
Abstract
Occupational therapy practitioners enable clients to improve performance in everyday occupations. As health care reform precipitates changes across health care service organizations, occupational therapy professionals must seize the opportunity to apply their unique skills and perspective to meet the changing needs of clients and other stakeholders. In this article, we explore the role and distinct value of occupational therapy practitioners in one area of changing need: medication management. We find that occupational therapy practitioners have unique skills that complement the factors affecting medication nonadherence and evidence-based interventions. With reforms to research, teaching, and practice, occupational therapy practitioners can better integrate medication management into regular evaluation and treatment, thereby contributing to broader patient outcomes defined by the Affordable Care Act.
In 2010, Congress passed the Patient Protection and Affordable Care Act (ACA; Pub. L. 111–148). The ACA shifted the focus of health care from healing the sick to the “Triple Aim” of improving health experiences, promoting population health, and reducing the cost of care (Berwick, Nolan, & Whittington, 2008). The ACA provides occupational therapy practitioners with many opportunities, including allowing the profession to broaden its scope of influence. However, occupational therapy policy experts warn that there are also risks. For example, occupational therapy may not be seen as a part of health care reform and therefore may not be fully integrated into future systems of care (Fisher & Friesema, 2013; Leland, Crum, Phipps, Roberts, & Gage, 2015). Subsequently, policy experts call on occupational therapy professionals to better describe the profession’s distinct value and contributions to broader patient outcomes.
In this article, we provide a response to the experts by exploring the role of occupational therapy in medication management. Through this process, we seek to accomplish three goals: (1) define medication management and understand its importance within the scope of health care reform, (2) describe the distinct value of occupational therapy within the context of medication management, and (3) understand the changes needed to help the profession reach full potential as a service provider in this area. Through this discussion, we seek to inform stakeholders and occupational therapy practitioners to improve provision of medication management services.
Defining Medication Management
Medication management is an interprofessional issue that includes prescribers, nurses, pharmacists, occupational therapy practitioners, and related technicians and assistants. Each profession has essential and irreplaceable duties as well as an individualized definition of medication management (Bluml, 2005). In this article, we discuss medication management as it relates to occupational therapy practitioners.
Within occupational therapy, medication management refers to the daily systems and processes of taking medications as prescribed (American Occupational Therapy Association, 2017; Sanders & Van Oss, 2013). A brief activity analysis reveals that to manage one medication, a client must negotiate with the physician for a prescription, fill the prescription at the pharmacy, interpret complicated health information, take the medication on a daily basis, and refill the prescription in a timely manner. Occupational therapy practitioners cannot prescribe medications or alter the medical advice from a physician or pharmacist, but they can help clients better navigate many of the tasks associated with medication management.
Medication adherence is defined as “the extent to which a person’s behavior—taking medication … corresponds with the agreed recommendations from a healthcare provider” (World Health Organization [WHO], 2003, p. 2). Medication adherence is often described as a percentage, indicating the ratio of pills consumed over those prescribed. An adherence rate of 100% indicates perfect adherence, with higher numbers indicating overdosing and lower numbers indicating underdosing. The goal of medication management intervention is to help clients attain perfect (or near perfect) medication adherence.
Occupational Therapy’s Distinct Value in Medication Management
As demonstrated by the activity analysis, clients’ medication adherence is related to their ability to manage their daily medications. Occupational therapy practitioners have a specialized skill set that prepares them to address the occupational performance of this instrumental activity of daily living.
Intervention
Unique skills enable occupational therapy practitioners to implement quality evidence-based medication management interventions. To define these unique skills, we compared the skills of practitioners on the medication team. We analyzed data from the Occupational Information Network (O*NET), a federal database of standardized job descriptions (https://www.onetonline.org/).
The O*NET database provides an objective way to compare job skills. O*NET researchers identified 35 skills inherent across jobs. For each job, occupational analysts familiarize themselves with the position’s requirements. They then rate the importance of each of the 35 skills on a scale from 0 to 100, with 100 indicating very important. The use of trained occupational analysts strengthens the O*NET data, because it instills reliability across data points and prevents professionals from inflating their own job ratings to influence policy decisions.
For this analysis, we compared occupational therapist O*NET skills ratings to the ratings of three professionals typically involved in medication management: general internist physicians, registered nurses, and pharmacists. We calculated the average importance of each of the 35 job skills for the three professions historically on the medication management team. We then compared the skills ratings for occupational therapists with the average ratings of the other professions (Table 1).
Job Skill Comparison of Occupational Therapists to Professionals Historically on the Medication Team
Note. M = mean scores of MD, RN, and Pharm; MD = internist physician; OT = occupational therapist; Pharm = pharmacist; RN = registered nurse; SD = standard deviation. Three job skills (not listed)—installation, equipment maintenance, and repairing—were rated as 0 for all four health professionals.
Standard deviations between OTs and other professionals: – = 1 SD below; – – = 2 SDs below; + = 1 SD above; ++ = 2 SDs above; no symbol = within 1 SD .
Generally, occupational therapists had similar skills as the other professionals. In 25 of the job skills (71%), occupational therapists were rated within 1 standard deviation of professionals typically involved in medication adherence. Occupational therapists did score 1 standard deviation below the other professionals in science (scientific problem solving) and 2 standard deviations below in mathematics and quality control analysis. Occupational therapists had higher ratings in seven categories. They were 1 standard deviation higher in operations analysis (analyzing needs and creating a plan to meet needs), service orientation (helping people), and time management and 2 standard deviations higher in learning strategies (selecting the best educational training methods), monitoring, persuasion, and technology design.
Although prescribing medications relies heavily on knowledge of math and science, interventions for medication adherence are often behavioral. Evidence-based medication adherence interventions include developing good provider–patient interactions, education, behavior change techniques, training in self-monitoring, incorporating medications into daily schedules, and assistive technology (Nieuwlaat et al., 2014; Schaffer & Yoon, 2001; Zullig, Peterson, & Bosworth, 2013). This analysis revealed that compared with the other professions, occupational therapists’ skills best complement the evidence-based intervention approaches needed to support clients’ medication adherence.
Remediating Impairments
Occupational therapy skills not only complement evidence-based adherence interventions but also can address many of the factors that affect nonadherence. For example, Williams et al. (1995) found that 42% of low-income hospital patients could not understand the labels on their prescription bottles. Occupational therapy practitioners can implement health literacy interventions to improve clients’ capacity to decode complicated health information, adapt the health literacy environment by making materials easier to understand, and support other team members in creating quality patient education experiences (Smith & Gutman, 2011).
Occupational therapy practitioners can also address medication adherence in people with good health literacy who struggle with other components. For example, people fail to take their medication as prescribed for either intentional or unintentional reasons. Gadkari and McHorney’s (2012) survey of more than 24,000 adults with chronic health conditions found that few people intentionally neglect their medications. The survey indicated that only about 30% of people attribute their nonadherence to intentional reasons. Eighteen percent of participants reported skipping medications to make them last longer, and 14% indicated altering the dose of a medication to suit their own needs. Conversely, 70% of survey participants attributed their nonadherence to unintentional factors. Specifically, participants reported forgetting (62%), running out of medications (37%), or simply being careless (23%).
Although many people report forgetting their medications, people forget for different reasons. For example, as the number of daily doses, number of prescribing physicians, or complexity of medication instructions increases, the client is more likely to forget a dose (Coleman et al., 2012; Marek & Antle, 2008). Researchers have identified several factors that affect medication adherence (Figure 1; Gadkari & McHorney, 2012; Vlasnik, Aliotta, & DeLor, 2005; WHO, 2003). Analysis of adherence barriers reveals that occupational dysfunction in medication management is likely due to a complex interaction of factors among the person, the environment, and the task.
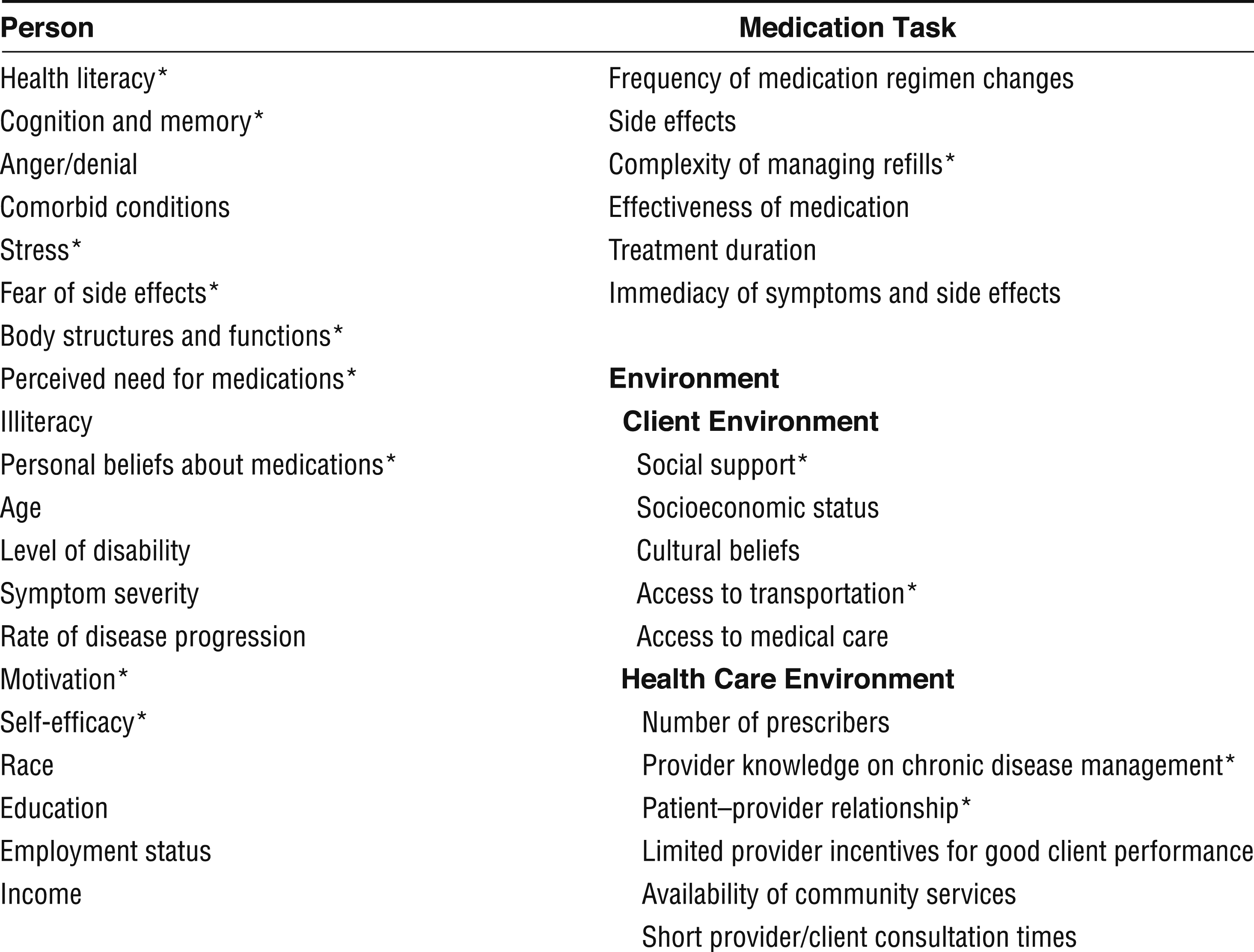
Factors that affect medication adherence.
To further complicate matters, each person experiences an inimitable set of barriers to medication adherence. Each client has a particular set of health conditions that affects his or her ability to manage medications. For example, arthritis may create barriers in manipulating containers, whereas dementia can impair cognitive aspects of the task. Each client also takes an exclusive set of medications based on his or her symptoms, health insurance, and prescribers’ preferences. Finally, each client experiences different barriers and supports related to his or her environment, previous experiences, and beliefs. Although there are common themes in medication nonadherence, infinite combinations of health conditions, medications, and individual experiences influence nonadherence, meaning that each person’s nonadherence is caused by a unique set of barriers.
Research reveals that almost no one fails to take medication with the intent to cause harm. Instead, people are overcome by a series of multidimensional individualized barriers. Many of the factors that affect medication adherence are responsive to occupational therapy intervention (Figure 1). Occupational therapy practitioners can help clients overcome medication adherence barriers by creating a client-centered plan that includes developing cues, prescribing assistive technology, or altering the environment (Sanders & Van Oss, 2013). Occupational therapy practitioners have the skills to address the most common causes of medication nonadherence. The Appendix describes a case study that demonstrates the potential of occupational therapy services in medication management.
Current Practice
Although occupational therapy practitioners have the skills to address medication management impairments and implement evidenced-based interventions, few occupational therapy professionals seem to be incorporating medication adherence into research, teaching, or practice. For research, a search for the term medication in the title or abstract of articles in the American Journal of Occupational Therapy reveals only 13 publications. A similar lack of coverage is seen in key teaching resources. For example, a search of Pedretti’s Occupational Therapy Practice Skills for Physical Dysfunction (using Amazon’s inside-the-book search) reveals 2 mentions of medication adherence and 15 mentions of medication management in 1,328 pages (Pendleton & Schultz-Krohn, 2013). In practice, a recent national survey on a purposefully selected group of 70 occupational therapists reported that only about a quarter of therapists working in adult physical dysfunction settings consistently evaluate or treat for medication management impairments (Schwartz & Smith, 2014). The majority of survey respondents specifically reported that they do not engage in medication management because of lack of knowledge, lack of interest, lack of resources, or time constraints. Therefore, although the opportunity is present, occupational therapy professionals are limited by their knowledge of medication and evidence supporting practice in this area.
Importance Within Health Care Reform
Occupational therapy professionals should improve their capacity to address medication management because they already have unique skills that can improve clients’ medication adherence and because this issue is strongly aligned with the broader patient outcomes of the ACA. Medication adherence directly affects the Triple Aim, that is, population health, cost of care, and patient experience.
Population Health
Medication nonadherence is a population health issue. The National Center for Health Statistics (NCHS; 2014) reports that half of Americans take medications. Specifically, 90% of older adults, 60% of adults, and 24% of children have taken one or more prescription drugs in the past 30 days (NCHS, 2014). Although many people take medication, few do so correctly. Approximately half of people on medications are nonadherent (Nieuwlaat et al., 2014; Osterberg & Blaschke, 2005; Vlasnik et al., 2005; WHO, 2003). Therefore, in the United States, approximately 80 million people do not take their medications as prescribed
Everyone occasionally forgets to take prescribed medication, but consistent nonadherence can quickly affect health outcomes. Researchers have estimated that a person must take at least 80% of a medication to receive the benefits of intervention (Fitzgerald et al., 2011; Osterberg & Blaschke, 2005; West of Scotland Coronary Prevention Study Group, 1997). These studies have shown that when clients’ adherence drops below 80%, their health outcomes are more consistent with placebo control groups than with intervention groups. In other words, if a person forgets as few as six pills of a once-daily medication in a 1-mo period, he or she may fail to benefit from the treatment.
When clients’ poor adherence limits treatment effects, they often experience declines in health and function. For example, people who fail to take their diabetes medications have higher glycated hemoglobin levels than their adherent peers (Bogner, Morales, de Vries, & Cappola, 2012). Prolonged periods of elevated blood sugar may lead to impairments such as peripheral neuropathy, kidney failure, and diabetic retinopathy (Estes, 2012). These health conditions are frequently associated with declines in the occupational performance of everyday activities. Moreover, people who are nonadherent to their medications are not only sicker but also have significantly higher rates of all-cause mortality (Currie et al., 2012; Fitzgerald et al., 2011; Osterberg & Blaschke, 2005). These studies suggest that improved medication adherence can decrease symptoms, reduce the risk of mortality, and increase functional performance of large client populations.
Cost of Care
Medication nonadherence is linked to health care spending and hospitalizations. Researchers have identified that people who are not adherent to their medications are more likely to be admitted (or readmitted) to a hospital and discharged to a long-term care facility (Col, Fanale, & Kronholm, 1990; Johnson & Bootman, 1995; Schoen, DiDomenico, Connor, Dischler, & Bauman, 2001; Sokol, McGuigan, Verbrugge, & Epstein, 2005). Because of the increased time in the hospital, people who are nonadherent to their medications spend an average of 41% more than their adherent peers on inpatient health care (Egede et al., 2012; Sokol et al., 2005). Altogether, researchers have estimated that in the United States, more than $100 billion per year is spent on hospitalizations related to medication nonadherence (Lewis, 1997; Osterberg & Blaschke, 2005). These studies suggest that improved medication adherence may reduce health care spending and rehospitalizations.
Health Care Experience
It is no surprise that nonadherent clients, who are sicker and have higher health care expenditures, are not satisfied with their care. Pollack, Purayidathil, Bolge, and Williams (2010) found that nonadherent adults with diabetes experienced increased negative symptoms (e.g., weight gain, water retention, headaches) and reduced treatment satisfaction. Researchers across diagnoses have found similar findings, indicating a strong association between satisfaction and medication adherence (Roberts, 2002; Wroth & Pathman, 2006). These studies suggest that efforts to improve the health care experience may go hand in hand with efforts to improve medication adherence.
Implications for Occupational Therapy Practice
Occupational therapy health policy experts have suggested that for the profession to thrive, occupational therapy researchers, clinicians, and educators must “develop strategies that will align the practice of occupational therapy with the Triple Aim of health care reform” (Leland et al., 2015, p. 4). This article demonstrates that medication management is an issue strongly associated with the Triple Aim and that occupational therapy practitioners have the skills needed to remediate impairments and deliver evidence-based interventions. Despite their strong practice skills in enhancing health literacy, prescribing assistive technology, creating cueing systems, and developing supportive environments, practitioners seem to be lacking knowledge and skills specific to pharmacology. Therefore, this article has the following implications for occupational therapy practice:
New and experienced occupational therapy practitioners need more preservice and continuing education to help them better understand medications (i.e., demonstrate competence in types of medications, jargon, drug interactions, and the profession’s scope of practice at the state and federal level).
Researchers need to better support administrators and clinicians by creating evidence about occupational therapy evaluation, intervention, and outcomes in medication management.
With foundational pharmacology knowledge and evidence to support evaluation and treatment, occupational therapy professionals can begin to integrate medication management into practice to meet the demand from clients and health service organizations.
Conclusion
As a profession, occupational therapy has an opportunity to enable millions of Americans to have healthy, productive lives by enhancing medication management performance and subsequent medication adherence. Occupational therapy practitioners are ideally positioned to support physicians, pharmacists, and other health care professionals and their clients in the pursuit of health and well-being. Practitioners have a unique and valuable skill set that includes a high regard for clients, time management, education, monitoring, persuasion, and assistive technology. With a few changes to current practice, education, and research, the occupational therapy profession can become a leader in this issue. Health care reform has provided the motivation and timing to enable occupational therapy practitioners to affect change in the area of medication adherence. By engaging in medication management, the profession can demonstrate the value of occupational therapy to clients, professional peers, and payers.
Footnotes
Appendix: Medication Management Case Study
The purpose of this case study is to demonstrate the distinct value and unique skills of an occupational therapy practitioner in medication management.
Occupational therapy practitioners could have supported Nina and her care team in several ways. In the acute care setting, the occupational therapist could have evaluated Nina’s performance of medication-related skills, identified her risk of nonadherence, and recommended additional supports to reduce risk of nonadherence (and subsequent readmission). In addition, in acute care, the occupational therapy practitioner could have monitored Nina’s fatigue, dizziness, blood pressure, and heart rate while she performed everyday activities. Through this monitoring, the practitioner could have alerted the team to adverse medication reactions before discharge.
Across the continuum of care, practitioners could provide a variety of other supports for Nina. Practitioners can review Nina’s medications and ensure that she is using them as prescribed. The practitioner can also help Nina develop cues, adopt new assistive technology, or alter the home environment to help her better remember to take her medications as prescribed (Sanders & Van Oss, 2013). Practitioners may also train Nina on how to self-monitor her medication adherence, symptoms, and health metrics such as blood pressure to enable her health care team to create a more informed and data-driven plan of care. For clients like Nina, who experience adverse reactions, the practitioner can help with problem solving. For example, the practitioner can help identify which of Nina’s many doctors prescribed the medication, how to contact the doctor or pharmacist, and how to advocate for her needs in a large and complicated health organization. Finally, practitioners can educate Nina on the importance of adherence and describe the risks associated with delayed action. Occupational therapy practitioners can use their typical intervention approaches of occupation and activity, preparatory methods and tasks, education and training, and advocacy to support the medical team and enable the client to take his or her medication as prescribed.
Acknowledgments
This research was funded by the Distinguished Dissertation Fellowship from the graduate school at the University of Wisconsin–Milwaukee and the Student Research Grant Award from the College of Health Sciences at the University of Wisconsin–Milwaukee, and it was conducted at the University of Wisconsin–Milwaukee. This article was written in partial fulfillment of the requirements for the Doctor of Philosophy in Health Sciences degree at the University of Wisconsin–Milwaukee. Jaclyn K. Schwartz thanks her dissertation committee members, Michael Brondino of the Helen Bader School of Social Welfare, Ron Cisler of the Center for Urban Population Health, Brian Schermer of the School of Architecture and Urban Planning, and Virginia C. (Ginny) Stoffel of the Department of Occupational Science and Technology.