
Abstract
This study explored differences in perspectives on quality of life (QOL) between people affected by amyotrophic lateral sclerosis (ALS) and their caregivers. QOL is often thought of as related to physical limitations, without consideration of other factors (e.g., cognitive, emotional) that may be stronger predictors of QOL in people with long-term degenerative diseases. Because QOL is complex and influenced by multiple factors, people with ALS and their caregivers may have different perspectives on what constitutes QOL. This study investigated potential discrepancies in QOL perspectives between people with ALS and their caregivers. Thirty dyads from the Augusta University Health ALS Clinic completed a measure of QOL, and we compared the results and identified patterns. The most prominent finding was that members of the dyads misunderstood the mental experiences of one another.
Amyotrophic lateral sclerosis (ALS) is a progressive neurodegenerative disease that results in muscle atrophy, loss of voluntary muscle control, changes in reflexes, speech and swallowing difficulties, and cognitive challenges. These symptoms undermine the ability to perform tasks independently in the areas of basic self-care, functional mobility, and communication (Reed, 2014). Every day, on average, 15 people are diagnosed with ALS. As many as 30,000 people in the United States are currently affected by ALS, and each year ALS is responsible for 2 deaths per 100,000 population (ALS Association, 2016).
Research on Quality of Life in People With ALS
Improving quality of life (QOL) as it relates to physical and mental capabilities for patients with ALS is a critical area of study. QOL in patients with long-term degenerative neurological diseases has been a research topic of interest over the past 2 decades. The concept of QOL is multifaceted, making it difficult to find commonalities in research results (Bromberg, Anderson, Davidson, & Miller, 2001; Calvert et al., 2013; Reed, 2014). However, researchers agree that QOL is severely compromised by challenges associated with having a neurological disease or caring for someone with such a diagnosis (Bromberg et al., 2001; Calvert et al., 2013; Reed, 2014).
Calvert et al. (2013) looked at access to supportive care for people with rare long-term neurological conditions (rLTNCs), such as motor neuron disease, Huntington’s disease, cerebellar ataxia, progressive supranuclear palsy, multiple system atrophy, Charcot–Marie–Tooth disease, and postpolio syndrome, to determine how these conditions affect health-related quality of life (HRQL). The researchers asked 266 patients with rLTNCs to complete a survey designed by the research team about supportive care and HRQL over a period of 6 mo. HRQL was also assessed using the EQ–5D, a self-administered, standardized instrument developed for use as a health outcome measure. HRQL was substantially lower for people with rLTNCs than for the general population. The results highlighted potential issues with access to supportive care; patients reported having less access to health care and social services than they needed.
Nordeson, Engström, and Norberg (1998) examined the impact of therapy intervention on QOL in patients with progressive neurological disease. The researchers collected data over 12 weeks from 52 participants at a rehabilitation center using the Quality of Life: Status and Change tool, a generic (i.e., not disease-specific) self-report instrument. In general, participants rated their QOL as positive, and those who had been receiving therapeutic intervention longer (i.e., who had made more than one visit to the rehabilitation center) rated their bodily health, well-being, and general life more positively. The reasons for the positive ratings by all participants, and especially those receiving therapy longer, are uncertain and somewhat counterintuitive, indicating that QOL is a multifaceted concept and varies across individuals (Bromberg et al., 2001; Calvert et al., 2013; Reed, 2014).
In research investigating outcomes of treatments for people with neurological disorders, the focus is often on motor disabilities, and the cognitive and emotional domains are left out of the treatment strategy. Behari, Srivastava, and Pandey (2005) addressed this deficit in a study of 278 participants with Parkinson’s disease using Hoehn and Yahr staging, the Schwab and England Activities of Daily Living Scale, and the Unified Parkinson’s Disease Rating Scale; depression was assessed using criteria from the Diagnostic and Statistical Manual of Mental Disorders (3rd ed., rev.; American Psychiatric Association, 1987), and QOL was assessed using the Parkinson’s Disease Quality of Life Questionnaire. Female gender, decreased independence, increased medication use, and a depression diagnosis had a significant impact on QOL, with depression having the greatest impact. The researchers concluded that improving motor impairments should not be the only focus when seeking to enhance QOL in patients with Parkinson’s disease; QOL can be improved if depression is recognized and treated appropriately.
In another study of factors beyond physical function, Simmons, Bremer, Robbins, Walsh, and Fischer (2000) assessed QOL in patients with ALS using the McGill Quality of Life Questionnaire and the Sickness Impact Profile ALS–19 (SIP/ALS–19); strength and function were assessed using manual muscle testing and the ALS Functional Rating Scale, and spirituality and religiousness were assessed using the Idlar Index of Religiosity. Results revealed a high correlation between psychological and external support and QOL, indicating that patients’ perspectives on their own QOL extended beyond motor function and emphasizing the importance of looking into factors beyond physical capabilities to assess QOL in patients. The degree and quality of external support appear to be influencing factors (Connolly, Galvin, & Hardiman, 2015; Creemers et al., 2014; Williams, Donnelly, Holmlund, & Battaglia, 2008).
As ALS progresses, people rely increasingly on external support, often from a primary caregiver. Because ALS is such a debilitating disease, the caregiver assumes increasing caregiving responsibility throughout the disease process. Along with the physical demands of providing caregiving to a loved one, caregivers also are responsible for making crucial decisions about medical interventions for the person with ALS. The strenuous emotional and physical support caregivers provide daily can lead to depression (Rabkin, Albert, Rowland, & Mitsumoto, 2009). Studies have shown that caregivers of people with ALS are depressed at twice the rate of typical adults their age (Vitaliano, Zhang, & Scanlan, 2003). Caregivers are at just as much at risk as the care recipient, if not more, of decreased QOL.
To evaluate QOL in both people with ALS and their caregivers and to examine the dynamic interaction of perspectives on QOL between the dyad, better methods of assessment are needed. Currently, no assessment specifically addresses similarities and differences in perspectives on QOL between people with ALS and their caregivers. Assessments such as the SIP/ALS–19 and the ALS Assessment Questionnaire focus on the patient’s perspective (Bromberg et al., 2001). An assessment geared toward analyzing the dyadic relationship between people with ALS and their caregivers would assist clinicians in providing optimal care to improve QOL in and facilitate enhanced understanding within the dyad.
The high level of burden among caregivers of people with ALS greatly influences their perspective on the care recipient’s QOL, and perspectives on QOL among people with ALS are highly variable, potentially leading to miscommunication within the patient–caregiver dyad. Physical ability is not as influential as psychosocial, emotional, and spiritual factors in overall QOL perspectives (Simmons et al., 2000). Spirituality has been found to promote QOL in ALS caregivers, often being a top positive predictor for caregiver QOL. Patients’ and caregivers’ spirituality is significantly correlated; therefore, spirituality among both patients and caregivers is related to overall QOL perspectives within the dyad (Calvo et al., 2011). Determining the patterns in QOL differences and similarities between people with ALS and their caregivers can help clinicians facilitate enhanced communication within the dyad, potentially leading to more effective therapy solutions (Simmons, 2015). Hence, proactively discussing topics such as religion and spirituality with people with ALS and their caregivers may be vital to optimizing care and the therapeutic role of clinicians.
The original idea for this research project grew from observed differences in perspectives on QOL between people with ALS and caregivers witnessed in the clinic. In searching previous studies, the research team found that although several studies addressed patients’ and caregivers’ QOL (Bromberg et al., 2001; Calvert et al., 2013; Nordeson et al., 1998; Rabkin et al., 2009; Reed, 2014; Vitaliano et al., 2003), little research compared perspectives on QOL within the dyad. Therefore, this research project aimed to begin a discussion in this area. The goals of this study were to understand similarities and differences between perspectives on QOL, specifically in the physical and mental domains, of people with ALS and their caregivers and to add to the current dialogue on the complexities of QOL in patients with ALS and their caregivers by exploring the aspects of life these dyads perceive as most influential.
Method
Participants
We recruited patients who were receiving treatment at Augusta University Health ALS Clinic. The lead physician and other health care workers were notified about the study and were asked to allow time during patients’ monthly clinic visits for the researchers to recruit participants. Patients with a confirmed diagnosis of frontotemporal lobe dementia, those without a caregiver present at the time of data collection, and non–English-speaking dyads were excluded. The study was approved by the institutional review board (IRB).
Thirty patient–caregiver dyads completed the study (26 White dyads and 4 African-American dyads) and were included in the analysis. Forty-five percent of participants were male (n = 27) and 55% were female (n = 33); ages ranged from 30 to 84, with a mean of 58. The dyads participated during their regularly scheduled clinic appointments. Two additional dyads that initiated the survey did not complete it; in 1 dyad, the patient felt that the caregiver present at the appointment could not accurately answer questions as primary caregiver, and 1 dyad had difficulty understanding the concept thoroughly. A third additional dyad completed the survey but was not included in the analysis because we later learned that the patient had a confirmed diagnosis of dementia.
Instrument
A pencil-and-paper survey, the Short Form–12 Health Survey Questionnaire Version 2 (SF–12; Ware, Kosinski, Turner-Bowker, & Gandek, 2002), was administered to patients and caregivers who agreed to participate. This shortened form of the SF–36 is a generic assessment of HRQOL from the respondent’s perspective. The SF–12 consists of 12 questions and takes approximately 2–3 min to administer (Ware et al., 2002). For our study, participants were given the option to self-administer the survey or to complete it through an interview with a researcher who read the questions to the participant and circled the indicated answer. The widespread use of the SF–12 influenced our decision to select this outcome measure.
A screening tool used to measure both physical and mental health aspects of QOL, the SF–12 measures functional health and well-being from the respondent’s perspective in eight domains, including the physical domains of (1) general health, (2) physical functioning, (3) role–physical, and (4) bodily pain and the mental domains of (5) vitality, (6) social functioning, (7) role–emotional, and (8) mental health. Two composite scores are obtained from this assessment representing physical health and mental health.
A sample physical domain item asks how much a respondent’s health limits his or her ability to perform moderately strenuous activities, such as moving a table, pushing a vacuum cleaner, bowling, or playing golf. A sample mental domain item asks how much during the past 4 weeks a respondent has accomplished less than he or she would have liked as a result of emotional problems (e.g., feeling depressed or anxious). Respondents use a Likert scale from 1 (e.g., all of the time) to 5 (e.g., none of the time); specific descriptions for the numbers in response scales differ across items.
Research has shown the original version of the SF–12 to be reliable and valid. Younsi and Chakroun (2014) found support for the construct validity, internal consistency, and convergent validity of the SF–12 in a stratified representative sample (n = 3,582) of people age ≥18 yr. Additionally, the SF–12 has been shown to have no measurement bias based on age, gender, and education level (Bourion-Bédès et al., 2015).
Procedure
A member of the research team entered the patient’s room between visits with the various health care workers at the clinic. The team member introduced the study and clearly described the background and objectives. The patient and caregiver were then given the option to participate or not. If both the patient and caregiver agreed, they reviewed and signed the IRB consent form. A team member administered the SF–12 to patients twice during their time at the clinic, once to assess their perspective on their own QOL (physical and mental domains) and a second time to assess their perception of their caregiver’s QOL (physical and mental domains). Caregivers were also administered the SF–12 twice, once to assess their perspective on their own QOL and a second time to assess their perception of the patient’s QOL.
Data Analysis
Data were entered into the QualityMetric Health Outcomes Scoring Software Version 4.5.1 (QualityMetric Inc., Lincoln, RI), which generated physical and mental health composite scores. For analysis, data were exported into IBM SPSS Statistics Version 23 (IBM Corp., Armonk, NY). A multivariate analysis of variance (MANOVA) was conducted followed by post hoc analyses of variance (ANOVAs) paired with post hoc Tukey tests. The MANOVA compared physical and mental health composite scores for patients’ assessment of themselves, patients’ assessment of their caregiver, caregivers’ assessment of themselves, and caregivers’ assessment of the patient. Post hoc ANOVAs were used to investigate separate comparisons for the independent variables of physical health composite scores and mental health composite scores. Finally, post hoc Tukey tests were used to determine which of the ratings differed significantly among physical and mental health composite scores. Four comparisons were made: (1) patient self-assessment versus caregiver self-assessment, (2) patient self-assessment versus caregiver assessment of the patient, (3) patient assessment of the caregiver versus caregiver self-assessment, and (4) patient assessment of the caregiver versus caregiver assessment of the patient.
Results
The mean physical composite scores for the comparison groups are displayed in Figure 1 and Table 1. The mean mental composite scores for the comparison groups are displayed in Figure 2 and Table 2.
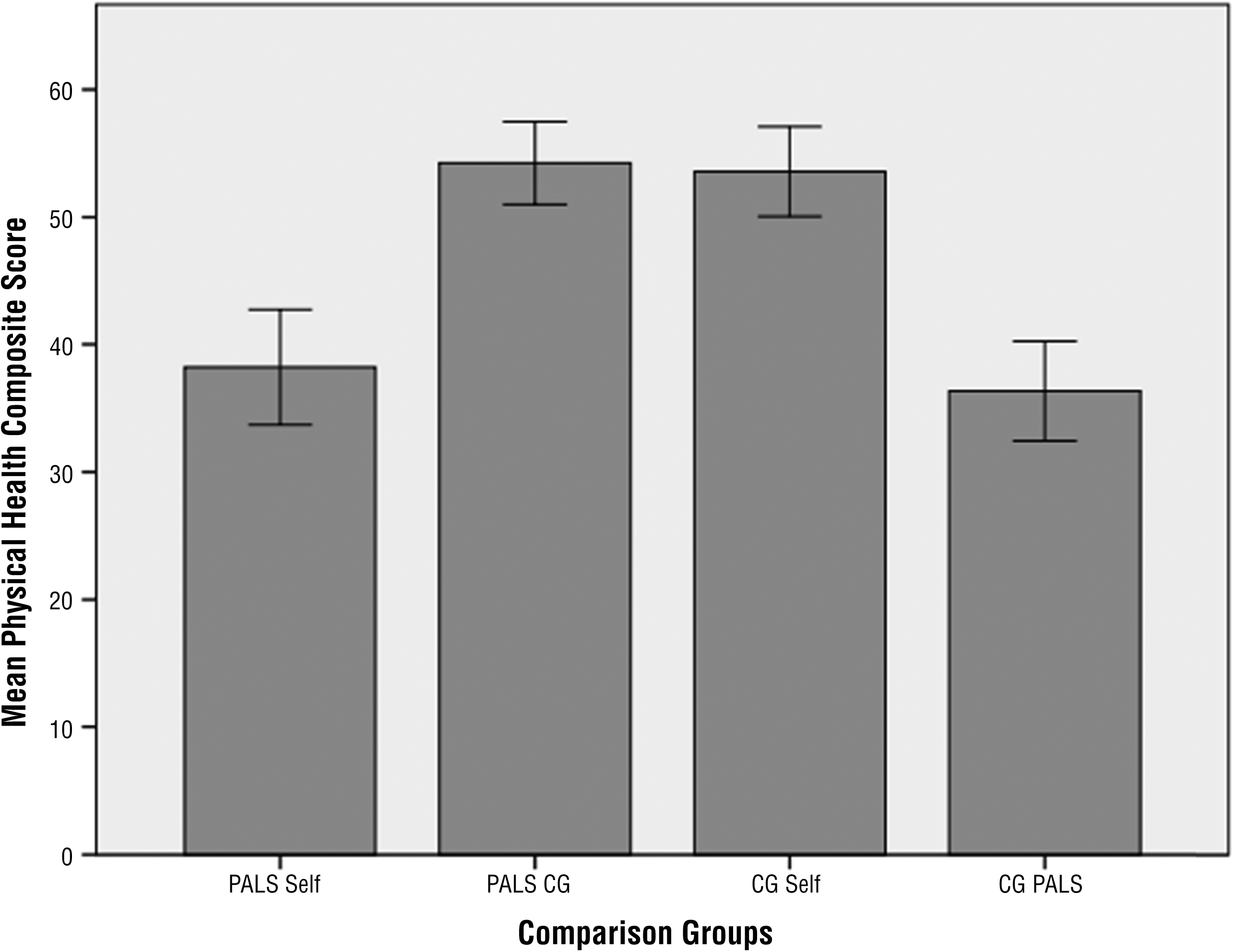
Mean physical health composite scores across comparison groups.
Mean Physical and Mental Health Composite Scores Across Comparison Groups
Note. ALS = amyotrophic lateral sclerosis; CG PALS = caregiver assessment of patient with ALS; CG Self = caregiver self-assessment; M = mean; PALS CG = patient with ALS assessment of caregiver; PALS Self = patient with ALS self-assessment; SE = standard error.
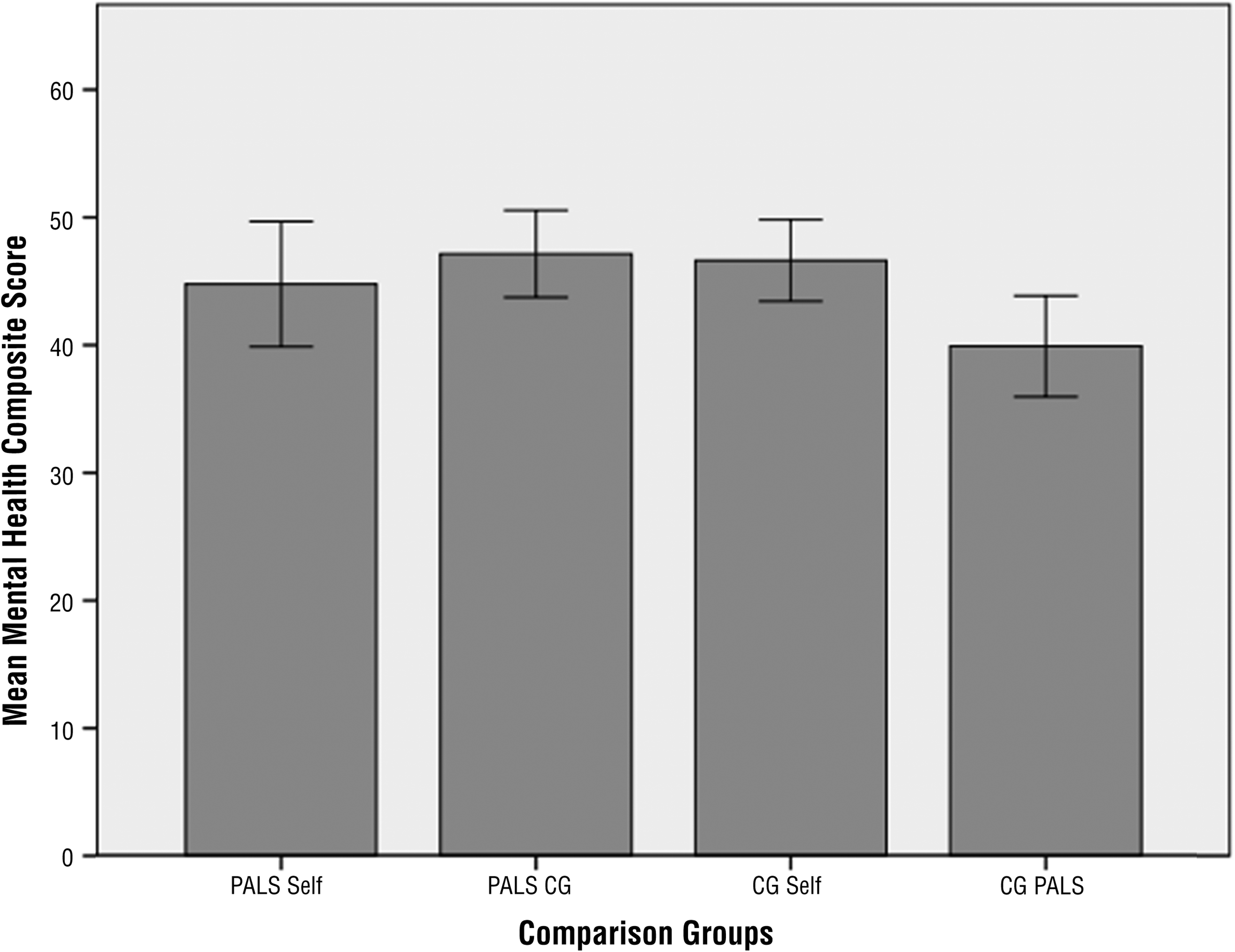
Mean mental health composite scores across comparison groups.
Post Hoc Tukey Tests Across Comparison Groups
Note. ALS = amyotrophic lateral sclerosis; CG PALS = caregiver assessment of patient with ALS; CG Self = caregiver self-assessment; M = mean; PALS CG = patient with ALS assessment of caregiver; PALS Self = patient with ALS self-assessment; SE = standard error.
Significant (p = .05) and marginally significant differences.
Results of the MANOVA indicated a significant effect of group ratings for the physical composite score and mental composite score, F(6, 232) = 11.64, p < .05. Two separate post hoc ANOVAs were conducted, one on the physical composite scores and one on the mental composite scores; further Tukey comparisons determined whether any specific differences existed between the group ratings.
The ANOVA for physical composite scores was significant, F(3, 116) = 25.434, p < .05. The results of the Tukey post hoc test revealed that all of the comparisons were significant (p < .05) except patient self-assessment versus caregiver assessment of the patient (p = .901) and patient assessment of the caregiver versus caregiver self-assessment (p = .995; see Table 2). The ANOVA for the mental composite scores was significant, F(3, 116) = 2.828, p < .05. Tukey post hoc comparisons indicated that the only two significantly different group means were patient assessment of the caregiver and caregiver assessment of the patient (p = .05). A marginally significant difference was found between the means of caregiver self-assessment and caregiver assessment of the patient (p = .078; see Table 2).
Discussion
In this study, we analyzed the dyads’ responses on the SF–12 to discover how each member viewed their own and each other’s QOL in two domains: physical and mental health. The results revealed perspective differences and similarities within the dyads. In terms of the more readily observed physical condition, patients with ALS and their caregivers gave similar ratings of each other’s status. However, regarding mental, social, and emotional well-being, patients with ALS and their caregivers did not have accurate views of the other’s mental state. This finding highlights the importance of clinicians emphasizing communication between patients and their caregivers in relation to each other’s emotional well-being, including spirituality, social wellness, and overall mental wellness.
Patients with ALS most frequently scored themselves as more burdensome than their caregivers rated them on the questionnaire. Although the caregivers may have felt that caregiving for their loved one added value and meaning to their life, the care recipients may have viewed caregiving only as adding burden and stress to the life of the caregiver. This finding is in agreement with recent research (Dassel & Carr, 2016) showing that caregivers experience benefits from caregiving, including growth in spirituality and faith, personal growth, and increased mastery. The discrepancy in perspectives within dyads highlights an interesting dynamic: Misunderstanding and miscommunication between a patient and caregiver have the potential to create stressors within the dyad that can be avoided if the members identify and address any misunderstanding.
Clinicians should be aware of and sympathetic to differences in how patients with ALS and their caregivers view emotional needs and QOL within the dyad. Clinicians can facilitate discussion between caregivers and patients with ALS to uncover and rectify misunderstandings. Clinicians can also refer caregivers and patients for mental health evaluation, if appropriate.
Limitations
This study has several limitations. Quantifying emotions using a Likert scale is difficult. We did not take stage of ALS into account, which can have an impact on caregiving load. Although the sample size was comparable to those of similar studies, it is a small convenience sample. The SF–12, although a gold standard for QOL measures, is generic and does not pertain specifically to patients with ALS and their caregivers. Last, some participants with an unconfirmed diagnosis of frontotemporal lobe dementia may have been included in this study.
Future Research
This study supports past research highlighting the multifaceted and complex nature of quality of life among patients and caregivers (Behari et al., 2005; Nordeson et al., 1998; Simmons, 2015; Simmons et al., 2000). The reasons for the differences found in perspectives on mental health require further investigation. Future research also is needed to develop a dual measure focused on QOL that simultaneously explores the psychosocial needs of both the patient and caregiver to inform a more holistic person- and family-centered care approach.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice:
QOL among patients and caregivers is multifaceted and complex, requiring comprehensive assessment and treatment strategies.
There is a need for the development of a dual assessment focused on QOL that explores the psychosocial needs of both the patient and caregiver simultaneously to guide a more holistic person- and family-centered approach to treatment.
Occupational therapy practitioners should use treatment strategies focused on enhancing communication between patients and caregivers.
Occupational therapy practitioners need to consider the mental health needs of patient–caregiver dyads, making referrals to other mental health professionals when needed.
Conclusion
People with ALS and their caregivers gave similar ratings of each other’s physical status. However, in regard to mental, social, and emotional well-being, people with ALS and their caregivers did not have accurate views of the other’s mental state. Occupational therapy practitioners should emphasize communication between patients and their caregivers about each other’s emotional well-being, including spirituality, social wellness, and overall mental wellness.
Footnotes
Acknowledgments
We thank Michael Rivner and the Augusta University Health ALS Clinic for their support of this research project. We also thank the participants for their contribution to this study.