
Abstract
In recent years, U.S. home health care has become a topic of increasing research and interest. The interest marks current efforts to move health care services for the management of chronic conditions from institutions and hospitals to the community, with an increasing emphasis on outcomes (Eastaugh, 2001; Hughes & Renehan, 2005). In addition, the importance of cost-effective care for the aging population has fueled these efforts (Eastaugh, 2001).
In response, home care services have grown (Hughes & Renehan, 2005). Most U.S. home health care services are funded by Medicare (National Association for Home Care [NAHC], 2008) and have been shown to be cost effective (NAHC, 2008); to reduce long-term institutionalization (Pande, Laditka, Laditka, & Davis, 2007), mortality (Rizzi et al., 2009), and hospitalization (Rizzi et al., 2009; Shaughnessy et al., 2002); and to improve health status (Shaughnessy et al., 2002). Medicare home care outcomes are currently monitored via the Outcomes and Assessment Information Set (OASIS; NAHC, 2008).
Occupational therapy is one type of service that is valuable in home health care. Several studies have indicated the prevalence of occupational performance problems among older adults residing in the community (Classen, Mkanta, Walsh, & Mann, 2005; Gitlin, Mann, Tomita, & Marcus, 2001; Mann et al., 2005). Despite a prevalent need for services, evidence has suggested that occupational therapy may be underused in home care (Krafft, 2006; Toto, 2006). For instance, only 8.5% of U.S. occupational therapists work in home and community practice (American Occupational Therapy Association [AOTA], 2006), compared with 16% in Canada (Canadian Association of Occupational Therapists, 2007). Occupational therapy was 3% of total Medicare home health spending in 2001, compared with 12% in skilled nursing facilities (Metzler, 2003). Additionally, in 2008 the ratio of physical therapy to occupational therapy full-time equivalents was approximately 4:1 in home health (NAHC, 2008) but <2:1 in skilled nursing facilities (Horowitz, 2002b).
Despite the need for occupational therapy in home health and its possible underutilization, no recent known study has explored the topic. Therefore, my primary purpose in this study was to examine literature addressing the current practice of occupational therapy in U.S. home health. My secondary purpose was to identify factors related to the current utilization of occupational therapy in home health. The study focused on literature published from 2000 to 2009 that could reasonably be applied to Medicare home health care, using these specific research questions:
What is known from the existing literature regarding occupational therapy utilization and practice in home health, including
What types of articles and studies exist, and what is their general content?
What characterizes occupational therapy interventions and practice in home health?
What factors might be related to current use?
What gaps in knowledge exist, and what potential research and practice recommendations can be made?
Method
Scoping Review
The aim of a scoping review is to examine literature addressing general topic areas with the purpose of identifying research gaps and making recommendations for future research. In contrast to a systematic review, a scoping study covers broad topic areas and does not evaluate the quality of evidence.
Literature Search
First, I entered the term occupational therapy into electronic key word searches for the journals Home Healthcare Management and Practice (2000–2009), Home Healthcare Nurse (2000–2009), and Home Healthcare Services Quarterly. Next, I conducted electronic database searches of OT Search (accessed at www.AOTA.org), EMBASE, CINAHL, and AGELINE using the key words occupational therapy plus practice analysis, practice patterns, home health, home care, service use, utilization, or health services research. I conducted an electronic search of PubMed using the MeSH terminology of occupational therapy plus home care services, utilization, practice analysis, or health services research. These searches produced approximately 2,100 potential articles. Article titles and abstracts were scanned for relevance according to the criteria discussed in the sections that follow.
Inclusion and Exclusion Criteria
To be included, the article had to
Mention home care or home health services or use home health or home care as a key word,
Be applicable to rehabilitation practices under Medicare home health services, and
Include occupational therapy as a major focus.
Because initial results produced only one article specifically focused on Medicare-based occupational therapy home health services, I expanded inclusion criteria to include some non–peer-reviewed articles that might lend insight into practice and utilization trends. AOTA publications (OT Practice Magazine, Special Interest Section Quarterly Newsletters) appeared to be most relevant or appropriate and were included to get a perspective on actual practice.
Articles were excluded if they
Focused on community-based practice, outpatient therapy, prevention, or home visits conducted from an inpatient setting;
Concerned pediatric-, adolescent-, or psychiatric-only services;
Were a book, book review, or e-newsletter;
Provided psychometric data for an evaluation or assessment; or
Reported utilization without describing factors related to access or utilization.
Of the original 2,100 articles, 65 met all inclusion and exclusion criteria.
Coding and Analysis
To answer Research Question 1a, I coded literature according to the descriptive variables of funding for services (Medicare, Medicaid, managed care, etc.), peer-review status, and type of article (experimental research, review, professional practice article, etc.). For Research Questions 1b and 1c, I noted general outcomes, conclusions, and topics of each article. For Research Question 1b, literature was coded by type of occupational therapy intervention. Specific interventions were grouped by similarities, and each group was given a category name.
To add support and depth to Research Questions 1a–c, I then analyzed the literature qualitatively to identify factors in occupational therapy practice and utilization. Qualitative analysis began with reading for content and coding emerging themes with first-level codes. A list of codes and code definitions was created, and a researcher experienced in qualitative methods coded portions of documents using the definitions to establish reliability. A coding sort was conducted to merge similarly coded blocks of text, and data were reduced to distill essential concepts and information. An additional researcher experienced in qualitative methods examined interpretations of results for consistency of interpretations. Concepts and themes were organized and displayed in paragraph form. Results from all areas were synthesized to identify gaps in knowledge and identify potential research and practice recommendations (Research Question 2).
Results
Descriptive Analysis
Most of the literature specifically mentioned or referenced Medicare home health practice. Articles fell into two basic types: research (21 articles; 32%) and professional practice (44 articles; 68%). Most research was experimental or quasi-experimental and did not specifically reference a funding source. Most practice articles were not peer reviewed and dealt with practice issues, with some mentioning Medicare practice specifically. Therefore, most of the Medicare literature consisted of non–peer-reviewed professional practice articles and only one research article.
General Content of Articles
Research Articles.
Research articles addressed four major topics: environmental and caregiver interventions for people with dementia, multicomponent home interventions and environmental modifications, general occupational therapy interventions, and occupational therapy practice patterns and role. Supplemental Table 1 (available online at http://ajot.aotapress.net; navigate to this article, and click on “supplemental materials”) summarizes each article.
The environmental and caregiver interventions for people with dementia consist mainly of Environmental Skill Building (ESB) program research (Gitlin, Corcoran, Winter, Boyce, & Hauck, 2001). The ESB program is a 6-mo home program consisting of six occupational therapist visits and three phone contacts using specifically trained occupational therapists providing services to caregivers of people with Alzheimer’s disease. Outcomes reduced problematic behaviors and declines in activities of daily living (ADLs) and instrumental activities of daily living (IADLs; Gitlin, Corcoran, et al., 2001) and increased caregiver ability while reducing upset (Gitlin et al., 2003). Many outcomes were sustained at 12 mo (Gitlin, Hauck, Dennis, & Winter, 2005), and factors predicting success and barriers were identified (Chee, Gitlin, Dennis, & Hauck, 2007). Other authors used shorter interventions, demonstrating similar outcomes in reduced caregiver burden and stress (Dooley & Hinojosa, 2004; Holmes, 2000; Sheldon & Teaford, 2002) and increased quality of life, affect, self-care status, and activity frequency (Dooley & Hinojosa, 2004).
Gitlin, Winter, et al. (2006; Gitlin, Winter, Dennis, & Hauck, 2008) offered a 6-mo program focused on multicomponent home interventions using four 90-min occupational therapist visits and three phone contacts. Outcomes indicated reductions in mortality risk, difficulty with ADLs and IADLs, fear of falling, and home hazards and improvements in self-efficacy and use of adaptive strategies. Most outcomes were sustained at 12 mo, and some factors predicting benefits were identified. Stark (2004) also demonstrated improved occupational performance and satisfaction with the ability to perform everyday activities after an occupational therapy home environment assessment and follow-up visits, with results sustained at 2 yr (Stark, Landsbaum, Palmer, Somerville, & Morris, 2009). McNulty, Johnson, Poole, and Winkle (2003) provided factors predicting success in implementing home safety changes.
Other interventions were described in a documentation analysis in a Medicare home health agency indicating improvements in lower-extremity dressing, toileting, and walking with use of occupational therapy (Matteliano, Mann, & Tomita, 2002). Cohen and Schemm (2007) demonstrated increased life satisfaction and taking on new life roles after an eight-visit occupational therapy home intervention among people with spinal cord injury.
Many studies used occupational therapy in a prescribed role and involved specific instructions for each of the indicated visits. Only one study (Matteliano et al., 2002) examined outcomes from current Medicare home health practice. In addition, much of the research focused on adaptation to and compensation for disability, with few remediation interventions.
Research on the role and practices of occupational therapists in home health consists of both health services research (Boutin-Lester & Gibson, 2002; Toth-Cohen, 2000) and descriptive research and survey data from AOTA (2006). General methods can be found in Supplemental Table 1, and content and outcomes are discussed in the Actual Practices of Home Health Occupational Therapists section.
Professional Practice Articles.
Articles addressed four topics: occupational therapy interventions for specific conditions/situations, practice issues, policy, and case reports, which can be found in Supplemental Table 2 (available online at http://ajot.aotapress.net; navigate to this article, and click on “supplemental materials”). Article content was grouped into subtopics, which are described in the Qualitative Analysis section.
Occupational Therapy Intervention
Of the 65 articles reviewed, 18 research articles and 41 professional practice articles indicated a role for occupational therapy in home health by referencing at least one type of intervention. The 6 ESB articles were counted only once in this analysis because multiple publications referenced different aspects of the same study. Similarly, the four multicomponent home intervention and two home modification studies were also counted only once. This grouping meant that a total of 9 research studies were counted in the analysis. The 50 articles indicating some role for occupational therapy generated 49 intervention topics.
Supplemental Table 3 (available online at http://ajot.aotapress.net; navigate to this article, and click on “supplemental materials”) displays the interventions and the authors referencing each, and Figure 1 summarizes all interventions. Using terminology from the Occupational Therapy Practice Framework: Domain and Process (2nd ed.; AOTA, 2008), interventions were categorized into seven topics. Topics are discussed here in order of most to least frequently cited.
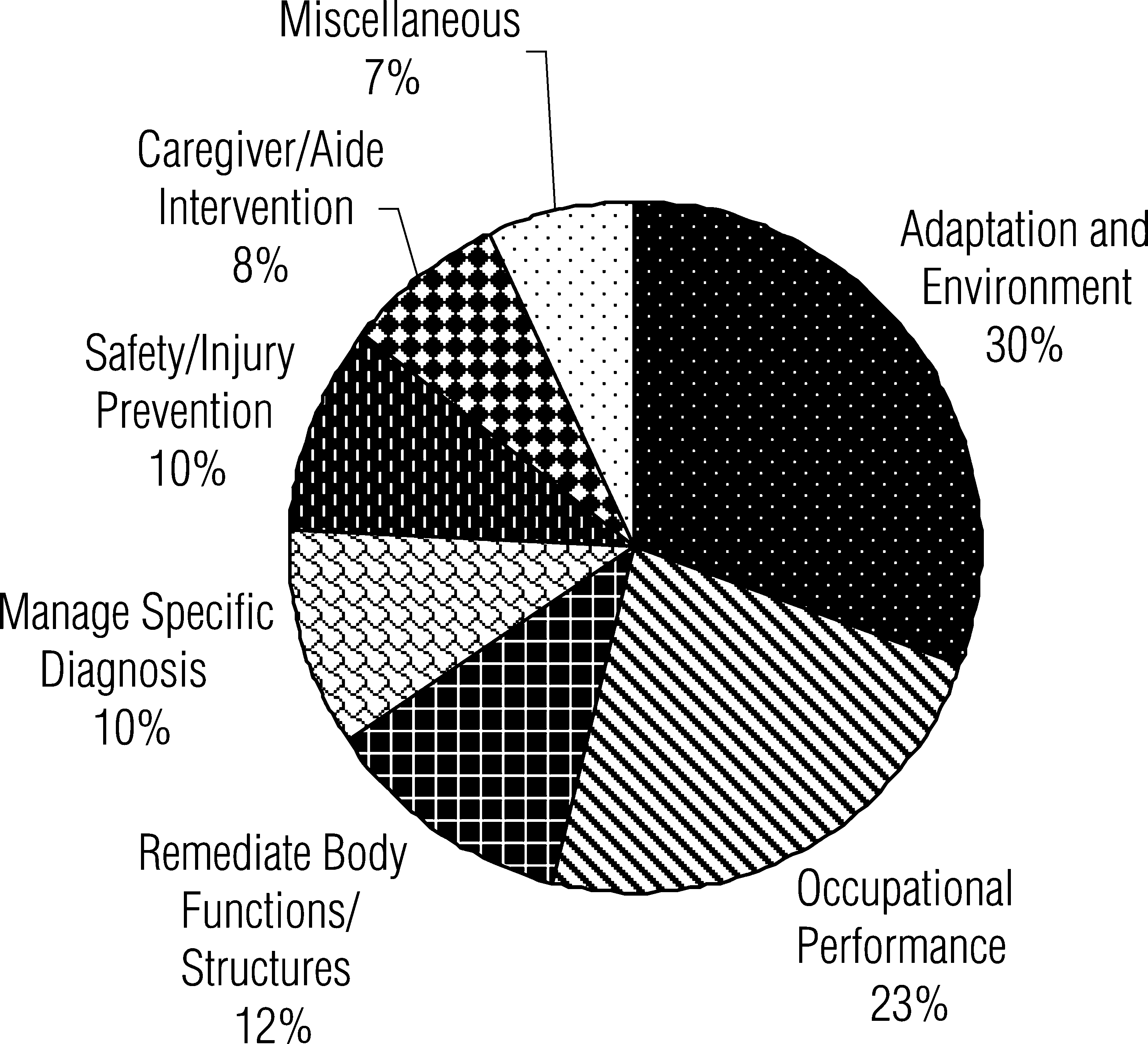
Occupational therapy interventions referenced in U.S. home health literature, 2000–2009 (N = 50 articles). Seven major intervention topics were found in the literature, indicating a role for occupational therapy in home care that emphasizes environment, adaptation, and occupation.
Adaptation and environment were the interventions most frequently referenced in the literature; they included adaptive devices, adaptive strategies and methods, and home and environmental modifications. Occupational performance was the second most referenced intervention; most authors discussed ADLs and IADLs in general or specific occupations, including medication management, community mobility, reestablishment of daily routines, and meal preparation.
Remediation of body functions and structures and performance skills was much less referenced and included (e.g., improving endurance and cognition and managing pressure ulcers). Managing specific diagnostic conditions was also indicated, with most literature focused on dementia management. Other conditions mentioned include stroke, mental health, and low vision. Safety and injury prevention, caregiver interventions, and home health aide collaboration were also represented in the literature.
Interventions not classified under other topics were considered miscellaneous, containing the fewest number of total references. Many of these interventions were psychosocial in nature.
Considering all specific interventions, ADLs and IADLs were the most frequently cited. Within this category, medication management was the most frequently cited single ADL or IADL, although the total citations were relatively low. Other specific interventions, in order of most frequently cited to least frequently cited, were home and environmental modifications, adaptive devices and equipment, home safety assessment and teaching, and adaptive strategies.
Qualitative Analysis
Factors Involved in Utilization
Three subtopics emerged here, including justification of need for services, reasons for current use, and suggestions for improving use.
Justification of Need for Services.
The literature justifies the need for services on the basis of two factors: (1) limiting inpatient hospitalizations and encouraging management at home and (2) addressing an increasing emphasis on outcomes. First, inpatient settings no longer provide in-home assessments as part of discharge, leaving a need to evaluate safety and equipment in the home (Sevigny, 2000). Siebert (2007) acknowledged that IADLs are frequently not addressed in inpatient settings. Fagan, Van Oss, Cabrera, Olivas De La O, and Vance (2008) acknowledged that the prevalence of people unable to manage conditions at home has increased. Miller (2003) noted the potential cost-effectiveness of occupational therapy in home safety to reduce injury. Second, Toto (2006) and Siebert (2005) noted that 23 of the 41 OASIS–C outcomes related directly to ADL and IADL performance and opportunities for occupational therapy services. Siebert (2006) noted an additional six OASIS–C outcomes that occupational therapy can address.
Reasons for Current Use.
One explanation for the underuse of occupational therapy was decreased awareness of services that occupational therapy can provide (Olivas De La O, 2008b, Siebert, 2005; Toto, 2006). Also, workforce shortages of occupational therapists might result in people from other disciplines filling in for occupational therapists (Olivas De La O, 2008b). Because most resources in home health rehabilitation focus on physical therapy (Krafft, 2006; Metzler, 2003), occupational therapy is often used only if the agency has not met the targeted number of rehabilitation visits (Barnes & Frock, 2003; Olivas De La O, 2008b). Currently, inclusion of occupational therapy depends on decisions made by other team members (Toto, 2006), noting that physical therapists often evaluate the need for occupational therapy (Sevigny, 2000). Krafft (2006) suggested that the justification for this evaluation is a common belief of agencies that physical therapy can address ADLs.
Other authors related the utilization patterns to Medicare policies. Toto (2006) and Metzler (2000, 2003) reinforced that unlike physical and speech therapy, occupational therapy cannot establish patient eligibility for home health services under Medicare. Analysts believe that if occupational therapy were made a qualifying service, a significant number of people would need only occupational therapy, increasing the cost of Medicare home health services (Metzler, 2003).
Suggestions for Improving Use.
One suggestion is to influence Medicare policy by showing that including occupational therapy minimally increases the number of people qualifying for home care, that increased occupational therapy would be cost-effective, or both (Metzler, 2000). To increase client referrals, Olivas De La O (2008b) and Costa (2006) suggested using ADL and IADL deficits indicated by an OASIS–C assessment to trigger an occupational therapy evaluation. Metzler (2009) described new proposed legislation that would allow occupational therapy to complete the initial OASIS–C if a qualifying discipline (physical therapy, skilled nursing, speech–language pathology) was on the physician order. Barney (2001) additionally suggested marketing occupational therapy within and outside home health agencies. Partnerships among AOTA, NAHC, and home health associations of other disciplines have formed to increase use of occupational therapy for Medicare home health beneficiaries (Fagan et al., 2008). In response to workforce shortages, occupational therapy assistants may also be used (Siebert, 2006; Steele, 2006).
General Practice Patterns
Three subtopics were evident: (1) actual practices of home health occupational therapists, (2) reasons for current practices, and (3) suggestions for improving practices.
Actual Practices of Home Health Occupational Therapists.
Several authors agreed that little research exists on U.S. home health occupational therapy practice (Boutin-Lester & Gibson, 2002; DePalma, 2006; Gitlin & Chee, 2006; Toto, 2006). The studies that do exist have pointed to a lack of meaningful occupations in practice (Boutin-Lester & Gibson, 2002; Toth-Cohen, 2000). Boutin-Lester and Gibson (2002) researched practice patterns of home health occupational therapists, noting most interventions were exercises, with only 1 participant reporting interventions incorporating occupation and the home setting. Toth-Cohen’s (2000) study added that incorporating the patient, family, and home environment during home care was a major shift for occupational therapists from their typical work setting. Time management, purposeful activity, community reentry, teaching caregivers (Olivas De La O, 2008a), and home modifications (Pynoos, Sanford, & Rosenfelt, 2002) were often overlooked. Accounting for this oversight was a decreased emphasis on client priorities and collaboration (Boutin-Lester & Gibson, 2002; Gitlin & Chee, 2006). As a result, clients were often dissatisfied with discharge (Boutin-Lester & Gibson, 2002).
The AOTA (2006) workforce survey added further depth. Compared with the national sample, occupational therapy home health practitioners were more likely to work <30 hr/week (30.8% vs. 22.4%) and to be paid for their work as contractors (32.3% vs. 25.9%). In addition, they were more likely to have direct client intervention as their primary role (94.4% vs. 83.1%) and less likely to have indirect or administrative responsibilities as their primary role (4.5% vs. 8.0%).
Reasons for Current Practices.
Many authors discussed health care system policies and procedures as factors in current occupational therapy practice. Fagan et al. (2008) acknowledged that most home health occupational therapy is provided after acute hospitalizations and is directive and prescriptive (Gitlin & Chee, 2006). Toth-Cohen (2000) offered that the reasoning of home health occupational therapists relates to their roles in institutional and cultural structures in health care and the dominance of the medical model (Siebert, 2003). Siebert (2003, 2005) added that occupational therapy interventions often focus on remediating body structures and functions. In addition, given that many occupational therapists in home care are part-time (AOTA, 2006) per diem employees (Toto, 2006) or contract therapists (Raptosh, 2003), coordination of care with other professionals is difficult (Toto, 2006).
Suggestions for Improving Practices.
Toth-Cohen (2000) suggested that comprehensive training programs may be necessary to transition into home care. Therapists should focus on areas that clients report as problematic: serving as consultants, helping clients solve problems, and offering strategy choices (Gitlin & Chee, 2006; Vance & Siebert, 2009). The focus should be on altering activity demands of ADLs and IADLs by means of assisted devices, environmental interventions, or task simplification (Siebert, 2003), emphasizing a balance between remedial and adaptive approaches (Merryman, 2006; Vance & Siebert, 2009). Ultimately, therapy should lead to a change in client health status rather than merely a change in skill or measurable body function (Siebert, 2005). Last, preventing deterioration and stabilization are needed, especially for people with declining conditions (Siebert, 2005). Other recommendations include partnering with home health aides (O’Sullivan, 2003) and providing home health internship programs for new occupational therapy graduates (McCaul, 2005).
Discussion
Summary of Current Practices
The literature indicates a comprehensive role for occupational therapy in home health, with ADLs and IADLs the most frequently mentioned intervention. The trend in describing occupational therapy’s role in home health appears to be moving toward compensatory and contextual approaches and away from remediation. This trend has been reinforced in research studies, which differ from professional practice articles by further emphasizing adaptation and environment while decreasing focus on remediation, which might suggest a practice trend that is unique to home health occupational therapy. Notable is the inclusion of people with dementia and caregivers as part of home health care treatment, perhaps because of the more favorable reimbursement (Dooley & Hinojosa, 2004). Given the limited reference to self-management and chronic disease management (Vance & Siebert, 2009) as a role for occupational therapists, the current literature does not yet reflect health care initiatives for chronic care management in the community.
Research in this area appears modest in quantity. Although determining the quality of research and outcomes in this area was not the focus of this study, studies involving specific home interventions (e.g., Gitlin, Corcoran, et al., 2001; Gitlin, Winter, et al., 2006) and the general practice of occupational therapy under Medicare (Matteliano et al., 2002) appear to demonstrate promising outcomes.
The need for increased occupational therapy services in the home is apparent. This topic is frequently discussed in professional practice articles. The presence of only one study of Medicare-based home health occupational therapy suggests that it may not be a well-known or common area of practice. In addition, the potential concerns regarding the cost of including occupational therapy as a qualifying service for home health under Medicare further indicate unmet needs in the aging and homebound community. The extent of the potential underutilization and need for services is suggested as a primary area of future research.
Proposed Factors in Current Utilization and Practice of Occupational Therapy in Home Health
Scarcity of Research in This Area.
As discussed, research is scarce, especially in the area of Medicare home health. The research that does exist uses occupational therapy in a role that is different from traditional Medicare-based home care practice. Research involving occupational therapy practice in Medicare home health services is recommended (including a systematic review analyzing the quality of current research), as well as basic research on utilization of and access to occupational therapy services in home care.
Current Occupational Therapy Workforce.
Occupational therapists in home health are more likely to work part time or as contractors and have less contact with other team professionals. Also, workforce shortages might cause other disciplines to perform duties traditionally reserved for occupational therapists. These factors suggest an absence of occupational therapy input on the treatment team that might affect its utilization. This problem might be addressed by starting fieldwork programs and internship programs (McCaul, 2005) and developing training and research partnerships with area universities. Agencies should attempt to integrate and include part-time or contract occupational therapists on the treatment team. In addition, occupational therapy assistants can be used more often (Siebert, 2006; Steele, 2006).
Lack of Occupation-Based Treatment in Home Health Care.
Current occupational therapy interventions might not be in the basic domain of ADLs or IADLs or incorporate the patient, caregiver, and environment, even though research indicates that they should do so (Gitlin, Winter, et al., 2006; Gitlin, Corcoran, et al., 2001). Agency orientation and training programs specific to home health occupational therapy may be limited. Consequently, home care practice may be similar to institutions in which occupational therapists receive more clinical training, as is evident by the focus on remediation of impairments. Agencies might then be less likely to refer to occupational therapists if they cannot address ADL and IADL outcomes important to home care.
I propose that OASIS outcomes in ADLs and IADLs delineate a clear role for occupational therapy. Interventions targeting ADLs and IADLs might address physical and social contexts, body functions and structures, performance skills and patterns, and activity demands (AOTA, 2008) while using a balance of remedial and adaptive approaches. Home care agencies should routinely provide orientation and training for occupational therapists, including areas for intervention and outcomes. Additionally, research determining occupational therapy practice patterns and outcomes is highly warranted to support this study’s preliminary findings.
Limited Knowledge of Occupational Therapy in Home Care.
This lack of knowledge might reflect or be a cause of current utilization. Limited knowledge would in turn limit the expectations for occupational therapy in delivering outcomes. Referring entities might not know to refer to occupational therapy for a specific concern, nor would practitioners be held accountable for delivering outcomes in basic areas of occupation.
As suggested here, scores from OASIS ADL and IADL measures could be a simple way to demonstrate the need for and role of occupational therapy services. Increased knowledge of occupational therapy might be accomplished by clarifying the role of occupation-based practice focused on outcomes. Encouraging professionals to acquire full-time or leadership positions within agencies might also have a positive effect on knowledge and use of occupational therapy.
Medicare Policy Limiting Occupational Therapy as a Qualifying Service.
The existing policy may indeed limit services for people who need occupational therapy. Inclusion of occupational therapy is often dependent on the decisions of other team members, such as physical therapists. Given the lack of knowledge of occupational therapy, whether appropriate referrals are made is unclear. Again, I recommend that scores from OASIS ADL and IADL measures identify the need for occupational therapy. The proposed legislation allowing occupational therapists to complete the initial OASIS (Metzler, 2009) might increase occupational therapy utilization by reducing reliance on non–occupational therapy gatekeepers. Further research is needed to determine the direct cost of a change in policy, as well as the potential cost-effectiveness of home occupational therapy services.
Implications for Occupational Therapy Practice
This review of articles in the area of home health practice has the following implications for occupational therapy practice:
Occupational therapy interventions in home health should fall into the basic domain of ADLs and IADLs; can use both a remediation and compensation approach; and should involve the patient, caregiver, and environment.
Occupational therapists working in or desiring to work in home health will likely need to provide education on the role and scope of occupational therapy to potential home health clients, physicians, home health agencies’ administration, and staff within home health agencies who complete the OASIS and serve as gatekeepers for service provision
Education regarding the role and scope of occupational therapy in home health might include ability to address ADLs and IADLs; ability to address OASIS outcomes in ADLs, IADLs, and other areas; ability to provide remediation and compensation interventions; ability to provide interventions to the patient, caregiver, and environment; and ability to collaborate with and provide supervision and education to home health aides.
Occupational therapists should be encouraged to seek work in home health settings to attempt to meet unmet client needs. Therapists working part-time or per diem could also seek to increase their hours.
Study Limitations
This study was limited by the types of articles reviewed, which included both peer-reviewed and non–peer-reviewed literature. Some appropriate articles may also have been missed. The small number of studies and articles for certain topics made it difficult to draw well-supported conclusions. Consequently, many conclusions drawn here are speculative and require additional research.
Conclusion
In this scoping review, I analyzed 65 publications regarding current occupational therapy utilization and practice in home health. Results indicate that research in this area, although scarce, looks at a variety of typologies and efficacy measures. However, utilization and practice patterns of occupational therapy in home health do not appear consistent with research. Factors explaining current utilization and practices were identified, and results indicate that system challenges may limit the utilization and practice of occupational therapy to deliver expected outcomes in home health. Limitations included study methodology, quantity and quality of articles reviewed, and interpretations of results. Hence, future studies systematically reviewing current evidence and providing research on occupational therapy utilization, practice patterns, and outcomes in home health are warranted to strengthen this study’s preliminary results.
Supplemental Material
Supplementary material for Current Occupational Therapy Publications in Home Health: A Scoping Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2012.003566.pdf for Current Occupational Therapy Publications in Home Health: A Scoping Review by Daniel G. Craig in The American Journal of Occupational Therapy
Footnotes
Acknowledgment
I thank Marcia Finlayson at the University of Illinois at Chicago for her support, guidance, and expertise during the study.
*
Indicates studies that were reviewed for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.