
Abstract
An estimated 313 million workplace accidents resulting in injury occur worldwide every year. Therefore, the burden of workplace injury and disability is present at the individual and the societal level and involves several stakeholders. There has been a shift in paradigm from workplace disability and injury treatment to workplace disability prevention. Occupational therapy practitioners are well positioned to address this multifaceted societal issue. Opening communication lines among stakeholders allows for a more holistic, collaborative, and comprehensive approach to disability, injury, and pain management. The positive results researchers have found at the individual level when using a holistic approach translate to benefits for all of the stakeholders involved. Occupational therapy practitioners may espouse a work disability prevention approach to reduce work disability rates and provide timely return-to-work outcomes for clients. The transition to the preventative model requires collaboration among stakeholders but would be beneficial to all stakeholders involved in the workplace.
Workplace injury and disability remain serious public health issues. An estimated 313 million workplace accidents resulting in injury occur worldwide every year (International Labour Organization, 2014). In 2013, more than 241,000 Canadians experienced workplace-related lost time, injury, or disease (Association of Workers’ Compensation Boards of Canada, 2013). These workplace injuries and disabilities directly cost the Canadian economy CAD $9.7 billion in 2008 and an estimated CAD $19 billion in 2010 (Gilks & Logan, 2010). In 2012, the number of working-age adults in the United States with chronic conditions had grown to 58 million, an increase of 25% over 10 years (Pendo, 2009). Furthermore, a survey conducted by Pricewaterhouse Coopers found that indirect costs to employers (e.g., missed days at work) in the United States were 4 times higher for individuals with chronic health concerns than for those who did not have such concerns (Mattke, Schnyer, & Van Busum, 2013). Therefore, the burden of workplace injury and disability is present at the individual and the societal level and involves several stakeholders. The literature has identified the individual, the workplace (e.g., the employer and the coworkers), and the compensation system, as well as the health care system, as stakeholders for workplace disability (Loisel et al., 2001; Maiwald, de Rijk, Guzman, Schonstein, & Yassi, 2011).
Occupational therapy practitioners are well positioned to address this multifaceted societal issue; more specifically, they are in a unique position to play a central role in the management of workplace disability and in the prevention of workplace disability. Disability management refers to a deliberate and coordinated effort to support client recovery through treatment and early intervention, prevent injury or disability, and create accommodations so clients can maintain employment after the onset of an injury or disability. Disability management is optimal when it consists of a collaborative effort among the stakeholders (employees, employers, and agencies providing disability services; Canadian Association of Occupational Therapists [CAOT], 2011). Workplace disability prevention (WDP) refers to interventions during the primary prevention stage or the subacute phase of a disease. The WDP model proposes implementing interventions early and therefore preventing disease or disability or the progression of such disease or disability (e.g., interventions during the subacute phase to prevent chronic back pain; Bell et al., 1995; Loisel et al., 2001; van Oostrom et al., 2009). Moreover, holistic approaches to health, such as the approach adopted by the field of occupational therapy, take into consideration the psychosocial factors associated with successful interventions, which establishes a more comprehensive approach to workplace disability management.
Argument
The holistic approach of occupational therapy considers not only the physical aspect of health in the workplace but also the mental, emotional, cognitive, cultural, and social, as well as the idiosyncratic, aspects of health (CAOT, 2015; Thibault, Loisel, Durand, Catchlove, & Sullivan, 2008). Moreover, these more comprehensive and inclusive approaches to workplace disability and its prevention may result in improved health outcomes (CAOT, 2015; Carragee, Alamin, Miller, & Carragee, 2005; Sullivan & Stanish, 2003; Thibault et al., 2008; Tjulin, Maceachen, & Ekberg, 2010). The literature posits that efforts to prevent or cure diseases from a purely physical perspective have shown limited results and more holistic methods are required (Carragee et al., 2005; Loisel et al., 2001; Sullivan & Stanish, 2003; Thibault et al., 2008; Tjulin et al., 2010). More recently, several studies have shown that the disability problem goes beyond the physical and incorporates personal characteristics (i.e., psychosocial) and environments (i.e., workplace, workers’ compensation systems) in terms of workplace disability and injury (Carragee et al., 2005; Loisel et al., 2001; Sullivan & Stanish, 2003; Thibault et al., 2008; Tjulin et al., 2010). Occupational therapy practitioners’ understanding of the relationships and interactions among the person, the environment, and the person’s occupations provides yet another unique perspective in the disability management process (CAOT, 2011).
The literature has also shown that consideration of psychosocial factors in workplace disability management yields more positive results and more positive health outcomes for clients and employers alike (CAOT, 2015; Carragee et al., 2005; Loisel et al., 2001; Sullivan & Stanish, 2003; Thibault et al., 2008; Tjulin et al., 2010). One study conducted by Carragee et al. (2005) on lower back pain found that taking psychosocial variables into account in conjunction with physical variables better predicted improvement of lower back pain over time, whereas physical variables alone had weak associations with long-term lower back pain and disability. They also found that psychosocial variables strongly predicted long-term and short-term instances of disability and health care visits for lower back pain. The predictive value of the psychosocial factors could help with the development of appropriate treatments and intervention strategies as well as with reducing workplace-related lost time (Carragee et al., 2005).
A study on return-to-work found that workplace-based interventions should extend beyond the technical and task-oriented accommodations involved with returning to work and consider the social context within which these interventions take place (Tjulin et al., 2010). Tjulin et al. (2010) suggested that the return-to-work process is a socially constructed event in which social interactions and relationships must adapt to changing needs and roles. Their findings indicated that early social contact during the subacute phase preceding return-to-work eliminates feelings of invisibility and uncertainty on the part of the employee who has suffered an injury or disability. Moreover, early social contact opens the lines of communication about how and when the person will return to work. Evidence has shown that early contact results in shorter durations of sick leave and lost work time (Tjulin et al., 2010). Note that Tjulin et al. proposed that further research should clearly and quantitatively define early social contact.
Tjulin et al. (2010) also found that most postreturn phases of return-to-work programs encompass modified jobs and tasks that eliminate the impact and presence of the worker’s disability but do not account for the social and psychological impact of the transition. Therefore, a more holistic approach that incorporates psychosocial factors into the return-to-work process could produce smoother transitions, fewer feelings of uncertainty, and shorter durations of lost work time.
These psychosocial factors should be taken into consideration not only in terms of the return-to-work paradigm but also in terms of pain management. Thibault et al. (2008) found that interventions that target pain intensity, pain catastrophizing, and the fears associated with pain could be effective means of reducing pain behaviors. Thibault et al. also found that the ability to address and reduce psychological factors associated with pain could act as a determinant of rehabilitation success. A similar study conducted by Sullivan and Stanish (2003) found that although psychological and social factors have been acknowledged as integral components of many tertiary care pain management programs, these factors have been underrepresented in primary and secondary prevention programs. Sullivan and Stanish noted that pain has thus far been predominantly conceptualized as “physical” in the literature and that pain management professionals should begin to view psychological interventions as fundamental components of such programs. They went on to suggest that psychologically based activity mobilization programs could have significant positive outcomes over the long term for both pain management and preventive programs.
An investigation by Loisel et al. (2001) proposed a shift in paradigm from workplace disability and injury treatment to workplace disability prevention. Loisel et al. suggested that this shift could help eliminate instances of chronic pain in workers and prevent the lost workplace time that affects all of the stakeholders involved (e.g., the employee, the coworkers, the employer, the insurance agency, the health care system) in workplace disability. This model follows the line of reasoning pertaining to shifting the focus from secondary and tertiary prevention to prevention at the primary stage (Bell et al., 1995; CAOT, 2015). The studies have shown that using the WDP approach of treating clients at earlier stages of injury “through patient reassurance and interventions linked to the workplace” (Loisel et al., 2001, p. 352) in place of the medical model of treating chronic pain once it already exists is a far more successful intervention strategy. This intervention strategy suggests that if rehabilitation health professionals use the model to address and prevent disability during the primary prevention phase, then the evolution of prolonged or chronic disability could be avoided. This approach to workplace injury and disability would be beneficial to all the stakeholders involved in workplace disability (Figure 1).
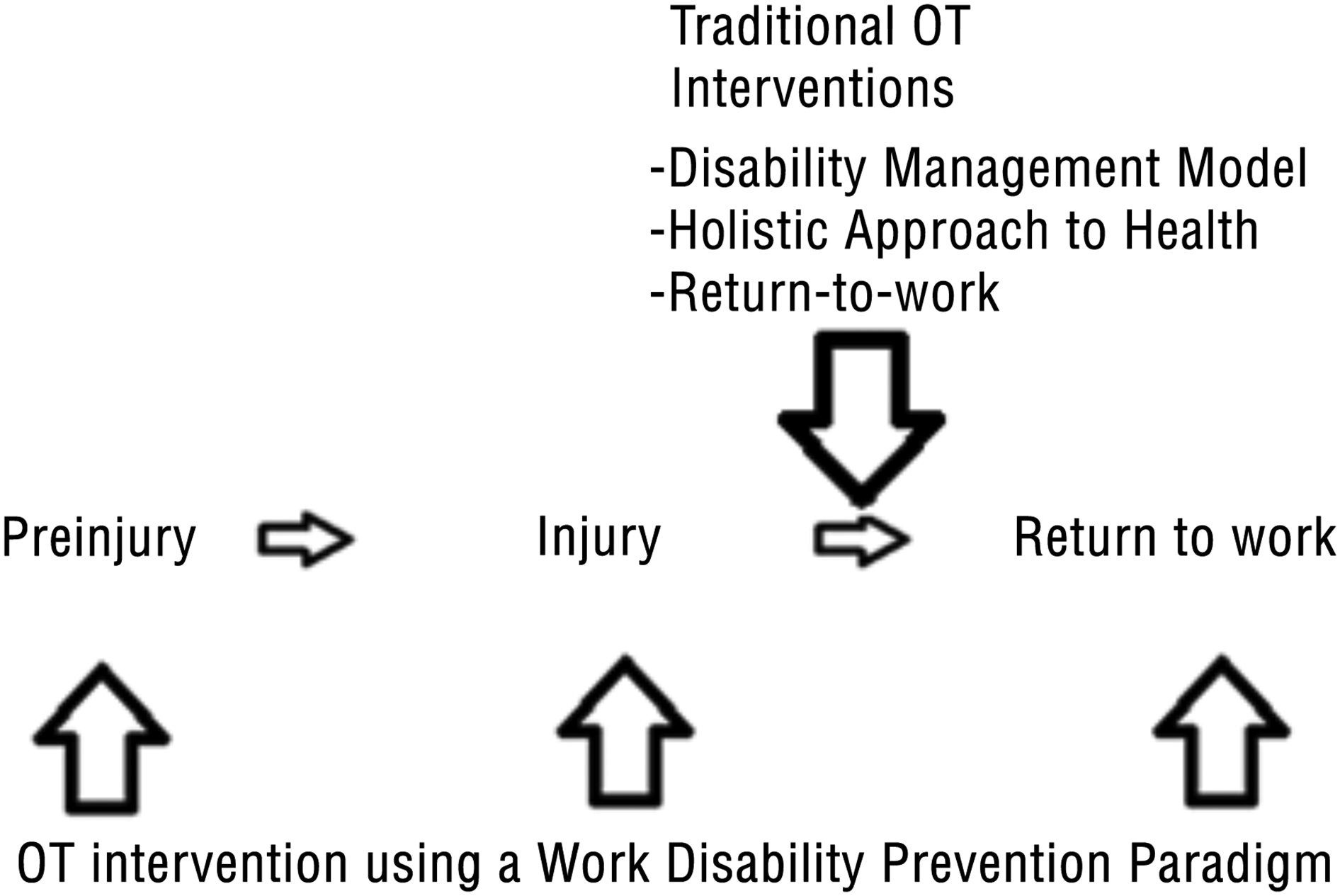
Occupational therapy and a work disability prevention approach.
Future Directions
Occupational therapy practitioners are in a unique position to improve and enrich the approach taken to workplace disability and injury. The literature has consistently shown that the implementation of a holistic approach to workplace disability and injury management produces more positive results and outcomes (CAOT, 2015; Carragee et al., 2005; Sullivan & Stanish, 2003; Thibault et al., 2008; Tjulin et al., 2010). Therefore, incorporating idiosyncrasies, psychosocial factors, environmental factors, and cultural factors in conjunction with the physical aspect of disability into disability management systems is a necessity. The positive results found at the individual level when using the holistic approach translate to benefits for all of the stakeholders involved by improving psychosocial relationships and reducing lost workplace time (CAOT, 2015; Carragee et al., 2005; Loisel et al., 2001; Sullivan & Stanish, 2003; Thibault et al., 2008; Tjulin et al., 2010). Moreover, the concept of opening communication lines between stakeholders allows for a more holistic, collaborative, and comprehensive approach to disability, injury, and pain management (CAOT, 2015; Carragee et al., 2005; Sullivan & Stanish, 2003; Thibault et al., 2008; Tjulin et al., 2010).
Introducing the disability management dialogue before the return-to-work phase has also exhibited more positive results in terms of disability management and should therefore be a standard component of return-to-work disability management (Tjulin et al., 2010). Likewise, addressing workplace disability and injury at the subacute phase by implementing interventions at earlier stages of injury and disability could help avoid and eliminate workplace injuries and disabilities (Jordan, Nowrouzi-Kia, Gohar, & Nowrouzi, 2015). This shift could potentially lower rates of workplace disability by transitioning the approach from the reactive medical model to disability management to the proposed preventive model (Loisel et al., 2001). The transition to the preventive model requires collaboration among stakeholders but would be mutually beneficial to all the stakeholders involved in workplace disability.
Future Recommendations
Ultimately, occupational therapy practitioners are well positioned to be leaders in the transition from the current reactive model to a preventive model of workplace disability. Their roles as advocates, educators, researchers, and solution strategists will be extremely beneficial to this transition. Practitioners play a crucial collaborative role among stakeholders to develop mutually beneficial goals and strategies for disability management. They can identify occupational risks through assessments, observational evaluations, and research to detect specific areas for intervention to facilitate elimination of workplace disability, and they are thus also well positioned to develop management models that address workplace disability from a holistic perspective. Occupational therapy practitioners’ expertise in areas such as injury prevention, body mechanics, ergonomics, and emotional health creates numerous opportunities for intervention, education, and research in occupational therapy.
The implementation of the preventive model described in this article also creates an opportunity for occupational therapy practitioners to develop evidence-informed practice for workplace disability prevention and an opportunity for the occupational therapy research base to expand and develop recognition at the societal level. This transition to a preventive model in health care could have the potential to help eliminate the larger scale financial burden of workplace disability. Moreover, the focus on wellness and health promotion in occupational therapy at the individual, population, and organizational levels could have significant positive health effects on society as a whole. Occupational therapy practitioners’ expertise allows them to assume a unique position of advocacy in replacing the reactive model of disability management with a preventive model.
Next Steps
Occupational therapy practitioners should play a more centralized and leadership role in workplace disability management.
Occupational therapy practitioners should implement comprehensive occupational therapy services and expertise at earlier stages of the disability management process (the subacute phase) to improve disability management outcomes for all involved stakeholders.
Future research should be conducted to support workplace disability prevention.