
Abstract
Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder affecting 5% of school-age children (American Psychiatric Association, 2013). ADHD is characterized by significant difficulties with executive functions (EFs), defined as self-regulation constructs for effective self-management to attain one’s goals. Included among EFs are emotional, cognitive, and behavioral regulation, such as inhibition and working memory (Barkley, 2012; Brown, 2013). Participation in occupations of personal care, household chores, academics, leisure, and social domains is often impeded by executive dysfunction among children with ADHD (Antshel, Hier, & Barkley, 2014; Biederman et al., 2004; de Schipper et al., 2015; Tseng & Gau, 2013).
The impact of neurocognitive deficits on participation among people with a variety of acquired or developmental disorders has been addressed by cognitive rehabilitation models in occupational therapy (Katz, 2011). Evidence has shown that these models have been effective for populations with EF impairment (Dawson et al., 2009; Polatajko, Mandich, & McEwen, 2011; Toglia, Johnston, Goverover, & Dain, 2010); however, they have not been systematically applied to children with ADHD (Cermak & Maeir, 2011). The Cognitive Orientation to daily Occupational Performance (CO–OP; Polatajko et al., 2011) is an important treatment approach that includes a major focus on metacognitive strategies within an occupational context. Although there is ample evidence for the use of the CO–OP approach for children with developmental coordination disorder (Polatajko et al., 2011), aside from a case study of a child with ADHD in which the CO–OP approach was used (Polatajko & Mandich, 2004) and a study in which the influence of this approach on motor-based occupational performance of children with ADHD was examined (Gharebaghy, Rassafiani, & Cameron, 2015), little evidence exists for its efficacy for children with ADHD.
In other studies, promising results have been shown. Halperin et al. (2012) conducted a study in which young children with ADHD attended play groups designed for cognitive enhancement, while their parents attended separate sessions comprising psychoeducation and group support. Parent and teacher ratings on ADHD symptoms pointed to significant improvement after treatment, with maintenance at 3-mo follow-up. Tamm, Nakonezny, and Hughes (2014) taught parents to administer a metacognitive EF training intervention to their young children with ADHD. The program was found to be feasible and well-accepted by participating parents.
The Cognitive–Functional (Cog–Fun) intervention for children with ADHD was developed on the basis of cognitive rehabilitation models in occupational therapy (Maeir, Hahn-Markowitz, Fisher, & Traub Bar-Ilan, 2012) and targets the cognitive, emotional, and environmental barriers to participation as they interact in an occupational context. This approach is in accordance with the International Classification of Functioning, Disability and Health (World Health Organization, 2001), which delineates the multidimensional bio–psycho–social implications of health conditions. The primary aim of Cog–Fun is to promote the acquisition of executive strategies and self-efficacy in occupational performance. Internalization of strategies is best achieved when children (1) learn to use them in their occupational context and language, (2) use them during enjoyable activities, and (3) experience them as tools that are worth the effort to use (Maeir, Fisher, et al., 2014; Maeir, Hahn-Markowitz, Fisher, & Traub Bar-Ilan, 2014).
This integrative approach relies on established occupational therapy practice models and harnesses three key change mechanisms: (1) executive strategy acquisition, (2) an enabling therapeutic setting, and (3) the use of environmental supports and procedural learning. Cog–Fun integrates learning and practicing executive strategies and behavioral skills within the context of playful activities and daily functioning. Supporting evidence for the effectiveness of Cog–Fun in improving EFs, self-efficacy, and participation was found in initial pilot studies (Hahn-Markowitz, Manor, & Maeir, 2011; Maeir, Fisher, et al., 2014; Maeir, Hahn-Markowitz, et al., 2014). Our aim in this study was to further examine the effectiveness of the Cog–Fun intervention for children with ADHD and its effect on EFs and participation in a randomized controlled crossover study.
Method
Research Design
In this study, we used a randomized controlled trial with a crossover design to examine the impact of the Cog–Fun intervention on school-age children with ADHD. Ethical approval for the study was obtained from the Helsinki committees of the two participating urban medical centers. Parents provided informed consent, and children provided assent.
Participants
The medical directors of the participating clinics referred children diagnosed with ADHD according to Diagnostic and Statistical Manual of Mental Disorders (4th ed.; American Psychiatric Association, 1994) criteria to the study. Inclusion criteria were age 7–10 yr, in Grades 2–4 at first assessment, enrollment in regular schools, stability in medication or no-medication status or other treatments for ADHD for the previous 2 mo, and executive dysfunction in daily life determined by the score (t score ≥ 65) on at least one subscale of the Parent version of the Behavior Rating Inventory of Executive Function (BRIEF; Gioia, Isquith, Guy, & Kenworthy, 2000) questionnaire. Exclusion criteria included intellectual disability, other chronic medical and neurological conditions, and primary psychiatric diagnosis (e.g., depression, anxiety, psychosis).
Instruments
Behavior Rating Inventory of Executive Function.
The BRIEF is an 86-item ecological rating scale completed by a parent or teacher, designed to reflect the neuropsychological constructs of EFs in everyday situations among children age 5–18 yr. It consists of eight subscales (Inhibit, Shift, Emotional Control, Initiation, Working Memory, Plan/Organize, Organization of Materials, and Monitor), two indices (Behavioral Regulation Index and Metacognitive Index), and a Global Executive Composite. Items are rated 1 (never), 2 (sometimes), or 3 (often). Raw scores are converted to t scores, with 65 or more considered clinically impaired (standard deviation = 10). Internal consistency, test–retest reliability (r = .72–.84 for Parent version over 3 wk), and discriminant validity have been established for children with ADHD, as well as convergent and concurrent validity (Gioia et al., 2000; Mahone et al., 2002; McCandless & O’Laughlin, 2007).
Canadian Occupational Performance Measure.
The Canadian Occupational Performance Measure (COPM; Law et al., 2005) is a semistructured, client-centered measure designed to help identify occupational difficulties and to detect change in daily occupational performance, on a 10-point scale, with a change of 2 points considered clinically significant. The COPM is standardized, valid, and reliable, with test–retest reliability of r = .80 for performance over 1–2 wk (Law et al., 2005). Parent ratings of the child’s performance on occupational goals defined over the course of therapy and after treatment completion are reported here as a measure of participation (Dunn, Cox, Foster, Mische-Lawson, & Tanquary, 2012).
Procedure and Data Collection
Attending physicians briefly described the study to parents of children who they deemed good candidates, and they provided the study coordinator (first author) with a list of parents who agreed to be contacted. The mothers of children who were referred received a telephone explanation by the study coordinator regarding the conditions of the study and to determine whether they were interested in participation. If oral consent was given, they were asked to complete the BRIEF questionnaire and were invited to an interview, where they received a complete description of the study and provided written consent. If the scores on the questionnaire were greater than the cutoff, the family was invited to participate in the study. Children were assigned randomly according to blocks (age group and gender) to intervention or wait-list control groups.
Twelve occupational therapists (9 in one clinic and 3 in the other) treated the child–parent dyads. Participants in the intervention group commenced Cog–Fun treatment after baseline, whereas those in the control group received no treatment. Three months later, participants in both groups underwent Assessment 2, after which crossover occurred. Assessment 3 (postintervention for controls and follow-up for intervention participants) took place at the end of an additional 3 mo (Figure 1).
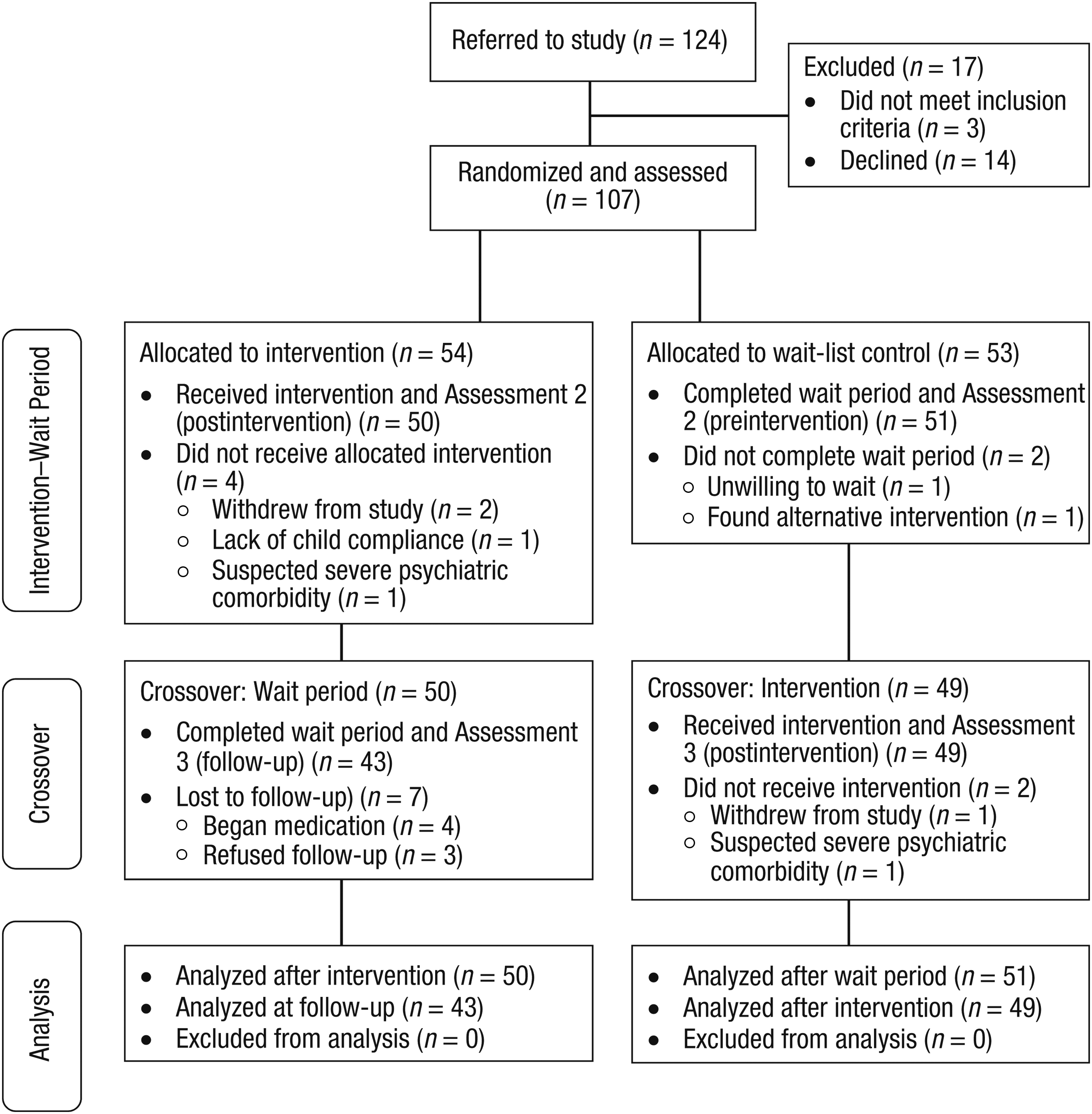
Participant flow diagram for the Cognitive–Functional intervention.
Parents completed the BRIEF at each assessment period, whereas the COPM was administered during treatment and at its conclusion (and not at the wait-list baseline assessment). Some occupational goals were not directly addressed in treatment because of various reasons such as clients’ priorities or treatment resources. These goals were designated “transfer goals” to examine whether performance would improve in an occupation beyond those dealt with in treatment. Blinding was not possible because of the nature of the study, except at baseline assessment, before randomization.
Cognitive–Functional Intervention
The Cog–Fun is a manualized approach (Maeir et al., 2012) that supports participation via metacognitive learning of executive strategies (e.g., stop, recruit effort and persist, check, plan) in an enabling context. It is administered by licensed occupational therapists with Cog–Fun certification, which is awarded on successful completion of a 6-mo, 60-hr theoretical training course and a 4-mo practicum.
In the current study, each occupational therapist completed a therapist’s log for each treatment session, which was examined by the study coordinator to verify fidelity of treatment. The program involves 12 consecutive 1-hr weekly sessions with child and parent in which the occupational therapist introduces executive strategies one at a time in a nonthreatening, playful atmosphere. The number of strategies learned over the course of treatment and the use of adaptations are tailored to the child’s cognitive and emotional profile as well as occupational goals. The strategies are practiced and applied to individualized functional goals that are meaningful to the child and parents. The goals are gradually introduced in therapy as the ecological context for strategy transfer. For example, the inhibit strategy is acquired and practiced in games such as “Red Light, Green Light, One, Two, Three” that are simulated in a social context identified as challenging to the child, such as “will wait until friend finishes her turn during a game before taking a turn.”
The parent plays a major role in Cog–Fun, attending each session to experience positive engagement with the child in playful activities, to learn the metacognitive language, and to provide necessary modifications (i.e., preparing materials in advance, reducing clutter and distractions) and supports (i.e., positive verbal mediation, daily planner, timer, checklists) to promote successful occupational performance and transfer of strategy use to the home. A weekly communication session by phone or email between the treating occupational therapist and parents is scheduled between sessions to support implementation of the program. In addition, one session is conducted in the home to help the occupational therapist further understand the child in his or her ecological setting and to facilitate transfer of learning.
A unique aspect of the intervention is the combination of structure with flexibility. The structure provides the necessary lucidity and supports to enable effective learning for families with a child with ADHD, whereas the flexibility allows for the unique individual executive and functional profile of each client. The protocol consists of seven intervention units: an evaluation unit, four units of executive strategy acquisition, a home visit, and a summary unit (Hahn-Markowitz, Berger, Manor, & Maeir, 2016).
Hypotheses
In this study, we proposed the following hypotheses:
Hypothesis 1: Significant Time × Group (research and wait-list control) interaction effects will be found on the BRIEF from baseline to Assessment 2.
Hypothesis 2: Significant time effects on the BRIEF and parent COPM will be found after crossover (replication of the treatment effect), with no Time × Group interaction.
Hypothesis 3: Treatment effects will be maintained at follow-up for the research group, with no significant changes.
Data Analysis
The data were analyzed with IBM SPSS Statistics (Version 19; IBM Corp., Armonk, NY). Descriptive statistics were carried out to present sample characteristic as well as BRIEF and COPM ratings. An analysis of variance was performed to compare the intervention and control groups on personal characteristics. Two mixed-effects multivariate analyses of variance (MANOVAs) with the within-subject main effect of time and the between-subjects main effect of group were performed: first, to examine the effect of treatment compared with wait-list controls on the BRIEF subscales and, second, to examine the effect of treatment after crossover in both groups on the BRIEF subscales and COPM. Significance was set at a level of .05. Effect sizes were represented by partial η2, with η2 of .04 considered a minimum practically significant effect, partial η2 between .04 and .24 considered a moderate effect, and a partial η2 of more than .24 considered a strong effect size (Ferguson, 2009).
Results
Parents of 107 children completed the BRIEF before randomization. Eight children left the study before treatment: 5 children dropped out of the study, and 1 child was excluded after baseline; additionally, 1 more child dropped out, and another child was excluded after Assessment 2, both from the control group. Ninety-nine children received treatment, and none dropped out after intervention had commenced. Eleven children in the research group and 10 children in the control group were receiving ongoing additional treatments for ADHD (art therapy, equestrian therapy, remedial education, psychotherapy, homeopathy, animal therapy, drama therapy). There was no significant difference in any sample attribute across groups (p > .05; Table 1).
Participant Characteristics at Baseline
Note. No significant difference existed at baseline between the intervention and control groups. M = mean; SD = standard deviation.
Occupational Goals
Each child–parent dyad defined an average of three occupational goals on the COPM in activities of daily living (ADLs), social participation, and academic and leisure domains. EF deficits typical of ADHD were reflected in their identified goals. The majority of goals portrayed difficulties in inhibition, followed by difficulties recruiting effort, monitoring performance, and planning. Examples of occupational goals and strategies in the different realms are as follows:
Social Participation: “I will wait until my friend finishes her turn (in game) before taking my turn.” (inhibit strategy); “I will make an effort to find a solution when my brother and I both want the [tablet] at the same time.” (recruit effort and persevere strategy)
ADLs: “I will check that all the shampoo is rinsed out of my hair before calling Mom.” (check strategy); “I will plan with Mom what sandwiches to take to school.” (plan strategy)
Academics: “I will turn off the TV after one program.” (inhibit strategy); “I will check to make sure that I return materials to their places after I finish doing my homework.” (check strategy)
Leisure: “I will make an effort to entertain myself for at least 15 minutes in the afternoon.” (recruit effort and persevere strategy); “I will plan an after-school activity from a list that Mom and I prepared.” (plan strategy).
Nineteen of the child–parent dyads had an additional transfer goal that was not addressed directly in treatment. Results for transfer goals were analyzed separately.
Before Crossover (Time 2): Time × Group Interaction Effects
At Assessment 2, mean scores for the intervention group on the BRIEF subscales improved by an average of 4.90 t points, whereas mean scores for the control group remained essentially unchanged. The overall MANOVA interaction effect between the intervention and control groups from baseline to Assessment 2 on the BRIEF subscales was Wilks’s Λ F (8, 92) = 3.82, p = .001. Significant univariate interaction effects were found on all BRIEF subscales, except on Working Memory and Monitor (Table 2).
BRIEF Comparisons From Baseline to Assessment 2 (Group × Time Interaction Effect)
Note. Executive dysfunction in daily life was determined by a t score ≥ 65 on at least one subscale of the Parent version of the Behavior Rating Inventory of Executive Function (BRIEF). Lower scores signify improvement on the BRIEF. M = mean; SD = standard deviation.
After Crossover (Time 3): Treatment Gains
Replication of the treatment effects was demonstrated on both measures after crossover (Table 3), with no significant interactions between groups. The overall MANOVA within-subject time effect (pre–post treatment) on the BRIEF subscales was Wilks’s Λ F (8, 90) = 10.90, p = .000, and the Time × Group interaction effect was not significant, F (1, 93) = 0.42, p = .907. Significant univariate time effects were found on all the BRIEF subscales with moderate to large effect sizes. Similarly, a significant time effect was found for the COPM including the transfer goals, with large effect sizes. Post hoc analyses of possible intervening variables (gender, medication status, age group, ADHD subtype, mother’s education level, or treatment site) revealed no significant interaction of these variables with the treatment effect (all ps > .05). Frequency analyses of number of participants who achieved positive–negative outcomes revealed that the overarching majority attained their goals and demonstrated improvements in their BRIEF scores. However, 6 children (3 in each group) did not demonstrate these positive outcomes.
BRIEF and COPM Performance After Crossover (Intervention Effect)
Note. Executive dysfunction in daily life was determined by a t score ≥ 65 on at least one subscale of the Parent version of the Behavior Rating Inventory of Executive Function (BRIEF). Lower scores signify improvement on the BRIEF. COPM = Canadian Occupational Performance Measure; M = mean; SD = standard deviation.
Degrees of freedom = 1, 97.
Degrees of freedom = 1, 17.
Discussion
The findings support the efficacy of the Cog–Fun occupational therapy intervention for improving EFs and participation among children with ADHD. Significant Time × Group interactions were found for EFs, confirming that positive effects cannot be attributed to time because the controls did not improve and, in some cases, worsened before crossover. The positive treatment effects in the intervention group were reproduced among controls after crossover. Thus, effects cannot be attributed to a random occurrence, to one sample, to a particular therapist, or to treatment site because findings were consistent across both sites and for all therapists. These results corroborate the findings of previous studies (Hahn-Markowitz et al., 2011; Maeir, Fisher, et al., 2014; Maeir, Hahn-Markowitz, et al., 2014) and substantiate the impact of Cog–Fun on parent-reported outcomes.
BRIEF scores after treatment mirror the parents’ perceptions of their children’s improved ability to self-regulate in the context of daily challenges in the home. COPM scores after treatment reflect the parents’ perceptions of their children’s improved participation in daily tasks, including transfer goals. Analysis revealed that transfer goals were no different from all other goals defined, and they were achieved with a large effect size. This finding could reflect success of the program in facilitating transfer of strategy use. However, these results should be interpreted with caution because not all the children had defined transfer goals.
Hypothesized Change Mechanisms
The positive outcomes may have been related to several change mechanisms related to the child and parent. Parent factors may include (1) realistic goal setting at the outset, (2) learning EF strategies and integrating them into daily language within the family context, and (3) noticing and supporting the child’s efforts to apply executive strategies when trying to achieve his or her goals and providing environmental adaptations. Child factors may include (1) effective acquisition of executive strategies, (2) increased repertoire of performance skills, and (3) improved self-efficacy. It is hypothesized that these mechanisms together contributed to narrowing the gap between occupational demands and child factors, thereby improving outcomes. These hypothesized change mechanisms are supported in education and rehabilitation literature. Recent research supports the impact of goal setting when comparing the academic performance of students who set personal best goals versus students who did not (Martin & Elliot, 2016).
Regarding the impact of strategy use on occupational performance, according to the Multicontext Treatment Approach (Toglia, 2011), the mechanisms include development of internalized language with awareness of the need for strategies, practice, and skill in strategy implementation. Modest supporting evidence for the far transfer of strategy training was demonstrated in application of the CO–OP to adults with brain injury who improved significantly more than controls on satisfaction and performance on untrained goals (Dawson, Binns, Hunt, Lemsky, & Polatajko, 2013). As to the hypothesized role of the parents, Piškur et al. (2012) found that the parents’ role in their child’s therapy enabled and supported performance of meaningful activities as well as facilitating, changing, and using the environment.
However, in light of anecdotal reports of some of the therapists in their logs, it is hypothesized that parent factors accounted for lack of treatment gains among 6 children, such as poor goal setting and lack of parent availability for significant learning or for supporting their child. Note that these parents were not perceived as noncompliant; rather, they expressed difficulty (i.e., lack of resources) in carrying over what was done in therapy to the home.
Limitations and Recommendations for Future Studies
The study has several limitations. The intervention was compared with wait-list controls and not to another treatment, such as parent education or another behavioral intervention. The sample comprised primarily educated, married parents; therefore, it may not be representative of the entire population of children with ADHD. The parents’ involvement in treatment may have served as a source of bias in its favor. Future studies that analyze Cog–Fun’s change agents (i.e., the therapeutic interaction with parents and child, the process of strategy acquisition, and specific skill-based learning) are recommended. Studies in which Cog–Fun is compared with another intervention are also recommended, as are studies in which Cog–Fun is used with other populations of children with chronic health situations.
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy practice:
Executive dysfunction among children with ADHD impedes their participation in typical occupations. Cog–Fun targets the effects of these deficits in an integrative approach.
Evidence supports the effectiveness of Cog–Fun in improving EFs and participation among children with ADHD.
The BRIEF and COPM are valid, occupation-based measures that can guide occupational therapy treatment and that are sensitive to changes affected by treatment.
Conclusion
This study contributes to the body of knowledge about occupational therapy interventions for children with ADHD and their parents. Participation among these children has been shown to be affected by EF deficits that are associated with ADHD. Cog–Fun offers an integrative approach that supports participation and targets EFs through metacognitive learning in an enabling environment. Occupational therapists play an important role in analyzing the occupational and executive profiles of children with ADHD and using the Cog–Fun intervention to help improve EFs and participation.