
Abstract
Children with pediatric acute-onset neuropsychiatric syndrome (PANS) experience sudden-onset neuropsychiatric symptoms, including obsessive–compulsive behaviors and restricted eating, after infection, environmental, or metabolic triggers (Murphy, Kurlan, & Leckman, 2010; Swedo, Leckman, & Rose, 2012). Additional problems may include attention problems, sensory defensiveness, dysgraphia, math regression, urinary frequency, and emotional lability (Swedo et al., 2012). The National Institute of Mental Health has taken a strong interest in PANS, and its director called this syndrome a “frontier” in mental health (Insel, 2010). To date, there have been no published studies of the full range of occupational performance limitations in children with PANS, making this a frontier for occupational therapy as well.
Background
In the mid-1980s and early 1990s, Swedo and colleagues (1989) identified ongoing obsessive–compulsive disorder (OCD) behaviors in children who recovered from Sydenham’s chorea (SC), an autoimmune neurological disorder involving involuntary movements after Group A Streptococcus (GAS) infections, such as strep throat. In SC, antibodies produced to fight GAS are thought to cross the blood–brain barrier and react with basal ganglia neurons, triggering neurochemicals including calcium/calmodulin–dependent protein kinase II (CaM kinase II), which is involved in dopamine production (Kirvan, Swedo, Heuser, & Cunningham, 2003).
In 1995, Allen, Leonard, and Swedo identified 4 boys with sudden-onset OCD and tics after either GAS or viral infection who improved with immune-modulating treatments, and they called the disorder pediatric infection-triggered autoimmune neuropsychiatric disorder (PITAND). Working with the known GAS model for SC, Swedo and colleagues (1998) later identified pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS) while studying 50 children with sudden-onset tics or OCD after a GAS infection. Similar to SC, blood serum from these children indicated that antibodies produced to fight GAS resulted in increased CaM kinase II (Kirvan, Swedo, Snider, & Cunningham, 2006). Swedo et al. (2012) introduced the term PANS to refer to children with sudden onset of obsessive–compulsive and other neurobehavioral symptoms, including children with PITAND, children with PANDAS, and children with exacerbations that are due to environmental or metabolic triggers.
Similar to SC, episodes of PANS are thought to be related to the following items:
A genetic predisposition to an abnormal immune response;
The creation of an antibody that interferes with neuronal tissue, triggered by infection with Streptococcus (PANDAS) or other bacterial or viral infections (PITAND); and
A breach in the blood–brain barrier, thought to be due to inflammation that allows the antibody to reach neuronal tissue and interfere with functioning (Swedo et al., 2012).
Although some children experience only one PANS exacerbation, many children experience subsequent exacerbations in a relapsing and remitting pattern (Murphy, Gerardi, & Leckman, 2014). Subsequent infections or causes of inflammation may trigger sudden and severe repeat exacerbations, with gradual return of function following a “saw-toothed” pattern when plotted over time (Swedo et al., 2012), which may not reach full return to baseline, leaving some children with ongoing impairment after exacerbation.
Occupational Performance Limitations
Researchers have reported sudden-onset sensory defensiveness, sleep disturbances, dysgraphia, inability to concentrate, separation anxiety, urinary frequency, food refusal, and rages during exacerbations (Frankovich et al., 2015; Murphy et al., 2015; Swedo et al., 1998, 2012, 2015), whereas parents have discussed difficulties in many aspects of daily living on parent forums. Developing a complete picture of the occupational performance needs of children with PANS is critical. Occupational performance deficits during exacerbation may be addressed by rehabilitation clinicians. Common patterns of occupational performance needs could also be used by physicians during diagnosis and could help health and education professionals working with children with sudden-onset symptoms to recognize potential cases of PANS, improving referral to physicians for diagnosis. Moreover, common patterns could serve as a basis for development of objective measures of exacerbation severity and as a basis for measuring effectiveness of interventions.
To develop such an understanding, we used the Occupational Therapy Practice Framework: Domain and Process (2nd ed.; American Occupational Therapy Association [AOTA], 2008) because it broadly identifies daily occupations in which children and families engage and the body functions and performance skills required for engagement. 1 The Framework is based on the World Health Organization’s (2001) International Classification of Functioning, Disability and Health; therefore, the language is understandable by professionals from a variety of disciplines. In this study, we used an online retrospective parent survey based on the Framework. Defining PANS exacerbation as “a period of marked deterioration in function associated with an infectious incident,” we sought to answer the following questions:
According to parents, what are the occupational performance, body function, and performance skill deficits experienced by children with PANS during exacerbation?
What is the severity of these deficits during exacerbation?
What additional comments do parents share regarding PANS exacerbations?
Method
In this mixed-methods study, we used an online, researcher-developed survey for parents of children identified by a physician as having PANDAS, PITAND, or PANS. When being developed, the online parent survey was reviewed by an occupational therapist and a neuroscience researcher specializing in PANDAS. This initial survey was pilot tested on 5 parents of children with PANDAS, PITAND, or PANS to establish face validity. The survey first asked neutral dichotomous questions indicating whether a child had a problem in each area during exacerbation. If parents indicated a problem was experienced in an area, they were prompted to respond to Likert-scale questions to indicate the degree of difficulty. An open-ended comment box for each question was included to allow parents to further describe the situation if desired.
After approval from the University at Buffalo’s institutional review board, we recruited parents using convenience sampling via an email invitation from a PANS parent support group, postcards sent to PANS physicians to share with families, and postcards for participants at a PANS parent workshop. After informed consent, the 20- to 40-min survey included demographic questions followed by dichotomous matrices asking parents whether their child had or had not experienced a decline in function during exacerbation in seven activities of daily living, one instrumental activity of daily living, five educational areas, four leisure areas, six mental functions, seven sensory functions, and three neuromuscular functions.
If an area was problematic, parents were asked to rate the child’s functioning during exacerbation on a 4-point Likert scale: 1 = The child did NOT display a problem in this area; 2 = The child displayed MILD DIFFICULTY in this area, but most people would not notice; 3 = The child displayed MODERATE DIFFICULTY in this area and required assistance and/or adaptation to remain functional; and 4 = The child displayed SEVERE DIFFICULTY in this area and was unable to function at a typical level, even with assistance and adaptation. Parents also provided optional comments throughout the survey to clarify or to expand on information; these comments provided the qualitative data in this study.
Quantitative analysis with IBM SPSS Statistics (Version 20; IBM Corp., Armonk, NY) included descriptive statistics for frequencies of all demographic variables and the percentages of children who experienced occupational performance limitations during exacerbation. Two occupational therapists familiar with PANS reviewed the optional parent comments describing limitations in each area of occupation, body function, and performance skill. These comments were compiled, coded into subcategories, reviewed again, and distilled further into themes, all of which was then reviewed by a third occupational therapist familiar with PANS for validity. Any discrepancies were discussed among the three reviewers until consensus was reached.
Results
Demographics
Information was gathered on 111 children (75 boys, 35 girls, 1 unstated; Table 1). Boys composed most of the sample, 67.60% (n = 75), as did children who were White non-Hispanic (n = 95) and those with a family income of $75,000 per year or greater (n = 85). The group ranged in age from 3 to 21 yr, with a median age of 10 yr for boys and 10.50 yr for girls. The range of ages at diagnosis with PANS was from 2 yr to >18 yr, with a median age of 8 yr for boys and 7 yr for girls. The age at which children showed the first signs of PANS ranged from <1 yr to 16 yr, with a median age of 5 yr for boys and 6 yr for girls (Table 1).
Summary of Demographic Information of Children With PANS (N = 111)
Note. Blank cells indicate that the category is not applicable. ADHD = attention deficit hyperactivity disorder; DO = Doctor of Osteopathic Medicine; MD = Doctor of Medicine; Mdn = median; PANS = pediatric acute-onset neuropsychiatric syndrome.
Research Question 1: Types of Limitations in Occupational Performance During Exacerbation
All surveyed areas of occupation (activities of daily living, one instrumental activity of daily living, school functions, and play and social participation) and each body function and performance skill (neuromusculoskeletal and movement-related functions and motor skills, sensory functions, mental functions, and process skills) were reported to be problematic for at least some children during exacerbation. In all, 109 of the 111 children (98.2%) experienced a problem in at least one area of occupation, 106 (95.5%) experienced a problem in at least one mental function, 79 (71.2%) experienced a problem in at least one sensory function, and 55 (49.5%) experienced a problem in at least one neuromuscular function. Figures 1 and 2 show the number of children for whom each area was not a problem (lightest shade of each bar at the bottom) and the number of children for whom each area was problematic at a mild, moderate, or severe level (darker shaded areas toward the top of each bar).
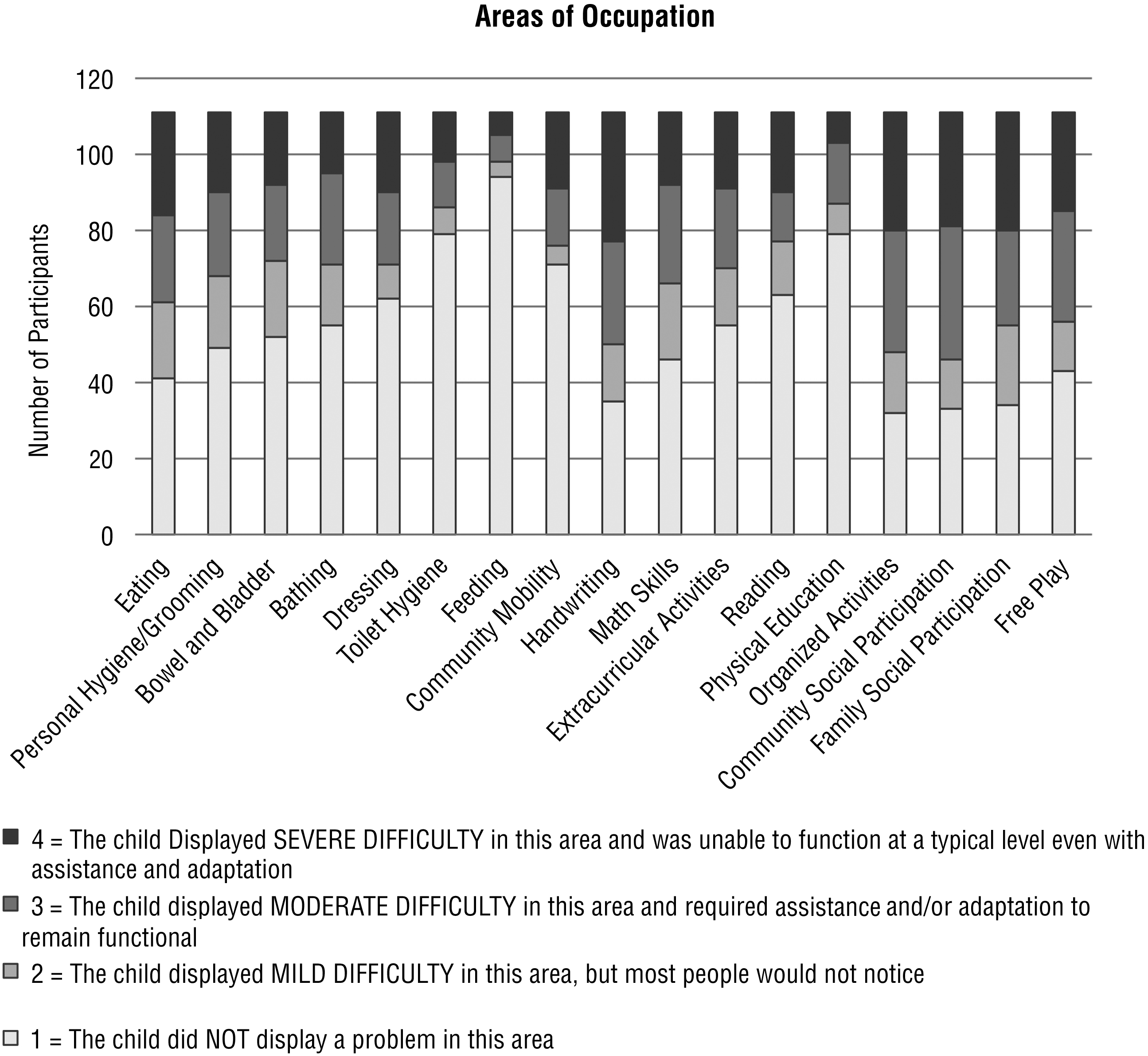
Parent report of difficulty in areas of occupation during exacerbation (N = 111).
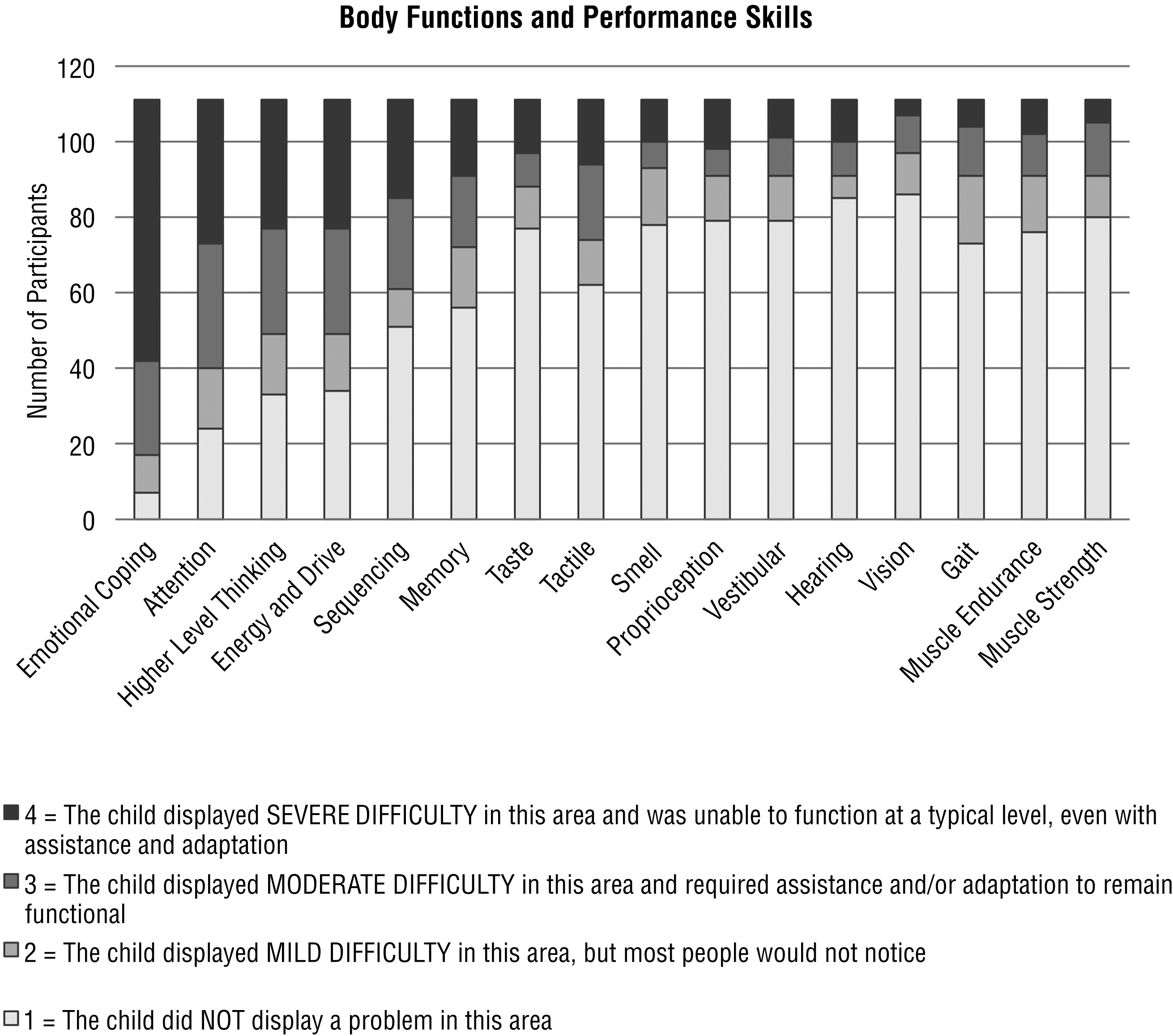
Parent report of difficulty in body functions and performance skills during exacerbation (N = 111).
More than 90% of the 111 children reportedly experienced deterioration in emotional coping during exacerbation, and more than half experienced deterioration in eating, personal hygiene and grooming, bowel and bladder management, bathing, handwriting, math, extracurricular and organized activities, community and family social participation, and free play. During exacerbation, more than half reportedly experienced difficulty in attention, higher level thinking, energy, and drive, as well as sequencing and memory. Although the vast majority of children experienced some type of sensory deficit, the specific sensory systems involved were widespread, with about 39% reporting problems with touch, and less than one-third reporting problems with taste, smell, the vestibular system and proprioception, hearing, and vision and seeing (see Figures 1 and 2).
Research Question 2: Severity of Limitations in Occupational Performance During Exacerbation
Of the children reported to have difficulty with areas of occupation, median Likert-scale scores for all areas were more than 3.0 on a 4-point scale, with the exception of math. Figure 1 separates the number of children who experienced mild, moderate, and severe difficulty, showing that most of the children who had difficulty during exacerbation either displayed moderate difficulty requiring assistance or adaptation to remain functional or displayed severe difficulty and were unable to function at a typical level, even with assistance and adaptation (see Figure 1).
Similarly, for children who were reported to have difficulty with mental functions, sensory functions, and neuromuscular functions, median Likert-scale scores were more than 3.0 in all of the mental functions as well as in hearing, proprioceptive, tactile, and taste functions. This finding indicates that most of the children either displayed moderate difficulty and required assistance or adaptation to remain functional, or they displayed severe difficulty and were unable to function at a typical level, even with assistance and adaptation (see Figure 2).
Research Question 3: Comments From Parents
Parents were given the opportunity to comment in an open-text section labeled “additional comments” after each question. Comments were neither specifically solicited nor encouraged. In all, 71 parents provided more than 450 optional comments to help clarify or to expand information, the majority of which followed areas identified as moderate or severe difficulty. The comments were coded and grouped for similarity, resulting in 35 subcategories, which were further distilled to the following 14 themes: cognitive inflexibility, sensory changes, functional cognitive impairment, anxiety and fear, adaptive and academic regression, motor changes, mood and energy dysregulation, decreased socialization, atypical eating (restricted or excessive), urinary frequency, tics and tremors, pain, related medical issues, as well as hallucinations.
Table 2 identifies the themes along with a list of the number of comments in each theme and sample comments. The full list of comments and coding depicts the extent of dysfunction in some children and is available from the first author. For example, when discussing hygiene, one parent stated, “went 6–8 weeks without showering with only one evening during that time period in a swimming pool, could not brush teeth, brushed hair violently, the hair on her head bothered her.” Eating difficulties are highlighted with several reports of fear of choking, and one parent noted, “went as long as 5 days without eating for fear of choking, got IV fluids in the hospital to stay hydrated.” When discussing handwriting, one parent stated, “horrible handwriting, improper grasp on pencil, struggle to write even short assignments,” whereas another parent stated, “incapable of writing anything—my wife and I scribed for him.” Regarding math, one parent stated, “could not remember simple number facts despite repetition,” and when discussing the impact on family socializing, one parent stated, “unable to leave the house, must be left behind for family activities, family unable to travel, no visitors allowed in the house.” The full set of original comments are rich—highlighting the impact of anxiety, obsessive–compulsive rituals, sensory processing problems, and cognitive difficulties on the child’s daily functioning.
Summary and Sample of Themes and Comments
Discussion
This study indicates that PANS exacerbations are quite pervasive, potentially limiting every aspect of daily life, including daily living skills, education, and play and leisure. Exacerbations may also affect all of the contexts in which the child functions, including the family, the school, and the community. Although parents who chose to comment may have children with more severe manifestations, parents commented on the need for hospitalization in extreme cases, and many parents commented on the need for special education or the child being unable to attend school. Such limitations are costly in terms of family functioning and in terms of health care and educational dollars.
Children in this study experienced a 2- to 3-yr lag between onset of symptoms and diagnosis, increasing the burden on child, family, and society before appropriate treatment could be initiated. To date, there are no cost-of-illness studies for PANS; however, this study indicates a need to analyze the economic burden of this disorder and the costs that could be saved with speedy diagnosis and effective intervention.
Occupational limitations in education have previously been identified by Bernstein, Victor, Pipal, and Williams (2010), who noted a lack of attention and decline in handwriting as possible factors leading to decline in school performance in children with PANDAS, and by Swedo et al. (1998, 2012), who identified deterioration in school performance, including handwriting, math skills, attention, concentration, ability to memorize, and problems in executive skills. The current study supports these findings and suggests that limitations in reading, memory, and higher level thinking could also contribute to school performance decline. It is important that teachers, occupational therapy practitioners, speech therapists, special educators, school psychologists, social workers, nurses, and other related professionals have prior knowledge of such potential decline to be prepared to recognize and help the child in crisis. Education of these professionals must be a priority for PANS support groups.
Additionally, limitations in the area of extracurricular activities are also important because these limitations affect the child’s ability to engage in the role of student and to develop assets thought to be beneficial for emotional resilience (Search Institute, 2016). Educators, school administrators, and related service personnel should be made aware of potential changes in these areas to provide appropriate accommodations and remediation activities for children during and after exacerbation, such as those suggested in recent PANDAS and PANS books (Doran, 2016; Greene, 2016).
Bernstein et al. (2010) reported change in gait during exacerbation, and this finding was supported by the current study, wherein 34% of respondents identified problems in their child’s gait during an exacerbation, along with joint pains, muscle weakness, and poor endurance. Both occupational and physical therapy should be involved with these children during exacerbation because strength training, gait training, aerobic fitness protocols, or modalities for joint pain may prove beneficial.
Effectiveness of therapy intervention has not been studied to date; however, it has been suggested that therapists should focus on accommodation and adaptation during the exacerbation, with remedial interventions used after the exacerbation for occupational therapy (Tona, 2016; Tona & Posner, 2011). During remission, occupational therapists can work with children and families to develop positive mental health and coping strategies that could be used daily for mental wellness and also be called into use during exacerbation. Cognitive and sensory programs addressing arousal level, self-regulation, and attention to task may be particularly beneficial, as would identification of leisure activities that could be continued if another exacerbation occurred. Family intervention identifying family supports, social participation opportunities, and accommodations in the family schedule can help to reduce the impact on the family during exacerbation.
Limitations and Strengths
This study was limited by the retrospective design, which may have caused the responses to be inaccurate because of poor recall. A prospective study of the areas identified as problematic could be a next step. In addition, the data are limited to a homogeneous group of participants with higher socioeconomic status and higher level of education than the mean of the United States. The comments provided were not specifically solicited, and they may represent comments from families with extreme experiences because families of children with milder exacerbations may not have shared comments. The online survey also limits verification of the responses. Although face validity has been established, reliability of the survey was not.
Strengths of the study include basing the survey on the Framework, thereby establishing a direct link for occupational therapy involvement and allowing practitioners to have knowledge of expected occupational performance limitations during exacerbation. The online reporting of information used in this study makes it feasible to collect data from families at regular intervals throughout the course of 1 yr or more, making a future longitudinal prospective study possible. In addition, the rich information gathered through parent comments could be used for further research of a qualitative nature to better understand the experience of children and families during exacerbation. Such information could prepare professionals to better serve these families and could help families to better understand their own situation and prepare for subsequent exacerbation.
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy clinical practice:
Children with sudden deterioration in occupational performance, sensory processing, cognitive skills, mental health functions, or motor skills may have biological underpinnings for those issues.
Health and education professionals should help families to understand this possibility so that children can be referred to a health care practitioner for evaluation for PANS when sudden-onset neuropsychiatric symptoms are seen.
Occupational deterioration can occur in any area of occupation and can affect community and family participation during exacerbation.
Accommodation and adaptation during exacerbation may help children to maintain occupational roles and community and family participation, and this area should be addressed in future studies.
Remedial activities as well as child and family education during remission may help children to regain skills and help children and families to establish a toolbox of techniques for accommodation during exacerbation; this area should also be addressed in future studies.
Future research ideas include prospective studies of occupations, body functions, and performance skills during exacerbation as well as studies regarding efficacy of adaptive and remedial interventions during and after exacerbation.
Conclusion
People with PANS experience a sudden onset of neuropsychiatric symptoms, which has previously been identified to affect handwriting, math skills, and sensory processing. In this study, the first to establish links between PANS exacerbations and the Framework, we have identified (1) limitations in nearly every aspect of occupational performance in at least some people with PANS; (2) several previously unreported limitations in occupational performance for the majority of participants, such as personal hygiene and grooming, bathing, extracurricular activities, and participation in all aspects of leisure activities; and (3) underlying impairments in client factors and performance skills. Armed with this knowledge, occupational therapists can use their skills to evaluate and address these occupational performance limitations and improve the quality of life for these children and families.
Footnotes
Acknowledgments
We acknowledge the following occupational therapists for their contribution to this work while students at the University at Buffalo, State University of New York: Sonya Eskew, Lindsay Frajdofer, Brie Georger, Cassandra Hawkins, Margery Henning, Danielle Pellegrino, Maureen McAnany, Erika Rogers, Nicole Schmidt, Molly Slattery, Stephanie Zahra, and Courtney Zempel. We also acknowledge Trudy Posner for review of the survey and Michele Youakim for sharing her expertise in the design of the study.
1
Although AOTA published the third edition of the Framework in 2014, the survey for the study was designed and participants were recruited and began using the survey prior to 2014. Therefore, terminology and definitions from the second edition were used in the study.