
Abstract
Systemic sclerosis (SSc), also known as scleroderma, is a rare autoimmune disease of the connective tissue characterized by fibrosis of the skin and internal organs and vascular insufficiency; the latter is known as Raynaud’s phenomenon (LeRoy et al., 1988). The two major subsets of SSc according to the extent and distribution of skin thickening are (1) diffuse cutaneous, characterized by widespread skin thickening and early internal organ involvement and (2) limited cutaneous, the milder form of the disease, characterized by skin thickening limited to the hands, fingers, and feet.
Studies have reported that people with SSc experience extensive limitations in daily occupations, particularly those that require extensive hand function (Bérezné et al., 2011; Poole, 2006; Poole, Watzlaf, & D’Amico, 2004; Sandqvist, Eklund, Åkesson, & Nordenskiöld, 2004; Sandqvist, Hesselstrand, & Eberhardt, 2009). Work disability is common for people with SSc and has been estimated to be greater than that for people with rheumatoid arthritis (Ouimet, Pope, Gutmanis, & Koval, 2008). The prevalence of work disability ranges from 28.0% for patients with a disease duration of <2 yr to 44.8% for patients with disease duration of 10–15 yr (Hudson et al., 2009).
SSc typically causes impairment in hand function because of contractures causing decreased flexion of the metacarpophalangeal joint, decreased extension of the proximal interphalangeal (PIP) joint, and decreased abduction of the thumb (Sandqvist et al., 2004). Almost 90% of people with SSc experience Raynaud’s phenomenon (Khanna, 2011), making people with SSc very sensitive to cold. Raynaud’s phenomenon can also lead to digital ulcers at the tips of the fingers and over the PIP joints, which are associated with reduced hand function (Bérezné et al., 2011; Mouthon et al., 2010). Although several studies have shown that hand involvement in SSc is related to the performance of daily activities, only a few studies have examined the impact of hand function on working (Bérezné et al., 2011; Poole, 2006; Poole et al., 2004; Sandqvist et al., 2004, 2009), although intensive hand use is common in all work situations (Allaire et al., 2006). Sandqvist, Scheja, and Hesselstrand (2010) reported that demands on arm and hand function were the most common work-related problems for people with SSc. Other studies have reported that grip, dexterity, and ulcers are related to work disability (Nguyen et al., 2010; Sandqvist, Scheja, & Eklund, 2008).
Computer operation, a task common to many jobs, requires high levels of hand function. According to the most recent statistics, at least 56% of the working population uses a computer, and this statistic is higher for white-collar jobs such as management, professional, or office administrative positions (Day, Janus, & Davis, 2005). Research on coping strategies to remain employed after the advent of a rheumatic condition has suggested that workers frequently transition to less physically demanding jobs (Gignac, Cao, Lacaille, Anis, & Badley, 2008; Mancuso, Paget, & Charlson, 2000), the type of job that frequently requires computer use. Thus, the ability to use a computer may be a key factor in preventing work disability for people with SSc. Yet despite the serious limitations in hand function experienced by people with SSc and the importance of hand function for computer operation, no study has examined the problems people with SSc experience during computer use, the necessary first step to develop interventions to help reduce such problems. The needs assessment described in this article is used to examine self-reported problems with computer operation experienced by people with SSc. It is also used to gather preliminary information on the types of accommodation strategies people with SSc typically use to alleviate these problems. We examined the following research questions:
What types of problems do people with SSc most frequently experience with equipment during computer use?
To what degree do problems with equipment affect computer use in people with SSc?
What types of accommodation strategies do people with SSc use to alleviate problems during computer use?
Method
Participants
This study was approved by institutional review boards of the University of Pittsburgh and the University of New Mexico. The sample was a subset of a sample from a larger parent study examining work disability in people with SSc. Participants in the larger study were recruited through an announcement on the Scleroderma Foundation Web site. Inclusion criteria were a diagnosis of SSc with a minimum duration of 5 yr for participants with limited SSc or 2 yr for those with diffuse SSc, U.S. resident status, ability to communicate in English by telephone, current employment of >8 hr per week, and self-perceived difficulty working because of SSc symptoms. The researcher (Janet L. Poole) determined eligibility by telephone once potential respondents contacted the researcher. The researcher ascertained self-perceived difficulty working by asking each potential respondent if his or her SSc symptoms interfered with work. The symptoms potential participants noted included Raynaud’s phenomenon, digital ulcers, hand contractures or edema, pain, fatigue, cardiac or pulmonary symptoms, and gastrointestinal symptoms. Potential participants who reported that three or more symptoms interfered with work were eligible for the parent study, and those who also reported that they used a computer at work or home were included in the present study.
Instruments
The Computer Problems Survey (ComPS; Baker, Rogers, Rubinstein, Allaire, & Wasko, 2009) is a self-administered survey developed to ascertain problems with computer use experienced by people diagnosed with arthritis. The test–retest reliability has been found to be acceptable (Baker et al., 2009). The survey is divided into four sections. The first section includes general demographic questions. The second section requests information about general computer use, including where and how often respondents use a computer and how important computer use is to them. The third section examines the types of discomfort respondents experienced in the past month resulting from use of the following computer equipment: chair, keyboard, mouse, and monitor. Respondents rate the discomfort caused by each piece of equipment as just noticeable, mild, moderate, or severe. The fourth section examines specific problems caused by each type of computer equipment; respondents are asked to check all problems experienced and all accommodation strategies used for each equipment type from a list. Respondents then rate the degree to which their overall computer use is affected by all problems for each specific equipment item using a 4-item scale (small degree, moderate degree, considerable degree, or very high degree).
Procedure
Respondents eligible for the parent study were mailed the consent form and the parent study forms and a stamped, self-addressed return envelope. If they reported that they routinely used a computer, they were then sent the ComPS. If respondents did not return the forms within 3 mo, they were reminded by either phone or e-mail.
Data Analysis
Data were analyzed using SPSS Statistics Version 18.0 (IBM, Armonk, NY). We calculated descriptive statistics for all variables, including frequencies and percentages for nominal data and means for continuous data. The number of problems reported for each equipment type was summed and then collapsed into three categories for analysis: 1–2 problems, 3–4 problems, and ≥5 problems. Because few respondents selected just noticeable to describe their level of discomfort, that category was collapsed into the mild category.
Results
A total of 36 respondents met the inclusion criteria and were sent the consent form and questionnaires; 33 returned the questionnaires. Of these 33 respondents, 30 reported that they routinely used computers at work or home and were sent the ComPS. Twenty-seven ComPS surveys were returned. The mean age of our sample was 47.9 yr; 81% were female, and 74% were White. Slightly more than half were diagnosed with diffuse SSc (58%), and the mean length of time since diagnosis was 10.2 yr. All but 1 of the respondents worked, and most (70%) worked full-time. Most respondents (73%) categorized their job as “managerial/professional” (Table 1).
Respondent Demographics and Computer Use Information (N = 27)
All respondents used a computer at home, and 92% used a computer at work. Respondents used a computer at home a mean of 8.4 hr/wk and at work a mean of 19.6 hr/wk. Those who worked rated the importance of using a computer for their job as very important (88%) or somewhat important (12%; Table 1).
Types of Problems
Figure 1 shows the percentage of respondents who reported having at least one problem with each of the four equipment types. All but 1 of the respondents (96%) reported at least one problem with at least one of the equipment types. The chair and the keyboard caused problems for the highest percentage of respondents (85% and 88%), whereas the mouse and monitor caused problems for 69% and 32% of respondents, respectively (Figure 1).
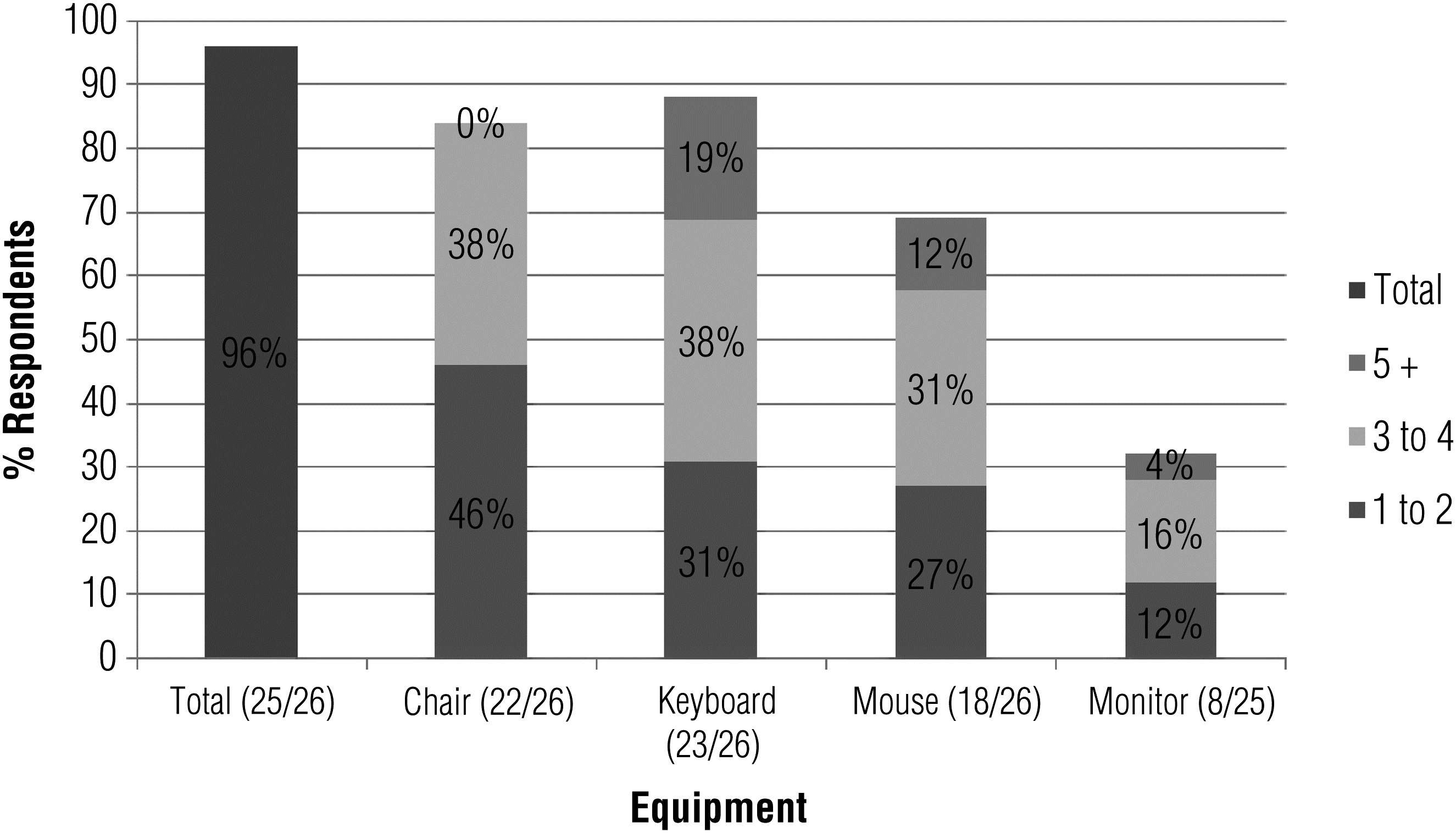
Percentage of respondents reporting one or more problems during computer operation.
Most respondents reported between one and four problems for each equipment type, although 19% and 12% of respondents with keyboard and mouse problems reported five or more problems. Table 2 shows the distribution of problems associated with each equipment type. Only five problems were chosen by more than half of the respondents, with “become very tired” (for keyboard, mouse, and monitor) making up three of those five. Otherwise, the problems respondents identified were widely distributed across all possible options. The perceived effect of computer problems on computer use was generally small (chair 58%, keyboard 42%, mouse 27%, monitor 17%), although a notable percentage of the respondents rated the degree to which problems affected computer use as considerable for the keyboard (27%) and mouse (23%).
Problems and Accommodation Strategies Reported for Each Equipment Type (N = 27)
Note. E = environmental accommodation; M = medication accommodation; P = performance accommodation; T = timing accommodation. Each accommodation strategy could be used for more than one problem.
Types of Discomfort
More than half of the 27 respondents reported equipment-related discomfort in the past month when using the chair (56%), keyboard (62%), and mouse (60%). Most respondents rated discomfort as mild (chair 26%, keyboard 12%, mouse 15%, monitor 19%) or moderate (chair 26%, keyboard 44%, mouse 30%, monitor 7%). Types of discomfort varied by equipment (Figure 2); the most common type of discomfort was stiffness, followed by fatigue and pain. Cold was reported primarily during keyboard and mouse use.
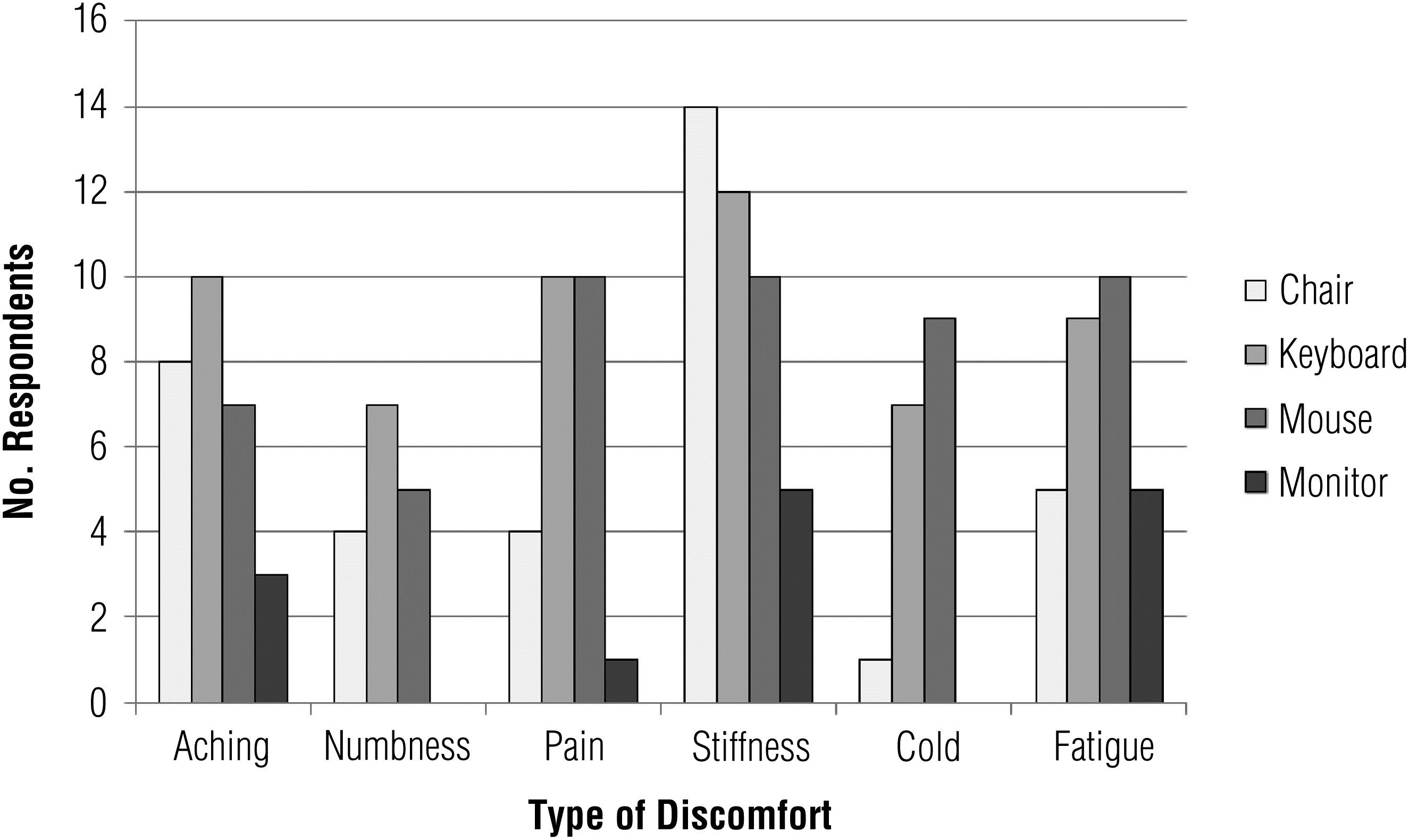
Number of respondents who experienced each type of discomfort for each equipment type during the previous month.
Accommodation Strategies
We categorized the list of accommodation strategies into four types: altering the environment, altering respondent performance, altering the timing of the task, and taking medication to help correct the problem. Table 2 lists the accommodation strategies respondents reported for each equipment type. As with the types of problems reported for each equipment type, respondents identified a wide variety of accommodation strategies. Only six of the strategies, however, were selected by more than half of the respondents reporting problems.
Discussion
In this sample of people with SSc, 96% reported at least one problem with at least one computer equipment type, with the keyboard and the chair causing problems for the highest percentages of respondents. In addition, more than half of the respondents reported experiencing discomfort associated with the chair, keyboard, and mouse in the past month.
Computer use typically requires the user to sit in a static, upright position for long periods. This frequently awkward position, coupled with the fatigue, muscle weakness, joint pain, and stiffness caused by SSc, may have resulted in the problems and discomfort respondents experienced while using a computer. Using a computer at work is essential for many people, including the respondents in this sample: 92% reported using a computer at work, and 88% reported computer use at work to be very important. For these respondents, the problems and discomfort they experience while using a computer may have affected their work performance and satisfaction.
The keyboard appeared to be the most problematic equipment type; 88% of respondents reported at least one problem with it, and more than half reported three or more problems (Figure 1). About one-third of the sample rated the effect of the keyboard on their computer use as considerable or high. The high number of keyboard problems is likely related to the effect of SSc on the hands. Skin thickening, digital ulcers, swollen fingers, and Raynaud’s phenomenon lead to limitations in finger flexion and extension (Sandqvist et al., 2004), which are needed for typing. Mouse use problems were reported by a smaller, but still notable, percentage of respondents. Using a mouse also requires some finger mobility but, more important, it is controlled by grasp, which is also affected in people with SSc (Poole, 1994). Given the nature of SSc and the problems these respondents reported, it is not surprising that keyboard and mouse use would be problematic.
Most respondents reported problems related to the chair, but they reported fewer problems and rated their effect on computer use as small. Chair problems were related to comfort and positioning. The results related to chair problems contrast with those from our study of computer use problems in people with rheumatoid arthritis, fibromyalgia, and osteoarthritis (Baker et al., 2009), in which the chair was the most common problem reported, followed by the keyboard and mouse. These differential findings suggest that SSc causes different types and degrees of computer use problems than other types of arthritis, namely problems with hand positioning and manipulation as compared with problems with proximal comfort and stability.
The specific accommodation strategies used by the respondents who reported problems were widely distributed, with no particular strategy being used by most respondents. Of the four strategy types (alteration in timing, performance, or environment and medication use) used for the keyboard, chair, and mouse, personal changes—alteration in performance or timing—were more commonly used than environmental changes or medication. Accommodation strategies that alter the environment, such as using adjustable or angled equipment or reconfiguring the environment to match worker characteristics, are considered to be the most effective when dealing with physical, manipulative, or postural issues (Weiss & Chan, 2008). These strategies, however, were used the least by respondents in this study, perhaps because of an unwillingness to change the work environment or a lack of knowledge about possible environmental strategies.
Implications for Occupational Therapy Practice
The results of this study suggest that people with SSc experience considerable problems and discomfort when using a computer; these problems could have a negative effect on their ability to use a computer at work or home. When evaluating a person with SSc, occupational therapists should discuss computer use to determine whether the person is experiencing problems. The following strategies may help people with SSc use their computers more effectively:
Occupational therapists working with this population should work with clients to identify environmental accommodations, rather than changes in performance, to reduce disability.
Interventions for people with SSc should focus first on the keyboard and mouse, whereas interventions for people with other types of arthritis should focus first on the chair.
Reconfiguring the workstation to match the anthropometrics of the worker can help reduce pain and fatigue.
Many alternative keyboards have fixed angles to reduce pronation, ulnar deviation, and wrist extension, and some keyboards can be adjusted to match the limitations of the hands. Keyboards with larger keys or keyguards may help reduce errors. Given the tendency for digital ulcers in this population, computer users who have SSc should use keyboards with a soft touch.
Users can be taught to use keyboard shortcuts to reduce mouse use. Using word processing functions such as “stickykeys,” which allows users to operate multiple keys simultaneously by pressing keys one at a time, can enhance the use of shortcuts and reduce mouse use. Many input devices are angled to reduce hand pronation and to place the wrist and fingers in neutral positions. An input device that eliminates grasping, such as a trackball, may also reduce fatigue.
Our sample reported problems with cold, particularly during mouse use, attributable to Raynaud’s phenomenon. Heated keyboards and mice can address this issue.
To address the fatigue reported by our sample and in other studies (Sandqvist et al., 2010; Sandusky, McGuire, Smith, Wigley, & Haythornthwaite, 2009), practitioners can provide computer operators who have SSc with education on energy conservation techniques and software reminders to take regular, short breaks.
Limitations
This needs assessment had limitations. Because SSc is rare, we were able to obtain only a small sample of respondents, limiting the ability to use statistical inference testing and the applicability of the results to the general population. Additionally, we did not examine factors such as workstation setup, typical length of time using the computer, and anthropometrics, all of which may have affected computer use in these respondents; our goal was to assess the basic problem areas, not their underlying causes. The results of this study suggest that further research in this area to understand underlying causes is necessary to develop appropriate interventions.
Conclusion
Because computer use is an important part of many occupations, the people who use computers at work need to have as few obstacles as possible to be productive and satisfied. This needs assessment is the first step toward an understanding of computer use by people with SSc, and the results demonstrate that this population experiences problems and discomfort related to use of computer equipment. These problems may lead to lowered efficiency, frustration, and dissatisfaction with their job. Occupational therapy practitioners who serve clients with SSc should consider interventions designed to reduce impairments associated with computer use, including computer workstation evaluations and changes. Practitioners should stress environmental accommodation strategies as a method of reducing the pain and discomfort experienced during computer use, as opposed to the personal strategies that many people with SSc appear already to use. Further research with a larger and more diverse sample needs to be done on computer use problems experienced by people with SSc to develop focused interventions that can improve computer use and work productivity.
Footnotes
Acknowledgments
This work was supported in part by a Health Professional Investigator Award from the American College of Rheumatology Research and Education Foundation to Janet L. Poole.