
Abstract
Approximately every minute of the day, another adult in the United States is diagnosed with Alzheimer’s disease (AD; Alzheimer’s Association, 2016). Currently, more than 5 million American adults live with the disease, a number that is expected to grow to 16 million by 2050 (Alzheimer’s Association, 2016). One of every 5 Medicare dollars is spent on AD, making it one of the most expensive health conditions in the United States (Alzheimer’s Association, 2016).
Memory loss that impairs the performance of daily activities is a common result of AD (Alzheimer’s Association, 2016), and it leads to difficulties in planning, problem solving, judgment, and completion of familiar activities. Memory loss often leads to decreased participation in work, leisure, and social activity as well as to changes in mood and behavior (Alzheimer’s Association, 2016). No prevention or cure exists for the disease.
Objective
The purpose of this systematic review was to examine the evidence for the effectiveness of interventions designed to establish, modify, and maintain occupations for adults with AD and other major neurocognitive disorders (NCDs). This systematic review was completed in collaboration with the American Occupational Therapy Association (AOTA) as part of the Evidence-Based Practice (EBP) Project. It was one component of an evidence-based literature review focusing on AD and related major NCDs that examined the evidence published from January 2006 to February 2014. This review was an update of Padilla’s (2011) review to reflect current knowledge on the topic. The previous review included 10 articles that provided strong evidence for occupations of self-care and leisure.
Method
The list of search terms for the review was developed with AOTA staff and an advisory group of expert practitioners and researchers. A medical librarian with experience in searches for systematic reviews confirmed the search terms and completed the searches. Table 1 lists the search terms used.
Search Terms for the Systematic Review of Interventions to Enhance Occupational Performance for Adults With Alzheimer’s Disease and Related Major Neurocognitive Disorders
We reviewed article citations and abstracts from MEDLINE, PsycINFO, OTseeker, and CINAHL, as well as sources of evidence-based medicine reviews including the Cochrane Database of Systematic Reviews, the Cochrane Controlled Trials Register, and the Database of Abstracts of Reviews of Effectiveness. We also reviewed abstracts referred from other focused questions and those found by hand searching journals and the reference lists of included articles. Both authors reviewed titles and abstracts individually to determine whether to obtain the article for further evaluation. We discussed discrepancies until we reached agreement. We used the same process to review the full text of potential articles. We then recorded a summary of each article in an evidence table, rated each article according to risk of bias, and synthesized the content of the included studies into themes and subthemes. The AOTA EBP Project consultant reviewed the evidence table to ensure quality control. Supplemental Tables 1, 2, and 3 (available online at http://otjournal.net; navigate to this article, and click on “Supplemental”) contain the evidence table and risk-of-bias tables for articles included in this review.
Several inclusion and exclusion criteria established structure for the review. The review included peer-reviewed scientific literature published in English between January 2006 and February 2014 on interventions within the scope of occupational therapy practice for participants with AD and other major NCDs including vascular dementia, Lewy body dementia, Parkinson’s disease dementia, frontotemporal dementia, Creutzfeldt–Jakob disease, cognitive impairment, and dementia. The interventions had to have the aim of establishing, modifying, or maintaining activities of daily living (ADLs), instrumental activities of daily living (IADLs), sleep, leisure, or social participation. With the exception of exercise interventions, which measured physical function, study outcomes had to include measurement of occupation. We included exercise interventions if the study authors considered exercise to be a leisure or health maintenance activity. The interventions were completed in the home, community, or institution.
We excluded data from non–peer-reviewed research literature, dissertations, theses, presentations, and conference proceedings. Descriptive studies and case reports were not included in this review because higher level evidence was available in each of the themes.
Results
We reviewed titles and abstracts of 2,597 articles. After this preliminary review, 256 articles were retrieved for further evaluation using the inclusion and exclusion criteria, of which 52 studies were included in the review. Figure 1 is a flow diagram of article selection. Of the 52 articles, 14 were Level I systematic reviews; 12 were Level I randomized controlled trials (RCTs); 16 were Level II nonrandomized, two-group, pretest–posttest design; and 10 were Level III one-group, pretest–posttest design. We categorized all articles into five intervention themes: occupation-based, sleep performance, cognitive, physical exercise, and multicomponent interventions.
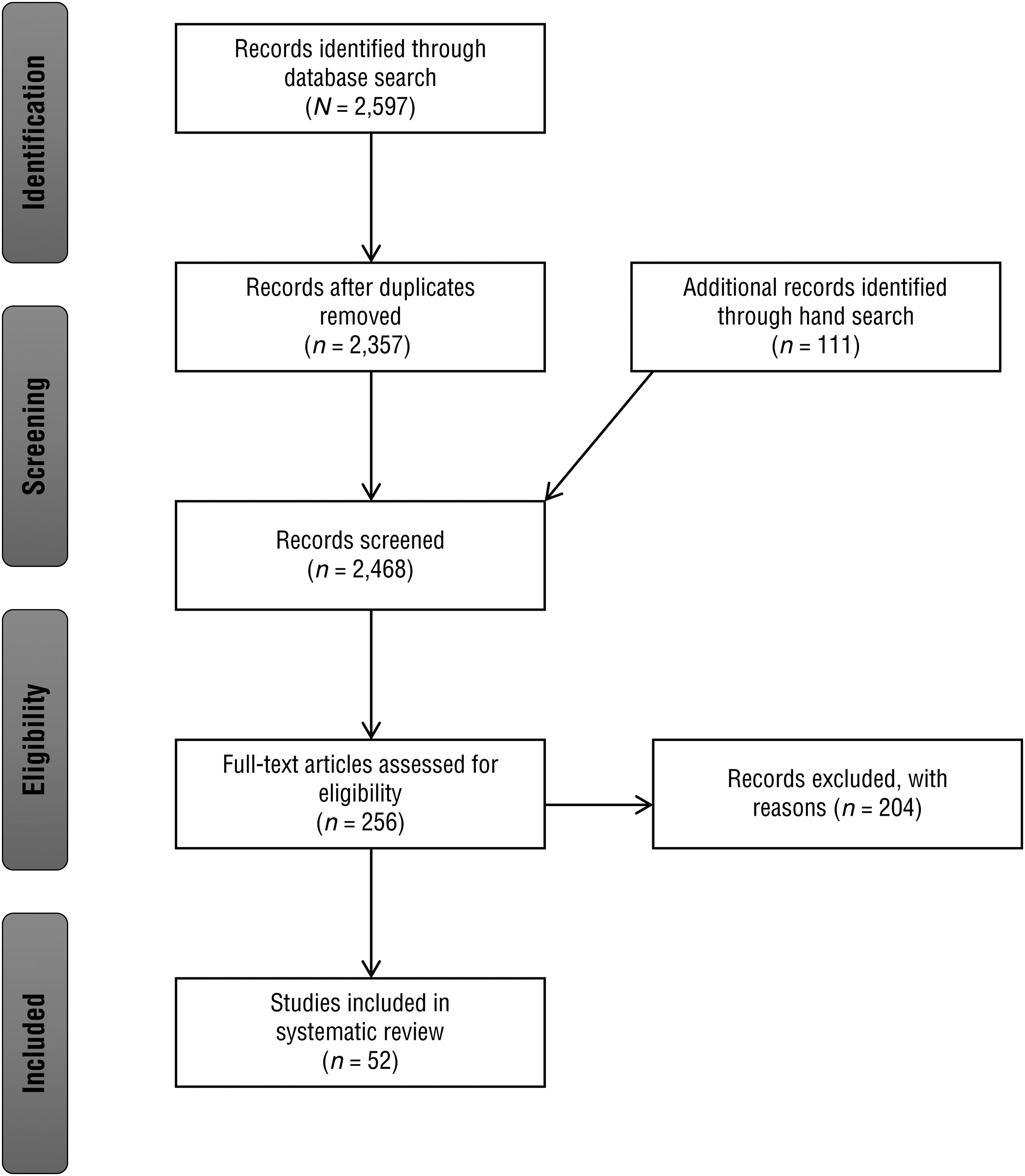
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram of published literature search.
We determined strength of evidence in each theme on the basis of the number of studies and the level of evidence using the U.S. Preventive Services Task Force (2014) recommendations as a guide. Consistent results from 2 or more Level I studies were rated as strong evidence, and consistent results from 1 Level I study plus 2 or more Level II or III studies were rated as moderate evidence. Results from a limited number of studies or studies of low quality were rated as limited evidence. Inconsistent results across studies were rated as mixed evidence, whereas both limited number and quality of studies in a theme were rated as insufficient evidence.
Risk of Bias
The risk-of-bias criteria recommended by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA; Liberati et al., 2009) were used to rate study quality. Twelve studies reported using random assignment; however, the majority of studies included in the review lacked blinding to group allocation, personnel, or outcome. Most of the studies reported an adequate number of participants; however, several experienced attrition for a variety of reasons, including a decline in health or death. The Assessment of Multiple Systematic Reviews (AMSTAR; Shea et al., 2007) criteria were used to rate the quality of the 14 systematic reviews. Ten of the systematic reviews included only RCTs. Good rigor was reported for the reviews; the majority of studies received positive markings in the 11 items on the AMSTAR tool. Supplemental Tables 2 and 3 (online) outline the risk-of-bias evaluation of all articles included in this review.
Effectiveness of Occupation-Based Interventions
Thirteen articles addressed occupation-based intervention (i.e., interventions involving activities of everyday life). Subthemes included occupation as the focus of intervention and outcome, occupation-based intervention strategies with outcomes other than occupation, and self-feeding strategies.
Occupation-Focused Interventions and Outcomes.
Research containing occupation-focused interventions and outcome measures included 3 Level I systematic reviews (McLaren, Lamantia, & Callahan, 2013; Olazarán et al., 2010; Padilla, 2011), 2 Level II studies (Baldelli, Boiardi, Ferrari, Bianchi, & Bianchi, 2007; Farina, Mantovani, Fioravanti, Rotella, et al., 2006), and 3 Level III studies (Braddock & Phipps, 2010; Sidani, Streiner, & Leclerc, 2012; Yamaguchi, Maki, & Takahashi, 2011). The 3 Level I systematic reviews reported that occupation-based interventions decreased decline in or improved ADL performance and improved performance in leisure activity. The 2 Level II studies found mixed results for improving ADL and IADL performance. The 3 Level III studies failed to demonstrate the effectiveness of occupation-based interventions to improve morning care, activity engagement, and use of video games.
The Level II and III evidence that does not support occupation-based interventions for the performance of daily activities is outweighed by the Level I studies supporting it. The quality and quantity of Level I research provide strong evidence to support occupation-based intervention for the performance of daily activities for adults with AD and related NCDs.
Occupation-Based Interventions Without an Occupation-Based Outcome Measure.
A smaller body of research has examined the use of occupation-based intervention to enhance other outcomes, including loneliness, behavior, and general well-being. Although occupation-based activity reduced agitation (van der Ploeg et al., 2013) and prevented further loneliness (Passmore, Lindenmeier, Tapps, & Gibson, 2007), the occupation of therapeutic gardening had no significant effect on well-being (Hewitt, Watts, Hussey, Power, & Williams, 2013). Because the variety of research in this subtheme is wide with limited research for each type of outcome, the evidence is limited to support occupation-based interventions for other outcomes.
Interventions for Self-Feeding.
Lin et al. (2010) and Lin, Huang, Watson, Wu, and Lee (2011) have studied the use of a Montessori-based intervention for self-feeding. Compared with control conditions completing routine activities, Montessori-based intervention produced significant improvements in self-feeding. These findings provide moderate evidence supporting Montessori methods to enhance self-feeding.
Effectiveness of Interventions to Enhance Sleep
Three studies included outcome measures related to sleep: 2 Level I systematic reviews (Brown et al., 2013; Eggermont & Scherder, 2006) and 1 Level II study (McCurry, LaFazia, Pike, Logsdon, & Teri, 2012). The great variety in interventions evaluated across the three studies limits synthesis of the results. However, strong evidence was found for the use of exercise, and moderate evidence was found for the use of individualized social activity to enhance sleep. McCurry et al. (2012) found positive results on sleep with a sleep education program for caregivers, providing limited evidence to support its use in practice. Insufficient evidence was found for the use of a variety of other interventions (e.g., music, outdoor activities, gardening, physical agent modalities) to enhance sleep; therefore, these interventions should be used cautiously until further research has been conducted.
Effectiveness of Cognitive Interventions
Twelve studies reported on cognitive interventions to support occupational performance in adults with AD and related NCDs. Of the 12 studies, 6 included cognitive rehabilitation, cognitive training, cognitive stimulation, or a combination of these interventions (Bahar-Fuchs, Clare, & Woods, 2013; Cooper et al., 2012; Farina, Mantovani, Fioravanti, Pignatti, et al., 2006; Kurz et al., 2012; Sitzer, Twamley, & Jeste, 2006; Woods, Aguirre, Spector, & Orrell, 2012). Four articles focused on errorless learning or other types of prompting for this population (Brenske, Rudrud, Schulze, & Rapp, 2008; Dechamps et al., 2011; Lee, Yip, Yu, & Man, 2013; van Tilborg, Kessels, & Hulstijn, 2011), whereas 2 studies (Nawate, Kaneko, Hanaoka, & Okamura, 2007; Wang, Yen, & OuYang, 2009) addressed reminiscence interventions.
Cognitive rehabilitation, or individualized therapeutic interventions for performing cognitive activities, was specifically addressed in 2 Level I systematic reviews (Bahar-Fuchs et al., 2013; Cooper et al., 2012), 1 Level I RCT (Kurz et al., 2012), and 1 Level II study (Farina, Mantovani, Fioravanti, Pignatti, et al., 2006). Combined, they provide mixed evidence for the use of cognitive rehabilitation strategies to improve ADL and quality-of-life outcomes.
Cognitive stimulation, defined as a wide variety of activities to engage the mind, such as puzzles, games, current events, and leisure activities, is another cognitive intervention strategy for adults with AD and related NCDs. Two Level I studies concluded that cognitive stimulation is effective for improving social interaction and quality of life; however, findings indicated uncertainty about the benefit of cognitive stimulation to improve the performance of daily tasks (Cooper et al., 2012; Woods et al., 2012).
Cognitive training, or the specific practice of cognitive tasks, was also included in the scope of this review. Bahar-Fuchs et al. (2013) and Sitzer et al. (2006) evaluated the effectiveness of cognitive training for the performance of daily activities. Bahar-Fuchs et al. found that cognitive training had no significant benefit on ADL performance, whereas Sitzer et al. found a large effect for both compensatory and restorative cognitive training for the improvement of ADL performance. Although a significant amount of evidence is available, the findings are mixed and inconsistent.
Four research groups (Brenske et al., 2008; Dechamps et al., 2011; Lee et al., 2013; van Tilborg et al., 2011) examined a variety of prompting interventions for the improvement of daily occupations. A growing body of literature has examined the use of errorless learning (Lee et al., 2013), error reduction learning (Dechamps et al., 2011), implicit and explicit learning (van Tilborg et al., 2011), and descriptive prompts (Brenske et al., 2008). All studies found that the provision of repetitive verbal instruction for correct task performance or the modeling of appropriate task performance enhanced the performance of ADLs and IADLs. Strong evidence thus supports the use of error reduction strategies to improve the performance of daily tasks.
Reminiscence intervention, or activities used to remember past events, was examined in 3 studies (Cooper et al., 2012; Nawate et al., 2007; Wang et al., 2009). Cooper et al. (2012) found no support for group reminiscence to improve quality of life in institutional settings, and Wang et al. (2009) found no difference between reminiscence therapy and themed intervention in effect on ADL performance. Nawate et al. (2007) found significant differences between intervention and control groups on cognitive function, affective function, and behavior. Because of the variety of interventions and outcome measures used across these studies, the evidence is insufficient to support reminiscence therapy.
Effectiveness of Physical Exercise Interventions
A significant amount of literature is devoted to the study of physical exercise interventions for adults with AD and related NCDs. Eleven Level I studies (Blankevoort et al., 2010; Eggermont & Scherder, 2006; Forbes, Thiessen, Blake, Forbes, & Forbes, 2013; Littbrand, Carlsson, et al., 2011; Littbrand, Lundin-Olsson, Gustafson, & Rosendahl, 2009; Littbrand, Stenvall, & Rosendahl, 2011; McLaren et al., 2013; Pitkälä et al., 2013; Potter, Ellard, Rees, & Thorogood, 2011; Rao, Chou, Bursley, Smulofsky, & Jezequel, 2014; Suttanon et al., 2013), 5 Level II studies (Canonici et al., 2012; Fan & Chen, 2011; Garuffi et al., 2013; Nascimento, Teixeira, Gobbi, Gobbi, & Stella, 2012; Thurm et al., 2011), and 2 Level III studies (Chang, Chen, Shen, & Chiou, 2011; Litchke, Hodges, & Reardon, 2012) were included in this theme.
The majority of evidence is of high quality and strongly supports the use of exercise to improve or maintain ADL performance and functional mobility in both community and institutional settings. Exercise interventions typically included endurance or aerobic exercise, balance training, and resistance training multiple times per week over the course of several weeks, although the frequency, duration, and intensity of the programs studied varied widely.
Effectiveness of Multicomponent Interventions
Ten studies reported on the effect of multicomponent interventions on the performance of occupations for adults with AD and related NCDs. Included in this theme are studies that addressed either comprehensive rehabilitation programs that included interventions within the scope of occupational therapy or use of multiple intervention strategies at the same time. Two studies were systematic reviews and thus contributed Level I evidence (Cooper et al., 2012; Olazarán et al., 2010), 3 were RCTs providing Level I evidence (Graessel et al., 2011; Luttenberger, Donath, Uter, & Graessel, 2012; Maci et al., 2012), 4 studies provided Level II evidence (Brooker, Woolley, & Lee, 2007; de Andrade et al., 2013; Schiffczyk et al., 2013; Viola et al., 2011), and 1 study provided Level III evidence (Raggi et al., 2007).
Multicomponent Interventions.
Seven studies included two or more interventions during the study period (Brooker et al., 2007; Cooper et al., 2012; de Andrade et al., 2013; Graessel et al., 2011; Luttenberger et al., 2012; Maci et al., 2012; Olazarán et al., 2010). The majority of these studies (Brooker et al., 2007; Graessel et al., 2011; Luttenberger et al., 2012; Maci et al., 2012; Olazarán et al., 2010) included physical activity, cognitive interventions, and socialization and/or ADL interventions. The majority of studies included an ADL outcome measure; however, the findings were mixed. Moderate evidence supports multicomponent interventions to address quality of life, and low-quality research provides limited evidence for increased activity variety to address physical function for adults with AD and related NCDs.
Comprehensive Rehabilitation Programs.
Three studies (Raggi et al., 2007; Schiffczyk et al., 2013; Viola et al., 2011) examined the effect of comprehensive rehabilitation programs on IADLs, ADLs, and quality of life. Combined, this research provides limited evidence for the effectiveness of a comprehensive rehabilitation program for this population because of the low quality of studies and the heterogeneity of the findings.
Discussion
Occupational therapy serves a valuable role in establishing, modifying, and maintaining occupations for adults with AD and other major NCDs. Results of the studies included in this review provide strong evidence for occupation-based interventions to maintain ADL performance and for routine exercise to improve sleep, daily activity, and physical function in this population. Although not all exercise programs are considered skilled occupational therapy service, occupational therapy practitioners can play a critical role in establishing physical exercise as part of daily routines for clients with major NCD. Strong evidence also supports the use of cognitive interventions, specifically errorless learning strategies, for maintaining performance of ADLs. Combined, these occupational therapy interventions can positively influence participation and engagement in occupations for adults with AD and other major NCDs.
Implications for Occupational Therapy Practice
The following recommendations include those that should be offered routinely and those that should be offered more selectively on the basis of individual client characteristics. Interventions recommended as a routine part of services are as follows:
Occupation-based interventions for ADLs
Physical exercise for improved sleep, ADLs, and physical function
Individualized social activity for improved sleep performance
Errorless learning or prompting for the performance of ADLs and IADLs
Cognitive stimulation activities for improved quality of life and socialization
Multicomponent interventions for improved quality of life
Montessori methods for self-feeding.
The following services should be offered selectively on the basis of individual client characteristics:
Cognitive rehabilitation and training for ADLs
Multicomponent and multidisciplinary interventions for ADLs.
Limitations
Systematic reviews are limited by the quality and type of evidence available; this review included a mix of study designs and rigor, with the majority of studies of medium to high quality. The studies included in this review used a variety of intervention strategies and outcome measures, and this heterogeneity across studies limited the synthesis of results. Finally, a significant number of studies were conducted outside the United States, which may limit generalization to the U.S. population and health care system.
Conclusion
The number of adults with decreased occupational performance secondary to a diagnosis of AD or other major NCD will continue to rise dramatically as the population ages. Occupational therapy practitioners are well suited to provide rehabilitation interventions to maximize performance of daily occupations and prevent premature decline in this population. The literature included in this review provides strong evidence supporting the use of occupation-based interventions, routine physical exercise, and errorless learning strategies when providing services to those with major NCDs. Occupational therapy practitioners and students should be trained to offer these interventions to their clients. Although a significant body of literature is available in this area of practice, future research using clearly defined interventions targeting occupational outcomes and appropriate dosages would provide further information to maximize the effectiveness and efficiency of occupational therapy services to this population.
Supplemental Material
Supplementary material for Effectiveness of Occupational Therapy Interventions to Enhance Occupational Performance for Adults With Alzheimer's Disease and Related Major Neurocognitive Disorders: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2017.024752.pdf for Effectiveness of Occupational Therapy Interventions to Enhance Occupational Performance for Adults With Alzheimer's Disease and Related Major Neurocognitive Disorders: A Systematic Review by Stacy Smallfield and Cindy Heckenlaible in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We thank Deborah Lieberman and Marian Arbesman for their guidance and support on this project. This work was presented at the 2015 AOTA Conference & Expo in Nashville, Tennessee.
*
Indicates studies included in the systematic review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.