
Abstract
This systematic review examined the literature published from January 2006 to April 2013 related to the effectiveness of occupational therapy interventions for children with autism spectrum disorder (ASD) and their parents to improve parental stress and self-efficacy, coping, and resilience and family participation in daily life and routines. From the 4,457 abstracts, 34 articles were selected that matched the inclusion criteria. The results were mixed and somewhat inconclusive because this body of literature is in its infancy. Studies of children with ASD do not routinely measure parental and family outcomes. Recommendations include an emphasis on family measures other than parental stress and a greater focus on measures of parental and family functioning in all future studies of pediatric interventions to more fully understand the impact of interventions in a wider context.
Keywords
Families are the most important and most enduring force in a child’s development (Schor, 2003). Families provide the foundation for children to learn, develop typically, engage in occupations, and participate in routines (Primeau, 2000; Schor, 2003; Segal, 2004; Stewart-Brown & Schrader-McMillan, 2011). “Children’s outcomes—their physical and emotional health and their cognitive and social functioning—are strongly influenced by how well their families function” (Schor, 2003, p. 1542). Family-centered care is therefore often considered best practice in the health care arena (Kuo et al., 2012), and an important aspect of clinical practice to promote positive child outcomes for children with special needs should be interventions to support and promote family wellness and functioning (Dunst, Hamby, & Brookfield, 2007). These interventions may be a particularly critical aspect of practice when working with families of children with autism spectrum disorder (ASD) because these children demonstrate a variety of symptoms that can have a considerable impact on the family.
A diagnosis of ASD is made when reciprocal social communication and social interaction skills are impaired and restricted or repetitive behaviors and interests are present. These features, according to the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders, must become present during early development and result in a significant impairment in social, occupational, and other areas of functioning (American Psychiatric Association, 2013). Children with ASD demonstrate communication deficits and inappropriate social engagement as well as cognitive and adaptive impairments (Davis & Carter, 2014; Kim, Paul, Tager-Flushberg, & Lord, 2014). Their developmental skills are often inconsistent, their responses to intervention vary (Brookman-Frazee, Stahmer, Baker-Ericzén, & Tsai, 2006), and they engage in self-injurious, aggressive, or rigid behaviors that may influence the entire family’s functioning (Meadan, Halle, & Ebata, 2010). Children with ASD frequently demonstrate multiple occupational performance deficits related to ASD symptoms that could have an impact on family routines and well-being.
Occupational Performance Deficits of Children With ASD and Family Impact
Children with ASD have difficulties in multiple areas of occupation, including activities of daily living, sleep, education, and play. Delayed performance of self-care has been reported (Jasmin et al., 2009), and parents have noted difficulties with feeding and toileting (Ahearn, Castine, Nault, & Green, 2001; McLennan, Huculak, & Sheehan, 2008). Parents also report difficulties with oral care and dental visits (Stein, Polido, & Cermak, 2012). Children with ASD experience feeding difficulties that are less transient than those of typically developing children (Provost, Crowe, Osbourn, McClain, & Skipper, 2010). Specifically, they resist sitting at the table during mealtime, eat less variety of foods, and have more difficulty eating in new environments, for example, a family picnic or a restaurant (Provost et al., 2010). Children with ASD may eat very limited diets or may be placed on special diets because of food allergies or parental desire (Lockner, Crowe, & Skipper, 2008; Millward, Ferriter, Calver, & Connell-Jones, 2004; Nadon, Feldman, Dunn, & Gisel, 2011).
Sleep routines may also be difficult for the family. Children with ASD have difficulty falling and staying asleep and frequently wake early (Park et al., 2012; Richdale & Schreck, 2009; Sivertsen, Posserud, Gillberg, Lundervold, & Hysing, 2012). Mothers tend to provide nighttime care when children have sleep difficulty, which interrupts maternal sleep and affects maternal health as well (Bourke-Taylor, Pallant, Law, & Howie, 2013). Sleep difficulties persist into adolescence and have a long-term impact on child and caretaker function (Goldman, Richdale, Clemons, & Malow, 2012).
Educational performance is often an issue for children with ASD, many of whom are placed in the special education system. Parents may have difficulty determining the appropriate educational placement for their child; even children with typical cognitive ability may demonstrate academic achievement that does not match their intellect as a result of atypical behaviors and social difficulties (Estes, Rivera, Bryan, Cali, & Dawson, 2011). Last, independent play, sibling play, and peer play also are commonly difficult for children with ASD (Mastrangelo, 2009; Mavropoulou, Papadopoulou, & Kakana, 2011; Oppenheim-Leaf, Leaf, Dozier, Sheldon, & Sherman, 2012). The extensive and pervasive nature of the difficulties experienced by many children with ASD leads to substantial parental stress.
Impact on Parental Stress
The literature has indicated a high incidence of reported stress among parents and families of children with ASD compared with parents of children with other developmental disabilities and parents of typically developing children (Hayes & Watson, 2013; Karst & Van Hecke, 2012; Montes & Halterman, 2007; Mugno, Ruta, D’Arrigo, & Mazzone, 2007; Schieve, Blumberg, Rice, Visser, & Boyle, 2007). Given the performance difficulties described earlier, parenting a child with ASD is especially difficult and stressful. In addition, the lengthy diagnostic process, lack of knowledge about the diagnosis, and uncertainty regarding prognosis may increase the stress experienced by parents of children with ASD (Dale, Jahoda, & Knott, 2006; Moh & Magiati, 2012). Other stressors reported by families include financial hardship resulting from the cost of intervention and parental absence from work, challenges around traveling to multiple medical appointments, and problems obtaining respite care (Harper, Taylor Dyches, Harper, Olsen Roper, & South, 2013; Montes & Halterman, 2008; Zablotsky, Kalb, Freedman, Vasa, & Stuart, 2014). These difficulties, as well as the prospect of lifelong or lengthy care from family, have a measurable impact on the stress felt by families of children with ASD (Karst & Van Hecke, 2012) and often create concerns for the future (Donaldson, Elder, Self, & Christie, 2011).
Impact on Family Routines
Along with the financial and access-to-care issues, stressors associated with raising a child with ASD include the need to have rigid or structured routines, which can restrict the family’s lifestyle and create social isolation (Bishop, Richler, Cain, & Lord, 2007; Davis & Carter, 2008; DeGrace, 2004; Larson, 2006; Schieve et al., 2007). Including the child with ASD in activities both in and outside of the home can be stressful or chaotic (Bagby, Dickie, & Baranek, 2012; Marquenie, Rodger, Mangohig, & Cronin, 2011; Schaaf, Toth-Cohen, Johnson, Outten, & Benevides, 2011). These types of difficulties may hinder the development of typical family routines.
Family performance patterns are often disrupted or altered when the home includes a child with ASD. The child’s rigid behaviors may lead families to adopt highly structured routines, but to engage in activities outside the home, families may need to become extremely flexible (DeGrace, 2004; Larson, 2006; Schaaf et al., 2011). Family activities often revolve around the needs of the child with ASD (DeGrace, 2004; Schaaf et al., 2011), and mothers report that they frequently engage in excessive planning to manage their child’s behaviors along with the needs of the family (Kuhaneck, Burroughs, Wright, Lemanczyk, & Darragh, 2010). The level of success in adequately planning, adapting, and balancing the needs of all family members is likely related to parents’ belief in their own self-efficacy.
Impact on Self-Efficacy
Self-efficacy is defined as one’s belief about one’s capability to perform or ability to succeed (Bandura, 1994, 1997). Self-efficacy is an important concept to consider in relation to parenting because belief in one’s capability as a parent may influence motivation, emotional state, and investment in intervention strategies. Sustaining a positive sense of parenting self-efficacy can be challenging for parents of children with ASD (Kuhn & Carter, 2006), because typical parenting strategies may not work, many child behaviors are extreme, and continually balancing the needs of all family members is demanding (DeGrace, 2004; Kuhaneck et al., 2010; Larson, 2006; Schaaf et al., 2011).
Coping and Resilience
Despite significant stress and difficult family situations, many parents of children with ASD cope effectively and demonstrate resilience (Bayat, 2007; Bekhet, Johnson, & Zauszniewski, 2012; Karst & Van Hecke, 2012; Lai, Goh, Oei, & Sung, 2015). The literature on resilience and family coping has suggested an interrelationship among multiple factors, such as family resources, the stressful event (having a child with a disability), and the way in which the family makes meaning of the event (Bayat, 2007). Reframing, or a parent’s ability to make the child’s disability mean something important for the family, allows the family to adapt and balance the demands of raising the child with other family needs. These reframed perceptions may be one key to family well-being (Karst & Van Hecke, 2012; Luther, Canham, & Young Cureton, 2005).
Other specific coping strategies used by parents of children with ASD include social and family supports, support groups, religion, and professional supports and services (Lai et al., 2015; Twoy, Connolly, & Novak, 2007). Certain types of coping strategies are more likely to have positive outcomes on parental mood, and others may have a more negative impact (Pottie & Ingram, 2008). Despite the importance of coping skills, however, few studies have investigated interventions to improve parental coping specifically in this population, and little is known about the impact of occupational therapy interventions on coping skills for parents of children with ASD.
Importance of Interventions for Families
Interventions to improve stress, parental self-efficacy, and coping skills are a critical aspect of family-centered care for families of children with ASD (Karst & Van Hecke, 2012). Strong parental self-efficacy may be particularly important for parents of children with ASD because self-efficacy has been found to mediate the relationship between parental mental health and child problem behaviors (Hastings & Brown, 2002). Thus, in theory, robust parental self-efficacy may allow parents to better maintain positive mental health in the face of difficult child behaviors.
Self-efficacy is influenced by multiple factors and has the potential to be improved. Studies have demonstrated that parental fatigue and well-being, contextual family factors, and child behaviors all affect self-efficacy (Giallo, Wood, Jellett, & Porter, 2013). In addition, parents’ ability to problem solve and use strategies to manage child-related challenges may influence their perceptions of self-efficacy (Foster, Dunn, & Lawson, 2013). Increasing parents’ knowledge of ASD may increase self-efficacy because they are better able to understand the child’s behaviors and, in turn, infer the child’s underlying needs and wants (Kuhn & Carter, 2006).
Self-efficacy may influence parental stress. Perceived parental self-efficacy was found to be directly related to parenting stress in parents of children with disabilities (Giallo et al., 2013). Kuhn and Carter (2006) similarly found that depression and stress were significantly negatively associated with feelings of maternal self-efficacy in mothers of children with ASD. Given the relationship between self-efficacy and stress, improving self-efficacy may decrease parental stress, although it has not been directly studied.
Coping is believed to affect psychological well-being through complex mechanisms that are not yet fully understood (Karst & Van Hecke, 2012; McStay, Trembath, & Dissanayake, 2015; Pottie & Ingram, 2008). Effective coping strategies may reduce the risk for parental mental health issues and may also help manage parental stress (Zablotsky, Bradshaw, & Stuart, 2013). Therefore, interventions to support coping skills may be essential, but this idea, too, has yet to be fully studied.
With the importance of family functioning for child outcomes (Schor, 2003), the high levels of stress present in parents of children with ASD, and the strong possibility of a negative impact on family well-being, it is imperative that service providers working with these families provide interventions that help improve family functioning and well-being (Karst & Van Hecke, 2012). Yet, little information is available to guide practitioners in providing these interventions.
Gap in the Knowledge Base
As the prevalence of ASD has increased (Autism and Developmental Disabilities Monitoring Network, 2007, 2014), so has the likelihood that occupational therapy practitioners will treat children with ASD and work with their families. Parents value the contribution of occupational therapy practitioners on the multidisciplinary team and have reported that occupational therapy is the third most commonly chosen intervention for people with ASD (Interactive Autism Network, 2008). Parents must perceive that occupational therapy practitioners bring something of value to their families, or they would not continue to choose this service with such great demand. Understanding of the interventions that best improve family functioning can increase occupational therapy’s value to the family as well as, perhaps, improve child outcomes through greater family-centered care practices (Dunst et al., 2007; Schor, 2003).
An extensive literature has supported the notion that parenting children with ASD is difficult and that parents of children with ASD are stressed and need help. The literature has suggested that self-efficacy may serve a protective function for parents. Less well known is what type of intervention is beneficial for improving parental and family well-being, coping, and resiliency. To date, few studies have specifically examined the impact of occupational therapy interventions on family functioning (Dunn, Cox, Foster, Mische-Lawson, & Tanquary, 2012), and this gap in the literature should be filled. More studies outside of occupational therapy have examined some aspects of family functioning in relation to specific interventions. Therefore, the purpose of this systematic review was to examine the broader literature on the effectiveness of occupational therapy interventions for people with ASD that improve parental self-efficacy, stress, family coping and resiliency, and family participation in daily life and routines.
Method
The systematic review on ASD was supported by the American Occupational Therapy Association (AOTA) as part of a larger evidence-based practice project. This systematic review was completed for the period January 2006–April 2013. The focused question that framed this review was “What is the evidence for the effectiveness of interventions within the scope of occupational therapy practice for people with ASD that improve parent self-efficacy, family coping and resiliency (including spouse and children), and family participation in daily life and routines?”
The search terms for this review were developed by the methodology consultant to the AOTA Evidence-Based Practice (EBP) Project and AOTA staff, in consultation with the review authors of each question, and by an advisory group. The search terms were developed not only to capture pertinent articles but also to make sure that the terms relevant to the specific thesaurus of each database were included. Figure 1 shows the search strategy related to population (ASD) and types of interventions included in the systematic review. A medical research librarian with experience in completing systematic review searches conducted all searches and confirmed and improved the search strategies. Databases and sites searched included MEDLINE, PsycINFO, CINAHL, ERIC, and OTseeker. In addition, consolidated information sources such as the Cochrane Database of Systematic Reviews were included in the search. Moreover, reference lists from articles included in the systematic reviews were examined for potential articles, and selected journals were hand searched to ensure that all appropriate articles were included.
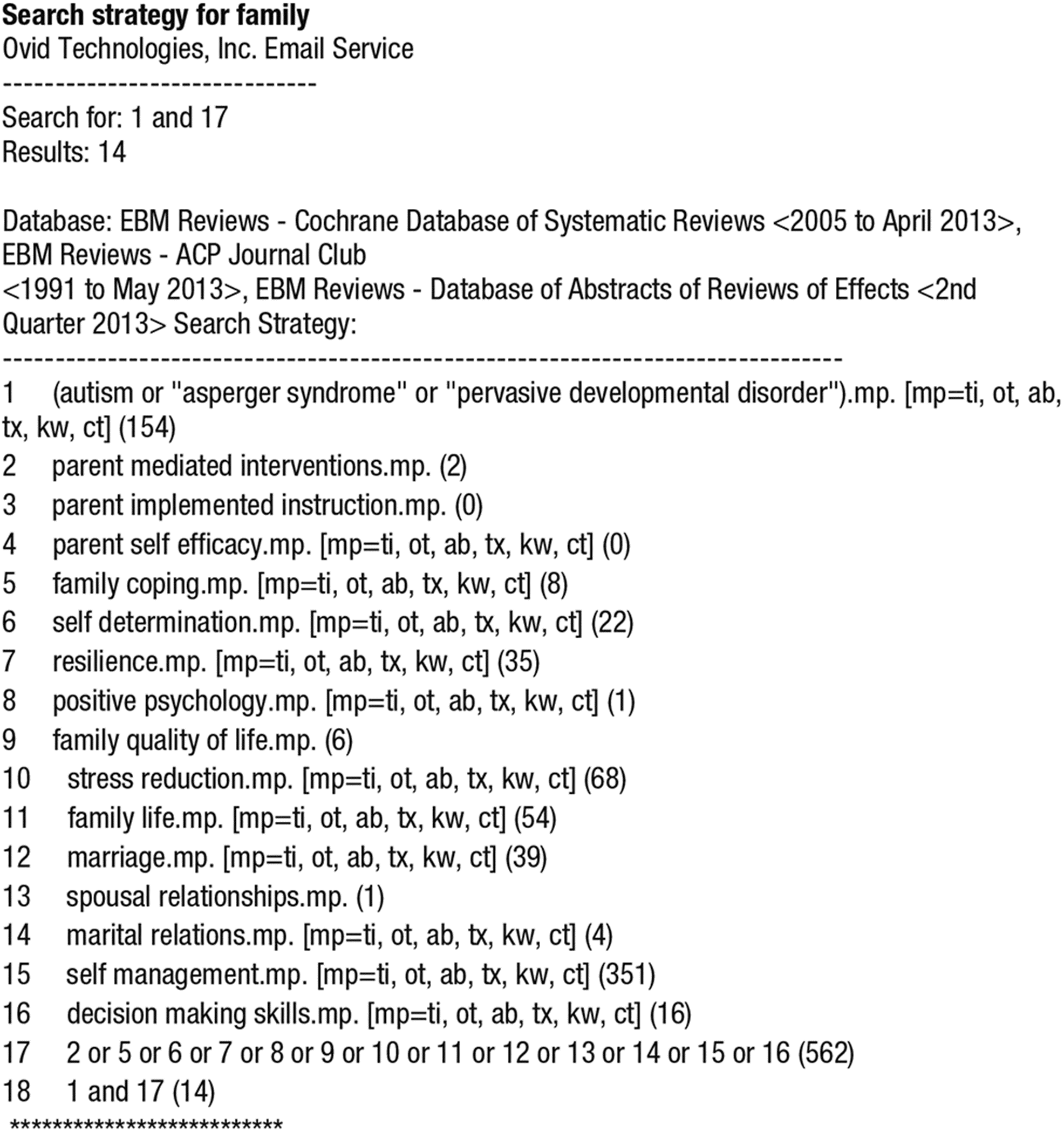
Search strategy.
The review was limited to peer-reviewed scientific literature published in English. The intervention approaches examined were within the scope of practice of occupational therapy. The literature included in the review was published between January 2006 and April 2013 and included study participants with ASD. The review excluded data from presentations, conference proceedings, non–peer-reviewed research literature, dissertations, and theses. Studies included in the review were Level I, II, and III evidence. Level IV and V evidence was included only when higher level evidence on a given topic was not found. In the levels of evidence used by AOTA, Level I includes systematic reviews of the literature, meta-analyses, and randomized controlled trials. Level II studies are those in which assignment to a treatment or a control group was not randomized (cohort study). Level III studies do not have a control group. Level IV studies use a single-case experimental design, and Level V studies are case reports and expert opinion such as narrative literature reviews and consensus statements. (See Sackett, Rosenberg, Muir-Gray, Haynes, & Richardson, 1996, for more information on levels of evidence.)
A total of 4,457 references were included for the focused question. The consultant to the EBP Project completed the first step of eliminating references on the basis of citation and abstract. The systematic reviews were carried out as academic partnerships in which academic faculty worked with graduate students to conduct the reviews. The review team, which consisted of the four authors, completed the next step of eliminating references on the basis of citations and abstracts. Two authors independently reviewed abstracts. A third author settled disagreements when necessary, and any discrepancies were resolved through discussion within the review team.
The full-text versions of potential articles were retrieved, and the review team determined final inclusion in the review on the basis of predetermined inclusion and exclusion criteria. Two people reviewed each article and rated it according to quality (scientific rigor and lack of bias) and level of evidence. Each article included was then abstracted by two authors in an evidence table (see Supplemental Table 1, available online at http://otjournal.net; navigate to this article, and click on “Supplemental”) that provides a summary of the methods and findings of the articles. AOTA staff and the EBP Project consultant reviewed the evidence table to ensure quality control. See Figure 2 for a diagram of the review process. The strength of evidence was evaluated using the guidelines of the U.S. Preventive Services Task Force (2013).
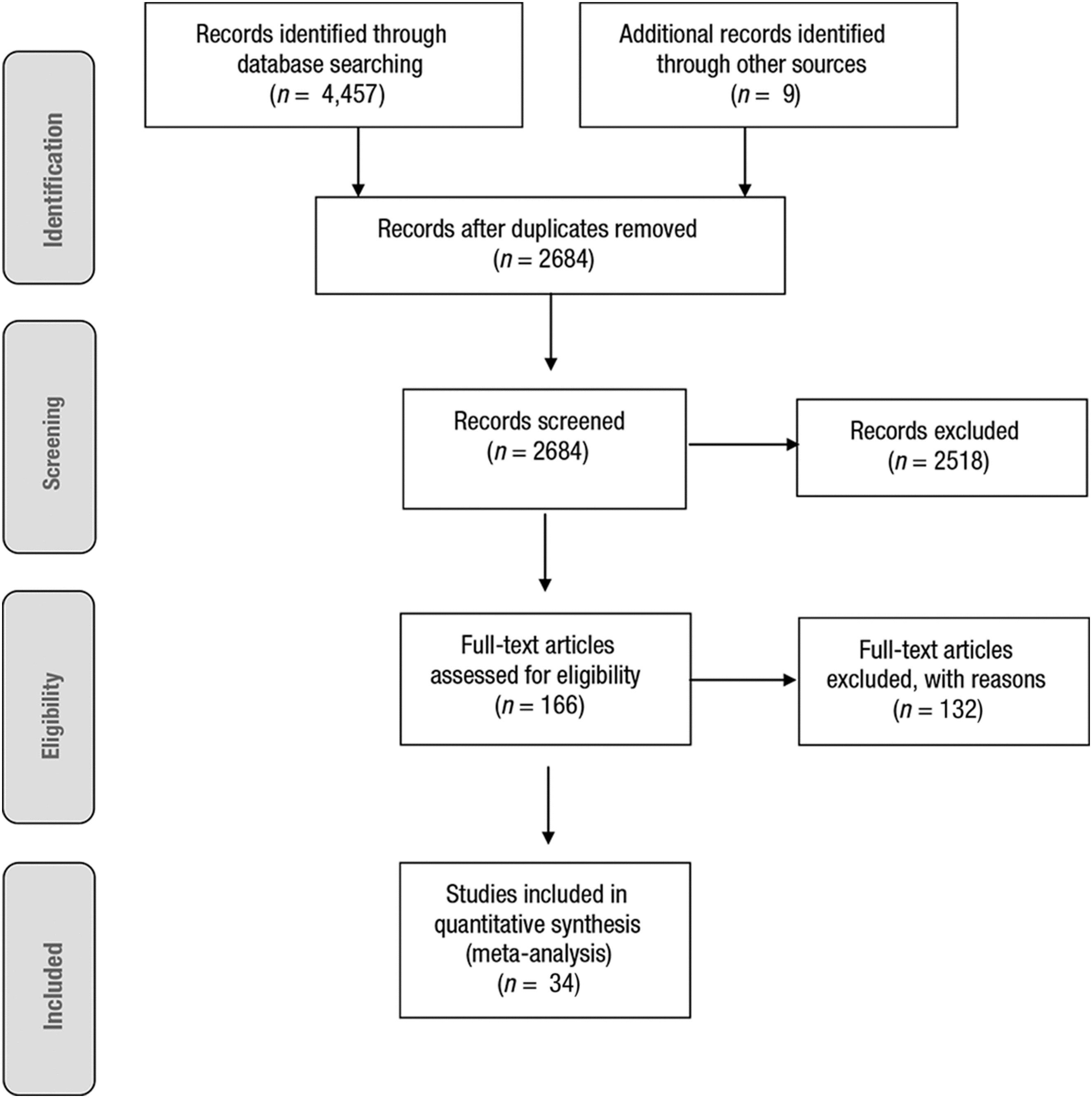
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of studies included in review.
Results
The literature search and assessment of eligibility resulted in a total of 34 articles that met the criteria. For each article included in the evidence table, the citation, design, level of evidence, interventions, selected outcome measures, and selected results related to the research question were extracted. Sixteen of the articles represent Level I evidence (McConachie & Diggle, 2007; Nefdt, Koegel, Singer, & Gerber, 2010; Raj & Salagame, 2010; Rickards, Walstab, Wright-Rossi, Simpson, & Reddihough, 2007, 2009; Roberts et al., 2011; Scarpa & Reyes, 2011; Schertz, Reichow, Tan, Vaiouli, & Yildirim, 2012; Schultz, Schmidt, & Stichter, 2011; Sofronoff, Attwood, Hinton, & Levin, 2007; Solomon, Ono, Timmer, & Goodlin-Jones, 2008; Tonge et al., 2006; Welterlin, Turner-Brown, Harris, Mesibov, & Delmolino, 2012; Whittingham, Sofronoff, Sheffield, & Sanders, 2009a, 2009b; Wong & Kwan, 2010), 4 articles represent Level II evidence (Fava et al., 2011; Keen, Couzens, Muspratt, & Rodger, 2010; Remington et al., 2007; Samadi, McConkey, & Kelly, 2013), 11 articles represent Level III evidence (Bendixen et al., 2011; Dunn et al., 2012; Gika et al., 2012; Okuno et al., 2011; Pillay, Alderson-Day, Wright, Williams, & Urwin, 2011; Probst & Glen, 2011; Reed et al., 2009; Research Units on Pediatric Psychopharmacology [RUPP] Autism Network, 2007; Reynolds, Lynch, & Litman, 2011; Roberts & Pickering, 2010; Smith, Greenberg, & Mailick, 2012), and 3 represent Level IV evidence (Binnendyk & Lucyshyn, 2008; Singh et al., 2006; Steiner, 2011). These articles were published in 22 different journals, with the Journal of Autism and Developmental Disorders (4 articles), Research in Autism Spectrum Disorders (4 articles), and Journal of Positive Behavior Interventions (3 articles) represented most frequently. Intervention and study length varied considerably; the shortest was just 3 wk, and the longest was 25 hr/wk for 2 yr.
Population
In 16 of the articles, the caregivers of children with ASD were the study participants. The children with ASD were the study participants in 8 articles, and 9 focused on both the caregiver and the children. The last article studied teams composed of the child, parents, and the professionals working with the child, including occupational therapists. As is typical of ASD, the majority of child participants were male, and they ranged in age from 1 to 17 yr. The majority of caregivers were mothers. Nine studies (27%) occurred outside the United States, 4 in Australia and 1 each in Canada, Germany, Greece, Hong Kong, and Japan.
Outcome Measures
The studies used 31 different published assessment tools for data collection, most of which were parent-report measures, along with study-specific assessments, Goal Attainment Scaling, video coding, and interviews. The tool most commonly used to measure the impact of an intervention on the family was the Parenting Stress Index (Abidin, 1995), which was used in 15 of the studies (see Supplemental Table 1). With such variability in measures, outcomes were categorized into two primary categories: (1) parental self-efficacy, confidence, and competence and (2) parental decreased stress, improved family coping and resiliency, and quality of life. The second category included any measures of parental mental health, such as level of depression.
Summary of Study Themes
Two primary themes emerged from this review. The first was intervention type, and the second was location. Interventions commonly either were based in behaviorism and often used a parent-mediated intervention focus with the child or followed a parent training–coaching model that often used a more child-directed approach. These studies as a whole took place in one of two primary locations: in a center such as a rehabilitation or educational center or in the home. Each type of intervention was studied in each location for various outcomes. Some studies combined center-based programming and home programs.
The majority of interventions for parents were a form of parent training, education, or coaching, either alone or in combination with a parent-mediated intervention directed toward the child. Curriculum content for the parent training varied and most frequently promoted enhanced communication and interaction–play between the caregiver and the child, a decrease in problem behaviors in the child, and the establishment of effective routines. Information about ASD and available services was often included as part of the intervention or as part of parent exchanges in study-specific parent groups. One study examined the impact on parents of relaxation techniques, another examined mindfulness training, and a third examined comments focused on the child’s strengths rather than deficits. Overall, evidence for specific occupational therapy interventions or occupational therapist involvement was limited.
Autism-specific behavioral intervention methods included in these studies included discrete trial training, Early Intensive Behavioral Intervention, incidental teaching, Picture Exchange Communication System, pivotal response training, and Treatment and Education of Autistic and related Communication Handicapped Children (TEACCH). Cognitive–behavioral therapy was used as an intervention in 2 studies.
Parent Education and Coaching in Center-Based Programs
The strength of evidence for parent education and coaching provided in a center was moderate for improving general efficacy and confidence (Okuno et al., 2011; Pillay et al., 2011; Reynolds et al., 2011) and task-specific efficacy (Raj & Salagame, 2010). This group included 3 Level III studies and 1 Level I study.
The strength of the evidence for the ability of these interventions to reduce stress and improve family coping and resiliency when provided in a center was mixed. Five Level I studies, 2 Level II studies, and 3 Level III studies found either decreased stress (RUPP Autism Network, 2007; Samadi et al., 2013; Schultz et al., 2011; Wong & Kwan, 2010) or no change in stress (Fava et al., 2011; McConachie & Diggle, 2007; Reed et al., 2009; Smith et al., 2012; Solomon et al., 2008; Tonge et al., 2006). One Level III study documented that family atmosphere improved (Probst & Glen, 2011).
Parent Education and Coaching in the Home and in Home and Center Combined
The strength of evidence for parent education and coaching provided in the home or the home and a center combined was limited. This group included 1 Level I study, 1 Level II study, and 3 Level III studies and resulted in positive outcomes of improved confidence (Nefdt et al., 2010) and improved efficacy only for those parents with initial low efficacy (Keen et al., 2010).
The strength of the evidence for parent coaching in the home or home and center to reduce stress and improve family coping and resiliency was also limited. One Level I, 1 Level II, 2 Level III, and 1 Level IV studies were included in this category. Of those, 4 documented decreased stress (Bendixen et al., 2011; Dunn et al., 2012; Keen et al., 2010; Schertz et al., 2012), and 1 documented improved quality of life (Binnendyk & Lucyshyn, 2008). The evidence that parent coaching interventions can improve family participation in daily life routines was insufficient; it was documented in only 1 Level III study (Dunn et al., 2012).
Behavioral Interventions in Center-Based Programs
Five Level I studies suggested moderate to strong evidence that interventions provided in a center can improve confidence (Roberts et al., 2011; Scarpa & Reyes, 2011; Sofronoff et al., 2007), improve parental efficacy at 6-mo follow-up (Whittingham et al., 2009a), and improve parental attributions (Whittingham et al., 2009b). Mixed evidence exists related to the impact of center-based behavioral interventions on parental stress, coping, and quality of life. This category included 1 Level I study, 2 Level II studies, 1 Level III study, and 1 Level IV study. One study demonstrated decreased stress (Rickards et al., 2009), and another found decreased stress in the control group but no change in the treatment group (Fava et al., 2011). One found improved well-being (Roberts & Pickering, 2010), and another documented increased paternal depression (Remington et al., 2007).
Behavioral Interventions in the Home
Two Level I studies suggested moderately strong evidence that behavioral interventions in the home had no effect on family outcomes related to self-efficacy, confidence, or perceived competence (Rickards et al., 2007; Roberts et al., 2011). In relation to these interventions and parental stress, coping, and quality of life, the evidence is mixed. One study documented decreased stress (Rickards et al., 2009), and others found no changes (Rickards et al., 2007; Welterlin et al., 2012). In 1 study, paternal depression increased (Remington et al., 2007).
Interventions Focused on Relaxation, Mindfulness, and Strengths
A few studies examining parent outcomes used interventions that did not neatly fall into the behavioral or parent training models. These interventions may improve stress (Gika et al., 2012); satisfaction with parenting (Singh et al., 2006); or parental interaction, affect, and physical affection (Steiner, 2011), but at this time the evidence is insufficient.
Discussion
The results of this systematic review suggest a body of literature in its infancy. Although ample evidence has documented the excessive stress of parents of children with ASD (Karst & Van Hecke, 2012; Montes & Halterman, 2007; Mugno et al., 2007; Schieve et al., 2007), this review found limited evidence that interventions can improve parental stress levels and some evidence that interventions can in fact increase it or lead to greater levels of depression. However, the evidence is somewhat stronger that center-based interventions can at least improve parental confidence, competence, and feelings of self-efficacy. Given the inverse relationship found between stress and self-efficacy (Giallo et al., 2013; Raikes & Thompson, 2005), improving self-efficacy may be one method of effectively reducing stress over time (Jones & Prinz, 2005). The somewhat stronger evidence for center-based programs may reflect the greater intensity of the interventions provided in the center as opposed to the home, or it may reflect the greater emphasis on research in the center-based programs, with higher levels of evidence available generally for center-based programs than for home-based ones, perhaps because of greater availability of resources for research. Despite the lack of strong evidence at this time, this review of the literature found slight improvements in comparison with similar earlier reviews of the literature (Brookman-Frazee et al., 2006; Schultz et al., 2011). The current systematic review contains literature of a higher level of evidence, with more studies that included measures of parental competence, standardized assessment tools, and examinations of fidelity.
Limitations
This review was limited to articles published in English from January 2006 to April 2013. Systematic reviews are also limited by the quality of the evidence being reviewed, based on the design and methods of the individual studies. The risk of bias in this group of literature as a whole is high (see Table 1). Issues included small sample sizes and limited descriptions of the psychometric properties of outcome measures. In addition, many of the studies included concurrent interventions; therefore, separating the effects of the interventions can be difficult. Many of the articles reviewed had multiple additional issues, including outcomes reported primarily via parent-report measures, limited measures of fidelity to intervention, and limited measures or reports of attendance levels and participation of participants. Intervention length varied greatly between studies, making comparison difficult. In addition, the samples were frequently nonrepresentative, mostly White, and with higher socioeconomic status and educational levels, and the studies as a whole were skewed almost completely to the voice of mothers. Many (27%) were completed outside the United States, and different cultures may have different family expectations. Most articles provided limited information on the child’s characteristics, but the included children were mostly of younger ages.
Risk of Bias
Note. + = low risk of bias; ? = unclear risk of bias; − = high risk of bias; N/A = not applicable.
Implications for Future Research
Given the focus on routines in the Occupational Therapy Practice Framework: Domain and Process (3rd ed.; AOTA, 2014) and the importance of family-centered care, a major gap in the literature is a lack of evidence that occupational therapy can improve family function, participation in family routines, and family engagement. There is a huge need for more research in this area. Researchers in occupational therapy should consider including parental and family outcome measures in intervention studies completed with children. Future studies should investigate the length of intervention necessary to document changes in family outcomes, because the variation in the studies reviewed was enormous. In addition, one article found evidence suggesting that perhaps interventions for families need a lengthy time period to have an impact (Dunn et al., 2012).
There is a need for better measures for families as well. None of the articles specifically explored the impact of interventions on coping or resiliency; instead, the focus was most often on reducing stress. The most frequently used measure, the Parenting Stress Index, may not be the best measure of family functioning and is not meant to be a measure of participation in family routines or engagement in family activities. Perhaps more important, research on family functioning should focus on positive outcomes such as coping and resiliency, hopefulness, or even quality of life as opposed to merely reducing parental stress.
Two intriguing avenues for more rigorous study in the future were found. Parents reported a benefit of parent-to-parent coaching and interaction in qualitative comments and via questionnaires (Pillay et al., 2011; Probst & Glen, 2011; Roberts & Pickering, 2010; Sofronoff et al., 2007). Another article suggested that merely changing the therapists’ verbalizations to focus on a child’s strengths rather than his or her deficits may have an impact on family interaction (Steiner, 2011). These studies are important to replicate with more rigorous methods because they use intervention strategies that are low cost, are fairly easy to implement, and resonate with the philosophy of occupational therapy and family-centered care.
Implications for Occupational Therapy Practice
The results of this review have the following implications for occupational therapy practice:
Family-centered care has been widely supported as a critical part of treating children with disabilities (Dempsey, Keen, Pennell, O’Reilly, & Neilands, 2009).
The pervasive nature of ASD has a significant impact on daily life for both the child and the family; as a result, it is critical that providers consider the needs of the entire family (Hodgetts, Nicholas, Zwaigenbaum, & McConnell, 2013).
Occupational therapists support family-centered care because they recognize the interrelationship of the client’s skills, performance patterns, and environment, including the family and home environment (Rodger, Ashburner, Cartmill, & Bourke-Taylor, 2010).
Family-centered care for children with ASD must also address the well-being of parents, siblings, and other caretakers by using evidence-based interventions whose outcomes will benefit the family’s needs.
Occupational therapists can provide family-centered intervention through the purposeful consideration of how individual and family occupations interact with client factors and performance skills and patterns, taking into account the context and the environment (AOTA, 2014).
Families of children with ASD are stressed, and removing the stressors they face may be impossible. However, improving parental self-efficacy and coping and focusing on family resilience are important goals for occupational therapy interventions.
Supplemental Materials
Supplementary material for Effectiveness of Interventions for Children With Autism Spectrum Disorder and Their Parents: A Systematic Review of Family Outcomes
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2015.017855.pdf for Effectiveness of Interventions for Children With Autism Spectrum Disorder and Their Parents: A Systematic Review of Family Outcomes by Heather Miller Kuhaneck, Stephanie Madonna, Audrey Novak and Emily Pearson in The American Journal of Occupational Therapy
Supplementary material for Effectiveness of Interventions for Children With Autism Spectrum Disorder and Their Parents: A Systematic Review of Family Outcomes
Supplementary material, sj-pdf-2-aot-10.5014_ajot.2015.017855.pdf for Effectiveness of Interventions for Children With Autism Spectrum Disorder and Their Parents: A Systematic Review of Family Outcomes by Heather Miller Kuhaneck, Stephanie Madonna, Audrey Novak and Emily Pearson in The American Journal of Occupational Therapy
Footnotes
*
Indicates studies that were systematically reviewed for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.