
Abstract
This study investigated the effects of wearing a wrist support splint for 8 wk and receiving a formal education program on patients with carpal tunnel syndrome (CTS), as well as factors associated with patients’ desire to seek surgical intervention. Participants were recruited from a hospital surgical wait list and randomly assigned to an intervention group (n = 30) or a control group (n = 24). Significant improvements in measures of symptom severity and functional status over the duration of the study appeared in the intervention group but not in the control group. Logistic regression for the intervention group showed that symptom severity (odds ratio [OR] = 1.53, 95% confidence interval [CI] [1.20–1.93]), functional deficits (OR = 1.31, 95% CI [1.08–1.57]), pain score (OR = 1.25, 95% CI [1.11–1.61]), and symptom duration (OR = 1.11, 95% CI [1.01–1.24]) were positively associated with the desire to seek surgical intervention. This conservative CTS treatment program conducted by occupational therapists can improve symptoms and hand function in CTS patients.
Carpal tunnel syndrome (CTS), the most common nerve entrapment, is caused by median nerve compression in the carpal tunnel of the wrist and typically presents with paresthesia in the thumb, index, middle, and radial half of the ring finger (Burke, Bradley, Sinha, Wilgis, & Dubin, 2007; Stevens, Beard, O’Fallon, & Kurland, 1992). Other signs and symptoms include pain, disturbed sleeping patterns, reduced finger dexterity, and loss of functional grips. The manifestation of the condition depends on the duration and severity of the median nerve compression. If untreated, permanent impairment can occur (Gelfman et al., 2009; van Doesburg et al., 2010). The estimated prevalence of CTS in general practitioner clinics is 1.3 per 1,000 patient consultations (Bongers, Schellevis, van den Bosch, & van der Zee, 2007; van Doesburg et al., 2010), and according to a survey in Sweden, the prevalence of the condition can be as high as 3.8% in the general public (Atroshi et al., 1999). More CTS cases are diagnosed and symptoms are more severe in older than in younger populations (Gelfman et al., 2009). In the United States, CTS has been reported to account for 1.1% of work-related injuries requiring time off duty among workers in private industries (Bureau of Labor Statistics, 2007).
The exact etiology of CTS is unknown, and the associated causes are multifactorial and may include local pathogenesis factors (e.g., space-occupying lesions, fractures, tumors, inflammatory diseases), systemic factors (e.g., pregnancy, diabetes, hyperthyroidism, metabolic conditions), and mechanical factors (e.g., direct pressure, escalation of internal pressure of carpal tunnel as a result of extreme finger flexion and wrist movements; American Academy of Orthopedic Surgeons, 2008; van Doesburg et al., 2010). You et al. (2004) reported that factory workers who were exposed to repetitive stress on their wrists during manufacturing processes were more likely to develop CTS. After further risk analysis, You et al. concluded that repetitive manual tasks in cold working environments, poor social support, obesity, and poor premorbid health were other factors closely associated with development of the condition.
Research supporting the effectiveness of conservative treatment is limited (Uchiyama et al., 2010). In a systematic review of four randomized controlled trials on CTS management, Verdugo, Salinas, Castillo, and Cea (2008) concluded that surgical treatment relieved symptoms of CTS better than supportive splints. Other authors have also disputed the use of splinting to manage CTS, arguing that surgery is the preferred treatment because of its cost effectiveness and better clinical outcomes (Gerritsen et al., 2002; Korthals-de Bos et al., 2006; Verdugo et al., 2008). In comparing surgical treatment with a 6-wk comprehensive hand therapy program, Jarvik et al. (2009) reported that patients who underwent surgical interventions had better rehabilitation outcomes; however, the authors acknowledged that the difference was only modest from a clinical perspective.
Not all studies have supported surgery as the primary intervention for CTS, and factors such as the age of the patient may influence surgical outcomes. Mondelli, Padua, and Reale (2004) found that patients aged 50 yr and older showed less improvement in hand functions, lower electrophysiological nerve conductance test results, and worse symptom severity and functional status after surgery compared with younger cohorts.
In clinical practice, surgery is recommended for severe cases of CTS, whereas conservative treatment is recognized as an option for the acute onset of milder symptoms (Atroshi et al., 1999) or when clinical signs of median nerve denervation are first identified (American Academy of Orthopedic Surgeons, 2008). Burke et al. (2007) studied 490 CTS patients in the United States and the United Kingdom and recognized the role of nonoperative primary care management including education in task modifications and work simplification techniques, ergonomic interventions, and provision of a wrist splint. Cochrane reviews of nonsurgical treatment revealed significant improvement in CTS symptoms if a supportive splint was worn full time for 4 wk (O’Connor, Marshall, & Massy-Westropp, 2003; Piazzini et al., 2007; Walker, Metzler, Cifu, & Swartz, 2000). Walker et al. (2000) conducted a comparative study of splinting and concluded that full-time splinting was superior to nighttime-only splinting. To gain optimal benefits from a splint, Nuckols et al. (2011) and the American Academy of Orthopedic Surgeons (2008) recommended wearing the splint for 6 and 7 wk, respectively. Other clinical trials have adopted splint-wearing schedules for as long as 12 wk (De Angelis, Pierfelice, Di Giovanni, Staniscia, & Uncini, 2009). In the clinical setting, the optimal wearing time is dependent on many factors, such as the duration of symptoms, severity of the symptoms, daily activity requirements, wait time for surgery, and patient compliance.
Comprehensive education programs have been shown to reduce symptoms of cumulative trauma disorders and are an essential component of any successful therapy program (Eversmann, 1990). Knowledge empowers patients by enabling them to play an active role in their recovery and prevention of relapse (You et al., 2004). In reviewing the quality of measures for nonoperative treatment, the Carpal Tunnel Quality Group recognized patient education and activity modification as essential components in the success of treatment (Nuckols et al., 2011). Katz et al. (2005) studied 181 workers affected by CTS and concluded that to improve work absences, treatment should be multidimensional, including education. Many ergonomic factors, such as work station adjustment, sleep posture, and tool handles, can influence the pressure within the carpal tunnel. These factors can be improved through education and knowledge of task modification (Burke et al., 2007). In a multicenter study, Burke et al. (2007) found that in primary care, task modifications that improve symptoms of CTS patients at work and home were not adopted as a treatment modality.
Although previous research suggests that conservative CTS management programs have some merits, the evidence is insufficient to claim that the approach benefits all patients. Thus, general practitioners continue to refer patients with mild to moderate symptoms of CTS to hand surgeons for median nerve decompression as the first-line intervention (Atroshi et al., 1999).
The objectives of the current study were (1) to investigate whether a conservative treatment program of full-time wrist splinting and education could improve symptoms and hand function of participants with CTS and (2) to identify areas of improvement associated with participants’ desire to seek surgical intervention. The main hypothesis for this study was that a conservative treatment program for CTS would improve CTS symptoms and reduce participants’ desire to seek surgical intervention.
Method
Study Design
The purpose of this randomized controlled trial was to investigate the effectiveness of full-time wrist splinting and education in treatment of CTS. Participants were randomly assigned to either a conservative treatment group or a control group. The conservative treatment group received an 8-wk treatment program involving a full-time wrist splint and education sessions conducted by an occupational therapist. Control group participants were assessed and observed but received no intervention during the 8-wk study period. At the end of the study period, the participants in the control group were offered the conservative treatment program. The study was approved by the human research ethics committee of Sir Charles Gairdner Hospital (SCGH) in Western Australia. Each participant provided informed consent and could withdraw from the study at any time without consequences.
Intervention and Control Groups
The estimation of adequate sample size for the study was based on pilot data from 5 participants with CTS from the study groups. The primary outcome measure of the current study was the Boston Questionnaire for the Assessment of Carpal Tunnel Symptom Severity (Levine et al., 1993), and the standard deviation was calculated at 0.5. The expected change in score with treatment was 0.2; consequently, 25 participants were required in each group on the basis of an α of .05 and a β of .8. To allow for 20% attrition, we planned to recruit 30 participants in each comparison group from SCGH. We invited 174 patients to take part in the study; these patients had a diagnosis of CTS, were referred by their general practitioner to an outpatient surgery clinic, and were waiting for a surgical consultation.
An occupational therapist who was not an author or a treating therapist was employed to conduct the initial screenings to ensure patients met the selection criteria for the study. Inclusion criteria included the following: age ≥18 yr, paresthesia in the median nerve distribution in the night or day, clumsiness, grasp weakness, sleep disturbance, no medical intervention (e.g., no surgery or steroid injections), no conservative treatments (e.g., no wearing of hand splints) in the past 6 mo, and no pregnancy. Non-English speakers were not excluded, but any medical, cognitive, perceptual, or language deficits that prevented the comprehension of instructions or attendance at appointments resulted in exclusion. Participants could have symptoms in one or both hands, but only one hand, with the worst symptoms, was chosen as the study hand. Fifty-eight participants were excluded because they did not meet the selection criteria.
Participants who were invited and agreed to participate in the study were randomly assigned to the intervention or control group using a blocking strategy, implemented by the first author (Hall), to recruit participants to each study arm at equal rates. The third and fourth authors (Fitzgerald and Byrne) conducted an initial assessment to record a baseline in sensation, pain perception, severity of CTS symptoms, and hand functions for each participant. Changes in symptoms posttreatment were tracked with the same outcome measures at the end of the 8-wk study period. Once the treating occupational therapist was assigned, he or she followed individual participants throughout the assessment and treatment phase of the study. In Week 9, patients’ desire to seek surgical interventions was assessed.
Instruments
The Boston Carpal Tunnel Questionnaire (Levine et al., 1993) is a self-administered questionnaire and standardized measure of symptom severity and functional status for CTS. It is diagnosis specific, valid, reliable, and responsive to change (Leite, Jerosch-Herold, & Song, 2006; Ollivere et al., 2009). It has two scales, the Symptom Severity Scale (BQSS) and the Functional Status Scale (BQFSS), with each scale generating a final score ranging from 1 (no disability) to 5 (most disability). High internal consistency in BQSS and BQFSS scores were reported (Cronbach’s αs of .89 and .91, respectively).
The Visual Analog Scale (VAS) is a subjective pain measurement tool; participants mark their pain level on a 10-cm black line drawn on paper labeled at each end with 0 indicating no pain and 10 indicating worst pain. The VAS has validity and reliability in measuring pain (Williamson & Hoggart, 2005); good repeatability, with correlation coefficients ranging from .97 to .99 (Bijur, Latimer, & Gallagher, 2003); and high test–retest reliability of .79 to .81 in the acute pain setting (Bijur, Silver, & Gallagher, 2001).
A Jamar dynamometer (Lafayette Instrument Company, Lafayette, IN) is a standardized instrument for measuring grip strength that has very high instrument reliability and face validity (α = .99; Kirkpatrick, 1956). When three trial assessments are used, it has been shown to have high interrater reliability (intraclass correlation coefficients [ICCs] of .996–.998; Mathiowetz et al., 1985). The American Society of Hand Therapists (ASHT; 1992) Clinical Assessment Recommendations were used for testing procedures and calibration.
The Purdue Pegboard Test (Lafayette Instrument Company, Lafayette, IN) is a standardized test designed to measure finger dexterity. It is a valid and reliable tool to quantify functional impairment of CTS patients; test–retest reliability is high, with an ICC of .91 (Amirjani, Ashworth, Olson, Morhart, & Chan, 2011). Participants assemble collars, washers, and a small metal pin through the holes of a test board in a set order. A higher timed score indicates that participants require more time to complete activities requiring dexterity.
The Semmes–Weinstein Monofilaments (SWM) is a standardized test that measures light touch or cutaneous pressure thresholds by pressing nylon monofilaments of various thicknesses to the test area. It has been shown to have acceptable instrument reliability and repeatability. SWM testing has good intra- and interrater reliability, with ICCs of .91 and .86, respectively (Bell-Krotoski, Fess, Figarola, & Hiltz, 1995). The ASHT (1992) Clinical Assessment Recommendations were used for standardized testing procedures to identify changes in sensation.
The Phalen’s test (Phalen, 1972) is a provocative clinical test in which the participant places both hands in full wrist flexion to increase the pressure of the carpal tunnel. The test is deemed positive if this position produces or exacerbates numbness and tingling in the median nerve distribution within 60 s (Quality Standards Subcommittee of the American Academy of Neurology, 1993). A systematic review of more than 3,000 cases provided an estimate of 68% sensitivity and 73% specificity in identifying CTS cases (MacDermid & Wessel, 2004).
The satisfaction questionnaire is a self-administered nine-item survey designed by the lead author (Hall) to explore participants’ perceptions of treatment and desire to seek surgery. On completion of the 8-wk study period, we investigated participants’ intention to seek surgical intervention by inviting them to fill out this survey in the waiting room of the outpatient clinic.
Intervention: CTS Conservative Treatment Program
The CTS conservative treatment program included prescription and fitting of a wrist support splint and structured education sessions with a focus on self-management. Over the 8-wk intervention period, each participant received two treatment sessions in the first week and between Week 2 and Week 4 (average of 150 min total) and a 20-min phone call at Week 7.
The two occupational therapists selected to implement the CTS conservative treatment program each had at least 5 yr experience treating CTS patients. The lead author coached them in conducting the program. To ensure uniformity of treatment procedures, the therapists used an assessment and treatment procedure manual, which included step-by-step clinical guidelines, information handouts, and outlines of the content of each education session. The manual was developed by the lead author in consultation with five experienced occupational therapists working in the area of hand therapy and three orthopedic and hand surgeons. During the data collection and intervention phases of the research, the research team met regularly to discuss and address issues raised by the treating therapists. A summary of the procedures for the CTS conservative treatment program is provided in the Appendix.
The wrist splint prescribed was required to support the wrist in a neutral position and allow full finger and thumb motion. The selection of the splint followed a clinical reasoning process based on the experience and clinical judgment of the occupational therapists. From a list of four styles of wrist splints—Manu Basic (Otto Bock, Beijing), Manu Comfort (Otto Bock, Tallinn, Estonia), Roylan Enlarged Thumb Hole D-Ring Wrist Brace (Patterson Medical Ltd., Nottinghamshire, England), or custom-made thermoplastic wrist splint—the treating therapists selected and prescribed the splint that was most suitable for the lifestyle of the participant. For 1 participant, who frequently worked in wet conditions as a chef, the treating therapist fabricated a thermoplastic brace. Previous studies have suggested that the time frame to gain optimal benefits from a splint is 6 wk (Nuckols et al., 2011) to 12 wk (De Angelis et al., 2009). Participants wore the splint full-time throughout the 8-wk study period, and the therapists monitored the splint for fit and comfort during treatment sessions. A splint that interfered with the participant’s activities of daily living, was uncomfortable, or wore out was immediately replaced to improve compliance with treatment.
Participant education content included information on the pathology of CTS, risk identification, and goal setting designed to teach self-management of CTS symptoms. During the education sessions, therapists and participants discussed factors that contribute to or aggravate CTS, such as sleeping postures that increase the pressure in the carpal tunnel and daily activities that involve repetitive wrist and finger movements. Therapists also issued and explained handouts describing practical solutions to meet participants’ specific requirements. In addition, participants completed an action plan with assistance from the occupational therapist that involved formulating individual goals and setting target dates. The strategy used in the risk assessment was based on the CTS risk assessment model developed by You et al. (2004), which addresses both physical and psychosocial risk factors associated with CTS.
Data Collection and Analysis
The two treating occupational therapists, who were not blinded to group allocation, performed all data collection and provided interventions according to the study’s assessment and treatment procedure manual. Data were summarized to describe the characteristics of participants in the intervention and control groups, and χ2 tests and independent sample t tests were used to compare any differences between groups. Paired t tests were used to assess the statistical significance of changes in symptoms (perception of pain, functional status, and motor deficits) over the 8-wk treatment within each group. A backward stepwise logistic regression was conducted using participants’ vocational history, duration of CTS symptoms, treatment time, pain perception scores, Phalen’s test results, finger dexterity, symptom severity, and functional status as independent variables to determine which assessment tool results correlated with participants’ desire to seek surgical intervention.
Results
Of the 116 recruited participants, 76 agreed to participate, 62 appeared for their first appointment, and 31 were assigned to each group (treatment and control group). Eight participants withdrew, were excluded, or did not complete the study after group allocation (1 from the treatment group and 7 from the control group). Complete data from 30 participants who had received CTS conservative treatment and 24 from the control group were available for analysis. Seventy-one percent of participants were women, and the average age was 53.8 yr.
Demographic Characteristics
Participants’ demographic information is shown in Table 1. The treatment and control groups were of similar age, sex, and handedness. Participants’ occupations included manual work, office work, and retirement. Eighty-six percent of the treatment group had symptoms in both hands, and more than half reported arthritis or pathology in their hands other than CTS.
Participant Characteristics
Note. CTS = carpal tunnel syndrome; SD = standard deviation; — = not applicable.
χ2 tests or independent sample t tests.
Intervention Outcomes
The nighttime compliance rate for wearing the splint averaged 89%, but compliance dropped to 81% during the daytime. The reasons for noncompliance included vocational requirements that prohibited wearing of a splint during work hours and habitual participation in activities such as swimming or cooking that precluded wearing a splint. Discomfort and perceived negative cosmetic effects were also reported as reasons not to wear the splint.
The satisfaction questionnaire was used to explore participants’ experience in waiting for surgical intervention, their confidence in their ability to manage the pathology after conservative intervention, and their perceived need for surgical intervention. Figure 1 shows that the treatment group participants had better understanding of and stronger confidence in their ability to manage their condition. This group also had less negative reactions to the extended wait time required to see a surgeon for an initial consultation.
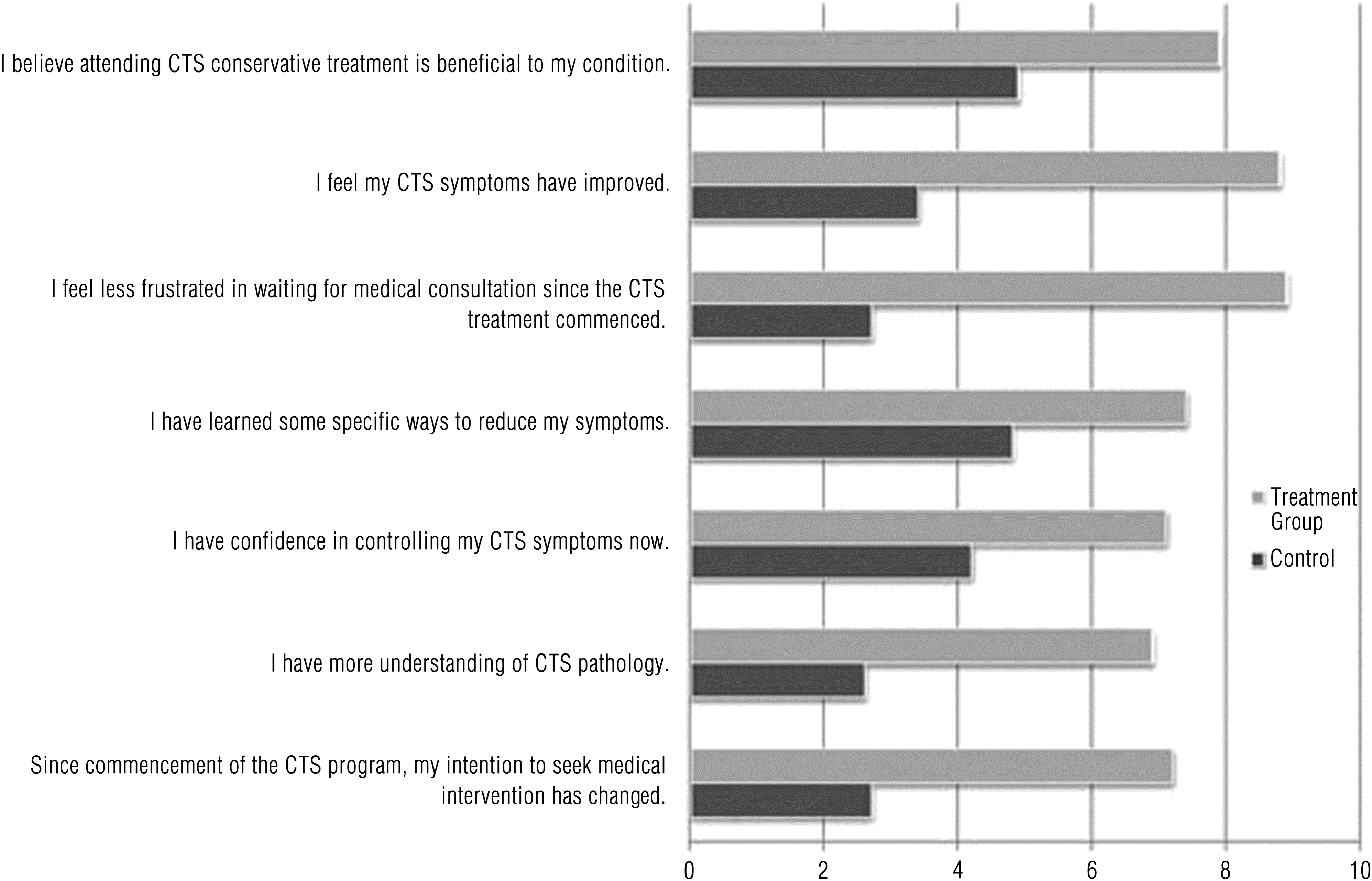
Satisfaction questionnaire results in Week 9: Self-reported degree of recovery and level of satisfaction with the CTS treatment program.
The treatment group data in Table 2 reveal that after the CTS conservative treatment program, symptom severity, functional status, pain perception, and grip strength improved. Some changes were noted in the pre- and postintervention scores in Phalen’s test results, finger dexterity, and sensation, but the changes were not statistically significant. The mean changes in all the outcome measurements listed in Table 2 differed from those of the control group; the control group experienced no change in CTS symptoms at the end of the 8-wk intervention.
Within- and Between-Group Outcome Measurement Differences After the 8-Wk Intervention
Note. BQFSS = Boston Questionnaire for the Assessment of Carpal Tunnel Symptom Functional Status Scale (1 = no difficulty to perform, 5 = unable to perform); BQSS = Boston Questionnaire for the Assessment of Carpal Tunnel Symptom Severity (1 = less severe and frequent, 5 = most severe and frequent); SD = standard deviation; SWM = Semmes–Weinstein Monofilaments; VAS = Visual Analog Scale (1 = less painful, 10 = most painful).
Factors Influencing Participants’ Desire to Seek Surgical Intervention
Nineteen participants (63%) reported they had decided not to pursue surgical intervention after the CTS conservative treatment program. Desire to seek surgical intervention was assessed in Week 9 using the satisfaction questionnaire. The posttreatment desire to seek surgical intervention was classified as yes or no, and a logistic regression model was used to identify factors associated with a positive response. The model was fitted using a backward elimination strategy, in which all potential independent variables are initially included and then the least significant variable is dropped, one at a time, until all variables remaining in the model are significantly associated with the dependent variable (p < .05). The results obtained from the regression model are shown in Table 3.
Significant Factors Affecting Treatment Participants’ Self-Reported Desire to Seek Surgical Intervention From Stepwise Logistic Regression (n = 30)
Note. BQFSS = Boston Questionnaire for the Assessment of Carpal Tunnel Symptom Functional Status Scale; BQSS = Boston Questionnaire for the Assessment of Carpal Tunnel Symptom Severity Scale; VAS = Visual Analog Scale. R 2 = .753 (Nagelkerke, 1991), r = .413 (Hosmer & Lemeshow, 1989), Model χ2(6) = 87.96, p < .001.
Symptom severity, functional status, and pain scores were positively associated with the desire to seek surgical intervention; the higher the score (e.g., more severe pain, less hand function), the stronger the desire to seek surgical intervention. According to the fitted model, each point of increase in the symptom severity score was associated with a 53% increase in the odds of the desire to seek surgical intervention; each point of increase in the functional deficit score, with a 31% increase in desire; and each point of increase in the pain perception score, with a 25% increase in desire. In addition, the model indicated that an increase of 1 mo in experiencing the symptom could elevate the desire to seek surgical intervention by 11%. Age, Phalen’s test result, sensation, grip strength, and finger dexterity were considered in the regression analysis, but they were excluded from the stepwise logistic regression analysis (p > .05). The goodness of fit of the logistic regression model was satisfactory, R 2 = .753 (Nagelkerke, 1991). As a next step, the 4 participants with unilateral CTS were excluded, but the model fit and significance of the variables shown in Table 3 remained essentially unchanged.
Discussion
This study revealed that participants wearing a wrist splint full-time for 8 wk and receiving a structured education program conducted by an occupational therapist had greater symptom relief and better functional outcomes than the control group. Study participants commonly experienced paresthesia and throbbing pain in both hands, engaged in occupations involving manual tasks, and also had comorbid hand conditions commonly found in the CTS population (e.g., arthritis). The 8-wk treatment period included two face-to-face treatment sessions and one follow-up phone call. The participants had had symptoms of CTS for an average duration of 2–3 yr. The participants were highly motivated to take part in the CTS conservative treatment program; the compliance rate with wearing a splint for 24 hr exceeded 80%. After attending the education sessions, participants reported that they felt more confident in self-managing the CTS and positive about the services they had received.
Previous research has suggested that conservative management can reduce symptoms of mild CTS in its early phases (Uchiyama et al., 2010), when symptoms are transient (Piazzini et al., 2007; Rose & Probert, 2009; Storey, Dear, Bradley, Couchman, & Burke, 2008), but the results of the current study show that patients who have had symptoms of long duration can also experience relief. Patients with mild symptoms may achieve full recovery and require no surgical intervention following the conservative treatment program, and those with moderate and severe symptoms can learn management strategies to alleviate their symptoms (Rose & Probert, 2009; Storey et al., 2008). This conclusion is pertinent for the sample population in this study, who were experiencing lengthy waits for surgical consultation for CTS. Intervention to improve symptoms and education in self-management strategies can increase wait-time satisfaction, provide symptom relief for patients unsuitable for surgery, and improve postoperative outcomes for patients who eventually undergo surgery by improving their preoperative status.
The high prevalence of CTS in the community and limited health care resources are some of the factors contributing to the unreasonably long waiting period. Provision of timely clinical intervention can prevent long-term damage to the median nerve, reduce health care costs, and improve outcomes for patients with CTS. Further benefits of the treatment program used in this study are its simplicity and cost-effectiveness. Prompt evaluation and treatment of patients with CTS by an occupational therapist can also provide valuable information on symptom resolution, the severity and duration of symptoms, and the need for the surgical consultation.
Adoption of Reliable Clinical Assessment Tools for CTS
Improvements in symptom severity and hand functions were captured by the BQSS, the BQFSS, and the VAS pain measurement scale. The BQSS was developed in 1993 (Levine et al., 1993) by a panel of hand surgeons, rheumatologists, and patients, who identified six critical domains for the evaluation of CTS: pain, paresthesia, numbness, weakness, nocturnal symptoms, and overall functional status. Its validity and reliability were established through evaluation of the difference between perceived and actual improvement in the CTS cohorts (Levine et al., 1993). Previous research has successfully used the Boston Carpal Tunnel Questionnaire to measure rehabilitation outcomes (Mondelli et al., 2004) and to assess patients who are likely to respond to conservative treatment (Ollivere et al., 2009). The current study found that the Boston Carpal Tunnel Questionnaire is also sensitive to factors related to how patients make decisions regarding their medical treatment. Methods used to evaluate CTS rehabilitation outcomes vary widely in clinical practice. In line with the contemporary trend of client-centered practice in hand therapy, occupational therapists should use measurement tools that are sensitive to the decision-making processes of patients, such as the Boston Carpal Tunnel Questionnaire, to facilitate clinical decisions.
Important Role of Education in CTS Rehabilitation
The risk assessment and goal-setting treatment sessions of the current study enabled participants to identify individual risk factors in their daily activities, empowering them to modify their routines to minimize the impact of CTS. The multifactorial aspects of managing CTS patients postulated in You et al.’s (2004) risk assessment model were a useful guide in developing the CTS education sessions. The education component of the treatment program may have influenced the high rates of splint compliance in the current study because participants understood the reasons why they should actively engage in and take responsibility for their treatment. Others authors (Burke et al., 2007; Nuckols et al., 2011) recognized the role of education, suggesting that it facilitates the patient’s understanding of CTS, knowledge of risk factors, and engagement in activity modification to manage symptoms. Education is a crucial component of CTS conservative treatment in that it encourages an active role in recovery and develops patient confidence in self-management. Occupational therapists have a unique skill set in the role of patient education.
Limitations
Because of our observation that participants waited an average of 32 mo to see a surgeon, we made the assumption that all participants were keen to seek surgical intervention before commencement of the CTS conservative treatment program. Nearly two-thirds of the participants reported that they had decided against seeking surgical intervention after the treatment program. However, reporting their intention to the therapists who treated their condition may have introduced a social desirability bias. The current study did not use electrodiagnostic testing as an outcome measure. Advanced diagnostic tools can assist in establishing a clinical diagnosis for patients with CTS. Although the omission of electrodiagnostic testing because of cost may have been a limitation of the study, in the clinical setting, full resolution of CTS symptoms with conservative management eliminates the need for such testing for these patients (Szabo, Slater, Farver, Stanton, & Sharman, 1999).
The objective of the study was to investigate the effectiveness of a conservative treatment program. The treatment was provided by more than one occupational therapist; consequently, the improvement experienced by participants may have differed because of differences in skill of the treating therapists. Although it was not practical to deploy one therapist to complete all the treatment and data collection in the host hospital, the researchers limited themselves to two therapists to treat and assess participants. Effort was also made to ensure an approximately equal number of participants in each group by randomly assigning participants to a group in blocks of four. However, dropout after recruitment to the study resulted in some disparity in the number of participants in the treatment and control groups. Another limitation of this study is that the interventionists were not blinded to study purpose or group assignment, which again was not possible in the settings where the research was conducted.
Implications for Occupational Therapy Practice
Clinicians recognize paresthesia and weakness as primary CTS symptoms and subsequently treat the symptoms vigorously in clinical practice. Pain is not typically a key feature of CTS. Nevertheless, pain was reported as a predominant symptom in a recent study of 112 patients with CTS (Modi, Ho, Hegde, Boer, & Turner, 2010). The authors reported that the increasing frequency of pain was associated with an increased severity of median nerve motor fascicle compression, resulting in prolonged impulse latencies and, consequently, motor retardation and clumsiness in hand function. Moreover, patients do not always understand medical terminology and may use the term pain to describe the tingling, heavy, or numb sensations occurring with median nerve compression. In the current study, pain was identified as strongly associated with a patient’s desire to seek surgical intervention; therefore, it should be recognized as an important component of CTS symptoms and receive adequate attention in treatment by occupational therapists. The other clinical implications of this study are as follows:
An 8-wk program of wrist splinting and structured education can effectively improve symptoms in people with CTS.
Structured education programs for CTS should include knowledge of the disease, risk factors, risk assessment, and goal setting.
Reliable outcome measures such as the Boston Carpal Tunnel Questionnaire provide information to enhance clinical decision making.
Patients whose symptoms do not resolve should seek further medical advice.
Implications for Occupational Therapy Research
The relatively short-term monitoring of participants over 8 wk in the current study provided insufficient information to draw conclusions concerning the long-term effects of splinting and education for CTS patients. In reviewing the effectiveness of splinting and task modifications in alleviating the CTS symptoms of 75 patients, Burke et al. (2007) reported that 18 to 30 mo after conservative treatment, 44% did not require a referral to the hand surgery unit for 23.9 mo on average (range = 18–30 mo). A study with a longer follow-up period of up to 1 yr would provide more reliable information regarding the long-term impacts of the conservative treatment on CTS patients.
Further research into the conservative management of CTS is crucial to support evidence-based practice in occupational therapy. The splint protocol in the current study supported patients’ wrist in a comfortable neutral position with full-time wear. Further investigation should include a longitudinal study of the role of the occupational therapist in enhancing the management of CTS in primary care, wrist splint wearing times, splint design, and the use of tendon and nerve gliding exercise in alleviating CTS symptoms.
Conclusion
A conservative treatment program including full-time splinting and formal education as key components can improve symptoms and hand function in patients with CTS. The CTS conservative treatment program used in the current study has been incorporated into a clinical pathway used in the management of CTS patients referred to the authors’ hospital. Conservative management should be considered for symptom reduction in all patients awaiting surgical intervention and as an option for symptom management of patients with CTS.
Footnotes
Acknowledgments
We thank the medical and allied health professionals working in the Hand and Upper Limb Clinic and the Plastics and Orthopaedic Surgery Department of SCGH.
Summary of Carpal Tunnel Syndrome Conservative Treatment Program
| Treatment Session | Therapeutic Interventions or Activities |
| Week 1 |
Provide splint prescription and fitting. Give patient splint instructions handout and explain that he or she is to wear splint full time for 8 wk. Give patient education handout “What Is Carpal Tunnel Syndrome?” Instruct patient to remove splint (Figure A1) for showering or wet activities. |
| Weeks 2–4 |
Complete splint checklist assessment form and necessary splint adjustments. With the therapist guiding the 1:1 session, complete the Assessment of Risk Factors and Education for CTS form with patient: - Focus on identification of risk factors, including sleeping postures, repetition, postures, force, and environmental and psychosocial factors. - Record problems or potential risk factors. - Review solutions checklist for each risk factor. - Formulate action plan by summarizing solutions checklist. - Set target dates for implementing solutions. |
| Weeks 5–8 |
Review patient education content and use risk factor form to review patient’s progress with action plan formulated in Session 2. Provide splint follow-up or adjustments if required. |
Note. This appendix provides an abbreviated version of the treatment manual. The complete version can be obtained from Hoe C. Lee.