
Abstract
Cognitive impairment is a major health and safety problem for the growing population of older drivers in the United States. In 2012, 5,560 people over age 65 were killed and 214,000 were injured in motor vehicle traffic crashes, with older people comprising 17% of all traffic fatalities and 9% of all people injured in traffic crashes during the year (National Highway Traffic Safety Administration, 2014). Dementia is a major underlying cause of significant driving impairment among older adults. Many of the research studies and public policies addressing dementia and driving have focused on defining methods to detect and retire unsafe drivers (Carr & Ott, 2010).
Driving is an important component of independent living; it supports occupational, volunteer, self-maintenance, religious, and social activities and is among the most complex and demanding instrumental activities of daily living (Sherman, 2006). Nevertheless, relatively little attention has been paid to possible interventions to prolong the time for which older drivers with cognitive impairment can drive safely and maintain their transportation independence. This gap in knowledge and practice is related, at least in part, to the absence of even preliminary clinical trials in the area (Classen, Monahan, Auten, & Yarney, 2014). Although programs providing educational and cognitive training to healthy older adults have yielded encouraging prospects for enhancing driver safety (Bédard et al., 2008; Edwards, Delahunt, & Mahncke, 2009; Lavallière, Simoneau, Tremblay, Laurendeau, & Teasdale, 2012; Marottoli et al., 2007; Roenker, Cissell, Ball, Wadley, & Edwards, 2003), implementation would be challenging for people with cognitive impairment and would be unlikely to have a lasting benefit for drivers with a degenerative brain condition, such as Alzheimer’s disease, because of its progressive nature.
A more intensive, individualized behavioral program that directly addresses participants’ problem driving behaviors, with the involvement of family members, is more likely to be successful in this group of at-risk drivers. Postdrive feedback using in-car technology holds great promise for the design and implementation of such a program (Lee, 2009; Toledo & Lotan, 2006; Vrkljan & Polgar, 2007).
One technology that could be readily adapted for this purpose is g-force–generated video event recording, such as DriveCam® (Lytx, San Diego, CA). Research in which DriveCam feedback was used helped reduce unsafe driving events among 26 high-risk teen drivers by 76% (McGehee, Raby, Carney, Lee, & Reyes, 2007), with persistence of effect maintained over a subsequent 8 wk period of monitoring (McGehee, Carney, Raby, Lee, & Reyes, 2008). In a follow-up study of 18 other teen drivers who received 40 wk of video feedback intervention, unsafe driving events were reduced by 61% and did not significantly increase during a 6-wk follow-up period (Carney, McGehee, Lee, Reyes, & Raby, 2010). A 13-wk study of 90 parent–teen dyads, randomized to immediate warning light–only feedback versus video event feedback, showed a large effect size (Cohen’s d = 1.67) for video event feedback but not for immediate warning light–only feedback (Simons-Morton et al., 2013).
DriveCam was also shown to be effective in two studies involving professional drivers. A study of 80 truck drivers reported reductions in frequency of events per mile of 37% to 52% (Hickman, Hanowski, & Ajayi, 2009). A study of 54 ambulance drivers showed significant reductions in events per mile, events per call, and severity of events over 2 yr (p < .0005; Myers, Russi, Will, & Hankins, 2012).
The specific aims for this pilot study were to demonstrate that (1) g-force technology can effectively detect unsafe driving events in an older adult population and (2) older adults with cognitive impairment can improve their driving safety with an in-car video feedback intervention.
Method
Participants
Participants were age 60–90 yr and were being treated at the Rhode Island Hospital outpatient memory clinic. Neurological examinations were judged to be normal for age, and all participants scored <28 on the Mini-Mental State Examination (Folstein, Folstein, & McHugh, 1975). All had an adult family member or other caregiver who participated in counseling feedback. Participants taking antidementia medications were required to have been on a stable dosage before enrollment. To exclude people who should not be driving because of moderate dementia (Carr & Ott, 2010; Iverson et al., 2010), all participants were required to have a Clinical Dementia Rating (CDR; Morris, 1993) score of 0.5 or 1.0 (CDR range = 0 [normal] to 3 [severe dementia]; those who scored ≥2.0 were excluded). Also excluded were people who had ophthalmologic, physical, or neurological disorders other than dementia that impaired their driving ability; visual acuity worse than 20/40 in the best eye; hemianopia; musculoskeletal disorders causing major physical disability; alcohol or substance abuse within the past year; use of sedating medications; language impairment that would interfere with the ability to participate in the intervention; and a previous road test evaluation or the opinion of a caregiver or health professional indicating that the person was not able to drive safely.
Twelve drivers were enrolled over the course of 9 mo. Their ages ranged from 68 to 90; 8 were female and 4 were male, and 9 had child caregivers and 3 spouse caregivers. All participants had very mild dementia (CDR = 0.5, n = 3) or mild dementia (CDR = 1.0, n = 9), and all signed a hospital-approved institutional review board consent form.
Procedures
The initial visit included installation of a DriveCam monitoring video device. The palm-size camera was mounted in a bracket secured to the windshield behind the rearview mirror with an adhesive. Once installed, the camera continuously captured video and temporarily saved the previous several seconds in a video buffer. If the device was not triggered by excessive g-forces, all data were deleted permanently 10 s later. The camera provided views of the forward roadway and the driver in the vehicle interior.
When the camera sensed excessive g-forces above a preset threshold (lateral, longitudinal, or shock), it saved the previous 8 s and continued to record and save the next 4 s, then stored that “event” for later transmission to the DriveCam’s video driving analysis center. Events were sent back to DriveCam via a cellular network. The central video raters at DriveCam were blind to the participants’ diagnosis, other clinical information, and study goals.
GPS data allow the determination of speed and geographic speed limits. Unsafe driving events were rated according to eight major categories of concern: (1) distractions, (2) poor awareness, (3) driver conduct, (4) fundamentals, (5) following too closely, (6) driver condition, (7) traffic violations, and (8) other concerns. The specific events or problems were graded for safety risk on a 0- to 10-point demerit scale. A single unsafe driving event could have more than one demerit category, such as judgment error combined with poor awareness of an intersection, leading to a combined driving severity rating score for the individual event. The severity rating scores derived and reported by DriveCam experts were previously used in a longitudinal study of ambulance drivers to demonstrate reduction in not only numbers of events but also severity scores for events (Myers et al., 2012). The primary quantitative outcomes from these ratings for our study were total number of unsafe driving events (events scored >5 points) per 1,000 miles driven and total unsafe driving event severity score per 1,000 miles. Secondary qualitative outcomes included the types and severity of unsafe driving events that were recorded.
During the baseline phase of 3 months, the event recording lights were disabled, and there was no feedback training. The DriveCam professional staff and a research assistant monitored the captured and transmitted driving behaviors throughout the 9-mo course of the study; these behaviors were reviewed and discussed at a weekly meeting by the research team. During the intervention phase (Months 4–6), the event recording lights actively flashed. Every week, participants received from research staff a progress report in the mail, along with a DVD of recorded unsafe driving events. The report included advice for reducing such unsafe events as well as positive commendations when few or no safety events were recorded. The study neuropsychologist contacted each participant and his or her caregiver weekly to answer questions, provide additional coaching, and verify that they had read the information and reviewed the DVDs. During the postintervention monitoring phase (Months 7–9), the event recording lights were again disabled, and there was no feedback training. At the end of the study, all participants and their caregivers completed an 11-item paper-and-pencil questionnaire on which they rated their satisfaction with aspects of the program on a scale ranging from 1 (not at all) to 4 (very much so).
Results
At baseline, the mean number of unsafe driving events was 16.3 ± 21.0 (range: 1–69) for the 12 participants. Figure 1 illustrates the range of driving behaviors observed and the types of unsafe driving events for all participants enrolled during the baseline and intervention phases. The most frequent errors were unsafe speed (n = 139), not scanning at intersections (n = 58), judgment errors (n = 38), not looking far enough ahead (n = 34), rolling stops (n = 28), and distracted driving (n = 25).
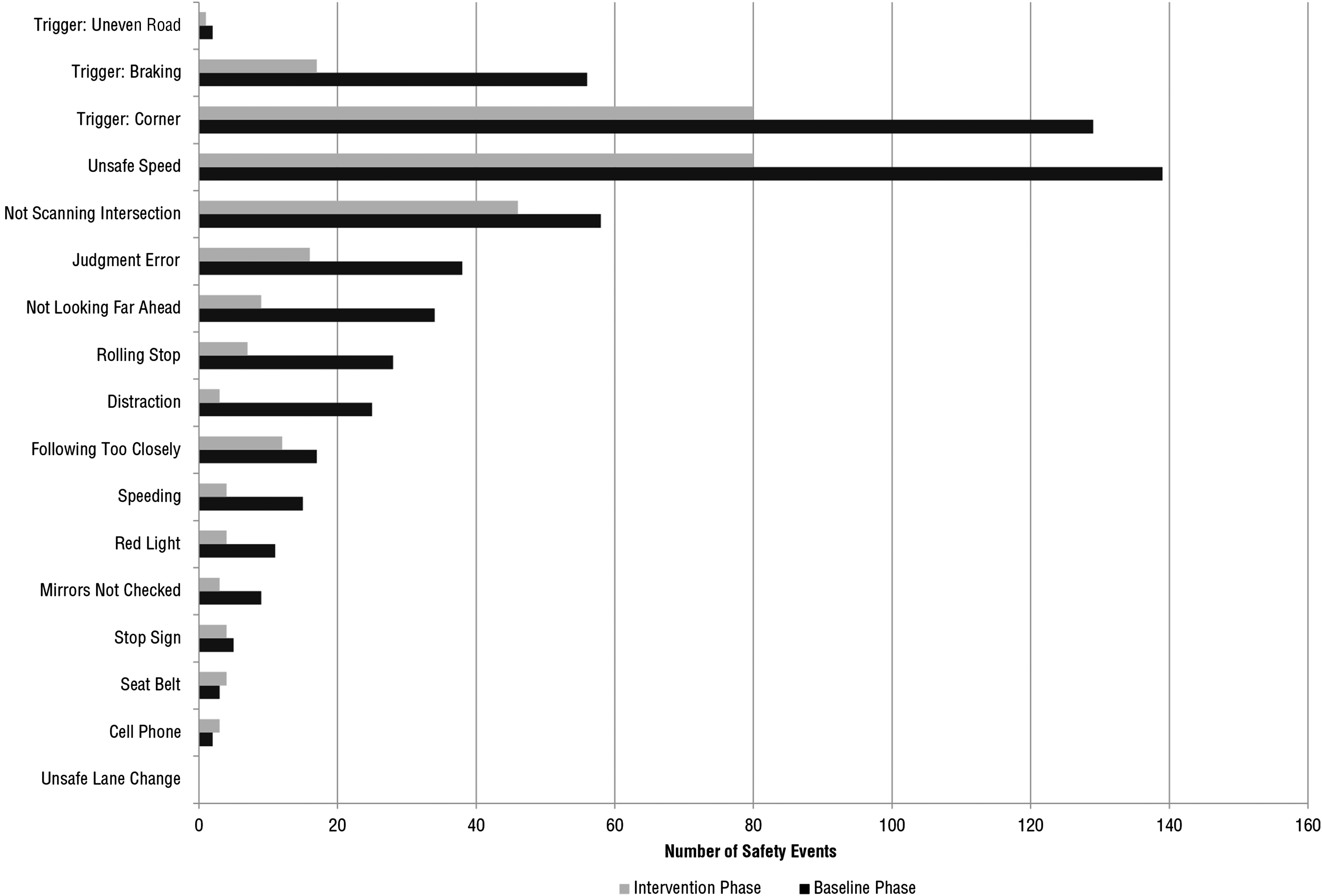
Total number of unsafe driving events recorded for all participants during baseline (N = 12) and intervention phases (N = 11).
The numbers of unsafe driving events and the unsafe driving severity scores during each phase, corrected for miles driven, are presented in Figures 2 and 3. Because of the small number of participants and relatively high dropout over the course of the study, three separate bars are shown in the figures representing all drivers enrolled at each phase, those who completed the intervention phase, and completers who were rated at highest risk at baseline (for illustration purposes, we defined high risk as >1 unsafe event/wk). Five participants withdrew during the course of the study (1 during the baseline phase; 2 during the intervention phase, both of whom were high-risk drivers; and 2 during follow-up phases, 1 of whom was a high-risk driver) at the request of their adult child caregivers, who thought their parent should retire from driving after reviewing the videos. Nine completed the intervention phase.
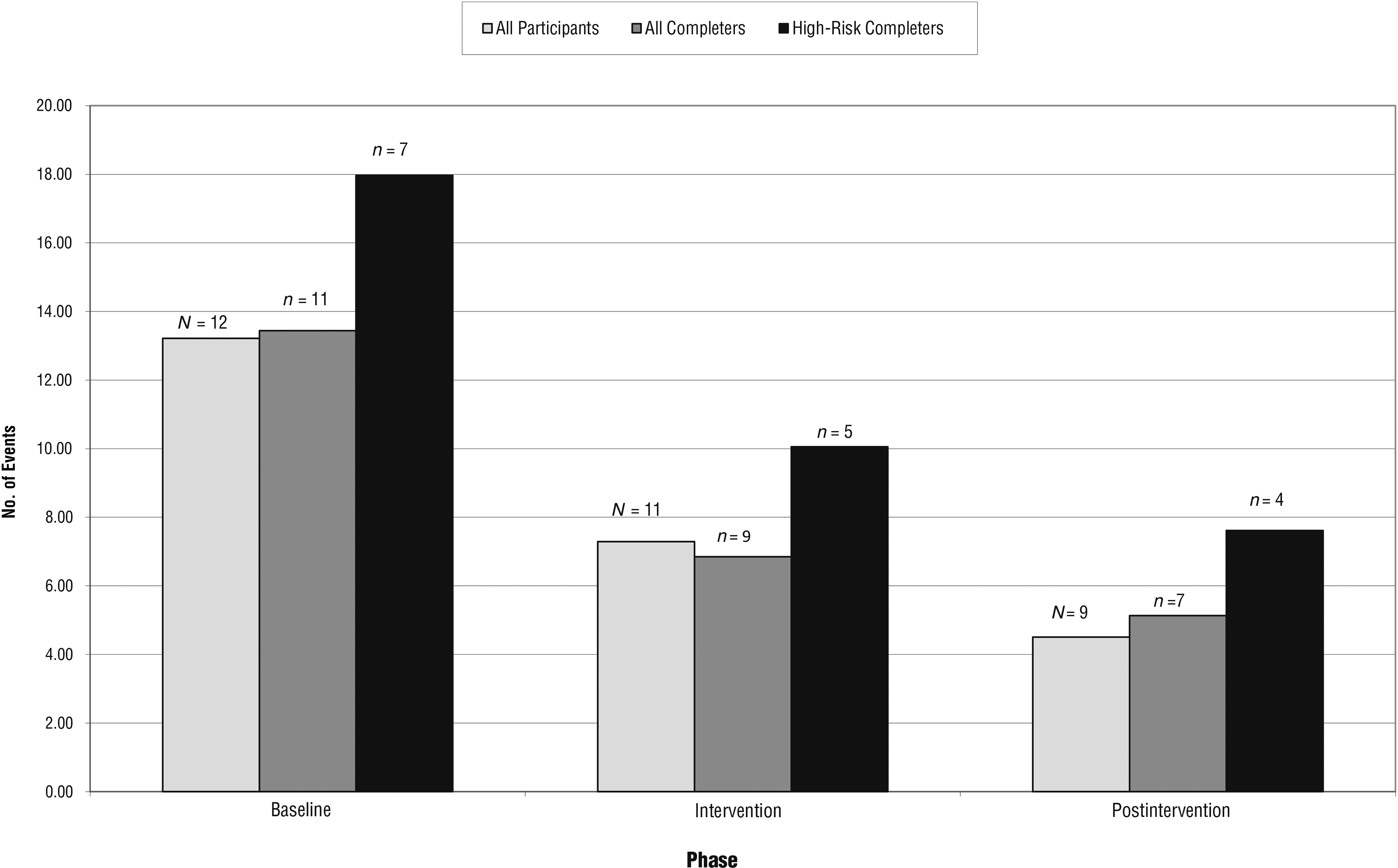
Mean total unsafe driving events (per 1,000 miles).
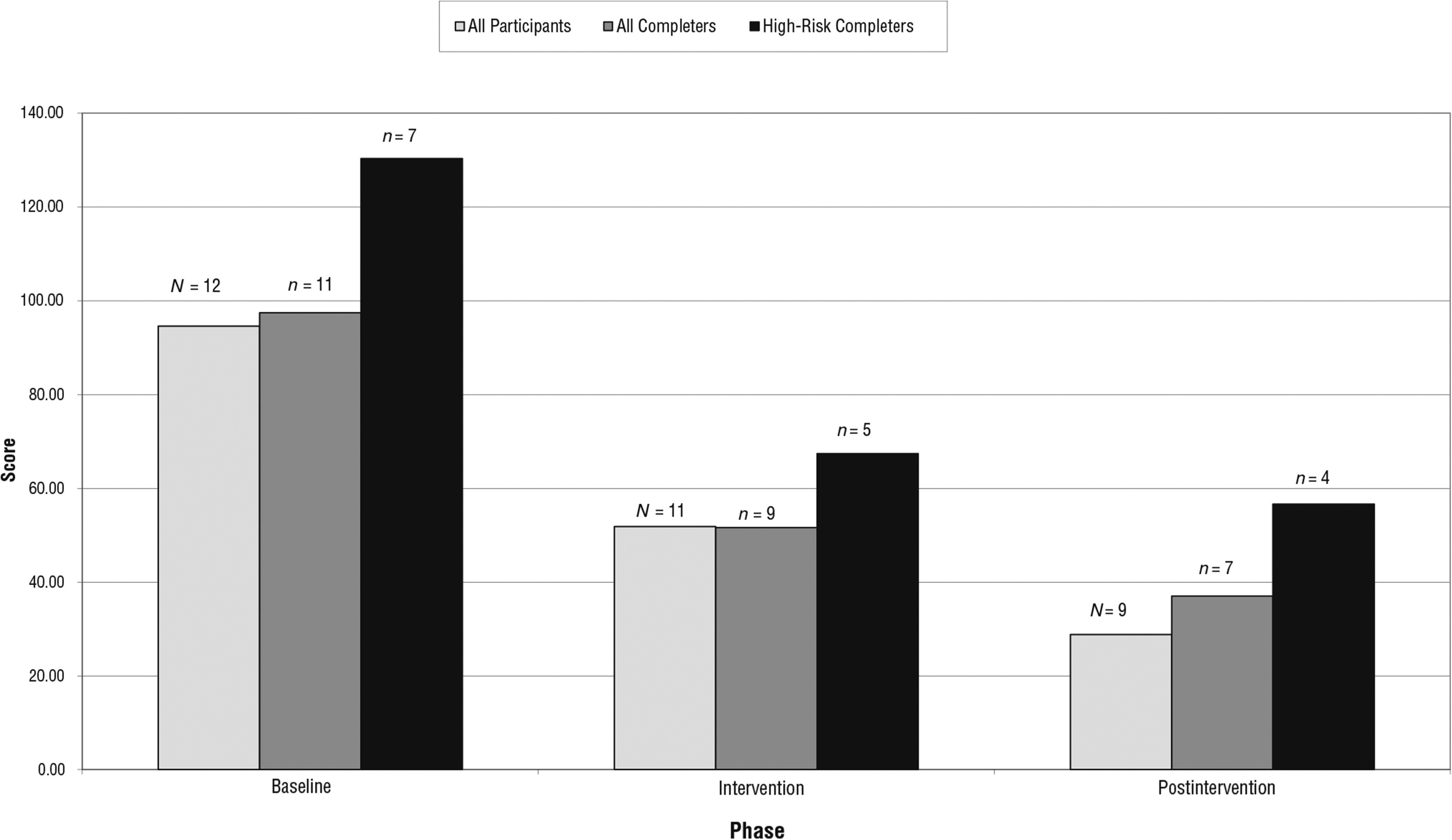
Mean total unsafe driving severity score (per 1,000 miles).
The mean frequencies of unsafe driving events during baseline, intervention, and follow-up phases are shown in Figure 2. Compared with their individual baseline values, mean total unsafe driving events per 1,000 miles were reduced by 38% for the 9 completers during intervention. Compared with their individual baseline values, mean total unsafe driving events per 1,000 miles were reduced by 55% for the 7 completers of the postintervention phase.
The mean unsafe driving severity scores are shown in Figure 3. Compared with their individual baseline values, mean total unsafe driving severity scores per 1,000 miles were reduced by 43% for the 9 completers during intervention. Compared with their individual baseline values, mean total unsafe driving severity scores per 1,000 miles were reduced by 56% for the 7 completers of the postintervention phase.
No major accidents or injuries occurred throughout the course of the study. Because of the small number of participants, statistical analyses were not performed.
Satisfaction questionnaires from participants who completed the intervention indicated that they had few problems with the camera, did not pay attention to the camera’s flashing light, and did not find the DVDs helpful. They found the written feedback and phone calls helpful, made an effort to change their driving behavior, and were very satisfied with the program overall. The caregivers indicated few problems with the camera and noticed few drivers responding to the camera’s flashing light. Few noticed a change in the participants' driving or evidence of the participants’ insight into their driving behaviors. Overall, caregivers found all aspects of the feedback helpful and were satisfied with the program (see Table 1).
Satisfaction Survey Results
Note. Responses ranged from 1 (not at all) to 4 (very much so).
Discussion
Participation in a prolonged, individualized video feedback program with active coaching reduced unsafe driving behaviors by up to 56% in a group of older adults with cognitive impairment. The magnitude of the safety effect is comparable to those in similar studies of truck (Hickman et al., 2009) and ambulance drivers (Myers et al., 2012) but not as high as that reported in a study of teenage drivers using DriveCam feedback over a similar time period (57%–83%; Carney et al., 2010; McGehee et al., 2007, 2008).
Benefits of the intervention appeared to be sustained for up to 3 mo, despite the participants’ memory impairment. We suspect that this enhanced delayed effect is related to the caregivers’ becoming more effective “home coaches” through their experience with the intervention. This form of intervention is ideally suited to drivers with dementia because it not only may lead to safer driving practices for those who continue to drive but also provides a means for family members, professionals, and other caregivers to monitor the drivers’ driving practices and helps with the difficult decision making and counseling necessary to recommend driving retirement.
This pilot study has several limitations beyond its small sample size. Our effect size may have been reduced by participant factors such as progressive disease. The feedback program had multiple components, and we could not determine the relative contribution of the blinking camera light, DVD, letters, and telephone contact to reductions in unsafe driving events and severity scores. On the basis of the surveys we received from participants, as well as a report of teenage drivers that showed no effect of lights-only feedback (Simons-Morton et al., 2013), it is unlikely that the blinking light alone provided adequate feedback to prompt change in driving habits.
Naturalistic approaches to solving safe driver problems in general are desirable because of their face validity, although such approaches are difficult to carry out because of a lack of control variables and participants. Although the use of more heavily instrumented vehicles in observational research studies, such as the 100-Car Naturalistic Driving Study (Dingus et al., 2006), provides more abundant naturalistic driving data, we believe the DriveCam technology is superior for real-world intervention applications such as ours because of its cost, efficiency, and proven efficacy in certain groups of drivers.
A larger randomized controlled clinical trial of this intervention will be required to demonstrate efficacy before it can be recommended or implemented in clinical practice. To our knowledge, this is the first study to attempt to improve the driving practices of older adults with Alzheimer’s disease (Classen et al., 2014). Simply demonstrating that this group can learn how to drive more safely through an intervention could pave the way for other approaches to improve the safety of this expanding pool of older at-risk drivers.
Implications for Occupational Therapy Practice
Driving is a major instrumental activity of daily living that helps older people maintain their independence and quality of life. This study provides occupational therapy practitioners information about a potentially useful video feedback intervention that could enhance the safety of older drivers with cognitive impairment. This study has the following implications for occupational therapy practice with older adult drivers:
In-vehicle video event recorder feedback technology may be useful for monitoring driving behaviors and enhancing driver safety.
Future advances in video technology may be incorporated into occupational therapy practice with medically at-risk older drivers.
Footnotes
Acknowledgments
This research was supported in part by Grant R03AG046472 from the National Institute on Aging to Brian R. Ott and by an internal grant from the Rhode Island Hospital Department of Neurology to Brian R. Ott. The results of this pilot study were presented at the Alzheimer’s Association International Conference in Washington, DC, July 21, 2015. The ![]() Protocol Record Number is 263758-14.
Protocol Record Number is 263758-14.