
Abstract
Keywords
Every day in the United States and throughout the world, many children are born low birthweight (LBW) or preterm (World Health Organization [WHO], 2013). Birthweight is the first weight measurement obtained after birth. Newborns who weigh <2,500 g are classified as LBW (WHO, 2013). According to the National Vital Statistics Report of 2010, the U.S. LBW rate was 8.15% of total births (Martin et al., 2012). Preterm birth occurs when a child is born before 37 wk gestation or is fewer than 259 days gestational age (WHO, 2013). An estimated 28% of neonatal deaths are attributable to preterm births (excluding children born with malformations; Beck et al., 2010). Although data are insufficient to estimate the global incidence of preterm birth, some developed countries, such as the United States, the United Kingdom, and the Scandinavian countries, have had a dramatic rise in preterm births over the past 20 yr (Blencowe et al., 2012). Preterm birth is usually associated with LBW.
Children born prematurely have higher rates of mental function deficits and neuromusculoskeletal and movement-related dysfunctions during their first years of life compared with children born at normal birthweight or full term (Beck et al., 2010). Deficits in mental functions and neuromusculoskeletal and movement-related functions in children born LBW or preterm may have important effects on school readiness and academic achievement (Aarnoudse-Moens, Smidts, Oosterlaan, Duivenvoorden, & Weisglas-Kuperus, 2009; Anderson & Doyle, 2003 ; Bora, Pritchard, Moor, Austin, & Woodward, 2011; Gidley Larson et al., 2011). Dysfunctions such as cognitive deficits, learning disabilities, attention problems, behavioral problems, and neuropsychological deficits become evident in approximately 50%–70% of children born prematurely when they reach school age (Sullivan & Hawes, 2007). Cognitive impairments, including difficulties with phonological processing, attention, and executive functions, are associated with lower academic attainment and poorer educational outcomes (Johnson, Wolke, Hennessy, & Marlow, 2011).
The first few years of life are crucial for any child, and it is vitally important that children reach each developmental milestone to prepare them for success in their school-age and adult occupations. Infants and children born LBW or preterm can benefit greatly from early intervention and family education at an early age (Parlakian, 2003). Multidisciplinary team members, such as occupational and physical therapy practitioners, nurses, and physicians, deliver early intervention services and education to infants and children born LBW or preterm, and the families are very much involved in the process (Feldman, Eidelman, Sirota, & Weller, 2002; Gardner, Walker, Powell, & Grantham-McGregor, 2003; Johnson, Ring, Anderson, & Marlow, 2005; Nordhov et al., 2010; Sajaniemi et al., 2001).
Defining early intervention is not an easy task; the term has been defined in many different ways. According to the National Center for Infants, Toddlers, and Families, early intervention consists of identifying that an infant or a child is having developmental problems and other issues that could affect his or her life (Parlakian, 2003). The Individuals With Disabilities Education Improvement Act of 2004 (IDEA 2004) stipulates that infants and toddlers ages 0–3 yr who are eligible should be provided early intervention (Part C) services and an individualized family service plan (IFSP) as soon as their issues have been detected to prevent further problems and help them succeed in life (Opp, 2009). Additionally, the law supports the transition to appropriate services such as special education or preschool services under IDEA Part B for children and youth ages 3–22 yr if the multidisciplinary team finds them still to be eligible for additional services to address cognitive, physical, communication, social or emotional, or adaptive development. The American Occupational Therapy Association has defined early intervention as a group of therapies and services offered to infants and children with developmental delays and their families (Opp, 2009).
It has long been hypothesized that early intervention produces positive outcomes when introduced in the appropriate time frame (Wood, 1981). To understand the effect of early intervention on infants born LBW, Ohgi, Fukuda, Akiyama, and Gima (2004) provided a Neonatal Behavioral Assessment Scale–based intervention combined with developmental support for 12 high-risk LBW infants. The early intervention group had higher scores on the Bayley Mental Developmental Index than the comparison group, who received routine medical nursing care without early intervention (Ohgi et al., 2004).
In another study, Lekskulchai and Cole (2001) investigated motor performance in three groups of infants born preterm: 43 infants in an intervention group, 41 infants in a control group, and 27 low-risk infants in a comparison group. The early developmental intervention program comprised 12 activities, including home-based activities, and motor performance was assessed using the Test of Infant Motor Performance (Campbell, Kolobe, Osten, Lenke, & Girolami, 1995). The preterm infants who received early intervention showed greater motor progression than the preterm infants who did not receive the intervention (Lekskulchai & Cole, 2001).
Studies on early intervention have used different tools and assessments, making it difficult to categorize specific treatment activities or interventions as early intervention (Gianní et al., 2006; Kaaresen et al., 2008; McCormick et al., 2006; Melnyk et al., 2001; Olafsen et al., 2006; Tessier et al., 2003; Teti et al., 2009; Westrup, Böhm, Lagercrantz, & Stjernqvist, 2004). To investigate the association between early intervention and improvement in mental or neuromusculoskeletal and movement-related functions in children born LBW or preterm, a meta-analysis is ideal because the analyses account for variability in intervention by standardizing scores. Therefore, the purpose of this study was to perform a meta-analysis to investigate whether an association exists between early intervention and improvement in mental or neuromuscular and movement scores in children born LBW or preterm.
A recent exhaustive magnetic resonance imaging study of 137 participants ages 13–22 yr showed that both LBW and preterm birth are associated with reduced gray matter density bilaterally in the temporal lobe structures and cerebellum (Spencer et al., 2008). The study concluded that these brain anomalies persist into adolescence. Additionally, in a separate but related meta-analysis, we found that both preterm birth and LBW were associated with deficits in mental and neuromuscular and movement-related functions in a similar way (Spittle, Orton, Doyle, & Boyd, 2007). Thus, in the current study, we pooled scores from children born LBW or preterm to form a single group to increase the number of effects.
Method
Independent and Dependent Variables
The independent variable for this meta-analysis was whether the children were participating in an early intervention program. Early intervention programs used in the studies included the Newborn Individualized Developmental Care and Assessment Program (Als et al., 2003; Westrup et al., 2004); the kangaroo care intervention (Feldman et al., 2002; Tessier et al., 2003); the Mother–Infant Transaction Program (Gianní et al., 2006; Kaaresen et al., 2008; Nordhov et al., 2010); Creating Opportunities for Parent Empowerment (Melnyk et al., 2001); the Avon Premature Infant Project (Johnson et al., 2005); the Infant Behavioral Assessment and Intervention Program (Koldewijn et al., 2009; Verkerk et al., 2012); a modified version of the Vermont Intervention Program (Olafsen et al., 2006); and other motor, behavioral, and cognitive programs (Gardner et al., 2003; McCormick et al., 2006; Sajaniemi et al., 2001; Teti et al., 2009; Table 1).
Summary of Studies of Early Intervention for Children Born Low Birthweight or Preterm
Note. NA = not applicable; NICU = neonatal intensive care unit.
The dependent variable was improvement in performance scores of children born LBW or preterm on mental or neuromusculoskeletal and movement-related function tests. Some of the tests used were the Assessment of Preterm Infants’ Behavior, British Ability Scales, Movement Assessment Battery for Children, Child Behavior Checklist, Peabody Picture Vocabulary Test, Woodcock–Johnson Tests of Achievement, Bayley Scales of Infant Development II, Wechsler Preschool and Primary Scale of Intelligence–Revised, Griffiths Mental Development Scales, Global IQ test, and Early Social Communication Scales (Table 1).
Sample
Data were collected from studies that searched for a correlation between early intervention and the effectiveness of mental or neuromusculoskeletal and movement-related functions in LBW or preterm children. The search was conducted on the Web through Florida International University’s library databases (e.g., EBSCO host, PubMed, ScienceDirect). The following key words and combinations were used to maximize the yield of pertinent studies: preterm, low birthweight, premature effectiveness, early intervention program, early intervention, mental function, cognition, motor function, premature, movement, and neuromusculoskeletal. These key words were chosen on the basis of the aim of this study. The key terms were used to search all aspects of early intervention programs that addressed mental or neuromusculoskeletal and movement-related functions. In addition, the reference lists of obtained studies were scrutinized for other compatible publications.
Inclusion and Exclusion Criteria
We examined the articles to establish whether the studies fulfilled the following inclusion criteria: original research; empirical design with direct observation of children; publication in English between 2000 and 2013; inclusion of children born LBW or preterm who participated in an early intervention program; presence of a comparison group who did not receive early intervention; inclusion of a mental or neuromusculoskeletal and movement-related function component using standardized and nonstandardized testing; and provision of test scores (means and standard deviations) to enable effect-size calculation. Studies were excluded if they assessed parents instead of children who underwent early intervention, if they did not meet the inclusion criteria, or if the outcomes did not allow us to calculate the effect size (Ottenbacher, Heyn, & Abreu, 2009).
Data Extraction and Coding of Studies
To thoroughly analyze each of the studies used, we extracted and coded the following information: authors and year; mental or neuromusculoskeletal and movement-related function components; early intervention treatment; length of treatment; score, time, or error type of test; treatment group (mean, SD, n); comparison group (mean, SD, n); chronological age; and moderators. All relevant data were entered into an Excel spreadsheet. Data were run through Comprehensive Meta-Analysis (CMA) software (Borenstein, Hedges, Higgins, & Rothstein, 2005) to interpret the data. The studies were coded into the following two categories:
Early intervention program and mental function assessments
Early intervention program and neuromusculoskeletal and movement-related function assessments
Data Analysis
Effect Size.
To determine the effect sizes, we used CMA software (Borenstein et al., 2005). CMA uses means, standard deviations, and sample sizes to generate the effect size of the association between early intervention and mental function assessment or neuromusculoskeletal and movement-related function assessment. The effect sizes (d) are classified as small (.20), medium (.50), or large (.80; Rosenthal, 1991). For each effect-size estimate, a standardized mean difference and 95% confidence intervals were calculated in a fixed- and random-effects model. A positive effect size indicates that the group of children who received early intervention did better in both mental and neuromusculoskeletal and movement-related functions than the comparison group who did not receive early intervention program, and a negative effect size indicates that the comparison group did better.
Heterogeneity Test.
We used heterogeneity statistics to find the extent of variability among the group of studies, important to consider when performing a meta-analysis. Heterogeneity is tested using Q and I 2 values. A significant Q value (p < .10) indicates the presence of heterogeneity between studies. The I 2 value indicates the extent of heterogeneity: absent (0), low (25), medium (50), or large (75 or higher; Shiroma, Ferguson, & Pickelsimer, 2010). In the presence of heterogeneity, we used the random effects model, whereas we used the fixed effects model for homogeneity. In the present meta-analysis, we report both fixed and random effects models because they both were generated by the CMA software.
Publication Bias.
In general, researchers tend to report positive results in the literature. Therefore, it is not unusual to find only positive results when conducting a meta-analysis. To test for publication bias, we used a funnel plot and Egger’s regression intercept test (Egger, Smith, Schneider, & Minder, 1997). The funnel plot provides a visual demonstration of publication bias. A symmetrical funnel plot indicates inclusion of both positive and negative results, and an asymmetrical funnel plot (i.e., leaning toward one side) indicates a publication bias. In addition, Egger’s regression intercept test can statistically detect a significant publication bias (p < .05; Egger et al., 1997).
Results
Study Characteristics
A total of 16 studies were included in this meta-analysis. All included studies addressed early intervention comparing an intervention and a comparison group and were published between 2000 and 2013. The total combined number of participants in all studies was 2,094. The number of participants in each study ranged from 26 to 377. The average chronological age of the participants ranged from 1 mo adjusted age to age 5 yr.
Each study provided and assessed an early intervention in two categories: (1) mental functions and (2) neuromusculoskeletal and movement-related functions. Eight studies assessed mental functions only, 1 assessed neuromusculoskeletal and movement-related functions only, and 7 assessed both mental and neuromusculoskeletal and movement-related functions. The studies generated a total of 97 effects for comparison, 74 for mental functions and 23 for neuromusculoskeletal and movement-related functions. The studies used different types of interventions and assessments to address the children’s need or assess their level of development before starting the early intervention.
Effect Size
The effect size for the effectiveness of early intervention in improving performance in mental and neuromusculoskeletal and movement-related functions is small (d = .219). Using fixed effects analysis, the d for mental functions was .250 (p < .0001) and for neuromusculoskeletal and movement-related functions was .118 (p < .0001). The overall Q value was 93.787 (p > .001), and the overall I 2 value was 0.000, suggesting no heterogeneity (Table 2).
Fixed and Random Effect Sizes for Each Outcome Measure
Note. Heterogeneity scores are not shown for random effects analysis because they are the same as for the fixed effects analysis.
Publication Bias
The funnel plot of standard error by standard difference in means showed 97 values distributed inside and 3 values outside the funnel. The distribution of data inside and outside the funnel is asymmetrical (Figure 1). In addition, the p value in Egger’s regression intercept test (intercept 1.213, range = 0.636–1.790) is lower than .05, suggesting that the publication bias was significant (Table 3).
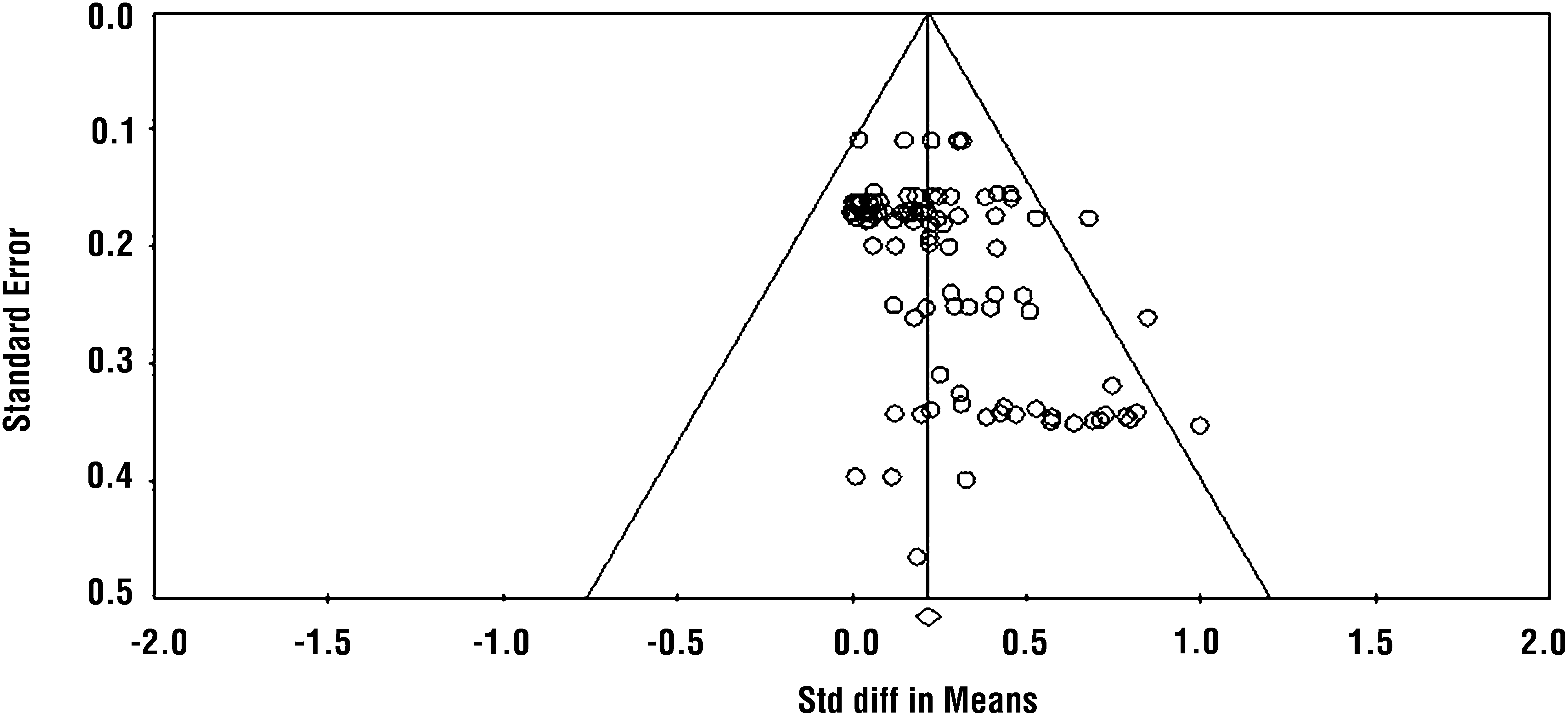
Funnel plot indicating publication bias.
Egger’s Regression Intercept Test Results
Note. df = degrees of freedom, p < .05.
Discussion
The results of this study support the hypothesis that children born LBW or preterm may benefit significantly from early intervention as evidenced by improved development of mental and neuromusculoskeletal and movement-related functions compared with children born with the same conditions who do not receive early intervention. The results show that early intervention programs, in general, significantly improved mental functions of children born LBW or preterm with respect to increased verbal performance, executive functioning, and IQ scores. Additionally, regarding neuromusculoskeletal and movement-related functions, children born LBW or preterm who received early intervention made better behavioral and neurobehavioral improvement than comparison groups who did not receive early intervention.
The results further suggest that early intervention is beneficial in improving functional outcomes of LBW or preterm children by providing them with services needed to support development. The present meta-analysis provides evidence that early intervention may provide important intervention for the development of daily living, learning, academic, emotional, and social skills in children because mental and neuromusculoskeletal and movement-related functions play a great role in the development of children and their functions (Anderson, De Luca, Hutchinson, Roberts, & Doyle, 2010; Bayless & Stevenson, 2007; Bora et al., 2011). Therefore, intervening early in areas of mental and neuromusculoskeletal and movement-related functions may lessen the risk of neurodevelopmental delays during the school years. Early intervention might be helpful in reversing the complex developmental delay and poor school performance of children born LBW or preterm (Aarnoudse-Moens et al., 2009; Oliveira, Magalhães, & Salmela, 2011; van Baar, Vermaas, Knots, de Kleine, & Soons, 2009).
In general, mental and motor development and functions have been studied as separate and independent processes. However, a plethora of research suggests a tight interdependence between mental and neuromusculoskeletal and movement-related functions in terms of global development and functions (Diamond, 2000; Koziol, Budding, & Chidekel, 2012; Wassenberg et al., 2005). Children with mental dysfunctions are likely also to have impairments in movement-related functions (Diamond, 2000). Diamond (2000) further noted that movement problems are common in children with developmental disorders such as dyslexia, specific language impairment, autism spectrum disorder, and attention deficit hyperactivity disorder, indicating a coupling between mental and movement-related functions. Anatomical evidence indicates that this coupling stems from regular coactivation of the dorsolateral prefrontal cortex and contralateral cerebellum (de Zubicaray et al., 1998; Schlösser et al., 1998). Therefore, it is reasonable to assume that mental functions are important for proper movement-related performance. On the basis of the results of this meta-analysis, we suggest that early intervention address both mental and neuromusculoskeletal and movement-related functions.
Missiuna, Gaines, and Pollock (2002) argued that it is important to recognize both mental and movement-related problems in children born LBW or preterm as soon as possible. IDEA 2004 recognized that a well-timed early intervention not only helps children born LBW or preterm maximize their potential for catching up from developmental delay but also reduces special education costs when they reach school age and enhances their capacity for independent living in the community. Therefore, the results of this meta-analysis suggest that clear early intervention strategies should be integrated into early intervention plans to maximize the effectiveness of intervention and should address mutuality between mental development and movement-related development.
Implications for Occupational Therapy Practice
The results of this meta-analysis have the following implications for occupational therapy practice:
Both mental and neuromusculoskeletal and movement-related functions are important components in a child’s development of activities of daily living, academic skills, and social skills that stretch into adolescence.
Early intervention programs are significantly beneficial in improving mental and neuromusculoskeletal and movement-related functions in children born LBW or preterm.
Early information about children who have mental and movement-related dysfunctions could lead to timely early intervention to minimize mental and movement deficits.
Multidisciplinary early intervention teams should integrate both mental and movement-related aspects when designing early intervention program.
Limitations
A possible weakness of this study is the difficulty we had in identifying which among the wide variety of services constituted early intervention services. The terms we used to search the topic of focus were varied because participants are categorized in many ways (e.g., children, infants, toddlers, babies, newborns). Many of the articles we searched and browsed did not include sufficient data (e.g., mean, standard deviation, and sample size) to allow us to determine the program’s effectiveness using meta-analytic techniques and so were not included in the analysis.
Conclusion
The results of this meta-analysis support our hypothesis that an association exists between participation in an early intervention program and improvement in mental and neuromusculoskeletal and movement-related functions for children born LBW or preterm. These findings suggest the need for proper early diagnosis and for implementation of integrated multidisciplinary early intervention. When planning intervention strategy, early intervention providers should identify correlations between mental dysfunctions and movement-related deficits in children born LBW or preterm and include both areas in intervention.
Footnotes
Acknowledgment
This meta-analysis was part of the master’s project development in occupational therapy at Florida International University. We thank Florida International University for providing facilities and software to conduct this study.
Indicates studies that were included in the meta-analysis.