
Abstract
Preterm birth has been associated with cognitive, motor, neurological, language, attention, and behavior difficulties in children (Arpi & Ferrari, 2013; de Kieviet, van Elburg, Lafeber, & Oosterlaan, 2012; Kessenich, 2003; Sansavini, Guarini, & Caselli, 2011). Few studies, however, have explored sensory processing differences in children born preterm. Sensory processing refers to how the nervous system detects, regulates, interprets, and responds to sensory information, and it is central to cognitive processes such as attention, memory, visual perception, and planned action (Ahn, Miller, Milberger, & McIntosh, 2004; Gardner & Johnson, 2013). Dunn’s (1997) theoretical model of sensory processing postulates that each person has a unique threshold for noticing and responding to sensory information. This threshold influences people’s choices and is mirrored in their mood and temperament and how they structure and participate in their lives (Dunn, 1997, 2001, 2007).
Emerging evidence has supported the idea that early sensory organization is dependent on experience (Lickliter, 2011). Infants born preterm face significant modifications in sensory experience, leaving the womb and entering the neonatal intensive care unit (NICU) environment, where they receive sensory input that can overstimulate auditory, visual, and tactile systems and understimulate the vestibular system (Lickliter, 2011). Preterm infants are also exposed to noxious stimuli and painful procedures, such as heel lances for blood collection, intubation, and suctioning. These experiences cause further stress to preterm infants and are associated with alterations in regional brain structure and function (Brummelte et al., 2012; Grunau, 2013; Zwicker et al., 2013). Given their biological vulnerability and early environmental experiences, preterm children may be at risk of developing atypical sensory processing (Lickliter, 2011). Atypical sensory processing is problematic because it has been associated with behavioral problems, immature social skills, impaired fine and gross motor skills, and difficulties performing activities of daily living (Gourley, Wind, Henninger, & Chinitz, 2013; Parham & Mailloux, 2010).
To date, only a few studies have investigated the prevalence of sensory processing differences in children born very preterm (28–32 wk gestational age). Wickremasinghe et al. (2013) found that 39% of the preterm children in their study had atypical sensory processing patterns. Atypical sensory processing of very preterm children at age 2 yr is associated with male sex, higher social risk, longer hospital stay, and white-matter injury and is related to poorer development (Eeles et al., 2013a, 2013b). Although studies have suggested associations between preterm birth and atypical sensory processing in early childhood, to our knowledge only one study (Wickremasinghe et al., 2013) has evaluated sensory processing in children born very preterm beyond age 2 yr. The full extent of sensory processing differences may not be apparent until later childhood.
The primary purpose of this study was to describe the prevalence and type of sensory processing differences in a retrospective cohort of children (age 4.5 yr) born very preterm (≤32 wk gestational age). Moreover, we aimed to determine the neonatal risk factors for atypical sensory processing patterns. We hypothesized that the majority of very preterm children would display atypical sensory processing, with sensory sensitivity being the most common pattern, and that younger gestational age at birth, early illness severity, and longer NICU stay would predict sensory processing differences.
Method
Research Design
We used a retrospective cohort study design with prospectively collected standardized instrumentation in a targeted clinical population. This study was approved by the University of British Columbia and the Children’s and Women’s Health Centre of British Columbia research ethics board. Parents or legal guardians provided written consent.
Participants
The study sample consisted of 160 children born very preterm who were seen during a follow-up visit at age 4.5 yr in the Neonatal Follow-Up Program (NFUP) at the BC Women’s Hospital (Vancouver, British Columbia) from February 2011 to December 2013. Recruitment criteria for the NFUP included birthweight ≤800 g, gestational age ≤25 completed weeks, Grade 4 intraventricular hemorrhage, cystic periventricular leukomalacia, severe retinopathy of prematurity (≥ Stage 3 or requiring laser treatment), infant home oxygen therapy, or participating in funded research studies. Children who met these criteria and had a caregiver who was able to independently complete a questionnaire were eligible to participate in this study.
Data Collection
Data regarding neonatal characteristics were obtained through detailed chart review. Neonatal variables collected included gestational age (in weeks), birthweight (in grams), 5-min Apgar score (Apgar, 1953), score on the Score for Neonatal Acute Physiology–II (SNAP–II; Richardson, Corcoran, Escobar, & Lee, 2001), abnormal cranial ultrasound, days of invasive ventilation, days on supplemental oxygen, and length of stay (in days) in the NICU until first discharge home. The Apgar and SNAP–II are both measures of neonatal physiological state. The Apgar test evaluates five criteria at 1 and 5 min after birth: heart rate, respiration, reflex irritability, muscle tone, and skin color; lower scores indicate a greater need for medical intervention. The SNAP–II measures illness severity on the 1st day of life by quantifying six physiological variables, with higher scores reflecting more disturbances in neonatal physiology.
Instrumentation
The primary measure for this study was the Short Sensory Profile (SSP; Dunn, 1999), a 38-item validated caregiver-completed screening questionnaire designed for children ages 3–10 yr that assesses a child’s responses to normally occurring sensory stimuli in seven domains: Tactile Sensitivity, Taste/Smell Sensitivity, Movement Sensitivity, Underresponsive/Seeks Sensation, Auditory Filtering, Low Energy/Weak, and Visual/Auditory Sensitivity. The parent reports how frequently the child responds to sensory events using a 5-point Likert-type scale ranging from 5 (never) to 1 (always).
Internal consistency of the sections ranges from .70 to .90 (Dunn, 1999). The SSP has been standardized into three categories with cutoff scores as follows: typical, within 1 standard deviation of the mean and higher; probable difference, between 1 and 2 standard deviations below the mean; and definite difference, more than 2 standard deviations below the mean. Initial studies have demonstrated that the SSP has a discriminant validity of >95% in identifying children with and without sensory processing differences (McIntosh, Miller, Shyu, & Dunn, 1999; Tomchek & Dunn, 2007).
Data Analysis
Statistical analyses were performed with IBM SPSS Statistics (Version 22; IBM Corporation, Armonk, NY). Descriptive statistics were used to describe the sample characteristics and the prevalence and type of sensory processing patterns on the SSP. For the purpose of analysis, we combined “probable” and “definite” difference scores (1 and 2 standard deviations below the mean, respectively) into one variable, atypical. Subsequently, we determined differences between typical and atypical sensory processing groups using Fisher’s exact test for categorical variables and the Mann–Whitney U test for continuous variables. Variables that differed significantly between groups were considered for entry into the regression model. Spearman rank-order correlations were conducted to determine which neonatal variables were highly correlated to avoid multicollinearity (r > .70). Logistic regression was then conducted to compare the independent predictive value of neonatal variables with atypical sensory processing patterns.
Results
Cohort Characteristics
Our sample consisted of 160 children (51% of whom were male) born at a median age of 26 wk gestation (interquartile range [IQR] = 25–28) with a median birthweight of 823 g (IQR = 700–1,094) and a median length of stay in the NICU of 65 days (IQR = 25–100). Additional characteristics of the cohort are provided in Table 1.
Cohort Characteristics (N = 160)
Note. IQR = interquartile range; NICU = neonatal intensive care unit; SNAP–II = Score for Neonatal Acute Physiology–II.
Sensory Processing Patterns
The percentage of participants scoring in each range on the SSP are depicted in Figure 1A. Almost half (46%) scored in the atypical range for sensory processing, with 18% scoring in the probable difference range and 28% scoring in the definite difference range. Figure 1B shows atypical sensory processing across the seven sensory domains of the SSP. The most common atypical pattern demonstrated in this cohort was Underresponsive/Seeks Sensation.
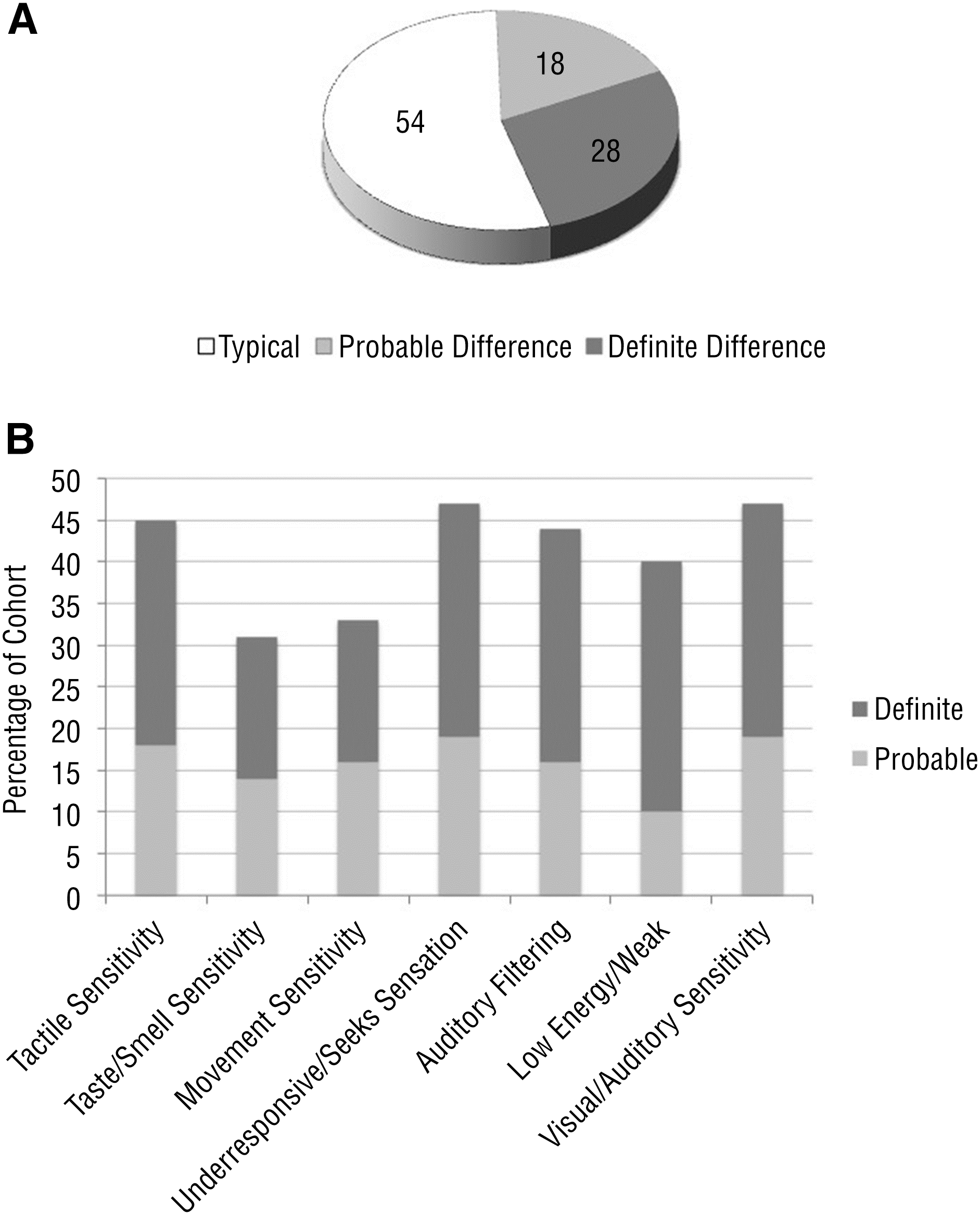
Percentage of participants scoring (A) in each range on the SSP at 4.5 yr and (B) in the atypical range across the seven SSP sensory domains.
Association Between Neonatal Variables and Sensory Processing
Analysis revealed that children with atypical sensory processing patterns had a younger gestational age (p = .02) and a significantly lower birthweight (p < .001), a lower Apgar score (p = .02), significantly more days of ventilation (p < .001), and a longer stay in the NICU (p = .001) than children with typical sensory processing patterns. The groups did not differ in terms of sex, SNAP–II scores, abnormal cranial ultrasound, or days on supplemental oxygen (Table 2).
Associations Between Neonatal Variables and Sensory Processing
Note. NICU = neonatal intensive care unit; SNAP–II = Score for Neonatal Acute Physiology–II.
Fisher’s exact test.
Mann–Whitney U test.
Spearman’s rank-order correlations were conducted to examine correlations among neonatal variables that differed significantly between the typical and the atypical sensory processing groups. Because birthweight and gestational age were highly correlated (r = .74), we entered gestational age in the regression model as a reflection of physiological immaturity (Table 2). Days of ventilation and days in the NICU (r = .80) were highly correlated. Because we hypothesized that exposure to the NICU environment would be associated with sensory processing differences, we entered this variable into the model. Thus, our regression model included gestational age at birth, 5-min Apgar score, and days in the NICU. The regression model (Table 3) revealed that Apgar scores (p = .03) and days in the NICU (p = .02) were independently associated with atypical sensory processing. Gestational age was not associated with sensory processing patterns.
Neonatal Variables Predictive of Atypical Sensory Processing
Note. CI = confidence interval; NICU = neonatal intensive care unit.
Discussion
Prevalence of Atypical Sensory Processing Patterns
We found that almost half of our cohort of children born very preterm exhibited atypical sensory processing patterns. Contrary to our hypothesis that sensory sensitivity would be the most prevalent pattern, more than 40% of the cohort displayed greater underresponsiveness or sensory seeking, suggesting they had a high threshold for stimulation. However, more than one-third of the cohort displayed visual–auditory, taste–smell, movement, and tactile sensitivity, which suggests a low neurological threshold in these sensory domains.
Our study corroborates previous findings that children born preterm may be at risk for developing sensory processing differences. Previous studies have reported that preterm infants show altered sensory processing in toddlerhood (Bart, Shayevits, Gabis, & Morag, 2011; Case-Smith, Butcher, & Reed, 1998; Wiener, Long, DeGangi, & Battaile, 1996). Our findings show that children born very preterm continue to experience sensory processing differences at age 4.5 yr.
Wickremasinghe et al. (2013) found that auditory, tactile, and vestibular processing were most affected in their cohort of very preterm children assessed between ages 1 and 8 yr, with 39% having sensory profiles in the atypical range. This prevalence is lower than that in our current study; almost half of our participants had atypical sensory processing patterns. This result may have been due to the low median birthweight and gestational age in our cohort of children who receive follow-up through NFUP. Although Wickremasinghe et al. found that no perinatal or neonatal factors were associated with increased risk of atypical sensory processing in children born prematurely, they found a trend toward increased risk of altered sensory processing and brain injury.
Eeles et al. (2013a) compared the sensory processing patterns of very preterm children and term-born control children at age 2 yr using the Infant/Toddler Sensory Profile (Dunn, 2002). The very preterm group exhibited more atypical sensory processing patterns and more frequent sensory processing behaviors than the controls. Male sex, higher social risk, longer hospital stay, and moderate to severe white-matter abnormalities were predictive of atypical sensory processing patterns. Although we also found that longer hospital stay was significantly associated with sensory processing, we did not find a significant association with male sex or abnormal cranial ultrasound, perhaps because Eeles et al. (2013a) used data from magnetic resonance imaging, which is more sensitive than cranial ultrasound.
Atypical sensory processing patterns have been correlated with poorer neurodevelopmental outcomes at age 2 yr in children born very preterm (Eeles et al., 2013b). Because we found that sensory processing differences were still present in almost half of preterm children at age 4.5 yr, future research is warranted to fully understand the impact of sensory processing differences on development and functional outcomes in this high-risk population. School entry may be particularly difficult for very preterm children with sensory processing differences, which have been shown to affect social adaptive behaviors and participation in academic and social activities (Ben-Sasson, Carter, & Briggs-Gowan, 2009).
Apgar Scores and Length of Stay in the Neonatal Intensive Care Unit
In our cohort, children with atypical sensory patterns were more likely to be of lower gestational age and birthweight, have a lower Apgar score, have more days of ventilation, and have a longer stay in the NICU than children with typical patterns. Apgar score and length of NICU stay were independently associated with sensory processing patterns outside of the typical range. A lower Apgar score suggests a greater need for resuscitation and medical intervention early in life, but it may also reflect other prenatal or perinatal risk factors that may be associated with altered sensory processing patterns. Contrary to our hypothesis, early illness severity was not associated with atypical sensory processing, but early life events increase an infant’s risk of having sensory processing differences.
In addition, an odds ratio of 1.009 for duration of NICU stay suggests that every day spent in the NICU increases an infant’s risk of developing atypical sensory processing. This finding is consistent with those of Eeles et al. (2013a), who found that longer hospital stay was predictive of atypical sensory processing patterns. Length of stay may be related to how sick the baby is or to other exposures in the NICU, such as invasive procedures or infection. Severity of early illness, postnatal infection, and pain-related stress has been associated with slower brain development (Brummelte et al., 2012; Chau et al., 2012; Zwicker et al., 2013). Although Wickremasinghe et al. (2013) did not find associations between perinatal or neonatal factors, they did report a trend between brain injury and atypical sensory profiles. Further examination of the relationship among exposure in the NICU, brain development, and sensory processing outcomes is warranted.
In an effort to decrease procedural pain and improve neurodevelopmental outcomes, the current standard of care in the NICU is to reduce aversive sensory stimuli, such as noise and light, and to attempt to create a womblike atmosphere through swaddling and facilitated tucking (Aucott, Donohue, Atkins, & Allen, 2002). These procedures, however, may or may not improve sensory processing outcomes. Even with these interventions in place, almost half of the children in our cohort developed atypical sensory processing. Conversely, the prevalence of sensory processing differences may have been higher without these interventions.
Limitations
Several limitations of this study should be noted. This study did not account for other confounders that may have had an impact on the study participants’ sensory status, such as procedural pain. Because our aim was to explore perinatal risk factors for sensory processing differences, we did not adjust for multiple comparisons, nor did we complete separate analyses for children who scored in the probable versus definite difference ranges in sensory processing. Our statistical analysis included neonatal data only to initial discharge, which did not account for readmissions. Our measure of sensory processing differences was limited to caregiver report. Last, prenatal risk factors and socioeconomic risk factors were not collected.
Implications for Occupational Therapy Practice
The results of our study suggest that children born very preterm are at high risk for developing atypical sensory processing patterns, which have the following important implications for occupational therapy practitioners who work with these infants and children across their lifespan:
Sensory processing differences may be related to prenatal or perinatal factors, neonatal illness, or NICU environmental exposure. The current standard of care in the NICU is to reduce aversive sensory stimuli, but whether this practice has an impact on sensory processing outcomes is unknown. Future research on interventions to prevent atypical sensory processing patterns in this vulnerable population is needed.
Given the high prevalence of sensory processing differences in children born very preterm, referral to occupational therapy for routine evaluation may be appropriate for this population.
Children with sensory processing differences may experience difficulties in the performance of daily occupations and could benefit from occupational therapy intervention (Polatajko & Cantin, 2010). By considering the sensory aspects of behavior, occupational therapy practitioners offer a unique perspective on the delivery of service to children with these difficulties (Ermer & Dunn, 1998).
Conclusion
Our study adds to the growing body of evidence suggesting that children born very preterm are at increased risk for atypical sensory processing. In addition, this study shows that perinatal factors and length of NICU stay are associated with altered sensory processing patterns. Further research on the prevention of sensory processing differences and the effect of interventions to reduce sensory input in the NICU is needed. Given the high prevalence of atypical sensory processing patterns in children born very preterm, routine evaluation of sensory processing differences in this population is recommended.
Footnotes
Acknowledgments
Stephanie C. Crozier and Jennifer Z. Goodson contributed equally to this work and share first authorship. We are grateful to the children and families who participated in this research and the Neonatal Follow-Up team, especially Arsalan Butt for managing the data. This study was unfunded but included preterm infants in studies funded by the Canadian Institutes of Health Research (MOP79262; principal investigators, Steven Miller and Ruth Grunau). Ruth Grunau holds a Senior Scientist award from the Child and Family Research Institute, and Steven Miller is the Bloorview Children’s Hospital Chair in Paediatric Neuroscience. Jill G. Zwicker is supported by the Michael Smith Foundation for Health Research and the Canadian Child Health Clinician Scientist Program. Preliminary findings were presented at the Canadian Association of Occupational Therapists Annual National Conference, May 2014, in Fredericton, New Brunswick.