
Abstract
Stroke is the most serious disabling condition in the United States and the developed world (Lopez, Mathers, Ezzati, Jamison, & Murray, 2006; Murray & Lopez, 1997). Long-term outcomes following stroke are poor. About two-thirds of patients living in the community 6 mo after the event report participation restrictions (Mayo, Wood-Dauphinee, Côté, Durcan, & Carlton, 2002), and about half remain dependent in activities of daily living (Appelros, Samuelsson, Karlsson-Tivenius, Lokander, & Terént, 2007; Mayo et al., 2002); patients report still further decline in participation over the following 2 to 4 yr (Desrosiers et al., 2006). Even after inpatient rehabilitation, most people do not achieve their functional goals following a stroke (Brock et al., 2009).
To improve functional outcomes for people with stroke, a new intervention paradigm must be found that shifts the focus from traditional component-focused rehabilitation to more comprehensive, holistic approaches that, at a minimum, support maintenance of therapeutic gains postrehabilitation and, optimally, support the generalization and transfer of skills that will lead to continued improvement, rather than further deterioration, over time. To address this need, our research group explored the utility of a goal-oriented, cognitive-based approach, Cognitive Orientation to daily Occupational Performance (CO–OP; Polatajko & Mandich, 2004), to improve performance in self-selected functional goals in people living with the effects of stroke.
CO–OP is a complex treatment approach that combines task-specific training and cognitive strategy use in a novel, client-centered manner. Clients self-select three skills to be the focus of treatment. An adaptation of Meichenbaum’s problem-solving strategy, Goal–Plan–Do–Check (e.g., Meichenbaum & Goodman, 1971), forms the main global cognitive strategy framework for the CO–OP approach. Through an iterative process, the therapist uses guided discovery, rather than explicit instruction, to help the patient carry out dynamic performance analyses and discover domain-specific strategies that form solutions to performance problems. Thus, in CO–OP, the process of task-specific training becomes self-directed; that is, the standard approach to task-specific training is augmented by strategy use and self-directed problem analyses and solutions. The process of learning dynamic performance analysis and problem-solving strategies in concert with meaningful skill acquisition enables the patient to transfer both strategies and skills to novel situations.
Previous research by our group includes three studies using single-case methods (Henshaw, Polatajko, McEwen, Ryan, & Baum, 2011; McEwen, Polatajko, Huijbregts, & Ryan, 2009, 2010). These studies provided preliminary evidence of CO–OP’s capacity to improve performance in adults with stroke. Two in-depth case studies revealed the importance of motivating, self-selected goals and the need to support participants in using this problem-solving approach, which is very different from the therapist-directed approaches most had previously experienced (Henshaw et al., 2011). In our initial single-case experimental series, each of 3 participants showed significant performance improvements in at least 2 trained skills postintervention and at 1-mo follow-up (McEwen, Polatajko, et al., 2009). A second series of 3 participants demonstrated both significant skill performance in all trained skills and transfer to untrained skills (McEwen, Polatajko, Huijbregts, & Ryan, 2010).
Research Question
The single-case studies provided evidence that CO–OP is associated with improved skill performance, but they provided no information about CO–OP in comparison with other treatment approaches. In this pilot study, we posed the following questions:
Is there a difference in performance improvements on self-selected goals when comparing CO–OP intervention to standard occupational therapy (SOT) in adults at least 6 mo poststroke?
What is the direction and magnitude of the difference?
Methods
Research Design
We conducted a pilot randomized controlled trial. Participants were randomized to receive either CO–OP or SOT, both administered by experienced occupational therapists. We obtained institutional review board approval and informed, written consent from all participants.
Participants and Recruitment
Participants were recruited using the Cognitive Rehabilitation Research Group (CRRG) database (Wolf, Baum, & Conner, 2009) or on discharge from the Rehabilitation Institute of St. Louis. Participants were required to be at least 6 mo poststroke and living in the community and to have a National Institutes of Health Stroke Scale (NIHSS; Goldstein & Samsa, 1997) score of 13 or less, an IQ score of 80 or more, and no more than minimal aphasia.
Interventions
Two experienced occupational therapists were trained to use the CO–OP approach and used the published textbook as a protocol manual (Polatajko & Mandich, 2004). Two other experienced therapists who had not been exposed to CO–OP administered SOT. Both CO–OP and SOT therapists administered the Canadian Occupational Performance Measure (COPM; Law et al., 2005) to participants to help them self-select three personally meaningful goals to be the focus of treatment. Both CO–OP and SOT were designed to be delivered in ten 1-hr individual treatment sessions.
The CO–OP treatment guidelines were taken from a book detailing the approach (Polatajko & Mandich, 2004). CO–OP is a goal-oriented, performance-based approach that makes use of two types of cognitive strategies: (1) Goal–Plan–Do–Check, a global cognitive problem-solving strategy adopted from Meichenbaum and Goodman (1971), and (2) domain-specific strategies, derived through dynamic performance analysis and identified by the client through guided discovery in the plan phase. At the outset, the occupational therapist teaches the global strategy to the client, and the client uses the strategy in all subsequent sessions as the main problem-solving framework to facilitate domain-specific strategy identification, skill acquisition, and goal achievement. The client identifies a goal, and the therapist guides him or her in discovering a plan to meet the goal. The client then does the plan and subsequently checks to see if the plan worked. If the client does not achieve the goal, the therapist guides the client in modifying the plan. For example, a participant with a goal of cooking who is experiencing difficulty chopping cucumbers may articulate a plan to keep the wrist straight while using a knife—for example, by telling herself to “be strong” (a self-talk domain-specific strategy) while cutting. If she is still unable to cut with this plan (i.e., the check determines that the plan didn’t work), the therapist guides her to discover a new plan, such as telling herself to “keep the knife blade perpendicular to the cutting surface” (a task specification domain-specific strategy) or to switch to using her nonhemiplegic hand on the knife and the hemiplegic hand to stabilize (a task modification domain-specific strategy).
With each new plan, the client repeats the Do–Check cycle until he or she has a plan that achieves the goal. Throughout, the therapist regularly seeks opportunities to promote generalization of skills and strategies to other environments (“Could you try cutting vegetables at home?”) and to encourage transfer to novel skills (“Could you use this strategy for other cooking skills?”).
Because no publication identifying standard occupational therapy intervention with stroke exists, the authors held a focus group with expert occupational therapists to define treatment guidelines that reflect current practices. The approach the therapists proposed began with an interview to learn about what the client was doing before the stroke and to ask the client to identify personally meaningful goals. The next steps were to observe the client to determine issues that interfere with performance and to suggest exercises and tasks that would lead to skills to support the client’s achievement of his or her goals. Each therapist and client agreed to this intervention plan and implemented it over a maximum of 10 sessions. Specific treatment techniques and short-term goals were therapist driven and included a combination of component-based and task-specific training. For example, if the participant-selected goal was independent upper-extremity dressing, the therapist might propose a short-term goal of increasing active shoulder abduction to 90° and have the participant work on shoulder range of motion (ROM; task component) and repeatedly practice the whole task of donning and doffing a jacket.
CO–OP and SOT are similar in that both begin with three participant-selected goals, but they differ in two main ways: (1) In SOT, treatment plans are completely therapist driven, whereas in CO–OP they are participant driven with guidance from the therapist, and (2) in SOT, the emphasis is on impairment-level or component-level treatment (e.g., working on ROM) in addition to whole-activity treatments, whereas CO–OP focuses entirely on activity-level treatments.
Instruments
We assessed the main outcome, change in performance on self-selected goals, using the therapist-rated Performance Quality Rating Scale (PQRS; Miller, Polatajko, Missiuna, Mandich, & Macnab, 2001) and the participant-rated COPM. Both were administered before (T1) and after (T2) intervention.
The PQRS was designed for evaluating performance on self-selected skills and has previously been used in CO–OP research. The therapist rates the client’s performance on a 10-point scale (1 = can’t do the skill at all and 10 = does the skill very well; Miller et al., 2001). Interrater reliability in the stroke population was estimated using the intraclass correlation coefficient at .71 (McEwen, Polatajko, et al., 2009).
The COPM (Law et al., 2005) is a standardized instrument for eliciting performance issues from the client’s perspective and for capturing perceived changes in performance over time. In our study, therapists used the COPM to elicit participant-selected goals and participant-perceived ratings of performance and performance satisfaction for each goal. A 10-point visual analog scale is used to obtain these ratings (1 = low performance or performance satisfaction and 10 = excellent performance or performance satisfaction). The COPM has demonstrated test–retest reliability of .89 in people with stroke (Cup, Scholte op Reimer, Thijssen, & van Kuyk-Minis, 2003). A change of 2 points or more on the COPM is considered clinically significant (Law et al., 2005).
Data Collection
Before the intervention, a research assistant blinded to group assignment administered the CRRG standard battery of physical, health status, and neuropsychological tests. Because use of the PQRS and COPM is inherent in the CO–OP intervention, blinding was not possible, and treating therapists administered these assessments before and after both interventions for each of the three participant-selected goals.
Data Analysis
Analysis was conducted with PASW Statistics Version 18.0 and SPSS Version 17.0 (SPSS Inc., Chicago). The significance level for all tests was set at p < .05. To examine baseline between-group differences, independent samples t tests were used for continuous data and χ2 for categorical data. Between-group baseline comparisons were made on age, gender, education, and NIHSS scores. Additional analyses were done to compare participants who withdrew from the study with those who had complete data on age, gender, education, NIHSS score, and the CRRG neuropsychological assessment battery. Means and standard deviations were calculated for both groups for the two main outcome measures, PQRS and COPM. Because of the small sample size and the ordinal data, nonparametric Mann–Whitney U scores were used to compare between-group PQRS and COPM change scores. To address the direction and magnitude of between-group differences, a simple linear regression analysis was conducted to estimate the difference in treatment effect of CO–OP compared with SOT on change in PQRS, COPM Satisfaction, and COPM Performance. Unadjusted regression coefficients were calculated using pre–post change in PQRS, COPM Satisfaction, and COPM Performance as outcome variables and group (CO–OP or SOT) as the explanatory variable.
Results
Recruitment and Retention
Thirty-seven (37) potential participants were recruited, of whom 20 met eligibility criteria. Nine were randomized to the SOT treatment condition and 11 to the CO–OP condition; 5 participants withdrew from SOT and 7 from CO–OP, leaving 4 per group (Figure 1, CONSORT Flow Diagram).
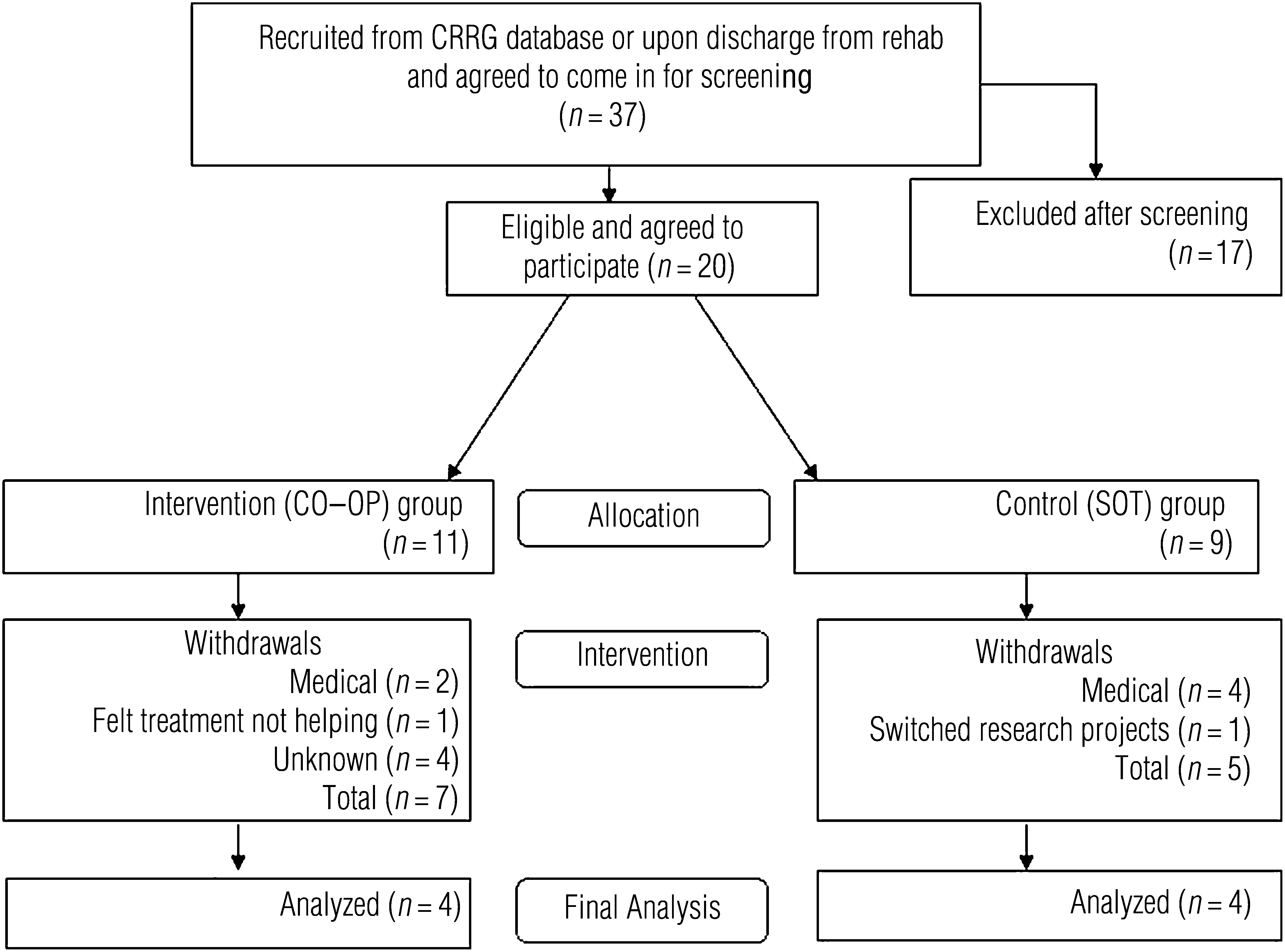
CONSORT flow diagram.
Participant Characteristics
The 20 eligible participants had a mean age of 60.4 yr and a mean NIHSS score of 7, and 57.9% were women. Although those who completed the study (n = 8) and those who withdrew (n = 12) did not differ in age, gender, education, or NIHSS scores, those who withdrew had significantly poorer scores on a number of neuropsychological tests, particularly those measuring memory, task switching, and vocabulary. Specifically, independent samples t tests revealed significantly poorer scores for the withdrawn group on immediate recall, short delay recall, and long delay recall using the California Verbal Learning Test (Delis, Kramer, Kaplan, & Ober, 2000); on vocabulary using the Weschler Abbreviated Scale of Intelligence (Wechsler, 1999); and on color and trails from the Delis–Kaplan Executive Function System (Delis, Kaplan, & Kramer, 2001).
Both completing groups were comparable on age, gender, education, and NIHSS score. Both groups selected personally meaningful goals that spanned impairment, activity, and participation. Goals selected by SOT group participants included bathing (2), engaging in studies, managing e-mail, improving left extremity dressing, transferring to and from floor, attending church, cooking (2), gardening, eating, and improving left arm control. CO–OP participant goals were reading, driving, gardening, organizing bills, obtaining Medicaid, making jewelry, dressing, using the bathroom, standing, improving memory, participating in activities with grandkids, and repairing the house.
Intervention Outcomes: Between-Group Differences
Intervention outcomes are displayed in Table 1. CO–OP participants showed greater improvement in PQRS (U = 0.0, p = .02) and in COPM Performance (U = 0.0, p = .02) compared with SOT participants. No group difference was found on COPM Satisfaction (U = 5.0, p = .38). The regression coefficients displayed in Table 1 provide an estimate of the difference in treatment effect of CO–OP compared with SOT on change in PQRS, COPM Satisfaction, and COPM Performance using the specific units of each measure; all three measures use 10-point ordinal scales. Pre–post improvement in the CO–OP group was 3.0 PQRS units (confidence interval [CI] 1.4–4.6) and 3.0 COPM Performance points (CI 0.2–5.9) higher than in the SOT group. Thus, we estimate that CO–OP had a positive treatment effect in the magnitude of about 3.0 units for PQRS and COPM Performance. Because the CI for COPM Satisfaction spanned both negative and positive numbers, no conclusions about the direction of treatment effect could be drawn for that outcome.
Pre- and Postintervention Mean Scores on Outcome Measures and Effect Size Estimates
Note. CI = confidence interval; CO–OP = Cognitive Orientation to daily Occupational Performance (Polatajko & Mandich, 2004); COPM = Canadian Occupational Performance Measure (Law et al., 2005); PQRS = Performance Quality Rating Scale (Miller, Polatajko, Missiuna, Mandich, & Macnab, 2001) SD = standard deviation; SOT = standard occupational therapy; T1 = preintervention; T2 = postintervention.
Unadjusted simple linear regression coefficient, derived from using change in the corresponding outcome as the dependent variable and group (categorical, CO–OP, or SOT) as the independent variable.
Discussion
The data from this pilot study suggest that CO–OP is associated with larger performance improvements on self-selected goals in people living with stroke than standard occupational therapy. Although promising, these results must be viewed as preliminary. This pilot study had a small sample and some methodological limitations. In this discussion, we address the therapeutic mechanisms that may explain these positive results and describe the study limitations that must be addressed in future research.
Both the CO–OP group and the SOT group chose their own treatment goals using the COPM, but in the CO–OP group, the therapists taught participants a global cognitive strategy (Goal–Plan–Do–Check) and used a guided discovery process to help participants create their own performance plans and evaluate those plans. Although the specific active ingredients in the CO–OP approach aren’t known, our experience with the approach suggests that providing participants with the autonomy to contribute their ideas in treatment sessions and a structured global problem-solving strategy enables them to achieve higher levels of skill performance than they would from SOT.
A recent review article investigating cognitive strategy use to improve motor skill acquisition in people with stroke concluded that further development of novel cognitive strategy-based interventions with the intention of improving long-term stroke outcomes is supported (McEwen, Huijbregts, Ryan, & Polatajko, 2009). Two previous randomized controlled trials demonstrated the successful use of global cognitive strategy-based treatment approaches to improve functional skill acquisition in people with subacute stroke (Geusgens et al., 2006; Liu, Chan, Lee, & Hui-Chan, 2004); participants in both trials demonstrated improved skill performance in trained and untrained functional skills. Evidence also supports increased autonomy for people undergoing poststroke rehabilitation. Proot, ter Meulen, Abu-Saad, and Crebolder (2007) wrote about the transition to autonomy in stroke rehabilitation. Using a grounded theory approach, they analyzed interviews from 22 clients undergoing stroke rehabilitation and proposed that people in stroke rehabilitation desired a gradual transition to shared decision making at discharge and that this often didn’t happen to the degree that people with stroke desired. Our group has conducted a qualitative study examining experiences with CO–OP and concluded that participants perceived they had benefitted from the increased autonomy, responsibility, and confidence associated with developing treatment plans (McEwen, Polatajko, Davis, Huijbregts, & Ryan, 2010).
Study limitations include nonblinding of assessment administration, high withdrawal rates, and high recruitment-to-enrollment ratio. Treating therapists administered both the COPM and the PQRS, introducing a potential scoring bias. In future CO–OP trials, efforts should be made to have research assistants blind to group allocation score the outcome measures. The withdrawal rate was 64% in the treatment group and 45% in the control group, and post hoc analysis revealed that participants who dropped out of both groups had lower verbal, memory, and task-switching scores. Because the withdrawal rate was high in both groups, it is not clear if the problem lay with recruitment, the fragility of the population, or some other unrecognized systemic problem. The high recruitment-to-enrollment ratio and the high withdrawal rate all represent threats to the internal validity of the study, and future trials should give careful attention to these issues.
Implications for Occupational Therapy Practice
The CO–OP approach shows promise to improve skill performance in adults living with the effects of stroke. Further study is required, however.
Conclusion
Both treatment groups improved their performance of complex, self-selected activities, but CO–OP treatment was associated with significantly greater improvements than SOT despite a very small sample size. In view of CO–OP’s positive treatment effect and armed with the practical experience gained in this pilot study, a larger-scale investigation with additional control and rigor is warranted so that firmer conclusions can be drawn.
Footnotes
Acknowledgments
This project was funded by the James S. McDonnell Foundation. SEM received support from the Social Sciences and Humanities Research Council, Canada, and JDR received support from the Canada Research Chairs Program. This article was presented in poster form at the American Congress of Rehabilitation Medicine (ACRM) and American Society of Neurorehabilitation (ASNR) Joint Educational Conference, Denver, CO, October 7–11, 2009 (Polatajko, McEwen, Ryan, & Baum, 2009).