
Abstract
The development of bowel control is an important activity of daily living in early childhood, and challenges in this area can limit participation in key occupations. Retentive fecal incontinence (RFI) is a common disorder in children. Up to 50% of children do not respond adequately to initial medical intervention, and behaviors around toileting, some related to sensory overresponsivity (SOR), may be partly responsible. Therefore, this study investigated the relationship between RFI and SOR and also examined the discriminative validity of the Toileting Habit Profile Questionnaire (THPQ). Per parent report, children with RFI (n = 16) showed significantly more behaviors related to SOR compared with typically developing children (n = 27). In addition, results indicated that the THPQ effectively discriminates between children with RFI and typically developing children. Results are discussed regarding RFI and SOR, the impact of RFI on childhood occupational engagement, and the role of occupational therapy with this population.
Toileting, including bowel management, is an important activity of daily living (ADL; American Occupational Therapy Association, 2014), and issues in this area can limit a child’s independence and social participation. Additionally, acquiring continence of bowel is considered an important milestone of childhood, generally achieved by age 3 (Schum et al., 2002). Therefore, addressing issues related to bowel management is an important component of occupational therapy practice.
Background
Retentive fecal incontinence (RFI) is a common disorder in children that often leads to impaired social acceptance, relationships, and development (Friman, Hofstader, & Jones, 2006). Of the main symptoms of constipation, RFI occurs when soft stool from the bowel slips around a hard mass of stool that remains accumulated in the rectum (Cohn, 2011). Constipation is one of the most common gastrointestinal complaints in children (Tabbers, Boluyt, Berger, & Benninga, 2011); worldwide prevalence is estimated to be 12% in the general childhood population, with peak incidence occurring during toilet training (Mugie, Benninga, & Di Lorenzo, 2011). Compared with typical children, children with long-lasting symptoms of constipation are at risk for experiencing lower health-related quality of life as adults, including ongoing health concerns and body pain (Bongers, van Dijk, Benninga, & Grootenhuis, 2009).
Although the cause of RFI has not been clearly identified, behaviors have been identified that seem to be partly responsible for the development and maintenance of the condition (Benninga, Voskuijl, Akkerhuis, Taminiau, & Büller, 2004; Cox, Morris, Borowitz, & Sutphen, 2002; van Dijk, Benninga, Grootenhuis, & Last, 2010). Stool-withholding behavior has been recognized as one of the most common causes of development and maintenance of childhood constipation (Cohn, 2011; Tabbers et al., 2011; Whitehead, di Lorenzo, Leroi, Porrett, & Rao, 2009). Stool toileting refusal or fear of sitting on the potty are other identified behavior problems in children that have been associated with constipation, stool withholding, late toilet training, and fecal incontinence (Blum, Taubman, & Nemeth, 2004; Taubman, 1997; Taubman, Blum, & Nemeth 2003). Refusal behaviors are also reported to contribute to the maintenance of RFI because they interfere with conventional medical management (Karagiozoglou-Lampoudi et al., 2012; Kaugars et al., 2010; Kuhl, Felt, & Patton, 2009; Sullivan, Alder, Shrestha, Turton, & Lambert, 2012; Taubman & Buzby, 1997; Vitito, 2000).
Conventional medical management is the first line of treatment of constipation and RFI, often consisting of dietary recommendations; stool softener, laxative medication, or both; and implementation of toileting routines (Cohn, 2011). Currently, only about 50% of patients are free of complaints and off laxatives after 6–12 mo of medical management (Pijpers, Bongers, Benninga, & Berger, 2010). Although identified behavioral issues related to RFI are not necessarily causal, closer examination of the problem behaviors associated with constipation and RFI could contribute to developing more effective treatment programs to augment conventional medical management.
It has been hypothesized that difficulty processing and integrating sensory information could be a factor contributing to the development of certain problematic behaviors in children (Dunn, 2007; Hazen et al., 2008; Roberts, King-Thomas, & Boccia, 2007; Schaaf et al., 2010). For example, exaggerated responses to normal sensory stimuli, often referred to as sensory overresponsivity (SOR), have been associated with refusal to comply with parental demands or atypical habits regarding other types of self-care activities (Cermak, Curtin, & Bandini, 2010; Chatoor, 2002; Dunn, 2007; Hazen et al., 2008; Nadon, Feldman, Dunn, & Gisel, 2011; Schaaf et al., 2010). It has also been hypothesized that some of the behaviors typical of children with RFI could be related to SOR (Beaudry Bellefeuille & Ramos Polo, 2011; Beaudry Bellefeuille, Schaaf, & Ramos Polo, 2013; Handley-More, Richards, Macauley, & Tierra, 2009). In addition, SOR has been documented to be associated with other gastrointestinal dysfunctions (Bakker, Boer, Benninga, Koelman, & Tijssen, 2010; Mazurek et al., 2013). For instance, children with dysfunctional elimination syndrome (DES), a disorder characterized by abnormal bowel and bladder voiding in the absence of anatomical or neurological disease, have been found to have more sensory responsivity difficulties than typically developing children, providing evidence of a link between toileting issues and sensory responsivity difficulties (Pollock, Metz, & Barabash 2014).
At present, there is little documentation of a potential relationship between SOR and RFI. Therefore, the focus of this study was to investigate this relationship and establish initial clinical validity of the Toileting Habit Profile Questionnaire (THPQ; Beaudry-Bellefeuille, Lane, & Ramos-Polo, 2016), a tool designed to screen for sensory-based toileting difficulties.
Method
Research Design
We examined construct validity using a known-group design to determine the ability of the THPQ to distinguish between children with identified RFI and typical children. Subsequently, scores from both the typical children and the children with RFI were analyzed together using a correlational study design to explore the relationship between THPQ scores and SOR scores. Parents of 3- to 5-yr-old children with RFI were asked to complete two different questionnaires: the THPQ and the Spanish version of the Short Sensory Profile (SSP; McIntosh, Miller, Shyu, & Dunn, 1999) revised for Spain (S–SSP–R; Beaudry-Bellefeuille & Lane, 2015). A comparison group of parents of typical children, age and gender matched, was also recruited and asked to complete both questionnaires.
Participants
A conservative estimate based on clinical experience with the THPQ showed an expected difference of 7 points in the mean scores of typical children and children with RFI. Using this estimate and N-Query Advisor® (STATSOLS, Boston, MA) sample size calculations for a Wilcoxon rank–sum test, we determined that a minimum of 19 parents should be included in each group. Regarding the correlation of TPHQ and SOR scores, sample size calculations for an expected correlation of 0.4, with a power of 0.8, were done using G*Power version 3.1.5 (Heinrich Heine University, Düsseldorf, Germany), and a sample size of 46 was recommended.
Accordingly, over a period of 4 mo, efforts were made to recruit two groups of 25 parents of children ages 36–71 mo. Local pediatric gastroenterologists and occupational therapy practitioners from both public and private clinics were contacted for recruitment of parents of children with RFI who had not responded to an initial trial of conventional medical treatment by the child’s pediatrician. Parents of typically developing children were recruited through the parent–student associations of local schools. The parent of each child signed an informed consent form. Approval by the Virginia Commonwealth University institutional review board was obtained before the beginning of the study.
Parents whose 3- to 5-yr-old children experienced fecal incontinence as part of the symptoms of functional constipation according to Rome III criteria (Drossman, 2006) and had no other diagnosis were included in the RFI group. Diagnosis of RFI and screening for medical conditions was done by the child’s referring physician as part of the standard medical management of constipation and fecal incontinence. If parents with children with suspected RFI were interested in participating in the study and were referred by sources other than physicians, their children were referred for medical screening by a physician before participation.
Children with organic causes of RFI, including Hirschsprung’s disease, muscle disorders, prior rectoanal surgery, spina bifida, mental retardation, or hypothyroidism, were not eligible. For both the RFI and the typical group, parents of children with intellectual disability; neurological conditions, such as cerebral palsy; or psychiatric disorders, such as bipolar disorder or oppositional defiant disorder, were excluded. In Spain, 3- to 5-yr-old children are typically enrolled in preschool programs, which screen for developmental disorders. Therefore, children who had a curricular adaptation at school or who qualified for their school’s special needs program were excluded. Public health services pediatricians also periodically screen children for mental health and developmental disorders and refer them to early intervention programs accordingly. Therefore, children who had been referred to these programs were excluded.
The recruitment period yielded 16 participants for the group comprising parents of children with RFI. For the group comprising parents of typically developing children, 27 participants were recruited. Because sample sizes of 25 were not achieved for both groups, the data have been analyzed and treated as a pilot study to provide information for a larger study in the future. Participant demographics are presented in Table 1.
Participant Descriptive Statistics
Note. Percentages may not total 100 because of rounding. RFI = retentive fecal incontinence; TYP = typically developing.
Per family member.
p < .05.
Measures
Toileting Habit Profile Questionnaire.
A caregiver report tool, the THPQ was designed as a screening questionnaire to help differentiate between typical defecation behaviors and behaviors associated with constipation and fecal incontinence potentially related to sensory responsivity concerns. Items are organized into two sections: an SOR section, which contains 8 items, and a sensory underresponsivity section, which contains 2 items (Figure 1). This study focused on questions in the SOR section. Scored using a 5-point Likert scale (ranging from 1 = almost always to 5 = never), this tool underwent face and preliminary content validation using a panel of experts consisting of pediatric gastroenterologists and occupational therapists with expertise in Ayres Sensory Integration® (Beaudry-Bellefeuille et al., 2016).
Items from the Toileting Habit Profile Questionnaire (Beaudry-Bellefeuille, Lane, & Ramos-Polo, 2016).
Short Sensory Profile.
The S–SSP–R was used to assess sensory responsivity abilities and concerns. The SSP is a 38-item condensed version of the original 125-item Sensory Profile (SP; Dunn, 1999). Both the SP and the SSP are caregiver questionnaires that measure responses to sensory events in daily life in children ages 3–10 yr. The validity of these tools is well established. The data provided by these questionnaires allow clinicians to analyze how certain patterns in sensory processing may be related to performance and participation difficulties in daily occupations (Dunn, 1999). The Spanish version was originally aimed at Spanish speakers in the United States. Verification of the validity of the Spanish version in Spain was done through cognitive interviewing of caregivers and review by an experienced linguistic consultant (Beaudry-Bellefeuille & Lane, 2015). The newer version of the SP, the SP2 (Dunn, 2014), was not available at the time of this study.
Data Analysis
Between-group comparisons (children with and without RFI) on the THPQ and the S–SSP–R were conducted using the Mann–Whitney U test. Differences were considered statistically significant at p < .05. A Spearman correlation coefficient was calculated to analyze the relationships between the SOR score and the THPQ score. Because scores are based on ordinal data, nonparametric statistical tests were chosen.
Because the purpose of the study was to develop a better understanding of the relationship between RFI and SOR, data analysis used only a subset of relevant items from the THPQ and the S–SSP–R. For the THPQ, the analysis included the score obtained on the SOR section of the questionnaire. For the S–SSP–R, analysis was done as described by Mazurek and colleagues (2013). An SOR score was calculated using the items designed to detect overresponsivity: tactile sensitivity (Items 1–7), taste/smell sensitivity (Items 8–11), movement sensitivity (Items 12–14), and visual auditory sensitivity (Items 34–38).
Results
Between-Group Differences
Lower THPQ scores are more indicative of behaviors hypothesized to be specific to children with RFI. In the THPQ 8-item SOR section, 40 represents the maximum possible score and 8 represents the minimum possible score. Results of the Mann–Whitney U test analysis indicated a significant difference between children with RFI (median [Mdn] = 23.50, first quartile [Q1] = 17.50, third quartile [Q3] = 28.00) and the typical group (Mdn = 36, Q1 = 34, Q3 = 38; p = .000). Results are represented in Figure 2.
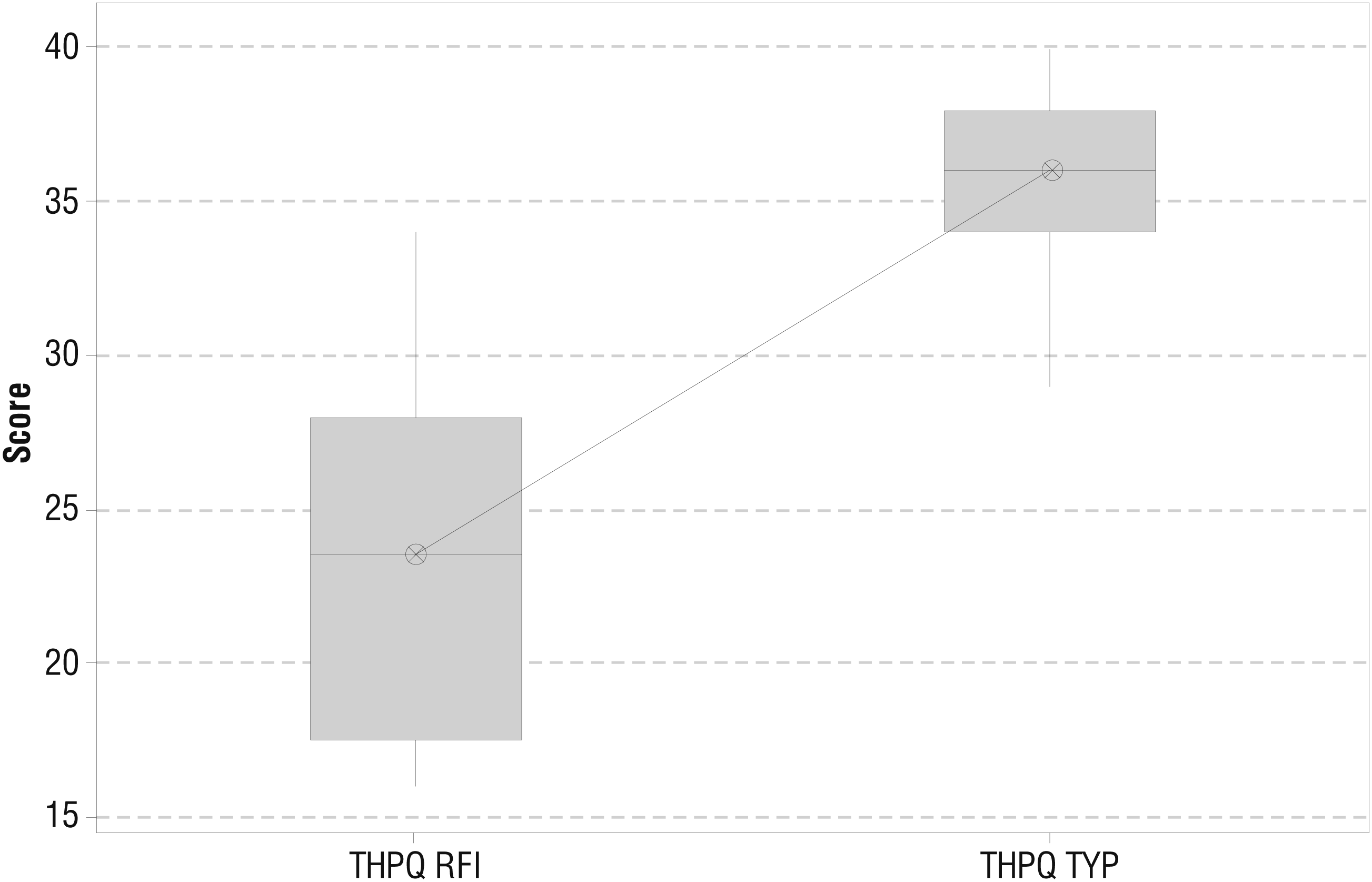
Boxplot of Toileting Habit Profile Questionnaire scores.
An SOR score was calculated from the S–SSP–R using the items designed to detect overresponsivity. Lower SOR scores are indicative of greater SOR. Results of the Mann–Whitney U test analysis indicated a significant difference between median scores for children in the RFI group (Mdn = 76.50, Q1 = 71.25, Q3 = 85.25) and the typical group (Mdn = 84.00, Q1 = 76.00, Q3 = 90.00; p = .0346). Results are represented in Figure 3.
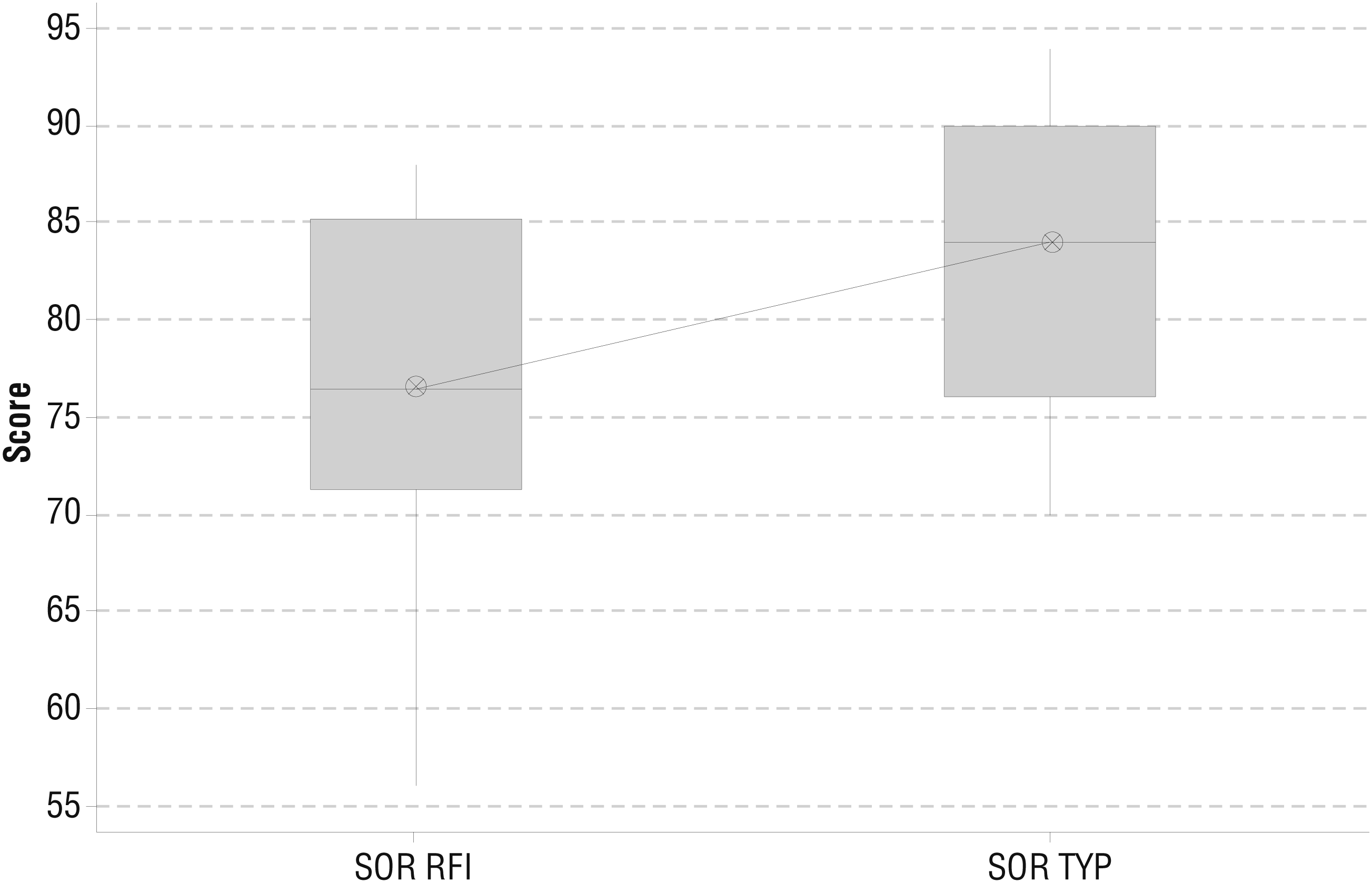
Boxplot of sensory overresponsivity scores.
Relationship Between Scores
A Spearman correlation between SOR scores and THPQ scores produced r s = .423, which confirms a moderate but significant (p = .005) linear dependency between SOR and THPQ scores.
Discussion
Fecal incontinence and constipation are two of the most common gastrointestinal complaints in children (Tabbers et al., 2011), and success rates for conventional medical treatment of children with these concerns remains limited (Pijpers et al., 2010). Identifying underlying factors that have not previously been considered is crucial to improve treatment outcomes. Results from this pilot study suggest that SOR is one of these underlying factors and should be considered in children with conventional medical treatment–resistant RFI. In addition, because occupational therapy practitioners have expertise in occupational engagement and sensory modulation disorders such as SOR, they have a role to play in identifying and treating sensory concerns in children with RFI.
The age range of 3–5 yr was chosen for multiple reasons. First, studies have shown that most children acquire fecal continence by approximately age 3 yr (Schum et al., 2002; Wald et al., 2009), and ongoing toileting concerns become apparent in children in this age range. Second, it has been hypothesized that the symptoms of feeling pain upon defecation and toilet avoidance may be more significant at younger ages (Borowitz, Cox, & Sutphen, 1999). Clinically, it appears that children who have long-standing constipation habituate to the sensations that they initially found painful and motivated them to withhold stool. However, once caught in the cycle of constipation and atypical bowel habits, many struggle to reacquire healthy defecation even in the absence of pain. Third, clinical experience and research have suggested that feeling pain upon defecation and toilet avoidance is related to SOR to the sensations associated with defecation. Thus, these factors are linked to the onset and maintenance of the difficulties children with RFI have establishing healthy toileting routines (Beaudry Bellefeuille & Ramos Polo, 2011; Beaudry Bellefeuille et al., 2013; Handley-More et al., 2009). Finally, this age range has also been reported to be the age of highest prevalence for childhood constipation (van den Berg, Benninga, & Di Lorenzo, 2006).
No previous studies have specifically examined the link between RFI and SOR, although related evidence indicates a relationship between SOR and gastrointestinal problems. Existing evidence indicates that children with autism with any type of gastrointestinal problem, including chronic constipation, show higher levels of SOR than children without such problems (Mazurek et al., 2013). A link between the auditory startle reflex, a measure of hyperarousal, and irritable bowel syndrome and functional abdominal pain syndrome has also been established (Bakker et al., 2010). In addition, although SOR has not been specifically addressed in children with DES, the broader group of sensory responsivity difficulties has been found to a greater extent in children with DES than in a typical population (Pollock et al., 2014), reinforcing the need for consideration of sensory issues in children with elimination difficulties. Study findings add to this literature and support the coexistence of gastrointestinal difficulties and SOR. They help complete the picture of this relationship in clinical populations and lay a foundation for use of alternative interventions when routine medical interventions fail.
The results of this study substantiate that the behaviors described in the first section of the THPQ, meant to explore SOR, are associated with SOR, as determined by select items from the S–SSP–R. In addition, this pilot study provides preliminary support for the discriminative validity of the THPQ in distinguishing between the toileting behaviors of children with RFI and those of typically developing children. The THPQ is a unique tool, designed to screen for sensory-based defecation difficulties and to explore child behaviors that may contribute to ongoing RFI—no other clinically available tools tap into these concerns (Beaudry-Bellefeuille et al., 2016). Response to sensations related to the evacuation of stool seems to influence the acceptance of toilet training and the reponse to the urge to defecate in some children, affecting the development of age-appropriate toileting habits (Beaudry Bellefeuille & Ramos Polo, 2011; Beaudry Bellefeuille et al., 2013; Handley-More et al., 2009). We previously established content validity for the THPQ (Beaudry-Bellefeuille et al., 2016), and in the current study, we further reinforce the usefulness of this tool in distinguishing between children with and without RFI.
Problems in bowel management have the potential to significantly limit a child’s independence and often lead to impaired social acceptance, relationships, and development (Friman et al., 2006). The unpleasant odors caused by feces are often the cause of rejection and ridicule by peers, which can affect social participation and participation in key activities of childhood (Handley-More et al., 2009). Therefore, deepened understanding and identification of unresolved issues regarding bowel management are crucial and lay the foundation for appropriate occupational therapy intervention for this important ADL.
Limitations and Future Research
Although this study adds to the existing literature, it has limitations. First is the small sample size. Second, because participants were obtained mainly from private pediatric gastroenterologists and occupational therapists in one Spanish city, sampling heterogeneity was limited. Thus, this study should be viewed as a pilot investigation, warranting further consideration and a larger, more diverse sample.
Another limitation to consider is that assessment data relied on caregiver report; objective assessment data were not collected. Nonetheless, caregiver report is reported to be a valid method of data collection in other areas (Feldman et al., 2005; Harvey et al., 2010) and can be easily used to collect data from large groups, an important factor to consider for future studies. Because of the study design, the lead investigator (Isabelle Beaudry-Bellefeuille) was not blind to group membership. Thus, future studies with researchers blinded to condition are needed to gain a better understanding of the discriminative ability of the THPQ, the specific sensory issues faced by children with RFI, and how these issues may affect toileting habits and participation in daily activities.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice:
Results provide initial validation for the use of the THPQ to discriminate between the toileting behaviors of children with RFI and those of typically developing children and provide pilot support for the hypothesis that the behaviors described in the first section of the THPQ are associated with SOR.
Occupational therapy practitioners, with expertise in sensory integration and processing, can make valuable contributions as part of the interdisciplinary teams identifying children with RFI and stool-withholding behavior, potentially complicated by SOR.
Identifying RFI in conjunction with SOR can alert health care providers to consider additional treatment options for these children, addressing their sensory sensitivities, to optimally support their participation in healthy and socially acceptable toileting routines.
Footnotes
Acknowledgments
The authors thank Leroy Thacker for his support in the analysis of the data.