
Abstract
Keywords
An estimated 1.7 million people sustain a traumatic brain injury (TBI) each year. Of these, about 50,000 die, constituting about one-third of the injury-related deaths in the United States (Centers for Disease Control and Prevention [CDC], 2014). TBI has been referred to as a “silent epidemic” because its complications, such as changes in emotion, thinking, language, or sensation, are not readily apparent (Faul, Xu, Wald, & Coronado, 2010).
The most severe TBI causes profound disturbances of consciousness. About 17% of people who survive TBI have a period of complete unconsciousness or coma with no awareness of themselves or their surroundings (Whyte et al., 2013). As people recover from TBI, they usually pass through various phases of recovery, and recovery can stop at any one of these phases. Transition between stages is usually very gradual and highly idiosyncratic, depending on factors such as the type and location of injury, past medical history, age, and access and response to treatment (Masel & DeWitt, 2014). The long-term effects of a severe TBI can affect all aspects of a person’s life, including the ability to participate in activities of daily living (CDC, 2014).
The Glasgow Coma Scale (GCS) is the most frequently used measure to determine severity of TBI within 48 hr of injury (Steiner, 2015). Lower GCS scores indicate more severe brain injury. Coma results from a disturbance in the function either of the brainstem reticular activating system (RAS) above the mid pons or of both cerebral hemispheres (Greenberg, Aminoff, & Simon, 2012). People in a coma are unaware and unresponsive but not asleep; there is no sleep–wake cycle. While in a coma, people are unable to speak, follow commands, or open their eyes. They may have a simple reflex in response to touch or pain, but essentially they show no meaningful response to external stimuli. Awareness of self and the environment is absent, even with vigorous external stimulation. Coma can last from hours to days, depending on the severity of the brain damage, and some people remain in a comatose state for months or even years (White & Giacino, 2013). A person in a coma may experience some improvement and transition to a vegetative state, in which more lower brain functions (e.g., sleep cycles, heart rate regulation) and some upper brain functions (e.g., eye opening, sound production) are present (White & Giacino, 2013).
Environmental (i.e., sensory) deprivation can slow recovery and development of central nervous function, further depressing the threshold of activation of the RAS (Li et al., 2014). Some studies have suggested a correlation between coma duration and overall recovery, hypothesizing that the degree to which the RAS remains depressed is a predictor of post-TBI functional recovery (Duff, 2001; Hendricks, Geurts, van Ginneken, Heeren, & Vos, 2007). Arousal is a prerequisite for the selective attention necessary to recognize and process information. A growing body of knowledge suggests that recovery processes in TBI are activated immediately after injury (Duff, 2001; Lannin, Cusick, McLachlan, & Allaous, 2013). One such recovery process, plasticity, allows the brain to modify its organization and function (DeFina et al., 2009). Enhancement of plasticity is known to occur through both endogenous factors, such as release of nerve growth factor, and exogenous factors, such as environmental or sensory stimulation.
Sensory stimulation programs, which provide controlled exposure to environmental or sensory-specific stimuli, vary on the basis of the senses being targeted. Different procedures may be adopted, but the method typically includes presentation of stimuli that are simple, frequent, and repetitive, possibly with autobiographical and emotional content. Moreover, stimuli are typically administered through multiple sensory channels and with a moderate to high intensity (Abbate, Trimarchi, Basile, Mazzucchi, & Devalle, 2014). Various configurations of sound, including familiar and unfamiliar voices, music, and environmental voices, have been studied in relation to their effect on intracranial pressure and cerebral perfusion pressure (Cremer et al., 2005). Multimodal stimulation (e.g., auditory and tactile, tactile and gustatory) has been studied in relation to wake cycles, purposeful movement, and alertness (Lombardi, Taricco, De Tanti, Telaro, & Liberati, 2002).
It has long been theorized that regulated sensory stimulation may promote positive outcomes but that people exposed to an undifferentiated bombardment of sensory information may lose the ability to process information because of habituation (Wood, Winkowski, Miller, Tierney, & Goldman, 1992). Occupational therapy practitioners, who are knowledgeable about the principles of sensory regulation, can provide the controlled sensory stimulation that may meet the higher threshold of reticular neurons and thus increase cortical activity (Lannin et al., 2013). The purpose of this systematic review was, therefore, to answer the question, “What is the evidence for the effectiveness of sensory stimulation to improve arousal and alertness of people in a coma or persistent vegetative state after TBI?” to provide guidance for therapeutic programming.
Method
This systematic review is one of six reviews of the TBI literature relevant to occupational therapy conducted under the auspices of the American Occupational Therapy Association (AOTA) Evidence-Based Practice (EBP) Project. The six review questions were based on the earlier set of reviews that covered the literature from 1986 to 2008 (Golisz, 2009) and were updated to reflect present clinical practice. An advisory board consisting of experts in the field and the review authors provided feedback on the development of the questions. The reviews were carried out through academic partnerships with the review team for each question. The methods for the reviews were specified in advance and documented in a protocol for the authors.
Search Strategy
The inclusion criteria for this review were as follows: Studies were published in peer-reviewed scientific literature between 2008 and 2013, 50% of participants in the study sample were adults with TBI, articles were written in English, and interventions were within the scope of practice of occupational therapy. One article published in 2003 was included because although it had not been incorporated in any of the systematic reviews included in this review, it offered information pertinent to answering the focus question. Using the evidence hierarchy described by Sackett, Rosenberg, Muir Gray, Haynes, and Richardson (1996), descriptive outcome studies such as single-subject and case series designs (Level IV evidence) and case reports, narrative literature reviews, and consensus statements (Level V evidence) were included only when Level I (systematic reviews, meta-analyses, randomized controlled trials [RCTs]), Level II (two-group nonrandomized studies), or Level III (one-group nonrandomized studies) evidence was not found. The reviews excluded qualitative studies and reports from presentations, conference proceedings, non–peer-reviewed research literature, dissertations, and theses.
The methodology consultant to the EBP Project and AOTA staff identified the search terms in consultation with the review authors and the advisory group, with the terms selected in keeping with the specific thesaurus of each database included in the search. A medical research librarian with experience in completing systematic review searches further refined the search strategies and conducted all searches. The databases and sites that were searched included Medline, PsycINFO, CINAHL, OTseeker, and the Cochrane Database of Systematic Reviews. The review teams examined reference lists from articles that were identified for inclusion for additional potential articles and hand searched selected journals to ensure that all appropriate articles were included. See Supplemental Appendix 1 for one of the electronic search strategies for this question (available online at http://otjournal.net; navigate to this article, and click on “Supplemental”).
Study Selection, Data Extraction, and Risk of Bias Assessment
The EBP Project methodology consultant first eliminated references for each question on the basis of citations and abstracts. The review team (the authors) eliminated additional references on the basis of citations and review of the abstracts. We retrieved the full-text versions of the articles and reviewed them for relevance to the question, study quality, and level of evidence. Each included article was abstracted using an evidence table that included the level of evidence, a summary of the study methods, and findings relevant to the review question. Supplemental Table 1 summarizes the characteristics of included studies (available online at http://otjournal.net; navigate to this article, and click on “Supplemental”). AOTA staff and the EBP Project consultant reviewed the evidence tables to ensure quality control before we undertook more in-depth review and summarization.
We assessed the risk of bias of individual studies using the methods described by Higgins, Altman, and Sterne (2011) and of the systematic review using the measurement tool developed by Shea et al. (2007). The first author completed the risk of bias table, and the second author reviewed it. Discrepancies were discussed until consensus was achieved. Supplemental Tables 2 and 3 (also available online) summarize the risk of bias for each study.
Data Synthesis
Given the heterogeneity of the included studies, we used a qualitative approach to data synthesis. We examined the studies selected for review for similarities across participants, settings, interventions, and outcomes and grouped related studies into themes. The strength of the evidence for each theme was adapted from the system proposed by the Agency for Healthcare Research and Quality, U.S. Preventive Services Task Force (2012). The designation of strong evidence indicates consistent results from at least 2 RCTs. A designation of moderate evidence is made on the basis of 1 RCT or 2 or more studies with lower levels of evidence. The designation of limited evidence is based on few studies, flaws in available studies, or some inconsistency in the findings across individual studies. A designation of mixed evidence indicates that the findings were inconsistent across studies in a given category. Finally, a designation of insufficient evidence is used when the number and quality of studies were too limited to make any clear classification. Risk of bias appraisals were considered in strength of evidence designations.
Results
Nine studies in total were reviewed, of which 3 were Level I, 1 was Level II, 4 were Level III, and 1 was Level IV (Figure 1). The Level IV study was reviewed because it argued for the use of median nerve stimulation (MNS) as part of a sensory program, and no other studies addressed this type of sensory stimulation. These studies addressed three themes: unimodal stimulation, multimodal stimulation, and nerve stimulation. All studies used the GCS as either a primary or a secondary outcome measure.
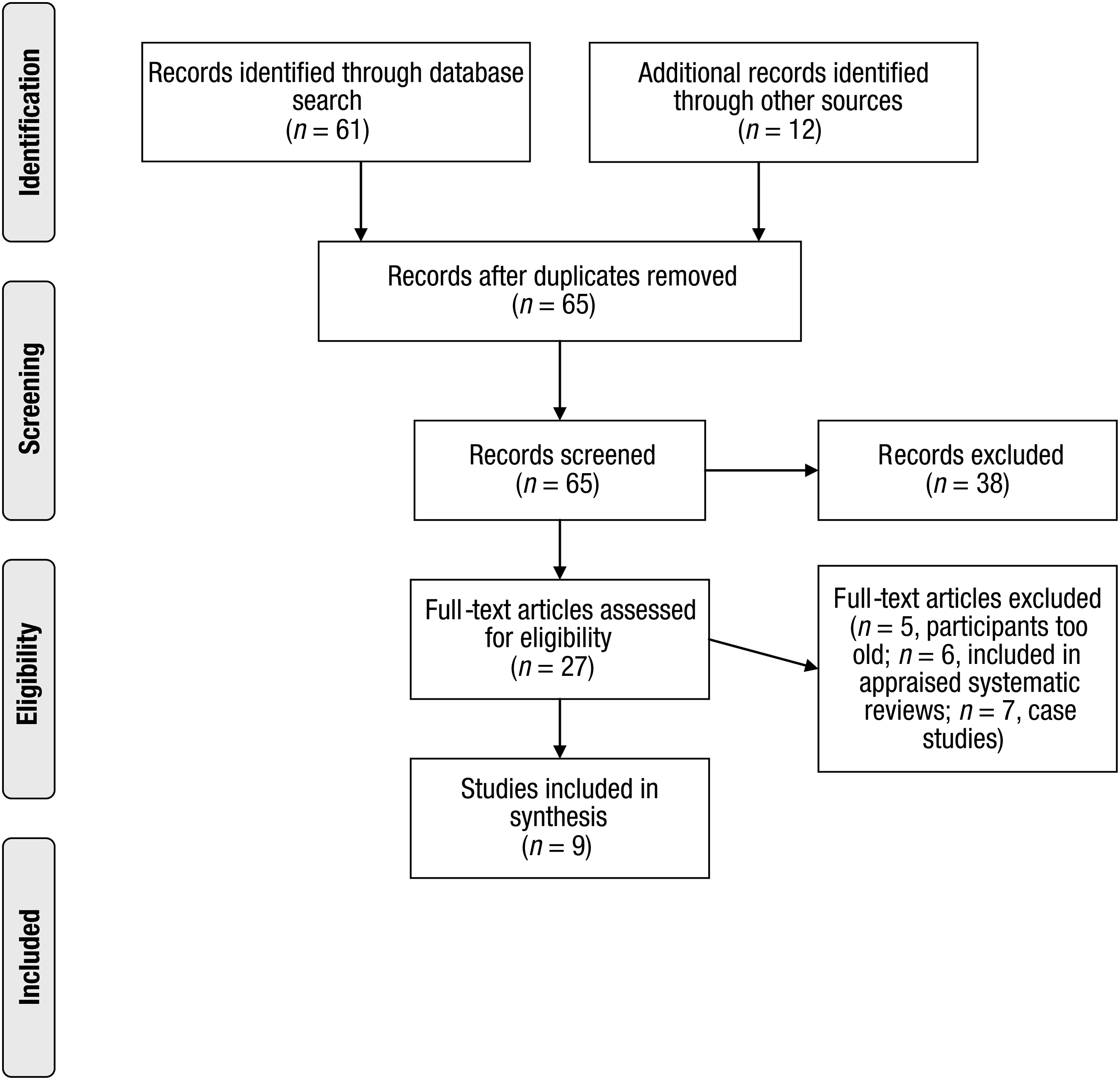
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram of published literature search.
Unimodal Stimulation
Unimodal interventions include stimulation through any one of the five senses. A typical approach involves the stimulation of several sensory modalities, with each sense stimulated one by one in a standard session (Abbate et al., 2014).
Auditory stimulation has received the greatest research attention. Cheng et al. (2013, Level III) tested localization of auditory stimulation (i.e., head or eye movement toward the sound) and response to a ringing bell and use of patient’s name. Use of patient’s own name was more successful in eliciting a response than was a neutral sound such as a bell, and persons in a vegetative state were significantly more likely to localize to sound than those in a coma. No significant change in GCS outcome occurred during the study, likely because of its short duration.
In a Level I systematic review, Meyer et al. (2010) appraised eight reports on sensory stimulation and several other studies related to pharmacological and electrical interventions to promote emergence from coma. Only 1 of the sensory stimulation studies was an RCT. Although the authors indicated that some of the reviewed studies were of unimodal interventions, they did not specify how many or which senses were stimulated. They concluded that the evidence provided by the studies on auditory stimulation was conflicting. Although the studies reported improvements on a variety of physiological measures, they did not report on the primary outcome of posttreatment GCS score. The authors were unable to reach any conclusions on the findings of the other studies because of their methodological heterogeneity.
Multimodal Stimulation
Several studies suggest that attention tends to orient more easily toward sensory inputs that possess multisensory properties. Brain cortical processing is multisensory to begin with in primary and associative cortices; therefore, multisensory stimulation might better engage people’s preserved islands of higher order cortical functioning (Abbate et al., 2014).
Meyer et al.’s (2010) Level I systematic review included one before-and-after study on music therapy with people in a persistent vegetative state that was a side study of a bromocriptine and levadopa/carbidopa clinical trial. Patients were treated with vertical motions on a trampoline (two attendants supported them in sitting position) three times each day for 7 min while they listened to live music in synchrony with the movement. The authors concluded that music alone did not improve level of consciousness but that music paired with the motion of the trampoline to provide multimodal stimulation did increase awareness. The intervention was found to be most effective when initiated within 6 mo of injury and appeared to enhance clinical outcomes in trials of bromocriptine and levadopa/carbidopa. The authors noted that a limitation of this study may be the impracticality of this treatment.
Several other studies tested the effect of a combination of auditory and tactile stimulation on consciousness level. In a Level I study, Abbasi, Mohammadi, and Sheaykh Rezayi (2009) incorporated a specific auditory and tactile stimulation routine in a family visiting program (i.e., greeting the patient by name, sitting in a chair by the head of the bed, using normal intonation in conversations, holding the patient’s hands gently, and softly touching the patient’s face in short intervals). Megha, Harpreet, and Nayeem (2013; Level I) and Urbenjaphol, Jitpanya, and Khaoropthum (2009; Level II) tested multimodal intervention at various intensities. Although the authors of these studies did not describe the stimulation protocols in detail, they concluded that the stimulation of all five sensory systems through at least two daily sessions 5 days/wk and for a minimum of 2 wk increased participants’ level of consciousness as measured by the GCS.
Similarly, 4 Level III studies (Cheng et al., 2013; Di Stefano, Cortesi, Masotti, Simoncini, & Piperno, 2012; Noé et al., 2012; Oh & Seo, 2003) tested various combinations of familiar sensory stimuli and concluded that multimodal sensory stimulation was more effective in increasing consciousness of patients in a minimally conscious state (i.e., those who can follow simple commands inconsistently and have some gestural responses and purposeful behaviors) than in people in a coma or vegetative state. Although the results were mixed in terms of effect size, combinations of familiar tactile, olfactory, and gustatory stimulations yielded generally positive results.
All studies found that frequent repetition of multimodal stimulation in the initial stages after injury was efficacious in increasing level of consciousness, especially if stimuli were associated with the person’s past experiences and preferences. Although noticeable changes were documented after 6 days, significant increases in consciousness were evident after 2 wk (Oh & Seo, 2003), and repetitive stimulation for a longer period provided more sustained results (Abbasi et al., 2009; Cheng et al., 2013; Megha et al., 2013; Meyer et al., 2010; Noé et al., 2012; Urbenjaphol et al., 2009). Behavioral response to multimodal stimulation also depended on the complexity of stimuli rather than intensity alone (Di Stefano et al., 2012; Noé et al., 2012), and active responses decreased during recession periods during which only ordinary medical care was provided (Oh & Seo, 2003). Significant changes in attention and cognition in these studies appeared between 6 and 14 days after initiation of intervention in dosages that ranged from 7 to 20 min for 3–5 sessions per day.
Median Nerve Stimulation
Neuropharmacological therapies are commonly prescribed for people with disorders of consciousness under the premise that improvements in dopaminergic and noradrenergic neurotransmitter systems can enhance arousal and behavioral responsiveness (Giacino et al., 2012). Electrical stimulation is a common therapeutic approach used in rehabilitation of a variety of neurological conditions. The median nerve supplies the sense of feeling in the first four fingers of the hand and innervates the thenar muscles. The median nerve is also an important component of the somatosensory system. Because the hand exhibits disproportionately large cortical representation, it is thought that MNS mimics the brain activity that occurs during movement or even when a person contemplates moving his or her hand. This brain activity, in turn, is thought to elevate dopamine levels, which stimulates the RAS to maintain wakefulness (Cooper & Cooper, 2003).
Meyer et al. (2010) and DeFina et al. (2010) found that it was not possible to isolate the effect of tactile and other sensory stimulation during MNS. Three studies on MNS met the inclusion criteria for Meyer et al.’s systematic review. The studies had set out to measure changes in cerebral perfusion and dopamine levels as they related to level of consciousness. However, the researchers noticed that participants appeared to attempt to localize the percutaneous stimulus by redirecting their gaze toward it or seeking to touch it with the opposite hand. Because this finding was not an intended primary measure of the studies, no statistical analysis of changes in attention and cognition was performed, but the possible effect suggests the need for future studies in this direction.
DeFina et al. (2010) included MNS in their Advanced Care Protocol, which they provided to people with TBI. This protocol included other interventions in addition to MNS, such as traditional therapies (occupational, physical, and speech) and pharmaceuticals. They documented clinical improvement in all the participants but were unable to isolate the effect of MNS. The authors of both reports concluded that although MNS showed some promise and no negative side effects, the evidence was conflicting as to whether this type of stimulation results in significant coma arousal after TBI and that further research is warranted (DeFina et al., 2010; Meyer et al., 2010).
Discussion
Occupational therapy recognizes sensory events as embedded in the experience of being human. Therefore, sensory processing has been of interest throughout the evolution of the profession (Dunn, 2001). Practitioners construct sensory intervention options on the basis of what is respectful of and compatible with the person’s past life experience. Results of the studies included in this review suggest diverse levels of certainty regarding the effectiveness of sensory stimulation to improve arousal and alertness in people in a coma or persistent vegetative state. As a whole, these studies provide strong evidence that multimodal sensory stimulation improves arousal and enhances clinical outcomes; moderate evidence that auditory stimulation, especially in the form of a familiar voice, increases arousal in the short term; limited evidence that the complexity of stimuli is more important than the intensity; and insufficient evidence for MNS as an intervention that contributes to RAS arousal. These results have several implications for practice, education, and research.
Implications for Occupational Therapy Practice
Multimodal sensory stimulation directed at improving arousal and enhancing clinical outcomes for people in a coma or persistent vegetative state should be tailored to patient tolerance and premorbid preferences. Bimodal (i.e., auditory and tactile) or multimodal (i.e., all five senses) strategies are most likely to have an effect on attention and cognition. Such stimulation should begin early, be frequent (i.e., 3–5 times/day for 20-min sessions), and be sustained until more complex activity is possible, with changes likely within 2 wk.
The effectiveness of auditory stimulation, especially in the form of a familiar voice, is greater for people who are closer to being in a minimally conscious state. The content of the auditory stimulation should be self-referential and provided by people with a voice familiar to the client (i.e., family members) and with whom the client has a preexisting emotional bond. Multimodal stimulation paired with action initiation cues, for example, may improve level of consciousness and environmental awareness, such as tracking or localizing a stimulus. MNS is not recommended for coma stimulation until more research clarifies its utility.
Implications for Occupational Therapy Education
Educational programs for occupational therapy practitioners should ensure that students understand the various systems for determining the severity of TBI, especially the GCS, which is the most widely used system. In addition, familiarity with multiple forms of sensory stimulation and strategies to grade the complexity of such stimulation should be part of entry-level curricula. Students should be familiar with concepts of gradation of intervention to help clients avoid developing sensory deprivation because of insufficient stimulation or habituation caused by undifferentiated bombardment with sensory information. Environmental adaptation strategies should also be part of students’ education regarding this population.
Implications for Occupational Therapy Research
Further research is needed to better determine the dosage of stimulation and the impact of sensory stimulation on long-term functional outcomes for people in a coma or persistent vegetative state. Larger sample sizes with randomized allocation to intervention will permit further analysis of the impact of the intervention.
Limitations
The appraised studies have limitations that must be considered when evaluating the evidence. Many studies had a small sample and short intervention period with no long-term follow-up. In addition, incomplete description of procedures suggests heterogeneity in intervention, limiting the ability to compare studies.
Conclusion
Sensory stimulation for people in a coma or persistent vegetative state can take many forms, as suggested by the studies reviewed. Unimodal stimulation, multimodal stimulation, and median nerve stimulation were all explored, with mixed findings in regard to effectiveness in increasing awareness and arousal. The strongest evidence was in support of multimodal stimulation, with some promise for other types of sensory stimulation as well. MNS is not recommended at present as an intervention to increase arousal. Additional studies are warranted to provide more definitive results because of the many limitations present in the current research.
Supplemental Material
Supplementary material for Effectiveness of Sensory Stimulation to Improve Arousal and Alertness of People in a Coma or Persistent Vegetative State After Traumatic Brain Injury: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2016.021022.pdf for Effectiveness of Sensory Stimulation to Improve Arousal and Alertness of People in a Coma or Persistent Vegetative State After Traumatic Brain Injury: A Systematic Review by René Padilla and Anna Domina in The American Journal of Occupational Therapy
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.