
Abstract
Play is one of the primary occupations of children (American Occupational Therapy Association [AOTA], 2008). It is a daily occupation that takes place within a context and is influenced by the intrinsic and extrinsic elements of a child’s environments, such as personal or physical factors (Knox, 2005). These intrinsic and extrinsic elements are also influenced by a child’s sensory processing.
Sensory processing is a term that has evolved from the work of Ayres (1972a, 1979); it refers to the process and organization of sensations for use throughout daily occupations (Fisher & Murray, 1991). For children, their daily occupations include play (Canadian Association of Occupational Therapists, 1996; Couch, Deitz, & Kanny, 1998; Rodger, 2010). Ayres (1979) believed that “play consists of the adaptive responses which make sensory integration happen” (p. 7).
Reilly began an extensive investigation into the area of play within occupational therapy practice (Parham, 1996); she explored the many facets of play using an occupational perspective (Reilly, 1974). The initial understanding of the relationship between play and sensory processing was that children with sensory processing difficulties exhibited decreased ability to play, such as less active play, more sedentary play, less socially interactive play, and shorter periods of time in play with toys (Bundy, Shia, Qi, & Miller, 2007; Schaaf, Merril, & Kinsella, 1987). Lindquist, Mack, and Parham (1982) explained this link by stating that “sensory integration is viewed as an ongoing process that underlies the development of play; play experiences, in turn, influence the development of sensory integration” (p. 437). The link between sensory processing and children’s participation in daily occupations has received some attention in the empirical literature to date (Ashburner, Ziviani, & Rodger, 2008; Brown & Dunn, 2010; Dunn, 2007; Koenig & Rudney, 2010).
In the late 1980s, Bundy and colleague (Bundy, 1989; Clifford & Bundy, 1989) began to examine play and sensory processing in an attempt to understand the relationship between the two constructs. Contrary to the belief that children with sensory processing difficulties exhibit poor play, Bundy (1989) suggested that children with sensory integrative (processing) difficulties may compensate for their deficits and exhibit play within the normal range for their peers (Clifford & Bundy, 1989). Bundy (1991, 2002) stated that poor tactile discrimination or poor motor coordination does not always result in a disruption of play skills. She argued that sensory processing provides just one foundation for play and that there are many other influences on children’s play. Indeed, Bundy et al. (2007) noted that “because deficits in sensory processing interfere with the ability to interact with people and objects, it seems logical that children with sensory processing disorder (SPD) may have difficulty playing” (p. 201).
To explore the relationship between play and sensory processing in children, we undertook a systematic review of literature. The research question was, What is the relationship between sensory processing and play in children ages 3–12 yr? The aims of the systematic review were to identify (1) how much research has been undertaken in this area and (2) the quality of the evidence available. To enable clarity in the systematic search of the literature, we defined play and sensory processing.
Defining Play
For this review, play was defined as activities that, among other characteristics, have internal motivation, have freedom from external rules, transcend reality as well as reflect reality, focus on means rather than ends, are spontaneous and safe, and require active participation of the player (Reilly, 1974; Stagnitti, 2004). Play involves social competence, communication, cognition, symbolic use of objects, motor ability, and organizational and adaptive skills (Bundy, 1991, 2002; Stagnitti, 2004). It is influenced by the environment (such as play materials) and interactions with the physical and social environment.
Defining Sensory Processing
Ayres (1979) described the brain as a sensory processing machine whereby the brain senses stimuli and processes and integrates the stimuli into the central nervous system, enabling the body to respond adaptively as the sensory information is used to plan and organize behavior (Ayres, 1972a, 1979; Fisher & Murray, 1991). Ultimately, sensory processing consists of receiving, integrating, and reacting to sensations (Fisher & Murray, 1991). Ayres (1979) defined this process as “the organization of sensation for use” (p. 5). Since 1972, several terms have evolved within the field, and AOTA recommended changes to the terminology with the aim to provide clarity within the field (Miller, Anzalone, Lane, Cermak, & Osten, 2007; Miller, Cermack, Lane, Anzalone, & Koomar, 2004). Miller et al. (2004) proposed that sensory processing disorder be used as the global term and that under this term sit the subtypes of sensory modulation disorder, sensory discrimination disorder, and sensory-based motor disorder.
Dunn (2007) formulated a model of sensory processing that hypothesized a connection between a person’s nervous system and strategies for self-regulation. A continuum of neurological thresholds is a core concept in Dunn’s (2007) model. For example, people who have a low threshold for sensory stimuli do not need strong input to notice the stimuli, whereas if they have a high threshold they often miss noticing stimuli. The other core concept is self-regulation, and this, too, is on a continuum in which people are either passive or active in their reaction to sensory input. Where these two continua intersect, Dunn proposed four patterns of sensory processing: sensory seeking, sensory avoiding, sensory sensitivity, and low registration. Dunn’s four patterns of sensory processing have been conceptualized by Miller et al. (2004) as sensory modulation disorder (which includes sensory overresponsivity, sensory underresponsivity, and sensory craving). Miller et al. included sensory modulation disorder as a subtype of sensory processing disorder.
Method
We followed the PRISMA guidelines (Moher, Liberati, Tetzlaff, & Altman, 2009) in conducting this systematic review. We searched the key databases Academic Search Complete, CINAHL with Full Text, Cochrane Library, Embase, ERIC, Global Health, Health Source, Nursing/Academic, Medline with Full Text, OTseeker, PEDro, PsycARTICLES, PsycINFO, and PubMed. The following key words were used during the database searches: play, leisure, sensory processing, sensory integration, sensory, sensorimotor, proprioception, children, kids, occupational therapy, Anita Bundy, Winnie Dunn, and Lucy Miller.
In addition, we conducted a hand search of the British Journal of Occupational Therapy, Australian Occupational Therapy Journal, American Journal of Occupational Therapy, and Canadian Journal of Occupational Therapy. Hand searching of journals was limited to journals published from 2007 to 2012 because of accessibility of journal issues kept in the university library. Reference lists in book chapters and books were searched for relevant literature.
Finally, we contacted key scholars in the field of play and sensory processing, including those undertaking doctorates in the area, by email or post to inquire of their knowledge of any publications on the topic. Responses were received from two researchers.
In determining which studies to include, we defined play broadly. For example, play was understood to include physical or sensory exploration of toys and the environment, time spent in manipulation of objects or toys either alone or with others, and spontaneous engagement of the child. Play included abilities such as imaginative play, manipulation, social interaction, or fine and gross motor skills. Included studies had to meet the following additional inclusion criteria: Data were collected on play; sensory processing was defined and measured; the study was a published research study; data gathering methods or assessment were included; children ages 3–12 yr were in the sample; the study was published during the years 1990 to 2012; and the study was peer reviewed, available in full text, and published in English. The last four criteria allowed direct accessibility to research studies and a deeper understanding of methodologies and results that cannot be obtained from an abstract. The identification of studies is presented in Figure 1. Articles were excluded if they did not meet the inclusion criteria, for example, the sample included adults, the study was not published in English, or methods did not include data gathering for sensory processing or play ability.
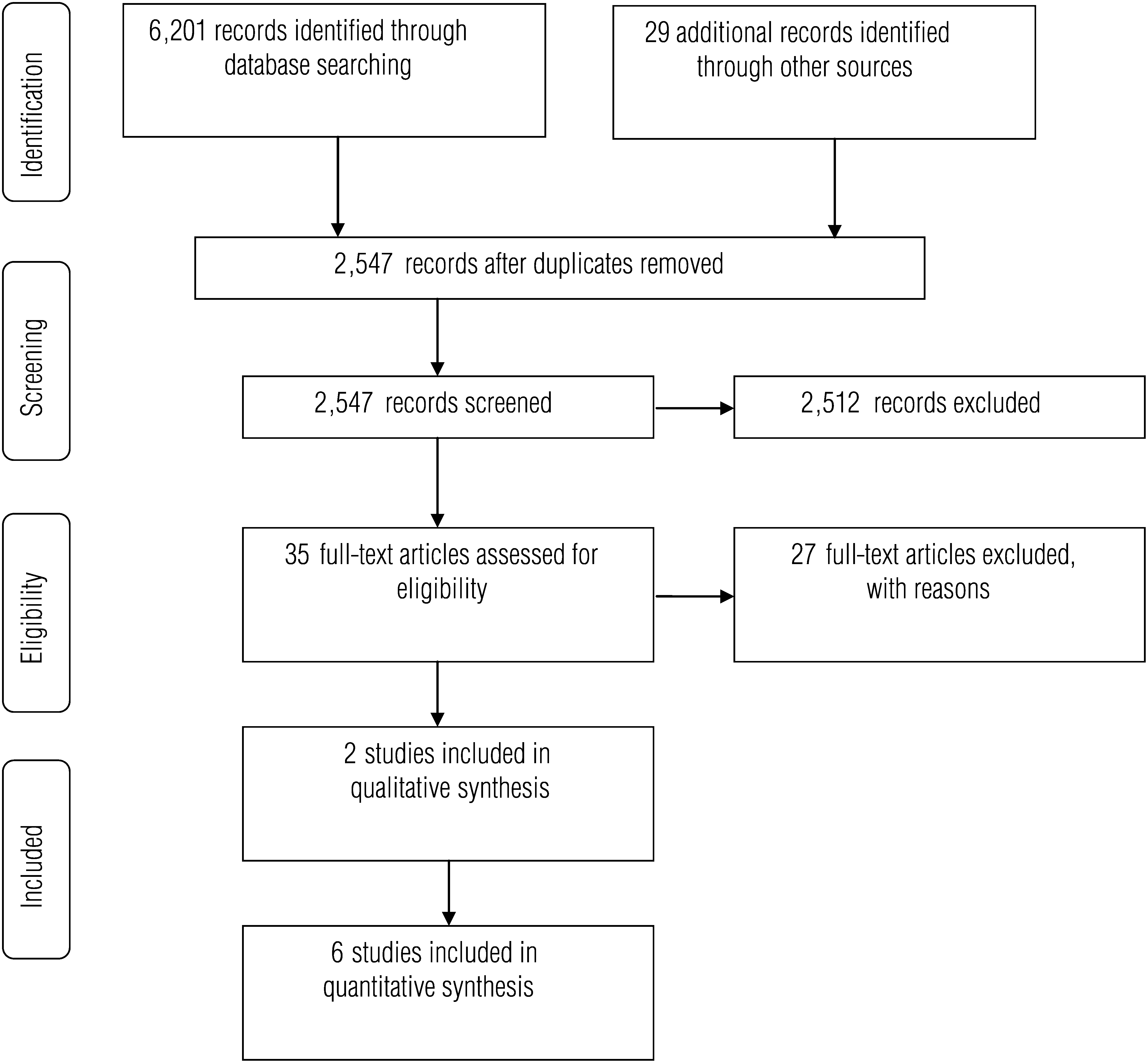
Identification of Studies. From “Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement,” by D. Moher, A. Liberati, J. Tetzlaff, D. G. Altman, & The PRISMA Group, 2009, PLOS Medicine, 6, e1000097. http://dx.doi.org/10.1371/journal.pmed.1000097. © 2009 by the authors. Used under the terms of the Creative Commons Attribution License.
Results
Electronic and hand searching of literature yielded 2,547 articles after duplicates were removed (see Figure 1). After screening, we assessed 35 full-text articles for eligibility, and of the 35, 8 studies met the inclusion criteria. Of the 8 studies, 2 were qualitative studies and 6 were quantitative studies. All studies were conducted in the United States. The 2 qualitative studies presented a single case report on a child with sensory processing deficits. Of the 6 quantitative studies, 2 studies used a comparison design to examine children with sensory processing disorder or autism spectrum disorder (ASD) against typically developing children and 4 studies used correlational designs. The 8 studies are summarized in Table 1.
Synthesis of Studies Examining Play and Sensory Processing (SP) in Children by Level of Evidence
Note. ASD = autism spectrum disorder; NHMRC = National Health and Medical Research Council; SI = sensory integration; SPD = sensory processing disorder.
Critical Appraisal and Level of Evidence
The sample of 8 studies was appraised according to their quality (scientific rigor and lack of bias) and level of evidence, also reported in Table 1. To critically appraise each article before a level of evidence was given, a McMaster Critical Review Form was completed for each study. That is, the McMaster Critical Review Form–Quantitative Studies was completed for 6 studies and the McMaster Critical Review Form–Qualitative Studies was completed for 2 studies (Law et al., 1998; Letts et al., 2007).
Articles were then assigned a level of evidence. The Australian National Health and Medical Research Council’s (NHMRC; 1998) levels of evidence were used to assign evidence levels for quantitative studies. The Rosalind Franklin–Qualitative Research Appraisal Instrument (Henderson & Rheault, 2004) was used to assign evidence levels for the qualitative studies. The NHMRC (1998) has six levels of evidence; Level 6 is the highest (e.g., systematic reviews) and Level 1 is the lowest (e.g., case series with either posttest or pretest–posttest outcomes; NHMRC, 2007). The Rosalind Franklin–Qualitative Research Appraisal Instrument has five levels of evidence, which reflect a study’s credibility, ability to be transferred to other situations, dependability, and attempts to enhance objectivity by reducing bias (Henderson & Rheault, 2004).
Key Findings
Studies Conducted in United States.
All studies were conducted in the United States. Because the origins of occupational therapy research into sensory integration theory originated in the United States (Ayres, 1972a, 1979; Dunn, 1999; Reilly, 1974), this finding is not surprising.
Delayed Level of Play.
Four studies found that children with sensory processing problems had a delayed level of play compared with peers (Baranek et al., 2002; Benson, Nicka, & Stern, 2006; Cosbey, Johnston, Dunn, & Bauman, 2012; Reynolds, Bendixen, Lawrence, & Lane, 2011). Using a nonstandardized play observation method to gather information on a child’s play, Benson et al. (2006) found that the child in their case study was less likely to explore and more likely to imitate previously seen play scenes (such as a movie plot) than spontaneously add original ideas to his play. The child had a limited play repertoire that was not typical of his peers. Baranek et al. (2002) determined that children with sensory issues had decreased engagement in play compared with peers and therefore decreased occupational performance in play. Using the Child Behavior Checklist: Competence Scales (Achenbach & Rescorla, 2001) to assess play quality, Reynolds et al. (2011) ascertained that children with sensory processing issues had less involvement in dramatic play such as “playing school” (p. 1502) or play scenes that involved socially interacting with other children.
Reynolds et al. (2011) examined children with a diagnosis of ASD. Play ability deficits in children with ASD are well documented, with evidence of play in these children being restricted, being stereotypical, having a preference for tactile and gustatory exploration of toys to visual exploration, having less variety in functional play, and having difficulties with pretend play and stereotyped repetitive play (Baron-Cohen, 1996; Naber et al., 2008; Roley & Jacobs, 2008). In Benson et al.’s (2006) study, one child had developmental delay and motor coordination difficulties, whereas in Baranek et al.’s (2002) study the children had a diagnosis of fragile X syndrome. Children who have cognitive deficits because of fragile X syndrome or a developmental delay can encounter difficulties in their play (Roley & Jacobs, 2008).
The children in Cosbey et al.’s (2012) study were typically developing or had a diagnosis of sensory processing disorder with no other concerns. Cosbey et al. found that children with SPD had a limited ability to respond to social cues and resolve conflict within play. The children with SPD displayed less engagement in mature socially based play compared with their peers.
These 4 studies revealed that a child’s sensory processing affected negatively their level of play; however, 3 of these studies included children who had a diagnosis with already-known difficulties in engaging in play. More research is needed.
Play Preferences.
Children’s play preferences appear to be influenced by sensory preferences (Mische Lawson & Dunn, 2008; Welters-Davis & Mische Lawson, 2011). Mische Lawson and Dunn (2008) found that children who were sensory seeking sought toys that met their sensory needs, such as creative art toys or building blocks the child would knock down. Welters-Davis and Mische Lawson (2011) explored the relationship between the parent’s play and sensory processing preferences and their child’s play preferences. They used the Parent–Child Play Scale (Dunst, 1986) to measure play and the Sensory Profile (Dunn, 1999) to measure sensory processing of the child. Welters-Davis and Mische Lawson found that parents chose toys or offered play opportunities that suited the parent’s play and sensory preferences, thereby influencing the child’s preferences.
Responding to Therapy Methods.
Schaaf (1990) examined the play behavior of a child and the effect of occupational therapy sessions using sensory integration. Schaaf found that the sensory integration–focused sessions increased the child’s tactile-based activities and imaginative play. After the therapy sessions, the child was also found to have an increase in social interactions and improved attention span. Data were gathered using the Southern California Sensory Integration Tests (Ayres, 1972b) and the Parent/Teacher Play Scale (Schaaf et al., 1987).
DeGangi, Wietlisbach, Goodin, and Scheiner’s (1993) study compared sensory integration therapy with a child-centered, play-based approach. Children were assessed before and after intervention using the Functional Emotional Assessment Scale (Greenspan, 1992), Touch Inventory for Preschoolers (Royeen, 1987), and DeGangi–Berk Test of Sensory Integration (Berk & DeGangi, 1983). Children were observed to make considerable gains in sensory processing skills from both therapy methods (70% gain from structured sensory integration therapy and 56% gain from child-centered therapy; DeGangi et al., 1993). Although there were no conclusive findings for play behavior and skills, DeGangi et al. concluded that child-centered therapy was more beneficial for organizing play and developing play skills, whereas structured sensory integration therapy appeared to be more beneficial for the development of gross motor play skills and other functional skills.
Measurement of Play and Sensory Processing.
In 6 studies, the play measures used were devised for the study or observations of children’s play. Three studies measured play through play items embedded within other scales. For example, the Functional Emotional Assessment Scale (Greenspan, 1992) was used in DeGangi et al.’s (1993) study and the Child Behavior Checklist: Competence Scales (Achenbach & Rescorla, 2001) were used by Reynolds et al. (2011). No studies assessed play using standardized instruments.
In all studies, sensory processing was measured through standardized assessments such as the Sensory Profile (Dunn, 1999). The internal consistency of the Sensory Profile Cronbach’s coefficient alpha ranged from .47 to .91 (Dunn, 2008). These values indicate poor to good reliability (Portney & Watkins, 2009). We found evidence of convergent validity with significant correlations with the Sensory Processing Measure (Brown, Morrison, & Stagnitti, 2010; Parham, Ecker, Miller Kuhaneck, Henry, & Glennon, 2007). Construct validity evidence in the form of factor analysis results is reported in the Sensory Profile manual (Dunn, 1999). Evidence of the Sensory Profile being able to discriminate between groups with known differences has also been reported (Brown, Leo, & Austin, 2008; Tomchek & Dunn, 2007).
Discussion
The relationship between sensory processing and play in children is “not simple, nor is it clear” (Bundy, 1991, p. 65). Although this systematic review generally upholds Bundy’s (1991) view, some findings, which have implications for practice, do contribute toward understanding this relationship. Children with sensory processing issues appear to have a delayed level of play, particularly in the complexity of their social play, and a decreased duration of time engaging with toys and objects, and they prefer toys that satisfy a sensory need. For example, children who were identified as having sensory seeking issues sought out play materials that could be interpreted as having sensory properties (Mische Lawson & Dunn, 2008). The selection of play materials by children, however, is further complicated: Welters-Davis and Mische Lawson (2011) found that children’s play preferences can be influenced by the play and sensory preferences of the parent. Case study evidence suggested that sensory integration therapy does affect a child’s play (Schaaf, 1990), but the type of play appears to be limited to gross motor play (DeGangi et al., 1993).
The level of evidence for the relationship between sensory processing and play is low to medium. Three studies did not isolate the influence of a child’s diagnosis from the child’s sensory processing. Educators should be cautious in teaching about the relationship between sensory processing and play because the evidence needs more rigor.
Limitations and Future Research
This review included only articles that were published in English and available in full text. There was a consensus in the literature on what defines sensory processing, and all the articles measured sensory processing with a standardized measure. Defining play, however, was less clear. In this review, play was defined in terms of play materials, active and spontaneous participation of the child, and types of play. This broad definition of play allowed the inclusion of more articles than if the definition of play had been focused only on certain types of play (e.g., imaginative play, gross motor play, fine motor play). This broad definition also made answering the research question more difficult because across the sample of articles, none of the studies used a standardized measure of play.
In terms of the research found to answer the question, 3 studies had the confounding variable of including children with a diagnosis in which play ability is already known to be limited. For example, children with ASD have been reported to have repetitive play and difficulty with social and imaginative play (Naber et al., 2008).
This review has highlighted that there is still a need for high-quality quantitative, qualitative, and mixed-methods research to understand the relationship between sensory processing and play. In 1989, Bundy highlighted that research in the area of sensory processing was limited, and she proposed that further research was necessary (Bundy, 1989; Clifford & Bundy, 1989). A more in-depth understanding of this relationship would give occupational therapy practitioners valuable insight into how sensory processing difficulties in children affect their play and whether and how sensory processing and play influence each other. Many questions remain to be answered, such as, Does play have a more direct impact on sensory processing or vice versa? What is the relationship between exploratory play and sensory processing in children? We recommend that future studies add more rigor to the methods by having samples of children who present with sensory processing disorder with no other diagnoses; using standardized measures of play and sensory processing that are valid, reliable, and sensitive to change; and using a large number of children in a cohort study to allow for multivariate analysis of data.
Implications for Occupational Therapy Practice
Why is research in this area so important to occupational therapy practitioners? Understanding the relationship between play and sensory processing in children would have the following implications for occupational therapy practice because practitioners could
Guide therapy focus and the development of intervention through evidence-based practice,
Ensure that children receive the best possible therapy, and
Highlight the importance of play and sensory processing for the development of the child.
The relationship between play and sensory processing in children is still in need of further exploration so that occupational therapy practitioners can fully understand this relationship and develop more targeted interventions.