
Abstract
Asymmetrical impairments in children with hemiplegic cerebral palsy (CP) often affect movement efficiency and performance of daily living activities (Fedrizzi, Pagliano, Andreucci, & Oleari, 2003; Pagliano et al., 2001). Functional impairments associated with this condition are accompanied by diminished use of the involved upper extremity (UE), compromising the performance of bimanual activities (Van Zelst, Miller, Russo, Murchland, & Crotty, 2006). Although evidence of the efficacy of specific rehabilitation approaches is generally weak (Sakzewski, Ziviani, & Boyd, 2009), studies suggest a potential benefit of intensive training of the involved UE, such as in constraint-induced movement therapy (CIMT) and bimanual training.
CIMT involves the restriction of the noninvolved UE along with intensive unimanual training of the involved UE (e.g., Taub, Uswatte, & Pidikiti, 1999). When CIMT is used in the pediatric population, training activities are selected according to the child’s interest and tailored to target the major impairments deemed to have direct relation to the impaired use of the involved UE (Charles & Gordon, 2005; Eliasson & Gordon, 2008). Considering that this training involves exclusive provision of unimanual activities, realistic functional activities involving bimanual UE use are not practiced during its implementation (Charles & Gordon, 2006; Gordon & Friel, 2009). Nevertheless, increasing evidence suggests that CIMT results in improvements in use of the involved UE in both unimanual and bimanual activities (Charles, Wolf, Schneider, & Gordon, 2006; Deluca, Echols, Law, & Ramey, 2006; Eliasson, Krumlinde-Sundholm, Shaw, & Wang, 2005).
Bimanual training is another approach that targets the involved UE of children with asymmetrical impairments. Hand–arm bimanual intensive training (HABIT) is a highly structured technique that provides intensive training with graded functional activities tailored to the child’s specific impairment and interests, and intervention focuses directly on bimanual hand use (Charles & Gordon, 2006). Children are encouraged to use the involved UE during functional bimanual activities such as self-care and play (Charles & Gordon, 2006). In a randomized controlled trial (RCT), Gordon, Schneider, Chinnan, and Charles (2007) tested the effects of a 10-day HABIT protocol in children with hemiplegic CP and found significant improvements in bimanual hand use postintervention.
Recent studies have compared the effects of CIMT and bimanual training on discrete components of manual use, including manual dexterity and the quality and amount of use of the involved UE and bimanual function (Gordon et al., 2011; Sakzewski et al., 2011b). In a quasi-randomized trial comparing CIMT and HABIT, similar unimanual and bimanual improvements were found for both groups as measured by standard clinical tests (Gordon et al., 2008).
These findings have recently been replicated in larger randomized trials (Gordon et al., 2011; Sakzewski et al., 2011b). Sakzewski et al. (2011a) compared the impact of CIMT and bimanual training on functional goals established by parents and found that children from both treatments showed similar improvements; in this study, however, in addition to the performance of unimanual activities, children from the CIMT group also practiced goals with both hands without using the constraint, which is not typically done in traditional CIMT protocols. Improvements in functional goals have also been reported in a combined CIMT and bimanual training protocol (Aarts, Jongerius, Geerdink, van Limbeek, & Geurts, 2010). Thus, it is not clear whether the improvements in functional goals can be attributed to the CIMT or to the combination of unimanual and bimanual training. Evidence regarding the effects of intensive protocols, such as CIMT or HABIT, on activities of daily living and on functional goals established by families illustrates the functional impact of interventions (Ahl, Johansson, Granat, & Carlberg, 2005; Øien, Fallang, & Østensjø, 2010).
In the current study, we aimed to compare children’s functional skills and independence in self-care activities following unimanual (CIMT) or bimanual (HABIT) training and to examine the interaction between magnitude of change and type of intervention. We also aimed to analyze caregivers’ perception of their child’s functional goal achievement following administration of these training protocols in children with hemiplegic CP. The specific research questions include the following:
Does CIMT or HABIT lead to improvement in daily functioning outcomes?
Are changes in functional outcomes different after the two intervention protocols?
Do caregivers perceive that the children achieve functional goals as a result of these two intervention protocols?
We hypothesized that greater improvements would be observed in children receiving bimanual training because many daily activities require the use of both hands (i.e., specificity of practice), whereas only subcomponents of these activities may be practiced during CIMT (Shea & Wright, 1995; Thorndike, 1914).
Method
Research Design
We conducted an RCT with a subset of children with hemiplegia from a larger RCT (Gordon et al., 2011). The institutional review board of Teachers College, Columbia University, approved the study, and we obtained informed consent from all participants and their caregivers.
Participants
We recruited the last 16 children with hemiplegia enrolled in a larger RCT (Gordon et al., 2011) of CIMT and HABIT (data collected from December 2008 through July 2009) to complete the assessments and intervention procedures. Descriptive information for each child is shown in Table 1. Inclusion criteria for participation were as follows: hemiplegia with a difference of at least 50% between the two limbs on timed motor tasks of the Jebsen–Taylor Test of Hand Function (without the writing subtest; Jebsen, Taylor, Trieschmann, Trotter, & Howard, 1969), ability to extend the wrist at least 20° and fingers 10° from full flexion, and normal cognitive abilities (mainstreamed in school).
Participant Characteristics (N = 16)
Note. CIMT = constraint-induced movement therapy; HABIT = hand–arm bimanual intensive training; MACS = Manual Ability Classification System (I = the child is able to hand most objects independently; II = the child is able to handle most objects, but may present reduced dexterity; III = the child is able to handle objects, but may need adaptations, modifications in the task or assistive devices).
Instruments
We classified the children’s hand function using the Manual Ability Classification System (Eliasson et al., 2006), which focuses on children’s manual abilities in performing daily routine activities such as eating, dressing, and playing. This system includes five levels of hand function, from Level I, indicating the child is capable of easily manipulating objects without restrictions in daily living activities, to Level V, indicating the child requires full assistance to handle objects.
To evaluate the children’s daily functioning, parents were interviewed by the first author (Marina de Brito Brandão) using the Pediatric Evaluation of Disability Inventory (PEDI; Haley, Coster, Ludlow, Haltiwanger, & Andrellos, 1992; Mancini, 2005) and the Canadian Occupational Performance Measure (COPM; Carswell et al., 2004; Law et al., 1990). The PEDI consists of a semistructured interview with caregivers focused on the child’s functioning in daily living activities at home, such as self-care, mobility, and social function. For the current study, we assessed the children’s self-care functional skills and independence. The Self-Care Functional Skills scale of the PEDI comprises 73 items indicating the child’s ability to perform activities related to tasks such as eating, grooming, dressing, bathing, and bladder and bowel management. Items are scored 0 = child is unable to perform or 1 = child is capable of performing it. We used the Caregiver Assistance scale as a measure of the children’s independence; this scale consists of eight items that indicate the amount of assistance the child usually receives in his or her daily routine to perform the self-care tasks. Each item is scored on a 6-point rating scale ranging from 0 = complete assistance to 5 = independence. We used the raw scores from both scales. The PEDI is considered a valid and reliable test (moderate concurrent validity r = .70–.80 with the Battelle Developmental Inventory Screening Test; Feldman, Haley, & Coryell, 1990).
The COPM was designed to identify and measure, by means of interview, changes in functional problems clients consider to be relevant in the areas of self-care, productivity, and leisure performance. The client or caregiver defines the most relevant functional goals to be accomplished, ranks their importance, and rates their child’s performance ability (hereinafter referred to as performance) and their own satisfaction level (hereinafter referred to as satisfaction; Carswell et al., 2004; Law et al., 1990; Verkerk, Wolf, Louwers, Meester-Delver, & Nollet, 2006). The COPM is valid and reliable for use with parents (agreement between parents and children, −2.4–2.3; Verkerk et al., 2006), and its use is of particular interest because it provides flexible and consistent outcome measurements that are relevant to children and their families (Cusick, McIntyre, Novak, Lannin, & Lowe, 2006; Randall & McEwen, 2000).
In the current study, caregivers were interviewed by de Brito Brandão before the intervention to establish functional goals for desired activities. Parents were asked to rank the importance of the activities on a 1–10 rating scale. The parents chose their five most important goals and rated their perception of their child’s current performance and their own satisfaction on these five goals using a 1–10 scale. We used the parents’ mean scores on the performance and satisfaction scales at pre- and postintervention for analysis. We further categorized the functional goals parents established into bimanual and unimanual categories of self-care, play, or school activities. The children practiced these goals during the intervention period consistent with their interests and current abilities and the materials available at the intervention setting. Duration of functional training ranged from 0–30 min/day. Children in the CIMT group did not practice bimanual goals because of the use of the constraint, which allowed only exclusive training of unimanual components related to the established bimanual functional goals.
Intervention
Participants were randomized to the HABIT or CIMT groups using offsite (concealed) allocation, stratified by age and severity. The interventions were provided for 15 days, 6 hr daily, totaling 90 hr, at Teachers College, Columbia University, New York. Training took place in two separate rooms, one designated for CIMT and the other for HABIT. Each participant was assigned to a trained interventionist who was responsible for choosing and monitoring specific activities customized to the child’s needs, interests, and progress. Interventionists included occupational and physical therapists as well as graduate students in kinesiology, neuroscience, speech pathology, or psychology who were supervised by occupational and physical therapists experienced with the CIMT and HABIT protocols. The interventionists were trained before administration of interventions. Moreover, an occupational and a physical therapist provided constant supervision, helping the interventionists choose the appropriate activities and monitoring the suitability of intervention procedures.
An interventionist assisted each child individually, and children worked individually or in groups throughout the day (always maintaining the 1:1 interventionist–child ratio). The activities used in the training included fine motor activities (e.g., small blocks and beads), board and card games, self-care activities (e.g., eating, dressing), and gross motor activities (e.g., balls, bowling), individually selected according to the child’s interests and movements elicited (see Charles & Gordon, 2006). Activities were individually graded to promote the children’s success in performance; the difficulty level was increased after improvements in performance.
Grading procedures focused on increasing activities’ complexity, speed, and accuracy demands. For both treatments, children participated in group activities, such as games and arts, every day to increase motivation. Interventionists provided positive reinforcement and knowledge of results during training (Charles & Gordon, 2006; Gordon et al., 2007). Both treatments used structured (part and whole) task practice embedded in play and functional activities. Whole-task practice involved sequencing successive movements within an activity (e.g., card games); these activities were performed continuously for at least 15 to 20 min. Targeted movements and spatial and temporal coordination were practiced within the context of completing the task. Part-task practice involved breaking down motor skills into smaller components (e.g., card flipping to promote forearm supination) while increasing repetitions and task complexity (Charles & Gordon, 2006; Gordon et al., 2011).
For the CIMT group, children’s nonaffected UEs were restrained with cotton slings, and they performed unimanual activities with the affected UE. The sling was strapped to their trunk with the distal end sewn shut to prevent use. For the HABIT group, no physical restraints were used, and children engaged in age-appropriate bimanual activities. The interventionists selected activities to foster improvement of the main neuromotor impairments that prevented each child from using the involved UE and structured activities to encourage bimanual hand use with the involved UE progressively performing various roles (e.g., active or passive assist, stabilizer, manipulator; Charles & Gordon, 2006; Gordon et al., 2007).
At home, parents completed a 1-hr daily exercise program with their child consisting of unimanual (without a physical restraint) or bimanual practice of activities of daily living and play. Parents completed a daily log to monitor compliance and enhance communication with interventionists (Charles & Gordon, 2006; Gordon et al., 2007). Additional information about the techniques and the larger trial can be found elsewhere (Gordon, Charles, & Wolf, 2005; Gordon et al., 2011).
Data Collection
A trained occupational therapist (Marina de Brito Brandão) not blinded to children’s groups conducted the interviews with parents for the administration of the PEDI and COPM. The measures were administered at two time points: (1) preintervention, after the randomization process, and (2) postintervention, on the day after completion of the intervention.
Data Analysis
The Shapiro–Wilk test (IBM SPSS Statistics, Armonk, NY) was used to test the Gaussian characteristics of the dependent variables, revealing normal distribution. Mixed 2 (Groups) × 2 (Assessments) analyses of variance, with repeated measures on the latter factor, were used to compare group mean scores on the PEDI and COPM. Main effects were further examined using preplanned contrasts. Partial η2 was reported as an estimator of the effect size that describes the ratio of variance from the dependent variable that is accounted for by a predictor variable while controlling for other predictors (values range from 0 to 1).
Clinically important changes in performance and satisfaction scores on the COPM were determined as gains in functional goals of 2 or more points (Law et al., 1998). For the PEDI scales (functional skills and independence in self-care), changes greater than 2 standard errors of measurement (Kerlinger, 1986) indicated statistically robust changes, which were considered changes greater than chance or measurement error. This criterion was used because of the lack of evidence on magnitude of difference suggestive of clinically meaningful changes resulting from use of the PEDI with children with hemiplegic CP.
Fisher’s exact test (IBM SPSS Statistics, Armonk, NY) compared the frequency distribution of children who achieved clinically important changes in scores on the COPM performance and satisfaction scales and on the PEDI functional skills and independence scales across intervention groups.
We also analyzed the amount of time spent practicing the functional goals established at the COPM preintervention assessment and COPM scores for practiced and unpracticed goals. Independent t tests were used to compare group means [PEDI] on the amount of time spent in unimanual and bimanual goals practiced in the intervention and home settings. Moreover, because COPM scores from practiced and unpracticed goals showed normal distribution, further mixed 2 (Groups) × 2 (Assessments) ANOVAs were used to compare pre- and postintervention assessments and to test Group × Assessment interactions. The significance level was established at α = .05.
Results
Daily Functioning Outcomes
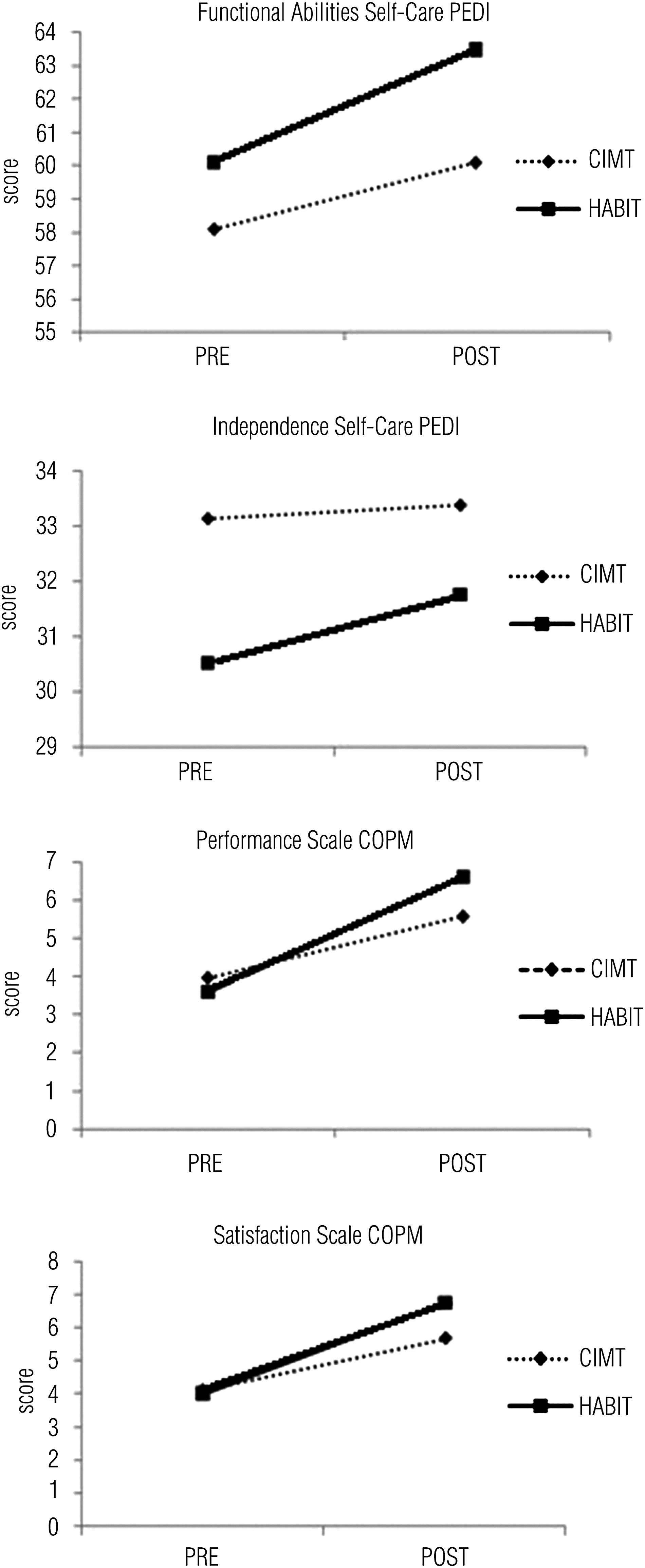
Before intervention, the groups had similar mean scores on PEDI self-care functional skills (CIMT, mean (M) = 58.12, standard deviation (SD) = 6.51; HABIT, M = 60.12, SD = 6.12) and independence (CIMT, M = 28.87, SD = 7.47; HABIT, M = 30.5, SD = 4.87). The two groups showed improvements at the postintervention evaluation on PEDI self-care functional skills (CIMT, M = 60.12, SD = 6.13; HABIT, M = 63.5, SD = 5.01), F (1, 14) = 67.76, p = .0001, partial η2 = .83, and independence (CIMT, M = 29.12, SD = 7.26; HABIT, M = 31.75, SD = 4.4), F(1, 14) = 8.40, p = .01, partial η2 = .37 (Figure 1). The Group × Assessment interaction approached but did not reach significance (p = .054 for functional skills, p = .074 for independence). The frequency distribution of children who showed robust changes in PEDI scores was not significant across interventions (p = 1.00 for functional skills, p = 1.00 for independence; Table 2).
Changes in PEDI and COPM Scale Scores
Note. CIMT = constraint-induced movement therapy; COPM = Canadian Occupational Performance Measure; HABIT = hand–arm bimanual intensive training; PEDI = Pediatric Evaluation of Disability Inventory.
Scales on the PEDI. bScales on the COPM. cMinimum clinically important change.
Satisfaction and Performance Outcomes
Of the goals chosen by parents from both groups during administration of the COPM, most were bimanual activities (94.4% for the HABIT group, 87.2% for the CIMT group). No group difference was found at the preintervention assessment for performance (CIMT, M = 3.95, SD = 1.25; HABIT, M = 3.56, SD = 0.66) or satisfaction (CIMT, M = 4.14, SD = 1.54; HABIT, M = 4.03, SD = 0.92). Both groups improved in performance scores (CIMT, M = 5.54, SD = 1.7; HABIT, M = 6.58, SD = 1.19), F(1, 14) = 54.00, p < .000, partial η2 = 0.79. A Group × Assessment interaction effect was observed, with greater improvements in performance for children undergoing HABIT compared with CIMT, F(1, 14) = 5.15, p = .04, partial η2 = .27 (see Figure 1).
Improvements in COPM parent satisfaction scores were significant for both groups (CIMT, M = 5.68, SD = 2.06; HABIT, M = 6.78, SD = 1.64), F(1, 14) = 35.46, p = .0001, partial η2 = .72, with no interaction (see Figure 1). The frequency distribution of children who showed clinically important changes in COPM scores was similar across interventions (p = .61 for performance, p = .13 for satisfaction; see Table 2).
Functional Goals and Practice
Of the 76 COPM activities parents selected as functional goals at preintervention assessment, the children practiced 31 (40.8%) in the intervention or home settings or both (Table 3). Table 3 also summarizes the time children spent practicing unimanual and bimanual goals during the intervention and at home. Most of the functional goals practiced in the intervention setting for children from both groups (CIMT and HABIT) consisted of bimanual activities. No significant difference was evident between groups in the amount of time spent practicing goals in both settings.
Functional Goals Established by Parents in the Preintervention Assessment and Total Time Spent Practicing the Goals
Note. Cells with two letters indicate two separate activities in that category for that child. B = bimanual goal; CIMT = constraint-induced movement therapy; HABIT = hand–arm bimanual intensive training; U = unimanual goal.
Activities practiced at the intervention setting. Children from the CIMT group practiced bimanual goals unimanually at the intervention setting because of the use of the constraint. bActivities practiced at home. cActivities included praying, getting into and out of the car. dActivities practiced unimanually (with the affected upper extremity).
After treatment, both groups differed significantly on number of practiced and unpracticed functional goals in the intervention setting and in performance and satisfaction mean scores. Six of the 8 children in the CIMT group and 5 of the 8 children in the HABIT group practiced some of their parents’ goals during the intervention. Both groups showed improvements in performance scores (mean pre–post improvement for CIMT = 2.83, SD = 1.75; for HABIT = 3.2, SD = 1.04), F(1, 9) = 45.51, p = .0001, partial η2 = .84, with no Group × Assessment interaction. Satisfaction scores for the practiced goals also improved (mean pre–post improvement for CIMT = 2.0, SD = 2.21; for HABIT = 3.07, SD = 1.88), F(1, 9) = 16.34, p = .003, partial η2 = .65, with no Group × Assessment interaction.
All 16 children had goals they did not practice during intervention (totaling 57 goals across all children), but they also showed improvements in performance of unpracticed goals (mean pre–post improvement for CIMT = 1.31, SD = 0.78; for HABIT = 2.62, SD = 1.56), F(1, 14) = 40.39, p = .0001, partial η2 = .74. Group × Assessment interaction approached but did not reach significance (p = .053, partial η2 = .24). Parent satisfaction regarding unpracticed goals also improved in both groups (mean pre–post improvement for CIMT = 1.82, SD = 2.12; for HABIT = 2.66, SD = 1.71), F(1, 14) = 21.68, p = .0001, partial η2 = .61, with no Group × Assessment interaction.
Discussion
In this study, children with hemiplegic CP showed improvements in functional skills and independence in self-care activities and in the achievement of functional goals established by their parents following CIMT and HABIT interventions. In general, similar gains in self-care skills and independence were observed for both groups. Parents of children in the HABIT group perceived superior improvements in their children’s performance of specific functional goals the parents had selected before intervention, but parents in both groups were equally satisfied with their children’s performance. The results suggest that specificity of training (i.e., practice of the same functional underlying requirements as those involved in the desired outcome) occurred only for the performance of specific goals established by parents and that both intensive techniques can be used to increase children’s daily functioning.
Improvement in Daily Functioning Following Intensive Training Protocols
Recent studies have tested the contribution of CIMT and bimanual training to children’s acquisition of self-care skills and to the amount of caregiver assistance provided to support children’s task performance at home. These studies combined CIMT with some form of bimanual training during or after the intervention period, and they documented positive effects on children’s daily functioning (de Brito Brandão, Mancini, Vaz, Pereira de Melo, & Fonseca, 2010; Sakzewski et al., 2011a) The present study provides support for these previous studies by documenting improvements in daily functioning following CIMT or HABIT training. Although the interaction effect was not significant, a tendency was seen toward greater improvement in the HABIT group on both self-care functional skills and caregiver assistance (independence) scores.
It is unknown whether the lack of group difference in self-care outcomes can be attributed to an insufficient number of participants or if the high-intensity component of both protocols resulted in gains in these outcomes. Moreover, it is possible that the PEDI scales are not sensitive enough to capture any subtle differences between groups. In fact, because the PEDI self-care scales (functional skills and independence) do not quantify the manner in which the child uses his or her hands in daily activities, it is possible that such performance was accomplished by means of specific strategies not requiring use of the affected hand. Also, some items from this functional test are unrelated to hand function (e.g., bladder and bowel management). Overall, the improvements in both groups extend previous findings by showing that 90 hr of exclusive unimanual (CIMT) or bimanual (HABIT) training were sufficient to promote children’s self-care functional skills and decrease the amount of caregiver assistance directed to children’s self-care task performance.
Specificity of Training and Functional Goals
Most of the functional goals established by parents from both groups were related to bimanual activities of children’s daily repertoire in the home and school environments. This observation corroborates the belief that bimanual use of the hands in functional activities is one of the most important aspects of the treatment of people with unilateral impairments (Eliasson, Shaw, Pontén, Boyd, & Krumlinde-Sundholm, 2009).
In agreement with the hypothesis of training specificity, in which the best learning occurs when practice characteristics are the same as those of the outcome measured (Shea & Wright, 1995; Thorndike, 1914), children from the HABIT group showed superior improvements in the COPM performance scale at postintervention assessment compared with the CIMT group. Similarly, children with congenital hemiplegia receiving HABIT showed greater improvements in bimanual coordination during a functional bimanual drawer-opening task compared with children receiving CIMT (Hung, Casertano, Hillman, & Gordon, 2011). One possible explanation for the observed difference between intervention groups may be the fact that HABIT procedures encompass the use of both hands to perform the activities. Thus, these children were exposed to situations in which two hands are used together, leading to the development of strategies aiming at performing bimanual activities. The nature of the intervention involving the bimanual training may favor the accomplishment of goals that are important in relevant contexts. Both groups, however, showed improvements in parent satisfaction regarding functional goals, corroborating previous findings from combined CIMT and bimanual goal training (Aarts et al., 2010; Sakzewski et al., 2011a). It seems that the high-intensity component of unimanual or bimanual training is sufficient to provide parents with an awareness of their children’s abilities to accomplish meaningful activities in their contexts.
The children practiced some goals in the intervention setting, but they were unable to practice others because of the nature of the goal (e.g., outdoor activities), lack of available equipment (e.g., playground, bicycle), or lack of interest and ability in the children. To maintain a child-friendly approach by providing activities that were appropriate and interesting to children, interventionists chose some activities to be practiced during the intervention, with a time limit up to 30 min/day across all goals. During the practice of these functional goals, the interventionists in both intensive training protocols were able to observe the transfer of abilities.
In addition to improvements in the goals the children practiced in the clinical setting, parents noted improvements in the performance of and satisfaction with the goals the children did not practice during both the HABIT and CIMT interventions, possibly illustrating the transfer of new abilities to children’s performance of important functional activities. Although the difference was not significant, the HABIT group showed a tendency for greater improvement in the unpracticed goals. It should be noted, however, that the improvements observed for both groups in the unpracticed goals were smaller than the improvements documented for the practiced ones, suggesting an important role of task-specific practice.
Limitations and Future Research
The current study shows positive effects of CIMT and HABIT on children’s daily functioning. Some limitations should be considered, however. One is the lack of follow-up measures; because of practical issues, we were unable to reevaluate the children to examine retention of observed effects. Also, because parents were not blind to the children’s group allocation, their knowledge of a specific protocol might have influenced their choice of functional activities preintervention and their postintervention evaluations of the children’s performance and their own satisfaction. The majority of activities the parents chose, however, required the use of both hands, even for the CIMT group. Furthermore, the sample size was small, potentially affecting the results that approached but did not reach significance.
Finally, the study relied solely on the parents’ perception of important functional goals to be accomplished and the levels of satisfaction and performance of daily living activities. We were unable to conduct the COPM interview with the children because some participants were too young to comprehend the abstract content of this interview and provide appropriate grading. Studies investigating the use of intensive training with older children could provide information on whether these techniques can lead to relevant outcomes from the children’s own perspective. Moreover, future studies should investigate which specific components of unimanual (e.g., CIMT) or bimanual (e.g., HABIT) training, such as duration, length, or specificity of training, or which combination of unimanual and bimanual components may favor children’s acquisition of skills to perform daily living activities.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice:
Both CIMT and HABIT interventions had a positive impact on the functional self-care skills and independence of children with hemiplegic CP.
Children submitted to the HABIT protocol showed greater functional goal performance than children who received the CIMT intervention.
The opportunity to practice bimanual functional activities (i.e., HABIT) fosters changes in the daily living activities considered relevant by parents of children with CP.
Occupational therapists’ choice of CIMT or HABIT may rely on their own expertise, the child’s needs and interests, and characteristics of established client goals; the chosen protocol should include opportunity to practice goals that the child and caregiver deem important.
Conclusion
This study revealed positive effects of the CIMT and HABIT interventions on the functional self-care skills and independence of children with hemiplegic CP. Moreover, parents of children from the CIMT and HABIT groups reported improvements in their children’s performance in relevant daily living activities and their own satisfaction with that performance. Children in the HABIT group showed greater improvements than children in the CIMT group only on the functional goal performance scale, suggesting that the opportunity to practice bimanual functional activities during HABIT implementation may lead to changes in the performance of daily living activities that parents consider important. Rehabilitation professionals may choose CIMT or bimanual training on the basis of their own expertise, the child’s needs and interests, and characteristics of established client goals, but with either treatment, professionals should include the opportunity to practice goals the child and caregiver deem important.
Footnotes
Acknowledgments
This work was supported by a grant from the Thrasher Research Fund and CVS Landmark Cares. Funding was also provided by the Brazilian government agencies National Counsel of Technological and Scientific Development (CNPq) and Foundation for Research Support of Minas Gerais (FAPEMIG). We thank our evaluators and volunteer interventionists for their dedicated efforts and the participants and families who participated.