
Abstract
Keywords
Children with developmental coordination disorder (DCD), disorders of attention (e.g., attention deficit hyperactivity disorder [ADHD]), specific learning disabilities (LD; e.g., speech and language disorders, specific reading disabilities), and sensory integrative (SI) dysfunction often have similar or overlapping symptoms such as diminished attention, diminished motor coordination, and reading or mathematical disturbances (American Psychiatric Association [APA], 2000). Although the severity of children’s disability can vary, their symptoms are often not readily visible compared with the more prominent symptoms of children with severe neurological or cognitive disabilities (Pellegrino, 2007). Therefore, we use the term mild disabilities when referring to this group of children. This term has previously been used in occupational therapy (Munkholm, Berg, Löfgren, & Fisher, 2010) and educational research (Cook, 2001) to refer to such children.
Children with mild disabilities also have in common that their primary symptoms significantly interfere with activity of daily living (ADL) task performance (APA, 2000; Barkley & Fischer, 2011). Previous research that has examined ADL ability of children with mild disabilities has mainly been based on self-report by the children or proxy report by their parents (Dunford, Missiuna, Street, & Sibert, 2005; Dunn, Coster, Orsmond, & Cohn, 2009; Rodger et al., 2003; Summers, Larkin, & Dewey, 2008; Wang, Tseng, Wilson, & Hu, 2009). However, valid instruments for evaluating ADL performance problems of children with mild disabilities are lacking (Blank, Smits-Engelsman, Polatajko, & Wilson, 2012; Geuze, Jongmans, Schoemaker, & Smits-Engelsman, 2001).
The Assessment of Motor and Process Skills (AMPS; Fisher & Jones, 2012a, 2012b) is an internationally standardized observational assessment of ADLs in which a person is rated on the quality of his or her performance on 16 ADL motor and 20 ADL process items (performance skills) observed during two chosen and relevant ADL tasks that present a challenge. More specifically, the ADL motor and ADL process items of the AMPS encompass small, observable units of ADL task performance (e.g., grasping, choosing, and lifting a toothbrush and then initiating brushing one’s teeth). When these actions are linked together, they result in a chain of actions that reflect ADL task performance, not underlying body functions (Fisher, 2009). The ADL motor and ADL process items are rated in terms of any observed increase in physical effort or clumsiness, decrease in efficiency, and decrease in safety or need for assistance during ADL task performance. Afterward, the item scores for each observed ADL task are entered into the AMPS scoring program (AMPS Project International, 2010), which is used to implement many-facet Rasch (MFR) analyses to convert the person’s raw item scores into an ADL motor ability measure and an ADL process ability measure. These ADL ability measures are adjusted during the MFR analysis to account for the challenge of the ADL tasks observed and the severity of the rater who scored the performance (Fisher & Jones, 2012a).
Extensive evidence supports the validity of the AMPS ADL measures (Fisher & Merritt, 2012), including that the AMPS is valid for people with diverse disabilities. For example, Kottorp, Bernspång, and Fisher (2003) compared 178 people with mild intellectual disabilities and 170 people with moderate intellectual disabilities and found that the ADL motor and ADL process item hierarchies remained stable between groups. When the ADL performance of 50 children with spina bifida was compared with that of a matched sample of children without a diagnosis, the ADL motor and ADL process ability measures were sensitive enough to discriminate between groups (Peny-Dahlstrand, Ahlander, Krumlinde-Sundholm, & Gosman-Hedström, 2009). The AMPS measures have also been shown to detect age-related differences in ADL ability in people ages 3–93 (Hayase et al., 2004) and to be free of gender (Merritt & Fisher, 2003) and cross-regional bias (e.g., Gantschnig, Page, & Fisher, 2012).
Earlier studies of observed ADL task performance among children with mild disabilities have all used the AMPS, and findings have varied. For example, Gol and Jarus (2005) compared 24 children without a diagnosis or symptoms suggestive of a mild disability and 27 children with ADHD, ages 5–8, and found a significant difference in mean ADL process ability between groups but no significant difference in mean ADL motor ability. In contrast, significant differences were found in both mean ADL motor and ADL process ability when White and Mulligan (2005) compared ADL performance in 21 children without a diagnosis and 12 children with ADHD (ages 5–13), and again when White, Mulligan, Merrill, and Wright (2007) compared ADL performance of 30 children without a diagnosis with that of 38 children with sensory processing deficits (ages 5–13).
These conflicting results and small sample sizes support the need to verify, with a larger, international sample, whether the ADL motor and ADL process ability measures of the AMPS are valid for identifying ADL problems among children with mild disabilities. Therefore, our aim in this study was to evaluate whether the ADL motor and ADL process ability measures of the AMPS are valid for detecting differences in ADL ability between (1) children without a diagnosis or any symptoms suggestive of having a mild disability and (2) children with mild disabilities. More specifically, we hypothesized that the two groups would differ significantly in ADL ability and that differences could be detected at all ages from 4 to 15.
Method
Research Design
This study was a retrospective, cross-sectional study based on data extracted from the international AMPS database (Center for Innovative OT Solutions, Fort Collins, CO). The use of preexisting, anonymous data from the AMPS database for this study was approved by the Regional Ethical Review Board, Faculty of Medicine, Umeå University, Sweden (Dnr03–509). The Ethics Committee of Canton Zurich confirmed that the secondary analysis of anonymous medical data does not need to be submitted to the Ethics Committee in Switzerland.
Participants
The participants for this study were selected from the international AMPS database in May 2011 if they met the following inclusion criteria: (1) were between ages 4 and 15 yr; (2) were without a diagnosis, at risk for (i.e., not diagnosed but having symptoms suggestive of a mild disability) or diagnosed with mild disabilities (i.e., ADHD, DCD, LD, or SI); and (3) had no other neurological disorders (e.g., traumatic brain injury, cerebral palsy), pervasive developmental disorder, mental health problem (e.g., childhood depression), or intellectual disability. We chose age 4 as the lower boundary because although the AMPS database includes data for persons age 2 and older, the data for children with mild disabilities at ages 2 and 3 were insufficient. We selected age 15 as the upper boundary because both ADL motor and ADL process abilities increase until age 15 and then plateau between ages 16 and 50 (Hayase et al., 2004). Note that the sample of children with mild disabilities in the AMPS database includes children typical of those commonly referred to occupational therapy for evaluation or intervention, but they may not be representative of the entire population of children with mild disabilities because many are not referred for occupational therapy services.
We excluded children who had been scored by raters in an invalid manner (i.e., were not free of rater scoring error, which can occur when raters are unexpectedly lenient or strict). For more details, see Fisher and Jones (2012a, Chapter 14). An analysis with an anticipated effect size of ≥.80, α = .05, and power of .80 revealed a needed sample size of 21 in each group for the probability of finding significant group differences when differences really exist. We did not match the group of children with mild disabilities with the group of children without a diagnosis because of the preferred premise of using the largest possible sample (Zumbo, 1999). Demographic data of the participants are presented in Table 1.
Demographic Data: Gender, Diagnosis, and Age Characteristics of Participants
Note. Typical = children without a diagnosis; mild = with mild disabilities; risk = children with symptoms suggestive of a mild disability; ADHD = attention deficit hyperactivity disorder; DCD = developmental coordination disorder; LD = specific learning disabilities; SI = sensory integrative dysfunction; comorbid = children with two or more diagnosed mild disabilities. NA = North America; UK/Ireland = United Kingdom and Republic of Ireland; Nordic = Nordic countries; SoCenAm = South and Central America and Caribbean; WEurope = Western Europe; ANZ = Australia and New Zealand; MidEast = Middle Eastern countries; MEurope = Middle Europe; SEurope = Southern Europe.
The participant data had been submitted to the AMPS database by 4,678 occupational therapists from different world regions who had taken AMPS training courses and been calibrated as valid and reliable AMPS raters. All participants were evaluated using the AMPS according to standardized testing procedures as outlined in the AMPS manuals (Fisher & Jones, 2012a, 2012b). These procedures require that all participants be observed performing two familiar and relevant ADL tasks that present at least minimal challenge and are chosen by the participant from among more than 120 ADL tasks included in the AMPS manuals. All AMPS observations were carried out in naturalistic environments (e.g., kitchens, bedrooms), either community based or clinical, and the AMPS rater ensured that the child was completely familiar with the test environment before initiating the AMPS observations.
Data Analysis
We first generated the ADL motor and ADL process ability measures for each child using FACETS, an MFR analysis computer program (Linacre, 2011) that is used to convert ordinal ADL motor and ADL process item raw scores into linear ADL motor and ADL process ability measures expressed in logits (log-odds probability units; Bond & Fox, 2007). The specific feature of the MFR model of the AMPS is that person ADL ability, rater severity, task challenge, and item difficulty are considered simultaneously and are all estimated along the same linear ADL motor and ADL process continua. We performed two MFR analyses, one to generate the ADL motor ability measures and one to generate the ADL process ability measures. In each analysis, each rater’s severity, each ADL task challenge, and each item difficulty was anchored at preestablished values based on those in the current AMPS scoring program (AMPS Project International, 2010).
We then implemented two forced regression analyses, using PASW Statistics, Version 19.0 (PASW, Chicago), to evaluate for significant differences in mean ADL motor ability measures and mean ADL process ability measures between groups. The model can be clarified with the following equation:

where Y is the mean ADL motor or mean ADL process ability measure; age, group, and Group × Age are the independent variables; β0 is the intercept; β1–3 are the effects for group, age, and Group × Age interaction; and ε is the normally distributed error. We set the level of significance for these analyses at α = .05.
Finally, we tested for differences in ADL motor and ADL process ability measures between the groups by age category using post hoc one-tailed t tests. We used Levene’s tests to evaluate for equality of variances between groups. When the results of Levene’s tests failed to support the assumption of equality of variances between groups, we used the t values for samples for which equality of variances is not assumed. We used Bonferroni multiple comparison corrections to avoid the risk of false positive results, which is known to be a conservative method for ensuring a familywise α level of .05. With 12 comparisons each for ADL motor and ADL process, the critical value for α was set at .004. As for standardized effect size, we calculated d as
Cohen’s d provides an index of how much two groups differ when compared with their pooled standard deviation. A value of .2 is considered to be a small effect size; .5, moderate; and .8, large (i.e., the standardized mean difference between groups is of crucial practical and clinical importance; Cohen, 1988).
Results
Meeting the inclusion criteria were 10,996 children between ages 4 and 15 (mean = 8.7, standard deviation = 3.2), 5,328 (48%) boys and 5,668 (52%) girls. Of these, 9,615 (87%) were children without a diagnosis and 1,383 (13%) were children at risk for or having mild disabilities. The participants were from a variety of world regions (see Table 1).
The mean ADL motor and ADL process ability measures by age for each group are shown in Table 2. The results of the first forced regression analysis revealed no significant differences between groups in mean ADL motor ability measures, B = 0.021, 95% confidence interval (CI) [−0.061, 0.103], p = .308, t = 0.503, df = 10,994, R 2 = .361. In contrast, we found a significant main effect for age, B = 0.139, 95% CI [0.129, 0.149], p < .001, t = 26.187, df = 10,994, R 2 = .361, and a significant Age × Group interaction effect, B = −0.031, 95% CI [−0.038, −0.021], p < .001, t = −6.612, df = 10,994, R 2 = .361 (Figure 1).
Differences in Mean ADL Motor and ADL Process Abilities (Log-Odds Probability Units) Between Children Without a Diagnosis and Children With Mild Disabilities
Note. The critical Bonferroni corrected value was set at α = .004. A d = 0.2 is considered to be small; 0.5, moderate; 0.8, large. ADL = activity of daily living; CI = confidence interval; df = degrees of freedom; M = mean; mild = mild disabilities or having symptoms suggestive of a mild disability; SD = standard deviation; typical = children without a diagnosis.
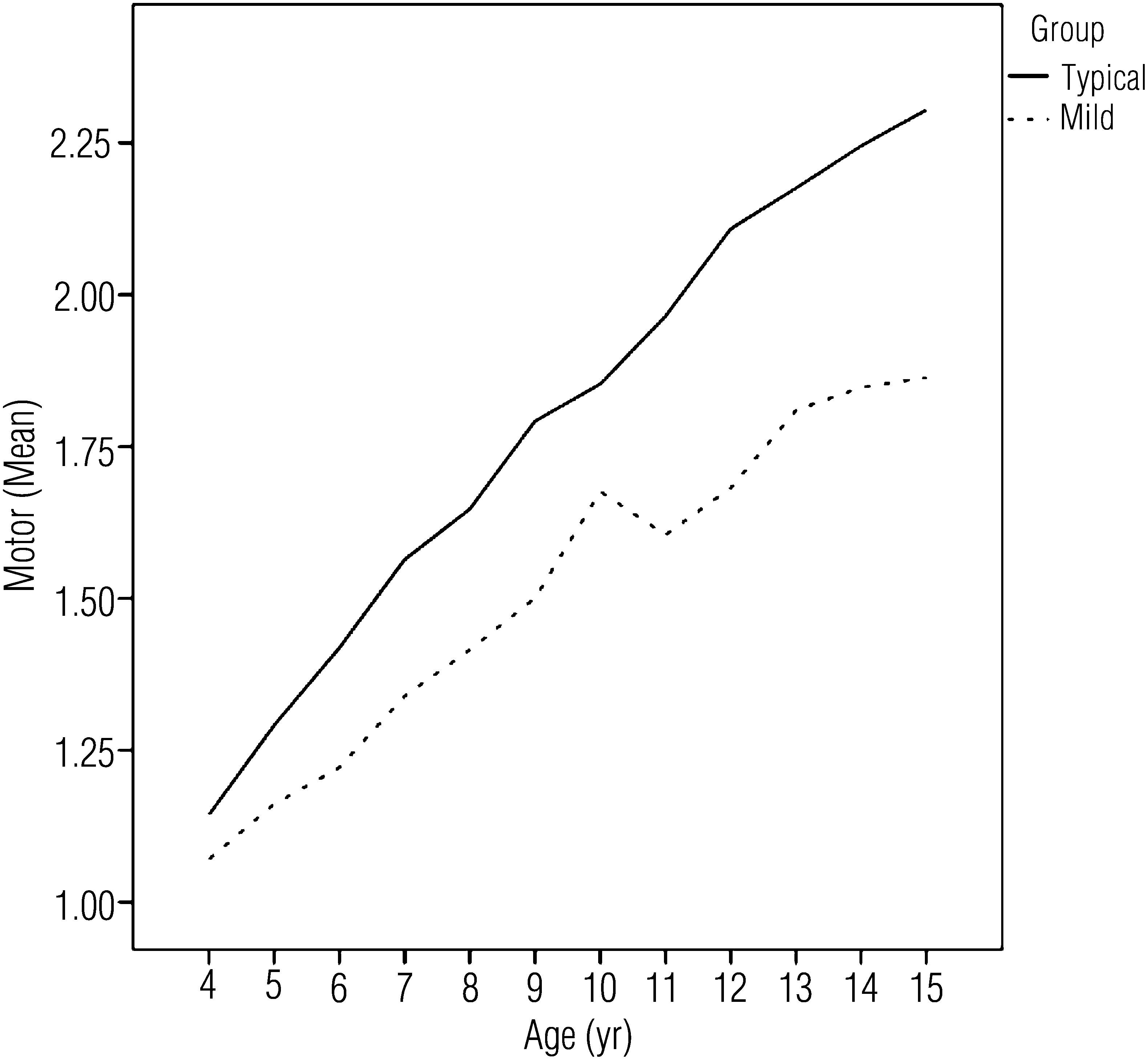
Graphic representation of differences in mean ADL motor ability measures between groups with increasing age.
The second forced regression analysis revealed significant differences between the two groups in mean ADL process ability measures, B = −0.166, 95% CI [−0.242, −0.090], p < .001, t = −4.296, df = 10,994, R 2 = .367. Moreover, we found a significant main effect for age, B = 0.122, 95% CI [0.112, 0.132], p < .001, t = 24.751, df = 10,994, R 2 = .367 and a significant Age × Group interaction effect, B = −0.027, 95% CI [−0.035, −0.019], p < .001, t = −6.204, df = 10,994, R 2 = .367 (Figure 2).
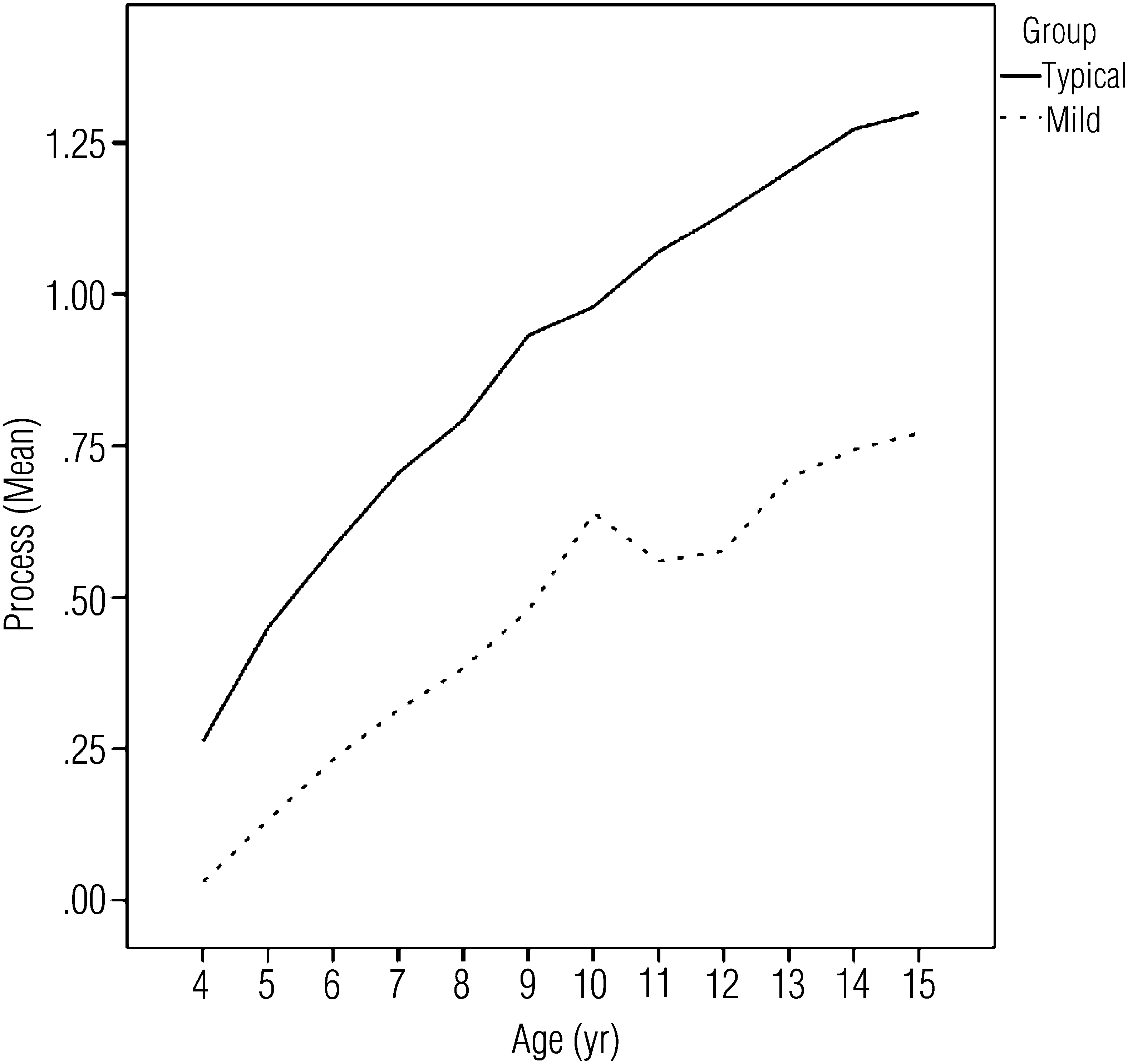
Graphic representation of differences in mean ADL process ability measures between groups with increasing age.
Given the significant Age × Group interaction effects, we proceeded to perform post hoc t test evaluations for significant group differences in ADL motor and ADL process ability at each age. With the exception of ADL motor ability measures for 4-yr-olds, the children without a diagnosis in all age groups had significantly higher mean ADL motor and ADL process ability than did the children with mild disabilities (t ≥ 3.62, p < .001; see Table 2). Effect size calculations revealed that most ADL motor effect sizes were medium to large beginning at age 7, and ADL process effect sizes were medium at ages 4 and 5 and large beginning at age 6 (see Table 2).
Discussion
As outlined earlier, our aim was to evaluate the validity of the AMPS measures for identifying diminished ADL ability among children with mild disabilities. Our results suggest that the AMPS can be used to identify problems with ADL task performance as early as age 4. The results also suggest that the ADL process measures of the AMPS are more sensitive than the ADL motor measures, because significant differences were identified at all ages (4–15) and, more important, the ADL process effect sizes were consistently moderate to large at all ages. These effect sizes are important to consider because they provide an index of the standardized group difference.
Moreover, in contrast to t values, effect sizes are independent of sample size. That is, although there might be concern that we had too much power in our data and overidentified group differences, the use of Cohen’s d suggests that power was not an issue. Large effect sizes found for ADL process ability as early as age 6 indicate that the mean differences are of crucial practical and clinical importance (Cohen, 1988). The large effect sizes emerged at this age because the diagnoses of DCD and ADHD can typically be assured at age 5 and older (APA, 2000; Blank et al., 2012).
Our results are also in line with those of earlier studies showing significant differences in mean ADL process ability measures among children without a diagnosis and children with ADHD (Gol & Jarus, 2005; White & Mulligan, 2005) and sensory processing deficits (White et al., 2007). In contrast to our findings, Gol and Jarus (2005) found no significant differences in mean ADL motor ability measures between children without a diagnosis and children with ADHD.
This study is the first designed to evaluate the validity of an ADL instrument for detecting problems in ADL task performance over a wide age span and based on observed quality of ADL task performance. An important clinical finding is that it becomes clear that the problems of at least some children with mild disabilities are clearly present during adolescence. Although the Age × Group interaction effect might even suggest that the differences between groups increase with age, our results should be interpreted with caution. That is, this study was based on cross-sectional data. Moreover, we had no available method to control for or evaluate the severity of each child’s disability, and the older children may possibly have been more severely affected. Further research, based on a prospective longitudinal design, is indicated to determine whether the extent of problems with ADLs among children with mild disabilities increase as ADL tasks become more challenging.
Although the significant interaction effect overrides the nonsignificant group main effect for ADL motor ability, it is noteworthy that there were proportionally more older children without a diagnosis, whereas the largest proportional sample sizes for the children with mild disabilities were for those who were ages 6–10. More children were also at risk in the younger age groups. These group differences may have somewhat attenuated the mean differences in ADL motor ability between groups. We chose not to match our sample on the basis of the preference for using all available data (Zumbo, 1999).
The use of a combined sample of children with ADHD, DCD, LD, or SI dysfunction might be seen as another potential limitation. We chose to include children with different diagnoses because these children face similar risks for ADL performance problems (APA, 2000). We recognize, however, that differences among these groups also exist.
Another consideration when evaluating our results is that children with ADHD, DCD, LD, or SI dysfunction do not always have ADL performance problems (APA, 2000). Our sample did, however, include those who had been referred for occupational therapy evaluation, intervention, or both. It is possible, therefore, that our sample included a higher proportion of those who do have problems with ADLs. If this is true, they may not be representative of all children with these diagnoses, but our findings can likely be generalized to those children who are referred for occupational therapy services.
The finding that problems with ADLs, especially ADL process ability, can be identified as early as age 4 suggests the possibility of developing intervention programs aimed at minimizing problems with ADL task performance. Future research needs to evaluate the efficacy of such programs to determine whether children’s ADL problems can be alleviated and whether the AMPS can be used to document the effectiveness of such interventions.
Finally, that the ADL process measures are more sensitive supports clinical observations and parental reports that although these children, especially those with DCD and SI dysfunction, are often described as being clumsy, their major difficulties are related to spatial–temporal organization of ADL task performance (e.g., slowness, buttons in the wrong holes, clothing back to front, socks upside down, and shoes on the wrong feet; Summers et al., 2008).
Implications for Occupational Therapy Practice
The results of this study suggest that
The AMPS ADL motor and ADL process measures are valid for purposes of evaluating for ADL problems among children with mild disabilities older than age 4.
The detected problems in ADL performance of children with mild disabilities are of crucial practical and clinical importance and support the need to evaluate ADL performance problems to design and implement effective occupational therapy interventions that increase children’s ADL abilities.
At least some children with ADHD, DCD, LD, or SI dysfunction have problems with ADLs that are present as they enter adulthood.
Footnotes
Acknowledgments
This study was funded by the Swiss National Science Foundation (13DPD6-127161) and supported by the Austrian, German, and Swiss Associations of Occupational Therapy. We especially thank André Meichtry and Hans Stenlund for their statistical support. We also thank all occupational therapists who collected data on their clients and contributed to the AMPS validation process.