
Abstract
Although the term self-regulation is appearing more frequently in the occupational therapy literature, the extent to which it is consistently conceptualized is not clear. The aim of this scoping review was to examine how the term self-regulation is used by occupational therapists in research and practice literature. A total of 58 publications that included occupational therapy and self-regulation in the title, key words, or abstract were identified. Self-regulation was not explicitly defined by more than half of the authors. Four theoretical orientations seem to guide conceptualization: synactive development, sensory integration, cognitive–behavioral theory, and self-regulation theory. Conceptualization differed according to the population, levels of strategy use, source of strategy implementation, and desired outcomes. A lack of definitional clarity and conceptual consistency of the term self-regulation was noted. Use of an explicit definition in relation to an identified theoretical framework is recommended to promote intra- and interprofessional communication, education, and research.
The use of the term self-regulation has been increasing in occupational therapy research and practice literature. The term can be found in occupational therapy literature exploring a variety of topics, including interventions with preterm babies in neonatal intensive care units (e.g., Grenier, Bigsby, Vergara, & Lester, 2003), sensory integration programs with toddlers (e.g., Roberts, King-Thomas, & Boccia, 2007) or school-age children (e.g., Zeidler, 2012), task-oriented interventions with school-age children (e.g., Jokić, Polatajko, & Whitebread, 2013) and adults (e.g., Paquette, Egan, & Martini, 2013), and driving behaviors of seniors (e.g., Baldock, Mathias, McLean, & Berndt, 2006). A clear understanding of how the term is conceptualized is extremely important to ensure theoretical consistency in interventions and to promote intra- and interprofessional communication.
Although the concept of self-regulation is used by several disciplines, each discipline emphasizes different aspects or perspectives of the concept (Dinsmore, Alexander, & Loughlin, 2008). For instance, in social psychology, the definition of the term places a greater emphasis on the derivation of knowledge from the environment, whereas in education, the emphasis seems to be more on person processes such as cognition (Dinsmore et al., 2008). It is not yet clear whether occupational therapy favors a specific definition of the concept that is aligned with a particular framework within other disciplines or whether the profession has developed its own hybrid concept of self-regulation. The purpose of this article is to provide an overview of the use of the term self-regulation within the occupational therapy research and practice literature with the goal of lending greater theoretical understanding for intervention and improved clarity to intra- and cross-disciplinary discussions.
Scientific disciplines use concepts that are current within their particular fields; however, if no appropriate concepts are available, a discipline will borrow terms from other disciplines and use them for the development of its own knowledge. Fields that are new or that have not developed their own specialized concepts or terminology are particularly vulnerable to this phenomenon of conceptual cross-fertilization (Schopman, 1986). Such cross-fertilization of concepts from one scientific field to another expands understanding and is crucial for building knowledge (Lee, 2010; Schopman, 1986). However, as a construct is newly applied within a field, its conceptualization and operationalization may morph from those of the original, contributing to a lack of conceptual clarity (Alexander, 2008). This consequence has been noted in the field of education, where “precise or agreed-upon meaning for its most central constructs” is elusive (Alexander, 2008, p. 370).
Similarly, in occupational therapy, concepts and theories are often derived from a variety of fields such as psychology, medicine, and education. Although conceptual cross-fertilization has enriched the occupational therapy profession, there is a risk that confusion in constructs may occur if the origins and meanings of constructs are not well understood. Moreover, as a concept is used more frequently by a discipline, the possibility that conceptual clarity can be compromised increases (Alexander, 2008). The resulting conceptual confusion obscures the interpretation of research findings and hinders the progress of understanding (Lajoie, 2008). It is thus important to clarify constructs and maintain their distinctiveness (Dinsmore et al., 2008).
The concept of self-regulation originated in the 1970s. Initially, there appear to be two distinct orientations to the development of the construct: cognitive and neobehavioristic (Dinsmore et al., 2008). The cognitive orientation was based on the construct of metacognition, or thinking about thinking (Flavell, 1971, 1979). Flavell (1979) operationalized metacognition into the key areas of metacognitive knowledge, metacognitive experience, goals, and the activation of strategies but did not explicitly use the term self-regulation. Baker and Brown (1984) conceptualized metacognition as knowledge about cognition (monitoring) and mechanisms, identified as self-regulatory, that contain monitoring as a central focus. They developed a more specific operationalization of self-regulation: “checking the outcome, planning, monitoring effectiveness, testing, revising, and evaluating strategies” (Dinsmore et al., 2008, p. 393). Researchers began to refer to metacognitive control processes and self-regulatory metacognitive mechanisms, combining the construct of self-regulation and metacognition, thus expanding the original concept of metacognition as conceived by Flavell (Dinsmore et al., 2008).
The neobehavioristic orientation was based on the work of Albert Bandura, which used the term in the context of behavioral and emotional regulation. Bandura (1977) referred to human functioning as a person–behavior–environment interaction, whereby self-regulation involved the interaction between the environment and the person, mediated through behavior (Dinsmore et al., 2008). From the neobehavioristic orientation, this interaction between contextual factors and person variables and processes is a critical aspect of the self-regulation process (Dinsmore et al., 2008).
Following these early conceptualizations, an increased focus on self-regulation in academic settings occurred in the 1980s and 1990s, producing yet a new term—self-regulated learning (SRL; Dinsmore et al., 2008). The concept of SRL began as a theory of learning (Corno & Mandinach, 1983) with a broad regulatory focus, seeking to address the contribution of the interaction among cognitive, motivational, and contextual factors. The consideration of both cognitive and volitional factors derives from the two original orientations of the term self-regulation (cognitive and neobehaviorist). Whereas the terms metacognition and self-regulation were developed within broad contexts of activity, the development of the term SRL was grounded within the academic context (Fox & Riconscente, 2008). Over the years, SRL has been used beyond the academic setting, that is, in the home and wider community (Kaplan, 2008), physical education (e.g., Kolovelonis, Goudas, Hassandra, & Dermitzaki, 2012), sports (e.g., Martini, Rymal, & Ste-Marie, 2011; Ste-Marie, Rymal, Vertes, & Martini, 2011), and rehabilitation (e.g., Jokić et al., 2013; Paquette et al., 2013).
Dinsmore and colleagues (2008) posited that the terms metacognition, self-regulation, and SRL are distinct concepts that share a common core of self-awareness and regulatory action. Kaplan (2008) viewed this notion as restrictive and lacking in acknowledgment of the complexity of the interactions among the person, the environment, and the behavior that are critical to an understanding of monitoring and adapting one’s actions. He postulated that the terms metacognition, self-regulation, and SRL are really subtypes or dimensions of the one general phenomenon of self-regulated action. Not only would such a perspective recognize the multiple meanings of the term, but it would also facilitate awareness of the complexity of the self-regulation phenomenon and acknowledge the possibility that other types of self-regulated action may exist (Kaplan, 2008).
In occupational therapy, the term self-regulation seems to be appearing more frequently. It is not clear, however, whether the term is being used to refer to the concept as understood in psychology or education or in some other manner more specific to occupational therapy. Clear understanding of how self-regulation is being construed in the occupational therapy literature is critical to interprofessional dialogue and advancement in understanding of the concept and its applications to occupation. The aim of this scoping review was to examine how the term self-regulation is used by occupational therapists in the research and practice literature.
Method
A scoping review is a literature review on a general topic area undertaken to obtain a sense of the extent, range, and nature of concepts within a field of study (Arksey & O’Malley, 2005; Levac, Colquhoun, & O’Brien, 2010). In contrast to a systematic review, which synthesizes findings related to a highly focused research question, a scoping study provides a broad overview of what is known in a wide topic area. This type of review is useful to delineate a field of study and obtain a sense of the range within which a topic is understood. Like a systematic review, the methods used for data collection, analysis, and interpretation need to be rigorous and transparent.
Procedures
The present scoping review included four steps: (1) searching for relevant publications; (2) selecting publications on the basis of predefined inclusion criteria; (3) extracting data; and (4) collating, summarizing, and reporting results (Arksey & O’Malley, 2005; Levac et al., 2010). Although the process seems linear, the actual course of the review is generally iterative, with previous steps revisited as needed.
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) diagram in Figure 1 represents the process undertaken in the present review. For the current study question, the following databases were used: OTseeker, CINAHL, Scopus, PsycINFO, Embase, ERIC, and Medline. A search strategy was developed to define key words for all searches. For example, the Medline search strategy used was exp Psychology/ or Audiology/ or Speech–Language Pathology/ or (Human adj2kinetics).tw. or Occupational Therapy/ or Physical Therapy Specialty/ or Rehabilitation/ or Nursing/ or Education/ and [(self adj regulat*).tw. or (meta adj cognit*).tw.], limit to (English or French or Italian). No beginning date was identified, and the cutoff date was March 2014. Language inclusion criteria were limited to English, French, and Italian, with no other publication restrictions. All references were entered into a RefWorks file for processing (N = 1,804).
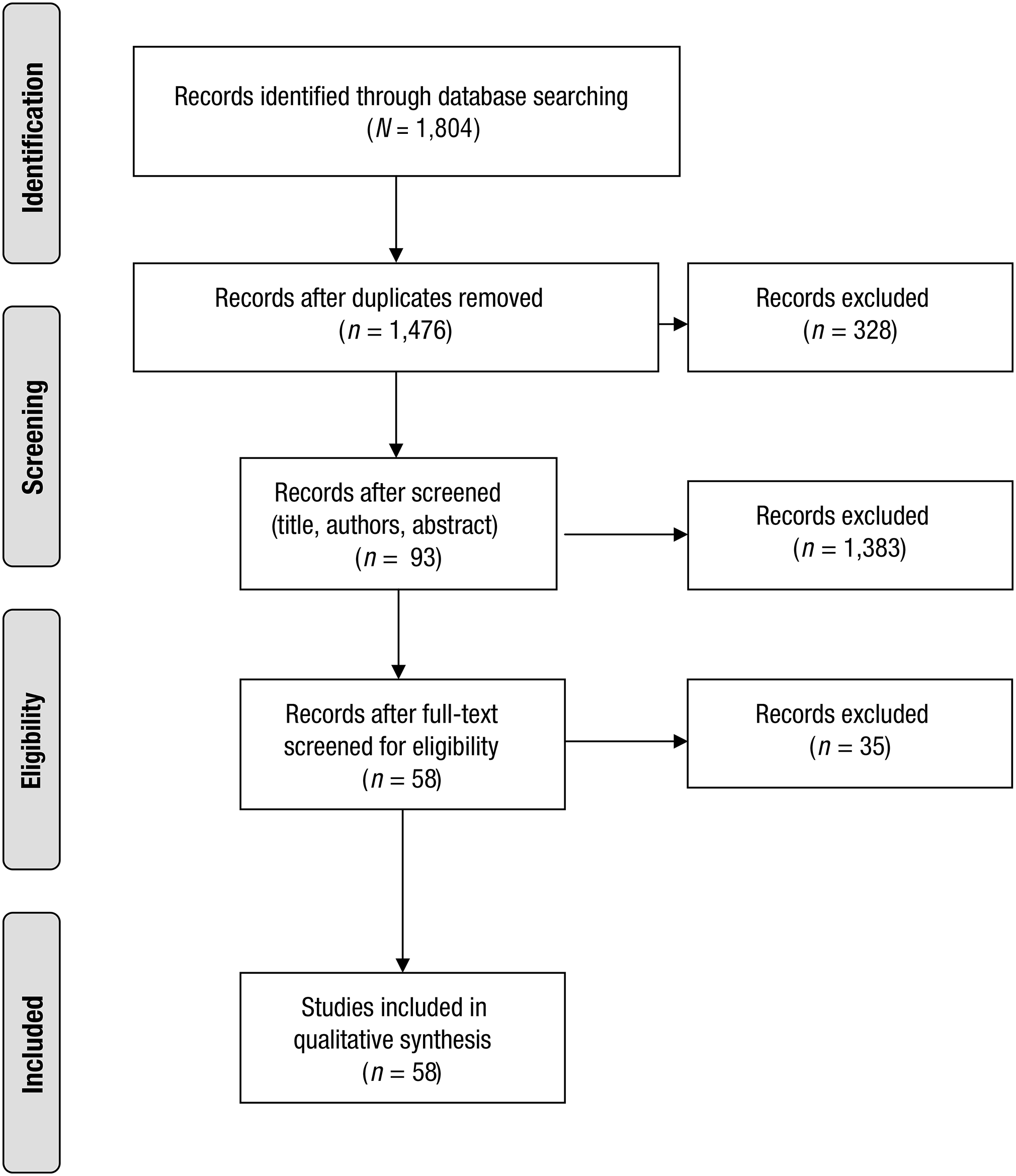
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram of articles identified, included, and excluded.
The original search captured 1,496 unique publications after duplicates were removed. These publications were evenly divided among the first three authors (Martini, Cramm, and Egan). At each step of the screening process, two of the three authors independently reviewed articles to determine inclusion. When disagreement occurred over study inclusion, the other author acted as a tie-breaker. The first screening round consisted of reviewing titles, authors, and abstracts. Full texts of articles were included for the second screening round if they contained the root terms occupational therapy and self-regulation in the title, key words, or abstract. This search resulted in 93 unique publications. These articles were then included for full review if at least one of the authors was an occupational therapist and if the publication included the term self-regulation. Articles were excluded if none of the authors was an occupational therapist or if the term self-regulation was not present or was used in relation to professional regulation. Editorials that introduced an article that included self-regulation and book chapters were also not included. Finally, only publications written in English were included.
Of the 93 publications identified from the review of abstracts, 35 were excluded (13 without an occupational therapist as an author, 11 that did not mention self-regulation, 5 concerning professional self-regulation, 1 thesis that was already described in an included article, 1 editorial describing an included article, 2 articles written in German, and 2 book chapters) and 58 were included. In reviewing the articles and their reference lists, an additional publication was identified, a book, and added to the already included publications.
The research team developed a data charting form to obtain key information from the 58 publications to be able to apply a common analytical framework. The identification of the data to be charted was an iterative process. As data charting proceeded, the team refined the extraction guide, testing it with parallel independent charting. They then met to determine whether the data charted were consistent across researchers. Once consistency was confirmed, two researchers (Martini and Egan) proceeded with the data charting for the rest of the publications. The following key items of information were identified and charted: author, year, type of publication, aim of study, population of concern, implicit and explicit definitions of self-regulation, assessment of self-regulation, interventions addressing self-regulation, associated outcomes, guiding theoretical framework, what is the focus of change, how is the change brought about, and who is initiating the change.
Data Analysis
To examine trends in the use of the term self-regulation in occupational therapy, data were analyzed quantitatively and qualitatively. Quantitatively, two frequency distributions were constructed. In the first, the number of articles in which self-regulation was mentioned was plotted over time. In the second, the number of articles by age group referred to was plotted, and the number of research versus practice papers was indicated.
Using thematic qualitative content analysis, two members of the research team (Martini and Egan) examined the charted data of the 58 articles regarding how the term self-regulation was used in each article (Arksey & O’Malley, 2005; Levac et al., 2010). First, explicit definitions were identified when present. When no explicit definition was provided, an implicit definition was determined on the basis of cited references or descriptions of the process and outcome of described interventions. Codes were then grouped into emergent categories. Once categories were generated, another member of the research team (Cramm) confirmed the themes and the classification of publications within these themes.
Results
The distribution of the 58 publications through time was explored. It seems that the term self-regulation first appeared in the occupational therapy literature in a 1973 theoretical article on the role of occupational therapy in the treatment of children labeled as hyperactive (Cermak, Stein, & Abelson, 1973). After this appearance, the term was not found in the occupational therapy literature until 1983, in a review of the behavioral frame of reference in which a self-regulation model was introduced to occupational therapy for clients with anxiety disorders (Stein, 1983). The term then reappeared once more in 1996, in the book How Does Your Engine Run? (Williams & Shellenberger, 1996). This book, written by occupational therapists, describes an intervention program that teaches children how to determine their level of alertness and choose appropriate strategies to change or maintain this state of alertness. After 2000, a steep increase was noted in use of the term, particularly in the past 10 years, when 47 of the 55 remaining articles were published (8 articles between 2000 and 2004, 25 between 2005 and 2009, and 22 between 2010 and April 2014).
The use of the term self-regulation in the occupational therapy literature spanned all age groups; however, most references were to school-age children. The majority of references (42 of 58) were found in research journals; however, some (11 of 58) were found in practice magazines, and the majority of these (7 of 11) related to school-age children.
As noted in Table 1, of the 58 publications, only 21 provided an explicit definition of self-regulation, leaving 37 (64%) publications that used the term but did not define it. Although 16 of the publications that defined self-regulation did so within a theoretical construct, 5 publications either did not identify a particular theoretical framework or referred to several different theories.
Summary of Publications in the Final Analysis
Note. CBT = cognitive–behavioral theory; CO–OP = Cognitive Orientation to daily Occupational Performance.
The thematic analysis led to the emergence of five major organizing categories: (1) theoretical framework, (2) how self-regulation is achieved, (3) who acts to achieve self-regulation, (4) what is regulated, and (5) age group. The distribution of articles according to these categories is portrayed in Figure 2. Two articles are not included in this diagram: One discussed the application of psychobiological measures (White & Mulligan, 2009), and the other was an Eleanor Clarke Slagle Lecture that introduced Dunn’s model of sensory processing (Dunn, 2001); neither article referred to a particular age group. Four theoretical orientations were identified—(1) synactive theory of development, (2) sensory integration theory, (3) self-regulation theory, and (4) cognitive–behavioral theory—or, conversely, no theory was identified.
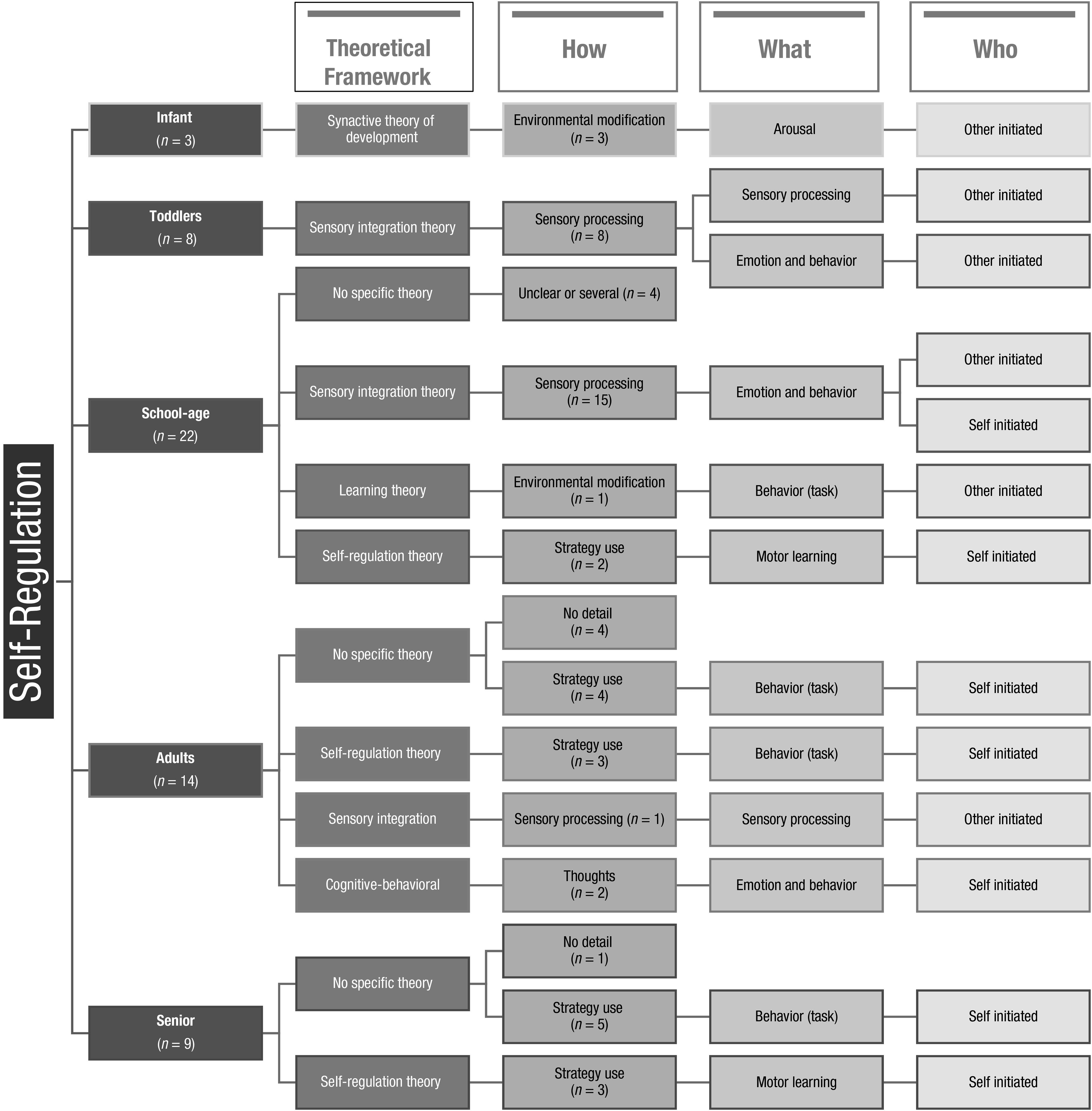
Distribution of articles according to thematic analysis.
The theoretical frameworks that guided conceptualization of the self-regulation process appear to be influenced by age. The youngest population with whom the term was used was infants being treated in neonatal intensive care units. The 3 related articles referred to the synactive theory of development (also known as the individualized developmentally supportive care model). This framework guides environmental modifications, such as the use of positioning, to help ensure that infants’ arousal levels are not elevated to the point at which adverse physiological reactions are triggered that limit their abilities to carry out volitional behavior that might be effective in self-calming.
Although 1 of the 8 publications concerning toddlers did not refer to a specific theory, the remaining 7 alluded to underlying sensory integration theory. The subject matter referred to guiding the modification of sensory processes (the way sensory information is perceived or integrated) to change sensory reactions (e.g., tactile response, sensory avoidance, sensory seeking) or emotion and behavior (e.g., frustration, anger, engagement). Actions to achieve change were carried out by someone other than the child (e.g., therapist, parent, teacher). In all 8 articles, the goal was to change infants’ responses to stimuli.
Of the 22 publications involving school-age children, a specific theoretical framework could not be discerned for 4. In 3 of these publications, no theories were referenced, whereas for 1 Cahill (2007), a variety of theories were alluded to. Of the remaining 18 publications, the predominant theoretical framework appeared to be sensory integration theory.
Similar to the articles on toddlers, change was often viewed as being caused by others (e.g., providing sensory integration treatment). However, when publications related to older children, the process of intervention included having the child become actively involved in applying strategies to mediate sensory processes. Specifically, the child was taught to use metacognitive strategies to recognize physical sensations related to different activity levels or emotions and to respond using preselected sensory strategies (e.g., squeezing stress balls, listening to music) to help modify sensory processes (e.g., sensitivity to sound or touch) with the end goal of managing emotions and behavior (e.g., to avoid becoming frustrated and throwing a pencil). In this way, then, the child produces the change. For this age group, some authors began to refer to the term self-regulation within a self-regulation theory framework (see Figure 2), where the focus is no longer on arousal, sensory processes, or emotions and behavior but instead on learning motor tasks through the use of metacognitive strategies. Moreover, it was noted that when the term self-regulation was used within a self-regulatory framework, it was always explicitly defined. However, when the term was used within a sensory integration framework, it was rarely defined.
With respect to publications concerning adults, the majority of publications (8 of 14) referred to the use of metacognitive strategies to change either task learning or behavior around how tasks are accomplished. Whereas metacognitive strategy use in 3 of these publications was guided by self-regulation theory, the remaining 5 publications (of the 8 referring to metacognitive strategies) did not mention a particular theory or framework. The term self-regulation was also used within a cognitive–behavioral framework (in 2 articles), particularly when the focus was on emotion and behavior. Again, in contrast to the conceptualization of the term in articles referring to children, when adults were the focus, self-regulation was no longer considered within a sensory integration framework. The exception was when cognitive functioning might be compromised (e.g., adults diagnosed with autism). In the publications relating to adults, in all instances, the changes were initiated by the client him- or herself, except when cognitive functioning was viewed as compromised.
All publications concerning older adults referred to the use of metacognitive strategies to learn a task (guided by self-regulation theory) or to reflect on and carry out appropriate task behavior (e.g., modifications to driving routines). Interestingly, in these latter instances, no theoretical framework was referred to. Note that in these instances, the term self-regulation was not explicitly defined.
Finally, a trend was noted across age categories with respect to who initiated the self-regulatory process. In babies and toddlers, all self-regulation processes were initiated by others, whereas in school-age children, there was a mix of initiation by others and self-initiation, and in adults and older adults, all self-regulation processes were self-initiated (except when dealing with groups typically labeled as cognitively delayed).
Discussion
This scoping review was undertaken to gain an understanding of how occupational therapy authors use the term self-regulation. Self-regulation has become an increasingly popular term in the occupational therapy literature. Whereas only 11 articles published between 1973 and 2004 used this term, 47 articles over the past 10 yr have used the term. The review indicates that the term has been used to characterize intervention across ages and diagnostic categories.
Definitional Ambiguity
The concept of self-regulation is complex. The ambiguity of this concept has been reported in education (Dinsmore et al., 2008) and in psychology (Bloch, Moran, & Kring, 2009). Our scoping review indicates that a lack of clarity is also evident within occupational therapy. Several factors contribute to this lack of clarity. First, this analysis of 58 publications shows that more than half of the occupational therapist authors who used the term self-regulation did not provide an explicit definition of the term. A similar finding was noted by Dinsmore et al. (2008) in their analysis of 255 studies in education; they found that when researchers used the term self-regulation they either provided no definition of the concept, misidentified the concept, or incorrectly operationalized the concept (Kaplan, 2008). The term self-regulation was used interchangeably with the terms metacognition and self-regulated learning or, in some cases, the two terms were embedded within each other (Lajoie, 2008).
Second, the influence from other domains is notable; our analysis identified four different theoretical frameworks that have guided the use of the term self-regulation in the occupational therapy literature. Further examination indicates that these frameworks seem to align with both the neobehavioristic orientation and the cognitive orientation described by Dinsmore et al. (2008). Three of the four theoretical frameworks used by occupational therapists (synactive theory of development, sensory integration, and cognitive–behavioral theory) principally target internal, unobservable processes. The study of self-regulation guided by the fourth theoretic framework, self-regulation theory, tends to target task learning or accomplishment, a more observable process.
When a definition of self-regulation was provided, definitions subsumed within the synactive theory of development referred to regulation of processes such as autonomic functions and arousal (e.g., Grenier et al., 2003). Within a sensory integration framework, definitions in publications on toddlers referred to abilities to regulate responses to stimuli (e.g., Roberts et al., 2007; Tirella & Miller, 2011) and definitions in publications on school-age children referenced controlling emotions and behaviors as well as self-recognition of feelings (e.g., Cyzner, 2000). Definitions derived from self-regulation theory tend to refer to a more cognitive process and an outcome such as acquisition or learning (e.g., Hyland & Polatajko, 2012; Paquette et al., 2013).
Several publications that did not identify a theoretical framework did provide a definition. These articles most often included a conscious or cognitive element and referred to monitoring of performance or behavior. The variety of elements included in the different definitions attest to the influence of the various theoretical frameworks. Such a variety in the conceptualization of the term is also present in the publications in which a definition was not provided.
Implicit Levels of Strategy Use
The process of self-regulation entails the application of strategies. Another source of ambiguity when considering conceptualizations of self-regulation in occupational therapy seems to be that most publications refer to strategy as a single common notion. When it comes to self-regulating behavior, the present examination seems to indicate two levels of strategy: (1) those focused on arousal or emotional state and (2) those focused on thinking.
In the first level of strategy use, when authors refer to self-regulation, the aim is to influence behavior through changing physiological or emotional arousal. These strategies act as a catalyst that brings about a change in emotion or arousal, which will in turn foster a change in behavior. The applications of these catalyst strategies tend to be initiated by certain internal states (e.g., low level of arousal) or emotion (e.g., anxiety). These strategies can be initiated by others or self-initiated. When they are initiated by another person (e.g., swaddling a baby, providing a weighted vest to a child), it is usually with younger populations (e.g., toddlers) or populations with potentially compromised cognitive ability (e.g., people with autism). In addition, in these cases, the strategies tend to be guided by the synactive theory of development or the sensory integration framework. When these strategies are self-initiated (e.g., positive self-talk), they are usually within a cognitive–behavioral framework and used by adults or older children.
The second level of strategy use is focused on thinking and has been labeled metacognitive (Flavell, 1979). This “thinking about thinking” guides strategy selection or problem-solving processes. Because metacognitive strategies involve thinking, they are always self-initiated; in the literature we identified, they were always used by an adult or older child. Metacognitive strategies are found in the self-regulation process described within self-regulation theory and are applied to task learning and accomplishment. They are also found in cognitive–behavioral theory, in which they are used to monitor the application of strategies aimed to regulate internal behavior such as emotion.
In our examination of the use of self-regulation within the sensory integration theory framework in populations older than babies and toddlers (e.g., school-age children), we found that authors tended to describe both the application of strategies focused on arousal or emotion (initiated by others or by self) and the application of metacognitive strategies to provide insight on the emotional or sensory state (e.g., level of alertness; feelings of anger, frustration, stress) so that the input from the environment can be modified (e.g., use headphones to listen to music, hand fidgets or putty, wall push-ups) to alter the level of arousal or emotional state (i.e., strategies aimed at the emotional or sensory level). In these situations, the authors simply referred to self-regulation and did not differentiate between the functions of strategy application that were present, that is, the metacognitive strategy to guide the strategy selection (when and what catalyst strategy to use) and the catalyst strategy applied that would precipitate the change in sensory or emotional state. This approach leads to confusion because it not clear whether self-regulation refers to the process of applying a strategy to change the sensory and, by extension, emotional state or to the metacognitive process of strategy selection and application.
Consistency of Theoretical Framework and Strategy Level
In occupational therapy, self-regulation refers to several concepts. Note that the term has relatively consistent meaning when applied to work with infants and adults. However, when used to describe work with children, there is a fair amount of variation that seems to be influenced by the underlying theoretical frameworks. Although there are several reasons to ensure a clear conceptualization of the term, an important one is communicating a logical connection to an underlying theoretical framework, which is critical in practice, research, and education.
First, without reference to an underlying theoretical framework, from an intervention perspective, it is challenging to select and defend the use of particular self-regulation strategies. As clinicians, it is important that practitioners understand strategies conceptually. With such an understanding, the practitioner can appreciate the hypothesized mechanism of action of the intervention and the expected results. Understanding the mechanism of action ensures that methods are applied appropriately and can be adapted, when necessary, in a manner that still supports the outcome. Understanding the expected results makes it possible to clearly communicate them to clients and evaluate therapeutic effectiveness appropriately.
For example, in the synactive theory of development, in which self-regulation strategies aim to change physiological arousal (e.g., noted by flailing limbs and arching of back in premature babies), the effectiveness of the strategy (e.g., swaddling to maintain flexion) is determined by evaluating change in physiological arousal (e.g., infant’s sleep will be organized, agitation prevented). In the self-regulation theory framework, the strategies aim to guide a self-monitoring or problem-solving process (e.g., self-assessing performance, such as driving or throwing a ball, and changing the time of driving or ball-throwing technique accordingly). In these cases, the effectiveness of the self-regulation strategy would be ascertained by evaluating whether the client did self-assess and change when he drives or how he throws the ball.
When self-regulation strategies appear to be aimed at two levels, as previously described, it is important to evaluate the effectiveness of each level of strategy. For instance, in the ALERT Program, which is guided by sensory integration theory, Williams and Shellenberger (1996) referred only to self-regulation strategies, but they appeared to be alluding to two levels of strategy. The first level consists of catalyst strategies (e.g., manipulating a stress ball, listening to quiet music), which aim to change the sensory or emotional state (e.g., frustration, arousal). The second level consists of metacognitive strategies, which encourage the child to self-monitor frustration or arousal level. To evaluate the first level, practitioners might ask, “Does the child’s use of music calm him?”; to evaluate the second level, practitioners might ask, “Is the child able to self-monitor his arousal level?” “Is the child able to select an appropriate catalyst strategy?”
Table 2 presents the different theoretical frameworks identified in the occupational therapy literature search on self-regulation regarding the two levels of strategy application (catalyst and metacognitive) and the two types of initiation (by others and by self). This table demonstrates conceptual confusion because sensory integration theory can appear in all applicable quadrants, that is, within both levels of strategy application and both types of initiation.
Theoretical Frameworks by Initiation Type and Strategy Application
Note. NA = not applicable.
Second, from a research perspective, clear conceptualization of self-regulation and related concepts is essential for the development and refinement of occupational therapy interventions. Rigorous definitions of these concepts and an understanding of their relationship to each other are critical to developing a body of knowledge that demonstrates the validity of occupational therapy theories and the effectiveness of resulting procedures. Similarly, occupational therapy practitioners will be able to make use of advances from other fields only if they appreciate how the understanding of these concepts aligns with or differs from other fields. Conversely, lack of such understanding would make it difficult to translate occupational therapy research to other disciplines. For example, research in education can provide helpful information regarding the use of metacognitive strategies when occupational therapy defines self-regulation in terms of these strategies. Moreover, psychology research on sensory processing would be useful regarding the regulation of internal behaviors such as degree of sensory or emotional arousal when occupational therapy defines self-regulation in these terms.
Finally, from an education perspective the lack of conceptual clarity regarding self-regulation limits opportunities for students to fully understand how such occupational therapy interventions produce change and which changes they might logically produce. Therefore, an understanding of the underlying framework that guides strategy use in the self-regulation process is necessary.
Future Research
Several critical issues should be considered when engaging in research that encompasses the concept of self-regulation to ensure that it leads to theoretically valid and replicable outcomes. First, researchers should not assume that readers, whether they are clinicians, researchers, or educators, will know what self-regulation is. Lack of adequate definitions of essential concepts in research articles frequently causes confusion for readers trying to understand research results (Lajoie, 2008). Inconsistent definitions of essential concepts across studies often contribute to conflicting research results (Schunk, 2008). Although imposing one common definition is neither realistic nor desirable, it is reasonable and necessary for researchers to clearly define the term self-regulation when communicating their research results.
Second, researchers need to explicitly reference the theoretical frameworks that guide their research in self-regulation. As noted in this scoping review, in the occupational therapy domain, the study of self-regulation is guided by several theoretical frameworks, each with its own set of constructs and conception of self-regulation. The concept and definition of self-regulation is derived from the theoretical framework, so it is only by explicitly recognizing the relevant constructs that the vision, structure, and direction of the study can be properly understood. It permits the researcher to appropriately determine the relevant variables to explore, identify the outcomes to measure, and provide a context for the interpretation of results.
Finally, the aims of self-regulation strategies should be specified. The fact that self-regulation is applied in different domains and at different levels contributes to the complexity and confusion related to this concept. Although indicating the theoretical framework may be helpful in clarifying the domain in which the term is being used, as we have seen from our review, it may not provide clarity regarding the level at which strategies are being used, making it difficult to determine the appropriate variables or outcomes on which to focus.
Limitations
This scoping review has several limitations. There is always the possibility that literature may have been missed despite the search strategy and process being conducted with the support of an experienced research librarian (Lindsey Sikora). A certain level of inherent subjectivity is inevitable in the decision-making process when considering inclusion and exclusion of studies and in conducting the thematic analysis. To address the issue of bias in the study selection, all decisions were made independently by two reviewers, and a third reviewer acted as a tiebreaker. A similar process was undertaken for the data charting process. Finally, to reduce subjectivity in the thematic analysis, themes were derived by two reviewers and later verified by a third reviewer.
Implications for Occupational Therapy Practice
With clients of all ages and for a variety of outcomes, occupational therapy assessment and intervention consider self-regulation. Our findings have the following practical implications for occupational therapy practice:
Clinicians should be aware of and understand the conceptual framework and theories surrounding the self-regulation construct they are using.
To ensure proper application and evaluation of the effectiveness of self-regulation strategies, it is important for clinicians to consider what they aim to change through the use of these strategies and how this change is being brought about.
When two levels of self-regulation strategies are applied, it is important for clinicians to evaluate the effectiveness of each level.
When communicating, within and outside of the profession, practitioners should not assume that everyone possesses the same understanding of self-regulation. They should facilitate understanding by specifying the expected results (e.g., change in a particular behavior or emotion vs. new application of a strategy).
Conclusion
The term self-regulation within the occupational therapy literature does not convey a unique and uniform meaning. When occupational therapists discuss self-regulation in the literature, they are often explicitly or implicitly referring to different concepts. The results of this scoping review indicate that the meaning of self-regulation depends on the theoretical framework embraced, which itself seems to be guided by the intended population. As such, undefined use of the term can lead to lack of clarity, conceptual confusion, and poor communication within and outside of the profession. To ensure conceptual accuracy and consistency, researchers should explicitly reference one of the four identified theoretical frameworks and clearly specify the level of strategy used. This approach is key for researchers to advance the understanding of self-regulation and its complex nature at different levels of interactions and for clinicians to foster their clients' ability to self-regulate.
Footnotes
*Indicates article included in the scoping review.