
Abstract
Keywords
Occupational therapy practitioners treating patients with hand injuries must demonstrate skills and knowledge relevant to a range of conditions and be proficient in assessing, treating, and evaluating the outcome of treatments. The healing process depends on the nature of the trauma and the surgical repair. A patient’s ability to use an injured hand during activity can be hindered by problems with range of motion (ROM), pain, edema, and weakness. For a patient to reach the goal of increased function and activity performance, it is important for occupational therapy practitioners to educate and work closely with the patient. Therefore, practitioners need to continuously develop and enhance the practice of hand therapy (Dimick et al., 2009; International Federation of Societies for Hand Therapy, 2010).
Distal radius fractures (DRFs) are the most common fractures that physicians see (Diaz-Garcia, Oda, Shauver, & Chung, 2011). DRFs have an annual incidence of 26 per 10,000 inhabitants in Sweden (Brogren, Petranek, & Atroshi, 2007). The energy of the trauma needed to cause the fracture differs. In young people, high-energy trauma is necessary, whereas in older people with osteoporosis, low-energy trauma is sufficient. About 10% of all White women age >65 yr sustain a DRF. In the United States, DRFs have an annual incidence of 57 to 100 per 10,000 population older than age 65 yr. Traditionally, DRFs in older adults have been treated with closed reduction and cast immobilization. More than 50% of these fractures result in malunion, but patients may still have satisfactory functional results. Other conventional treatment methods that result in fewer malunions and also have satisfactory functional results are percutaneous fixation with Kirschner wires and external bridging or nonbridging fixation (Diaz-Garcia et al., 2011).
Plate fixation has increased in popularity for DRF treatment during the past decade (Diaz-Garcia et al., 2011; Minegishi, Dohi, An, & Sato, 2011). At the orthopedic clinic in Linköping, Sweden, physicians started to operate on DRFs using plate fixations, mostly volar, in 2005. Approximately 80 patients per year undergo this procedure. Several studies have investigated outcomes after DRF, but previous research has mainly focused on comparisons of surgical procedures (Abramo, Kopylov, Geijer, & Tägil, 2009; Estrella & Panti, 2012; Grewal, MacDermid, King, & Faber, 2011; Wright, Horodyski, & Smith, 2005; Zenke, Sakai, Oshige, Moritani, & Nakamura, 2012). The most common outcome measures are ROM, grip strength, radiology, and the Disabilities of the Arm, Shoulder, and Hand (DASH) Questionnaire (Atroshi, Gummesson, Andersson, Dahlgren, & Johansson, 2000). Outcome measures usually do not focus on activity and participation, and changes over time are usually restricted to ≤1 yr. Hand therapy, as a concept, emphasizes body function and structure, and so has the research within the field of hand therapy. Other domains or life areas are less frequently addressed, and this gap in the literature is highlighted by reviews of hand therapy studies (Kus et al., 2011; Winthrop Rose, Kasch, Aaron, & Stegink-Jansen, 2011). The aim of this study was to explore differences in ROM, grip strength, and patients’ experienced pain and disability over time after DRF plate-fixation surgery.
Method
Research Design
We used a prospective repeated-measure design with four measure points (6 wk, 6 mo, 12 mo, and 24 mo after surgery), with the last follow-up at 24 mo in the form of a patient questionnaire. Disability was measured with the DASH Questionnaire. Because preinjury DASH scores were not available, we estimated the preinjury level of function by obtaining DASH scores by retrospective recall at 6 wk after injury. Patients were asked to fill out the questionnaire using their best recollection of function before injury. The research ethics committee of the Faculty of Health Science, Linköping University, Sweden, approved the study, and patients gave informed consent for participation.
Participants
Between October 2008 and March 2010, all patients in the orthopedic clinic, County Council of Östergötland, Linköping, Sweden, who underwent plate fixation after DRF and who met the inclusion criteria were asked to participate in the study. Inclusion criteria were at least age 18 yr and ability to assimilate information and follow instructions (in Swedish). The exclusion criterion was mental disorder (such as dementia). Ultimately, 101 patients participated in the study.
Postoperative Intervention
Five experienced occupational therapists working at the orthopedic clinic treated study patients according to written guidelines for postoperative hand therapy. The guidelines consisted of a schedule for introducing different interventions. The therapists were experienced in hand therapy and, after discussion, reached consensus about the treatment protocol. All patients were immobilized with casting for 2 wk after surgery, after which the cast was removed and exercises were introduced for the wrist, fingers, and thumb. All patients received a wrist lacer splint to use between exercises until 6 wk after surgery. Six weeks after surgery, all patients except 9 were allowed to use their hand in activities as they normally did. For these 9 patients, permission to use their hand in activities was delayed until 8 wk after surgery because they had a more complex fracture or a higher grade of osteoporosis than the others. All patients also received written information about the injury, exercises, and advice about using the hand in activities. During the period up to 24 mo after surgery, 18 patients had the plate removed because it caused problems such as crepitation, local tenderness, and swelling over the plate. The mean time for plate removal was 15.3 mo.
Outcome Measurements
ROM of the affected wrist was measured with a goniometer (Norkin & White, 2003) and a prosupinator and consisted of wrist extension and flexion (lateral goniometer placement), radial and ulnar deviation (dorsal goniometer placement), and pronation and supination. The uninjured hand was also measured to compare ROM. Goniometer measurement is a valid and reliable instrument with a commonly accepted measurement error of 5° (Norkin & White, 2003). Reliability of measurement can increase by the use of the same instrument and guidelines defining measurement position, anatomical landmarks, and goniometric placement (Cambridge-Keeling, 2002).
Grip strength was measured with a Jamar hand dynamometer (Fess, 1987), and patients’ scores were compared with typical values (Mathiowetz et al., 1985). With proper calibration, the Jamar dynamometer is a reliable instrument and has a very high acceptance criterion of +0.9994 or better correlation coefficient. The Jamar dynamometer is valid for measuring direct force rather than pressure (American Society of Hand Therapists, 1992).
Pain was estimated with the Visual Analog Scale (VAS; DeLoach, Higgins, Caplan, & Stiff, 1998), ranging from 0 (no pain) to 100 (unbearable pain). The VAS is easy to use and has shown good test
Disability in the upper extremity was measured with the Swedish version of the DASH Questionnaire (Atroshi et al., 2000; Hudak, Amadio, & Bombardier, 1996), which has a 30-item disability–symptom scale ranging from 0 (no disability) to 100 (most severe disability). The DASH Questionnaire was created as an outcome measure for upper-extremity disorders with the upper extremity as a functional unit. It is a reliable and valid instrument for patients with diverse upper-extremity disorders affecting the arm, wrist, and hand (Atroshi et al., 2000; Gummesson, Atroshi, & Ekdahl, 2003). A DASH score of 10.1 (standard deviation [SD] = 14.68) is considered typical and is based on a sample from the general U.S. population (n = 1,706; Hunsaker, Cioffi, Amadio, Wright, & Caughlin, 2002). A change of 15 points has been proposed as a clinically important change in a sample of patients with shoulder and wrist–hand disorders (Beaton et al., 2011).
Patients’ self-perceived occupational performance and satisfaction over time were estimated with the Canadian Occupational Performance Measure (COPM; Law et al., 2005), which ranges from 1 (impossible to do/not satisfied at all) to 10 (can do extremely well/extremely satisfied). It can be used for patients of all ages with various diseases (Law et al., 1994). The validity and reliability of the instrument have been evaluated in many studies, and the results have been very positive (Law et al., 2005).
The overall rating of discomfort of the wrist after treatment was estimated with the Global Assessment Scale (GAS; Endicott, Spitzer, Fleiss, & Cohen, 1976), which is a 4-point Likert scale ranging from 0 (no discomfort) to 3 (severe discomfort). The GAS evaluates the overall functioning of a person during a continuous time period from psychological or psychiatric sickness to health. The GAS is suggested to be useful in a wide variety of clinical and research settings because of its relative simplicity, reliability, and validity (Endicott et al., 1976). All measurements for this study were performed by the same occupational therapist.
Data Analysis
Data are presented as means and SDs unless otherwise stated. Data were analyzed with STATISTICA 10 (StatSoft, Tulsa, OK).
Descriptive statistics were used for the sample characteristics. Wrist ROM was analyzed for extension, flexion, and total active ROM. Total active ROM of the wrist was calculated as extension plus flexion. Analysis of radial deviation, ulnar deviation, and pronation and supination was also performed. The sample was divided into subgroups consisting of older (≥65 yr) and younger (<65 yr) patients and of patients who had the plate removed within 2 yr postoperatively and those who did not. The significant differences between the subgroups were analyzed with a Mann–Whitney U test.
Repeated measures analysis of variance (ANOVA) and Bonferroni post hoc analysis (ROM, grip strength, and pain) or the Friedman Test and Wilcoxon signed rank test with Bonferroni post hoc analysis (nonparametric variables) were used to analyze significant difference between follow-ups. Statistical significance was defined as p < .05.
Results
Of 141 patients consecutively asked to participate in the study, 40 patients declined and 101 patients gave informed consent and were included in the study. Participant characteristics are presented in Table 1. Participants and dropouts at different measure points are presented in Figure 1.
Participant Demographic and Clinical Characteristics (N = 101)
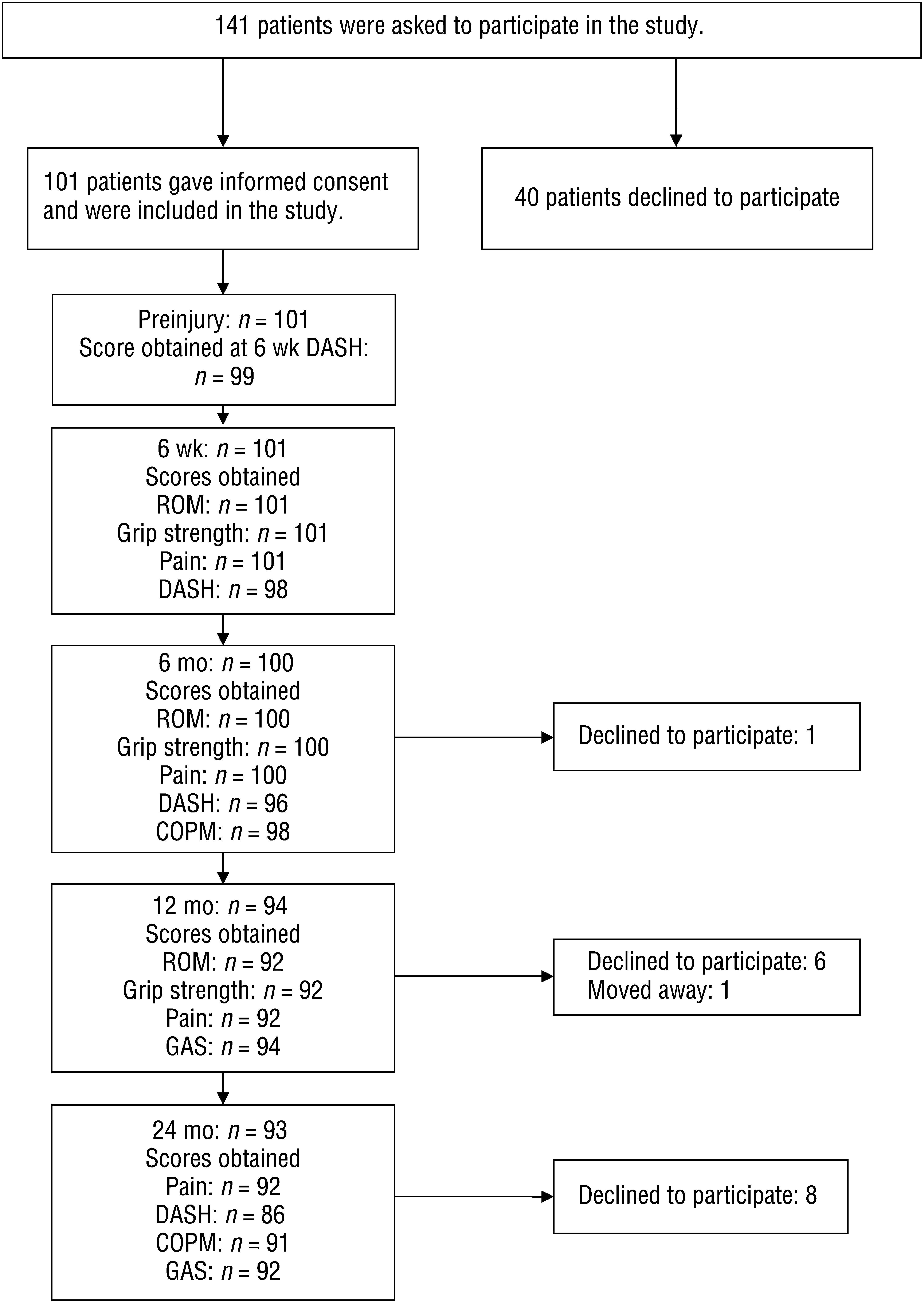
Participants and dropouts at different measure points.
A significant improvement was seen over time in all aspects of ROM in the injured hand (Table 2). Little difference existed between the injured and uninjured hands 12 mo postoperation (see Table 2). Grip strength improved significantly in the injured hand (see Table 2). Pain during activity and rest was significantly improved up to 6 mo postoperatively, and between 6 and 12 mo no further changes were seen. Pain increased between 12 and 24 mo postoperation but did not reach the levels found at 6 wk (see Table 2). At 24 mo postoperation, 32.6% (n = 28) of patients reported increased pain at rest and 41.9% (n = 36) during activity.
Injured Hand ROM, Grip Strength, and Pain Scores After Surgery
Note. M = mean; ROM = range of motion; SD = standard deviation; — = not applicable.
Measured with Jamar hand dynamometer. bMeasured with Visual Analog Scale. cFrom 6 wk to 6 mo, p < .05. dFrom 6 wk to 12 mo, p < .05. eSignificant difference from 6 mo to 12 mo, p < .05. fFrom 6 wk to 24 mo, p < .05. gFrom 6 to 24 mo, p < .05. hFrom 12 to 24 mo, p < .05.
Patients who had the plate removed experienced a higher rate of pain during activity at 12 mo (plate not removed, VAS 6.1 mm [SD = 15.9], and plate removed, VAS 28.5 mm [SD = 23.0]; p < .001) and more discomfort from the wrist (plate not removed, GAS 1.7 points [SD = 0.7], and plate removed, GAS 2.9 points [SD = 0.8]; p < .01) than patients whose plate had not been removed. At 24 mo, patients who had the plate removed still experienced more discomfort from the wrist (plate not removed, GAS 0.7 points [SD = 0.7], and plate removed, GAS 1.3 points [SD = 0.8], p < .02) than those who did not have it removed.
The DASH score decreased from 6 wk up to 6 mo, and no further change was seen up to 24 mo (Table 3). At 24 mo, the DASH score was still significantly worse compared with preinjury (see Table 3). The results of GAS showed that at 24 mo, 83.7% (n = 77) of participants reported no or mild discomfort compared with 78.7% (n = 74) at 12 mo after surgery.
Scores on Outcome Measures Before and After Surgery
Note. M = mean; SD = standard deviation; — = not applicable.
From preinjury to all follow-ups, p < .05. bFrom 6 wk to 6 mo, p < .05. cFrom 6 wk to 24 mo, p < .05. dFrom 12 mo to 24 mo, p < .05.
When comparing patients age 65 yr and older with those younger than age 65, the only statistically significant difference was seen in grip strength in the injured hand, measured with the Jamar dynamometer (kg), where younger patients were stronger at 6 mo (older age, 20.6 kg [SD = 9.3], and younger, 23.9 kg [SD = 10.0 kg]; p = .03) and at 12 mo (older age, 23.0 kg [SD = 8.9], and younger, 26.9 kg [SD = 10.6]; p = .02). Performance of and satisfaction with the most important activity in the COPM showed a not statistically significant deterioration from 6 mo to 24 mo (see Table 3).
Discussion
This study showed that at 12 mo after surgery, patients had regained almost the same ROM in the treated hand as in the uninjured hand, had almost as much grip strength as that in the typical population, and had decreased pain at rest and during activity. However, pain at rest and during activity increased between 12 and 24 mo. Disability measured with the DASH improved over time after surgery but was still higher compared with preinjury.
The findings in this study of residual pain at rest and during activity at 24 mo after surgery are in line with previous research by Kurimoto, Tatebe, Shinohara, Arai, and Hirata (2012), showing a substantial number of patients with residual wrist pain 18 mo after surgery using a volar locking plate as fixation. It is uncertain whether residual pain at rest and during activity was the result of the surgical technique because little has been written about pain over time after DRFs treated with plate fixation. We have not found any studies comparing surgical methods and experienced pain over time. Previous research has shown a higher rate of tendon complications after plate fixation (Margaliot et al., 2005), which may have an effect on residual pain. In 18 cases, the plate was removed because the patient attributed problems to the plate’s presence. The need for plate removal is a serious issue with plate fixation, which has been reported in previous research (Williksen, Frihagen, Hellund, Kvernmo, & Husby, 2013). Patients in the current study who had the plate removed had significantly more pain and were not as satisfied with the result at either 12 or 24 mo after surgery.
One might assume that pain would affect ratings of disability, but the DASH score decreased significantly between 6 wk and 24 mo. The decrease of 23.3 points was more than the minimal clinically important difference, according to Beaton et al. (2011). DASH scores preinjury and at 24 mo were within typical values (Hunsaker et al., 2002).
Limitations and Future Research
One limitation of this study was the study dropouts; however, 65.9% of patients asked to participate completed all follow-ups. Another limitation was that the preinjury DASH score was based on a rating at 6 wk after surgery; therefore, bias may have been introduced by patients having to recall how they functioned before injury. Marks et al. (2011) described how a patient’s perception of a satisfactory outcome is complex and is influenced by several factors, such as symptoms; activities in daily life and function; and embodiment, which refers to how the person takes his or her body for granted once the body parts are not problematic. In this study, we did not measure intervention fidelity. However, written guidelines for the hand therapy intervention were used; the occupational therapists were experienced and reached a consensus about the guidelines; and all patients received the planned postoperative hand therapy, although some were delayed a few weeks.
To capture how patients perceived discomfort after the injury and how the DRF affected their daily life, we used the GAS and the COPM. The COPM could have been used at all follow-ups; however, we wanted to investigate how patients experienced their activity performance after a longer period of time. To highlight areas other than body function, it would perhaps have been of interest to use COPM at each time point. GAS showed that a majority of participants experienced no or mild discomfort from the injury, and performance and satisfaction ratings for the most important activities were high at 24 mo despite increased pain levels.
The first measure point, at 6 wk, was chosen because patients were then allowed to use their hand in a typical manner. In retrospect, we could have added a 3-mo follow-up to measure short-term outcome, but at 6 mo the healing process had progressed further. The DASH was not used at the 12-mo follow-up, which is a limitation because it would have captured the variations in the course of rehabilitation and would have shown whether self-reported disability followed the course of patients’ experienced pain levels. The final follow-up, a questionnaire, was at 24 mo after surgery. Using only a questionnaire was a limitation because it would have been beneficial to compare the physical measure of ROM and grip strength with the increasing pain levels. However, we chose this time point to avoid the problem of other diseases affecting patients during a long interval before final follow-up.
This study’s finding of residual pain at 24 mo would be interesting to explore further, for example, with radiographic assessment. It would also be interesting to investigate whether the process takes the same course when using other surgical methods. A possible explanation for residual pain could be that patients expect to have less pain than they actually do after 24 mo. Further studies are needed to compare patients’ expectations with the actual outcome. It is important to provide patients with this information about the long-term effects of a DRF.
Implications for Occupational Therapy Practice
DRF treated with plate fixation enables early postoperative mobilization.
Postoperative hand therapy can contribute to recovery of ROM and grip strength during the first year after surgery.
Twelve months after surgical treatment of DRF with plate fixation, ROM and grip strength were almost fully regained.
Occupational therapy practitioners need to be aware of the risk of long-term pain issues among patients with DRF with plate fixation, especially among patients in need of plate removal.
It is important to provide patients with information about the possible lengthy effect of a DRF.
Footnotes
Acknowledgments
We thank the Orthopedic Clinic and the Department of Hand Surgery, Plastic Surgery, and Burns, Linköping University Hospital, for providing practical support.