
Abstract
Despite recognition of the rights of disabled people to sexuality, occupational therapists continue to not address sexuality in practice. This failure can be understood as a consequence of social discourses relating to sexuality and disability and a professional discourse that values certain occupations over others. Given the importance of sexuality to the human experience and the evidence of the link between the opportunity for sexual expression and well-being, occupational therapists need to change their practice in relation to sexuality and disability. One method of achieving this change may be to adopt a rights-based approach to sexuality and disability. This article presents the possibilities offered by such an approach, discusses implications for occupational therapy practitioners, and proposes suggestions for future actions to ensure that the rights of disabled people to sexuality are embedded in occupational therapy practice.
Despite recognition of the needs and rights of disabled people1 to sexuality, many health care professionals report reluctance to address sexuality (Esmail, Darry, Walter, & Knupp, 2010). Much of this reluctance can be traced to social discourses that limit the right to sexuality to an idealized young, heterosexual, able-bodied male and subsequently deny the sexuality of those who do not fit this model (Tepper, 2000). In occupational therapy, the situation is also influenced by professional values that are grounded in a middle-class worldview, which privileges certain occupations over others (Hammell, 2009) and in which sex and sexuality are restricted to a private domain and remain hidden.
The aim of this article is to discuss how the combination of social discourses about sexuality and disability and professional understandings of occupation has shaped current occupational therapy practice relating to sexuality. We offer suggestions for devising a more inclusive approach to sexuality and disability framed in a human rights perspective and discuss the implications of such an approach for occupational therapy practice, education, and research.
Importance of Sexuality
Human sexuality is a concept that encompasses gender identities and roles, eroticism, sexual orientation, intimacy, sex, and reproduction (World Health Organization, 2006). A large body of empirical evidence has supported the link among well-being, quality of life, and sexuality (Diamond & Huebner, 2012). Research among disabled people has consistently indicated that being able to express one’s sexuality is an important dimension in the construction of a good life (Bahner, 2012; Sakellariou, 2006, 2012).
Sexuality and Occupational Therapy
Occupational therapy practice is shaped by the social and cultural context in which it occurs. Despite frequent designation of sexuality as a private matter in which the state should play no part, a wide variety of sociopolitical institutions regulate who can do what to whom, when, where, and how (Shildrick, 2007; Weeks, 2002). In Western society, this control over sexuality is also supported by a social discourse that privileges monogamous heterosexual relationships between young, able-bodied adults that are genitally and reproductively focused (Shildrick, 2007; Tepper, 2000; Weeks, 2002). This dominant discourse is problematic for many people because it focuses on the behavioral aspects of sexuality and downplays the emotional and relational aspects (Yip, 2010). In addition, this discourse presupposes a single normative sexuality and thus fails to account for the diversity and richness of human sexuality (Sakellariou, 2012).
Sexuality has an acknowledged innate occupational dimension (Hattjar, 2012), and people can express their sexuality through a broad range of occupations, including grooming, caring for a partner, dating, or having sex (Hattjar, 2012; Sakellariou & Simo Algado, 2006a). Despite acknowledgment of the occupational nature of human sexuality, research has suggested that irrespective of national or clinical context, occupational therapists frequently fail to address sexuality in practice (Couldrick, 1998; Hyland & Mc Grath, 2013; McGrath & Lynch, 2014; Penna & Sheehy, 2000).
Many explanations have been offered in the literature for the gap between professional ideology and practice in relation to sexuality, including lack of knowledge among therapists (Hyland & Mc Grath, 2013; McGrath & Lynch, 2014); client factors such as age, marital status, and gender (Couldrick, 1998; McGrath & Lynch, 2014); concerns regarding the therapist’s safety (Couldrick, 1998; Penna & Sheehy, 2000); fear of causing offense or anger (Couldrick, 1998; Hyland & Mc Grath, 2013); perceived lack of relevance and importance of sexuality for people with disability (Couldrick, 1998; Hyland & Mc Grath, 2013); institutional practices and policies that do not prioritize sexuality (Hyland & Mc Grath, 2013; McGrath & Lynch, 2014); personal beliefs and attitudes (Couldrick, 1998; Yallop & Fitzgerald, 1997); and lack of clarity regarding professional roles and concerns regarding damage to professional reputation (Couldrick, 1998; Hyland & Mc Grath, 2013; McGrath & Lynch, 2014). Each of these factors reduces the likelihood that occupational therapists will identify and prioritize issues of sexuality during rehabilitation, and combined they create a professional culture in which sexuality is routinely ignored.
Why has so little progress been made in the practice of occupational therapy in relation to sexuality? We suggest that the failure of occupational therapists to address sexuality reflects a professional enactment of both a social discourse that prizes “corporeal wholeness and predictability above any form of bodily anomaly” (Shildrick, 2007, p. 54) and a professional construction of occupation that is based on “the way of life and associated ideology of middle-class, white, economically secure Westerners” (Kantartzis & Molineux, 2011, p. 73). Combined, these discourses mean that despite the wishes of disabled people (Shildrick, 2007) and a stated professional commitment to holistic practice (Hammell, 2009; Sakellariou & Simo Algado, 2006b), occupational therapists continue to exclude sexuality from everyday practice.
Conceptualizations of Occupation and Sexuality
Several authors (Hammell, 2009; Kantartzis & Molineux, 2011) have suggested that much of occupational therapy professional practice has been influenced by a particular subset of Western values. These values include the need for humans to act on and seek control of their environments, the belief that occupations should lead to achievement of purposeful goals, and the belief that people should engage in occupations that fit within socially regulated temporal patterns and routines of daily activities (Kantartzis & Molineux, 2011). In this way, occupation has come to be understood as something that is “active and self-directed, involving a powerful process of taking control and acting on the environment” (Kantartzis & Molineux, 2011, p. 73).
This understanding of occupation is closely linked to the assumption that occupations can be grouped according to their purpose into three categories: self-care, productivity, and leisure (Hammell, 2009). Such categorization leaves little room for occupations such as sexuality that are not usefully categorized as self-care, 2 productivity, or leisure. Hammell (2009) also noted that occupational therapists have frequently prioritized and promoted occupations relating to self-care and productivity and by doing so have excluded occupations directed toward other concerns from professional practice.
Kantartzis and Molineux (2011) traced occupational therapy’s prioritization of self-care and productive occupations to the influence of a Protestant way of life on the profession’s development. In this way of life, intense activity underpinned by hard work took on a central role, and the desires of the individual were subjugated to the will of God (Kantartzis & Molineux, 2011). In this context, it is perhaps not surprising that occupational therapists have struggled to include sexuality in professional discourse and practice (Sakellariou & Simo Algado, 2006b). Although sexuality fits within a broad classification of occupation as offered by the World Federation of Occupational Therapists (2010), the explicit link between sexuality and desire, as opposed to duty and obligation, appears to support the delegitimization of sexuality as a valid concern when therapists are confronted with limited resources and competing demands in practice settings (Hyland & Mc Grath, 2013; McGrath & Lynch, 2014).
The delegitimization of sexuality as a valid concern is also a product of the classed construction of the profession. Occupational therapy, at least in North America, Europe, and parts of Oceania, is a White, middle-class, female profession. These epithets apply not only to the membership of the profession but to the profession itself and the values it enacts (Sakellariou & Pollard, 2008). If occupational therapy was founded on middle-class values, it is possible that middle-class values regarding sexuality resulted in the decision to treat sexuality as something private that should not be spoken about (Kennedy & Ullman, 2003).
Toward a Sexual Rights Approach in Occupational Therapy
Sakellariou and Pollard (2008) argued that if occupational therapy is to be client centered, then therapists must be willing and able to respond to needs expressed by their clients. For disabled people, these needs and desires frequently include the opportunity for sexual expression (Vansteenwegen, Jans, & Revell, 2003). We propose that occupational therapists should consider adoption of a rights-based approach to sexuality to respond to the needs and desires of disabled people.
Adopting a rights-based approach to sexuality warrants discussion of the nature of human rights. Wronka (2008) described three categories of human rights. The first category of rights, civic and political rights, includes rights such as freedom to express one’s self or to practice one’s religion. The second category of rights, economic, social, and cultural rights, includes rights to food, education, work, and health care. The third category of rights refers to solidarity rights and requires substantial international cooperation between states to prevent war, famine, and pollution and to provide disaster relief.
The extent to which these rights are enacted varies, but Lottes (2013) suggested that human rights are typically underpinned by 11 core characteristics, including (1) universality, (2) equality, (3) individual or group focus, (4) nation-state responsibility, (5) autonomy and self-determination, (6) dignity, (7) diversity and nondiscrimination, (8) interconnectivity and interdependence, (9) indivisibility, (10) entitlement, and (11) international guarantee and legal protection. Each of these underlying characteristics is described in Table 1.
Core Characteristics Underpinning Human Rights
Note. From “Sexual Rights: Meanings, Controversies, and Sexual Health Promotion,” by I. L. Lottes, 2013, Journal of Sex Research, 50, p. 369. Copyright © 2013 by Taylor & Francis. Adapted with permission.
For disabled people, human rights–based approaches may offer a useful way to promote equal access to sexuality. Adopting a rights-based approach to sexuality implies that disabled people have the same rights to sexuality as able-bodied people, that these rights should be protected by governments, and that sexual rights should not be seen as less important than other human rights. Moreover, constructing sexuality as a human right suggests that disabled people have the right to choose how they express their sexuality.
Human rights are closely linked to understandings of citizenship. Extending the concept of rights to include sexual rights therefore implies a new form of citizenship, that of sexual or intimate citizenship (Richardson, 2000; Weeks, 2002). Weeks (2002) considered sexual citizenship to be concerned with protecting the choices for one’s private life in a more inclusive society. Richardson (2000) suggested that sexual citizenship is underpinned by nine distinct sexual rights (see Figure 1). For disabled people, implementation of these rights bridges the gap between the private and the public and emphasizes the cultural and political aspects of sexuality.
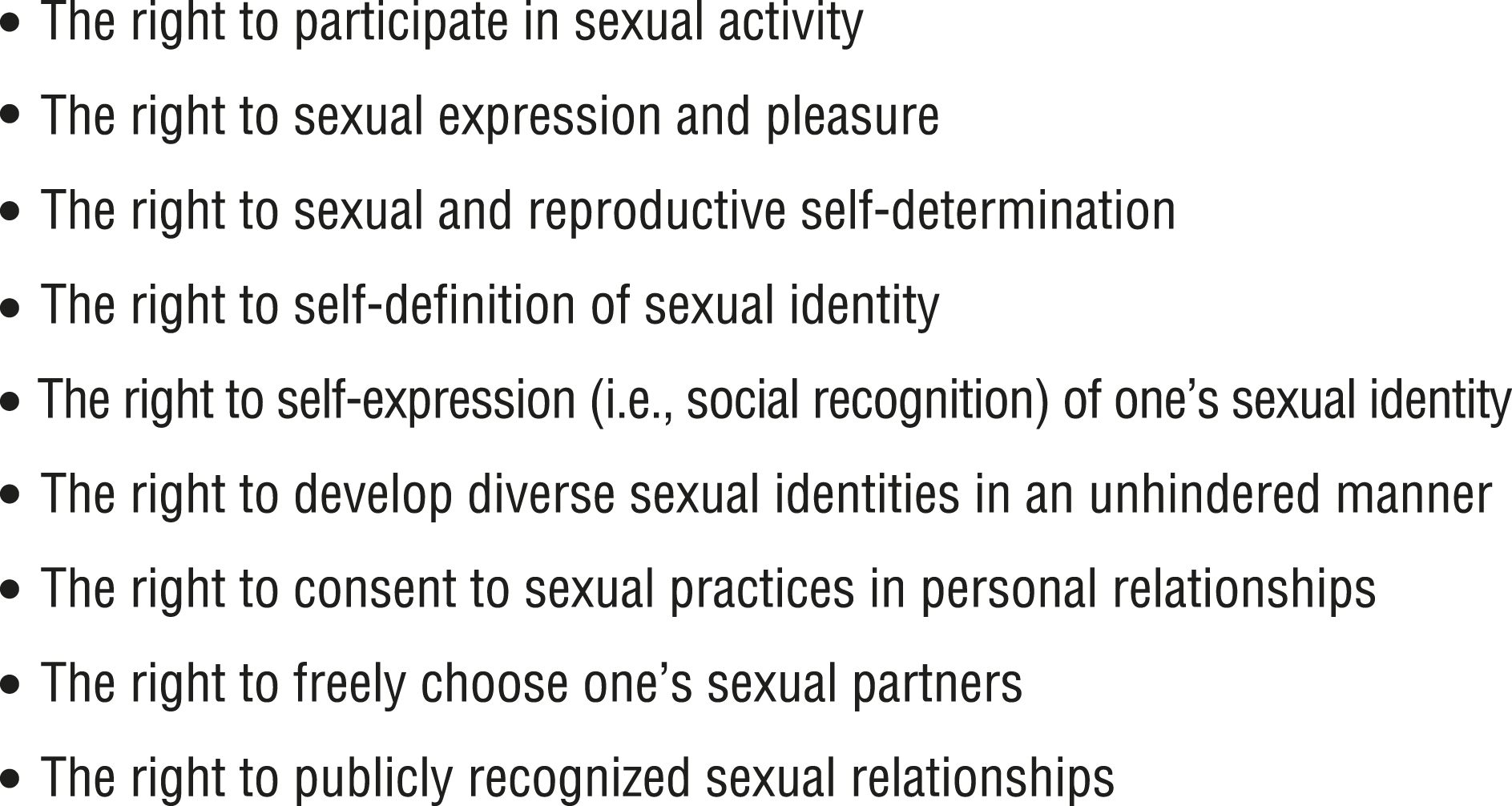
Sexual rights (Richardson, 2000).
Implications for Occupational Therapy Practice, Education, and Research
Adopting a rights-based approach to sexuality means that occupational therapists need to be supported to acknowledge the right to sexuality, respect sexual diversity, and recognize sexuality as an area of human occupation and apply their skills if an occupational interruption is present. Acknowledging the right to sexuality requires that occupational therapists include questions relating to occupational performance and sexuality as a routine part of their assessment and intervention practices. It is worth noting that disabled people are subject to the same sociopolitical discourses about sexuality that influence professional practice. Research has suggested that although many disabled people would value the opportunity to discuss concerns regarding sexuality with health care professionals, they frequently experience discomfort in raising these issues because of prevailing norms regarding sexuality and disabled people (Nosek & Simmons, 2007). To support disabled people in identifying occupational performance issues relating to sexuality, occupational therapists must begin by giving their clients permission to discuss sexuality. Although such permission is unlikely to completely overcome prevailing social norms, it can act to raise awareness of the rights of disabled people to sexuality and promote the development of services to support these rights.
Respecting diverse sexualities requires occupational therapists to refrain from adopting heteronormative attitudes toward sexuality in practice. Occupational therapists should consider their own attitudes and beliefs regarding sexuality and determine the extent to which they feel prepared to address sexuality in practice. Research has indicated that occupational therapists feel ill prepared to address sexuality (Couldrick, 1998; Hyland & Mc Grath, 2013; McGrath & Lynch, 2014; Penna & Sheehy, 2000) and that there is a need to consider how therapists’ confidence in addressing sexuality might be developed. The majority of reported training (e.g., Higgins et al., 2012) has relied on the use of the PLISSIT model developed by Annon (1976), which describes four levels of involvement by health care professionals in addressing sexual well-being: permission (P), limited information (LI), specific suggestions (SS), and intensive therapy (IT). For educators, application of this model implies developing training that addresses personal values and beliefs regarding sexuality, providing knowledge of the scope of practice of occupational therapy in relation to sexual rehabilitation, and increasing awareness of interventions that can support sexual expression. Emphasis must be placed on ensuring that therapists are prepared to implement occupation-focused, client-centered practice that incorporates the wishes of disabled people.
Understanding the occupational nature of sexuality requires occupational therapists to explore how sexualities are constructed through occupational performance. Research is needed regarding how sexuality is expressed through occupation across the life course, among different populations, and in different sociocultural contexts. This information will support occupational therapists to articulate the place of sexuality within occupational therapy and to develop appropriate assessment and intervention strategies.
Interventions should be based on the principle that disabled people have the same rights to sexuality as able-bodied people. Practice must be informed by the wishes of the individual and should address occupational aspects of sexuality. One of the key consequences of this approach is to highlight the need to approach both research and intervention in relation to sexuality as extensions of broader struggles for human rights and social justice. For occupational therapists, this means that sexuality should be given the same priority as other areas of occupational performance, and consequently therapists must advocate for recognition of the sexual rights of their clients by policymakers and service providers alike.
Conclusion
Sexuality occupies an uneasy position within occupational therapy. Although occupational therapists recognize the legitimacy of sexuality and sexual expression for disabled people, they continue to exclude sexuality from practice. This article has sought to challenge the profession of occupational therapy to consider how professional values and assumptions about the nature of human occupation, combined with a strong social discourse of normative sexuality, act to exclude disabled people from experiencing full sexual citizenship. We suggest that a rights-based approach toward sexuality is a useful framework to support occupational therapists in addressing sexuality in their practice and acknowledging the sexual dimension in the lives of service users.
Footnotes
1
Our use of the term disabled people is informed by critical disability studies, and we use it with the explicit intent to draw attention to the fact that disability is not a personal characteristic of the individual but the outcome of a process through which a person becomes disabled.
2
Although sexual activity is classified as a self-care occupation in the ![]() Occupational Therapy Practice Framework: Domain and Process (3rd ed.), such a classification reduces sexuality to the physical act of sexual intercourse and does not allow for the many other occupations through which sexuality can be expressed.
Occupational Therapy Practice Framework: Domain and Process (3rd ed.), such a classification reduces sexuality to the physical act of sexual intercourse and does not allow for the many other occupations through which sexuality can be expressed.