
Abstract
Keywords
Dual tasking is performance of two tasks simultaneously (Kahneman, 1973; Pashler, 1994). Combinations of hand dexterity tasks and cognitive tasks, such as speaking on the telephone while writing a message or listening to the teacher while taking notes in class, are ubiquitous in daily activities. People pay less attention to each task when the demands of dual tasking exceed their attention capacity (Kahneman, 1973); this decrease in availability of attention for each task is termed interference. Increased understanding of clients’ concurrent motor and cognitive task performance is essential for evaluating their daily functioning (Christofoletti, Andrade, Beinotti, & Borges, 2014; Haggard, Cockburn, Cock, Fordham, & Wade, 2000).
Studies of dual-task performance in people with schizophrenia have suggested that they experience more difficulties with concurrent cognitive and perceptual tasks and concurrent motor tasks than healthy control participants (Fuller & Jahanshahi, 1999; Granholm, Asarnow, & Marder, 1996; Schwartz et al., 1989, 1991). Only one study has explored performance of a concurrent motor and cognitive task in people with schizophrenia (Lallart et al., 2014). Participants were required to count forward, count backward, and speak animal names spontaneously (verbal fluency) while walking. The participants with schizophrenia showed poorer walking performance than the healthy control participants because the cognitive tasks caused greater interference under the dual-task condition (Lallart et al., 2014).
Like walking capacity, hand dexterity is critical in daily functioning, and impaired hand dexterity has been correlated with compromised daily functioning in people with schizophrenia (Green, Kern, Braff, & Mintz, 2000; Lehoux et al., 2003; Midorikawa et al., 2008; Sasayama et al., 2014). However, no studies to date have considered hand dexterity when investigating dual-task performance in people with schizophrenia. In addition, deterioration in performance of dual tasks associated with poor daily functional performance was reported in a study of people with neurological deficits such as brain injury and stroke (Haggard et al., 2000). Nevertheless, no studies have yet investigated the relationship between daily activities and dual-task performance in people with schizophrenia.
This study had two objectives: (1) to compare hand dexterity in single-task and dual-task conditions in participants with schizophrenia with that of healthy control participants and (2) to examine the relationship between discrepancy in hand dexterity between conditions and daily functioning in the participants with schizophrenia. We hypothesized that in the dual-task condition hand dexterity would decline significantly more in the participants with schizophrenia than in the control participants and that daily functional performance would be negatively correlated with discrepancy in hand dexterity between conditions in participants with schizophrenia such that the smaller their discrepancy in hand dexterity, the better their daily functioning.
Method
The protocol for this study received ethical approval from the National Taiwan University Hospital’s institutional review board.
Participants
Occupational therapists recruited 16 patients with schizophrenia being treated at a psychiatric clinic and day care rehabilitation center at the National Taiwan University Hospital. Inclusion criteria were diagnosis of schizophrenia by a psychiatric clinician according to World Health Organization (2010) diagnostic criteria, age of 20–65 yr, stable status with no change in antipsychotic medications in the previous 3 mo, adequate cognitive abilities reflected in scores on the Mini-Mental State Examination (MMSE) >24 (Folstein, Folstein, & McHugh, 1975; Heun, Papassotiropoulos, & Jennssen, 1998), and signed informed consent. The control group consisted of 16 healthy, age- and gender-matched volunteers. Exclusion criteria were presence of another neurological or psychiatric diagnosis and MMSE score of ≤24.
Measures
Purdue Pegboard Test.
The Purdue Pegboard Test (PPT; Tiffin & Asher, 1948) measures hand dexterity. Although the test comprises four subtests, we used only three: placing small metal rods into holes in a pegboard (1) with the preferred hand, (2) with the nonpreferred hand, and (3) with both hands. (The fourth subtest involves assembly and measures not only dexterity but constructional praxis, so we chose not to use it.) The sequence of subtests was determined randomly by drawing lots. The participants were instructed to place the rods individually into holes as quickly and correctly as possible, and the number of rods placed in the pegboard in 30 s was recorded. All participants completed two trials for each subtest in the single- and dual-task conditions, and the averages of each pair of trials were used in the analysis.
The reliability of the PPT ranges from .60 to .91 and the validity from .07 to .76 (Tiffin & Asher, 1948). The test–retest reliabilities of the subtests are moderate to good in people with schizophrenia (intraclass correlation coefficient [ICC] = .73–.88; Lee et al., 2013).
Serial Sevens Subtraction Test.
We chose the Serial Sevens Subtraction Test (SSST; Manning, 1982) as a cognitive task for the dual-task condition. All participants were instructed to subtract 7 from the beginning number and then to subtract 7 from each successive answer as quickly and correctly as possible. Clinicians commonly administer the SSST starting from 100 to examine cognitive ability; to avoid a learning effect, we started with a random number between 290 and 300 (Proud & Morris, 2010). Participants completed two trials in both the single- and dual-task conditions, and the average number of correct responses in each pair of trials was used in the analysis (Manning, 1982; Proud & Morris, 2010; Smith, 1967).
University of California, San Diego, Performance-Based Skills Assessment–Brief Version.
The University of California, San Diego, Performance-Based Skills Assessment–Brief Version (UPSA–B; Patterson, 2010) is designed to directly assess functional capacity. This performance-based test contains communication and financial domains. The communication domain uses an unplugged telephone in a series of role-play situations, including making emergency calls, calling directory assistance to request a telephone number, and rescheduling a medical appointment. The financial domain involves counting out given amounts and reading, filling out, and using a check. Higher scores indicate better functional capacity (Mausbach et al., 2011).
Test–retest reliabilities of the UPSA–B ranged from r = .66 to r = .81 over follow-up periods of up to 36 mo in people with schizophrenia (Leifker, Patterson, Bowie, Mausbach, & Harvey, 2010). The UPSA–B has adequate psychometric properties, predicts residential independence, is sensitive to change, and requires only 10 to 15 min to administer (Mausbach, Harvey, Goldman, Jeste, & Patterson, 2007).
Activities of Daily Living Rating Scale–III.
The Activities of Daily Living Rating Scale–III (ADLRS–III; Chu, 2004) is a self-administered scale that assesses daily functioning in people with schizophrenia. Items address 10 topics: independence, hygiene, leisure, graphics, news, words, finance, traffic, communication, and adaptation. Included are self-reported questions (e.g., Could you go out for shopping?), questions of general knowledge with standard answers (e.g., Who is the president now?), and approaches to problem solving (e.g., When you are in a bad mood, what do you do?). Each item is scored from 0 to 10, with a maximum total score of 100, and higher scores indicate better functional abilities (Chu, 2004; Chu & Hsieh, 2004). The ADLRS–III has demonstrated good test–retest reliability (ICC = .87, p < .001), convergent validity, and discriminant validity in psychiatric patients (Chu & Hsieh, 2004).
Procedures
Participants were individually evaluated in two sessions and performed the tests in the same sequence. For the single-task condition, participants completed the ADLRS–III, then the UPSA–B, then the SSST, and finally the PPT. For the dual-task condition, participants were instructed to complete the SSST and PPT simultaneously and as quickly and correctly as possible.
Statistical Analysis
We used IBM SPSS Statistics Version 19.0 (IBM Corporation, Armonk, NY) to analyze study data. Demographic data were analyzed using t tests and χ2. We used the t test to examine change in hand dexterity by comparing the PPT scores under the dual-task versus the single-task condition as follows: discrepancy in dexterity = [number of pegs under single-task condition − number of pegs under dual-task condition] × 100/[number of pegs under single-task condition] (Lin, Cermak, Kinsbourne, & Trombly, 1996). We also used two-way mixed analysis of variance (ANOVA) with one between-subjects factor (Group: participants with schizophrenia vs. healthy control participants) and one within-subjects factor (Condition: single task vs. dual task) to analyze differences between the two groups in two conditions. We used Spearman correlation analysis to investigate the relationship between discrepancy in hand dexterity and daily functioning in the group with schizophrenia. The significance level was set at .05, and effect size, Cohen’s d, and partial η2 were used to estimate the magnitude of the effects.
Results
Participants
Demographic and clinical characteristics of the 16 participants with schizophrenia and 16 healthy control participants are summarized in Table 1. The schizophrenia group had significantly lower educational levels and MMSE scores than the control group.
Participants’ Demographic and Clinical Characteristics
Note. MMSE = Mini-Mental State Examination; SD = standard deviation.
Purdue Pegboard Test
Both groups placed fewer pegs in the dual-task condition than in the single-task condition when using the preferred and the nonpreferred hand (Figure 1). Significant differences in hand dexterity were found under the dual-task versus single-task condition between the two groups for the preferred, the nonpreferred, and both hands (p < .03, d > .7 for all; Table 2). Two-way mixed ANOVAs showed a significant interaction effect for both hands (p = .02, ηp 2 = .17), a marginal interaction effect for the nonpreferred hand (p = .06, ηp 2 = .11), and a moderate interaction effect for the preferred hand (p = .19, ηp 2 = .06). Significant Condition and Group effects were documented for preferred, nonpreferred, and both hands (p < .001, ηp 2 > .52 for all; Table 2). The performance of the participants with schizophrenia declined considerably from the single-task to the dual-task condition, and the participants with schizophrenia placed fewer pegs than the control participants.
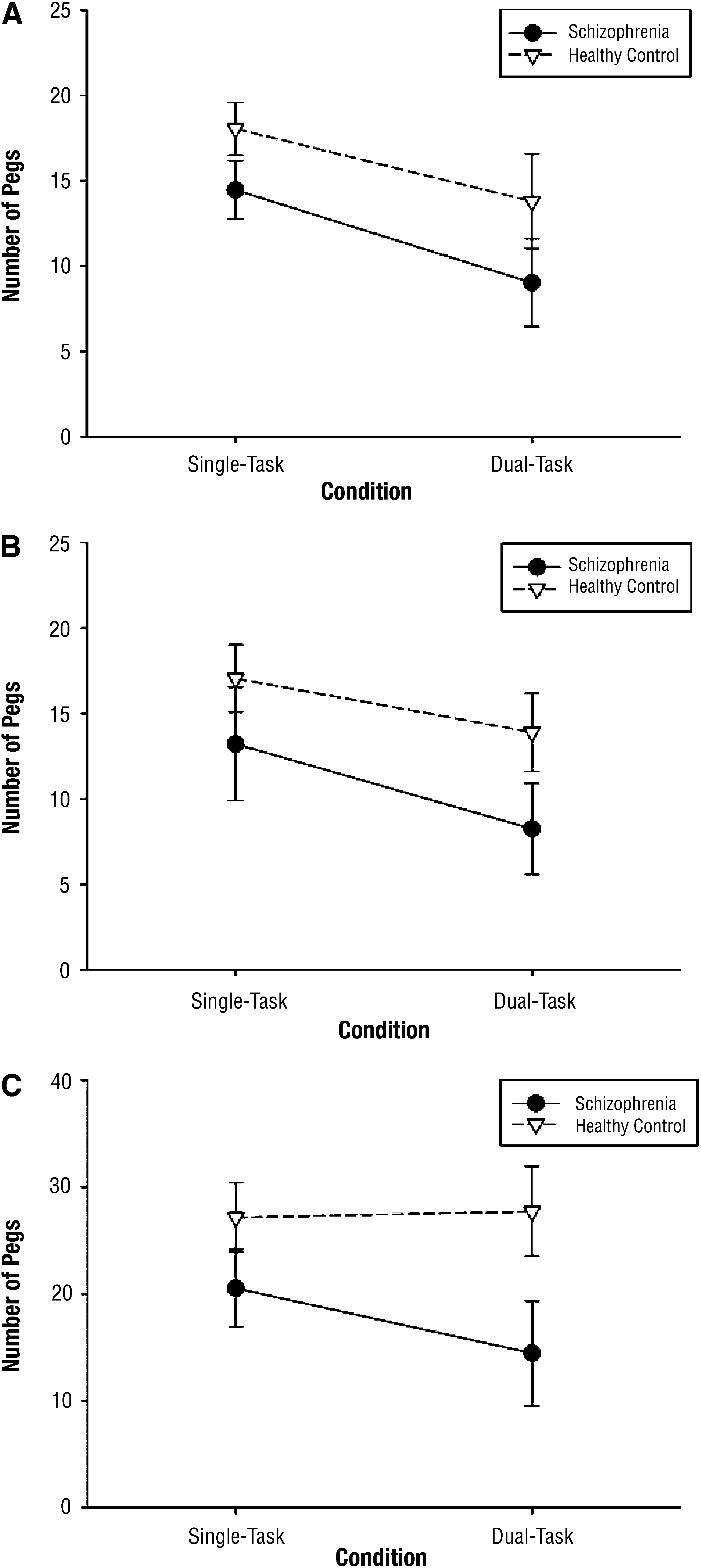
Number of pegs placed under single- and dual-task conditions in two groups, (A) by preferred hand, (B) by nonpreferred hand, and (C) by both hands.
Participant Performance on the Purdue Pegboard Test
Note. M = mean, SD = standard deviation.
Relationship Between Discrepancy in Hand Dexterity and Daily Functioning in Participants With Schizophrenia
Negative correlations were found between discrepancy in hand dexterity from the single- to the dual-task condition and daily functional performance in the schizophrenia group (Table 3). Only one correlation, between discrepancy in dexterity for both hands and ADLRS–III scores, was significant (r = −.50, p = .047). Although the other correlations were not significant, the effect sizes were medium to high (r > −.30, p > .05; Table 3).
Correlation Between Daily Functioning and Discrepancy in Hand Dexterity Under Dual-Task Versus Single-Task Conditions in Participants With Schizophrenia (n = 16)
Note. ADLRS–III = total scores on the Activities of Daily Living Rating Scale–III; UPSA–B = total scores on the University of California, San Diego, Performance-Based Skills Assessment–Brief Version.
Discussion
To our knowledge, this is the first study to investigate performance in concurrent hand dexterity and cognitive tasks in people with schizophrenia. Adding a cognitive task interfered with hand dexterity to a greater extent in the schizophrenia group than in the control group. This finding is consistent with studies indicating that cognitive interference with motor function is greater in people with schizophrenia (Lallart et al., 2014), in older people with mild cognitive impairment (Montero-Odasso et al., 2009), and in people with Parkinson’s disease (Fuller et al., 2013; Proud & Morris, 2010).
The fact that all participants in our study displayed better hand dexterity under the single-task than the dual-task condition when using the preferred and nonpreferred hand provides evidence for the capacity model of attention, which indicates that people have lower capacity for mental work when performing dual tasks and that implementing incompatible tasks interferes with the performance of both (Kahneman, 1973; Pashler, Johnston, & Ruthruff, 2001; Ruthruff, Pashler, & Klaassen, 2001). In our study, participants performing the PPT (dexterity) and the SSST (cognition) at the same time experienced similar dual-task interference.
Moreover, the schizophrenia group exhibited significantly worse hand dexterity under the dual-task condition than did the control group. The effort participants with schizophrenia required to perform the dexterity tasks rose gradually when they changed from the preferred hand to both hands, but for the control group the discrepancy in dexterity decreased gradually as they moved from the preferred hand to the nonpreferred hand and then both hands. These findings imply that the healthy control participants could modulate and allocate attentional effort better to meet the activity demands and complete tasks. For the participants with schizophrenia, however, limited attentional resources may have combined with cognitive deficits to result in poor attentional modulation and performance. The other plausible explanation is that because the dorsolateral prefrontal cortex is involved in dual-task conditions (D’Esposito et al., 1995; Hartley, Jonides, & Sylvester, 2011; Tachibana et al., 2012), deficits in the dorsolateral prefrontal cortex in the participants with schizophrenia may have resulted in their poor performance in the dual tasks (Behere, 2013; Chen et al., 2014; Palaniyappan, Park, Balain, Dangi, & Liddle, in press; Rubinov & Bullmore, 2013).
In addition, discrepancy in hand dexterity was negatively associated with daily functional performance in the schizophrenia group. That is, the smaller the decrease in hand dexterity performance from the single- to the dual-task condition was, the better the participant’s daily functional performance was. This negative correlation may indicate that people with schizophrenia whose hand dexterity decreases more when they perform dual tasks will exhibit worse daily functional performance. Although only one negative correlation was significant (i.e., dexterity for both hands and ALRS–III scores), the effect sizes of all correlations were medium to large. A similar result was found in a study that revealed a negative correlation between gait performance and scores on the Barthel Activities of Daily Living Index (Novak, Johnson, & Greenwood, 1996) in a dual-task condition (Haggard et al., 2000).
When performing activities of daily living, people often must do more than one task at a time. People with schizophrenia may experience dual-task interference that results in difficulties dealing with the hand dexterity and cognitive demands of daily functional activities. It follows that dual-task training that includes hand dexterity and cognitive activities may help people with schizophrenia improve their daily functioning.
Limitations and Future Research
Our study has several limitations. First, we used convenience sampling, and our sample size was relatively small. All participants in the schizophrenia group were from one hospital, and the healthy control group consisted of volunteers. The small sample size limits the power of our analysis and the generalizability of the results. The study used a controllable experimental task, so it is unknown whether the findings can be transferred to real-life situations.
Second, although we matched our participants with schizophrenia by age and gender with healthy control participants, the educational levels of the two groups were significantly different; the early onset of symptoms in the schizophrenia group likely interfered with their educational attainment. Future studies should match the educational levels of the experimental group with those of the control group.
Third, all participants with schizophrenia received antipsychotic treatment during the study, which might have influenced their cognition and motor function. Therefore, the test results should be interpreted with caution.
Several issues need further investigation. First, replication of this study with a larger population and probability sampling is recommended to verify our preliminary findings. Second, according to the capacity model of attention, the degree of difficulty of a cognitive task may influence performance, so it would be worth investigating whether decreasing the degree of difficulty of the cognitive task would promote dual-task performance. Third, future research could investigate whether providing participants with feedback, such as whether they perform each element of the cognitive task correctly, might facilitate their dual-task performance. Finally, serial observations could be done to compare performance in varied conditions within one group of people with schizophrenia. Doing so could reduce overall variability and remove participant differences to make the error components independent from condition to condition.
Implications for Occupational Therapy Practice
Our findings have the following implications for occupational therapy practice:
Dual-task performance can be considered a behavioral marker to assist in designing intervention programs to address daily functional performance in people with schizophrenia (e.g., work hardening programs, maintenance functions within the areas of self-care and productivity).
To improve or avoid deterioration in hand dexterity, occupational therapy practitioners can simplify tasks and contexts for people with schizophrenia.
Practitioners can consider using dual tasks as a therapeutic activity for people with schizophrenia; improvements in hand dexterity in a dual-task situation might promote ADL function.
Conclusion
This study is the first to examine the effects of performing a dual task (a manual plus a cognitive task) on hand dexterity in people with schizophrenia. Participants with schizophrenia had poorer hand dexterity than healthy control participants when engaging in dual tasks, and the amount of discrepancy in hand dexterity between the dual-task and single-task conditions was associated with daily functioning. Occupational therapy practitioners providing treatment for people with schizophrenia might consider using dual tasks as a therapeutic activity. Future research with larger probability sampling and cognitive activities of varying difficulties is warranted to validate the findings.
Footnotes
Acknowledgments
This study was supported in part by the National Health Research Institutes (NHRI-EX104-10403PI), the Ministry of Science and Technology (102-2314-B-002-154-MY2, 102-2628-B-182-005-MY3, and 103-2314-B-182-004-MY3), the Healthy Aging Research Center at Chang Gung University (EMRPD1E1711), and the Chang Gung Memorial Hospital (CMRPD 1C0402) in Taiwan.