
Abstract
This article is the first part of a systematic review of evidence for the effectiveness of cancer rehabilitation interventions within the scope of occupational therapy that address the activity and participation needs of adult cancer survivors. This article focuses on the importance of physical activity and symptom management. Strong evidence supports the use of exercise for cancer-related fatigue and indicates that lymphedema is not exacerbated by exercise. Moderate evidence supports the use of yoga to relieve anxiety and depression and indicates that exercise as a whole may contribute to a return to precancer levels of sexual activity. The results of this review support inclusion of occupational therapy in cancer rehabilitation and reveal a significant need for more research to explore ways occupational therapy can positively influence the outcomes of cancer survivors. Part 2 of the review also appears in this issue.
Cancer may result in impairments, activity limitations, and participation restrictions (Fialka-Moser, Crevenna, Korpan, & Quittan, 2003; Grov, Fosså, & Dahl, 2010; Hewitt, Rowland, & Yancik, 2003; Hwang, Lokietz, Lozano, & Parke, 2015). Cancer survivorship covers the time from diagnosis until the end of life (National Cancer Institute, 2015). Cancer survivors may have declines in functioning and participation in areas ranging from mobility to return to work (Hwang et al., 2015; Kroenke et al., 2004; Nomori, Watanabe, Ohtsuka, Naruke, & Suemasu, 2004). Adults with cancer experience decreased levels of physical functioning and participation in social, work, and leisure activities compared with before diagnosis regardless of the kind of cancer or type of treatment received (Ganz et al., 2004; Grov et al., 2010). The lowest function is experienced after treatment, with function increasing over time, although functional recovery is moderated by pain and co-occurring diseases (Hwang et al., 2015; Ko, Maggard, & Livingston, 2003).
The Institute of Medicine and National Research Council have strongly suggested that cancer survivor research should include expanded exploration of alternative models of survivorship care, such as supportive care and rehabilitation programs (Hewitt, Greenfield, & Stovall, 2006; Institute of Medicine, 2013). However, a major problem in the U.S. health care system is that cancer survivors are frequently not referred for and do not receive specialized rehabilitation care appropriate for their diagnosis (Cheville, Troxel, Basford, & Kornblith, 2008; Pergolotti, Cutchin, Weinberger, & Meyer, 2014). Rehabilitation is the standard of care for conditions such as heart disease or stroke but, unfortunately, not for cancer and cancer survivorship (Cheville et al., 2008; Segal et al., 1999).
Cancer rehabilitation can benefit people with cancer from diagnosis to end-of-life care. The goals of cancer rehabilitation might focus on symptom management or helping a survivor return to work or community participation (Gamble, Gerber, Spill, & Paul, 2011). The role of occupational therapy practitioners is well suited to helping cancer survivors at all stages of illness.
Objective of the Systematic Review
The objective of the cancer rehabilitation review was to systematically search for and assess interventions within the scope of occupational therapy practice to improve occupational engagement. The focused question guiding selection of research studies for review was “What is the effectiveness of cancer rehabilitation interventions within the scope of occupational therapy practice to address the activity and participation needs of adult cancer survivors in activities of daily living, instrumental activities of daily living, work, leisure, social participation, and rest and sleep?”
This systematic review was supported by the American Occupational Therapy Association (AOTA) as part of the Evidence-Based Practice (EBP) Project (Lieberman & Scheer, 2002). Because of the breadth of the systematic review, the results were divided into two parts. In this article, we report on Part 1 of the systematic review, which is focused on the importance of physical activity and symptom management for cancer survivors. Part 2, also in this issue, is focused on multidisciplinary rehabilitation and interventions that address psychosocial outcomes, sexuality, and return to work.
Method
Process
The research question and search terms for the reviews were developed by the methodology consultant, AOTA staff, and the advisory group in consultation with the review authors. The search terms were related to population (adult cancer survivors), types of intervention, outcomes, sequelae, and types of study design to be included in the systematic review. A medical research librarian with experience in completing systematic review searches conducted all searches and confirmed and improved the search strategies. Databases and sites searched included Medline, PsycINFO, CINAHL, and OTseeker. In addition, consolidated information sources, such as the Cochrane Database of Systematic Reviews, were included in the search. Reference lists from articles included in the systematic reviews were examined for potential articles, and selected journals were hand searched to ensure that all appropriate articles were included.
Inclusion Criteria
Included in the review were peer-reviewed scientific articles on adults with cancer published in English between 1995 and 2014 and within the scope of practice of occupational therapy. The review excluded data from presentations, conference proceedings, non–peer-reviewed research literature, dissertations, and theses. The review also excluded studies focusing on caregivers, family members, or friends rather than cancer survivors; studies of childhood cancer; and interventions that required an academic degree other than occupational therapy (e.g., music therapy, neuropsychology). AOTA uses standards of evidence modeled on those developed in evidence-based medicine (Lieberman & Scheer, 2002; Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996):
Level I: Systematic reviews, meta-analyses, randomized controlled trials (RCTs)
Level II: Two-group, nonrandomized studies (e.g., cohort, case control)
Level III: One-group, nonrandomized studies (e.g., pretest and posttest)
Level IV: Descriptive studies that include analysis of outcomes (e.g., single-subject design, case series)
Level V: Case reports and expert opinion that include narrative literature reviews and consensus statements.
Studies included in the review provide Level I, II, and III evidence. Level IV and V evidence was excluded from this part of the review.
Data Extraction
The team of three reviewers (Hunter, Gibson, D’Amico) worked together to evaluate all articles at all stages of the review. Eligibility assessment was performed independently in an unblended, standardized manner by the three reviewers. Disagreements among reviewers were resolved by consensus. The synthesis entailed a detailed reading of the studies and completion of an evidence table describing each study specifically. Figure 1 depicts the flow of abstracts and articles through the process, and the evidence table is provided in Supplemental Table 1 (available online at http://ajot.aotapress.net; navigate to this article, and click on “Supplemental Materials”). The articles were grouped into themes and analyzed and reported by theme.
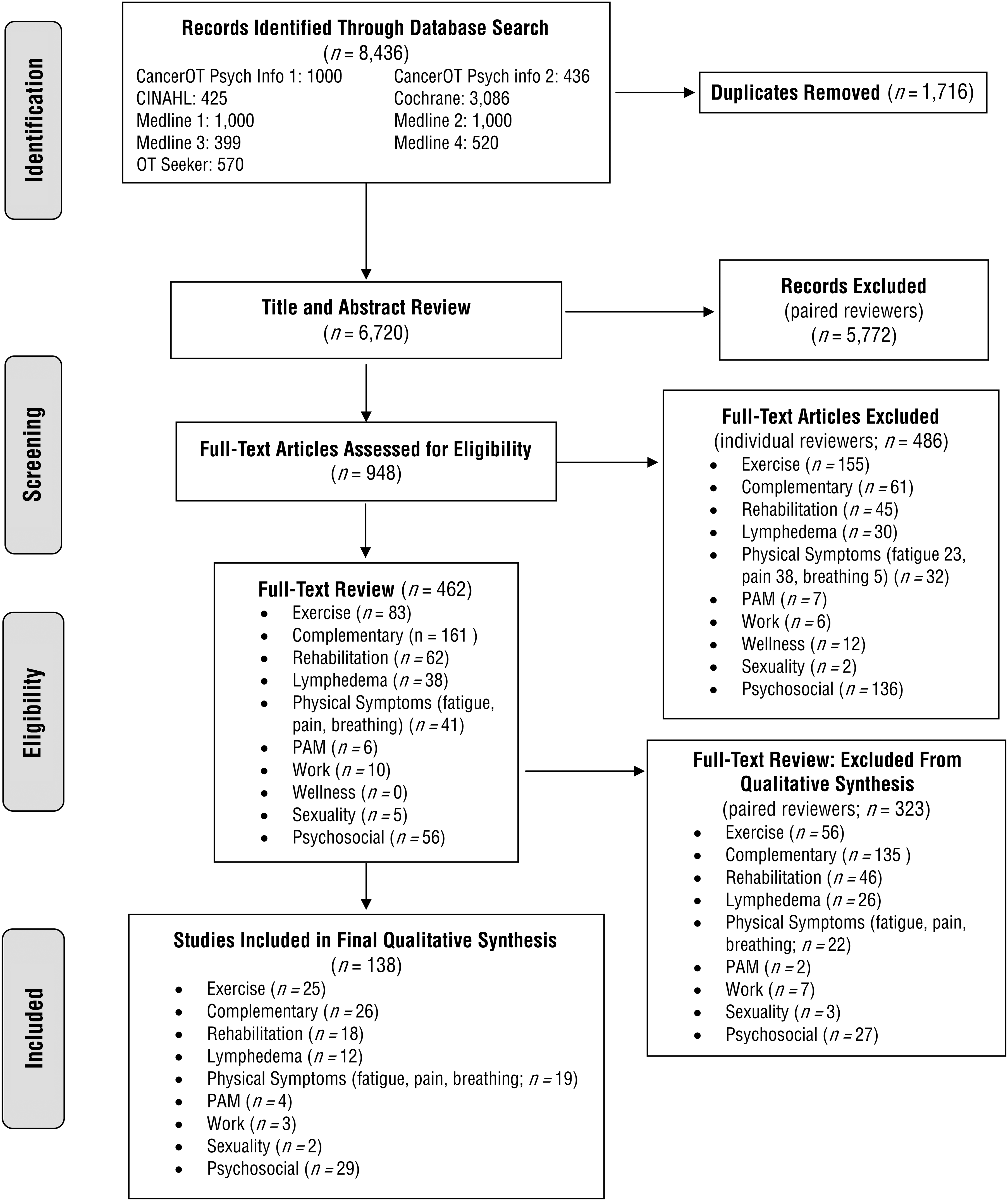
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of physical activity and symptom management studies included in the systematic review.
Analysis
AOTA staff and the EBP Project consultant reviewed the evidence tables to ensure quality control. Analysis of study design, outcomes, and risk of bias determined which studies were assessed as strong or moderate evidence. Strong evidence typically includes 2 or more well-designed RCTs. Moderate evidence includes 1 RCT, 2 or more studies providing lower level evidence, or inconsistent findings from well-designed projects. Only selected articles from the systematic review are mentioned in this article.
Results
The review team identified 138 articles for inclusion in the final qualitative synthesis; 86 articles are included in this article (Part 1). The remainder are discussed in Part 2. The articles provide Level I evidence, with the exception of 1 Level III article. Articles were organized into two broad intervention areas: (1) physical activity interventions, including exercise (25 articles) and complementary and alternative medicine (CAM; 26 articles), and (2) symptom management interventions, including pain, fatigue, and breathlessness (19 articles); lymphedema (12 articles); and physical agent modalities (PAMs; 4 articles). Details about each article are given in Supplemental Table 1 (online).
Risk of Bias
The risk of bias of individual studies was assessed using the Cochrane risk-of-bias guidelines described by Higgins, Altman, and Sterne (2011; see Supplemental Table 2, online). The method for assessing the risk of bias of systematic reviews was based on the Assessment of Multiple Systematic Reviews (AMSTAR) system developed by Shea et al. (2007; see Supplemental Table 3, online).
Physical Activity Interventions
Twenty-five Level I articles related to exercise met the criteria for the review; 11 were systematic reviews and 14 were RCTs. Twenty-six Level I articles related to complementary and alternative medicine met the criteria and were included in the review; 21 were systematic reviews and 5 were RCTs. CAM physical activity interventions included yoga, Qigong, Tai Chi, and dance.
Strong Evidence.
Strong evidence was found that exercise is safe and beneficial for the majority of cancer types, at all stages including end of life, and regardless of age (Adamsen et al., 2009; Albrecht & Taylor, 2012; Baumann, Zopf, & Bloch, 2012; Beaton et al., 2009; Daley et al., 2007; Henke et al., 2014; Hwang et al., 2008; Spence, Heesch, & Brown, 2010). Exercise, particularly aerobic exercise, reduced cancer-related fatigue (CRF; Andersen et al., 2013; Kuchinski, Reading, & Lash, 2009; McMillan & Newhouse, 2011; McNeely et al., 2006). Exercise also increased muscle tone and strength and lung capacity (Granger, McDonald, Berney, Chao, & Denehy, 2011; Keogh & MacLeod, 2012). Exercise was found not to cause lymphedema or to make existing lymphedema worse (Cormie et al., 2013; McClure, McClure, Day, & Brufsky, 2010).
Moderate Evidence.
Moderate evidence was found that exercise improves health-related quality of life (HRQOL) for some survivors. Rehabilitation using physical training (strength, interval, and home-based activities) was significantly better than usual care in terms of HRQOL (Basen-Engquist et al., 2006; Beaton et al., 2009; Korstjens et al., 2008). Supervised exercise was better than nonsupervised exercise (Knols, de Bruin, Shirato, Uebelhart, & Aaronson, 2010), and counseling and telephone support were helpful in keeping people exercising (Knols et al., 2010). Diet and exercise interventions reduced the rate of self-reported functional decline (Morey et al., 2009; Rogers et al., 2009). Exercise improved sleep quality for people undergoing cancer treatment (Sprod et al., 2010; Tang, Liou, & Lin, 2010).
Moderate evidence was found that yoga, regardless of type, benefits mental health, quality of life, sleep, and sense of well-being and decreases stress (Cramer, Lange, Klose, Paul, & Dobos, 2012; Harder, Parlour, & Jenkins, 2012; Mustian et al., 2013; Shneerson, Taskila, Gale, Greenfield, & Chen, 2013). Qigong improved quality of life, mood, fatigue, and immune response and reduced inflammation (Chan et al., 2012; Oh et al., 2012; Zeng, Luo, Xie, Huang, & Cheng, 2014).
Symptom Management Interventions
Nineteen articles addressing pain, fatigue, and breathlessness in cancer patients and survivors met the criteria for the review; 5 were systematic reviews, and 14 were RCTs. Twelve articles related to lymphedema treatment; 6 were systematic reviews, 5 were RCTs, and 1 was a Level III study. Finally, 4 articles related to the use of PAMs to treat lymphedema met the criteria for the review; 1 was a systematic review, and 3 were RCTs.
Strong Evidence.
Strong evidence was found that exercise reduces CRF and increases quality of life (Kuchinski et al., 2009; Wanchai, Armer, & Stewart, 2011). Nonpharmacological interventions, such as problem solving, energy conservation, and education, reduced the symptom of breathlessness (Corner, Plant, A’Hern, & Bailey, 1996; Zhao & Yates, 2008). The use of neuromuscular electrical stimulation in conjunction with traditional swallowing training facilitated greater recovery than swallowing training alone for adults after head and neck cancer treatment (Ryu et al., 2009).
Regarding lymphedema management, compression bandages worn on a daily basis were found to be important for volume control (Devoogdt, Van Kampen, Geraerts, Coremans, & Christiaens, 2010; Kim & Park, 2008; King, Deveaux, White, & Rayson, 2012; Preston, Seers, & Mortimer, 2004). Exercise was found not to make lymphedema worse and to improve mood, quality of life, range of motion, and weight loss (Kim, Sim, Jeong, & Kim, 2010; McClure et al., 2010).
Moderate Evidence.
Moderate evidence was found supporting sleep therapy modifications, education and problem solving for pain management, and cognitive–behavioral therapy in CRF management (Armes, Chalder, Addington-Hall, Richardson, & Hotopf, 2007; Berger et al., 2009; Gielissen, Verhagen, Witjes, & Bleijenberg, 2006; Jacobsen, Donovan, Vadaparampil, & Small, 2007; Ling, Lui, & So, 2012; Oldenmenger, Sillevis Smitt, van Montfort, de Raaf, & van der Rijt, 2011). Moderate evidence also supports the use of PAMs, including low-frequency, low-intensity electrotherapy to reduce feelings of pain, heaviness, and tightness when treating lymphedema of the arm (Belmonte et al., 2012).
Discussion
Part 1 of the systematic review provides evidence that physical activity is helpful for people diagnosed with cancer. The type of physical activity in these studies was varied and included aerobic, light and heavy resistance, walking activities, aquatic exercise, yoga, Qigong, and Tai Chi, among others. Occupational therapy practitioners can help clients incorporate physical activity into their daily routines to enhance health, wellness, and quality of life. Physical activity can help reduce CRF, improve the quality of sleep, increase physical function, and increase HRQOL regardless of type or stage of cancer. It is beneficial for some clients pretreatment and for most clients during and after treatment (Spence et al., 2010).
Strong evidence indicates that exercise, including resistance, aerobic, or a combination of the two, does not exacerbate lymphedema and provides other physical and mental health benefits. Moderate evidence exists for the use of CAM; the strength of this evidence is negatively affected by the quality of the studies and high risk of bias. Moderate evidence supports the use of the CAM interventions of yoga, Qigong, and mindfulness-based interventions to improve quality of life and mental health outcomes.
Symptom management is another area in which occupational therapy intervention is useful. The most common symptoms assessed in the literature were pain, fatigue, and breathlessness. Occupational therapy practitioners should include exercise and other physical activity and occupation-based interventions such as problem solving, energy conservation, and education to address these symptoms. Cognitive–behavioral therapy and psychoeducational programming also can be useful in treating CRF. Additionally, occupational therapy practitioners can feel confident in suggesting physical activity to clients with lymphedema.
Many studies were found that addressed treatment of lymphedema, but the majority did not qualify for this review because they addressed only arm volume and not functional outcomes. The studies included in the review show strong support for the use of compression bandages to improve functional outcomes, particularly when combined with therapy that includes skin care, range of motion, and strengthening.
Overall, the evidence indicates that use of PAMs can be beneficial in treating lymphedema for some people diagnosed with cancer. PAMs can improve the pain that accompanies lymphedema, along with the feelings of heaviness and tightness. Currently, no evidence indicates that transcutaneous electrical nerve stimulation improves chronic pain among cancer survivors.
Three major gaps exist in the research examining cancer rehabilitation interventions. First, more high-quality, rigorous study designs are needed to provide the best, most reliable results. Second, most studies were not specific about the use of or return to meaningful activities and participation for either assessments or outcomes. Third, only a handful of the studies examined occupation-based interventions. As occupational therapy practitioners develop and take part in high-quality studies in the area of cancer rehabilitation, they should ensure that these studies include outcomes that go beyond physical function to address activity and participation.
Implications for Occupational Therapy Practice
Most studies in this review are within the scope of occupational therapy practice but lack a focus on important outcomes of function and participation. This evidence should be viewed as indicating initial steps toward achieving functional outcomes and not achievement of the outcomes themselves. Occupational therapy practitioners must interpret and apply this evidence within their unique professional understanding of function, engagement, and participation.
Occupational therapy practitioners can use a wellness or health promotion approach to encourage meaningful activity and exercise. AOTA (n.d.) has called on practitioners to help people prevent and manage chronic disease through a health and wellness model. Practitioners can feel confident in incorporating physical activity into their practice because strong evidence indicates that exercise helps in multiple ways (e.g., mental health, physical health, symptom management) and does not make symptoms worse (i.e., lymphedema, fatigue). Exercise is clearly beneficial, but it does not have to consist of lifting weights at the gym; yoga and Qigong were found to be beneficial as well. Physical activity is helpful for maintaining weight, increasing muscle strength, improving sleep, and reducing cancer-related fatigue (CRF), among other positive outcomes.
Occupational therapy practitioners are well suited to conduct individual and group yoga, Qigong, and mindfulness interventions to improve symptom management, mental health, quality of life, participation in daily living occupations, and social engagement. These are important factors for cancer survivors and are not always addressed as fully as they could be. Practitioners need to keep in mind that cancer survivorship symptom management is far more than lymphedema care. Although this is the symptom rehabilitation professionals have focused on most fully, CRF, pain, sleep disorders, and breathlessness are more common and less often addressed.
Implications for Research
More rigorous, better designed research is needed to provide a greater understanding of which people need what type of intervention at what point in their cancer care and survivorship. Specifically, more research is needed that focuses on participation outcomes and occupation-based interventions.
The area of exercise is the best researched and has the most robust outcomes in terms of cancer survivorship and cancer rehabilitation, but the occupational therapy focus of participation and occupation is missing in this research. Most of the exercise studies looked at the use of traditional exercise as an intervention; the occupational therapy point of view might provide a richer understanding of how to incorporate the broader idea of physical activity into a client’s life.
In terms of symptom management, most interventions were not conducted by occupational therapy practitioners. The vast majority were conducted by nurses, social workers, or psychologists. Occupational therapy–specific studies are needed that look at return to participation and occupation-based interventions as they relate to managing symptoms in cancer survivors. In general, few of the studies moved into the realm of occupation, particularly in terms of outcomes. Occupational therapy researchers could make strong contributions toward filling this gap in research.
Limitations
Limitations of the systematic review result from limitations in the individual studies’ designs and methods, including small sample sizes, short intervention periods, limited use of standardized assessment, and short follow-up periods. Many studies included multiple interventions, so pinpointing the effects of any single intervention may not be possible. Finally, the role of occupational therapy in the multidisciplinary interventions was seldom discussed. Many studies focused on impairment interventions and the outcomes of symptom management and quality of life rather than the occupational therapy’s concern with function, occupational engagement, performance, and social participation.
Conclusion
Occupational therapy practitioners working with survivors of cancer of all types, stages, and points on the survivorship continuum have a body of evidence to support current and future practice. More research is needed to support occupation-based interventions geared toward positive activity and participation outcomes for this large and continually growing population.
Supplemental Material
Supplementary material for Systematic Review of Occupational Therapy and Adult Cancer Rehabilitation: Part 1. Impact of Physical Activity and Symptom Management Interventions
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2017.023564.pdf for Systematic Review of Occupational Therapy and Adult Cancer Rehabilitation: Part 1. Impact of Physical Activity and Symptom Management Interventions by Elizabeth G. Hunter, Robert W. Gibson, Marian Arbesman and Mariana D’Amico in The American Journal of Occupational Therapy
Footnotes
Note. Each issue of the 2017 volume of the American Journal of Occupational Therapy features a special Centennial Topics section containing several articles related to a specific theme; for this issue, the theme is occupational therapy's role in cancer treatment and recovery. The goal is to help occupational therapy professionals take stock of how far the profession has come and spark interest in the many exciting paths for the future. For more information, see the editorial in the January/February issue, ![]() .
.
*
Indicates studies that were systematically reviewed for this article.
Acknowledgments
We thank Deborah Lieberman, Program Director, AOTA Evidence-Based Practice Project, for her guidance and support during the process of this review. Marian Arbesman is Methodology Consultant, AOTA Evidence-Based Practice Project; no other potential conflicts of interest are reported.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.