
Abstract
In this study, we examine the feasibility and acceptability of a 6-wk, interdisciplinary, occupation-based theater project for facilitating community engagement and substance use disorder (SUD) recovery in veterans. All data were collected at baseline, postintervention, and 6-wk and 6-mo follow-up intervals. Of the invited veterans, 24% consented to participate (n = 14), and 50% were retained (n = 7). Average attendance was 91%. Considerable improvements in social and occupational participation were noted at postintervention and at 6-wk follow-up but were not retained at 6 mo. No important change in self-efficacy was noted. Of the participants, 86% remained abstinent for 6 wk following the intervention. Theater provides a feasible and acceptable resource for potentially facilitating SUD recovery. Larger controlled effectiveness studies of theater are needed to examine whether robust and notable recovery outcomes in people with SUDs can be linked to participation in theater.
Keywords
Community engagement has been shown to be an integral component of sustained (as opposed to intermittent) recovery from substance use disorders (SUDs; Alverson, Alverson, & Drake, 2000; Chiu, Ho, Lo, & Yiu, 2010). For example, Alverson et al. (2000) demonstrated that regular engagement in enjoyable activities within the community, along with positive and accepting relationships, strongly correlated with effective long-term abstinence efforts in people with SUDs. Community engagement can offer opportunities to build a positive quality of life, providing new ways to spend time as one begins to abstain from drug use. Moreover, some literature has convincingly suggested that participating in community-engaging occupations can ameliorate the biopsychosocial consequences of SUDs (such as neurological, cognitive–behavioral, and motivational changes) that impede community engagement and thwart long-term recovery efforts (Alexander, 2008; Bickel, Yi, Landes, Hill, & Baxter, 2011; Boisvert, Martin, Grosek, & Clarie, 2008; Volkow, Wang, Tomasi, & Baler, 2013; Wasmuth et al., 2015).
Although it is well known that community engagement can facilitate SUD recovery on many levels (Salyers & Tsemberis, 2007), the literature has suggested that as many as 80% of people recovering from SUDs relapse within the first year (Bart, 2012); moreover, studies of veterans in recovery have illustrated an 85% relapse rate after only 1 mo (Vest et al., 2014). Recent studies have suggested that frequently co-occurring severe mental illnesses (SMIs) often contributed to SUD relapse rates, indicating a need for integrated services that can simultaneously address difficulties faced by clients with a dual diagnosis of SUD and SMI (Perron, Bunger, Bender, Vaughn, & Howard, 2010). Occurrence of dual diagnosis is greater among veterans than the general population (Seal et al., 2011), and dual diagnosis is associated with several health-related harms that can negatively affect quality of life and substance use outcomes (Ralevski, Gianoli, McCarthy, & Petrakis, 2014). Thus, it is arguable that researchers aiming to effectively address SUDs with interventions must consider both the frequency with which SMI co-occurs with SUD and the impact that SUD–SMI comorbidity can have on SUD outcomes.
Integrated dual-disorder treatment (IDDT), an evidence-based comprehensive approach that combines services, has been shown to improve recovery-related outcomes for people with a dual diagnosis (Tsai, Salyers, Rollins, McKasson, & Litmer, 2009). For instance, Tsai et al. (2009) demonstrated reductions in homelessness, incarceration, and hospitalization as well as greater employment and longer retention in SUD treatment. However, despite the addition of IDDT for clients with a dual diagnosis, overall SUD prevalence remains high, and relapse rates continue to be troublesome. These data illustrate the critical need for continued efforts to better facilitate long-term recovery from SUDs while considering potential factors contributing to outcomes, such as the presence of dual diagnosis. Enabling community engagement through the intervention proposed in this study is one promising means for addressing this need.
Occupational therapists are specifically trained to address barriers to social participation and to facilitate engagement in occupations within the community. As described in the Occupational Therapy Practice Framework: Domain and Process (3rd ed.; American Occupational Therapy Association [AOTA], 2014), occupational therapists are prepared to address client factors inhibiting social participation, such as the presence of psychological or mental disorders, while working to build healthier and more inclusive communities that facilitate participation (Kronenberg, Algado, Pollard, Werner, & Sinclair, 2005). Prior research has indicated that a theater-based intervention—a form of occupational therapy that was used relatively often as a mental health intervention during occupational therapy’s founding years but has become increasingly uncommon in the modern medical climate—may be particularly powerful, not only for facilitating community engagement but also for specifically addressing the biopsychosocial changes observed in people with SUDs (Jones, 2007; Noice & Noice, 2008; Rutten et al., 2010; Ryan, 1976). For instance, literature on addiction has suggested that the activities involved with engagement in a theater intervention can (1) affect the neuropathological changes in the reward center and executive systems that result from drug use (Bechara, 2005; Bickel et al., 2011), (2) improve psychological and cognitive flexibility as well as function (Noice & Noice, 2008, 2013), and (3) improve social cognition while providing opportunities for positive social recognition (Rutten et al., 2010). Building on this literature, in this study, we examined whether an occupation-based application of theater in the community (as opposed to theater-related activities within the context of a clinical therapy session) had beneficial outcomes that supported the ability to maintain abstinence from addictions.
A long-term aim of this work is to investigate the potential effectiveness of theater as a community-engaging form of occupational therapy that can be administered alongside other services for veterans with SUDs (such as SUD interventions and IDDT services). However, a necessary preliminary step to a large-scale effectiveness study is the examination of both the feasibility (do veterans volunteer and participate?) and the acceptability (can a meaningful range and depth of data be obtained?) of such an intervention. Thus, the purpose of this study is to (1) test the feasibility of a theater-based intervention for enhancing community engagement and recovery-related outcomes, as indicated by the successful recruitment of and completion by veterans recovering from SUDs, and (2) assess the acceptability of the intervention, as indicated by documentation of attendance and participation rates as well as data collection and analyses documenting areas of potential improvement, including social and occupational participation, self-efficacy, and substance use.
Background
According to criteria of the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; American Psychiatric Association [APA], 2013), SUDs are defined in terms of the degree to which compulsive use of the substance in question causes significant functional impairments, such as interfering with participation in other meaningful occupations or instigating health problems (Alexander, 2008). Occupations are activities that people do to structure time and to create meaning and an identity (AOTA, 2014). In Kielhofner’s (2008) Model of Human Occupation (MOHO), engaging in occupations was described as a means of structuring time through developing roles and routines, shaping identities, and helping people establish values. Occupations create an interpersonal context and allow for mastery experiences and opportunities for social participation (Kielhofner, 2008). In short, MOHO has illustrated that participation in occupations contributes to a positive identity within changing environments. According to MOHO, ongoing well-being depends on occupational adaptation as personal and environmental factors shift throughout a lifetime.
From this perspective, if drug use and related activities dominate the lives of people with SUDs and thereby interfere with other meaningful occupations, notable consequences will be observed in many areas. Such a shift in one’s occupational life will likely affect one’s personal identity, relationships, roles, routines, habits, volition, and performance capacities in complex and interrelated ways. In fact, the literature has demonstrated that identity confusion, social isolation, lack of temporal structure, and deficits in metacognitive mastery (the ability to use self-reflection and an understanding of others’ thoughts in everyday challenges; Semerari et al., 2003) are prevalent among people with SUDs (Alexander, 2008; APA, 2013; Greene et al., 1999; Kielhofner, 2008; Lysaker et al., 2014; Wasmuth et al., 2015).
As suggested earlier, the consequences of SUDs can affect people on many levels. Illustrating some of the biopsychosocial consequences of SUDs, studies have suggested that, at the neurological level, strengthened connections in reward center processing and weakened inhibitory pathways from executive systems are linked to the compulsive drug use that characterizes SUDs and that interferes with participation in other occupations, thus impeding community engagement (Bechara, 2005). These neurological changes also affect people on a psychological level. For instance, some changes impede motivation for activities other than drug use and therefore limit the degree to which people feel engaged and interested within contexts other than those surrounding their addiction (Volkow, Fowler, Wang, Baler, & Telang, 2009). Additionally, the contribution of SUDs to increased and ongoing social isolation as well as to problems with interpersonal communication and metacognitive mastery in turn affects community engagement (Link, Struening, Rahav, Phelan, & Nuttbrock, 1997; Wasmuth et al., 2015).
Several specific characteristics of theater make it a promising intervention for addressing the biopsychosocial consequences of SUDs. First, seen through the lens of MOHO, participating in theater provides an occupation and thus a means for structuring time; creating new roles, routines, and habits; and developing new performance capacities as people begin to abstain from their addictions. Considering that SUDs tend to dominate the occupational lives of people, attempts at abstinence call for new occupations to provide meaning, structure, and new identities. Moreover, participation in theater may bring enjoyment and thus affect volition.
More specifically, reading the roles of different characters, enacting and discussing scenes, and being able to respond to various social situations—including those involving conflict—can provide broader understandings of social dynamics and also make it possible to respond to conflict from the safety of doing so in a role other than one’s self. Thus, participation in theater is likely to facilitate improvements in metacognitive mastery.
Additionally, in a theater intervention, emphasis is placed on performing in front of others at the conclusion of the intervention. This emphasis arguably provides a strong motivational impetus for knowing one’s lines and focusing one’s attention on the future so as to not be embarrassed in front of a crowd. This practice of forward thinking and valuing the outcome of future events contrasts with the process of temporal discounting—the tendency to focus primarily on small immediate rewards over long-term larger rewards (Bickel, Jarmolowicz, Mueller, Koffarnus, & Gatchalian, 2012)—which has been found to span all types of addiction. The emphasis on forward thinking thus may make theater intervention beneficial to people in recovery.
Further supporting this line of thought, it has been argued that executive system exercises, such as memorization, can help strengthen inhibitory pathways to weaken the highly reinforced reward pathways that contribute to addictive behavior in people with SUDs (Bickel et al., 2011, 2012). The task demands that a theater intervention places on executive functioning—such as memorizing lines and responding in the moment to varying conditions during rehearsals and performances—may thus be beneficial in reshaping neuropathological phenomena that contribute to SUDs and their harms.
Finally, a theater intervention may be particularly beneficial because it incorporates performing for the surrounding community members and receiving positive regard. Several studies have shown that family- and community-oriented approaches to treatment facilitate promising outcomes for people with addictions (Rigter et al., 2013; Slesnick, Erdem, Bartle-Haring, & Brigham, 2013). As Thoits (2013) emphasized, “Almost all approaches in psychiatry and clinical psychology . . . view individuals’ mental health as at least partly influenced by positive self-conceptions, high self-esteem, and/or the possession of valued social identities” (p. 357). This is particularly important in light of the negative stigma, social isolation, and identity confusion that have been associated with SUDs (Alexander, 2008).
Although the use of theater for veterans with SUDs will undoubtedly pose its own unique challenges, successful use of theater in other vulnerable populations is encouraging. Historically, theater has been used internationally in the occupational therapy departments of prominent hospitals, with positive outcomes noted in social and occupational participation and reduced symptoms of SMI (Jones, 2007). One study provided preliminary data illustrating theater interventions as contributing to prosocial behavior and decreasing antisocial behavior in male adolescent youths (Rutten et al., 2010), and another study demonstrated that theater-based interventions improved social deficits in people with autism spectrum disorder (Corbett et al., 2014). A study by Noice and Noice (2008) showed that a 4-wk, theater-based intervention increased cognitive and social function in a sample of community-dwelling adults with cognitive decline as well as, on a separate occasion, less educated, low-income older adults living in subsidized retirement homes (Noice & Noice, 2013). Drama therapy in a clinical context (rather than a full-fledged theater intervention) has been implemented in Veterans Affairs (VA) hospitals to address posttraumatic stress disorder, and promising preliminary outcomes have been reported (James & Johnson, 1996); moreover, evidence has historically supported theater for prisoners as considerably reducing the rate of rearrest more than any other motivational program in correctional systems across the United States (Ryan, 1976). These findings encourage further investigation of theater as an intervention to bolster SUD recovery outcomes in veterans.
Method
Design
This study entailed concurrent quantitative and qualitative data collection with an explanatory sequential mixed-methods design (Creswell & Tashakkori, 2007). Although only quantitative, feasibility, and acceptability outcomes are reported in this initial article, they are in no way conceptually distinct or separate from qualitative data, analysis, or theoretical framework. Qualitative and quantitative data were integrated in several ways, as suggested by mixed-methods experts (Fetters, Curry, & Creswell, 2013). Qualitative themes (e.g., obtained via thematic analysis of focus group transcripts) allowed for expansion of quantitative findings (Aarons, Fettes, Sommerfeld, & Palinkas, 2012), whereas quantitative data illustrated that a change occurred, and qualitative data illuminated how and why these changes occurred, providing insight into the mechanisms of change underlying quantitative outcomes.
The sequential study design and the length of this article contributed to our decision to lead with this report of quantitative and feasibility findings. We consulted with mixed-methodology experts before reaching consensus that this initial report would not compromise the overall integrated design as described. Qualitative findings illustrating mechanisms of change are reported elsewhere (Wasmuth, Rollins, & Pritchard, 2015).
Sample
We anticipated a relatively high attrition rate because of the intensive nature of the intervention and the nature of the disorder being studied (Stark, 1992). We determined that, ideally, 10 participants would allow an appropriate cast size for the intended theater intervention and production. Anticipating a 30% attrition rate, we aimed to recruit 15 veterans. We recruited from the Substance Use Disorder Recovery Program (SUDRP) at one VA medical center and from a residential rehabilitation center for veterans. Inclusion criteria were (1) a current diagnosis of an SUD and (2) initial enrollment in SUDRP intensive outpatient services or domiciliary residential services for SUD rehabilitation. We did not require veterans to remain active in these treatment programs to continue as participants in our study. Considering the notable rates of SUD–SMI comorbidity among veterans (Ralevski et al., 2014), volunteers with SMI were not excluded; doing so allowed for a reasonable degree of external validity.
Procedures
Recruitment.
Clinicians at recruitment sites informed all veterans of the opportunity to participate in this study, and those interested were provided with more information by the principal investigator (Wasmuth) before consenting to participate. Researchers obtained Health Insurance Portability and Accountability Act of 1996 (Pub. L. 104–191) authorization, written informed consent for the study, and additional consents for audiovisual recording in a private room. At this time, participants were asked to provide all schedule conflicts, from which rehearsal and performance schedules were created. Schedules were given to all participants during baseline assessments.
Data Collection.
The principal investigator reviewed medical records for inclusion criteria and demographic data. Drug use data obtained via urine drug screens performed by the two treatment centers and documented in medical records were recorded for the 6-wk period leading up to the intervention as well as throughout the intervention and for 6 wk following the intervention. Baseline data collection was administered within 1 wk of the start of the intervention and was repeated within 1 wk after the end of the intervention and at both 6-wk and 6-mo follow-up points. Interviews were audio recorded and securely stored behind VA firewalls, and assessments were stored in a locked cabinet on a locked floor at a VA medical center. Participants received $10 gift cards for each interview and assessment session completed.
Measures.
Demographic data—including drug test results, Axis I and II diagnoses, treatment notes, and all substance- and addiction-related information—were obtained from electronic medical health records. Sample recruitment tracking was used as a measure of feasibility. We tracked the number of veterans who received study information, who expressed interest, and who consented to take part in the project.
Attendance rates at rehearsals, final production, and baseline and follow-up assessments were tracked as a measure of acceptability. To assess the range and depth of data available as an additional measure of acceptability, we measured and analyzed social and occupational participation and perceived self-efficacy.
To measure social and occupational participation, we used the Occupational Circumstances Assessment Interview and Rating Scale (OCAIRS; Forsyth et al., 2005)—a brief, audio-recorded interview that provides structure for gathering and analyzing the extent and nature of a person’s occupational participation. It has a 1–4 rating scale to assess roles, habits, personal causation, values, interests, skills, short- and long-term goals, interpretation of past experiences, physical environment, social environment, and readiness for change, and we used it as a pre–post effectiveness measure. The OCAIRS has been shown to have adequate concurrent validity (Brollier, Hawkins Watts, Bauer, & Schmidt, 1989) and excellent interrater reliability (Kielhofner, 2008).
To measure perceived self-efficacy, we used the General Self-Efficacy Scale (GSE; Schwarzer, Babler, Kwiatex, Schroeder, & Zhang, 1997). The GSE has been suggested as a means for assessing, in addition to self-efficacy, changes in quality of life at pre- and postinterventions. It consists of 10 items assessed with a 1–4 rating scale. The Perceived Self-Efficacy construct reflects a belief that one can perform difficult tasks and cope with adversity in various domains of human functioning, such as goal setting, effort, and persistence in adversity. Reliability has been demonstrated in samples from 23 nations, with Cronbach’s αs ranging from .76 to .90 on a unidimensional scale; moreover, the GSE has shown convergent and discriminant validity, correlating positively with self-esteem and optimism and correlating negatively with anxiety, depression, and physical symptoms (Schwarzer et al., 1997).
The pretest–posttest OCAIRS and GSE were administered and scored by a research assistant who was not involved in the intervention. The research assistant did not have access to participant information or contact with participants outside interview and assessment sessions.
Intervention.
The intervention consisted of 6 wk of 3-hr rehearsals, 3 times per week. Rehearsals were held in rooms at the VA medical center. The script used for this intervention was written by a local playwright who served as the director for the intervention production. The play was a modern-day adaptation of seven Greek myths that discreetly touch on themes of addiction, thus allowing for discussion of these themes in a way that everyone could relate to, regardless of SUD status, and therefore enabling all personnel (not just study participants) to actively participate in discussions. Because the script was written by a collaborator on this project, it could easily be adapted to the number of recruited participants and dropouts.
Personnel included an occupational therapist, a professional director and playwright, a professional actor, an occupational therapy student, and an art therapist. The actor performed the roles in the play that the director was unable to assign to veterans because of recruitment limitations, dropouts, aptitude, or other barriers. The actor also led actor-based warm-up and wrap-up sessions at each rehearsal and served as a peer mentor for participants.
Generally speaking, rehearsals consisted of increasingly demanding exercises designed to have participants experience the essence of acting, as described by Noice and Noice (2008), “to become engrossed in communicating the meaning of the dialogue so that obvious situation-specific cognitive, affective, or physiological alterations occur in demeanor” (p. 60). The director and occupational therapist led discussions of the script during table work—a process that allows participants to examine the content of the play, dynamics of scenes, and traits of characters. In the discussions, the participants examined in detail the relationships among characters in different scenes and how these related to participants’ own lives and experiences. The occupational therapist guided discussions toward the significance of engaging in occupations and the importance of examining differences in various kinds of occupational engagement.
Specifically, participants were encouraged to talk about the ways in which the occupations of the Greek mythology characters brought on problems for these characters and why. Participants explored differences between themselves and their assigned characters. This process naturally led to conversations about how once-enjoyable occupations had become problematic addictions in participants’ lives. In addition, table work led to many discussions that revealed how members of the group perceived the same scenes differently and brought different personal experiences to the play as they developed their characters, scenes, and, eventually, the full production.
The director prepared veterans for the final production through scene rehearsal as well as blocking and staging directions. The art therapist was available to help veterans process any emotional struggles that arose during the rehearsal process and met with veterans one on one during rehearsals. The occupational therapy student facilitated participation by addressing the veterans’ needs, such as assisting with cognitive strategies for line memorization during rehearsals.
The first rehearsal established a safe space through the use of warm-up exercises in which participants were encouraged to share while keeping their comments focused on themselves. All rehearsals began with warm-up sessions, and the last 20–30 min of every rehearsal was reserved for a wrap-up session to allow participants enough time to describe and process any problems or feelings that may have emerged during the day’s rehearsal. During the first rehearsal and throughout the intervention period, it was continually emphasized that all participants and personnel were there to share in the experience; personnel were encouraged to share their own struggles and life journeys throughout the process, facilitating the removal of barriers to open communication and eliminating the dynamic of power from the room. All members in the room were acknowledged as equals, interested in participating in the process for their own well-being. It was emphasized early on that therapists, directors, and professional actors should not be seen as having the right view or answer during discussions.
After 6 wk of rehearsals, the veterans performed the play on 2 consecutive nights; the play was advertised as free and open to the public. The community response was overwhelming, leading to two sold-out performances. Each performance was followed by a talk-back session between audience members and veterans that involved a question-and-answer–style discussion of veterans’ experiences of the intervention. The production was filmed by a local public media station, which also interviewed veterans about their experiences (WFYIOnline, 2014).
Analyses.
We tracked veteran participation at various stages from recruitment to follow-up assessments, examining potential factors contributing to feasibility and acceptability. We compared drug use data, pre–post scores of self-efficacy, and social and occupational participation to assess potential areas of improvement to be examined in future trials.
Results
Recruitment Tracking
Data indicated that 14 of 58 veterans (24%) who were made aware of the study via a recruitment announcement at the VA SUDRP and Domiciliary Rehabilitation Program consented to participate. Four participants (29%) dropped out before baseline assessment, and 3 (21%) dropped out in the 1st wk of the intervention, yielding a dropout rate of 50% (this rate was not specific to the study; these participants also dropped out of the treatment program, and consultation with treatment facilities suggests that these rates are typical of the study population). All participants after Week 1 were retained. Thus, 7 veterans (12%) initially introduced to the study completed the intervention process. The demographics, attendance rates of participants during the intervention, and drug use data are depicted in Table 1.
Demographic Data, Attendance, and Drug Use for Active Participants (N = 7)
Note. NOS = not otherwise specified; PTSD = posttraumatic stress disorder.
Attendance
The mean attendance rate was 91% for the 7 active participants. Of the 7 active participants, 3 participants missed one rehearsal, 3 participants missed two or more rehearsals, and 1 participant did not miss any rehearsals.
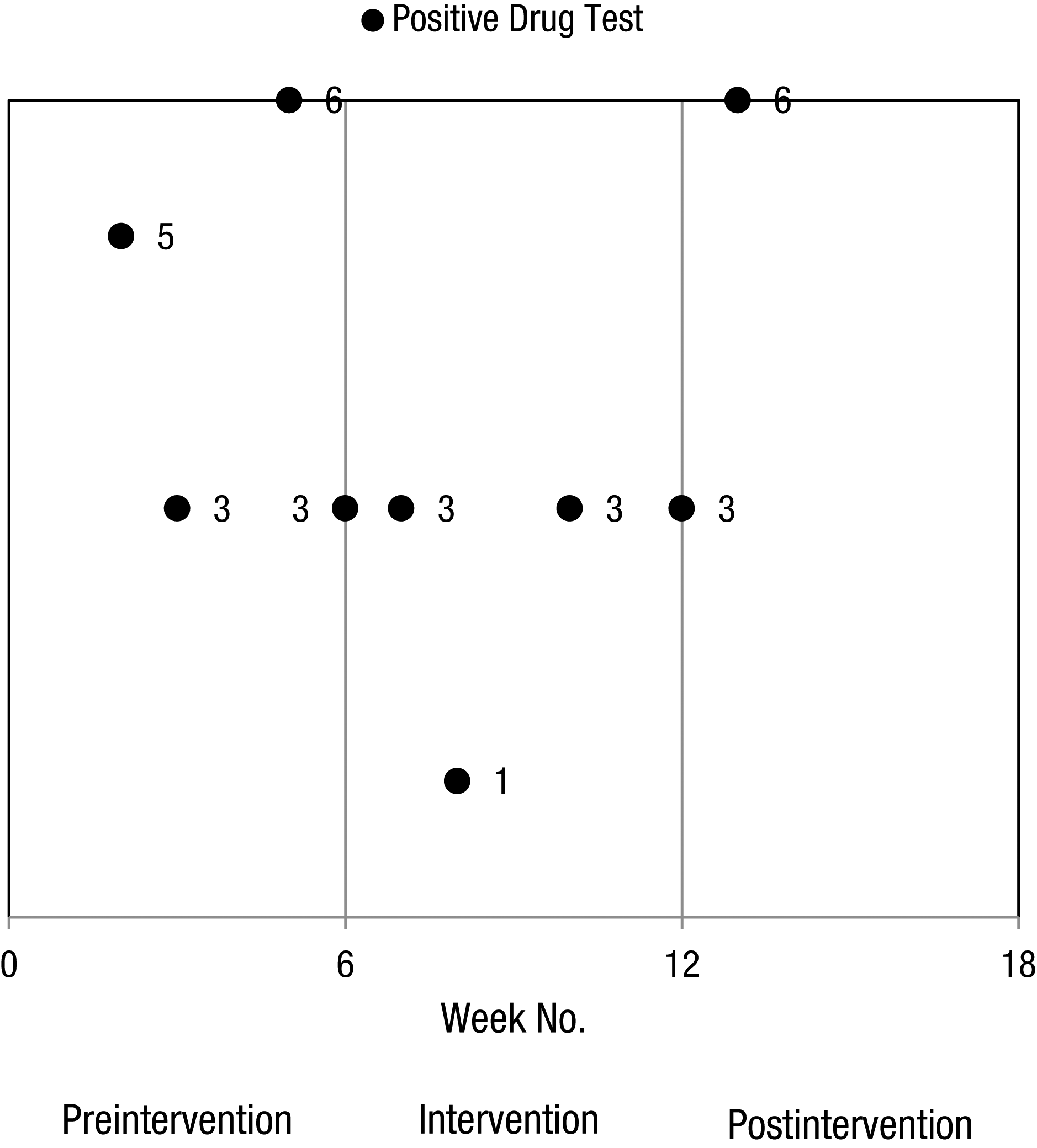
Drug Use
Random drug tests were taken weekly at each recruitment facility. Results of these tests were recorded for the 6 wk before intervention, during the 6-wk intervention, and for 6 wk after the intervention. Drug test data are documented in Table 1. Before the intervention, 4 of 7 participants regularly tested positive for drug use (2 participants for cocaine and 2 participants for benzodiazepines), whereas during the postintervention period, only 1 participant had a positive drug test result. Thus, we observed a 43% abstinence rate before the intervention compared with an 86% abstinence rate for the postintervention observation period. Two participants (29%) had positive drug test results during the intervention. More specific details regarding drug test data can be observed in Table 1 and Figure 1.
Pre–Post Outcomes
At baseline, veterans who remained active participants in the theater intervention were not significantly different than veterans who dropped out in regard to mean baseline OCAIRS raw scores (mean [M] = 34, standard deviation [SD] = 5.77 vs. M = 36, SD = 4.43) and GSE scores (M = 32, SD = 7.46 vs. M = 33, SD = 2.54). Regarding OCAIRS raw scores, a paired-samples t test exhibited no significant difference at the .05 level: t (6) = −0.60, p = .569 (two-tailed); 95% confidence interval [−5.78, 3.49]; d = −0.22. Regarding GSE scores, a paired-samples t test showed no significant difference at the .05 level: t (6) = −0.34, p = .749 (two-tailed); 95% confidence interval [−7.12, 5.40]; d = −0.15. Because no significant differences were seen at baseline between active participants and dropouts, our findings have greater external validity.
We then examined whether significant differences existed in active participants from baseline to 6 mo following the intervention. A one-way analysis of variance of OCAIRS raw scores for active participants at baseline (M = 34, SD = 5.77), postintervention (M = 44, SD = 2.07), 6-wk follow-up (M = 43, SD = 3.31), and 6-mo follow-up (M = 41, SD = 5.80) revealed a significant difference, F(3, 20) = 6.51, p < .01, with a large effect size (η = .89; Cohen, 1988). Post hoc power analysis indicated power of >80% with 7 active participants. Levene’s test supported the assumption of homogeneity of variance (F = 0.88, p = .471). To determine points at which significant differences in OCAIRS raw scores occurred, we performed a post hoc analysis using Bonferroni correction. Post hoc testing indicated a significant difference between baseline OCAIRS raw scores and scores obtained postintervention (p < .01) and at the 6-wk follow-up (p < .01). No significant differences were found between baseline raw scores and scores obtained at the 6-mo follow-up (p = .198).
Active participants had the following GSE scores: baseline (M = 32, SD = 7.46), postintervention (M = 32, SD = 2.43), 6-wk follow-up (M = 34, SD = 3.60), and 6-mo follow-up (M = 32, SD = 2.63). A one-way analysis of variance revealed no significant difference in GSE scores, F(3, 20) = 0.25, p = .864, with a small effect size (η = .19; Cohen, 1988). Levene’s test supported the assumption of homogeneity of variance (F = 3.05, p = .052).
Discussion
In this preliminary study, we examined the feasibility and acceptability of a community-engaging occupational therapy theater intervention. The recruitment of 24% (n = 14) of veterans informed of this study (n = 58) with a retention rate of 50% (n = 7) suggests that recruitment and retention for this type of intervention is challenging but, given the positive results, worthwhile. We can infer that this intervention is feasible for at least a subpopulation of veterans with SUDs, although specific identifiers of that subpopulation would require further analysis. It is notable that veterans who remained active participants attended >90% of rehearsals throughout a fairly rigorous rehearsal process consisting of 3-hr rehearsals, 3 times per week for 6 wk. The community response to this study also supports its feasibility. Both performances were at full capacity; moreover, the production drew local media stations, and the feedback and discussions during talk-backs were overwhelmingly positive.
Our finding that participation in a theater intervention resulted in considerable improvements in social and occupational participation for up to 6 wk following the intervention suggests that this community-engaging form of occupational therapy may be beneficial for people recovering from SUDs who are in need of new social and occupational opportunities. Although an improvement in the mean OCAIRS score was observed between the postintervention data and the 6-mo follow-up, the difference was not statistically significant. It is possible that our small sample contributed to a lack of power and thus likelihood of a Type 2 error and that with larger samples, 6-mo outcomes may reach significance. Nonetheless, it will be important to continue to explore ways in which the intervention can maximize long-term outcomes. For instance, one possibility may be to include participants in future productions as peer mentors, assistant directors, or stage managers.
No notable change was found in mean GSE scores. One explanation for this is that the theater intervention did not influence self-efficacy. Another explanation is that the intervention did influence self-efficacy but that changes were not captured by the GSE. Schwarzer and Fuchs (1995) wrote about the importance of cultivating self-efficacy in addiction recovery and highlighted five categories of self-efficacy pertaining to addictive behaviors (Marlatt, Baer, & Quigley, 1994). Specific measures of each of the five categories may better capture improvements in addiction-related self-efficacy in future studies of a theater intervention.
Drug test data demonstrate that overall drug use among active participants declined. Although our sample is too small to speak of the effectiveness of a theater intervention in reducing drug use, our data suggest that the intervention may help with abstinence efforts in early SUD recovery. It is worth noting that some participants (n = 2) relapsed during the intervention period yet persevered. For 1 participant, the positive drug test result was an isolated event; for the other, it occurred repeatedly. Neither of these participants dropped out of the study; however, the participant with recurring relapses had multiple missed rehearsals (3.5) and was unable to memorize his lines. To compensate for this deficiency, we shortened his role to a single monologue, and we provided him with cue cards during performances to deliver it. It is also worth noting that although this participant had positive drug test results before and during the intervention phase, he did not have any positive drug test results during the 6-wk follow-up period. Positive drug tests for this participant were for cocaine. Because cocaine and its metabolites are rapidly excreted from the body (Mieczkowski & Newel, 1997), drug test results for this participant should not be attributed to false positive results from drugs staying in his system. Rather, it is likely that this participant was using before and through the intervention period but was abstinent following the final performance and that this abstinence was maintained for the 6-wk follow-up phase.
One limitation of this study is that a large number of veterans dropped out before or in the 1st wk of the intervention. High dropout rates limit the scope of this type of intervention in reaching large numbers of veterans in SUD recovery. Comparison of baseline OCAIRS and GSE scores between dropouts and active participants revealed no significant differences, but there may have been other factors that contributed to whether participants remained in the study. Previous substance abuse treatment research has indicated that a variety of factors decrease attrition: social support, convenience of clinic location, proportionate therapist-to-client ratio, and the clinicians’ therapeutic use of self (Stark, 1992). Although the high rate of attrition observed in this study mirrored the attrition within the treatment programs from which we recruited, future research in which some of these potential factors contributing to dropout rates are explored could provide important information for the possibility of increasing retention.
Although the absence of a control group and small sample size limit the validity of effectiveness outcomes and effect sizes reported here, our documentation and analysis of potential areas of improvement provide important information for future studies regarding potential mechanisms of change related to participation in occupation-based theater interventions. The effects on social and occupational participation obtained via analyses of the OCAIRS indicate that theater interventions are an important area for further exploration in larger, controlled trials.
The fact that 6 of 7 active participants had dual diagnoses may indicate that our findings represent the feasibility and acceptability of theater within a dual-diagnosis population rather than within an SUD population. However, because of the high rate of comorbidity of SUD and SMI (Perron et al., 2010), we felt that excluding participants with a dual diagnosis would unnaturally limit our sample and would fail to accurately represent a population with an SUD. Examining differences in outcomes between clients with a dual diagnosis and clients with an SUD in future trials will be an important area of investigation to determine potential differences.
An occupation-based theater intervention is intended to complement rather than replace other services. Particularly in the context of clients with a dual diagnosis, the theater intervention may be seen as complementing delivery of IDDT. A challenge in studying effectiveness of a theater intervention is its complexity. Especially in a population with a dual diagnosis in which integrated services are the evidence-based approach, it becomes difficult to determine the specific factors contributing to outcomes. It will be important in future studies to first limit inclusion criteria to either clients with a dual diagnosis or clients with only an SUD. When examining effectiveness of the theater intervention with clients with a dual diagnosis, theater plus IDDT could be compared with IDDT alone. When examining clients with an SUD, the theater intervention plus treatment as usual could be compared with treatment as usual alone.
Finally, this intervention was led by a group of professionals who brought specific personalities, expertise, and insight into this process. It remains to be seen whether and how outcomes might be affected by the inevitably different dynamics that a different group of personnel and a new group of participants would bring to this process.
Implications for Occupational Therapy Practice
Theater-based interventions provide a feasible and acceptable resource for occupational therapists wishing to facilitate community engagement and SUD recovery. Larger effectiveness studies of theater-based interventions are needed to examine whether robust and notable outcomes can be linked specifically to participation in the intervention. Further development of a protocol for this type of intervention that facilitates more long-term participation may allow for more extended outcomes to facilitate longer term recovery. The results of this study have the following implications for occupational therapy practice:
Providing theater as a new opportunity for social and occupational participation may bolster occupational therapy outcomes for SUD recovery.
Further development of a theater intervention protocol will aid occupational therapists in implementing theater for people recovering from SUDs.
Footnotes
Acknowledgments
This study was funded by the Indiana Institute for Medical Research, and it would not have been possible without Q-Artistry and the extraordinary efforts of Ben Asaykwee, Lauren Briggeman, Tessa Faraone, Angela L. Rollins, Linda Collins, Paul Lysaker, and the veterans who so eagerly participated in this project. We also thank the countless others who so enthusiastically supported this work.