
Abstract
Fatigue can be defined as “a multifaceted condition characterized by diminished energy and an increased need to rest, disproportionate to any recent change in activity level” (Mitchell & Berger, 2006, p. 374). According to de Groot, Phillips, and Eskes (2003), there is a distinct difference between pathological fatigue and normal fatigue. Normal fatigue is feelings of tiredness resulting from overexertion that can be improved with rest, whereas pathological fatigue is not related to exertion level and cannot be remediated with rest (Ahlberg, Ekman, Gaston-Johansson, & Mock, 2003; de Groot et al., 2003). Fatigue is a serious and problematic concern for people living with chronic disease conditions such as multiple sclerosis (MS), fibromyalgia, chronic fatigue syndrome, cancer, and stroke. For people with a chronic condition, fatigue may become a distressing symptom that is tolerated as part of the disease process (de Groot et al., 2003). However, such fatigue is often debilitating, interfering with daily functioning and quality of life (Benedict et al., 2005; Finlayson, Preissner, Cho, & Plow, 2011). Specifically, fatigue may affect patients and family members physically, socially, mentally, vocationally, emotionally, and spiritually (Mitchell & Berger, 2006).
Fatigue is a common symptom addressed by occupational therapy practitioners typically through the use of fatigue management education. The goal is to reduce the impact of fatigue on patients and to improve participation in meaningful occupations (Fox, 2010). The Managing Fatigue program, a 6-wk energy conservation course, was developed by occupational therapists to help people with fatigue resulting from a chronic condition (Packer, Brink, & Sauriol, 1995). In this group course, participants learned energy conservation strategies and implemented them into their daily lives. As a result of the course, many participants made behavioral and environmental changes to conserve energy and improve their occupational performance and quality of life (Finlayson, 2005).
An initial study found the course to be effective in reducing the impact of fatigue and increasing self-efficacy and some aspects of quality of life among participants with mild to moderate MS (N = 54; Mathiowetz, Matuska, & Murphy, 2001). A second study yielded similar results in reducing the impact of fatigue among participants with moderate to severe MS (N = 37; Vanage, Gilbertson, & Mathiowetz, 2003). Moreover, results were maintained 6 wk and 8 wk poststudy (Mathiowetz et al., 2001; Vanage et al., 2003).
In 2005, Mathiowetz, Finlayson, Matuska, Chen, and Luo conducted a randomized controlled trial (RCT) to assess short-term efficacy of the 6-wk energy conservation course for people with MS. There was a significant decrease in fatigue impact (ds = 0.52–0.74) and a significant increase in self-efficacy (d = 1.82) and some aspects of quality of life: vitality (d = 0.99) and mental health (d = 0.53). In 2007, Mathiowetz, Matuska, Finlayson, Luo, and Chen conducted a 1-yr follow-up RCT to determine whether the results of their 2005 study were maintained. Findings indicated significant improvements on all subscales of the Fatigue Impact Scale (Fisk et al., 1994) and on four subscales of the 36-item Short-Form Health Survey (Ware, Snow, Kosinski, & Gandek, 1993) 1-yr postcourse compared with precourse. The results of this study indicate that beneficial effects of the energy conservation course were maintained up to 1 yr postcourse (Mathiowetz et al., 2007).
Although the group course was found to be effective, it was limited to people who were able to travel to the instruction site (Finlayson et al., 2011). As a solution, the course was adapted into a teleconference format with 70-min calls once per week, taught by occupational therapists trained in the curriculum. After the 6-wk course, participants (n = 89) reported a decrease in fatigue severity and fatigue impact; however, the effect sizes were smaller (ds = 0.35–0.52) than those found in prior studies (Finlayson, 2005). Participants stated that lack of face-to-face contact and not seeing activities physically demonstrated were pitfalls of the course.
Although the group and teleconference formats of the 6-wk energy conservation course were found to be effective, the delivery methods are not practical for implementation in clinical settings (Fox, 2010). The Managing Fatigue course has recently been adapted into an in-person, one-to-one format (Fox, 2010), but its efficacy remains untested.
Purpose and Significance of the Study
The purpose of this study was to determine the effects of the one-to-one format of the 6-wk Managing Fatigue course developed by Fox (2010) on reducing fatigue and improving quality of life, self-efficacy, and energy conservation behaviors in people with chronic conditions and fatigue. Previous research has shown the effectiveness of other course formats in providing energy conservation strategies to manage fatigue in people with MS. Finding the one-to-one format to be effective will support its use in clinical practice for a broad range of chronic conditions and will enhance evidence-based practice in occupational therapy. In addition, the one-to-one format would make reimbursement for fatigue management education easier because some insurance companies do not cover group interventions. Finally, this more individualized format may benefit people with fatigue who are uncomfortable with a group format.
This study addressed the following research question: Does the one-to-one format increase the frequency and effectiveness of participants’ energy conservation behaviors at the 6-wk follow-up to the course? The two study hypotheses were
Participants with chronic conditions and fatigue will report a significant decrease in fatigue and a significant increase in quality of life and self-efficacy after participation in a one-to-one fatigue management course as compared with before the course.
The beneficial effects of the course will be maintained at the 6-wk follow-up.
Method
Design
This observational study used a one-group, pretest–posttest, follow-up design. A convenience sample of participants completed pretesting before starting the one-to-one fatigue management course. After completion of the course, posttesting determined the immediate effects of the course. After a 6-wk no-intervention period, follow-up assessments were administered to determine whether beneficial effects were maintained and whether energy conservation behaviors had changed.
Participants
Participants were recruited through the Midwest Chapter of the National Multiple Sclerosis Society, which sent recruitment flyers to all of its current members in the Twin Cities. Flyers were also distributed at churches and community centers. Occupational therapists also recruited participants through an outpatient rehabilitation center. Interested persons contacted the researchers and were screened over the phone.
The inclusion criteria were as follows: a diagnosis of a chronic disease, moderate to severe fatigue, age 18 yr or older, and the ability to read and understand English. During the phone screening, prospective participants were administered the Fatigue Severity Scale (FSS; Krupp, LaRocca, Muir-Nash, & Steinberg, 1989). An average score of 4 out of 7 or higher on the FSS was required to meet the inclusion criteria of moderate to severe fatigue. The exclusion criteria included a score lower than 18 on the full Montreal Cognitive Assessment (MOCA; version 7.1; Nasreddine, 2003), which represents moderate to severe cognitive impairment. The MOCA was administered at the first in-person session in an outpatient or community-based setting. This study was approved by the university’s institutional review board (No. 1406M51183), and all participants provided informed consent before completing the pretest assessments.
One-to-One Fatigue Management Course
The course was adapted for individual delivery by Fox (2010) 1 and consists of five modules: (1) Basics of Fatigue, (2) Communication and Fatigue, (3) Body Mechanics and Making the Most of Your Environment, (4) Analyzing and Modifying Activities, and (5) Living a Balanced Lifestyle. The Therapist Resource Guide provides background and instruction on how to use the course materials. The patient education materials consist of new content for each session and homework designed to challenge participants to apply the concepts to their life. Two additional handouts address secondary fatigue and cognitive fatigue (Fox, 2010). Instructors were occupational therapists and occupational therapy students. The latter had completed coursework on fatigue management, observed a 2-hr video of a group fatigue management session, and reviewed patient education materials with a fatigue management expert. All instructors followed the systematic instructions for course administration so that the course could be replicated.
During the first face-to-face meeting, participants were provided with an overview of the course and the first one or two modules. The researchers then gave the participants homework, answered questions, and set up a date for the next meeting. In subsequent sessions, homework was reviewed, questions were answered, and participants were instructed in the next module in the course. Sessions lasted 1–2 hr for four to six sessions until all modules and additional handouts were addressed.
Primary Outcomes
Functional Assessment of Chronic Illness Therapy–Fatigue Scale.
The Functional Assessment of Chronic Illness Therapy–Fatigue Scale (FACIT FS; Smith, Lai, & Cella, 2010) consists of 13 Likert-scale questions. Several of the questions speak to the way a person feels, and others ask about a person’s ability to complete daily tasks. The scale has been validated in various clinical populations and the general population, has high test–retest reliability (r = .90), and is highly correlated with other measures of fatigue (Smith et al., 2010). The FACIT FS was written at a fourth-grade level and is thus appropriate for use with people with limited literacy or comprehension skills (Webster, Cella, & Yost, 2003). The FACIT FS was deemed most appropriate for this study because of its simplicity and established reliability and because it has been shown to be accurate across various conditions associated with fatigue.
Functional Assessment of Cancer Therapy–General.
The Functional Assessment of Cancer Therapy–General (FACT–G; Cella et al., 1993) has 27 Likert-scale questions over four subscales that address physical, emotional, social, and functional well-being. The FACT–G has been widely validated for people with cancer, MS, and HIV (Webster et al., 2003). A study of cancer patients found the FACT–G to have high test–retest reliability, with r = .92 for the total scale and ranging from .82 to .88 for the subscales (Cella et al., 1993).
Self-Efficacy for Performing Energy Conservation Strategies Assessment.
The 14-item Self-Efficacy for Performing Energy Conservation Strategies Assessment (SEPECSA; Liepold & Mathiowetz, 2005) measures the confidence that people have in their ability to perform energy conservation and fatigue management strategies. People with high self-efficacy feel better about themselves and believe they can accomplish their goals (Liepold & Mathiowetz, 2005). A measure of self-efficacy is important to use with people with fatigue because they often have feelings of inadequacy in fulfilling their roles and accomplishing their goals. Mathiowetz et al. (2001, 2005) reported that the group energy conservation course increased self-efficacy.
The SEPECSA is scored by having participants rate their confidence in implementing the 14 energy conservation and fatigue management strategies addressed in the course on a scale ranging from 1 (not at all confident) to 10 (completely confident; Liepold & Mathiowetz, 2005). Researchers determined that the SEPECSA’s internal consistency was very high (α = .93; Liepold & Mathiowetz, 2005). It was also found to have some evidence of construct validity, because participants’ self-efficacy increased after the 6-wk energy conservation course as hypothesized and did not change after a no-treatment control period (Liepold & Mathiowetz, 2005). The study concluded that an increased score on the SEPECSA reflects a true change in a person’s self-efficacy because it was found to have high test–retest reliability (intraclass correlation coefficient [ICC] = .771, r = .776), and no significant difference was found between the pre- and posttest no-treatment control means (Liepold & Mathiowetz, 2005).
Secondary Outcomes
Energy Conservation Strategies Survey.
The Energy Conservation Strategies Survey (ECSS; Mallik, Finlayson, Mathiowetz, & Fogg, 2005) is a 14-item self-administered instrument that was designed and implemented with people with MS. It was used to identify and measure energy conservation and fatigue management principles 6 wk after the completion of the energy conservation course. For the survey, participants are first asked whether they have carried out a specific strategy learned during the course (Mallik et al., 2005). If participants answer “yes” to the first question, they report how many changes they made, how frequently they used the strategies, and how effective the strategies were for reducing fatigue (Mallik et al., 2005). Effectiveness of the strategies is rated on a scale ranging from 1 (not effective) to 10 (highly effective; Mallik et al., 2005). If participants answer “no” to the first question, they are asked to identify the reason for not carrying out a specific strategy (Mallik et al., 2005).
The ECSS demonstrated good internal consistency (α = .92). There was also a strong correlation (r s = .87) between the rank orderings of items from 6 wk to 7 wk postintervention, which suggests that the level of implementation of items is stable over time (Mallik et al., 2005). In addition, the effectiveness ratings showed high test–retest reliability (ICC = 0.79; Mallik et al., 2005), which supports the stability of the ECSS.
All primary and secondary outcome measures were self-assessments completed by participants. The course instructors distributed the assessments to the participants at the three testing times.
Procedures
After institutional review board approval, occupational therapists and occupational therapy students recruited and screened potential participants as described earlier. After screening, potential participants completed the consent process. Participants then completed demographics and medication forms as well as the FACIT FS, FACT–G, and SEPECSA to determine pretest outcomes. Over the next 6 wk, researchers delivered the course using the process described earlier. On finishing the course, participants were administered the outcome measures a second time to determine posttest outcomes. After posttest, the participants experienced a period of no intervention for 6 wk. The researchers arranged for a 6-wk follow-up meeting, at which participants completed the outcome measures for a third time, plus the ECSS. If participants were unable to meet in person, the researchers arranged to mail the scales to them with return postage.
Data and Statistical Analysis
Descriptive statistics were used to determine the means and standard deviations for pretest, posttest, and follow-up scores and some demographic variables. Inferential statistics were used to examine changes in FACIT FS, FACT–G, and SEPECSA scores. One-way repeated-measures analyses of variance (ANOVAs) were performed to analyze the data using IBM SPSS Statistics software for Windows (Version 22; IBM Corp., Armonk, NY). Paired-data t tests were used for post hoc analysis (pretest vs. posttest and posttest vs. follow-up), and p < .05 was used to determine significance. Results for the ECSS were analyzed using descriptive statistics. Frequencies and percentages were determined for those who adopted energy conservation behaviors.
Results
Figure 1 describes the progression of participants through the study. The occupational therapists and occupational therapy students received 142 phone calls, emails, and in-person requests from potential participants. Of the 55 participants enrolled in the study, 40 were instructed by the trained occupational therapy students, and 15 additional participants were instructed by the occupational therapists. The remaining eligible participants were not included in the study because of time constraints. Of the 55 participants, 6 dropped out. The data of the 49 remaining participants (35 women, 14 men) were included in the data analysis. Ages ranged from 35 to 77, with the average age being 56.4 (see Table 1). Eighteen participants reported being unemployed because their disability resulted in an inability to work. Although recruitment aimed to reach people with a variety of chronic conditions, 71.4% of enrolled participants had a primary diagnosis of MS. The other participants’ diagnoses are described in Table 1.
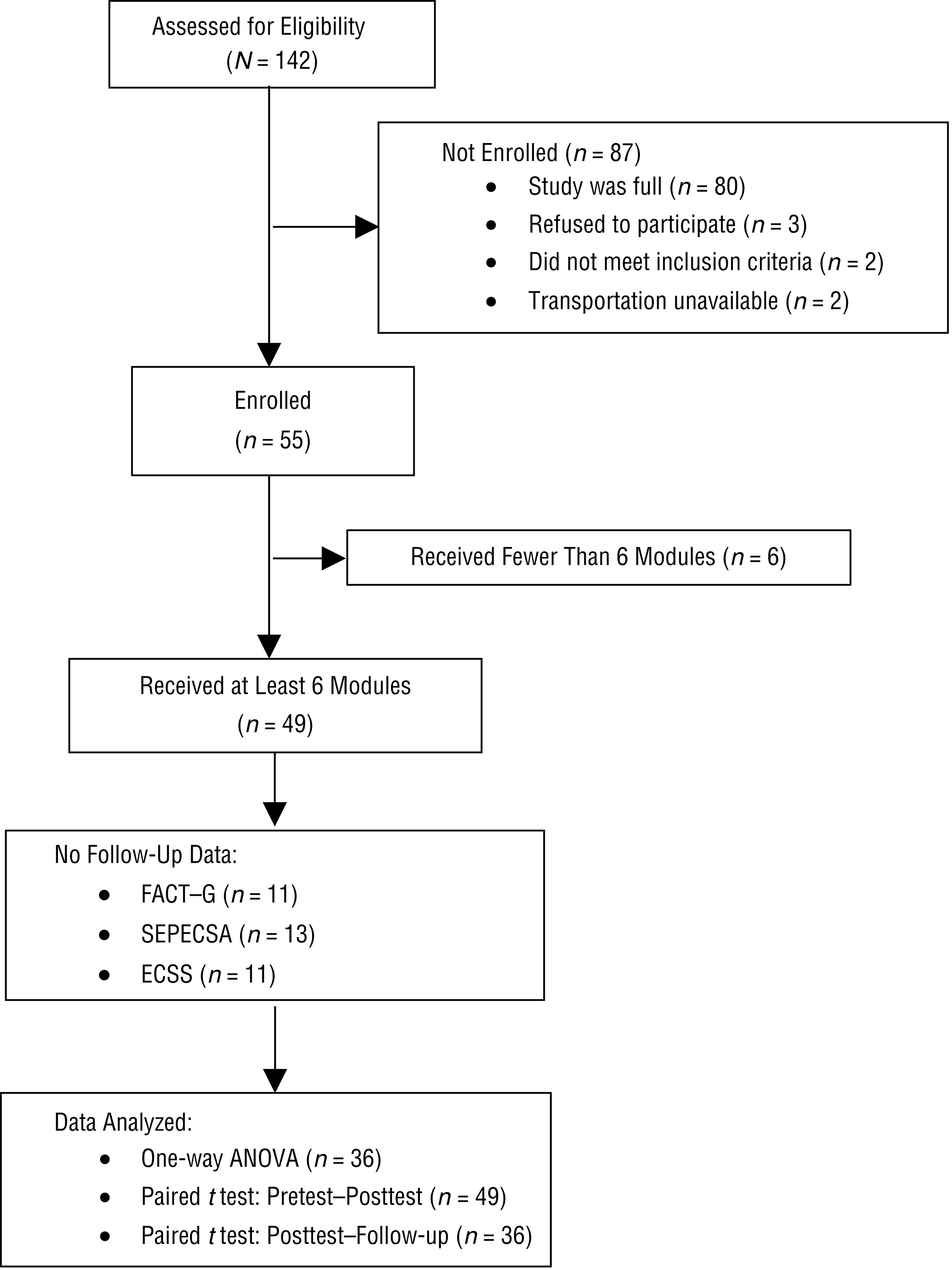
Progression of participants through the study.
Demographic Characteristics of Participants (N = 49)
Note. FSS = Fatigue Severity Scale; M = mean; SD = standard deviation.
Primary Outcomes
Participants experienced a reduction in their level of fatigue as measured by the FACIT FS, an increase in their overall quality of life as measured by the FACT–G, and an increase in self-efficacy as measured by the SEPECSA (see Table 2). One-way repeated-measures ANOVAs (p < .05) were performed on primary outcome scores. Significant within-subjects effects were found for the FACIT FS (p = .001), FACT–G total score (p = .021), and SEPECSA (p = .001). In addition, scores on three of the four FACT–G subscales were significant: Physical Well-Being (p = .002), Emotional Well-Being (p = .007), and Functional Well-Being (p = .024). In contrast, no significant within-subjects effect was found for the Social Well-Being subscale (p = .535).
Descriptive Data, Paired-Data t Tests, and Cohen’s d Effect Sizes for Outcome Measures
Note. For pretest vs. posttest, n = 49; for posttest vs. follow-up, n = 36. FACIT FS = Functional Assessment of Chronic Illness Therapy–Fatigue Scale; FACT–G = Functional Assessment of Cancer Therapy–General; SD = standard deviation; SEPECSA = Self-Efficacy for Performing Energy Conservation Strategies Assessment.
Subscales of the FACT–G.
Follow-up planned comparisons (paired t tests) were used to compare pretest versus posttest and posttest versus follow-up scores. With a Bonferroni correction for two comparisons, p < .025 was needed for significance. By the posttest, participants on average saw statistically significant improvements and large effect sizes across all primary outcome areas except the Social Well-Being subscale (see Table 2). Each of the positive changes had regressed slightly when measured at 6-wk follow-up, but this lessening was in no case statistically significant and had a small effect size (see Table 2).
Secondary Outcomes
The ECSS strategies that were implemented the most (≥75% of the participants) included modifying standards, adjusting priorities, and communicating the need for help. The strategies that were implemented the least (≤64% of the participants) included changing the location of equipment, height of work surfaces, and the time of day for activities. Of the energy conservation strategies, 71% were identified by the participants as effective (score range = 7.6–8.3). The most effective strategies (score ≥ 8.1) included planning days to balance work and rest, including rest periods, resting during fatiguing activities, and adjusting priorities. The least effective strategies (score ≤ 7.4) included changing height of work surfaces, changing body positioning, and communicating the need for help.
Discussion
Primary Outcomes
From pretest to posttest, participants showed significant reductions in fatigue and significant increases in self-efficacy and quality of life, except in social well-being. These results plus the large effect sizes provide strong support for Hypothesis 1, except for the one quality-of-life subscale. No significant differences in and small effect sizes among the primary outcomes were found between posttest and follow-up. These results provide strong support for Hypothesis 2, which predicted that the beneficial effects would be maintained in the 6 wk after the course.
These results are also consistent with the results of studies on the group fatigue management and energy conservation course (Finlayson et al., 2011; Mathiowetz et al., 2001, 2005, 2007; Vanage et al., 2003). This finding suggests that the one-to-one format has similar beneficial effects as the group format. Because the one-to-one format is more compatible with current clinical practice, it provides occupational therapy practitioners with a new tool for providing fatigue management education. A comparison of the one-to-one format with previous literature on the group format indicates that both formats were effective in increasing self-efficacy. However, the group format had a larger effect size (d = 1.92; Mathiowetz et al., 2005) than that found in this study (d = 0.93), which may be attributed to the fact that the group format allowed for greater social support, accountability, and problem solving among participants.
Secondary Outcomes
Findings indicated that participants implemented many of the 14 energy conservation strategies from the course into their daily lives and that they reported most strategies adopted to be effective. This finding suggests that what is being taught in the energy conservation and fatigue management course is reflective of the needs of the participants. Implementation of these strategies assists participants in managing their fatigue in a more effective manner to maintain participation in valued roles and occupations. Results indicate that the research question (Does the one-to-one format of the 6-wk fatigue management course increase energy conservation behaviors for people with chronic conditions and fatigue?) was strongly supported.
Comparison of the ECSS results from this study with those of Matuska, Mathiowetz, and Finlayson (2007) showed that the group and one-to-one format were similar. In both studies, most of the energy conservation strategies were rated as effective, and the highest rated strategies included rest (Matuska et al., 2007). Subsequently, the effectiveness of the one-to-one format may be attributed to the client-centered care, because participants were able to share private information in a comfortable environment and set their own goals. Because practitioners typically treat clients with chronic conditions individually, these findings are important because they provide evidence for the use of the standardized one-to-one fatigue management course (Fox, 2010) in clinical practice.
Strengths and Limitations of the Course
This fatigue management course has already been proven effective in the group and teleconference formats (Finlayson et al., 2011; Mathiowetz et al., 2001, 2005, 2007; Vanage et al., 2003). Previous researchers had postulated that the benefits of the course could be in part the result of social support provided by the group format (Mathiowetz et al., 2001), so it is encouraging to see that the one-to-one format has similar benefits. Two broad qualities of the one-to-one course, its interactive and personalized nature, may have contributed to its efficacy. Homework assignments and discussion prompts built into the course promoted interaction and encouraged participants to apply the course material to their own situation. Although the course material is standardized, researchers were able to spend more time on modules that participants found pertinent to their own situations. This is one advantage the one-to-one format has over the group format. In a group format, course delivery would be less responsive to the needs of any single participant. The one-to-one format also allowed researchers to use therapeutic use of self in a more targeted way.
Factors that might have limited course efficacy include lack of peer social support and application to social activities, emphasis on remediation of deconditioning, experiential teaching techniques, and accountability for homework completion. First, the course lacked the peer support offered by the group format. Peer groups can facilitate social support, peer problem solving, and discussions that incorporate a wide variety of views. The one-to-one format cannot match these strengths. Perhaps because of this lack of peer support, the Social Well-Being subscale of the FACT–G was the only subscale on which participants showed no significant improvement between pretest and posttest. Researchers initially questioned whether the course could be as effective without the peer support provided by the group format. Results indicate that it came relatively close, but a direct comparison of the group and one-to-one formats is needed to explore their relative strengths and weaknesses.
Second, the fatigue management concepts were applied more to self-care or work activities than to social activities. This limited emphasis on social activities might have contributed to the participants’ lack of change in social well-being on the FACT–G. Third, the course had limited emphasis on remediation of deconditioning. Content on graded activities and exercise to counteract deconditioning and to increase available energy would be a suggested addition to the course in the future. Fourth, the course was more discussion based than experiential, possibly limiting its efficacy for people who learn best using a more hands-on approach. Because course results were considered using averages, it is possible that the course was very effective for those whose learning styles best matched the teaching style of the course and ineffective for others.
Finally, some participants did not finish their homework, which may have limited course efficacy. In the future, course participants may benefit from beginning their homework during a session (rather than at home), which could lead to greater course efficacy. Participants could have been held more accountable through weekly goal setting, and instructors could have emphasized more the importance of completing homework to receive maximum benefits from the course.
Study Strengths and Limitations
Study strengths were, first, there were enough participants in the study to make drawing more general conclusions appropriate (the number of participants led to fair statistical power). Second, the standardization of the course means that occupational therapy practitioners can easily make use of the material. Third, the outcome measures used in the study were sensitive to change.
The major limitations of this study were the lack of random assignment and a control group. The lack of comparison between participants and a no-treatment control group made it impossible to rule out the Hawthorne effect and to ascribe the positive results noted by participants strictly to the intervention. The study also primarily consisted of participants with MS, which limits generalizability to other conditions. In addition, medication and therapy changes were not documented throughout the course of the study. It is uncertain whether the results observed in the study were solely due to the course or whether possible medication and therapy changes also contributed to participants’ improvement. Obtaining follow-up data was challenging because of the follow-up time frame and level of commitment required. Finally, this study used the FACIT FS tool to measure results, whereas previous studies used the Fatigue Impact Scale. This difference limits the ability to compare the efficacy of course formats across studies.
Recommendations for Future Research
Future researchers should consider implementing a large-scale study with random assignment and a control or alternative intervention group—for example, a study comparing the effectiveness of the one-to-one and group formats with particular effort made to identify their relative areas of strength and weakness. A larger study could provide further insight into which populations would benefit most from which course format. Monitoring changes in participant medication and placing an emphasis on obtaining an increasingly diverse sample would also be beneficial. Participants in future research studies may also find explicit goal setting during the course, with periodic review, to be advantageous.
Implications for Occupational Therapy Practice
This study’s findings provide evidence that the fatigue management course’s one-to-one format is effective in decreasing fatigue, increasing self-efficacy, supporting many aspects of quality of life, and increasing the implementation of energy conservation strategies for people with chronic conditions and moderate to severe fatigue, especially people with MS.
Footnotes
Acknowledgments
The authors thank the therapists, Robin Samuel, MSCS, OTR/L, and Laura Chiabotti, MOT, OTR/L, for help with recruitment and course administration; Megan Sparks of the Midwest Chapter of the National MS Society for help in recruitment; the MS Achievement Center for opening their space to the researchers; and all study participants, without whom the study would have not been possible.
Note. Each issue of the 2017 volume of the American Journal of Occupational Therapy features a special Centennial Topics section containing several articles related to a specific theme; for this issue, the theme is occupational therapy's role in health, well-being, and quality of life. The goal is to help occupational therapy professionals take stock of how far the profession has come and spark interest in the many exciting paths for the future. For more information, see the editorial in the January/February issue, ![]() .
.
1
These materials can be obtained from the author, Kara Jane Fox, at