
Abstract
Lower-extremity (LE) musculoskeletal disorders (MSDs) can have a major impact on the ability to carry out daily activities. The effectiveness of interventions must be examined to enable occupational therapy practitioners to deliver the most appropriate services. This systematic review examined the literature published between 1995 and July 2014 that investigated the effectiveness of occupational therapy interventions for LE MSDs. Forty-three articles met the criteria and were reviewed. Occupational therapy interventions varied on the basis of population subgroup: hip fracture, LE joint replacement, LE amputation or limb loss, and nonsurgical osteoarthritis and pain. The results indicate an overall strong role for occupational therapy in treating clients with LE MSDs. Activity pacing is an effective intervention for nonsurgical LE MSDs, and multidisciplinary rehabilitation is effective for LE joint replacement and amputation. Further research on specific occupational therapy interventions in this important area is needed.
Lower-extremity (LE) musculoskeletal disorders (MSDs), such as major joint replacement, hip fracture, amputation or limb loss, and osteoarthritis (OA), are common conditions that require people to seek medical and rehabilitation services. In the United States, the incidence of hip and knee OA is 88 per 100,000 person-years and 100 per 100,000 person-years, respectively (Oliveria, Felson, Reed, Cirillo, & Walker, 1995). Demand for major LE joint replacements is growing (Ravi et al., 2012; Weinstein et al., 2013), and in 2014 more than 400,000 procedures were performed that cost in excess of $7 billion just for hospitalizations (Centers for Medicare and Medicaid Services [CMS], 2016). In the United States, an estimated 300,000 older adults are hospitalized each year for hip fracture (National Center for Health Statistics, 2010), and the prevalence of LE amputation or limb loss is increasing (Ziegler-Graham, MacKenzie, Ephraim, Travison, & Brookmeyer, 2008).
The potential impact of LE MSDs on participation in meaningful life roles is immense. For example, approximately 80% of patients with OA have some movement limitation, with 25% unable to perform activities of daily living (ADLs; Centers for Disease Control and Prevention, 2015). LE MSDs can cause activity limitations and participation restrictions that require rehabilitation intervention (Gillen et al., 2007).
People recovering from or living with LE MSD may be referred to and receive occupational therapy services because these conditions regularly hamper participation in meaningful occupations (American Occupational Therapy Association [AOTA], 2014). Occupational therapy interventions for LE MSDs are frequently provided as part of an interdisciplinary care plan and typically focus on ADL and instrumental activity of daily living (IADL) performance areas affected by impaired LE functioning (AOTA, 2014). In addition, the new Comprehensive Care for Joint Replacement model implemented in April 2016 has implications for the delivery of and payment for occupational therapy rehabilitation services for patients undergoing hip and knee replacement (CMS, 2016). Considering the high incidence and prevalence of LE MSDs and the perceived value of occupational therapy services related to these diagnoses, it is important to investigate the effectiveness of occupational therapy interventions to ensure evidence-informed practice.
The objective of this systematic review was to identify, evaluate, and synthesize the literature related to occupational therapy interventions for people with LE MSDs. The focused question for this review was, What is the evidence for the effect of occupational therapy interventions for adults with MSDs of the LE (pelvis, hip, leg, ankle, and foot)? The question was developed by the review authors, an advisory group of experts in the field, AOTA staff, and the methodology consultant to the AOTA Evidence-Based Practice (EBP) Project.
Method
The review was carried out as an academic partnership between the AOTA EBP Project and the review authors, who worked as a faculty pair and used graduate research assistants to support the review process. The systematic review covers the period from January 1995 through July 2014, when the search was completed. Search terms for the review were developed by AOTA EBP Project staff and the methodology consultant, in consultation with the review authors and an advisory group. A medical research librarian with experience in completing systematic review searches conducted all searches and confirmed and improved the search strategies.
The AOTA EBP committee operationalized MSD as any acute or acquired injury or disorder involving bones, muscles, or other tissues, regardless of etiology. LE conditions meeting this definition and included in this review are reflected in the search terms (Table 1) and sample search strategy (Supplemental Appendix 1, available online at http://otjournal.net; navigate to this article, and click on “Supplemental Materials”). Databases searched included MEDLINE, PsycINFO, CINAHL, Ergonomics Abstracts, and OTseeker. Consolidated information sources, such as the Cochrane Database of Systematic Reviews, were also included in the search. In addition to the database searches, reference lists from articles included in the systematic reviews were examined for potential articles, and selected journals were hand searched to ensure that all appropriate articles were included.
Search Terms for Lower-Extremity Musculoskeletal Disorders
Note. ACL = anterior cruciate ligament; AAROM = active assistive range of motion; ADLs = activities of daily living; AROM = active range of motion; EMG = electromyography; IADLs = instrumental activities of daily living; NCV = nerve conduction velocity; PROM = passive range of motion.
This review was limited to peer-reviewed scientific literature published in English presenting Level I, II, and III evidence. Studies with Level IV and V evidence were considered only when higher level evidence on a given topic was not found. Presentation abstracts, conference proceedings, non–peer-reviewed literature, dissertations, and theses were excluded. To be included, studies must have examined an intervention approach within the scope of practice of occupational therapy for adult participants with LE MSD, including LE arthritis, and must have met minimal quality criteria on the basis of level of evidence.
For the purposes of this review, we focused on studies that included functional or occupation-based interventions (e.g., ADL and IADL training, home evaluations), outcomes that targeted improving function (e.g., improved ADL and IADL performance, independence or level of disability, participation, quality of life), and other interventions within the scope of practice of occupational therapy for the LE. Therefore, studies were excluded if they focused solely on nonfunctional or non–occupation-based interventions (e.g., only on orthotics, braces, or inserts; modalities; targeted LE exercise) or used only nonfunctional outcome measurements (e.g., increased range of motion or strength without discussion of implications for function). Involvement of an occupational therapy practitioner in the study was not a requirement for inclusion, provided the study met all other inclusion criteria, because many other professions treat LE MSDs and have some overlap with the domain of occupational therapy.
The flow of abstracts and articles through the process is detailed in Figure 1. After completion of the searches, the medical librarian performed an initial screening to eliminate references on the basis of title and abstract using broad inclusion and exclusion criteria (i.e., occupational therapy practice, LE MSD). Of the 10,533 total search results, 1,050 potential abstracts were identified and sent to the review authors for screening and selection using the detailed criteria described earlier. After removal of duplicates, 849 unique records were screened by the review authors, and 218 abstracts were identified as potentially meeting inclusion criteria. Full-text articles were retrieved and independently reviewed by the authors, who identified 43 articles meeting criteria for final eligibility.
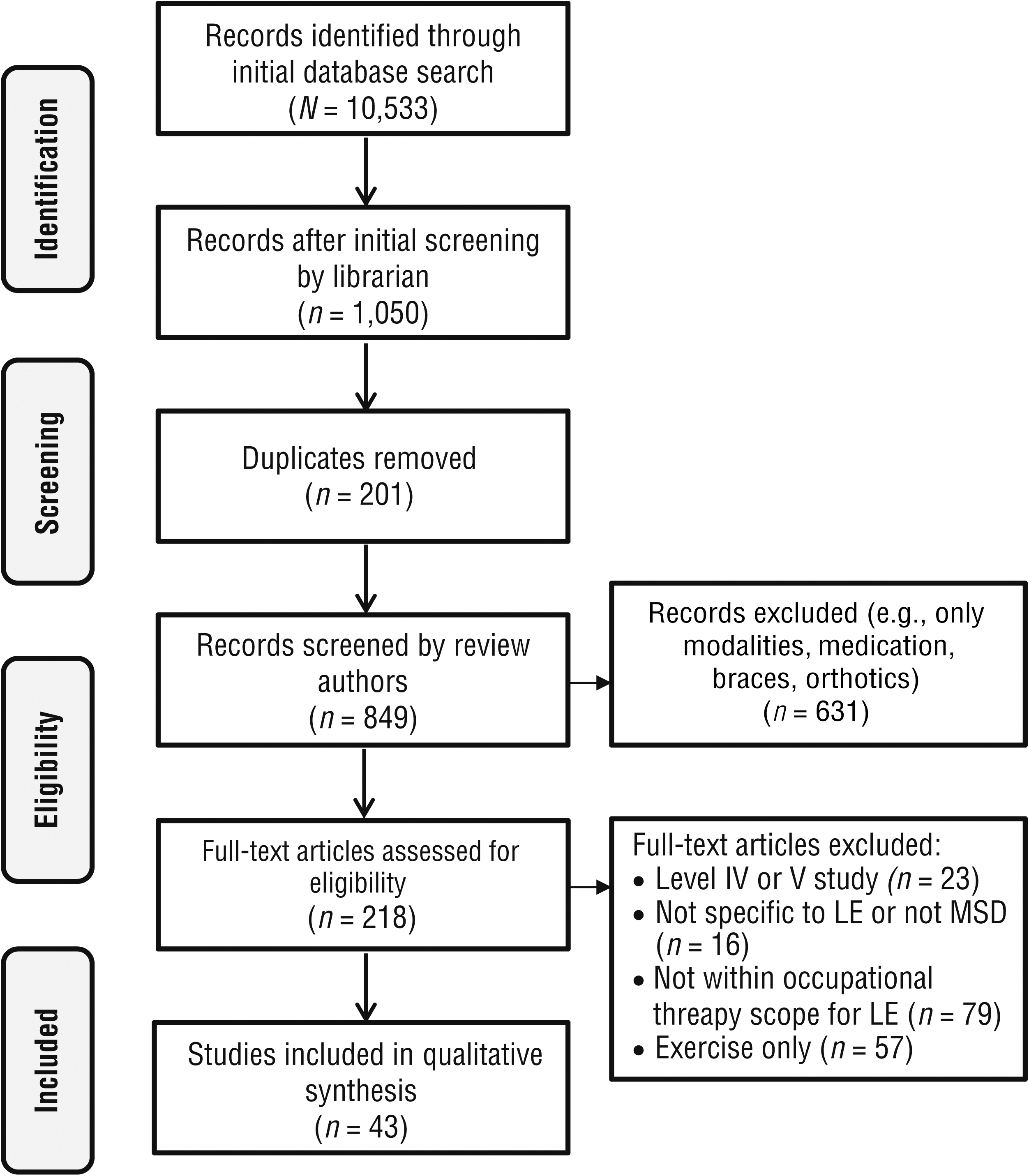
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of LE MSD intervention studies included in the systematic review.
At each step, when the review authors were unable to come to a decision regarding inclusion, the AOTA EBP team was consulted. When a systematic review was included, any articles synthesized within that systematic review were not considered individually and were thus excluded from this review. A systematic review was included if more than 1 article met the inclusion criteria, and then only relevant data were extracted and noted accordingly in the evidence table (Supplemental Table 1, online). For articles that were included, data on study sample, intervention methods, and results were extracted, and each article was accordingly abstracted into the evidence table. Articles were then summarized within diagnostic groups, and the review authors qualitatively synthesized outcomes. U.S. Preventive Services Task Force (2016) definitions were used to determine the strength of the evidence for the identified topics (i.e., population groups), classified as strong, moderate, limited, mixed, or insufficient. Each topic was evaluated on the basis of the quality of individual studies reviewed (i.e., risk of bias) and the number of studies at each level of evidence.
Results
Included Studies
The systematic review process resulted in 43 studies: 31 Level I, 10 Level II, and 2 Level III. The original intent was to categorize studies on the basis of interventions to more directly answer the focused question. However, the wide variety of interventions represented and limitations in how the interventions were described precluded us from doing so. Instead, we categorized and summarized the articles in four groups based on population: (1) hip fracture (n = 14), (2) elective hip or knee replacement (n = 14), (3) amputation or limb loss (n = 5), and (4) nonsurgical OA and pain (n = 10). Risk of bias was evaluated for all included articles using A Measurement Tool to Assess Systematic Reviews (AMSTAR; Shea et al., 2007) and the guidelines provided in the Cochrane Handbook for Systematic Reviews and Interventions (Higgins, Altman, & Sterne, 2011) for intervention studies.
The included systematic reviews were mostly of high quality, with many following the Cochrane system (Supplemental Table 2, online). The quality of included intervention studies varied, with common issues related to poor long-term follow-up, lack of participant blinding, and lack of or poorly described blinding of outcomes (Supplemental Table 3, online). The sections that follow synthesize the findings for studies within each population group.
Interventions for Hip Fracture
Of the 14 studies identified as providing interventions for people with hip fracture, 3 described the specific components of an occupational therapy intervention. A randomized controlled trial (RCT) that evaluated occupational therapy services combined with physical therapy on a rehabilitation unit found that patients who received occupational therapy experienced significantly lower emotional distress and less fatigue 6 mo after the start of treatment (Martín-Martín, Valenza-Demet, Jiménez-Moleón, et al., 2014). In addition, although function and independence significantly improved in both groups, those who also received occupational therapy had significantly better outcomes 6 mo after the start of intervention (Martín-Martín, Valenza-Demet, Jiménez-Moleón, et al., 2014).
A 2nd RCT found that occupational therapy training for caregivers of patients with hip fractures resulted in less anxiety and depression at 1- and 3-mo follow-up and reduced emotional distress, anxiety, and depression at 6 mo for caregivers (Martín-Martín, Valenza-Demet, Ariza-Vega, et al., 2014). In the 3rd study, a Level II quasi-experimental design, occupational therapy treatment guided by the Occupational Adaptation model was associated with more efficient achievement of functional independence and higher patient satisfaction with rehabilitation than was treatment guided by the Biomechanical Rehabilitation model (Jackson & Schkade, 2001).
Eleven additional articles directly described the occupational therapy interventions provided or had other study limitations that restricted the authors’ ability to draw conclusions regarding the interventions. Evidence in these studies was primarily suggestive of the positive impact of rehabilitation interventions; however, the direct contribution and effect of occupational therapy were not clearly described.
Setting and Frequency of Services.
In acute care, services provided at a high frequency resulted in increased ambulatory ability and functional recovery, as measured by FIM™ scores, and high-intensity exercises resulted in decreased length of stay (LOS) and more favorable discharge destinations (Chudyk, Jutai, Petrella, & Speechley, 2009). Moreover, the addition of occupational therapy to physical therapy services resulted in a larger increase in ambulatory ability and functional recovery. Similar findings were noted for patients receiving occupational therapy and physical therapy in an inpatient setting, with additional improvements noted in LE strength, balance, and falls self-efficacy (Chudyk et al., 2009).
In contrast, another systematic review found that patients receiving intensive occupational therapy, including home visits, had improved ADL status at discharge but did not differ significantly from a control group at 2-mo follow-up (Crotty et al., 2010). No significant differences were found in four domains of quality of life: physical function, general health, physical health, or emotional health (Crotty et al., 2010). This systematic review also found no significant differences between home rehabilitation (focused on physical therapy and functional therapy) and usual care or between group learning (focused on improved function) and no treatment. The group learning intervention did result in perceived improvements in social life immediately postintervention, but not after 12 mo (Crotty et al., 2010). However, 2 RCTs found that home-based rehabilitation programs provided by occupational therapy practitioners resulted in higher confidence in ADLs, higher FIM scores, and increased physical and social activity compared with clinic-based occupational therapy services (Zidén, Frändin, & Kreuter, 2008; Zidén, Kreuter, & Frändin, 2010).
Delivery Model.
Multiple RCTs evaluated outcomes of comprehensive interdisciplinary and multidisciplinary care for clients with hip fractures. One of these studies found that early mobilization and daily rehabilitation provided by physical therapy and occupational therapy practitioners resulted in increased mobility, increased return rate to prior residence, higher ADL function at discharge, and fewer postoperative falls (Stenvall, Olofsson, Nyberg, Lundström, & Gustafson, 2007). A 2nd study reported that a comprehensive care model resulted in ADL improvements and less risk of depression compared with interdisciplinary or usual care (Shyu et al., 2013), and a 3rd study found that interdisciplinary care resulted in more positive functional recovery than individual professional care as measured by mean Chinese Barthel Index scores (Tseng, Shyu, & Liang, 2012). Using a mathematical epidemiological model to investigate fall prevention programs meant to reduce hip fracture, a final study indicated that home modifications provided by occupational therapists, physical therapists, and nurses were more effective than and relatively cost-efficient compared with other interventions (Frick, Kung, Parrish, & Narrett, 2010).
Cognitive and Psychological Impairments.
In addition to physical impairments, people with hip fractures often have cognitive and psychosocial impairments requiring specialized attention. Findings of 3 studies reporting on the impact of and interventions for these impairments were mixed. One systematic review concluded that mild to moderate dementia was not an impediment to rehabilitation after hip fracture and that patients exhibited gains in function (e.g., ADL performance, mobility) similar to those of patients who were cognitively intact.
The evidence regarding the impact of moderate to severe dementia is limited (Allen et al., 2012). Specialized interdisciplinary or multidisciplinary care for cognitive impairments resulted in higher return to independent living, less decline in mobility, and decreases in both fall risk and fall incidence compared with standard care (Allen et al., 2012). In contrast, a Level II longitudinal study found that patients with cognitive impairments required more assistance with ADLs and mobility throughout treatment, at discharge, and at follow-up than the cognitively intact group (Young, Xiong, & Pruzek, 2011). However, the study included a variety of treatment settings and services. Similarly, 1 Level II prospective study found high rates of neuropsychiatric symptoms in patients with hip fracture that, when adjusted for Mini-Mental State Examination scores, resulted in lower motor FIM scores and longer LOS (Gialanella, Prometti, Monguzzi, & Ferlucci, 2014).
Interventions for Hip and Knee Replacement
Fourteen articles reported on interventions for patients who underwent elective hip or knee joint replacement. Although not always the primary focus of the study, the effect of client education by an occupational therapist or other occupational therapy interventions as part of varied service delivery models was evaluated in 8 articles.
Education and Service Delivery.
Four RCTs described the inclusion of occupational therapy as part of the multidisciplinary treatment team for hip or knee replacement in various service delivery models. Occupational therapy practitioners contributed to and delivered educational materials in each study, resulting in client reports of decreased pain intensity; increased general, physical, and mental health scores; decreased disability; increased self-management of the health condition; and a decreased number of occupational therapy visits (Berge, Dolin, Williams, & Harman, 2004; Butler, Hurley, Buchanan, & Smith-VanHorne, 1996; Hørdam, Sabroe, Pedersen, Mejdahl, & Søballe, 2010; Nuñez et al., 2006). Similar results were found in another RCT that found that individually tailored preoperative education focusing on self-care, adaptive equipment, and home modifications in addition to the standard preoperative clinic visit reduced LOS for clients with total hip or total knee arthroplasty (Crowe & Henderson, 2003).
In addition to these studies, another RCT and 1 Level III quasi-experimental study both considered multidisciplinary organization and multimodal interventions in which care was accelerated (Larsen, Hansen, & Søballe, 2008; Larsen, Sørensen, Hansen, Thomsen, & Søballe, 2008). These studies showed that accelerated perioperative care decreased LOS and increased health-related quality-of-life scores for participating clients, and both studies identified occupational therapy intervention as part of the early mobilization of clients with hip and knee replacement (Larsen, Hansen, & Søballe, 2008; Larsen, Sørensen, et al., 2008).
In addition to presurgical education and multidisciplinary postsurgical treatment, a Level III pretest–posttest intervention study showed significantly higher self-reported performance of, satisfaction with, and confidence in completing community-related tasks after completion of a community reintegration program in which occupational therapy practitioners focused on new task training in natural environments (Gillen et al., 2007). Six additional articles did not include enough specific information regarding the occupational therapy interventions.
General Psychosocial Outcomes.
One RCT examined strategies for clients with differing psychological profiles, including those with anxiety, denial about the procedure, and desire for information (Daltroy, Morlino, Eaton, Poss, & Liang, 1998). In this study, effects of a relaxation intervention on postoperative outcomes were limited because of inadequate practice of the intervention before surgery (Daltroy et al., 1998). A Level II longitudinal study found that clients reported less pain and fewer depressive symptoms after total hip replacement when participating in occupational therapy focusing on ADL performance, compensatory strategies for functional limitations, joint protection strategies, and use of adaptive equipment as part of a multidisciplinary approach (Dohnke, Knäuper, & Müller-Fahrnow, 2005). Moreover, these clients showed significant decreases in disability and an increase in depressive symptoms at discharge, whereas average depressive symptoms and pain at 6 mo postsurgery were less than symptoms reported on admission (Dohnke et al., 2005).
Comparisons Between Practice Settings.
One Level II prospective observational cohort study compared services provided to clients with hip and knee replacements in freestanding skilled nursing facilities (SNFs), hospital-based SNFs, and inpatient rehabilitation facilities (DeJong et al., 2009). More than half of clients’ time in occupational therapy was spent engaged in exercise, functional mobility, or lower-body dressing (DeJong et al., 2009). Inpatient rehabilitation facilities and hospital-based SNFs had shorter lengths of stay, likely the result of increased intensity and frequency of therapy interventions (DeJong et al., 2009).
Three studies compared practice settings in which occupational therapy made undefined contributions to the primary interventions. A systematic review concluded that multidisciplinary rehabilitation is effective in inpatient and home-based settings and that short-term gains in functional status occur faster when multidisciplinary rehabilitation is begun early and is organized (Khan, Ng, Gonzalez, Hale, & Turner-Stokes, 2008). A Level II prospective cohort study concluded that postacute care settings admitted different types of clients with hip and knee replacements (Mallinson et al., 2011). Optimal discharge dispositions for clients varied depending on their age, ability, and support system. Clients who needed postacute care services benefited from either inpatient rehabilitation or a SNF equally with respect to functional outcomes. Clients who were younger and more independent and who had support systems benefited most from home health services (Mallinson et al., 2011). Finally, a 2nd Level II prospective cohort study concluded that about 90% of all hip arthroplasty clients, elective or nonelective, received home health or outpatient therapy after the first rehabilitation setting, and patterns of care were driven by the initial care setting (Tian, DeJong, Munin, & Smout, 2010).
Interventions for Lower-Extremity Amputation or Limb Loss
Five studies in this review reported on interventions for patients with LE amputation or limb loss. One of the included articles specifically investigated the effectiveness of occupational therapy intervention for older adults with limb loss (Spiliotopoulou & Atwal, 2012).
Prosthetics and Stump Boards.
The systematic review by Spiliotopoulou and Atwal (2012) included 2 articles that described the use of prosthetics and stump boards. One study found that of the participants with LE limb loss, 81% used their prosthesis daily, and use was linked to client factors including level of physical independence, cognitive status, age, and satisfaction with the prosthesis (Spiliotopoulou & Atwal, 2012). In the other study, all occupational therapists used stump boards for clients with below-knee amputation to prevent knee flexion contractures and to reduce edema. Comfort in a wheelchair, stump protection, and amputation acceptance were reported benefits of using a stump board (Spiliotopoulou & Atwal, 2012).
Practice Setting.
Two articles, both describing Level II prospective cohort studies, evaluated people with dysvascular LE amputation resulting from peripheral vascular disease or diabetes and described outcomes on the basis of practice setting (Czerniecki, Turner, Williams, Hakimi, & Norvell, 2012; Pezzin, Padalik, & Dillingham, 2013). Clients who received comprehensive inpatient rehabilitation services from occupational therapy, physical therapy, rehabilitation psychology, and speech–language pathology within 12 mo of amputation demonstrated greater mobility success, or mobility that was the same as or greater than the premorbid level of mobility, 12 mo postamputation compared with clients who did not receive comprehensive inpatient rehabilitation (Czerniecki et al., 2012). People experienced fewer depressive symptoms and greater emotional and social functioning 6 mo after amputation in inpatient rehabilitation facilities than they did in SNFs and on return to their home (Pezzin et al., 2013). Although the outcomes measured in both articles were within the scope of practice of occupational therapy, the authors did not include any specifics related to occupational therapy beyond that it was part of the comprehensive rehabilitation team.
Sports and Physical Activities.
One systematic review examined participation in sports and physical activities in younger adults with nonvascular LE amputation or limb loss, confirming that participation in sports or physical activities improved general physical conditioning, cardiopulmonary function, and quality of life (Bragaru, Dekker, Geertzen, & Dijkstra, 2011). Sports-related injury patterns and rates of people with LE amputation were similar to those of able-bodied individuals, and the emotional benefits outweighed the risk of injury. Biomechanical aspects of performance varied greatly; overall performance was enhanced or hindered on the basis of various client, equipment, and sport-related variables (Bragaru et al., 2011).
Self-Management.
One RCT examined the effects of a community-based self-management program that consisted of nine sessions focused on self-management principles (knowledge, problem solving, skill acquisition, self-monitoring), pain management, and increasing activity participation and quality of life, among other related topics (Wegener, Mackenzie, Ephraim, Ehde, & Williams, 2009). The intervention was beneficial for lowering the odds of depression immediately postintervention and at 6 mo, reducing functional limitations at 6 mo, and increasing self-efficacy immediately after the intervention (Wegener et al., 2009). Although this program was led by trained volunteer leaders, the topics covered in the intervention fit within the scope of practice of occupational therapy practitioners, highlighting a potential role for occupational therapy with this population.
Interventions for Nonsurgical Disorders
Ten articles were included in the nonsurgical category, which included hip or knee OA and hip or knee pain, weakness, or both. Interventions were geared toward activity pacing (n = 3), self-management (n = 4), and education (n = 3).
Activity Pacing.
All 3 studies targeting activity pacing were RCTs and included occupational therapy as the main intervention. Murphy, Lyden, Smith, Dong, and Koliba (2010) described a pilot study, and Murphy, Smith, and Lyden (2012) and Schepens, Braun, and Murphy (2012) conducted secondary analyses of their data. Murphy et al. (2010) found that a tailored activity-pacing group resulted in significantly less negative effect on activity from fatigue but no difference in pain or severity of fatigue. Schepens et al. found that a tailored activity-pacing group for hip and knee OA showed significant improvements in self-perceived stiffness at 4 wk and 10 wk postintervention, whereas the control group’s stiffness returned to baseline at 10 wk. Murphy et al. (2012) found that the outcomes of the tailored activity-pacing group included a significant decrease in activity variability (defined as the standard deviation of the 5-day average of daily activity counts per minute) but no difference in average activity levels (defined as 5-day average of daily activity counts per minute).
Self-Management.
Brand, Nyland, Henzman, and McGinnis (2013) conducted a systematic review and meta-analysis that looked at the effects of self-management education and exercise for people with knee OA, and some of the included studies incorporated occupational therapy as part of the intervention. Self-management education plus exercise interventions did not improve outcomes; the outcomes were positive regardless of the inclusion of exercise. Other articles did not include occupational therapy but provided interventions that fell within the occupational therapy scope of practice.
One RCT investigated the effects of a self-management group led by physical therapists and found significant improvements in pain and function in the intervention group at 3-mo and 21-mo follow-up (Heuts et al., 2005). A 2nd RCT that investigated the impact of a 6-wk self-management program for hip or knee OA found no difference in health-related quality of life (HRQOL) at 12 mo (Ackerman, Buchbinder, & Osborne, 2012). In contrast, Kao, Wu, Tsai, Chang, and Wu’s (2012) Level II study found that participants in a 4-wk self-management program for knee pain had significant improvements in HRQOL from baseline to postintervention and at 8-wk follow-up, but they found no significant difference in self-reported disability level.
Education.
Tak, Staats, Van Hespen, and Hopman-Rock’s (2005) RCT found that an 8-wk tailored home exercise program and ergonomic education had a positive effect on pain, hip function, self-reported disability, and Timed Up and Go scores, but no effect on quality of life or observed disability. In this study, occupational therapists helped develop the intervention and provided the ergonomic education. In another clinical trial, an individualized educational intervention focused on knee OA pain management, joint protection, and problem solving for daily activities resulted in significantly lower disability scores and resting knee pain at 4 and 8 mo postintervention but not at 12 mo (Mazzuca et al., 1997). No significant effect was found on overall joint pain, general health status, or knee pain during walking, and occupational therapy was not involved in this study (Mazzuca et al., 1997). A final RCT conducted by Arnold, Faulkner, and Gyurcsik (2011) found that an aquatics program plus fall prevention education resulted in significant improvements in balance and falls efficacy; the control group experienced no effect on falls efficacy. This study did not include occupational therapy (Arnold et al., 2011).
Discussion
This is the first systematic review to evaluate the literature on the effectiveness of occupational therapy interventions for LE MSDs. The four most commonly mentioned diagnosis population groups were people with hip fracture, hip or knee replacement, LE amputation or limb loss, and nonsurgical OA and pain, which is consistent with trends in impairments and injuries in the United States. Although we initially set out to categorize the results on the basis of the occupational therapy interventions provided, it became readily apparent that this was not possible because of the small number of articles that fully described occupational therapy’s role in the intervention protocols.
This review presented us with a challenge to determine inclusion and exclusion criteria that were appropriate to the role of occupational therapy with the LE. Interventions that were excluded from this review because of a lack of focus on occupation or function may have been appropriately included in reviews for other questions, such as those concerning the upper extremity. For example, interventions that were primarily a modality (e.g., electrical stimulation) or based on targeted exercise (e.g., isolated quadriceps strengthening) were excluded because occupational therapy practitioners do not typically fill this role on the health care team for LE MSDs.
Although occupational therapy practitioners may use non–occupation-based interventions and outcome measurements, we were most interested in describing evidence that supported the distinct value of occupational therapy (Arbesman, Lieberman, & Metzler, 2014), which includes a focus on occupation and increased functional outcomes such as ADL performance. However, articles that did not include an occupational therapy practitioner in the intervention but that met all inclusion criteria were reviewed. This allowed for the evaluation of interventions within the scope of occupational therapy practice, with the recognition that occupational therapy may not have been involved in the study for a variety of reasons (e.g., country of origin, lack of availability). These decisions led to the results of this review, which add to the body of literature on LE MSDs.
Overall, strong evidence supports the role of occupational therapy in working with clients with hip fracture. However, because of the lack of occupational therapy–specific literature, the evidence to support specific occupational therapy interventions for hip fracture is insufficient. Strong evidence supports the role of occupational therapy practitioners on multidisciplinary teams working with people with hip or knee replacement. Moderate evidence supports the role of occupational therapy practitioners as part of a multidisciplinary rehabilitation team for people with LE amputation or limb loss. The evidence supporting specific occupational therapy interventions for LE amputation or limb loss is insufficient. Moderate evidence supports activity pacing as an occupational therapy intervention for hip and knee OA, but the evidence to support self-management as an occupational therapy intervention for hip and knee OA is insufficient. The evidence to support education as an occupational therapy intervention for hip and knee OA and pain is also insufficient.
Current trends in the health care system, such as the focus on management of chronic conditions through a primary care approach and CMS’s Comprehensive Care for Joint Replacement model, demand that attention be paid to rehabilitation services for LE MSDs. Occupational therapy has a distinct value with LE MSD populations, as seen in practice. However, the results of this systematic review highlight a significant gap in the literature regarding effectiveness of specific interventions used by occupational therapy practitioners, especially when occupational therapy is used in combination with other interventions or as part of an interdisciplinary care plan. This gap presents an opportunity to develop evidence that can inform occupational therapy interventions. Building the evidence base will help define occupational therapy’s value for people with LE MSD.
Strengths and Limitations of This Review
This systematic review followed an established methodology that has been used for previous EBP projects. Both review authors were involved in all decisions regarding the inclusion and exclusion of articles, which eliminated potential issues with interrater reliability. In addition, a large range of literature from varied disciplines was considered. However, the systematic review is limited by the reviewers’ judgment of the articles as being within the scope of occupational therapy for LE MSDs. Only 8 articles that investigated occupational therapy as the main intervention were included, which limited our ability to draw conclusions.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice:
Multidisciplinary rehabilitation for hip replacement and knee replacement, focusing on education, ADL performance, compensatory strategies for functional limitations, joint protection strategies, adaptive equipment training, functional mobility training, and upper-body exercise, is effective when provided in inpatient or home-based settings.
Occupational therapy services provided by a multidisciplinary rehabilitation team can benefit people with LE amputation or limb loss.
Occupational therapy practitioners should consider using activity pacing as an intervention for adults with LE OA.
This study points to the need for further research investigating the effectiveness of occupational therapy interventions for LE MSDs.
Supplemental Materials
Supplementary material for Effectiveness of Occupational Therapy Interventions for Lower-Extremity Musculoskeletal Disorders: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2017.023028.pdf for Effectiveness of Occupational Therapy Interventions for Lower-Extremity Musculoskeletal Disorders: A Systematic Review by Julie Dorsey and Michelle Bradshaw in The American Journal of Occupational Therapy
Supplementary material for Effectiveness of Occupational Therapy Interventions for Lower-Extremity Musculoskeletal Disorders: A Systematic Review
Supplementary material, sj-pdf-2-aot-10.5014_ajot.2017.023028.pdf for Effectiveness of Occupational Therapy Interventions for Lower-Extremity Musculoskeletal Disorders: A Systematic Review by Julie Dorsey and Michelle Bradshaw in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We thank Deborah Lieberman and Marian Arbesman for their assistance and support with this project. We also thank Ithaca College occupational therapy graduate students Meagan Toner, Jillian Hendzlik, and Katharyn Parini for their assistance during this project.
*Indicates studies that were included in the systematic review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.