
Abstract
Somatosensation and functional arm use are commonly impaired after stroke (Carey, 1995; Connell, Lincoln, & Radford, 2008; Tyson, Hanley, Chillala, Selley, & Tallis, 2008). Stroke survivors with upper-limb somatosensory loss are typically unable to differentiate limb positions or the shape, size, hardness, texture, or weight of objects (i.e., their discrimination skills are impaired; Carey & Matyas, 2011; Yekutiel, 2000). Approximately 50% of stroke survivors have somatosensory loss (Carey & Matyas, 2011; Kessner, Bingel, & Thomalla, 2016) with impaired processing in tactile and proprioception modalities and haptic object recognition (Carey, 1995; Connell et al., 2008; Kessner et al., 2016; Tyson et al., 2008).
Impaired somatosensation has a negative impact on motor functioning, including hand dexterity (Borstad & Nichols-Larsen, 2014; Kong, Chua, & Lee, 2011) and grasp and manipulation of objects (Blennerhassett, Matyas, & Carey, 2007; Nowak, Hermsdörfer, & Topka, 2003). Task-dependent practice is strongly recommended to treat upper-limb dysfunction, and positive treatment outcomes depend on people using their arm in life situations (Hubbard, Parsons, Neilson, & Carey, 2009; Liepert et al., 2000). Unfortunately, stroke survivors with somatosensory loss often learn to not use their affected arm in daily activities (Carey, 1995; Connell, McMahon, & Adams, 2014; Dannenbaum & Jones, 1993; Kessner et al., 2016; Yekutiel, 2000). Survivors report uncertainty regarding whether to use their sensory-impaired arm to perform tasks (Connell et al., 2014).
It is critical that rehabilitation assist stroke survivors with improving the use of their arm in daily life (Taub, Uswatte, Mark, & Morris, 2006); however, the evidence as to whether treatment of stroke-related upper-limb somatosensory impairment improves performance in daily activities and arm use is limited (Carey, Lamp, & Turville, 2016). Interventions for somatosensory loss include stimulation paradigms, robotics, mirror therapy, and discrimination retraining (Carey et al., 2016; Doyle, Bennett, Fasoli, & McKenna, 2010). Evidence for discrimination retraining, as a learning-based treatment, has indicated that retraining can improve somatosensation (Carey, Macdonell, & Matyas, 2011), but whether people change their daily arm use after sensory retraining is unknown. If stroke survivors with somatosensory loss increase their arm use during retraining, then gains in sensation, movement execution, and activity performance may be maximized.
In this study, we aimed to investigate individual differences in functional arm use in the treatment context of somatosensory discrimination retraining. We hypothesized that (1) participants would report a change in their daily arm use after somatosensory retraining and that arm use would differ considerably among participants; (2) participants’ self-report of daily arm use would be related to clinically measured upper-limb performance; and (3) changes in participants’ daily arm use would be associated with posttreatment somatosensation.
Method
This study involved pooled experimental treatment and assessment data of stroke survivors (N = 80) from two randomized controlled trials of somatosensory retraining: the Study of the Effectiveness of Neurorehabilitation on Sensation (SENSe) trial (Carey, Macdonell, & Matyas, 2011) and the Connecting New Networks for Everyday Contact Through Touch (CoNNECT) trial (Carey, Seitz, Levi, & Tournier, 2011). Data were pooled across studies because the recruited stroke participants had similar characteristics; the same measures were used; and the treatment protocol was the same, with the exception that participants in one study were also trained in specific occupational tasks. The current project was approved by the La Trobe University Human Ethics Committee, Melbourne, Victoria, Australia.
Participants and Recruitment
Participants recruited to the randomized controlled trials had been diagnosed with stroke and assessed as having upper-limb somatosensory impairment in at least two of three somatosensory modalities: tactile discrimination, proprioception, and tactile object recognition. Participants were medically stable and able to comprehend instructions and give informed consent. Exclusion criteria included central nervous system dysfunction other than stroke, peripheral neuropathy, and unilateral spatial neglect. Additional selection criteria for CoNNECT included participants being right-hand dominant, having no brainstem lesion, having had a single stroke, and being suitable for magnetic resonance imaging. Participants were at least 6 wk post-stroke for the SENSe trial and 12 wk poststroke for the CoNNECT trial. Stroke survivors participated in the trial once they had completed inpatient or outpatient treatment, particularly upper-limb rehabilitation.
Somatosensory Intervention
All participants received the experimental treatment of upper-limb somatosensory retraining. Retraining involved the following key principles (Carey, Macdonell, & Matyas, 2011):
Provision of graded somatosensory discrimination tasks that progressed from easy to difficult discriminations
Use of a variety of textures, limb angles, objects, and practice conditions to facilitate transfer of training effects
Intensive training across sensory discrimination tasks and sessions
Use of goal-directed attention to explore the somatosensory discrimination without vision
Trials designed with reduced discrimination options where the participant is prompted to anticipate what textures, objects, or limb positions might be felt
Provision of feedback on the accuracy of discrimination and method of exploration during the task by the clinician or vision
Use of vision or touch in the unaffected hand to calibrate somatosensory perception
Use of education about training principles and problem solving about how to use sensory retraining in daily tasks.
Participants engaged in a somatosensory program that used these principles to retrain discrimination and recognition skills in tactile, proprioception, and object recognition modalities. In addition, participants in the CoNNECT trial engaged in occupation-based retraining where they practiced sensory principles in two valued functional tasks (see Carey, Macdonell, and Matyas [2011] for further details about the sensory retraining program).
Treatment was delivered by an occupational therapist or physiotherapist experienced in neurological rehabilitation and trained in the specific treatment protocol. Treatment sessions occurred in an outpatient setting or participants’ home. Participants engaged in 10, 15, or 20 treatment sessions (depending on study design), with an average of 18 sessions (standard deviation = 7) for the pooled sample. Treatment sessions occurred 2–3 times per week; each session lasted 60–90 min.
Outcome Measures
Assessments occurred at pretreatment; posttreatment, immediately after the somatosensory treatment program; and follow-up, 3 or 6 mo after the somatosensory program as per study designs, with an average follow-up of 4.6 mo for the pooled sample. Clinicians who conducted assessments were blind to treatment condition.
Functional Arm Use.
The Motor Activity Log (MAL) was used to measure functional arm use (Uswatte, Taub, Morris, Light, & Thompson, 2006; Uswatte, Taub, Morris, Vignolo, & McCulloch, 2005). The MAL is a valid and reliable semistructured interview that captures participants’ perspective on how much they use their upper limb in performing daily activities (Park, Wolf, Blanton, Winstein, & Nichols-Larsen, 2008; Uswatte et al., 2005). For the purpose of this study, MAL scores were calculated as average score per item (total number of items divided by number of valid items) and measured participants’ perceived amount of arm use in daily task performance.
The Action Research Arm Test (ARAT) is a performance-based measure of ability to use the arm (Lyle, 1981). The participant performs 19 actions with his or her upper limb, and the clinician rates the quality of movement (van der Lee et al., 2001).
Somatosensory Outcomes.
Standardized somatosensory outcome measures were used to assess sensation in three modalities: tactile discrimination, proprioception, and tactile object recognition. Sensory modalities were tested separately, as recommended, and these modalities were investigated because they are typically impaired after stroke (Carey, 1995; Connell et al., 2008). Discriminative loss is the most common type of stroke-related upper-limb somatosensory impairment (Carey & Matyas, 2011); therefore, we investigated the following outcome measures for discrimination skills:
The Fabric Matching Test (FMT; Carey, 1993, 1995) was used to assess tactile discrimination. The FMT involves two identical sets of 10 cotton-based fabrics that vary along a continuum of roughness. With their vision occluded, participants are presented with two textures and are required to feel them with the index or middle finger. Participants indicate whether the two textures feel the same or different. If they feel different, participants move along the texture continuum until they perceive a match between fabrics. Results for the FMT are calculated from 10 trials and involve a correlation score (ρ score) of the rank order of actual and perceived roughness.
The Wrist Position Sense Test (WPST; Carey, Oke, & Matyas, 1996) was used to assess wrist proprioception. Each participant's hand is placed in a splint in a boxlike apparatus so that vision of the hand is occluded. The clinician moves the hand, and participants estimate their wrist position. Participants use a lever on a protractor scale to indicate the angle that matches their wrist position. The difference between actual and estimated wrist position is recorded in degrees. The results of 20 trials are averaged to determine the WPST score.
The functional Tactile Object Recognition Test (fTORT; Carey, Nankervis, LeBlanc, & Harvey, 2006) was used to assess tactile object recognition. Participants feel 14 everyday objects without being able to see them and are required to refer to a poster display of same, similar, or very different objects and select the object that they feel. The fTORT is based on Lederman and Klatzky’s (1987) work detailing seven sensory attributes and exploratory procedures of haptic object recognition. Results from fTORT are calculated as summed accuracy scores.
The FMT, WPST, and fTORT have good discriminative test properties, high reliability, and normative standards (Carey, Macdonell, & Matyas, 2011; Carey et al., 1996, 2006).
Valued Activities.
The Canadian Occupational Performance Measure (COPM; Law et al., 2005) was used for treatment planning in the CoNNECT trial. The COPM involves participants identifying occupations they are experiencing difficulties with and want to improve. In the CoNNECT trial, participants identified specific occupational goals that were negatively affected by the upper-limb somatosensory loss. Participants rated the importance of identified daily tasks using a 10-point scale ranging from 1 (not very important) to 10 (extremely important). In the current study, the COPM was used to explore the value and importance to participants of the daily activities to which they also responded on the MAL.
Data Analysis
Quantitative analyses of pooled data involved descriptive statistics, correlation, and regression modeling. We used IBM SPSS Statistics (Version 23; IBM Corp., Armonk, NY) to perform these analyses. Descriptive statistics were used to describe demographic data. We conducted post hoc analyses of the contribution of each trial to the pooled sample to ensure that the results were comparable and that neither sample biased the results. To understand daily arm use, we graphed MAL scores using box plots and analyzed them with descriptive statistics and Wilcoxon signed-rank tests as a result of skewed distributions.
Spearman’s rank coefficient was used to analyze the relationship between self-reported arm use (MAL scores) and performance capacity of the upper limb (ARAT scores). Spearman’s rank coefficient was used because visual inspection of the data showed skewed distributions. The statistical significance of differences between interrelated correlations was calculated using the method outlined by Zou (2007).
To explore the importance of MAL activities, we identified COPM activity goals that matched the items on the MAL. The importance ratings that participants gave the COPM activities were recorded; a participant example was randomly chosen for each activity item in the MAL to explore the importance of MAL daily activities.
Our main interest was the association between change in functional arm use and somatosensory discrimination skills after sensory retraining. To investigate this association, the data were inspected visually with scatterplots, and regression modeling was used. Standard linear multiple regression analyses were performed using the independent variables change in functional arm use (MAL score) and initial value of somatosensory impairment and the dependent variable posttreatment modality-specific somatosensory ability. Initial somatosensory impairment was also included in multiple regression analyses because it was likely to influence somatosensory recovery (Connell et al., 2008) and was correlated with functional arm use. Results related to initial somatosensory impairment are the subject of a related publication (Turville, Carey, Matyas, & Blennerhassett, 2016).
Results
A total of 80 participants were involved in this study. Participant characteristics were similar between the trials, as displayed in Table 1. Although the CoNNECT trial involved additional recruitment criteria, the majority of participants in the pooled sample (91%) were a minimum of 12 wk post-stroke and right-hand dominant. In regression modeling, negligible differences were found between the trials and treatment dosage. Moreover, superimposed scatterplots indicated that the two trials had strongly overlapped scatterclouds, and no possibility for a regression artifact was evident.
Participant Characteristics
Note. CoNNECT = Connecting Networks for Everyday Contact Through Touch; IQR = interquartile range; M = mean; SD = standard deviation; SENSe = Study of the Effectiveness of Neurorehabilitation on Sensation.
Participants’ Perceived Change in Daily Arm Use After Somatosensory Retraining
Participants reported changes in their functional arm use after somatosensory retraining (Figure 1). Median results suggest that participants initially reported very rarely or rarely using the affected arm to complete daily activities. After treatment, median findings indicate that arm use increased to half as much as prestroke use. The change in perceived arm use was statistically significant from pretreatment to posttreatment (z = −6.80, p < .01) and from pretreatment to follow-up (z = −6.17, p < .01). Both changes had large effect sizes (rs = .54 and .50, respectively). The change in perceived daily arm use from posttreatment to follow-up was not statistically significant (z = 0.89, p > .05). Despite changes in arm use after sensory retraining, arm use among participants was highly variable (see Figure 1). We found individual differences in arm use after retraining, with the interquartile range spreading from an average item score of approximately 1 (very rarely) to 4 (same as prestroke).
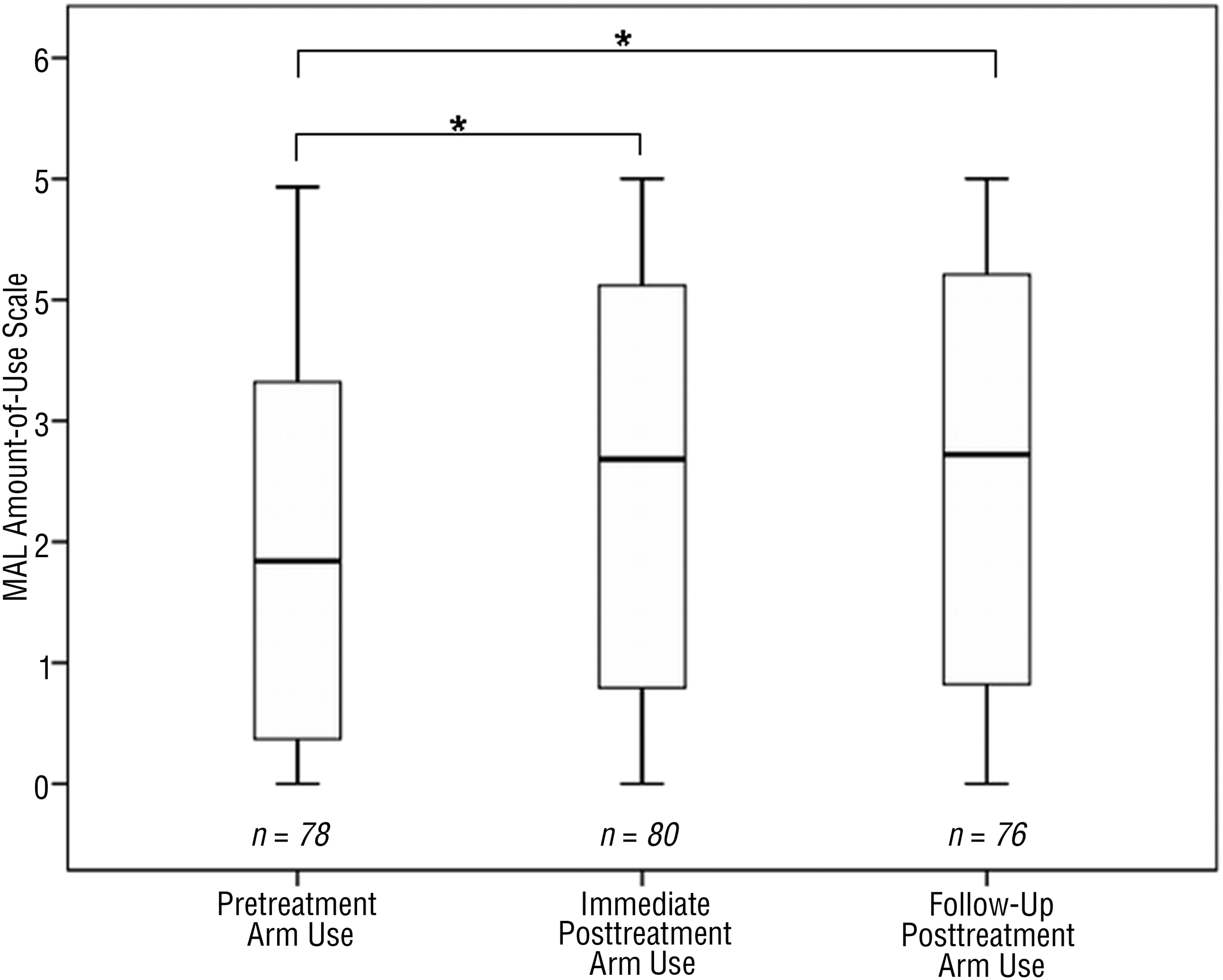
Participants’ report of daily arm use before and after somatosensory retraining.
To further understand what a change in arm use may have meant for stroke survivors, we explored whether and how much participants valued the subset of MAL activities aligned with COPM goals in the context of their lives. Table 2 presents examples of these activities and their importance to participants’ life situations. For some participants (25%), MAL items were identical to highly valued daily activities on the COPM (Table 2).
Examples of MAL Items and Ratings
Note. Participants were provided with pseudonyms for confidentiality purposes. Activities listed were MAL items and occupational goals participants identified using the COPM. Importance of activities was rated using the COPM’s 10-point scale, ranging from 1 (not very important at all) to 10 (extremely important). MAL amount-of-use ratings were as follows: 0 (never [used weaker arm]), 1 (very rarely), 2 (rarely), 3 (half prestroke), 4 (three-quarters prestroke), 5 (same as prestroke). Handwriting and typing are considered as one activity group in MAL but are separated here on the basis of COPM goal choice. COPM = Canadian Occupational Performance Measure; MAL = Motor Activity Log.
Parentheses contain raw pretreatment to posttreatment MAL amount-of-use ratings.
Relationship Between Participants’ Perceived Arm Use and Performance-Based Measures of Arm Use
Before treatment, the MAL and ARAT showed a positive relationship with a ρ of .69 (n = 29). After treatment, the relationship between the MAL and ARAT had an apparently higher ρ value of .91 (n = 29). This difference was not statistically significant, even after testing using the Zou (2007) method, which allows for interdependence of two correlations.
Change in Participants’ Functional Arm Use and Relationship to Posttreatment Somatosensory Outcomes
Table 3 summarizes the results of the regression analyses of the relationship between change in functional arm use (MAL score) and somatosensory outcomes after retraining. Change in functional arm use was uniquely associated with small amounts of variance in posttreatment somatosensory outcomes (i.e., 9.4% for tactile discrimination, 2.8% for proprioception, 1.5% for object recognition) and at follow-up (i.e., 1.9% for tactile discrimination, 4.2% for proprioception, 1.4% for object recognition). As displayed in Table 3, two of three regression results for each change time point achieved statistical significance (pre- to posttreatment change for tactile discrimination and object recognition and pretreatment to follow-up change for wrist proprioception and object recognition). Regression modeling from posttreatment to follow-up showed minimal association and no statistically significant differences (tactile discrimination, β = −0.01, p > .05; proprioception, β = 0.08, p > .05; object recognition, β = 0.08, p > .05). Visual inspection of the data showed heteroscedasticity; participants with change scores larger than 1 showed different variability. This phenomenon was replicated in the follow-up treatment data and was not noticeable in outcomes of tactile object recognition.
Regression Analyses of Relationship Between Changes in Functional Arm Use and Somatosensation Measures After Somatosensory Retraining
Note. MAL = Motor Activity Log.
Discussion
We investigated individual differences in functional arm use and their relationship to somatosensation after sensory retraining. Individual differences in self-reported change in arm use were associated with posttreatment somatosensation, after allowing for differences in initial sensory capacity. Participants’ perceived amount of daily arm use was related to performance capacity of the upper limb (e.g., grasp, reach). Stroke survivors differed considerably in their daily arm use and showed the capacity to increase their functional arm use after somatosensory retraining.
Participants who reported greater amounts of change in arm use were more likely to have higher levels of tactile and proprioceptive performance after retraining. Their increased arm use could affect practice of sensorimotor skills or, perhaps, vice versa. It is possible that participants with increased daily arm use were using somatosensory skills more often. Practice in using somatosensory feedback is necessary for upper-limb actions because this information informs feed-forward models of motor control (Frey et al., 2011; Kessner et al., 2016). Stated more broadly, experience is essential to promote adaptive neuroplasticity changes in the brain after stroke (Liepert et al., 2000; Nudo, 2007; Spengler et al., 1997).
Participants with lesser amounts of change in daily arm use had posttreatment somatosensory skills that ranged along the continuum of performance. Because change scores were used, one needs to consider what a small amount of change in arm use meant in the context of participants’ lives. Their arm use may have changed only a small amount, but they were still using their arm, possibly practicing, and using somatosensation. Alternatively, participants with reduced arm use may have not changed their daily arm use much because of more severe motor impairment. In interpreting these results, one must also consider that natural brain recovery processes may influence arm use and somatosensation.
The results suggest a relationship between participants’ perceived daily arm use and performance capacity of the upper limb (e.g., grasp, reach). This finding lends support to the validity of self-reported changes in arm use in this study. The use of self-reported upper-limb measures has been criticized (Doman, Waddell, Bailey, Moore, & Lang, 2016). Even so, our findings suggest that stroke survivors’ self-reported daily arm use was relatively consistent with upper-limb performance observed in the clinical setting.
Research has suggested that stroke survivors with somatosensory loss learn to not use their affected arm in daily tasks (Carey, 1995; Connell et al., 2014; Yekutiel, 2000). Our sample reported increased daily arm use after sensory retraining, indicating that they may have relearned to use their arm in daily tasks (i.e., reversal of learned nonuse) during the somatosensory retraining program. Researchers have proposed that the greater the learned nonuse of the upper limb, the greater the potential for change in limb use in daily life (Taub et al., 2006). CoNNECT participants reported changes in arm use in daily activities that were highly valued in the context of their life situations.
Results showed a large range in participants’ perceived amount of arm use in daily activities after retraining, which is consistent with the results of other stroke studies (Doman et al., 2016). Variability in functional arm use could be connected to other influencing variables. Initial severity of motor deficit is likely to have an impact on functional arm use after stroke (Chen & Winstein, 2009; Coupar, Pollock, Rowe, Weir, & Langhorne, 2012). Evidence for the influence of cognitive functioning on upper-limb use is inconclusive (Coupar et al., 2012), yet cognition, mood, psychosocial support, and prior functional status have been found to predict functional recovery after stroke (Hoffmann & McKenna, 2001). These psychosocial variables need to be considered from a clinical perspective and in future research.
Principles of somatosensory retraining used in this study contrast with those used in current clinical treatment of somatosensory loss, which focuses primarily on educating clients on the risks of somatosensory loss (e.g., burns, crush injuries) and compensating via vision and use of the unaffected limb (Doyle, Bennett, & Gustafsson, 2013; Pumpa, Cahill, & Carey, 2015). Compensation strategies seem to decrease use of the affected arm use in daily activities. Although safety concerns need to be addressed, sensory retraining teaches people to explore somatosensory features of the environment for arm use.
Limitations and Future Research Directions
This study has several limitations that require discussion. We took reasonable steps to ensure that the pooled sample used in this study was homogeneous according to participants, treatment, and outcome measurement, yet differences may have existed between trial samples. Differences in treatment protocols between the trials existed, but these differences were considered minimal given that we analyzed contributing samples and all participants received identical modality-specific sensory retraining in a program designed to facilitate transfer of learning. Participants were not excluded according to severity of hemiparesis, but this sample could differ from the broader stroke population on other characteristics. Moreover, correlation and regression results reported in this study do not imply causality and need to be interpreted from this perspective.
The MAL consists of self-reported data that may be subject to memory and social desirability bias. Further exploration of individual differences among participants who have a small amount of change in MAL score is needed using data triangulation and mixed methods. Variables likely to affect daily arm use during sensory retraining could be explored in a qualitative inquiry with stroke survivors. Results on the MAL and COPM could be further explored to understand the relationship between arm use and valued activity performance.
Implications for Occupational Therapy Practice
Findings from this study have the following implications for clinical practice:
Stroke survivors with impaired somatosensation can perceive positive change in use of the stroke-affected upper limb in daily tasks after somatosensory retraining, which may be related to reversal of learned nonuse, remediation of sensorimotor function, or both.
Individual differences in arm use appear to have a small and significant role in explaining the variance in somatosensory recovery after retraining.
Stroke survivors with somatosensory loss differ considerably in their daily arm use; therefore, it is essential that retraining be tailored to individual needs and wants.
Clinicians are encouraged to consider the individual differences in functional arm use among clients with somatosensory impairment and in the potential to improve arm use in valued activities in association with somatosensory retraining.
Footnotes
Acknowledgments
The study was funded by an Australian Government Research Training Program Scholarship (M. Turville), National Health and Medical Research Council (NHMRC) project grants (GNT1022684, Effective Sensory Rehabilitation After Stroke: Targeting Viable Brain Networks, and GNT191214, Effectiveness of Training Somatosensation in the Hand After Stroke: A Randomized Controlled Trial), the Perpetual Foundation, the James S. McDonnell Foundation 21st Century Science Initiative in Cognitive Rehabilitation–Collaborative Award (220020413), an Australian Research Council Future Fellowship (FTO992299), and an NHMRC Career Development Award (307905). The SENSe (ACTRN1260500060951) and CoNNECT (ACTRN12613001136796) trials are registered with the Australian New Zealand Clinical Trials Registry at ![]() .
.