
Abstract
This article builds on the work of Case-Smith and colleagues and proposes a roadmap to guide future research in occupational therapy. To foster best practice in the application of principles and practices of sensory integration (SI), the pillars of practice, advocacy, and education are identified as elements that provide the foundation for research. Each pillar ensures that SI research is conducted in a rigorous and relevant manner. To this end, achievements to date are discussed, with proposed goals presented for each pillar. Finally, the roadmap builds on the pillars and outlines implications for occupational therapy with the overarching theme that a wide array of scientists, educators, therapists, and service recipients will be needed to ensure that those who may benefit most have access to intervention that is evidence based, theory driven, and provided within the highest standards of service delivery.
Keywords
In 2014, Case-Smith, Weaver, and Fristad published a seminal systematic review of sensory interventions for children with autism spectrum disorder (ASD). Their article provided much-needed clarity regarding the differences between Ayres Sensory Integration® (ASI) intervention and other sensory interventions and has had far-reaching influence in interdisciplinary fields by clarifying the literature and research on these interventions. In addition, Case-Smith and colleagues challenged occupational therapy to conduct systematic, rigorous study of sensory interventions and their impact on participation and occupation. This article builds on Case-Smith and colleagues’ call to action by providing a summary of the state of the science in sensory integration (SI) and proposing a roadmap to guide future research that builds on advancements in practice, advocacy, and education. The intent of this article is to foster research and best practice and ensure that therapists and researchers use the principles and practices of SI with the highest standards in evidence-based service delivery.
State of the Science in Sensory Integration
The SI frame of reference has grown and evolved since Ayres (1963) introduced her theory, assessment, and intervention principles to the occupational therapy profession. In Fall 2001, a group of researchers, clinicians, and educators came together under a grant from the National Institutes of Health (HD41614–01; Lucy Jane Miller, Principal Investigator) to evaluate the state of the field in SI and to strategize about the research needed to inform practice. The goals included (1) identify and clearly define the principles of ASI and operationalize them into a replicable intervention manual that could guide practice and research; (2) create a measure of fidelity to assess treatment adherence in research and practice; (3) identify objective, sensitive outcome measures that capture both the functional and the quality-of-life changes reported to occur as a result of this treatment; (4) study the neural mechanisms of action that underlie deficits in SI to enable intervention targeted toward these mechanisms and to guide assessment of changes in these mechanisms; (5) conduct randomized controlled trials (RCTs) to evaluate the effectiveness of ASI intervention; and (6) increase access to the evidence (American Occupational Therapy Association [AOTA], 2015b).
Over the next 15 yr, many of these goals were realized by this group and by others, including the development of a fidelity measure (Parham, Cohn, Spitzer, et al., 2007) that defined the structure and process elements core to ASI intervention. Subsequent research documented the reliability and content validity of the ASI Fidelity Measure©, especially when used by therapists trained in SI (May-Benson et al., 2014; Parham et al., 2011). The Fidelity Measure has been useful in research and practice, laying the groundwork for a subsequent case report (Schaaf, Hunt, & Benevides, 2012) and two RCTs that focused on children with ASD (Pfeiffer, Koenig, Kinnealey, Sheppard, & Henderson, 2011; Schaaf et al., 2014).
Miller and colleagues (Miller, Coll, & Schoen, 2007; Miller, Wilbarger, Stackhouse, & Trunnell, 2002) conducted pilot intervention studies and provided important foundational work for future randomized trials. Subsequently, an intervention manual was developed to establish consistency and rigor in the implementation of ASI intervention, making it replicable and providing models and tools for future work (Schaaf & Mailloux, 2015). Mailloux et al. (2007) investigated Goal Attainment Scaling (GAS) as a means of defining outcomes that measure functional change after ASI intervention. They concluded that the GAS process was an effective means of establishing meaningful goals and measuring occupational performance outcomes (Mailloux et al., 2007). GAS was used in the aforementioned RCTs and found to be a sensitive outcome measure.
Multiple studies focused on examining the mechanisms underlying under- and overreactivity to sensation, finding autonomic nervous system correlates, specifically elevated sympathetic nervous system responses and slower habituation to sensory challenge in children with overresponsivity or hyperreactivity to sensation (Chang et al., 2012; McIntosh, Miller, Shyu, & Hagerman, 1999; Schoen, Miller, Brett-Green, & Nielsen, 2009). Children with attention deficit hyperactivity disorder (ADHD) and hyperreactivity were found to be more reactive to nonspecific stimuli during recovery from sensory challenges (Lane, Reynolds, & Thacker, 2010). Reynolds, Lane, and Gennings (2010) indicated that, on the basis of cortisol responses to sensory stressors, sensory overresponsivity may be a moderating variable for children with diagnoses such as ADHD. Schaaf and colleagues (Schaaf, Miller, Seawell, & O’Keefe, 2003; Schaaf et al., 2010) documented atypical parasympathetic nervous system responses to sensory challenges. Adults and children with difficulty modulating sensation have been noted to show less gating (filtering) of sensory input (Davies & Gavin, 2007; Kisley, Noecker, & Guinther, 2004). Davies and colleagues (Davies, Chang, & Gavin, 2009; Gavin et al., 2011) further found that children with modulation difficulties showed atypical sensory registration relative to typically developing children, and Brett-Green, Miller, Schoen, and Nielsen (2010) documented atypical multisensory integration. Recently, imaging studies documented diminished white matter microstructure in sensory processing pathways involved in multisensory integrative processes and single sensory processing (Chang et al., 2014; Owen et al., 2013). In many of these studies of mechanisms underlying the process of sensory modulation, links have been made to behavioral measures such as the Sensory Profile and Short Sensory Profile (Dunn, 1999) and the Sensory Processing Measure (Chang et al., 2012; McIntosh et al., 1999; Owen et al., 2013; Parham, Ecker, Kuhaneck, Henry, & Glennon, 2007; Schaaf et al., 2010) as well as performance activities (e.g., anxiety, sleep, adaptive behaviors; Lane et al., 2010; Lane, Reynolds, & Dumenci, 2012; Reynolds et al., 2010; Reynolds, Lane, & Thacker, 2012; Schaaf et al., 2010).
Advancements in the field of SI have paralleled developments in the field of ASD, including increased specificity in diagnostic criteria and efforts to identify effective treatments. Diagnostic criteria for ASD were refined in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2013) to include sensory features as one manifestation of the “restricted, repetitive patterns of behavior, interests, or activities” criteria. Consequently, interest is growing in understanding patterns of sensory features in ASD (AOTA, 2015b; Lane, Molloy, & Bishop, 2014), articulating best practices for assessment of sensory features (Schaaf & Lane, 2015) and implementing effective treatments to decrease the impact of sensory symptoms on behavior, learning, and functional skills (Schaaf et al., 2014).
Concurrently, the National Institute of Mental Health (NIMH) has shifted its research focus to dimensions of behavior rather than unitary clinical disorders. NIMH’s (n.d.) adoption of the Research Domain Criteria project created a framework to support research that examines common dimensions across clinical conditions. This paradigm shift is stimulating interest in how SI difficulties contribute to varying conditions, facilitating the translation of basic science into practice and supporting the development of knowledge of etiology and intervention for many diagnoses (NIMH, n.d.).
Collectively, the increased research and clarity about SI and the momentum in ASD research and practice mentioned earlier created a platform for realization of the vision created by Ayres and articulated more recently by Case-Smith and colleagues (2014). These synergies promoted conversations about SI in varied scientific venues and an increased recognition of ASI intervention as a potentially valuable intervention strategy. To build on this momentum and solidly situate SI within the scientific community, additional activities are needed. Here, we provide a roadmap to guide ongoing research in the field of SI. We identify three pillars (practice, advocacy, and education) that are built on the foundation of research and serve as supports for the advancement in and clarification of future research (Figure 1). We propose that these three pillars provide a framework for organizing work in this field and promoting continued growth in the science of SI.
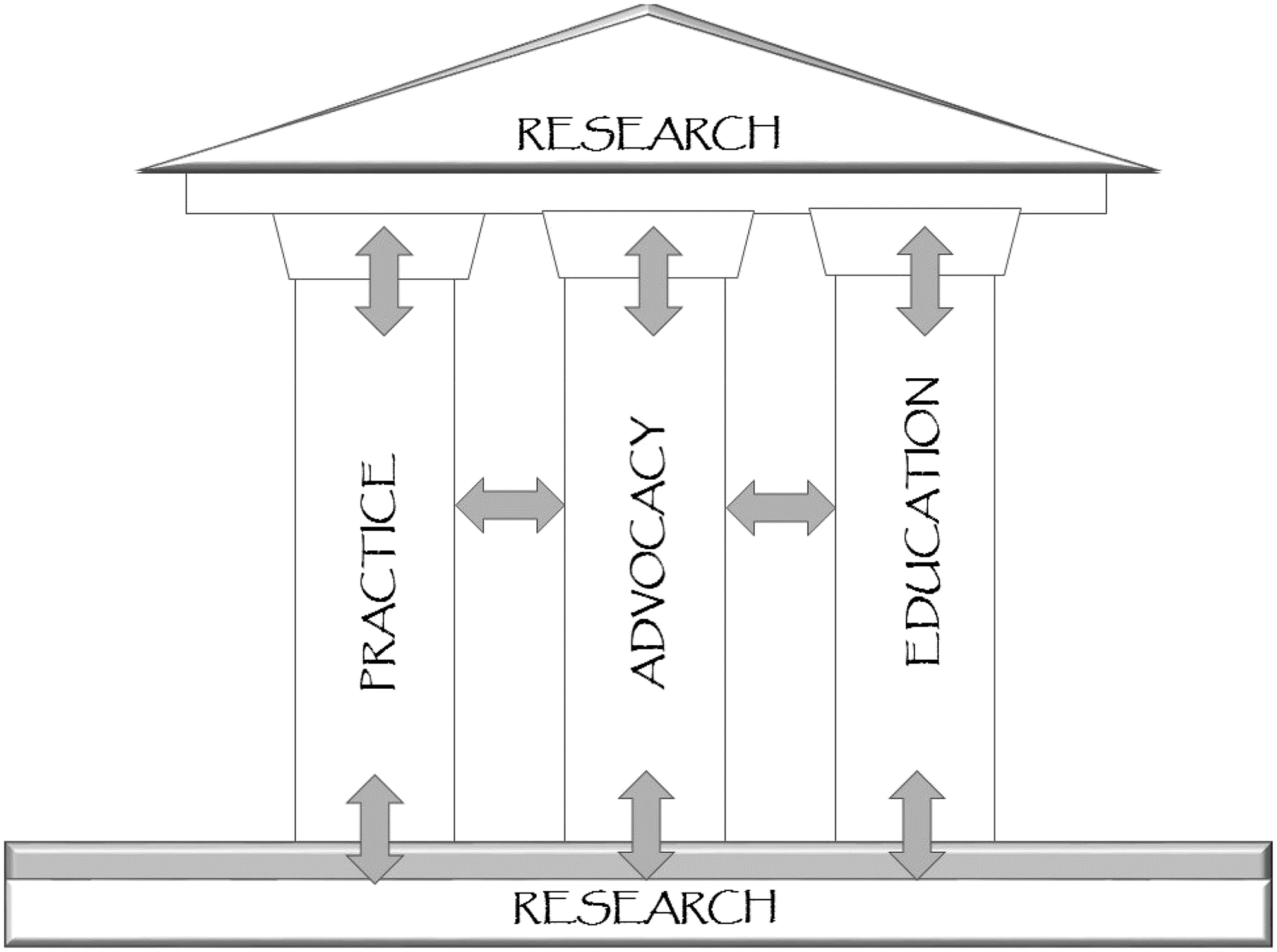
Critical elements for a roadmap for sensory integration research.
Practice
Although many advances in SI research have shaped practice, we note four activities that have had a substantial influence: (1) the development, publication, and testing of the Fidelity Measure for ASI intervention (Parham et al., 2011); (2) the publication of RCTs on ASI intervention (Miller, Coll, & Schoen, 2007; Pfeiffer et al., 2011; Schaaf et al., 2014); (3) the publication of a manualized approach for ASI describing a step-by-step, replicable guide to ASI (Schaaf & Mailloux, 2015); and (4) the trademarking of the term Ayres Sensory Integration, which serves to clearly distinguish ASI intervention from other interventions that may use sensory strategies or the same equipment or activities in similar types of settings (Smith Roley, Mailloux, Miller-Kuhaneck, & Glennon, 2007).
Schaaf et al. (2014) found that children with ASD (of varying severity) made significant gains in individual goals (p = .003, d = 1.2) as measured by GAS and in functional skills as measured by the Pediatric Evaluation of Disabilities Inventory (Haley, Coster, Ludlow, Haltiwanger, & Andrellos, 1992). Miller, Schoen, James, and Schaaf (2007) also found that children with sensory difficulties and no other clinical diagnosis showed improvement on individualized goals and measures of attention, and Pfeiffer et al. (2011) found that children with ASD improved in their individual goals with ASI intervention.
Although these RCTs provide important information to inform practice, more research is needed, specifically practice-based research that raises the question of dosage and outcomes and applies findings to multiple settings (Westfall, Mold, & Fagnan, 2007). This research might include case reports and single-subject research designs to facilitate research that reflects what happens in everyday practice and occurs in the setting in which children and families receive their ongoing care (Westfall et al., 2007).
Advocacy
Advocacy efforts at local, national, and international levels support policy changes, funding streams for services, and program development for the benefit of people with SI difficulties. Enhanced public awareness raises the likelihood that consumers will receive appropriate and effective services and that these services will be reimbursed accordingly. Research plays a critical role in advocacy because it furnishes data about the needs of people with SI difficulties, and it advances knowledge regarding how intervention can be implemented for maximal benefit.
Grassroots advocacy efforts by Ayres and colleagues in the 1970s included the creation of a nonprofit organization, the Center for the Study of Sensory Integrative Dysfunction, to support research, education, and practice. This group lobbied AOTA to create the Sensory Integration Special Interest Section. This section is now a long-standing and successful organizational body that serves as an important mechanism for fostering and publishing practice-based research, aids AOTA membership in understanding and disseminating information related to SI, and helps shape the future of ASI within the occupational therapy profession (AOTA, 2015b). Official documents from AOTA serve as resources for advocacy groups. These documents also furnish critical information that is used in formal responses and rebuttals to publications providing misinformation or unsubstantiated criticism about ASI (AOTA, 2015a).
Web-based groups such as the Sensory Integration Global Network (SIGN; http://www.siglobalnetwork.org), the ASI 2020 Vision (https://sites.google.com/site/2020asivision/home), and the Sensory Processing Disorder Foundation (http://www.spdfoundation.net) further these standards by providing resources for professionals and consumers. Public awareness about the effectiveness of ASI is bolstered when research studies, such as the RCT conducted by Schaaf et al. (2014), are highlighted by prominent organizations such as Autism Speaks (2003).
Although consumers are highly favorable toward ASI, more research is needed to capture parent- and consumer- and self-reported outcomes. Advocacy efforts must involve families and people who live with SI challenges themselves. Their input has the potential to increase funding streams for services and research as well as expand public awareness of the need for and effectiveness of SI intervention.
Education
Education in ASI theory, assessment, and intervention is critical for practitioners and researchers to understand and refine this body of knowledge and to effectively implement the assessment and intervention practices that emanate from it. To impart knowledge to students, colleagues, practitioners, and the public, it is imperative that educators, students, and practicing therapists be well informed regarding established and emerging knowledge in ASI.
In entry-level occupational therapy education, content on SI is minimal, even though ASI is a leading area of practice and research in the profession. Occupational therapists are the recognized experts in ASI and are frequently expected to provide ASI intervention. SI as a practice area is routinely used by 85% to 93% of pediatric occupational therapists (AOTA, 2010) as well as a growing number of occupational therapists practicing in the field of mental health. Moreover, ASI and sensory-based strategies are the third most commonly used intervention in the United States for children with ASD (Green et al., 2006). Unfortunately, entry-level occupational therapists are often hired to provide these interventions in diverse school, early intervention, and hospital settings without adequate preparation in entry-level education and without high-quality postprofessional education. Thus, core knowledge of ASI theory and intervention is important for entry-level therapists. Currently, the Accreditation Council for Occupational Therapy Education (ACOTE®) standards for doctoral and master’s degree entry-level programs do not specify theories or frames of reference that must be taught, and the standards that address sensory and motor functions could be met without any ASI content in the curriculum (AOTA, 2012).
Despite the fact that no ASI content is required for an entry-level occupational therapy program to be accredited, many occupational therapy faculty appear to be teaching at least some content related to ASI. In a survey conducted by Reynolds, Watling, Zapletal, and May-Benson (2012), 97.5% of the 40 responding schools (of 148 surveyed) reported teaching SI theory, and 94.7% of these schools reported teaching SI intervention. Curriculum hours dedicated to SI were limited and highly variable, with lecture time ranging from 1 to 8 hr and experiential lab or observation time ranging from 1 to 12 hr.
Ayres believed that practice in SI required specialized training and knowledge at the postgraduate level. Since the late 1990s, advanced training for SI certification has been administered jointly by the University of Southern California and Western Psychological Services as the USC/WPS Sensory Integration Certification Program (USC, n.d.) and, more recently, by the SI Network (http://www.sensoryintegration.org.uk), the South African Institute for Sensory Integration (http://www.instsi.co.za.winhost.wa.co.za), and the Seven Senses Association of Portugal (http://www.7senses.pt), among others. Information about these and other SI certification courses can be obtained from the respective websites or via the SIGN website (http://www.siglobalnetwork.org).
In addition to certification, mentorship is a critical aspect of postprofessional education in ASI, and it should be provided by occupational therapists with expertise in ASI clinical reasoning, assessment interpretation, and intervention implementation. Mentorship may be provided on a one-to-one basis in practice settings, through intensive training programs offered by various organizations and associations, or through online mentorship with expert practitioners. Parham et al. (2011) provided guidelines for mentorship, indicating that therapists providing ASI-based occupational therapy should have completed certification or training in SI or the Sensory Integration and Praxis Test (Ayres, 1989) with a minimum of 50 hr of advanced training mentorship in ASI by an experienced therapist. It is unlikely that many therapists who purportedly use ASI meet these minimum competencies for ASI practice.
To complement certification in SI, numerous continuing education courses are available in both in-person and online formats. It can be difficult for practitioners to know which continuing education opportunities offer quality information. When a practitioner seeks courses that will best support evidence-based practice of ASI intervention, care should be taken to ensure that courses are provided by therapists who are certified in SI and have proven experience in implementing ASI intervention. A record of therapists certified in SI is kept on the Western Psychological Services website (http://wpspublish.com).
A Roadmap
A substantial amount of research in SI exists, leading to clearer descriptions of ASI intervention and a growing body of evidence for its effectiveness. For the field to continue to move forward, additional practice, advocacy, and education activities are needed. The roadmap presented here identifies important areas that will support a robust infrastructure to ensure that ASI research is conducted in a rigorous manner so that its effectiveness, utility, and social validity will be continually evaluated. This roadmap necessitates participation by a wide array of scientists, educators, therapists, and service recipients to ensure that those who may benefit most from this approach are afforded the opportunity to do so and that those who use this approach in intervention will do so from an evidence-based, theory-driven perspective.
Practice
Develop practice-based research networks to focus on the following activities:
Conduct multisite studies of ASI
Define new research questions emanating from practice
Engage therapists in research-based activities to inform new research questions
Promote and ensure best practices that use theory, evidence, and outcome measurement
Use and evaluate ASI in varied settings, including the home, school, and community
Conduct clinical research that evaluates ASI outcomes at the neural and behavioral levels and links these levels of change with functional performance
Characterize and elucidate mechanisms underlying sensory integrative impairments and apply this knowledge to practice
Define client characteristics (phenotypic characterization) to more precisely tailor individually targeted ASI intervention
Conduct studies to identify the optimal intensity, frequency, and duration of intervention (i.e., dosage) across different clinical groups.
Advocacy
Occupational therapy practitioners can engage in the following advocacy activities:
Serve as peer reviewers on selected journals to ensure that knowledge dissemination has high validity and veracity
Serve on boards of professional and community groups that have an interest in ASI to guide decisions regarding reimbursement and service delivery models
Partner with and support various international, professional, and diagnostic-specific organizations to promote and provide information about ASI that accurately reflects the difference between ASI and sensory-based strategies
Increase access to documents that clearly describe ASI to the lay public
Advocate for funding to further study the underlying mechanisms of ASI intervention and expected outcomes
Educate constituents on the role of sensation and sensory–motor abilities as an important foundation for skilled performance of activities and participation in daily life.
Education
In education, efforts are needed in the following areas:
Develop appropriate guidelines and materials on core ASI content for occupational therapy curricula
Incorporate education on ASI into occupational therapy educational programs to ensure that entry-level therapists have the needed knowledge and skills to participate in practice and research in this area
Adequately prepare faculty in entry-level occupational therapy programs to teach concepts related to SI and ASI in the curriculum
Widely disseminate information regarding pathways to develop competencies in ASI and provide high-quality continuing education, postprofessional coursework, and direct mentorship from expert practitioners
Support opportunities for development of new researchers through education and mentorship programs, postdoctoral training, and options to work under the direction of funded researchers
Train practitioners in case study and single-subject methodology as a basis for engagement in practice-based research.
Implications for Occupational Therapy Practice
Although gains have been made toward a deeper understanding of SI function and impairment, much remains to be done. Occupational therapists have a crucial role to play in making important contributions to all aspects of the roadmap presented here. Specifically, implications for occupational therapy are as follows:
Practice: Use the evidence-based procedures available, tap into resources such as the ASI Fidelity Measure (Parham et al., 2011) and the ASI guidebook (Schaaf & Mailloux, 2015), visit sites where research and resources are available, and develop partnerships between clinicians and researchers
Advocate: Access the literature, understand what has been accomplished and what remains to be done, advocate for clients to have the best available SI services, and serve on boards and meet with policymakers to ensure that knowledge about SI is translated into reasonable policies
Educate: Work within existing systems to distinguish between ASI and sensory-based interventions and educate administrators, colleagues, and consumers about the existing research and available knowledge in the field.
Conclusion
The practice of ASI has grown exponentially since first introduced by Ayres in the 1960s. Recent research and scholarship have provided a strong foundation of knowledge relative to potential mechanisms underlying SI impairments. We propose a three-pronged roadmap to continue this forward momentum and support ongoing research and theory development. Practice must drive research, consistently adhere to the principles and procedures at the heart of ASI, be evidence based, and use available tools to ensure fidelity. Advocacy is needed from practitioners, professional organizations, and consumers to make certain that SI services are of the highest quality and are available to those who need them. Education must address critical issues in professional entry-level and postprofessional education to ensure that knowledge in ASI is being used appropriately in practice. These three pillars will stimulate discourse in the profession that will disseminate valuable knowledge and raise critical questions for researchers to answer.