
Abstract
Taking medications is a daily occupation for many of the 117 million people in the United States with a chronic health condition (Centers for Disease Control and Prevention, 2015). Unfortunately, 30%–50% of people do not take their medications as prescribed (Osterberg & Blaschke, 2005). Evidence suggests that many people fail to take their medications because of problems with medication management. Gadkari and McHorney (2012) surveyed 24,017 adults and found that the most common reasons for medication nonadherence include forgetting, running out of medication, or being careless about the medication-dosing schedule. Not taking medications as prescribed can result in poorer health outcomes, disability, hospitalizations, and higher rates of all-cause mortality (Davis, Edin, & Allen, 2010; Ho et al., 2006). Current medication adherence interventions are complex, costly, and not very effective (Nieuwlaat et al., 2014). New interventions are needed to help people with chronic health conditions take their medications as prescribed.
Historically, physicians have both prescribed and ensured adherence to medications. At present, many physicians do not have the time or full complement of expertise in health behavior change to counsel clients in medication adherence (Schwartz & Smith, 2017; World Health Organization, 2003). Researchers are increasingly testing interventions implemented by allied health professionals because they offer better generalizability to real-world situations (Nieuwlaat et al., 2014). Unfortunately, because of the complexity of the administered interventions and limitations in the methodology, it is unclear which aspects of allied health interventions generate positive effects. Allied health professionals need to better identify their unique contributions to complex interventions (Richardson et al., 2014).
We hypothesized that one allied health professional, the occupational therapy practitioner, can help people better manage their medications. The Ecological Model for Adherence in Rehabilitation suggests that occupational therapy practitioner–client teams can modify person factors, provider factors, intervention factors, the environment, self-determination, and knowledge to improve adherence (Radomski, 2011). Little research, however, has documented the effectiveness of defined occupational therapy interventions on medication adherence (Radomski, 2011; Sanders & Van Oss, 2013).
To test our hypothesis, we began with a Phase I study. The goals of a Phase I study are to define the intervention and evaluate its acceptability, feasibility, and safety (Gitlin, 2013). This project had three objectives: (1) evaluate the acceptability of the intervention, (2) understand whether the intervention is effective enough to warrant future research, and (3) define the intervention. Feasibility and safety have been discussed elsewhere (Schwartz, 2015; Schwartz & Smith, 2017).
Method
People with chronic health conditions and a history of poor adherence to medication regimens participated in a two-group experimental blinded randomized controlled trial (RCT). In the RCT, half of the participants received an occupational therapy intervention designed to help them develop new habits and routines to promote medication adherence. The other half of the participants received a pamphlet-based educational session on medication management.
At the end of the study, participants were interviewed about their experiences. For Objective 1 (acceptability), participants described their perceived need for additional medication management services during regular doctors’ visits. For Objective 2 (effectiveness), participants indicated effectiveness of the intervention in four ways: (1) self-perceived improvements in the ability to manage medications, (2) the magnitude of the self-perceived improvements, (3) quantitative improvements in adherence, and (4) the number of behavioral changes implemented after intervention. For Objective 3, participants were asked to describe the intervention in their own words. This helped the research team to better define the intervention and identify the most effective components of this allied health–implemented intervention. All procedures took place during the fall of 2014 and were reviewed and approved by the University of Wisconsin–Milwaukee institutional review board.
Participant Selection
We purposefully sampled persons with chronic health conditions and poor medication adherence. To be included in the study, participants were required to be adults diagnosed with a chronic health condition, on a medication regimen of five or more medications, who live in the community and independently manage their medications. They were required to indicate poor medication adherence. People were excluded from the study if they demonstrated significant cognitive impairment (indicated by a score of 10 or more on the Short Blessed Test; Katzman et al., 1983). There was no relationship established with the participants before the study, except for 3 participants who were students at the university where the study was conducted.
Study Staff
Six senior occupational therapy students served as research assistants (RAs) and collected data for this study. All the RAs were female students returning to the occupational therapy program and were, on average, age 23 yr. The RAs had completed coursework in research, chronic health conditions, and therapeutic communication (including motivational interviewing). Before data collection, the RAs completed approximately 6 additional hr of training that complemented their coursework. To demonstrate competence to administer the study protocols, the RAs completed a series of written and practical examinations (Schwartz & Smith, 2015). The RAs implemented the intervention and follow-up evaluation.
The primary investigator (PI; Schwartz) developed the intervention manual, recruited participants, screened potential participants, completed the baseline evaluation, obtained informed consent from the participants, trained the RAs, administered all enrollment and blinding procedures, monitored fidelity to the intervention by means of video recordings, and conducted the data analysis. At the time of data collection and analysis, the PI was a master’s-trained occupational therapist and a doctoral candidate with approximately 4 yr of practice experience. She had advanced training in research design and quantitative and qualitative methodologies.
Instrumentation
At baseline, each participant filled out a demographics questionnaire, indicating his or her health condition(s), age, race, sex, health insurance status, relationship status, and employment status. Participants were also trained to complete medication diaries. Each day, participants recorded the time and number of medications consumed. This information was used to triangulate participants’ perceptions of medication adherence with their actual medication adherence. At the conclusion of the study, all participants completed a brief semistructured exit interview. During the interview, the participants answered the following four questions:
Since you have become part of this study, have you started doing anything differently to manage your medications?
Do you think your ability to take your medications has improved, declined, or stayed the same?
You met with the occupational therapy research team to talk about medication management. What did you find to be most helpful?
You received your visit with the occupational therapy team as part of a research study. Do you think your doctor should offer services like these at his or her office?
The question route was standardized, but the RAs were instructed to ask probing questions as needed to understand the participant’s experience. The question route was pilot tested internally and improved before use.
Participants also completed a series of surveys at baseline and follow-up. Participants completed surveys on quality of life, self-efficacy, satisfaction, beliefs about medications, and their satisfaction with their pillbox; these surveys have been discussed elsewhere (Schwartz, 2015, 2016; Schwartz & Smith 2017). The purpose of the surveys was to understand the feasibility of using them in future studies with larger sample sizes.
Intervention
Occupational Therapy Intervention Group.
Half the participants received a manualized 30-min occupational therapy intervention, the Integrative Medication Self-Management Intervention (IMedS; Schwartz, 2015; see also Medication Management Research Project, 2014). An occupational therapist developed the IMedS intervention on the basis of theory, current practice, and best evidence (Schwartz, 2015). The intervention was then manualized on the basis of the recommendations of Blanche, Fogelberg, Diaz, Carlson, and Clark (2011). The intervention manual is available by request from the PI.
During administration of the IMedS, the interventionist and client progress through a three-step process. First, the interventionist and client reflect on past performance of medication management by reviewing a 2-wk medication diary and a medication adherence questionnaire. Second, the interventionist encourages the client to set a medication goal. The goal is generated by the client and can be pertinent to any portion of the medication process, such as requesting refills on time or taking a certain percentage of medication. Finally, the interventionist helps the client generate strategies to reach the goal. During strategy generation, the interventionist uses therapeutic use of self and motivational interviewing to help the client self-generate new medication management strategies. To be specific, the IMedS protocol prompts the interventionist to have the client consider strategies in the following six areas: (1) altering the activity, (2) advocacy, (3) education, (4) assistive technology, (5) environmental modifications, and (6) securing timely refills.
Throughout the discussion, the interventionist is prompted to ask open-ended questions, reflect on the conversation, and affirm comments. Several components of motivational interviewing were directly built into the intervention protocol, such as the collaborative spirit, providing a summary at the end of the session, and ending with a mobilizing question.
Standard Care Intervention Group.
The standard care intervention was a 30-min, pamphlet-based educational session. In the standard care intervention group (SCIG), participants and the RA first reviewed the pamphlet Managing Your Medicines: Our Guide to Effective Medication Management (American Heart Association & American Stroke Association, 2013). Then the interventionist engaged in active listening, during which she asked open-ended questions about the participants’ medication routines and provided simple reflections. For the standard care procedures, the interventionist was prohibited from providing affirmations, complex reflections, or summaries; facilitating problem solving; or suggesting any specific interventions.
Procedure
The participants had four interactions with the research team: (1) phone screen, (2) baseline evaluation, (3) intervention, and (4) follow-up evaluation. The baseline, intervention, and follow-up sessions were audio recorded, video recorded, or both and occurred either in the participant’s home or in a shared laboratory space at the university, according to the participant’s preference.
We posted paper flyers in community spaces that serve people with chronic health conditions. We also posted study information on websites such as Craigslist. Potential participants called the PI to participate in a 5-min phone screen, during which each person answered questions about the inclusion criteria, described his or her medication adherence, and completed the Short Blessed Test. In the 1-hr double-blind baseline evaluation, the PI informed the participant about the purpose of the study. Then the participant reviewed and signed the informed consent form and completed the demographics questionnaire.
Between the evaluation and intervention, the PI adaptively randomized the participants on the basis of age, gender, and extent of medication nonadherence to the occupational therapy intervention group (OTIG) or SCIG using the protocol described by Smoak and Lin (2001). Approximately 2 wk later, the participants engaged in a single, blind, 30-min intervention with one RA according to whether the participants had been randomized to the OTIG or the SCIG.
Last, 1 mo after intervention, the participants completed a blinded 1-hr follow-up evaluation in which they completed the exit interview. A different RA completed the follow-up evaluation, so she was initially blind to the participant’s assignment. During the interview, however, some RAs were able to deduce the participant’s assignment. Use of the standardized question route helped ensure similar treatment between groups.
Data Analysis
Through close-ended questions, participants indicated (1) whether medication management intervention should be part of regular care and (2) the extent to which they perceived changes in their own medication adherence. Their answers were tabulated using descriptive statistics. Participants follow-up comments to these questions were analyzed qualitatively and were coded by magnitude (strong, moderate, or weak; Saldana, 2013).
Next, the PI used grounded theory to identify the strategies implemented by participants and to describe the participants’ perceived intervention components (Corbin & Strauss, 2008). Codes were derived from the data, often using the participants’ own words. The PI completed open, axial, and selective coding to break down the data and then to understand themes across participants’ experiences (Saldana, 2013). These codes and the number of participants who described the same sentiments are described in Table 1 for strategies used and Table 2 for perceived intervention components. All analyses were completed in Dedoose (SocioCultural Research Consultants, Los Angeles), a cloud-based application for qualitative research.
Frequency of New Strategy Implementation, by Group
Note. OTIG = occupational therapy intervention group (n = 9); SCIG = standard care intervention group (n = 10).
Intervention Components Described by Participants
Note. OTIG = occupational therapy intervention group (n = 9); SCIG = standard care intervention group (n = 10).
Data from the medication adherence diaries were used to corroborate participants’ experiences. Paired and independent-sample t tests were used to evaluate the significance of change within and between groups before and after intervention.
Trustworthiness
Trustworthiness is an indicator of validity in qualitative data. Shenton (2004) suggested that the trustworthiness of a qualitative study is measured through credibility, dependability, and confirmability.
Credibility.
The research team used several methods to improve study credibility. First, the PI entered the study with a strong background in occupational therapy, qualitative research, and medication management. Moreover, she had a strong familiarity with the phenomena through clinical practice, her experiences as a medication consumer, and her experiences as a caregiver to family members with complex chronic health conditions taking multiple medications. Tactics were also used to ensure participant honesty. For example, all interviews were prefaced with the statement, “We value your honest opinion and are interested in your experiences in this study, both good and bad.” During the data collection, data analysis, and write-up, the research team met weekly to debrief and discuss findings. Finally, the data were subject to peer scrutiny at three national conferences where the PI was able to discuss the findings and receive feedback from experts in rehabilitation.
Dependability.
Dependability addresses the stability of the results over time and across people. To improve dependability, all the RAs received the same training, used similar scripted introductions and conclusions in both interventions, and engaged with a combination of OTIG and SCIG participants. Furthermore, both interventions were heavily manualized (Schwartz, 2015). All interactions between RAs and participants were video recorded and assessed for fidelity, and blinding was used when possible. These protections helped mitigate the risk of bias, improve the dependability of the results over time and participants, and ensure that differences were due to the intervention.
Confirmability.
Triangulation and saturation of the data support the confirmability of the research. Data were triangulated across multiple sources, including an interview, a medication diary, and a series of surveys. The findings were consistent across data collection measures over different time points (Schwartz, 2015). The data also demonstrated saturation, given that many participants reported similar beliefs about the acceptability of the active intervention components.
Results
Participants
Nineteen participants with chronic health conditions completed the study: 9 in the OTIG and 10 in the SCIG (Figure 1). Participants tended to be nonworking, older, female, White, and insured. Participants often had more than one chronic health condition. Those assigned to the SCIG reported conditions including heart disease (n = 6), anxiety (n = 4), depression (n = 3), arthritis (n = 2), asthma (n = 2), diabetes (n = 1), chronic obstructive pulmonary disease (n = 1), and stroke (n = 1). Participants assigned to the OTIG reported conditions including arthritis (n = 6), diabetes (n = 5), depression (n = 4), heart disease (n = 3), asthma (n = 2), anxiety (n = 1), HIV (n = 1), osteoporosis (n = 1), and stroke (n = 1). Demographics by group can be seen in Table 3.
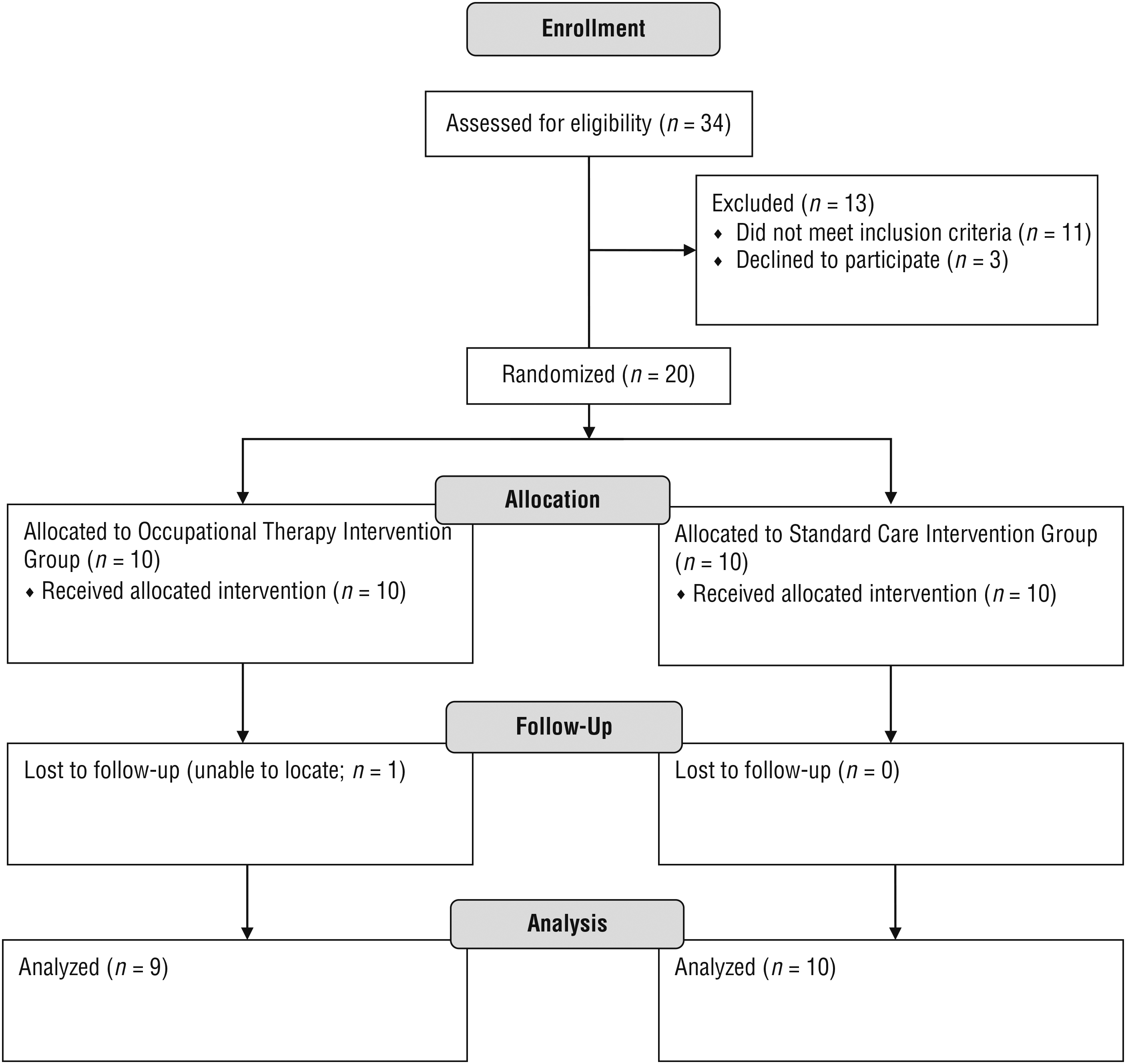
Research process and enrollment.
Demographic Characteristics of the Participants
Note. OTIG = occupational therapy intervention group (n = 9); SCIG = standard care intervention group (n = 10).
Objective 1: Acceptability
All participants in the OTIG and 90% of participants in the SCIG indicated that additional medication management services would be beneficial. For example, Participant 8 responded, “Yes, that would be great because [doctors] never ask if you are taking your pills on time, or where you keep them, or what’s going on with your medication.” Some participants went on to indicate that services may not be appropriate for everyone but may be particularly helpful to older adults, persons on a number of medications, persons on new medications, or persons with a record of poor adherence.
Objective 2: Effectiveness
Effectiveness of the intervention was described by participants’ self-perceived changes in medication management. Fifty-five percent (n = 5) of OTIG participants indicated that their ability to manage their medications had improved, but only 30% (n = 3) of SCIG participants felt they had improved. The remaining participants indicated they had stayed the same.
OTIG participants indicated a higher magnitude of change than SCIG participants, indicated by stronger language to describe their intervention experiences. They used more expressive adjectives, revealed deeper emotions, and often spoke longer. For example, Participant 8 of the SCIG stated that her medication adherence had “probably improved,” whereas OTIG Participant 2 said her medication adherence had improved because
I have a tendency at times to sway off and over take care of other people and not take care of myself, which I almost died doing that a couple of years ago, so you guys brought the alarm back to me to help me, and I really appreciate that. You’re going to make me cry. This is a present. Thank you.
Quantitative medication diaries were used to corroborate the participants’ perceived changes. According to the medication diaries, the average adherence rate in the OTIG stayed the same, changing from a mean percentage adherence of 98.58 (standard deviation [SD] = 8.53) at baseline to a mean of 98.95 (SD = 2.81) at follow-up. Percentage medication adherence in the SCIG decreased from a mean of 88.74 (SD = 22.38) at baseline to a mean of 86.06 (SD = 18.91) at follow-up. Paired and independent-samples t tests revealed no significant differences within or between groups.
We also monitored effectiveness by counting the number of reported behavioral changes after intervention. Sixty-six percent of participants in the OTIG and 40% of SCIG participants implemented new strategies. On average, OTIG participants implemented two (SD = 1) new strategies, whereas SCIG participants implemented only one (SD = 0.84) new strategy. Also, participants in the OTIG were able to identify eight types of strategies, whereas SCIG participants identified only four types of strategies implemented at home. A comparison of the strategies implemented by group is displayed in Table 1.
Objective 3: Describe the Intervention
Standard Care Intervention Group.
Participants in the SCIG identified six aspects of the standard care intervention as helpful: (1) awareness, (2) being listened to, (3) information, (4) caring, (5) feedback, and (6) validation. Most participants in the SCIG reported being more aware of medications. For example, Participant 9 reported that the process “just makes you more cognizant of your medication and when you’re taking that medication.” Participants also reported that they enjoyed being “able to tell stories and being able to talk about [their] experiences” (Participant 3). Moreover, participants liked interactions with the caring staff, saying that the RAs were “nice, respectful, and interested” (Participant 3). All participants in the SCIG received the pamphlet, but only 3 commented about the “helpful information.” Two participants felt that the feedback they received by keeping a medication adherence diary was helpful. Last, Participant 3 described feeling validated because the process “reinforced a lot of what I was doing.” Three participants reported they did not find any aspects of the standard care intervention helpful. Table 2 indicates the intervention components described by the participants.
Occupational Therapy Intervention Group.
Participants in the OTIG identified five intervention components as helpful: (1) strategies, (2) caring staff, (3) awareness, (4) feedback, and (5) validation. Most participants described how the RA helped them “develop solutions to the problems” (Participant 2). Participants then described the strategies they learned, such as alarms to remind them to take their medication, different types of pillboxes, and associating medication taking with routines. Intervention participants also noted the caring staff, but to a larger extent than the standard care participants. For example, Participant 10 made the following comments:
I think the personal conversation was always helpful. It takes it from the institutional level—and let’s not smile, and let’s not be in the moment, let’s just get the job done and move on—that’s not me. It’s a quality-of-life issue, it is called caring. It’s beyond the project. It takes so little to do that, and it’s so important.
Similar to SCIG participants, the OTIG participants reported that the intervention helped them become more aware of their medication routine, better self-monitor their adherence, and feel validated about their current routines. The intervention components between the intervention groups are compared in Table 2.
Discussion
Occupational therapy researchers have previously identified the role for the profession in medication management through theory and observational studies (Foster, 2014; Radomski, 2011; Sanders & Van Oss 2013; Schwartz & Smith, 2017). Limited research supports occupational therapy intervention in medication management (Chase, Mann, Wasek, & Arbesman, 2012; Haltiwanger, 2012; Yuen, 1993). In this Phase I study, we used within- and between-group comparisons to create a foundation for occupational therapy medication management intervention research; specifically, we qualitatively evaluated the acceptability, effectiveness, and active intervention components of a novel manualized occupational therapy intervention among persons with chronic health conditions and poor medication adherence.
Historically, doctors, nurses, or pharmacists have been responsible for addressing a person’s ability to take his or her medications as prescribed. In their recent review of the literature, Nieuwlaat et al. (2014) posited that there is a growing role for allied health professionals. Although occupational therapy practitioners are allied health professionals, it was unclear (because of a lack of literature and practice in this area) whether participants would accept an occupational therapy medication management intervention. Our results suggest that almost all participants (n = 18, 95%) believed that additional services are needed to help people manage their medications. This indicates that both the topic of medication adherence and the intervention are acceptable to clients with chronic health conditions on multiple medications.
The second objective was to identify whether the intervention was effective enough to warrant future research. The findings revealed that intervention facilitated new medication management habits and routines. Changes in habits and routines are associated with improved adherence because most participants in the OTIG (n = 5; 56%) believed that their ability to take their medications had improved as a result of the intervention, compared with 30% (n = 3) of participants in the SCIG. The results were supported by the single-subject analyses of the medication diary data (Schwartz & Smith, 2016). The single-subject data demonstrated that, of participants with valid medication diaries, 50% of the OTIG demonstrated significant improvements in medication adherence, compared with 14% of the SCIG (Schwartz & Smith, 2016). The results are also consistent with previous occupational therapy medication management research (Chase et al., 2012; Haltiwanger, 2012; Yuen, 1993). More research on this occupational therapy medication management intervention is warranted.
The third and last objective was to better define the intervention components. Before this study, the research team developed the IMedS intervention, which is based on theory, evidence, and best practice, resulting in an intervention with the following components: goal setting, motivational interviewing, altering the activity, advocacy, education, assistive technology, environmental modifications, and discussion of refills (Medication Management Research Project, 2014). Through interviews, the research team compared the intended intervention components with those perceived by the participants and found that many intervention components were received as delivered. Three intervention components—refills, altering the activity, and goal setting—did not resonate with the participants.
The participants in the present study identified two additional intervention components. First, several mentioned that the feedback they received through self-monitoring their medication adherence in the diary helped them to better take their medications. Second, participants suggested that good therapeutic rapport (identified by comments about caring staff, feelings of validation, and being listened to) facilitated the effectiveness of the intervention. Although therapeutic rapport is an underpinning of good occupational therapy practice, participants in this study indicated the importance of this skill as a component of the intervention. We believe that the strong sense of therapeutic rapport was facilitated by the motivational interviewing techniques used throughout the interventions. RAs who administered the occupational therapy intervention were coached to ask open-ended questions and provide affirmations, reflections, and summaries; therefore, it is likely that these techniques better conveyed the RAs’ interest in and concern for the person. Through the initial manualization and participant interviews, we successfully described the intervention.
Richardson et al. (2014) charged allied health professionals to better describe their distinct contributions to health interventions. The different outcomes between groups in this study suggest that professional training plays a role in the effectiveness of the intervention. Although participants in both groups gained exposure to similar information (e.g., the importance of using pillboxes, moving medications to more visual locations), participants in the OTIG were more likely to implement new strategies at home. This suggests that skilled delivery of the intervention by the occupational therapy professional (and his or her skills, background, and abilities) is an important component of the intervention.
Limitations and Next Steps
This study describes the experiences of a purposeful yet biased sample of 19 people with chronic health conditions. At this time, the results cannot be generalized to other people or settings. However, this study does provide a proof of concept that occupational therapy can improve medication management and medication adherence in some adults with chronic health conditions and poor medication adherence. Moreover, the findings suggest that it is the skills of the occupational therapy practitioner that make the intervention effective. Occupational therapy scholars have the opportunity to demonstrate the distinct value of the profession through increased research in the field. More research across domains of occupational therapy and medication adherence is needed.
Additional research is also warranted for the IMedS intervention. IMedS successfully met the criteria for a Phase I study and will benefit from Phase 2 research. Specifically, IMedS should progress to future studies with larger, more diverse samples; longer follow-up periods; and settings with higher external validity. Research is also needed to determine optimal dose and frequency of this behavioral intervention. In addition, future investigations should account for changes in functional outcomes and overall health.
Conclusion
Many people with chronic health conditions are not living healthy, productive lives because of the consequences of medication nonadherence. The medication adherence field combines the expertise of many health care professionals, but published research has not reflected the contribution of occupational therapy interventions. This study exemplifies why occupational therapy services are needed in this well-studied field. In this study, the OTIG participants demonstrated greater self-perceived improvements, developed more medication management strategies, and implemented more strategies at home than did participants in the SCIG. Moreover, participants indicated that the occupational therapy profession’s expertise in client education, advocacy, assistive technology, environmental modifications, self-monitoring, and therapeutic communication facilitated the intervention. Occupational therapy practitioners possess the opportunity and skills to improve clients’ medication adherence. Participant 5 indicated how the intervention helped her and described the important role of occupational therapy in improving medication nonadherence:
Because sometimes you do things sort of automatically, like taking pills—that gets pretty automatic after a while, and you forget there are all kinds of things you might be overlooking because you are so familiar with it. I think the questions I was asked made me think about, wait a second, you could do something different here.
Implications for Occupational Therapy Practice
An evaluation and 30 min of an occupational therapy intervention can lead to self-perceived improvements in medication management in adults with chronic health conditions. Although the occupational therapy intervention described in this study was not effective for everyone, it is brief and easy to administer and was associated with few drawbacks. Considering the risks and the benefits, occupational therapy practitioners may integrate evaluation and intervention of medication management into their practice with people with chronic health conditions so they can begin to address the needs of the 30%–50% of medication consumers with poor adherence (Osterberg & Blaschke, 2005). This study has the following implications for occupational therapy practice:
Occupational therapy practitioners can help clients improve their medication management through interventions related to advocacy, education, assistive technology, environmental modifications, and self-monitoring.
Good rapport and therapeutic communications skills help occupational therapy practitioners deliver skilled interventions that enable clients to self-generate and implement solutions to their occupational performance deficits.
Footnotes
Acknowledgments
This research was conducted at the University of Wisconsin–Milwaukee. It was funded by the Distinguished Dissertation Fellowship from the Graduate School at the University of Wisconsin–Milwaukee and a Student Research Grant Award from the College of Health Sciences at the University of Wisconsin–Milwaukee. This article was written in partial fulfillment of the requirements for the PhD degree in health sciences at the University of Wisconsin–Milwaukee. Jaclyn K. Schwartz thanks her dissertation committee members, Michael Brondino of the Helen Bader School of Social Welfare, Ron Cisler of the Center for Urban Population Health, Brian Schermer of the School of Architecture and Urban Planning, and Virginia C. (Ginny) Stoffel of the Department of Occupational Science and Technology. This study is registered under ID No. NCT02706548 at ![]() .
.