
Abstract
This case report is the first in a series of reports designed to determine the feasibility of implementing game-based neurorehabilitation using telehealth technologies (GbN+TT) for children with cerebral palsy, evaluate the responsiveness of relevant outcome measures to changes in motor impairment and activity participation after intervention, and identify technological challenges associated with implementation of GbN+TT. The participant completed more than 56 hr of game-based neurorehabilitation over 8 wk using the Timocco platform in his home. The primary measures of motor impairment (Bruininks–Oseretsky Test of Motor Proficiency, Second Edition) and function (Pediatric Motor Activity Log) were both sensitive to change. Results indicate that it is feasible to administer GbN+TT to a child with cerebral palsy and monitor outcomes using standardized assessments.
Cerebral palsy (CP) is a congenital, nonprogressive disorder of movement, posture, and muscle tone that occurs after damage to the developing fetal or infant brain. Cerebral palsy is the most common motor disability of childhood, with an average prevalence of 3.3 children per 1,000 live births (Centers for Disease Control and Prevention, 2016). The many types of cerebral palsy depend on the nature of the injury and area of involvement. Hemiparetic (unilateral) CP is an asymmetrical form of paresis that results in one side of the body being weaker than the other. Hemiparesis affects approximately 1 in 3 children with CP (Hagberg, 2000) and, when not effectively treated, may lead to lifelong impairment affecting unimanual and bimanual tasks. This impairment may lead to difficulties in performing typical occupations of childhood, including activities of daily living, school, and play (Taub, Ramey, DeLuca, & Echols, 2004).
Research suggests that intensive practice can improve motor performance and function of the more involved upper extremity in children with hemiparetic CP (Charles & Gordon, 2005). Intensive practice involving shaping (i.e., part practice) or repetitive task practice (i.e., whole practice) can promote neuroplastic changes and lead to new motor behaviors that are more skillful, complex, adaptable, or automatic (Gordon, Schneider, Chinnan, & Charles, 2007), making them easier to integrate into the child’s daily activities. Tasks are shaped to allow for successful completion, then made progressively harder (e.g., requiring greater speed, accuracy, or movement repetition) as the child improves performance (Gordon, Charles, & Wolf, 2005). As performance improves, simple tasks are combined into functional patterns and routines and practiced repetitively. Intensive therapies have great appeal for both therapists and caregivers of children with CP. Unfortunately, such approaches may be resource intensive and fatiguing (Christman, McAllister, Claar, Kaufman, & Page, 2015).
Motion-based video games have been used within rehabilitation contexts for the better part of a decade (Parry et al., 2014). By adapting commercially available gaming systems such as the Nintendo Wii (Nintendo, Kyoto, Japan), Microsoft Kinect (Microsoft, Redmond, WA), and Playstation Move (Sony Interactive Entertainment, Foster City, CA), therapists have found a motivating way to facilitate repetitive practice of motor skills (Sandlund, Waterworth, & Häger, 2011). For example, game-based neurorehabilitation (GbN) has been shown to be an effective treatment tool for improving trunk control (Barton, Hawken, Foster, Holmes, & Butler, 2013), upper-extremity function (Chen, Lee, & Howard, 2014), and functional mobility (Deutsch, Borbely, Filler, Huhn, & Guarrera-Bowlby, 2008). Similarly, virtual reality games seem to be effective in elevating self-efficacy, volition, playfulness, and motor function in children with CP (Parsons, Rizzo, Rogers, & York, 2009).
Although off-the-shelf gaming systems are appealing for several reasons, it is important to note that these systems were not designed with rehabilitation in mind. Thus, therapists have limited ability to manipulate control parameters such as the speed and accuracy of movement and to collect movement-specific data important for documenting progress. Another limitation of GbN is the need for the therapist to be present in the client’s home, where the majority of game play must occur to ensure that motor practice is of sufficient intensity.
The use of telehealth technologies (TT) such as video conferencing and remote monitoring in combination with GbN may help overcome these limitations. This research was undertaken in an effort to determine the feasibility of implementing GbN for children with CP using TT, evaluate the responsiveness of relevant outcome measures to changes in motor impairment and activity participation after intervention, and identify technological challenges associated with implementation of GbN+TT.
Method
Recruitment
Potential participants were recruited (Page & Persch, 2013) from rehabilitation clinics near a major, Midwestern academic medical center and were enrolled in the study if they met the following eligibility criteria:
Age 4–12 yr
Diagnosis of hemiparetic spastic CP
Ability to follow basic instructions and communicate needs and preferences as indicated by a Communication Function Classification System (Hidecker et al., 2011) assignment of Level I, II, or III
Difficulty using the more affected arm and hand as indicated by a Manual Ability Classification System (Eliasson et al., 2006) assignment greater than Level I
No serious comorbid medical diagnoses
No dystonia
No severe behavior problems
No major vision or hearing impairment
No botulinum toxin treatment within the past 6 mo
Stable and supportive family.
Assessment of eligibility was conducted in two parts: (1) Screening was conducted through a parent interview, and (2) the researchers confirmed eligibility at the time of enrollment. This case report was reviewed and approved by the local institutional review board.
Instrumentation
After eligibility screening and enrollment, the participant completed a battery of tests scheduled to occur 2 wk before and after treatment. The assessment battery included the Assisting Hand Assessment (AHA; Krumlinde-Sundholm, Holmefur, & Eliasson, 2007); the Bruininks–Oseretsky Test of Motor Proficiency, Second Edition (BOT–2; Bruininks & Bruininks, 2005); the Quality of Upper Extremity Skills Test (QUEST; Law et al., 1991); the Pediatric Motor Activity Log (PMAL; Taub et al., 2004); the Pediatric Evaluation and Disability Inventory—Computer Adapted Test (PEDI–CAT; Haley et al., 2011); and the Perceived Stress Scale (PSS–14; Cohen, Kamarck, & Mermelstein, 1983).
The AHA measures the respondent’s ability to use the more involved arm and hand to assist in bimanual activities. The assessment is intended for children ages 18 mo to 12 yr and incorporates semistructured play with specific items. The AHA has excellent reliability and validity (Krumlinde-Sundholm, Holmefur, Kottorp, & Eliasson, 2007). The BOT–2 is a standardized assessment of fine and gross motor ability designed for children and adolescents ages 4 to 21 yr. The BOT–2 has moderate reliability and strong validity (Deitz, Kartin, & Kopp, 2007). The QUEST is used to assess movement patterns and hand function in children with CP ages 18 mo to 8 yr and has strong reliability (Thorley, Lannin, Cusick, Novak, & Boyd, 2012) and validity (DeMatteo et al., 1993).
The PMAL is a parent-report assessment of functional upper-extremity use in natural environments for children ages 2 to 8 yr. The PMAL has strong reliability and validity (Wallen, Bundy, Pont, & Ziviani, 2009). The PEDI–CAT is a parent-report assessment of self-care, mobility, social function, and responsibility in children ages 6 mo to 21 yr. Psychometric evaluation of the PEDI–CAT indicates strong reliability and validity (Dumas & Fragala-Pinkham, 2012). The PSS–14 is a self-report measure of perceived stress in life situations that we used to assess the degree of stress in parents caused by GbN+TT. The PSS–14 has excellent reliability and adequate validity (Cohen et al., 1983).
In addition to these formal measures, we evaluated GbN performance metrics (Timocco, 2016) such as midline crossing, movement efficiency, and response time on an exploratory basis. We also used informal questionnaires, parent and child interviews, and session notes to evaluate the feasibility of GbN+TT.
Technology
After screening, enrollment, and pretest assessment, the participant was shipped the equipment necessary for GbN+TT. Detailed instructions for equipment setup and information about desired conditions for GbN+TT were included in this shipment.
Game-Based Neurorehabilitation.
Timocco (Timocco, Inc., Akron, OH) is a motion-based gaming web application designed by an occupational therapist with rehabilitation in mind. As such, it allows for extensive back-end control of movement parameters and access to relevant data. Timocco requires a computer with Internet access; a webcam; and one or two small balls or objects colored red, green, or blue. To play Timocco games, the child stands in front of the webcam holding on to the colored balls. The webcam recognizes the balls, and the app translates movement of the balls into movement of gaming elements. For example, the Falling Fruits game is designed to challenge midline crossing, range of motion, and bilateral coordination. The child is depicted on screen as a monkey. The child must catch fruits as they fall from the top of the screen and sort them into the correct basket at the bottom. Figure 1 shows the monkey catching a pear with two hands. The child’s next step is to move the arms toward the lower right to sort pears into the appropriate basket.

Screen capture of the Falling Fruits game on the Timocco platform.
Telehealth Technologies.
Synchronous videoconferencing was accomplished using the Kubi telepresence robot (Revolve Robotics, San Francisco, CA), an Apple iPad (Apple, Cupertino, CA), and a tripod. After pairing the robot with the iPad using Bluetooth technology (Bluetooth SIG, Kirkland, WA), a remote user (i.e., therapist or research assistant) was able to control the robot’s pan and tilt functions while video conferencing with the child and parent. This setup allowed the therapist to observe the child’s performance in his natural setting and to consult with the parents without the need for someone to hold and operate the iPad. The integration of GbN and TT is visually depicted in Figure 2.
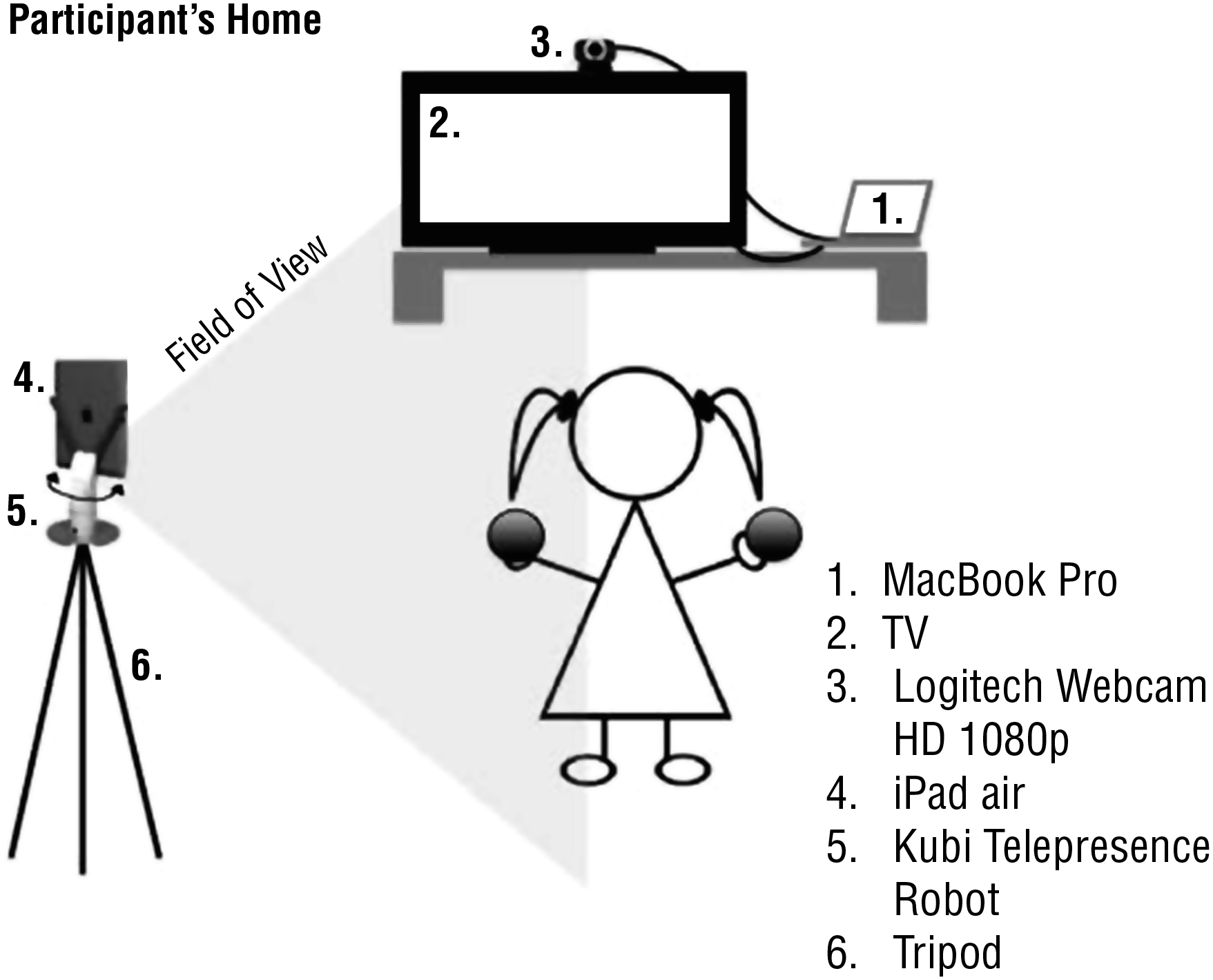
Schematic of game-based neurorehabilitation and telehealth technologies equipment setup.
Intervention Protocol
The participant was directed to complete a total of 7 hr/wk of GbN for 8 wk (56 hr total dose) using the Timocco platform. After the initial assessment, the researchers created GbN treatment plans using the back end of the Timocco interface. Games were selected on the basis of the child’s age, current skill level, and goals developed collaboratively. The researchers configured games to challenge the participant’s bilateral coordination, midline crossing, motor control and accuracy, motor efficiency, range of motion, reaction speed, and upper body strength and to enable them to monitor on a weekly basis parameters such as duration of game play, number of correct movements, number of errors, and response time. It was also possible to track and visualize movement patterns of the participant’s hands (e.g., Figure 3). Data were saved for key games and were extracted from the Timocco platform. The researchers modified GbN plans as the participant’s skills increased.
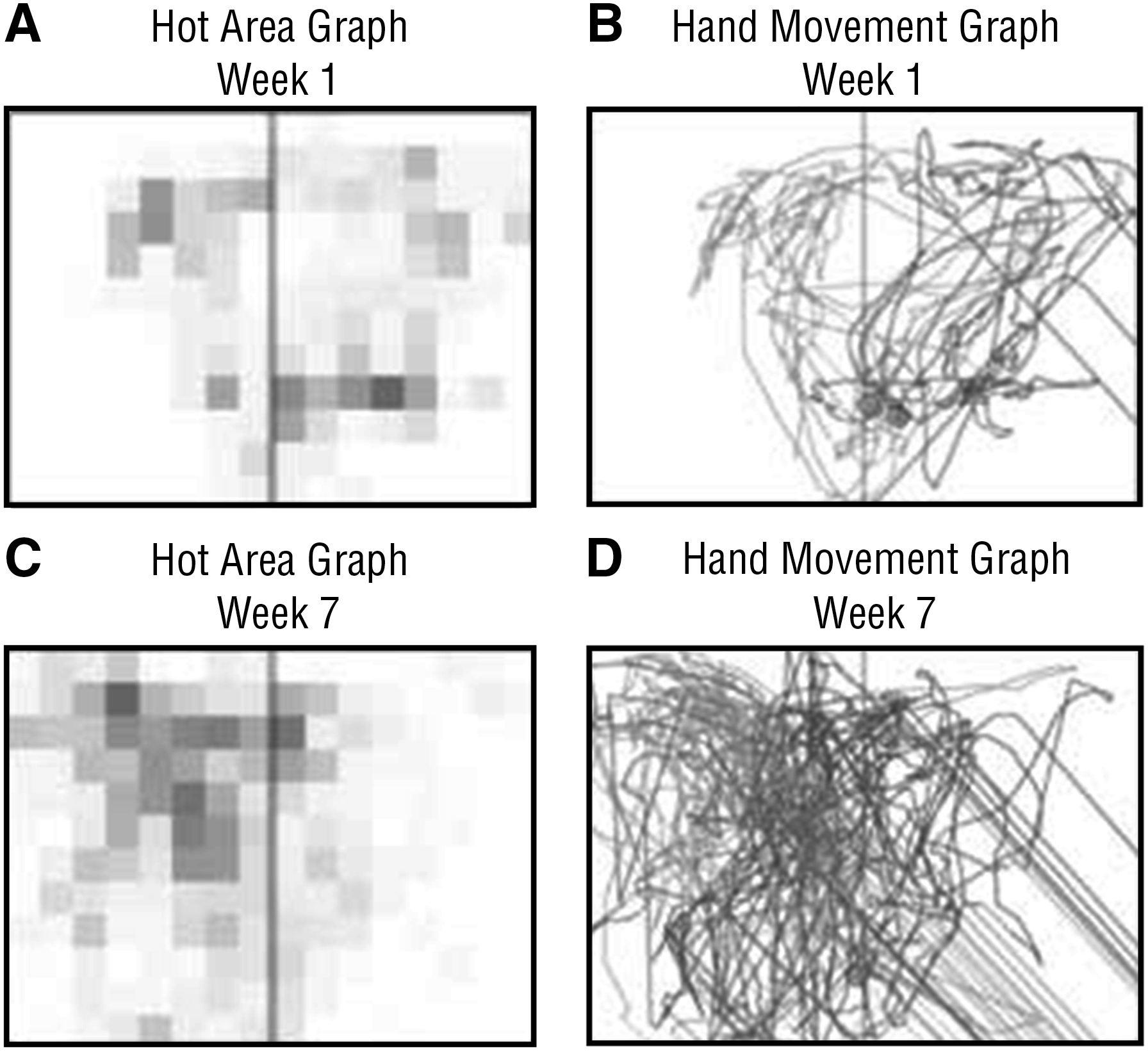
Visualization of hand tracking data.
In addition to the weekly dose of GbN, a member of the research team conducted 30-min synchronous consultations with the participant and parents each week (4 hr total) using TT. This approach allowed the researchers to observe performance in the home environment, problem solve technological issues, coach parents, provide feedback, and discuss any other treatment-related issues. For example, the researchers sometimes encouraged parents to reinforce a specific motor skill, such as bilateral reaching, using verbal praise, big smiles, hugs, or small tangible rewards during a particular week of the intervention. To our knowledge, this intervention was the first to combine GbN and TT within the field of pediatric rehabilitation for use with a young child.
Data Analysis
In alignment with the study design, data analysis focused on participant characteristics and changes in participant scores from pretest to posttest. We assessed demographic characteristics, such as age and gender, and reviewed the participant’s medical history. Descriptive statistics were used, as appropriate, to characterize the participant’s response to intervention.
Results
Participant
The participant was a White boy age 5 yr with a primary diagnosis of spastic hemiparetic CP; the pseudonym “Chris” will be used hereafter. Chris experienced a perinatal ischemic stroke resulting in right-sided hemiparesis and was diagnosed with CP at age 11 mo. Chris’s mother is a technologically sophisticated occupational therapist and was capable of providing detailed feedback and implementing researchers’ weekly recommendations.
Feasibility of the Intervention
In total, Chris completed more than 56 hr of GbN, as prescribed in the protocol, during the 8-wk intervention. His mother reported that Chris was highly motivated to play Timocco games, which was evident during weekly TT consultations; Chris eagerly described his efforts to “beat” games or progress to harder levels.
The PSS–14 results indicate that Chris’s mother’s stress decreased during the course of the intervention. There were no adverse events.
Responsiveness of Outcome Measures
Outcome measures were administered successfully at pretest. Posttesting was delayed 2 wk (i.e., in total, 4 wk after intervention ceased) because of unanticipated family travel. Chris’s performance improved for all outcome measures from pre- to posttest with the exception of the QUEST Dissociated Movements subscale, which remained the same (Figure 4). Of particular note, Chris’s raw score on the Fine Motor Integration subscale of the BOT–2 increased 10 points. His performance on the Fine Manual Control, Manual Dexterity, and Bilateral Coordination subscales of the BOT–2 improved by 2, 2, and 1 points, respectively. On the AHA, Chris’s logit score increased from 79 to 80. His standardized score for the Grasp subsection of the QUEST increased from 88.88 to 114.81. The PMAL indicated that Chris’s ability to perform functional unilateral activities such as turning a page in a book and opening a cabinet door improved from pre- to posttest. Finally, the PEDI–CAT revealed substantial improvement in Chris’s occupational performance and participation. His scaled scores for the Daily Activities, Mobility, and Social–Cognitive domains increased by 4, 2, and 1 points, respectively.
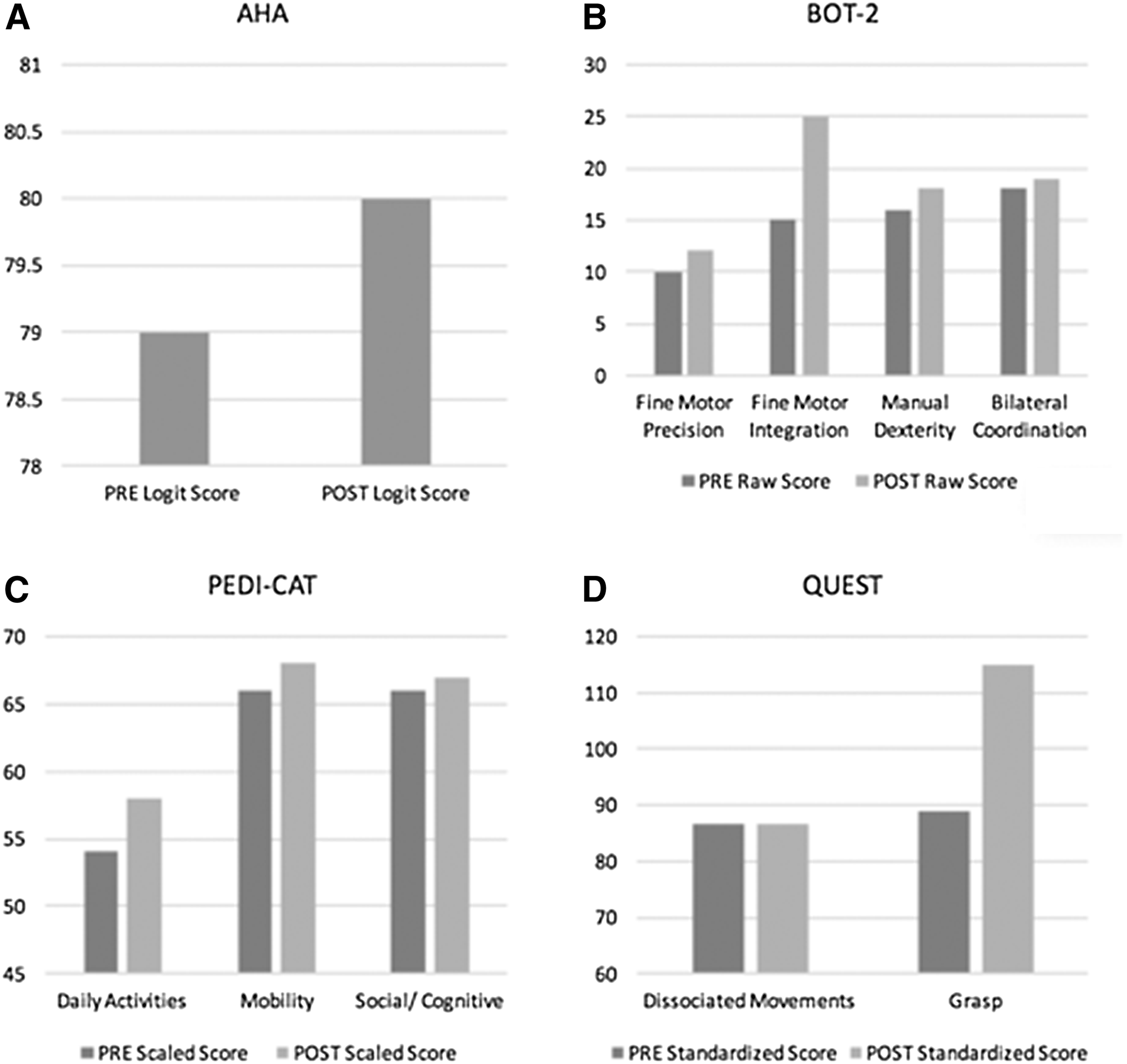
Performance on outcome measures.
Technological Challenges
Chris occasionally encountered technical difficulties and made sure to report them to the researchers. Although the family left GbN equipment set up throughout the week, they chose to use TT (i.e., Kubi plus iPad) only during weekly consultations. For this reason, researchers often had to ask Chris’s mother or father to reposition the TT so the Kubi pan and tilt functions would allow for full observation of performance. Internet access was maintained using the family’s personal WiFi network and an LTE hot spot. The quality of video for consultations was generally good enough to observe Chris’s movements but not good enough to see what was happening on the TV screen during GbN. Audio quality was consistently adequate for TT consultations.
Discussion
We evaluated the feasibility of GbN+TT using questionnaires, interviews, and review of session notes. Of primary interest is the finding that Chris had no difficulty completing the prescribed 56-hr dose of GbN+TT. Indeed, Chris’s total dose of GbN+TT exceeded that completed by three adolescents with CP in a separate study (Huber et al., 2010). This finding is encouraging because most intensive therapy protocols require a similar amount of practice. For example, signature pediatric constraint-induced movement therapy (Case-Smith, DeLuca, Stevenson, & Ramey, 2012), partial body-weight-supported treadmill training (Damiano & DeJong, 2009), and hand–arm bimanual intensive therapy (Gordon et al., 2007) require similar amounts of physical activity training.
It is also encouraging that Chris’s motivation remained high throughout the intervention. In a similar finding, Sandlund et al. (2011) found that children with CP were highly motivated to complete intensive motion-based video games. Additionally, Bryanton et al. (2006) reported that children with CP preferred video games over conventional exercises because the games were more fun and of greater interest. Like Chris’s mother, parents reported that they noticed their child’s interest in playing motion-based games and were more likely to facilitate gaming than conventional exercise (Bryanton et al., 2006).
Outcome measures were administered in the standardized manner and appeared to be sensitive to change associated with participation in the Gbn+TT intervention. Indeed, all measures but one showed improved scores from pre- to posttest. These findings parallel those of Sandlund et al. (2011), who successfully administered an assessment battery to children with CP before and after participating in motion-based video games. However, Chris’s pre–post changes for the selected outcome measures did not exceed minimal clinically important difference levels (Klingels et al., 2010). In addition, delayed administration of outcome measures at posttest deviated from the planned protocol and may have been prevented by additional questioning regarding family travel plans. That said, the family chose to travel with the GbN+TT equipment and completed the final week of intervention while on vacation, ceasing intervention after Week 8.
Finally, technological challenges did occur. Chris found software glitches and reported them during weekly TT consultations. This feedback was passed along to the software developers at Timocco, who corrected the issues in a timely manner. The research team also experienced technical difficulties related to faulty cables and adapters and the individual characteristics of Chris’s TV and Internet connection. Because other authors (Gulmans et al., 2010) have reported similar difficulties when using novel TT, we consider these challenges minor. Taken together, GbN+TT proved a feasible and motivating mechanism for engaging a child with hemiparetic CP in intensive task practice.
Limitations
Several limitations must be acknowledged. First, because the data presented here represent only one case, the results of this study are informative but not generalizable. Second, the GbN and TT equipment selected for this research (i.e., Timocco, Kubi, iPad) were familiar, convenient, and accessible to the authors. Although they mitigated many of the limitations of other GbN and TT equipment, other technologies or platforms may have achieved better results. Likewise, we selected a broad range of outcome measures of both impairment and participation, but other tools may have performed more optimally.
A selection bias resulted from enrollment of Chris and his occupational therapist mother, both of whom were known to the researchers before enrollment. Chris’s mother was able to provide valuable feedback throughout the intervention that will be used to refine the intervention for children and families who may not have similar experience with technology and therapy. Finally, we are not able to exclude the possible effects of maturation and the researchers’ expectation of intervention efficacy. The successful completion of this case study nevertheless will inform intervention for future participants within this case series and may lead to additional studies that include refined intervention and assessment techniques.
Implications for Occupational Therapy Practice
The method for provision of GbN+TT and findings presented in this article have the following implications for occupational therapy practitioners:
It is feasible to administer GbN+TT to a child with hemiparetic CP and monitor outcomes using common standardized assessments.
Game-based neurorehabilitation is highly motivating and fun and may be used to facilitate intensive task practice.
The use of a telepresence robot (i.e., Kubi) allows practitioners to observe performance in natural settings without traveling to the home or having someone hold a computer or iPad.
Telehealth technologies may enable occupational therapy practitioners to treat clients in underserved (e.g., rural, impoverished) communities.
The combination of GbN and TT allows practitioners to supervise high-dose (i.e., intensive) intervention using a consultation model that requires significantly less therapist time.
Conclusion
Neurorehabilitation using motion-based gaming is motivating for children and may be effective for treating motor impairment. The use of TT provides practitioners with a mechanism to supervise (e.g., consult, observe) treatment for clients in underserved communities. This research provides initial evidence that it is feasible to administer GbN and TT and monitor relevant outcomes. This novel integration of technologies allows practitioners to provide intensive therapies using a model that requires significantly less therapist time.
Footnotes
Acknowledgments
Timocco, Inc., provided the materials and website access for this study but did not have a role in data collection, data analysis, or manuscript preparation. The researchers have no financial interest in the technologies reported herein. This research was presented, in part, at the Ohio Occupational Therapy Association conference, September 2015, Columbus, OH; the Wisconsin Occupational Therapy Association annual conference, October 2015, Madison, WI; and the American Academy for Cerebral Palsy and Developmental Medicine annual meeting, October 2015, Austin, TX.