
Abstract
Computer use at both home and work has now become an aspect of everyday life for people around the world. In addition, laptop popularity has increased because of the ease of setting up at any place, manageable weight, and energy-saving properties (Malińska & Bugajska, 2010). However, despite the vast developments that have taken place regarding desktop and laptop use over the past few decades, their use can have adverse effects that should not be ignored, including a possible impact on posture.
The rate of work-related musculoskeletal symptoms (MSSs) and disorders (MSDs), particularly of the spine, has accelerated (Cholewicki & McGill, 1996; Gerr, Monteilh, & Marcus, 2006; Goel, Kong, Han, Weinstein, & Gilbertson, 1993). Since the 1980s, MSSs and MSDs related to computer use have been recognized as a common cause of sick leave, efficiency loss, and work-related sickness in Western societies (Driessen, Anema, Proper, Bongers, & van der Beek, 2008; Griffiths, Mackey, Adamson, & Pepper, 2012; IJmker et al., 2007; Jacobs et al., 2013; Van Eerd, Hogg-Johnson, Cole, Wells, & Mazumder, 2012; Varte, Rawat, Singh, & Majumdar, 2013). Over the next 20 yr, MSDs are expected to be the most widespread of the major disorders among employees in Great Britain (Jones & Braham, 2009). This risk of MSSs and MSDs to computer users has been reported to be associated with ergonomic and postural issues (Marcus et al., 2002; Sillanpää et al., 2003).
The angle of a computer screen (i.e., visual display unit [VDU]) plays a role in determining ideal posture during laptop or desktop use (O’Sullivan et al., 2002, 2006; Williams, Hawley, McKenzie, & van Wijmen, 1991). Consequently, it is important to quantify the biomechanical principles involved. Computer users face VDUs in three main ways: looking down, straight on, and up. Looking down, as often seen in laptop use, might increase lower cervical flexion, causing increased demand on neck extensor muscles as they support the head, thus causing neck problems (Chaffin, 1991; Cho, Lee, & Choi, 2008; Straker & Mekhora, 2000; Yoganandan, Pintar, Cusick, & Kleinberger, 1998). In addition, users who look down tend to lean their head forward (turtle neck posture). Such posture may lead to chronic neck pain, influence thoracic vertebrae and the shoulder blades, and cause general imbalance in the musculoskeletal structure (Ariëns et al., 2001; Griegel-Morris, Larson, Mueller-Klaus, & Oatis, 1992; Malińska & Bugajska, 2010; O’Sullivan et al., 2006).
It has been reported that muscle fatigue is linked to the use of a high-set VDU, particularly in both trapezius and cervical erector spinae (Seghers, Jochem, & Spaepen, 2003; Sommerich, Joines, & Psihogios, 2001). When the VDU is placed at eye level or just below 5°, investigators have found a proportional relationship between muscle activity and neck angle (NA) and head tilt (HT; Seghers et al., 2003; Sommerich et al., 2001; Straker, Pollock, Burgess-Limerick, Skoss, & Coleman, 2008). Therefore, the cervical region (upper and lower) should be studied in posture research because it may influence head position. Nonneutral head positions, such as a forward head posture, may compromise the resting spinal column’s double-S shape and the whole body (Annetts et al., 2012; Black, McClure, & Polansky, 1996; Gandavadi, Ramsay, & Burke, 2007; Gill & Callaghan, 1998; Keller, Corbett, & Nichols, 1998; Moore, 2004; Toosizadeh, Nussbaum, Bazrgari, & Madigan, 2012). The lumbar and pelvic areas also appear to be key factors in stability during sitting (Annetts et al., 2012; Black et al., 1996).
Various methods are available for analyzing posture, including radiographs, sensors, subjective measures, and digital photogrammetry (Bridger, 2003; Corlett, 2005; Wong & Wong, 2008; Wong, Wong, & Lo, 2007). Photogrammetry is the science of making measurements from photographs, and it is considered one of the most widely used methods for body posture evaluation (Davidson et al., 2012). Two-dimensional digital image analysis with MATLAB software (MathWorks, Natick, MA) has been used because of its longevity, cost-effectiveness, and reliability. In addition, this software allows one to obtain results free from subjective bias (Jones, Sparkes, Busse, Enright, & van Deursen, 2011). Previous computer use studies have overlooked some key posture elements, such as examining main body segments (i.e., head, neck, lumbar spine, and pelvis) simultaneously (Saito, Miyao, Kondo, Sakakibara, & Toyoshima, 1997; Seghers et al., 2003; Straker, Jones, & Miller, 1997; Straker, O’Sullivan, Smith, & Perry, 2009). Therefore, this preliminary study assessed differences in NA, HT, lumbar angle (LA), and pelvic tilt (PT) between participants using a laptop and a desktop in the sitting posture during a typing task.
Method
Research Design
A crossover design in a single session was used with randomization of the order of a typing task on a laptop and a desktop computer. This study was approved by the ethics committee of the School of Healthcare Sciences at Cardiff University.
Participants
This study included a convenience sample of 20 healthy postgraduate university students with a normal spine. Both men and women were recruited to secure a roughly equal gender balance, and 15 men and 5 women ultimately participated. People with congenital abnormalities such as scoliosis or incidences of MSDs (e.g., low back or neck pain) were excluded (Kee & Lee, 2012; Oakley, Harrison, Harrison, & Haas, 2005). Participants read information sheets and gave informed consent. Table 1 summarizes participant characteristics.
Participant Demographics
Note. BMI = body mass index; M = mean; SD = standard deviation.
Procedures
Participants were photographed as they performed a 5-min typing task on a laptop and a desktop computer. We used a digital camera (Cyber-Shot DSC-P93; Sony, Tokyo, Japan) with a 5.1-megapixel Super HAD CCD, 14.0-bit digital extended processor, and 3× zoom lens. This camera also has a high-resolution and advanced shutter system (maximum 1/1000 s; Pownall, Moran, & Stewart, 2008).We also used a tripod with two built-in spirit levels to maintain the perpendicular position of the camera and eliminate error and maximize the methodological reliability (O’Sullivan, McCarthy, White, O’Sullivan, & Dankaerts, 2012; Pownall et al., 2008).
The computers, a Sony PCV-7776 desktop and an HP Pavilion dv3 laptop (Hewlett-Packard Co., Palo Alto, CA), were chosen for their popularity. Participants performed tasks while sitting on an adjustable hydraulic office chair (Bambach Saddle Seat; Ergostyle, Christchurch, New Zealand), without a back and arm rests to facilitate seeing markers placed on anatomical landmarks. An adjustable monitor stand for the desktop was used to match each participant’s eye level. Figure 1A shows the workstation and camera setup.
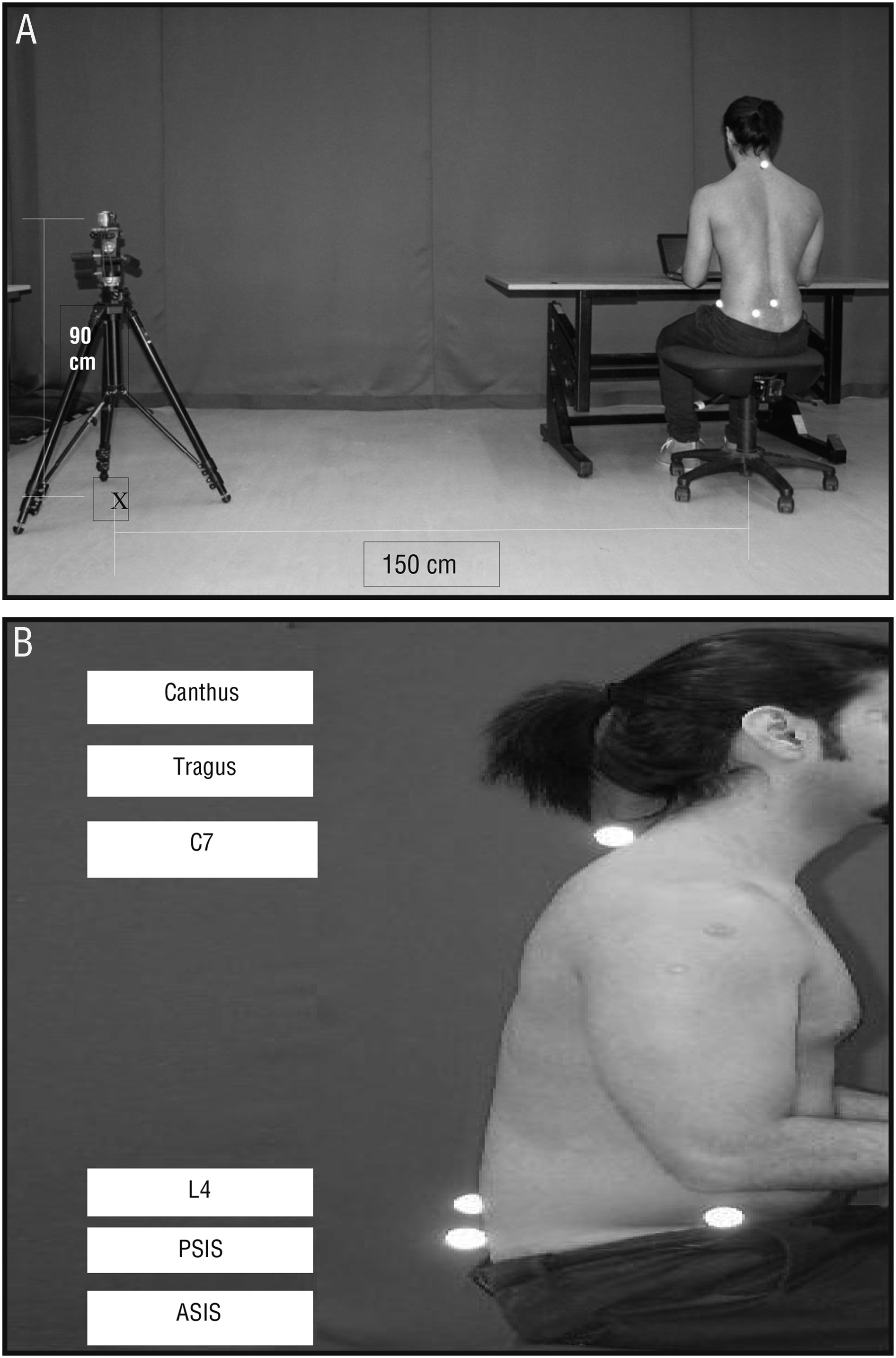
Research setup. (A) Workstation and camera. (B) Reflective markers on anatomical landmarks C7, L4, PSIS, and ASIS and paper markers on the canthus and tragus.
To easily identify anatomical landmarks and prevent markers from shifting if applied directly to participants’ clothing, women wore a tight-fitting vest and men were shirtless. Reflective markers (2.5 cm diameter) were positioned using double-sided adhesive tape on the skin over the seventh cervical vertebra (C7), the fourth lumbar vertebra (L4), the left anterior superior iliac spine, and the posterior superior iliac spine (Figure 1B). The left tragus and canthus were covered by small sticky paper dots (8 mm diameter). Larger reflective markers were used for obese participants for clear identification of the anatomical landmarks. Consistency of markers’ position was ensured while placing the markers by palpating the anatomical landmarks. To minimize misplacement of the markers, the same researcher placed the markers and remained during the whole study to ensure markers stayed in their positions, and markers were checked in the second trial.
The order in which participants used the laptop and desktop was randomly chosen (O’Sullivan et al., 2012), and participants were blinded to the timing of image capture (Kingma & van Dieën, 2009). At the last minute of each typing session, images were taken to ensure that participants adapted their typical typing habit. Because of the high reliability and validity of photogrammetry, one photograph from each session was imported to the MATLAB software to calculate participant angles (Jones et al., 2011; Kingma & van Dieën, 2009).
Participants were given instructions to sit with their knees, hips, and elbows at 90° (measured using a goniometer), with the height of the chair and desk adjusted accordingly and feet placed at shoulder-width distance (see Figure 1; Snijders et al., 1995). The top of the desktop’s VDU was at eye level (Straker et al., 2008), and viewing distance was about an arm’s length. The laptop’s screen–keyboard angle was between 119° and 126° (Nanthavanij, Jalil, & Ammarapala, 2008). Participants’ forearms were supported by the table (Aarås, Fostervold, Ro, Thoresen, & Larsen, 1997).
To avoid changes in the movement of participants’ neck and head, two windows of Microsoft Word 2010 (Microsoft Corp., Redmond, WA) were divided equally into vertical parallel pages on the VDU. The typing tasks included two different Word documents to avoid the learning effect (Atkinson & Nevill, 1998). Participants took a 2-min rest between each typing session to walk around the laboratory.
Photographic data on typing performance were analyzed using a bespoke program within MATLAB software, which has demonstrated excellent intra- and interrater reliability (Jones et al., 2011). This software allows lines to be drawn on still images between anatomical landmarks marked by markers and determines the angles between these lines.
Data Analysis
Normality of the data was examined before analysis. Dependent t tests were used to compare differences within the angles’ means. Significance level was set at a level of .05.
Results
Unlike the desktop, maximum NA positions were noted with the laptop, causing the highest forward head position, with a 9.11° difference between the two computers. HT had a similar result, with a difference of about 8°. Both computers resulted in a negative value in both LA and PT for the majority of participants (Table 2).
Means and Differences in Posture Angles Between Laptop and Desktop
Note. HT = head tilt; LA = lumbar angle; NA = neck angle; PT = pelvic tilt. Negative values denote either lumbar lordosis or posterior PT.
Forward lumbar kyphosis was revealed with the laptop, with a –2° difference compared with the desktop. In contrast, the greatest negative PT was found with the desktop, with roughly 50% more than the laptop. A single outlier for NA during laptop use and for HT during desktop use was found for a female participant, who was also the shortest participant (Figure 2).
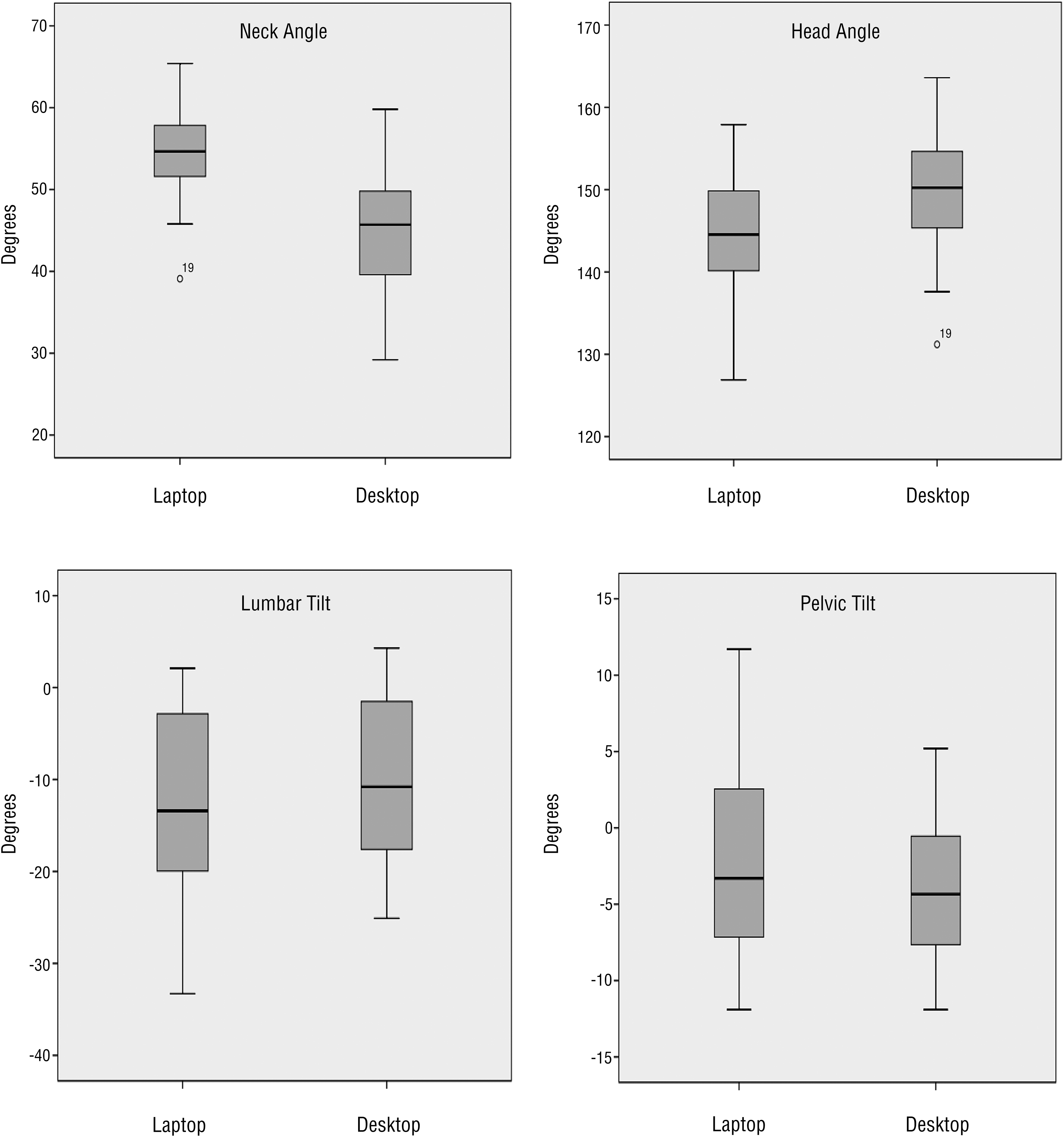
The data showed a significant difference in the mean NAs, t(19) = 8.93, p < .0005. These angles were significantly higher for the laptop task (mean [M] = 54.1°, standard deviation [SD] = 5.8) than for the desktop task (M = 45.35°, SD = 7.37). Similarly, the mean HT angles were significantly different, t(19) = −6.33, p < .0005, with the mean angles significantly lower for the laptop task (M = 144.27°, SD = 7.96) than for the desktop task (M = 149.81°, SD = 8.42).
Both LA, t(19) = −2.6, p ≤ .018, and PT, t(19) = 2.57, p ≤ .019, showed significant differences. The mean LAs were significantly higher for the laptop task (M = –11.84°, SD = 10.35) than for the desktop task (M = –9.8°, SD = 8.98), whereas mean posterior PT angles were significantly higher for the desktop task (M = –4.27°, SD = 4.76) than for the laptop task (M = –2.85°, SD = 5.96).
Discussion
This study demonstrated that significant differences exist in NA, HT, LA, and PT between the two computers. Similar findings were reported by Straker et al. (1997) and Saito et al. (1997) during a typing task on both devices. However, the descriptive figures are not relative to some extent. For example, variances in NAs and HTs were 6.6° and 8.1°, respectively, in Straker et al., whereas in the current study, they were 9.11° and 7.53°. Moreover, NA was 3.8° and HT was –16.4° in Saito et al. The lower value for NA in Straker et al. could be explained by the use of a manual calculation method, with deviations measured from a vertical reference mark, which reduced the reliability level compared with a ground reference for body segments (Dunk, Lalonde, & Callaghan, 2005). Moreover, the great difference in Saito et al. cannot be clarified because of the uncertainty of the measurement tool and because markers were used for the neck and head position. In contrast, Seghers et al. (2003) have reported a nonsignificant difference in NAs and HTs during both typing tasks. However, their study used a separate keyboard for the laptop, which might have reduced the internal validity of using the laptop’s own keyboard.
These variances in postural results may be related to the variation in design between the laptop and the desktop. For example, the laptop screen is likely to cause pulling of the head and neck downward and forward, and the upright posture in this study’s procedures could be an additional factor that exaggerates the position in the laptop task because of the position of the screen. Thus, an increase in the upper cervical (C1–C4) curvature and a decrease in the lower cervical curvature (C5–T1) could be a problematic consequence (Cho et al., 2008).
Extreme NA combined with the head tilted forward plays a major role in the load on cervical segment tissue, perhaps resulting in the development of MSD or MSS (Gerr et al., 2006). Loads affect not only the neck segment but also other structures, such as the first and second rib elevation; upper thoracic kyphosis alteration; and the scapulae elevation, protraction, and downward rotation (Malińska & Bugajska, 2010; Marcus et al., 2002). Forward HT increases the pulling forces on the spine, particularly the posterior part of the thoracic region because it works as a stabilizer (Moore, 2004). The cervicothoracic junction’s mechanism is therefore affected because these extremely limited (thoracic) and kinetic (cervical) segments are linked (Keller et al., 1998). Gill and Callaghan (1998) also reported that a secondary symptom may occur from abnormal proprioception in injured and irritated joints. Similar to the outcome of Annetts et al. (2012), a positive pattern has been recognized between both segment angles, that is, as the NA increased, the HT posture increased as well. This pattern could work to balance the head posture alongside the gaze at the VDU by maintaining the direction of the eyes for reading the screen.
The differences between LA and PT for the laptop and desktop may indicate lumbar lordosis and posterior PT, except for a single value in LA and two values in PT. One male participant’s LA may indicate a congenital deformity, and a female participant’s positive PT may be a result of gender posture differences because of the different pelvis shape, which requires further research (Dunk & Callaghan, 2005). To our knowledge, no reported studies have examined the differences in LA and PT between laptop and desktop use when participants sit upright while performing a typing task.
The laptop task had more influence on extreme lordosis, which possibly results from less posterior pelvic rotation. Unlike LA, PT was found to be high with desktop use; the angle differences were –2° for both the lumbar vertebrae and the pelvis, probably as a result of biomechanical considerations. A larger lordotic LA would probably be the result of smaller posterior PT, as supported by others (Annetts et al., 2012; Straker et al., 1997). Although upright sitting is usually characterized by less posterior PT and more lumbar lordosis, the large negative PT values during the desktop task may have been caused by use of a chair without a backrest. Additionally, viewing the desktop’s higher display may encourage erect head posture, perhaps combined with pushing the trunk backward. An explanation for the laptop’s influence on the lumbopelvic region may be its design (i.e., sharp viewing angle, low height, and close screen position). This design probably results in pulling the lumbar spine forward in an attempt to sit upright, thereby causing the vertebrae to draw toward each other.
Slight posterior PT during the laptop task could be the result of control by the iliopsoas as a hip flexor and erector spinae muscles as back extensors (Williams et al., 1991). O’Sullivan et al. (2006) reported that boosting paraspinal muscle activity results from reducing the posterior PT and increasing lumbar lordosis, perhaps leading to spinal shrinkage (i.e., reduced vertebral space); therefore, discomfort could result from sustained compression on the discs (Kingma, van Dieën, Nicolay, Maat, & Weinans, 2000). Hence, the laptop session was associated with more lordosis, which could possibly be a source of potential injury.
O’Sullivan et al. (2002) explained that sitting in a slumped posture for a long time could reduce muscle efficiency and weaken the lumbopelvic region, resulting in instability and strain caused by an increase in the load on the intervertebral disc and ligaments (Cholewicki & McGill, 1996; Goel et al., 1993). Thus, applying the correct working posture could be proposed to inform postural reeducation during clinical visits and training programs on computer work.
Because the data are statistically significant, clarifying the overall pattern for NA, HT, LA, and PT through the cervical and lumbopelvic segments is helpful. Black et al. (1996) maintained that a converse trend is noted between cervical and lumbar segments during sitting, in either a slumped or an upright position. Upright posture is characterized by cervical flexion, and the opposite is true for slumped posture; however, Black et al. (1996) reported this without alteration in the HT. Therefore, our study lends support to Black et al. (1996) except for HT posture.
The ideal posture for both lumbopelvic and cervical segments is not usually the same (Annetts et al., 2012). However, the opposite may be true. In other words, awkward lumbopelvic posture could be the result of awkward cervical posture, resulting in spinal misalignment (Gandavadi et al., 2007; Straker et al., 2009).
Limitations and Future Research
This study was carried out on healthy students between ages 25 and 35 yr; therefore, the results may not be applicable for older or younger populations. Because this is a pilot study on healthy people, it does not apply to people at risk for musculoskeletal injuries. Therefore, further research is necessary to understand the role of spinal angles for those who may be at risk for such injuries as a result of their work environment.
Implications for Occupational Therapy Practice
The findings of this study have several implications for occupational therapy practice, both ergonomically and clinically:
The design of ergonomic rules that support healthy body posture can make computer workstations safer by reducing biomechanical risks.
Practitioners can educate clients about how to effectively use computer workstations to avoid the risk of MSD associated with poor workstation design.
Because frequent laptop users are subject to injury caused by poor posture, practitioners can provide training on proper posture and preventive programs that can enhance computer users’ health.
Practitioners can advise frequent laptop users to use a docking station or an external VDU, keyboard, and mouse to create good workstation design.
Conclusion
Our findings reveal that the use of laptops may lead to postural restrictions and dysfunction. They also demonstrate ideal posture regarding neck flexion, forward head lean, and lumbar lordosis accompanying desktop use. Therefore, the desktop is good for maintaining proper posture, whereas the laptop is less ideal. In the case of workers who use laptops, using them less often than using a desktop computer is recommended. These findings also suggest converse trends between cervical and lumbar segments. This study supports the link between the cervical and lumbopelvic regions, either within upper and lower body segments or between them, which seems to be safer while working on a desktop. Laptop and desktop users should pay attention to this association, because it seems to influence poor posture. Thus, a proper evaluation of the workstation, which depends on individual anthropometry, besides appropriate postural instructions, is necessary.
Footnotes
Acknowledgments
The authors are thankful to the Deanship of Scientific Research, College of Nursing Research Center at King Saud University, for funding this research.