
Abstract
Stroke occurs once every 40 s in the United States, resulting in 795,000 new strokes per year and making stroke the leading cause of long-term disability (Lloyd-Jones et al., 2009). Two-thirds of stroke survivors experience upper-extremity (UE) impairment (Rosamond et al., 2008), which can lead to difficulty performing meaningful occupations (Trombly & Ma, 2002). UE motor function after stroke improves in response to activity-based movement therapy (Richards, Stewart, Woodbury, Senesac, & Cauraugh, 2008). This improvement has been linked to neuroplastic change (Cramer & Bastings, 2000; Johansson, 2011; Liepert et al., 1998; Nudo, 2003).
Occupation-based intervention is a form of activity-based therapy consisting of client-directed occupations that match client-identified goals (American Occupational Therapy Association [AOTA], 2008). Principles of occupation-based intervention (Trombly & Ma, 2002) appear highly concordant with principles of interventions to drive neuroplastic change (Kleim & Jones, 2008; Nudo, 2003). Therefore, occupation-based intervention could conceivably result in measurable neuroplastic change. However, no studies have directly measured neuroplastic change in relation to occupation-based intervention.
Thus, the purpose of this case study was to use transcranial magnetic stimulation (TMS) to investigate the nature and extent of neuroplastic change associated with occupation-based intervention and recovery of UE motor function in 1 research participant with chronic stroke. Researchers have made extensive use of TMS in measuring neuroplastic change associated with interventions to promote UE motor recovery (Bastings, Greenberg, & Good, 2002; Liepert et al., 1998; Rossini et al., 1998). By conducting the first investigation of neuroplastic change associated with occupation-based intervention, we can establish further evidence of how occupation-based intervention affects mechanisms underlying functional recovery after stroke.
Method
Research Design
This single-subject case report reflects a pretest–posttest design. We obtained informed consent per our institution’s Institutional Review Board mandates. Inclusion criteria included having had one stroke >1 yr before enrollment (i.e., chronic status). We structured exclusion criteria primarily to minimize risks associated with TMS and to control for potential confounding variables. Exclusion criteria included (1) history of head injury with loss of consciousness; (2) seizures; (3) severe alcohol or drug abuse; (4) severe psychiatric illness interfering with participation in the study; (5) cognitive deficits severe enough to preclude informed consent; (6) ferromagnetic material near the brain; or (7) cardiac or neural pacemakers. To approximate the treatment frequency and duration typically mandated by outpatient rehabilitation reimbursement entities, we conducted 55-min intervention sessions, 3 times per week for 5 wk. An occupational therapist with graduate education in rehabilitation sciences and 26 yr of clinical experience with neurological populations provided the intervention. The therapist had no involvement with administration of assessments.
Participant
The participant, “Will,” experienced a right middle cerebral artery infarct resulting in left hemiparesis. Will volunteered for our study in response to a referral from his attending rehabilitation physician. On enrollment in the study, Will was 55 yr old. His first and only stroke occurred 15 mo before enrollment. After his stroke, he received standard inpatient and outpatient occupational therapy. He completed his last round of outpatient therapy 4 mo before enrollment. He had right-hand dominance before and after his stroke. With cueing, Will used his affected UE as a gross active assist. Visual inspection revealed limited range of motion in all joints, limited isolated finger movements, and flexor synergy. He also had a Modified Ashworth Scale (Platz, Eickhof, Nuyens, & Vuadens, 2005) score of 2. On the basis of his Fugl-Meyer Assessment (FMA; Gladstone, Danells, & Black, 2002) score (Table 1), we classified his hemiparesis as moderate.
Results on the Fugl-Meyer Assessment (FMA) and Stroke Impact Scale (SIS)
Instruments
Behavioral assessments.
We completed three assessments of motor performance: the FMA, the Stroke Impact Scale (SIS; Carod-Artal, Coral, Trizotto, & Moreira, 2008; Duncan, Lai, Bode, Perera, & DeRosa, 2003; Duncan et al., 1999), and the Canadian Occupational Performance Measure (COPM; Law et al., 1998). The FMA is a quantitative measure of motor recovery, balance, sensation, coordination, and speed. Extensively applied with stroke clients, it is based on the principle that motor recovery occurs in a predictable progression (Gladstone et al., 2002). The FMA has high interrater reliability (.886–.984) and test–retest reliability (.99; Duncan, Propst, & Nelson, 1983). We administered the UE motor control portion of the FMA, which has a possible total score of 66 points.
The SIS is a participant self-report that uses a Likert scale to assess hand strength, function, mobility, activities of daily living and instrumental activities of daily living, memory and thinking, communication, emotion, and participation. It also includes a percentile scale to assess the participant’s perception of how much recovery has occurred. It has reliable psychometric attributes, including reliability (correlation coefficients ranging from .70 to .92) and validity (correlation coefficients ranging from .82 to .84). We administered all portions of the SIS.
The COPM is a subjective quality-of-life measure that uses a 10-point scale on which clients score their own occupational performance, as well as their satisfaction with performance, in relation to as many as five self-selected tasks. In this way, the COPM reveals tasks that therapists may use to support clients’ return to meaningful roles. The COPM is completed in an interview format and is designed to create a client-centered intervention. With a population with stroke, the COPM had high test–retest reliability for performance scores (.89, p < .001) and satisfaction scores (.88, p < .001), and its discriminant validity has been established (Cup, Scholte op Reimer, Thijssen, & van Kuyk-Minis, 2003). When working with people living in the community, McColl, Paterson, Davies, Doubt, and Law (2000) found that the COPM had moderate construct validity and high community utility. We administered all portions of the COPM.
Neurophysiological assessments.
For this project, we used TMS to measure changes in resting motor threshold (rMT) and cortical motor map. TMS delivers noninvasive brain stimulation via a handheld coil that uses a rapidly changing magnetic field to activate pyramidal neurons. The rMT is a measure of neuronal membrane excitability. In this study, we defined rMT as the minimum TMS intensity (measured to the nearest 1% of maximum stimulator output) required to elicit motor-evoked potentials (MEPs) of ≥50 μV in at least 5 of 10 consecutive trials (Rossini & Caremai, 1988). Cortical motor mapping measures cortical representation of a given muscle (Liepert et al., 1998; Wassermann, McShane, Hallett, & Cohen, 1992). To measure cortical map change, we calculated change in the normalized map volume (nMV) and the center of gravity (COG). The nMV is a simple measure of the spread of the motor representation over multiple scalp sites. The COG is an average of all active location vectors, each weighted by the MEP amplitude at that location (Wassermann et al., 1992). If there are N locations, the COG is calculated by
for the x coordinate (COGx) and similarly for the y coordinate (COGy; Liepert et al., 1998).
To perform TMS assessments, we placed monitoring electrodes over the belly of the extensor digitorum communis (EDC) muscles bilaterally. We selected the EDC muscle because it is the primary effector of finger extension and has been extensively studied in multicenter longitudinal studies evaluating the effects of intervention in stroke motor recovery (Sawaki et al., 2008). To ensure reproducibility of electrode placements at different time points, we created a plastic film template of the dorsal surface of the participant’s forearm. We continuously monitored relaxation of the target muscle by means of visual electromyographic (EMG) feedback and delivered TMS using a Magstim 200 stimulator fitted with a figure-eight coil (Magstim, Whitland, Dyfed, Wales). With the coil at the frontoparietal region optimal to elicit reliable MEPs on the contralateral EDC muscle, we set TMS intensity at 110% of rMT and delivered stimulation at a rate of 0.2 Hz to various sites on the scalp using a latitude- and longitude-based coordinate system. In accordance with this system, the participant wore a tight-fitting, flexible cap (Electro Cap International, Eaton, OH) premarked with a 1-cm coordinate grid referenced to the vertex (Liepert et al., 1998).
We delivered 10 stimuli at each grid site until we encountered sites at which stimulation elicited no motor response. Such sites constituted the borders of the motor map. The EMG response to each TMS pulse was amplified and filtered (band-pass 10 Hz–1 kHz) using an isolated bioelectric amplifier (World Precision Instruments, Sarasota, FL), digitized (3-kHz sampling rate) for online display, and recorded for offline analysis. We then calculated the average MEP amplitude of every series of 10 stimuli offline.
Descriptive assessments.
The treating therapist assessed and documented descriptive data about the participant’s performance throughout the intervention as it related to Will’s goals. She formatted these data into notes using the categories of subjective, objective, assessment, and plan (i.e., SOAP notes). She also informally logged client and family comments regarding occupation during the intervention period. This process of data collection was consistent with the occupational therapy process (AOTA, 2008).
Intervention
An occupational therapist who had no involvement in administering baseline and postintervention assessments delivered the intervention. To maintain intervention fidelity, the therapist structured intervention primarily with reference to baseline COPM data and according to the client’s changing occupational profile and performance throughout intervention. Also, the therapist used a restorative approach (AOTA, 2008)—that is, to restore impaired abilities and skills, the intervention emphasized treatment and use of the affected UE in a task repertoire that developed in keeping with return to desired roles (Table 2). Intervention took place almost exclusively in a hospital-based practice apartment that simulated a home environment. Environmental features included a table, stove, sink, bed, workbench with tools, vacuum, mop, ironing board, and washer and dryer. Some sessions took place in a nearby therapy gym containing the Baltimore Therapeutic Exercise Equipment (BTE) work simulator (BTE Technologies Incorporated, Hanover, MD). This computerized device has various handle attachments used in the simulation of activity demands associated with different jobs. The BTE identifies biomechanical variables of UE movement and monitors progress throughout intervention (Bhambhani, Esmail, & Brintnell, 1994).
Description of Factors Governing Intervention Sessions
Client factors such as decreased range of motion and increased spasticity interfered with Will’s participation in occupation. Thus, although sessions consisted primarily of occupation-based intervention, the therapist used preparatory methods (such as stretching or weight bearing) and purposeful activity (such as turning a key to develop functional pinch for dressing tasks) as ancillary forms of intervention (see Table 2).
Data Collection
To capture behavioral changes, an occupational therapist not involved with the intervention administered the FMA, the SIS, and the COPM at baseline and at completion of the intervention period. The therapist had formal training in administration of these assessments as well as 15 yr clinical experience working with patients with stroke. To capture neurophysiological changes, a biomedical engineer conducted TMS motor mapping procedures at baseline and at the completion of the intervention. This biomedical engineer routinely administers TMS as part of a multi-institutional stroke research program at the site of this study. To capture descriptive changes, the occupational therapist who delivered the intervention kept detailed documentation throughout the study regarding Will’s response to the intervention.
Data Analysis
We used Statview software (SAS Institute Inc., Cary, NC) to analyze baseline and postintervention data from the behavioral assessments (FMA, SIS, and COPM) as well as the TMS assessments (rMT, motor map volume, COGx, and COGy) of both hemispheres. Comparisons were made between the baseline and postintervention descriptive data to identify changes in functional movement and occupation.
Results
Behavior (Motor Function)
Table 1 summarizes FMA and SIS data. The change in FMA score shows that improvement in UE motor control occurred over the course of the intervention. Improvement occurred in all SIS domains except communication. The most notable increase in SIS scores occurred in the domains of hand function and memory.
Table 3 summarizes COPM data. These data indicate that Will perceived improvement in both occupational performance and satisfaction with performance. He reported a greater magnitude of change in his satisfaction than in his performance.
Results on the Canadian Occupational Performance Measure
Neurophysiology (Neuroplastic Change)
No notable difference existed between rMT at baseline (47% of maximum stimulator output) and rMT at postintervention (54% of maximum stimulator output). We noted a considerable bilateral increase in cortical motor map volume postintervention (Figure 1). More specifically, the contralesional motor map volume changed from 3.28 at baseline to 9.38 at postintervention (measured normalized MEP × cm2), and the ipsilesional motor map volume changed from 0 at baseline (indicating absence of MEPs) to 0.22 at postintervention. We observed no notable changes in contralesional COGx (3.66 cm at baseline; 3.68 cm at postintervention). Contralesional COGy moved posteriorly (−0.16 cm at baseline; −1.05 cm at postintervention).
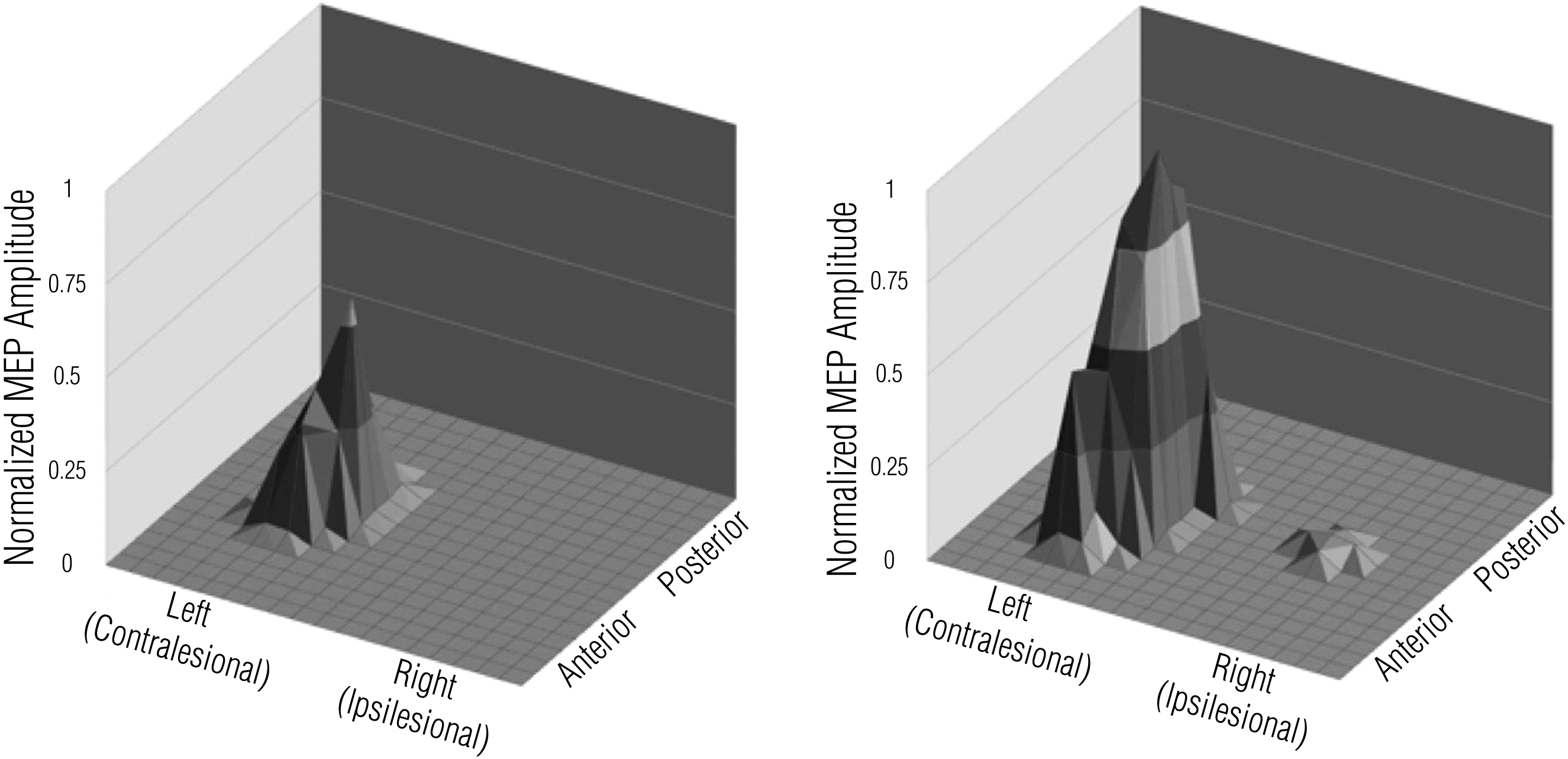
Neurophysiological change: TMS motor cortical mapping before and after 15 sessions of occupation-based intervention.
Description of Participation in Occupation
As intervention progressed, Will reported several changes taking place. More specifically, he reported increased motivation, increased confidence, increased component factors of affected UE function (including improved proprioceptive awareness), improved self-management of health routines (e.g., knowledge of effective stretching, pain management, and self-cueing supporting bilateral UE use), increased role competence, and increased self-direction in occupational performance. Table 1 provides additional details of Will’s descriptive results.
Discussion
The results of this case study indicate that a relatively brief period of occupation-based intervention in a hospital setting designed to simulate a home environment considerably enhanced affected UE motor recovery, neuroplastic change, and occupational performance for 1 participant with chronic stroke. Will’s FMA change in UE motor control exceeded the threshold for clinically meaningful change, which research has established as 3 points (Lo et al., 2010). Likewise, the changes in SIS scores for the summary of all domains, as well as the hand function domain, met or exceeded the threshold (10–15 points change) for clinical relevance (Duncan et al., 2003). Will’s SIS measurement of perceived overall recovery showed a notable gain as well. Because a COPM change of ≥2 points reflects clinical relevance (Law et al., 1998), Will’s COPM change showed that he experienced clinically meaningful effects with regard to occupational performance and satisfaction. Likewise, the descriptive outcomes reflect that Will experienced positive change in both occupational profile and occupational performance, ultimately improving his health and well-being.
Neurophysiological evaluations also reflected marked improvement since baseline. As a result of intervention, Will exhibited not only expansion of the contralesional motor map but also the first-time emergence of ipsilesional MEPs. The initial emergence of MEPs on the ipsilesional brain after intervention, at which time Will was 18 mo poststroke, strongly indicates an association of ipsilesional neuroplastic change with intervention. That motor map expansion occurred in the absence of notable changes in rMT indicates that nonspecific changes in corticomotor excitability are not likely to have confounded the interpretation of map area changes. Either or both of the following points may explain why corticomotor reorganization occurred bilaterally:
Intervention entailed bimanual tasks, which may have led to neuroplastic change related to each UE (rather than the affected UE only).
Because stroke can unmask the 10% of the corticospinal tract that remains uncrossed, intervention could affect this normally latent tract, in which case the results of intervention would not be restricted to ipsilesional (i.e., unilateral) neuroplastic change.
Limitations of this study affect the generalizability of our findings. First, evidence from a single case study cannot be generalized (Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996). However, single-case studies have value in that they can provide preliminary evidence for, as well as detailed descriptions of, specific interventions and outcomes. Second, one could argue that the inclusion of preparatory methods and purposeful activity as ancillary techniques to occupation-based intervention may have confounded this study’s results. However, we believe that regarding these ancillary techniques as constituent parts of or necessary precursors to occupation-based intervention is justifiable. This viewpoint necessitates ensuring that the recipient of intervention understands the essential connection between the preparatory method or purposeful activity and the occupation (Price & Miner, 2007). Notably, this approach helped facilitate the participant’s engagement in the occupation of managing preparatory health-related habits and routines (i.e., self-stretching and spasticity reduction) for enhancing general occupational performance outside the study.
Implications for Occupational Therapy Practice
This evidence demonstrates that TMS is a viable tool to measure results of occupation-based intervention and to build the occupational therapy evidence base. Moreover, this case report shows that occupation-based intervention can support adaptive rewiring of the brain and improved occupational performance.
Conclusion
In 1 participant with chronic stroke, a restorative approach to occupation-based intervention led to enhanced occupational performance, resumed competence in desired roles, improvement in affected UE functional use, and notable neuroplastic change as measured by TMS. To build on this study, we recommend future large-scale studies comparing behavioral, neurophysiological, and descriptive outcomes of various occupational therapy approaches for recovery from various levels of poststroke motor deficit (i.e., mild, moderate, or severe). In addition, we recommend that such studies incorporate a longer follow-up period.
Footnotes
Acknowledgment
We acknowledge and thank Linda Freudenberger, Daniel Aken, and R. Cameron Henzman for their contributions to this study.