
Abstract
The prevalence of obesity has escalated worldwide, and the World Health Organization (WHO; 2012) has noted that overweight or obesity is a major risk factor for several chronic diseases. Multiple factors are associated with increasing rates of childhood obesity (Brown, Kelly, & Summerbell, 2007), including low levels of activity and high levels of sedentary behavior (Telama, 2009) and parents’ weight (Davison & Birch, 2001) and socioeconomic status (Lissner, Johansson, Qvist, Rössner, & Wolk, 2000). Obesity is preventable (WHO, 2012), and contemporary research has found family-based lifestyle interventions to be useful in preventing and treating childhood obesity (Golley, Magarey, Baur, Steinbeck, & Daniels, 2007; Oude Luttikhuis et al., 2009; Reinehr, Kleber, Lass, & Toschke, 2010; Wilfley et al., 2007).
Health care practitioners agree that it is necessary to assess family lifestyles and support parents in establishing healthier family lifestyles (e.g., Ayoob, 2011). However, only a few examples of effective intervention strategies with this focus have been published (see Berge & Everts, 2011). The establishment of healthy family lifestyles is most likely based on many factors (Golan, 2006), including supportive environments and communities that encourage families to make healthier choices about food and regular physical activity. From a public health perspective, outreach to parents, who are the principal enactors of change in childhood obesity, has been recommended as an effective approach to help them establish proactive strategies early in their children’s lives (Nader et al., 2012).
An occupation-focused family intervention called Lighter Living (LiLi) was recently shown to be effective in reducing children’s body mass index (BMI) z scores by increasing the time family members spent together in shared occupations in the home environment (Orban, Edberg, Thorngren-Jerneck, Önnerfält, & Erlandsson 2014). During the year-long intervention, parents were encouraged to focus on occupational engagement and reflect on their patterns of daily occupation to identify areas they needed to change. Parents considered the support they received in implementing sustainable family routines to be a useful ingredient in the intervention. The time participating parents spent in various daily occupations, including time spent with their children on weekdays, increased significantly, and children’s BMI z scores decreased significantly from referral to the end of the intervention (Orban et al., 2014). However, not all participating parents changed the amount of time they spent with their children, and the factors associated with changes in time use have not yet been explored.
The aim of this study was to explore factors related to changes in the time parents spent with their children in three areas of occupation and changes in the children’s BMI z scores. The following research questions guided this study: To what extent does an occupation-focused family intervention effectively support parents in changing three areas of their time use: (1) time spent with their children preparing and eating meals, (2) time spent engaging in physically active occupations, and (3) time spent engaging in physically inactive occupations? To what extent does the intervention decrease children’s BMI z scores, and what factors are related to any decrease?
Method
Research Design
This study had an explorative and quasi-experimental design and was part of a larger study called the Lund Overweight and Obesity Preschool Study (LOOPS), a randomized controlled trial (RCT) described in detail elsewhere (Önnerfält et al., 2012). The overall aim of LOOPS was to determine whether family-based interventions aimed at parents (both mothers and fathers) of children ages 4–6 yr with overweight or obesity had a long-term positive effect on the children’s BMI. The study was approved by the Regional Ethical Review Board, Lund University (Dnr159/2008), and registered at ClinicalTrials.gov (NCT00916318).
Participants and Selection Procedure
Children who were overweight or obese were identified during a regular visit to their local child health center. The children were referred to a nearby children’s hospital, where parents received oral and written information from a pediatrician describing the family intervention, procedures, and confidentiality. Inclusion criteria for the LOOPS were that children be ages 4–6 yr, be obese, and have parents with satisfactory ability to communicate in Swedish. The exclusion criterion was presence of any other medical or endocrine disorders in the child. Once informed consent was obtained, participants were randomly assigned by blocking them in series of 10 (randomly allocated to two different intervention groups), stratifying them by parents’ weight (normal, overweight, or obese), and concealing their identities in numbered envelopes.
At the time of analysis, all parents allocated to the 1-yr LiLi intervention who provided the required time use data and completed the intervention were included in this study, yielding a total of 40 parents of 22 children with obesity (Figure 1). Data on parents of 11 children who never came to the group sessions were analyzed separately as nonparticipants, and parents of 7 children who did not write diaries throughout the entire intervention (i.e., participants with missing diaries) were analyzed separately. Sociodemographic characteristics at inclusion of all participants originally assigned to the LiLi appear in Table 1.
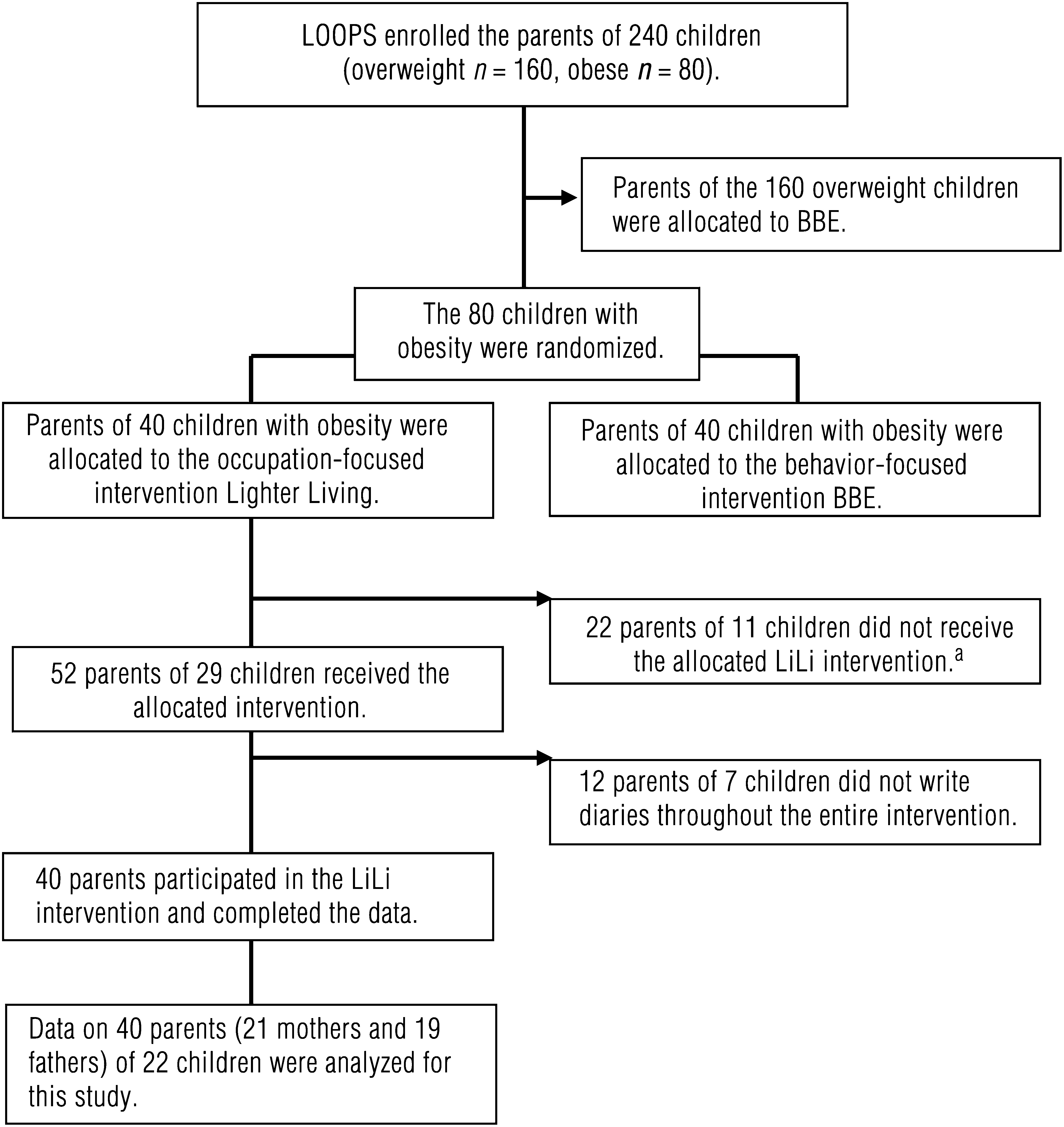
Flow chart of participant recruitment in the Lighter Living (LiLi) intervention.
Sociodemographic Characteristics of Parents of Children Randomized to the Lighter Living Program
Note. BMI = body mass index; SD = standard deviation.
Instruments and Data Collection
Time-Use Diaries.
Parents used time–geographic diaries (Ellegård, 1999, 2006) repeatedly during the intervention program to record when, where, and with whom they participated in occupations during a 24-hr period. All participating parents maintained an open diary, a small booklet in which they recorded the time they started each new activity during the 24 hr, the place, and the people with whom they performed each activity. We coded participants’ time use using a coding system of 600 general types of activities and transformed the codes into graphs using the software program Daily Life Version 2008 (Ellegård & Nordell, 2011). Each graph comprised 1,440 min of parent time use (e.g., co-occupations with children were displayed by recording with whom a given activity was completed). To ensure the validity of the data collected, the parents rated on a 5-point scale (1 = not at all to 5 = very well; median = 4.6) how well each documented 24 hr represented an average day in their current lives. The reliability of the coding was assessed through participants’ endorsement of the graph representing each diary. Participants wrote a total of 220 diary entries (average of 6) throughout the program; all 7 days of the week were represented.
Body Mass Index.
A trained registered pediatric nurse measured the children’s weight and height in a standardized way at inclusion, after 6 mo, and at the end of the intervention. BMI was calculated as weight (kg) divided by height (m) squared (i.e., BMI = kg/m2). The terms overweight and obesity were defined by BMI according to the definition set out by Cole, Bellizzi, Flegal, and Dietz (2000). We obtained BMI standard deviation scores (z scores) for age- and gender-specific reference values from reference data for Swedish children (Karlberg, Luo, & Albertsson-Wikland, 2001). The BMIs of both parents were measured at inclusion.
Occupational Value Instrument With Predefined Items.
The Occupational Value Instrument With Predefined Items (OVal–pd; Eklund, Erlandsson, & Persson, 2003; Eklund, Erlandsson, Persson, & Hagell, 2009) was administered at the beginning and end of the intervention. Each of the 18 items describes a separate aspect of perceived occupational value—that is, the experience derived from an occupation (e.g., sense of competence or enjoyment)—in the three dimensions of concrete value (e.g., “something important was accomplished”), symbolic value (e.g., “it led to other people getting in touch”), and self-reward value (e.g., “it was a true pleasure to do these things”). Respondents were asked to state how frequently they had perceived these aspects of occupational value during the past month by choosing a response from 1 = not at all to 4 = very often; totals ranged from 18 to 72 points. Eklund et al. (2003) found adequate convergent validity. Eklund et al. (2009) demonstrated a good fit of the 18 OVal–pd items to the Rasch model, suggesting that these items form a one-dimensional occupational value construct, and found that Cronbach’s α was good, at .91. Moreover, test–retest and internal consistency reliability of an American English version were very good (α = .92), and exploratory factor analysis confirmed its structural validity (Eakman & Eklund, 2011).
Study-Specific Questionnaire.
In addition, the pediatric nurse administered a questionnaire developed specifically for this study to participants at inclusion and after 1 yr of intervention. The questionnaire included the Swedish version of the Pearlin Mastery Scale (Pearlin & Schooler, 1978), the Mastery–S (Eklund, Erlandsson, & Hagell, 2012), to assess the extent to which parents felt that they were in control of their everyday lives and able to achieve their goals. Parents self-reported their degree of mastery by rating seven statements on a scale ranging from 1 = strongly agree to 4 = strongly disagree; total scores ranged from 7 to 28 points, with higher scores indicating a higher degree of perceived mastery. The original instrument has shown satisfactory psychometric properties (Pearlin, Menaghan, Lieberman, & Mullan, 1981) and good internal consistency (Chiesi, Galli, Primi, Innocenti Borgi, & Bonacchi, 2013; Majer, Jason, & Olson, 2004; Marshall & Lang, 1990). Rasch model testing of the Mastery–S showed that the items represent a logical continuum of the measured construct; although one item displayed misfit, it showed acceptable reliability (Person Separation Index = .70; Eklund et al., 2012).
In addition to the Mastery–S, the questionnaire included two specific questions. The first requested an overall estimation of subjective health using the question “In general, how would you evaluate your health?” Four response alternatives ranged from 4 = excellent to 1 = poor. Second, overall satisfaction with daily occupations was measured using the question, “In general, how would you evaluate your satisfaction with your daily occupations?” Five response alternatives ranged from 5 = excellent to 1 = poor.
Other Data.
Sociodemographic information regarding age, gender, marital status, education, profession, and finances was obtained. In addition, parents’ frequency of attendance at the targeted intervention (LiLi) and number of diary entries written during the intervention were also recorded.
Intervention
LiLi is a 1-yr occupation-focused family intervention program with a specific focus on facilitating healthy lifestyle changes in families. It was inspired by the Redesigning Daily Occupations (ReDO) program (Erlandsson, 2013), which has proved effective in encouraging lifestyle-related changes (Eklund & Erlandsson, 2011). LiLi takes a clearly occupation-focused approach to child weight management that differs from the traditional focus on dietary restriction, increased physical activity, and child weight loss. This alternative approach shifts the emphasis to supporting parents in revising their lifestyles, specifically by altering everyday routines to include more time spent in co-occupations, improving meal routines, and encouraging physically active occupations in the family. These changes, in turn, are presumed have a positive impact on children’s BMI.
The LiLi intervention was standardized in a manual (Erlandsson & Orban, 2008) outlining 12 two-hour sessions based on occupational therapy theory (Scaffa, Van Slyke, & Brownson, 2008; Wilcock, 2006) and evidence (Clark et al., 1997, 2012; Eklund & Erlandsson, 2011). The participants received course materials in a specially designed folder that included information specific to each session. A key component of the intervention is the use of time-use diaries to provide parents with insight into their daily routines and offer them opportunities to reflect and focus on healthy meal preparation and on participation in play and physically active occupations with their children.
Interveners
The LiLi program was directed by two occupational therapists (one of whom was the first author, Kristina Orban) experienced in family interventions and group dynamics. The therapists administrated all sessions according to the manual; they were blinded to group assignment, and all data collected from parents and children before and during the intervention were concealed.
Data Analysis
Analyses were conducted to identify and more fully understand differences among participants who completed the intervention, participants with missing diaries, and nonparticipants. Linear regression analyses were used to determine parents’ self-reported time-use change in minutes in three areas of co-occupation with their children: preparing and eating meals, engaging in physically active occupations, and engaging in physically inactive occupations. We selected these three areas because of their hypothesized links to the maintenance and treatment of childhood obesity (Davison & Birch, 2001). Standard descriptive statistics (mean and standard deviation [SD]) were computed for the children’s BMI z scores. Paired two-tailed t tests, Pearson correlations, analysis of variance, and χ2 tests were used to test statistical significance, set at p < .05.
Multiple linear regression analyses were used to identify the most systematic and statistically significant model predicting parents’ change in time use and children’s change in BMI z scores; thus, the dependent variables were (1) parents’ time-use difference and (2) children’s change in BMI z score. Parents’ time use and children’s BMI z score data were converted to individual difference scores according to how the data were collected throughout the intervention. Both parents may have influenced a child’s BMI change; therefore, the parental independent variables entered into the models using backward selection were occupational value difference (OVal–pd total score) during the intervention, frequency of program attendance, and number of diary entries written. Additional independent variables were parents’ sense of mastery, subjective health, satisfaction with everyday occupations, BMI, education, and finances at inclusion. Sample size requirements were considered, taking into account the number of independent variables included in the regression models (Tabachnick & Fidell, 2007); at each step, only the variables that made significant contributions to the model were kept. Because the sample was small, the adjusted R 2 for the model was used. Data analyses were conducted using SPSS (Version 18.0; SPSS, Inc., Chicago).
Results
At inclusion, no significant differences were found among participants who completed the intervention, participants with missing diaries, and nonparticipants on the variables of parents’ age, BMI, marital and employment status, number of children, children’s gender, or children’s BMI. The only significant difference we found was that parents in the nonparticipants group had significantly less education (p = .003; see Table 1).
Parents’ Change in Time Use
Parents increased the time they spent with their children by an average of 91 min per day during the intervention, F(1, 218) = 4.87, p = .028. Physically active occupations in particular increased, F(1, 218) = 5.96, p = .015 (Table 2).
Linear Regression Analysis of Change in Time Parents (N = 40) Spent With Children During the Intervention
Note. Q1 = first quartile; Q3 = third quartile.
The regression model for change in parents’ total time use revealed a final model that was statistically significant, F(4, 32) = 2.87, p = .038, and that explained 17.3% of the variance (Table 3). Predictors for time-use change in physically active occupations were number of diary entries written, finances, perception of occupational values, and low mastery at inclusion, which together accounted for 18.5% of the variance. Predictors for time-use change in physically inactive occupations were finances, parent BMI at inclusion, and perception of occupational values, which together accounted for 26.4% of the variance.
Factors Associated With Parents’ Time-Use Change and Children’s BMI Change
Note. BMI = body mass index; CI = confidence interval; NS = not significant; OVal–pd diff. = difference in scores on the Occupational Value Instrument With Predefined Items. Mean scores on independent variables entered into the regression: OVal–pd diff. (sum of concrete, symbolic, and self-reward value) at inclusion, 47, and at end, 52 (p = .002); mean scores at inclusion: mastery, 23.7; subjective health, 3.3; satisfaction with daily occupations, 3.6; education, high school; finances, satisfied; parents’ BMI, 28; frequency of attendance at Lighter Living sessions, 7.7; number of diary entries, 6.
Children’s Change in BMI z Scores
No statistically significant change was observed in children’s BMI z score at the end of the intervention. However, a clinically important decrease (Kolsgaard et al., 2011) in mean BMI z score was noted, from 3.08 (SD = 0.96) at inclusion to 2.93 (SD = 1.05) at the end of the intervention. The change in mean BMI z score was −0.15 (SD = 0.56), 95% confidence interval [−0.11, 0.40].
Factors associated with parent characteristics that predicted children’s change in BMI z score in a healthful direction were mothers’ mastery (high) and parental subjective health and fathers’ perceived occupational value and education. The final model was statistically significant, F(5, 15) = 9.05, p < .001, and explained 66.8% of the variance (Table 3).
Discussion
The results of this study indicate that a 1-yr occupation-focused group intervention for parents may contribute to changed time use in families and reduced BMI for children diagnosed with obesity. This article is the first to report that parent factors were significantly associated with changes in how parents spent time with their children and with children’s changed BMI z scores after the intervention. The parents who participated in the LiLi intervention increased the amount of time they spent with their children, particularly time spent in physically active occupations. The number of written diary entries was a strong predictor of time-use change in physically active occupations. The diary method used in the LiLi program thus constituted an important facilitator of change. The diaries enabled parents to reflect on and identify any need for change in the patterns of their daily occupations. Moreover, the results indicate that four to six diary entries written during the intervention were enough to contribute to a time-use change. Developers of future lifestyle interventions should consider including a diary component.
Parents’ financial situation was a strong predictor of change in time spent with children but not of changes in children’s BMI. Parents’ sense of control (mastery), subjective health, and education were stronger predictors of children’s change in BMI than finances, a result that contrasts with those of other studies showing that economic disadvantage predicts child obesity (see Lissner et al., 2000). In Sweden, paid parental leave promotes paternal involvement irrespective of economic situation, enabling both parents to spend time with their young children. It also allows all parents of children up to age 8 yr to work part time (instead of full time) if they choose. According to the findings of this study, parents who considered their current finances sufficient were better able to change their time use, perhaps by spending less time at work and more time with their children. However, our study showed parents’ subjective health, mastery, and education to be of greater importance than finances in facilitating a healthful reduction in child BMI.
Lower scores in parents’ sense of mastery at inclusion (i.e., total score of <23 on the Mastery–S) predicted greater change in time use. Parents who perceive a lower level of control over events and circumstances in their everyday lives may be more motivated to change and may benefit more from the targeted intervention.
The decreases in children’s BMI z scores after intervention were not statistically significant, although they might have been clinically important. Nowicka, Pietrobelli, and Flodmark (2007) found similar reductions, showing that low-intensity family therapy was useful in their clinical setting. Other studies have reported that reductions of 0.11–1.30 in BMI z scores are clinically significant (Epstein, Paluch, Roemmich, & Beecher, 2007; Golan, 2006), and according to Kolsgaard et al. (2011), even a modest reduction in BMI z score after a 1-yr intervention was associated with improvement in several cardiovascular risk factors. Parents’ time-use change in, for instance, physically active occupations performed with children might have contributed to a more physically active lifestyle. However, our hypothesis that changes in parents’ time use in daily occupations performed with their children would promote children’s weight normalization was not fully supported, even though the study results reflect slowed weight gain. Future research should investigate whether parental changes in time use can contribute to children’s weight reduction in the long term.
Parent involvement seems essential to children’s weight reduction. Our results show that increases in fathers’ perceived occupational value and level of education, parents’ self-rated health, and mothers’ reports of high mastery were predictors of a decrease in children’s BMI z scores. This finding aligns with those of previous studies showing that involved parents, especially fathers (Stein, Epstein, Raynor, Kilanowski, & Paluch, 2005), are essential partners in effective childhood obesity treatment programs (Golan, 2006; West, Sanders, Cleghorn, & Davies, 2010). A previous study investigating division of time and parental duties between mother and father (Orban, Ellegård, Thorngren-Jerneck, & Erlandsson, 2012) showed that fathers who were away from the family during most of the children’s waking hours had the most constraints on changing their time use patterns, resulting in mothers’ difficulty adjusting their own schedules, and children’s BMI reduction was limited (Orban et al., 2014). Thus, fathers’ cooperation in shared daily occupations with their children could be of vital importance.
Finally, the findings of this study confirm that parent involvement with children can be increased without requiring the children to participate in the group sessions. The changes our parents achieved in time use can be interpreted as the result of awareness they gained through reflection and collaboration during the occupation-focused intervention. This interpretation is consistent with the ideas behind the ReDO program (Erlandsson, 2013) and with research done by Bateson (1996) and Schön (2003), who accentuated opportunities for reflection and discussion as a requirement for learning and change. Thus, this study indicates that it might be just as relevant to highlight shared family occupations in the home environment and changes in parents’ lifestyle and that it may not be necessary to focus on the children’s weight and body size in interventions.
Limitations and Future Research
The 220 collected time-use diary entries that constituted our primary data provided subjective data. Note, however, that we did not inform the parents specifically that we would be analyzing the time they spent with their children in the three areas of occupation. This strategy provided parents, as well as researchers, with otherwise difficult-to-obtain insight into daily routines.
Some of the variables that predicted change were collected using psychometrically tested instruments and a study-specific questionnaire. Self-reported perceived perceptions are highly subjective, a fact that may affect reliability; further studies with larger samples are needed to confirm the results.
Because the LiLi program was one arm of an RCT, participants were assigned (i.e., did not choose) to participate in the occupation-focused program. Some parents might have expected or preferred a diet-focused or behavior-focused intervention. For various reasons, 27.5% of the parents randomized to LiLi decided not to participate; younger parents and those with lower education levels were more likely to decline. Barriers to attendance were identified well before the first intervention session. Attrition rates are commonly 20%–50% in child weight-management studies (Golley et al., 2007; West et al., 2010); the high rate of nonparticipation may threaten this study’s transferability. Future intervention programs must target parents’ needs more carefully and consider that different family types may need different strategies to accomplish lifestyle change. In addition, it was difficult to recruit certain groups of parents to the RCT, such as those belonging to various ethnic groups, same-sex parents, parents with functional limitations, and parents of low socioeconomic status. The fairly small and homogeneous sample limits the generalizability of these findings.
Implications for Occupational Therapy Practice and Research
The findings presented in this study can be considered an attempt to understand factors of importance when designing and developing occupation-focused interventions aimed at promoting a healthy lifestyle among children with obesity and their families. These findings have the following implications for occupational therapy practice and research:
Supporting parents in reflecting on the way they spend their time and engage in daily routines with their children might lead to sustainable lifestyle change by promoting an understanding of the relationship between time use, weight status, and well-being for the whole family.
Parents’ increased involvement in their children’s daily occupations may predict positive outcomes in both time use and child BMI.
Interventions in routine clinical settings should help both parents identify healthy occupational opportunities.
Collaboration with parents using an occupation-focused approach may be effective in interventions aimed at facilitating normal weight development in children.
Clients have different resources and capacities (e.g., finances, subjective health) at their disposal. Practitioners can identify and strengthen parental resources to enable engagement in meaningful occupations.
Future research needs to explore family constraints that limit opportunities to engage in desired family routines. The great challenge lies in identifying and reaching out to all parents who need support to effect changes in their daily occupations.
Footnotes
Acknowledgments
The authors thank the families who participated in the study and Anna Lindgren for statistical guidance. The research was supported by Vårdalinstitutet, Swedish Institute for Health Sciences. The authors have no competing financial interests to declare.