more than 70% of the participants considered their health status to be “good” or “excellent,” and only approximately 5% believed that they were in poor health.
Summary of Personal Factors (Demographics and Health-Related Information; N = 253)
Note. For Health Problems/Impairments, ns total more than 253 and percentages total more than 100 because respondents were asked to check all that apply.
Table 2 demonstrates the personal factors selected by the preliminary analyses (i.e., Pearson r, t test, ANOVA) for the entry of predictor variables to the regression model of each HELP scale and the total HELP. All eight personal factors were entered at least once into the regression analyses. As seen, the number of diseases or impairments and self-rated health was constantly included in the data entry of the regression analyses of the seven HELP scales as well as the total HELP, whereas marital status was selected only for the Exercise scale.
Personal Factors Selected for Regression Analysis of Each Health Enhancement Lifestyle Profile (HELP) Scale
Table 3 displays the results of regression analysis after stepwise selection of the significant predictor variables to form an optimal regression model solution for each HELP scale. All the regression model solutions were significant at p < .0001, and the values of adjusted R 2 ranged from .205 for the ADLs scale to .571 for the total HELP. Each model solution (HELP scale) consisted of two or more significant predictor variables (personal factors). For example, the Exercise scale can be best predicted by three factors: (1) the number of chronic diseases and impairments, (2) self-rated health, and (3) gender. With the exception of marital status, all other factors emerged as significant predictors for one or more HELP scales. Two factors, the number of chronic diseases or impairments and self-rated health, were found to be predictive of all seven HELP scales as well as the total HELP. In particular, both factors exclusively predict Diet, ADLs, and the total HELP.
Multiple Regression Analyses of Personal Factors Predictive of the Health Enhancement Lifestyle Profile Scales (N = 253)
Only the final models and significant predictors are presented.
Compared with the women, the men had a slightly more positive effect on the Exercise scale but a slightly more negative effect on both the Productive and Social Activities and Stress Management and Spiritual Participation scales. Employment (both full time and part time) contributed positively to Productive and Social Activities, whereas full-time employment had a negative impact on Leisure, in contrast with the unemployed/retired status. With regard to race, relative to White, the Asian/Pacific Islander and African-American groups presented less favorable effects on both the Productive and Social Activities and Leisure scales, whereas the Asian/Pacific Islander and Hispanic/Latino groups presented a more favorable effect on the Stress Management and Spiritual Participation scale. Moreover, education was a positive predictor of scores on the Leisure and Other Health Promotion and Risk Behaviors scales. Finally, age had a small positive effect on the Other Health Promotion and Risk Behaviors scale, along with other factors (i.e., the number of diseases and impairments, self-rated health, education).
Discussion
This study was conducted to determine the significance of eight personal factors in predicting health-related lifestyle of a sample of community-dwelling older adults. Regression analyses revealed that different aspects of lifestyle (as measured by the HELP scales) can be significantly predicted by several of the personal factors entered. Personal health conditions, including the number of chronic diseases/impairments and self-perception of health status, were found to be the best predictors of the lifestyle measure. In particular, these two factors exclusively accounted for 57% of the variance in the total HELP score. Demographic characteristics, including gender, employment status, race, education, and age, also demonstrated varied degrees of capability for predicting different aspects of health-related lifestyle in the older adults. Although all the resultant regression model solutions were significant at p < .0001, their adjusted R 2 values were mostly <.30. Not surprisingly, because of complexity in the context of health-related lifestyle, we did not expect these personal factors alone to be held accountable for a great deal of variance of lifestyle behaviors among older adults.
The number of chronic diseases and impairments was a strong inverse predictor for all seven HELP scales and the total HELP. The results suggest that older adults who demonstrate more positive lifestyle behaviors may have fewer adverse health conditions, and vice versa. Many studies have shown that chronic conditions and disability can be prevented, postponed, or diminished through positive lifestyle behaviors. For example, changes in exercise and diet, when used as a preventive intervention in older adults, can significantly reduce the risk of cardiovascular disease, osteoporosis, arthritis, diabetes, some forms of cancer, obesity, cognitive decline, and depression (Depp & Jeste, 2006; Koertge et al., 2003; Serra-Majem, Roman, & Estruch, 2006). Studies have also shown the positive correlations between levels of participation in social and productive activity and a range of health outcomes, including physical and cognitive functions, self-efficacy, and quality of life (Everard, Lach, Fisher, & Baum, 2000; Lawton, Winter, Kleban, & Ruckdeschel, 1999). These research findings support the protective effects of healthy lifestyle behaviors against the occurrence of chronic illness or disabling conditions among older adults. Our research findings, however, may only suggest the ability of the disease or impairment count to “mathematically” predict the pattern of health-related lifestyle in older adults. Clinically, all these relationships need not be causal. For example, people who demonstrate prolonged health risk behaviors may consequently suffer from more chronic diseases; conversely, it is possible that those who have chronic diseases, such as diabetes, become more health conscious and incorporate a range of health behaviors into their day-to-day self-management routine.
Self-rated health was also a significant predictor for all aspects of the lifestyle measure. This subjective rating of health has been considered “a simple, direct, and global way of capturing perceptions of health using criteria that are as broad and inclusive as the responding individual chooses to make them” (Idler & Benyamini, 1997, p. 22). That is, older adults’ perceptions of their health status are generally self-determining (DeSalvo, Bloser, Reynolds, He, & Muntner, 2006). Studies have shown that older adults with poor perceptions of health are less likely to engage in exercise routines (Rakowski & Mor, 1992) and self-care (Haug, Wykle, & Namazi, 1989) and are more likely to have health risk behaviors, such as smoking and heavy alcohol consumption (Hirdes & Forbes, 1993). Self-rating of health may hold the key to understanding the influences of various psychocognitive factors (e.g., self-efficacy, motivation, personal values, preferences) on health-promoting behaviors of older adults (DeSalvo et al., 2006).
Variations were found in the predictive strength and pattern of demographic characteristics toward different aspects of health-related lifestyle. In general, after the stepwise selection of the previous two predominant personal health factors, the demographic variables appeared to be less accountable for the variance of lifestyle behaviors (see β coefficients in Table 3), yet the levels of their predictive strength were still statistically significant. Although findings of population-based studies on various health outcomes (e.g., functional independence, life satisfaction, quality of life) have generally favored married older men and women (de Belvis et al., 2008; McCamish-Svensson, Samuelsson, Hagberg, Svensson, & Dehlin, 1999), our results did not suggest the effect of marital status on the outcomes of the lifestyle measure. Interestingly, as distinguished by Pender (1996) in her Health Promotion Model, personal psychocognitive factors, such as self-perception of health and self-efficacy, may have more direct influence on the pattern and frequency of health-promoting behaviors, whereas personal demographic characteristics, such as age, gender, race, and marital status, are considered modifying factors that have indirect effects on health behaviors.
The possible relationships between the demographic characteristics and different aspects of heath-related lifestyle after taking into account the contribution of personal health factors (i.e., the disease/impairment count, self-rated health) can be summarized as follows:
Older men are more likely than older women to engage in exercise but are less likely to participate in activities related to paid or volunteer work, social networking, stress management, and spiritual or religious participation.
Employment (both full time and part time) among older adults provides an opportunity for enhancing productivity and socialization; conversely, it may compromise leisure participation of older adults.
Compared with Whites, elderly Asian and African-Americans are less likely to participate in paid or volunteer work as well as social and leisure activities.
Compared with Whites, elderly Asians and Hispanic/Latinos are more involved in spiritual or religious activities.
A higher level of education correlates with a higher level of leisure participation as well as a higher frequency of health self-monitoring behaviors (e.g., routine check on blood pressure and body weight) and a lower frequency of health risk behaviors (e.g., smoking, frequent use of over-the-counter drugs).
The older the adult is, the lower is the frequency of health risk behaviors.
As discussed previously, given the multifaceted and dynamic features of the lifestyle context, caution in applying these findings is warranted.
Study Limitations
The generalizability of the findings is limited because of the use of a nonprobabilistic sample from southern California. In addition, personal factors included in this study were limited to those assessed in the personal information section of HELP. Other demographic variables, such as income, living arrangements, and health care coverage, as well as related psychocognitive variables, such as self-efficacy, motivation, and personal values and preferences, may also, as single entities or in combination, play a role in the already complex dynamics of health lifestyle behaviors. Future empirical investigations or cohort studies using large random samples and systematic control and analysis of multiple factors (e.g., path analysis, structural equation modeling) are suggested to strengthen both the validity and the depth of this study's exploratory findings as well as to establish some specific causal connections between personal factors and health lifestyle behaviors.
Conclusion
The findings of this study help make explicit the potential influence of personal factors on health-related lifestyles of community-dwelling older adults. The study used HELP (Hwang, 2010b) to allow for a comprehensive measure of lifestyle behaviors that extends beyond those few aspects (e.g., exercise, diet, smoking) frequently examined in population-based health surveys. As argued by Sobal, Revicki, and DeForge (1992), “engaging in one health behavior does not guarantee the practice of others” (p. 357); therefore, studies on health-related lifestyle should include an all-encompassing measure of health-promoting and health risk behaviors. In addition, we used a multivariate modeling method after the preliminary univariate correlational/comparative analyses to capture the complex dynamics of those interlocking variables. Our findings, although exploratory in nature, have yielded a conceptual framework that delineates the intricate relationships between personal factors and lifestyle behaviors in older adults.
Screening and counseling elderly clients about lifestyle choices should be integrated into the routine service of geriatric occupational therapy. Individualized plans that consider clients’ strengths and vulnerabilities potentially derived from personal health factors and demographic attributes will result in more effective lifestyle interventions. While recognizing the possible effects of age, gender, race, education, and employment status on the various health lifestyle behaviors, occupational therapists should also cautiously avoid stereotypical assumptions regarding individual clients.
It is also important to be cognizant that health-promoting behaviors observed in older adults are often driven by a desire for health rather than a fear of disease (Pender, 1996). The delicate causal connections between chronic diseases and impairments and health-related lifestyles can be scrutinized for each client through the inclusion of diverse personal and contextual and environmental factors in the evaluation. Moreover, the simple, subjective self-rating of health that has been considered an all-encompassing health indicator weighted not only by physical functioning but also by various psychocognitive factors (e.g., self-efficacy, motivation; DeSalvo et al., 2006; Idler & Benyamini, 1997) can be used as an additional estimate of health-related lifestyles among older adults. Accordingly, interventions or strategies to address older adults’ health self-efficacy beliefs and motivation can be provided to help sustain healthy lifestyle behaviors.
Footnotes
Acknowledgments
We thank the participants who contributed their time and effort to complete the HELP. We also thank the group of master’s-level occupational therapy students for their enthusiasm and participation in the training and data collection of the study. This study was funded by Sally Casanova Memorial Research, Scholarship and Creative Activities Program, California State University, Dominguez Hills.