
Abstract
Brachial plexus birth palsy (BPBP) occurs in approximately 0.4–4.6 of every 1,000 live births (Adler & Patterson, 1967; Hoeksma, Wolf, & Oei, 2000; Hogendoorn, van Overvest, Watt, Duijsens, & Nelissen, 2010). The most common type of BPBP affects the upper trunk of the brachial plexus (C5 and C6) and is referred to as Erb’s palsy (Abzug & Kozin, 2010; Hale, Bae, & Waters, 2010; Kozin, Chafetz, Barus, & Filipone, 2006). Damage to C5, C6, and C7—or extended Erb’s palsy—is the next most frequent classification of BPBP (Abzug & Kozin, 2010; Hale et al., 2010). Total or global plexus palsy affects the entire brachial plexus, C5 through T1 (Abzug & Kozin, 2010; Hale et al., 2010).
Although some infants fully recover, approximately one third of these patients experience lifelong complications (Hogendoorn et al., 2010; Pondaag, Malessy, van Dijk, & Thomeer, 2004). Residual BPBP is known to cause anatomical changes and motion deficits of the affected upper extremity such as
Reduced limb length (Abzug & Kozin, 2010; Bae, Ferretti, & Waters, 2008; Terzis & Kokkalis, 2010) and girth (Abzug & Kozin, 2010; Bae et al., 2008),
Abnormal scapular morphology (Duff, Dayanidhi, & Kozin, 2007; Kambhampati, Birch, Cobiella, & Chen, 2006; Kozin, 2004; Kozin et al., 2006; Kozin, Chafetz, Shaffer, Soldado, & Filipone, 2010; Soldado & Kozin, 2005; Van Heest, Glisson, & Ma, 2010; Waters, Smith, & Jaramillo, 1998),
Glenohumeral (GH) dysplasia and subluxation (Bhardwaj, Burgess, Sabapathy, Venkataramani, & Ilayaraja, 2013; Breton et al., 2012; Dodwell et al., 2012; Kambhampati et al., 2006; Kozin, 2004; Kozin et al., 2006, 2010; Pearl, Woolwine, van de Bunt, Merton, & Burchette, 2013; van Gelein Vitringa, van Royen, & van der Sluijs, 2013; Van Heest et al., 2010; Waters et al., 1998),
Muscle weakness, and
Range of motion (ROM) limitations (Abzug & Kozin, 2010; Bae, Waters, & Zurakowski, 2003; Fitoussi et al., 2009; Kozin et al., 2010; Mosqueda et al., 2004; Nikolaou et al., 2014).
Clinical measures, such as the modified Mallet classification (see Supplemental Figure 1, available online at http://otjournal.net; navigate to this article, and click on “Supplemental”), are used to assess development and progression over time as well as treatment outcomes (Abzug, Chafetz, Gaughan, Ashworth, & Kozin, 2010; Abzug & Kozin, 2010). The modified Mallet classification is used to evaluate the performance of certain tasks or movements that are commonly used during activities of daily living, such as reaching one’s mouth or midline. However, it provides no information regarding the scapulothoracic (ST) or GH contributions used to achieve these tasks (Blaauw & Muhlig, 2012; Fitoussi et al., 2009; Mosqueda et al., 2004). Knowledge regarding ST and GH function is critical because coordinated control of ST and GH movement is necessary for typical shoulder motion (Braman, Engel, Laprade, & Ludewig, 2009; Duff et al., 2007). Additionally, several conservative and surgical interventions commonly applied to the BPBP population target either ST or GH function. Motion capture technology provides a means of measuring ST and GH joint orientations in children with BPBP (Nicholson et al., 2014; Russo et al., 2014, 2015).
Scapular winging (i.e., ST internal rotation) is a frequent complaint of children with BPBP and their caretakers (Kozin, 2011; Pearl, 2009; Russo et al., 2015; Vander Have & Kozin, 2012; Wickstrom, Haslam, & Hutchinson, 1955) and is thought to be compensatory for decreased GH cross-body adduction (Russo et al., 2015). Similarly, increased ST excursion in all planes has been observed clinically in this population (Vander Have & Kozin, 2012; Waters, 2011). However, measurement of ST contributions to the modified Mallet positions with motion capture demonstrated that scapular excursion was similar to unaffected limbs (Russo et al., 2014). Altered resting position of the scapula shifted its arc of motion, which contributed to the visual appearance of increased scapular excursion (Russo et al., 2014). Conservative treatment of BPBP is aimed at preventing muscle tightness and subsequent joint contractures and includes modalities such as passive and active ROM exercises, participation in activities that promote upper-extremity use, therapeutic taping, splinting, and electrical stimulation (Ashworth & Kozin, 2011; Waters, 2011). However, there is little objective evidence supporting these treatments (Bradley, Baldwick, Fischer, & Murrell, 2009; Lin, Hung, & Yang, 2011; McConnell, Donnelly, Hamner, Dunne, & Besier, 2012; Thelen, Dauber, & Stoneman, 2008; Van Herzeele, van Cingel, Maenhout, De Mey, & Cools, 2013; Zanella, Willey, Seibel, & Hughes, 2001).
Existing reports in which the efficacy of scapular taping is evaluated are inconsistent (Bradley et al., 2009; Cools, Witvrouw, Danneels, & Cambier, 2002; Hsu, Chen, Lin, Wang, & Shih, 2009; Lee & Yoo, 2012; Lin et al., 2011; McConnell et al., 2012; Selkowitz, Chaney, Stuckey, & Vlad, 2007; Shaheen, Villa, Lee, Bull, & Alexander, 2013; Thelen et al., 2008; Van Herzeele et al., 2013; Walsh, 2010; Zanella et al., 2001) and represent different types of tape, tape application techniques, and populations (McConnell et al., 2012). Kinesio® Tex tape (Kinesio USA, Albuquerque, NM) has been reported to change scapular kinematics (Hsu et al., 2009; Van Herzeele et al., 2013), muscle activity (Hsu et al., 2009; Lin et al., 2011), and proprioception (Lin et al., 2011). However, in a randomized controlled trial, Thelen et al. (2008) compared therapeutic Kinesio taping and sham taping (two strips of Kinesio tape applied without tension) in young adults with rotator cuff pathology, and they found that therapeutic taping did not affect goniometer-measured scapular ROM during pain-free, maximum active ROM trials in abduction, forward flexion, and scapular plane elevation. In a case report of a child with BPBP, Walsh (2010) reported improved GH congruity and scapular orientation after a therapeutic taping intervention using Kinesio tape on the basis of radiographic evaluation. However, this is not an imaging modality typically used to assess pediatric GH joint morphology prior to ossification (Kozin et al., 2006; Waters et al., 1998).
The manufacturer has provided statements positing that Kinesio tape stimulates strengthening of weak muscles, reduces muscle fatigue by providing support, and provides proprioceptive input to assist with awareness (Kase, Martin, & Yasukawa, 2006). Additionally, Kinesio tape may encourage functional improvement by allowing the child to move in an optimally aligned position (Kase et al., 2006).
The purpose of this study was to determine whether therapeutic taping intended to stabilize the scapula changed ST, GH, and humerothoracic (HT) joint function at the time of tape application. Three-dimensional motion capture was used to accurately measure joint orientations to build on the case report shared by Walsh (2010) and to improve the generalizability of findings to the population with BPBP. We hypothesized that there would be no differences in ST, GH, or HT orientations in a resting, neutral position. Additionally, we hypothesized that there would be no differences in the ST, GH, or HT joint angles in each of the modified Mallet positions. Finally, we hypothesized that there would be no differences in the ST and GH displacements from the neutral position to each of the modified Mallet positions.
Method
Participants
Twenty-six children (M age = 9.9 ± 3.2 yr) with BPBP were recruited for this study following the institution’s informed consent and assent procedures. A registered and licensed occupational therapist with more than 25 yr of experience in pediatric occupational therapy, including more than 9 yr working with pediatric BPBP patients, confirmed that participants were appropriate candidates for scapular stabilization with therapeutic taping. The therapist subjectively assessed children for scapular winging that was increased compared with the unaffected limb and could be improved with manual manipulation. Patients who had spinal accessory nerve transfers or lower trapezius tendon transfers were excluded from the study because the selected therapeutic taping was intended to augment the middle and lower trapezius. Additionally, poor skin integrity or open wounds were considered contraindications for therapeutic taping and, therefore, study participation. Finally, excessive soft tissue that would hinder marker placement on the scapula was an exclusion criterion. No recruited participants were deemed poor candidates for scapular taping.
Data Collection
An eight-camera motion capture system (Vicon, Centennial, CO) operating at 60 Hz was used to collect three-dimensional coordinate data of markers placed on the following anatomical landmarks: spinous processes of T2 and T8, sternal notch, acromion process, and medial and lateral epicondyles of the humerus. Markers on the trigonum spinae and inferior angle of the scapula were repalpated in each tested position. Data were collected in a neutral position and each of the modified Mallet positions: global abduction, global external rotation, hand to neck, hand to spine, hand to mouth, and internal rotation (see Supplemental Figure 1).
An occupational therapist who was a certified Kinesio taping practitioner then applied Kinesio Tex tape to facilitate middle and lower trapezius function on the affected side (see Figure 1). Participants were asked to bring their shoulders “down and back,” and the alignment of the scapulae was manually maintained by the occupational therapist during tape application. The Kinesio tape was anchored medially at the spinous processes (T2–T3 for middle trapezius and T12 for lower trapezius) and was applied toward the acromion with paper-off tension (Kase et al., 2006). After application of the tape, the motion capture data were re-collected for all positions.

Therapeutic tape applied to the left shoulder to facilitate middle and lower trapezius function for the purpose of improving scapular stabilization.
Data Analysis
Coordinate systems for the thorax, humerus, and scapula were constructed such that the axes aligned with those recommended by the International Society of Biomechanics (Wu & Cavanagh, 1995). Helical angles were used to calculate the ST joint angles (upward and downward rotation, internal and external rotation, and anterior and posterior tilt), which are shown in Figure 2a (Woltring, Huiskes, de Lange, & Veldpaus, 1985). A modified globe method was used to calculate GH and HT joint angles (elevation, internal and external rotation, and cross-body adduction and abduction), demonstrated in Figures 2b and 2c. This deviated from the International Society of Biomechanics recommended Euler sequences for calculating ST, GH, and HT angles (Wu et al., 2005). However, Euler sequences best resemble clinical observation when the first rotation corresponds to the axis about which the greatest motion occurs and the last rotation occurs about the long axis of the distal segment. This limits the applicability of Euler rotation sequences for the multiaxial movements evaluated in this study with axes of greatest rotation that vary among participants. The use of order-independent joint angle calculations (helical angles and modified globe method) allowed for application to all tested positions. One modification to the previously described globe method was made: The GH internal or external rotation angle was calculated as the degrees of rotation about the long axis of the humerus between the neutral trial and each of the modified Mallet positions (Pearl, Harris, et al., 1992; Pearl, Jackins, Lippitt, Sidles, & Matsen, 1992). ST and GH joint angular displacements from the appropriate neutral position to each of the modified Mallet positions were also calculated (neutral position with no tape for the trials without scapular taping and neutral position with tape for the trials with scapular taping).
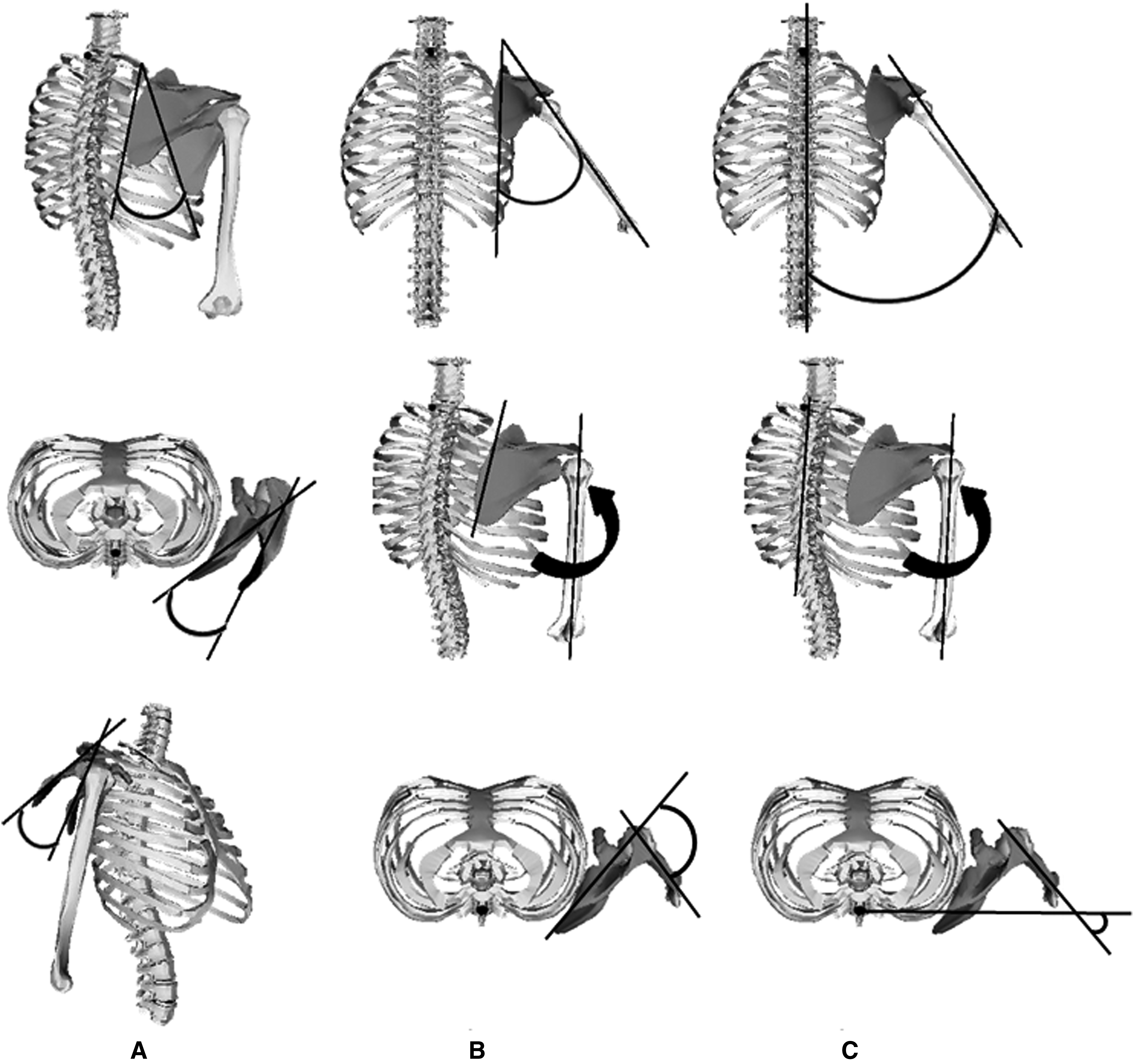
(A) Scapulothoracic joint angles from top to bottom: upward and downward rotation, internal and external rotation, and anterior and posterior tilt. (B) Glenohumeral and (C) humerothoracic joint angles from top to bottom: elevation, internal rotation, and cross-body abduction.
Statistical Analysis
The ST, GH, and HT orientations in the neutral position were compared before and after therapeutic taping with one-way, repeated-measures multivariate analyses of variance (α = .05; Harris, Sheean, Gleason, Bruemmer, & Boushey, 2012). The factor levels consisted of condition (with and without tape), and the dependent variables were each of the three joint angles (each anatomical axis). A Bonferroni multiple comparisons correction was applied to account for testing multiple joints. In the event of a significant Wilks’s λ, univariate analyses of variance were conducted to determine which joint angles produced significant differences. Bonferroni multiple comparisons corrections were also applied to the univariate tests to account for comparing the three anatomical axes. The same statistical approach was used to compare ST, GH, and HT joint angles—as well as ST and GH joint displacements—in each of the modified Mallet positions before and after tape application. All statistical analyses were performed with IBM SPSS Statistics (Version 20; IBM Corp., Armonk, NY).
Results
Participant characteristics and relevant surgical histories are shown in Table 1. The notable differences in the ST, GH, and HT joint angles with therapeutic tape for scapular stabilization compared with no tape for all positions are displayed in Table 2. Sample sizes were equal for all groups, and data were independently sampled. In the neutral position with therapeutic taping for scapular stabilization, children demonstrated significantly increased ST upward rotation (p = .007), significantly decreased ST internal rotation (p < .001), and significantly decreased ST anterior tilt (p = .007). At the GH joint, the cross-body adduction was significantly increased (p = .004), and external rotation was significantly decreased (p < .001).
In the abduction position with therapeutic tape in place, children demonstrated a statistically significant increase in posterior tilt end orientation (p < .001) but no resultant change in the ability to elevate the arm, as evidenced by no significant differences in the HT joint angles. In the external rotation position, children exhibited significantly less winging—that is, scapular internal rotation (p < .001)—and more upward rotation (p = .015) with taping. These differences resulted in a statistically significant increase of approximately 3° of HT external rotation (p = .010).
In the hand to neck position with therapeutic taping, children demonstrated significantly decreased scapular winging (p = .001) and increased posterior tilt (p = .005); however, they achieved no significant change in overall motion. In the hand to spine position, children demonstrated significantly less scapular winging (p < .001) and a statistically significant increase in GH internal rotation of about 5° (p = .002) with tape. There was no change in overall performance on the basis of the lack of change in HT joint angles. In the hand to mouth position with therapeutic tape in place, children demonstrated the greatest significant decrease in scapular winging (approximately 10°; p < .001). Additionally, they used significantly greater scapular posterior tilt (p < .001), significantly less GH external rotation (p < .001), and significantly more GH cross-body adduction (p = .006). However, HT cross-body adduction significantly decreased (p = .001). Finally, in the internal rotation position, children also exhibited significantly less scapular winging (p < .001) and a corresponding significant increase in GH internal rotation (p < .001) and cross-body adduction (p = .012) with therapeutic taping for scapular stabilization.
Participant Histories and Previous Shoulder Surgeries
Note. X = participant previously had the surgery or procedure indicated in the column heading.
ST, GH, and HT Joint Angles (M ± SD in Degrees) That Demonstrated Statistically Significant Differences With Scapular Taping
Note. The difference between joint angles with and without scapular taping is also shown as well as the p values from the univariate analyses of variance. Negative values represent an angle that is opposite of the expected direction—that is, negative external rotation reflects internal rotation. AT = anterior tilt; CBA = cross-body adduction; ER = external rotation; GH = glenohumeral; HT = humerothoracic; IR = internal rotation; M = mean; PT = posterior tilt; SD = standard deviation; ST = scapulothoracic; UR = upward rotation.
Regarding the joint angular displacements (difference between the Mallet position and the neutral position; i.e., joint excursion), the only significant differences in ST and GH angular displacements occurred in the abduction position (see Supplemental Table 1, available online at http://otjournal.net; navigate to this article, and click on “Supplemental”). ST posterior tilt displacement significantly increased (p < .001), and ST internal rotation displacement increased (p < .001) from 1.8° of external rotation to 5.4° of internal rotation with therapeutic taping. GH cross-body abduction displacement increased significantly (p = .003) with therapeutic taping in the abduction position.
Despite changes in the ST and GH contributions to motion, there were no changes in the modified Mallet scores. The joint angles and joint angular displacements that did not change significantly with scapular taping are displayed in Supplemental Tables 2 and 3 (available online), respectively.
Discussion
Therapeutic taping with Kinesio tape significantly decreased scapular winging (i.e., internal rotation) 8°, on average, at rest; moreover, it reduced scapular winging (5°–10°) in all modified Mallet positions except abduction. However, in the hand to mouth position, decreased scapular winging occurred along with decreased GH external rotation. In some children, this result was reflected in an anecdotally worsened trumpet sign, which has previously been associated with limited GH external rotation (Hentz, 2001). Overall, the decreases in scapular winging were relatively small from a clinical perspective but highly consistent. Additionally, there were statistically significant increases in GH joint angles in the hand to spine, hand to mouth, and internal rotation positions. Most of these gains were increased internal rotation and cross-body adduction angles; moreover, the only notable change in GH angular displacement was increased cross-body abduction in the abduction position. The sole gain in overall function, determined by HT orientation, was a statistically significant increase of approximately 3° of HT external rotation in the external rotation position, which holds little clinical meaning.
The observed changes in joint orientations are primarily attributable to reorientation of the existing arc of active ROM. The resting positions of the ST and GH joints were reoriented with the application of Kinesio tape, and these new orientations were largely maintained throughout the tested motions. The shift in the arcs of active motion provides explanation for the benefit of increased GH internal rotation angle with scapular taping. Traditionally, internal rotation contracture is considered one of the hallmarks of Erb’s palsy and the primary factor leading to the development of GH dysplasia. However, more recent evidence has demonstrated multidirectional GH joint motion limitations and altered ST posturing (Eismann, Little, Laor, & Cornwall, 2015; Russo et al., 2014, 2015). A portion of the apparent internal rotation posturing in children with Erb’s palsy is due to internal rotation (winging) of the scapula. The Kinesio tape was able to partially correct the ST winging without compromising function, as evidenced by increased GH joint internal rotation and cross-body adduction angles and largely unchanged HT orientations. Overall, the arcs of ST and GH motion (joint angular displacements) stayed the same but were reoriented with therapeutic taping. This did not change the Mallet scores, as evidenced by no clinically significant changes in HT joint angles, indicating no gain or loss in overall function of the upper extremity. If implemented early, these changes in ST and GH joint orientations may have a positive impact on the development of GH joint contractures and dysplasia. Therapeutic taping serves as a preparatory method of scapular stabilization that may help facilitate motor learning with an eventual goal of transitioning the patient to no taping requirement.
For all participants, the trials with scapular taping were collected after the baseline trials with no tape. Although it is possible that there could be a learning effect from repeating the positions, this is unlikely because 75% of the children participated in the research immediately after their routine clinic exams. During their exams, they performed all of the modified Mallet positions at least once, and most of the positions represent activities of daily living that the children are accustomed to performing regularly throughout the day. The statistically significant differences that were found, particularly decreased scapular winging, are not consistent with changes expected from a learning effect. Additionally, the potential for a placebo effect from the therapeutic taping was not evaluated in this study, and the effects of other therapeutic taping configurations remain unknown.
The long-term effects of therapeutic taping were not assessed in this study. This study served as initial investigation in a series of planned studies to assess the efficacy of therapeutic taping, and the primary purpose of this study was to determine whether therapeutic taping changed ST, GH, and HT joint function at the time of application. With no change at the time of application, long-term changes would be unlikely, making a long-term study futile; however, with changes in joint function after the application of therapeutic tape, the potential for a long-term effect exists. Future researchers investigating the long-term effects of a therapeutic taping intervention may benefit from recruitment of a younger participant population with a greater capacity for GH joint remodeling; however, the present participant cohort was suitable for evaluation of change in ST, GH, and HT joint function with the application of therapeutic tape for scapular stabilization. Finally, other factors that need to be considered when electing to use scapular taping for a child—such as potential for skin irritation, participant motivations, time, cost, and so forth—were beyond the scope of this study and should be considered on an individual participant basis.
The findings of this study are consistent with a previous case study in which Walsh (2010) reported reduced scapular winging in a child with BPBP after Kinesio taping. Additionally, increased posterior tilt of the scapula with arm elevation has been previously reported with therapeutic taping of the scapula in healthy handball players (Van Herzeele et al., 2013) and with therapeutic taping of the scapula in baseball players with shoulder impingement syndrome (Hsu et al., 2009). However, the long-term effects of therapeutic taping were not assessed in the current study. A prospective, randomized controlled trial is needed to investigate the impact on ST and GH joint function over time and to determine whether any clinically meaningful changes are maintained after the intervention has concluded.
Conclusion
The use of Kinesio tape to improve scapular stability by facilitating middle and lower trapezius function reduced scapular winging and, in some positions, increased the GH cross-body adduction or internal rotation joint angles. However, there were no clinically meaningful changes in overall ability to perform the modified Mallet positions, which represent movements used in activities of daily living. The reduction in scapular winging was relatively small from a clinical perspective, averaging less than 10° in all tested positions except hand to mouth. Nevertheless, the findings of this study demonstrate changes that may have a positive effect on GH joint development. Further investigation is needed to understand the mechanism of the observed changes with scapular taping in children with BPBP and the effects of alternative taping configurations. A prospective, randomized study is needed to assess the potential benefits regarding GH joint dysplasia and contracture development.
Implications for Occupational Therapy Practice
Therapeutic taping is a preparatory method available to occupational therapists for noninvasive management of scapular winging in children with BPBP. Although it is frequently used, there is a paucity of literature in which the efficacy of therapeutic taping is investigated for this purpose and population. This study provides evidence that scapular stabilization with therapeutic tape to facilitate the middle and lower trapezius does change ST and GH joint function at the time of application in children with BPBP. The decrease in scapular winging was clinically small but statistically significant. Future research is needed to assess the effect of the tape over time and long-term outcomes. However, the findings of this study have several implications for occupational therapy practice:
Facilitation of the middle and lower trapezius with therapeutic tape produces a small decrease in scapular winging at the time of tape application in children with scapular winging because of BPBP.
Facilitation of the middle and lower trapezius with therapeutic tape achieves small increases in GH joint angles in positions of rest, internal rotation, hand to mouth, and hand to spine at the time of tape application in children with scapular winging because of BPBP.
Facilitation of the middle and lower trapezius with therapeutic tape has little effect on overall shoulder function, measured by HT joint orientations and angular displacements.
The changes in ST and GH joint function have the potential for long-term benefit; however, the effect of therapeutic tape over time and the long term remains unknown.
Supplemental Materials
Supplementary material for Therapeutic Taping for Scapular Stabilization in Children With Brachial Plexus Birth Palsy
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2016.018903.pdf for Therapeutic Taping for Scapular Stabilization in Children With Brachial Plexus Birth Palsy by Stephanie A. Russo, Luisa M. Rodriguez, Scott H. Kozin, Dan A. Zlotolow, Ross S. Chafetz, Carolyn M. Killelea, Kristen F. Nicholson and James G. Richards in The American Journal of Occupational Therapy
Supplementary material for Therapeutic Taping for Scapular Stabilization in Children With Brachial Plexus Birth Palsy
Supplementary material, sj-pdf-2-aot-10.5014_ajot.2016.018903.pdf for Therapeutic Taping for Scapular Stabilization in Children With Brachial Plexus Birth Palsy by Stephanie A. Russo, Luisa M. Rodriguez, Scott H. Kozin, Dan A. Zlotolow, Ross S. Chafetz, Carolyn M. Killelea, Kristen F. Nicholson and James G. Richards in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
This research was conducted at Shriners Hospitals for Children (Philadelphia, PA).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.