
Abstract
The interdependence of community mobility and occupational engagement is a crucial component of wellness and prevention (American Occupational Therapy Association [AOTA], 2016a). Occupational engagement influences wellness by preventing the negative physical and psychological health effects of social isolation and limited mobility (Polgar, 2011; Stav, Hallenen, Lane, & Arbesman, 2012). Participating in community-based occupations, such as visiting family and friends, engaging in leisure pursuits, and attending places of worship, decreases risks by supporting social connectedness and access to the community (Al-Hassani & Alotaibi, 2014; Jacobs et al., 2008; Smith, 2012; Zunzunegui, Alvarado, Del Ser, & Otero, 2003).
Community mobility, an instrumental activity of daily living, has been defined as moving around the community, outside one’s home (AOTA, 2016a). Life expectancy exceeds driving ability; therefore, older adults must plan for community mobility and transportation needs as they cease driving (Silverstein, 2008; Stav, 2014). By 2050, the population of older adults will reach 83.7 million, making community mobility a national health priority (Ortman, Velkoff, & Hogan, 2014). A need exists for community-based programs to increase older adults’ knowledge of community mobility options and to aid in directing policy and resources to innovative programs that prevent disease and increase health and quality of life (QOL; AOTA, 2016b; DeGood, 2014; George & Berndt, 2015; U.S. Department of Health and Human Services, 2010). Let’s Go is one such program.
Mulry and Piersol (2014) described the Let’s Go program and its preliminary results. Let’s Go is rooted in the Person–Environment–Occupation–Performance (PEOP) Model, which addresses the fit between intrinsic personal factors and extrinsic environmental factors to facilitate successful occupational performance and participation and promote self-efficacy and confidence in community participation, leading to well-being and increased QOL (Baum & Christiansen, 2005). In Let’s Go, participants attend group and individual sessions and examine their PEOP fit. Participants identify desired community-based occupations and examine their physical and social environments and socioeconomic factors for supports and barriers to community mobility. Let’s Go demystifies alternative transportation; encourages its use; and facilitates practice through homework, an experiential component, and peer-supported trips. Resources are tailored to the needs of individuals in the groups, and one-on-one support and problem solving facilitate participation. This study examined whether the outcomes of an expanded implementation of Let’s Go supported participants’ community-based occupational engagement.
Method
A concurrent mixed-methods design combined a single-group pretest–posttest design and qualitative interviews that provided insight and meaning that could not be captured solely using standardized quantitative measures (DePoy & Gitlin, 2016). Participants were recruited from 1,131 residents of seven buildings housing older adults in urban areas of Mercer and Union Counties in New Jersey. After receiving approval from the institutional review board, on-site social services professionals promoted the program through fliers and held information sessions. Consistent with the inclusion criteria, participants were independent community-dwelling older adults without aphasia who were concerned about their community mobility and who engaged in functional mobility with or without an assistive device.
Let’s Go is a 4-wk multimodal education program; standardized facilitator and participant manuals were created to ensure fidelity in program delivery. The manuals were created by the first author, and all authors acted as facilitators. The first 3 wk consist of 45-min group education sessions followed by 15- to 30-min individual sessions. The three session topics are (1) benefits of and barriers to getting out into the community; (2) alternative community mobility options and funding, including a resource guide with local mobility options, funding, and community resources; and (3) community safety. In the 4th wk, participants attend an experiential group community outing. In addition, participants are encouraged to perform individually relevant occupations in the community as homework. Program outcomes were examined at baseline, 4 wk (program end), and 6 mo.
Outcome measures included subscales of the Impact on Participation and Autonomy Questionnaire (IPAQ), the Let’s Go Participant Survey, and semistructured interviews. The IPAQ, which measures a person’s perception of the impact of chronic disability on participation, has good responsiveness, and its content, construct, and discriminant validity and internal consistency have been deemed adequate and verified by Rasch analysis (Magasi & Post, 2010). Internal reliability of the IPAQ on all subscales is high (Cronbach’s αs >.80), and content validity of the Autonomy Outdoors (α = .81) and Social Life and Relationships (α = .86) scales is strong (Cardol, de Haan, de Jong, van den Bos, & de Groot, 2001).
The Let’s Go Participant Survey and semistructured interview questions were developed by the first author (Figure 1). The survey includes seven statements, rated using a 5-point Likert scale, that allow self-report of participation in community-based occupations, confidence in community mobility, sense of isolation, and frequency of community outings. Self-report scales have been cited as important for assessing health care issues in community-dwelling older adults (MacDermid & Michlovitz, 2008). The content validity of the survey was determined using cognitive testing (Collins, 2003). A paired t test was used to ascertain whether the program was effective at 4 wk, and a one-way analysis of variance (ANOVA) was used to test whether program outcomes were significant at 6 mo.
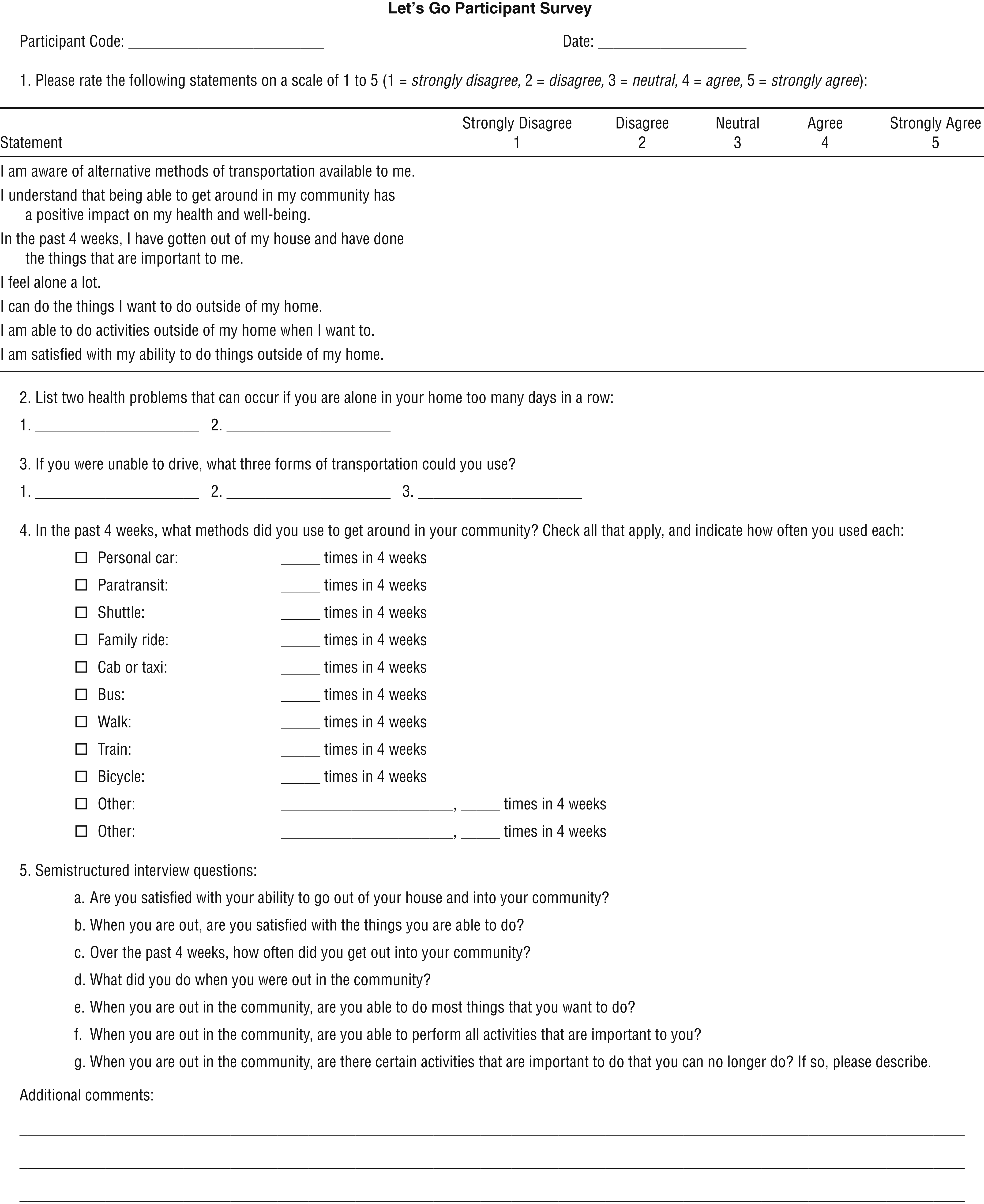
Let’s Go participant survey.
Using a phenomenological qualitative approach, all authors conducted semistructured interviews that were then transcribed and analyzed for themes. The authors evaluated each transcript; bins were created with categories, and common themes emerged. Field notes and an audit trail were kept. Member checks occurred at 6 mo.
Results
Of the 105 residents who attended the information sessions, 52 (13 men, 39 women) completed the 4-wk program; 41 (11 men, 30 women) participated in the 6-mo follow-up. Reasons for participant attrition included inability to commit to 4 consecutive weeks of programming, doctors’ appointments, family visits, and illness. Of the 11 participants not reached for the 6-mo follow-up, 5 had moved, 3 had disconnected phones, and 3 withdrew from the study citing scheduling conflicts.
Paired-samples t tests were used to evaluate differences in self-reported participation, confidence, isolation, and frequency of community trips and in IPAQ Autonomy Outdoors and Social Life and Relationships scores from baseline to program end (4 wk, N = 52). Significant differences were found for participation, t(51) = −2.9, p = .005, d = −0.41; confidence, t(51) = 1.1, p = 004, d = −4.2; frequency of trips, t(51) = −3.5, p = .001, d = 0.48; IPAQ Autonomy Outdoors, t(51) = 3.1, p = .003, d = 0.43; and IPAQ Social Life and Relationships, t(51) = 3.5, p = .001, d = 0.48. There was no significant difference in self-report of isolation, t(51) = −1.1, p = .296, d = 0.15.
A one-way repeated-measures ANOVA (n = 41) at 6 mo revealed significant differences for participation, F(2, 76) = 6.60, p = .001, and confidence, F(2, 82) = 7.12, p = .001. Participants reported increased frequency of community trips using any method of transportation, including walking, car, bus, train, bicycle, shuttle, and paratransit. Eighty-eight percent maintained or increased the frequency of their trips into the community at 4 wk, F(2, 80) = 5.51, p = .012. On the IPAQ, scores demonstrated significant improvement on both the Autonomy Outdoors, F(2, 80) = 9.06, p = .002, and Social Life and Relationships, F(2, 82) = 7.77, p = .005, scales. Self-reported feelings of isolation did not demonstrate a significant change, F(2, 82) = 0.06, p = .333. Although reports of decreased isolation did not reach significance, 80% of participants (n = 41) reported decreased feelings of isolation. Qualitative themes included decreased feelings of isolation, importance of peer and community support, increased knowledge of alternative mobility options and resources, and a shift from fear to confidence in community participation (Table 2).
Let’s Go Program Outcomes
Note. AO = Autonomy Outdoors scale; df = degrees of freedom; IPAQ = Impact of Participation and Autonomy; M = mean; SD = standard deviation; SLR = Social Life and Relationships scale.
p < .01. **p < .001.
Qualitative Themes and Examples
Note. T.R.A.D.E. refers to a paratransit program providing transportation for disadvantaged and older adults to medical appointments and for therapeutic and recreational trips.
Discussion
This study investigated outcomes of the Let’s Go program to see whether participants experienced changes in community mobility–related outcomes over time. Participants demonstrated significant improvements in participation in community-based occupations, confidence in community mobility, and frequency of community outings. Their perception of their autonomy outdoors and satisfaction with social life and relationships also improved. These findings echo those of Johansson and Björklund (2016), who found that occupation-based interventions improved older adults’ well-being. Community participation allows for spiritual engagement in faith communities, leisure pursuits, social participation, and role fulfillment, all of which increase QOL and wellness.
The group and individual sessions explored participants’ intrinsic motivators and capabilities for community mobility and analyzed them in relation to their environmental supports and barriers. This collaborative problem solving enabled participants to generate solutions and build confidence in their ability to engage in community mobility. Let’s Go used small group learning similar to that used in the Well Elderly Study (Clark et al., 2011). The group format allowed participants to motivate and support each other to try new methods of transportation. Individualization of treatment enabled participants to address their individual needs.
Community mobility programming has the potential to promote wellness in older adults through increases not only in community trips but also in role performance, social participation, confidence and, ultimately, QOL. The Centers for Disease Control and Prevention (2015) emphasized the importance of community participation for wellness and QOL. Participants in this study demonstrated that experiential learning helps build confidence and increases the frequency of community trips; likewise, Jacobs et al. (2008) examined the health, functional, and psychosocial status of 323 ambulatory community-dwelling older adults and found functional loss in participants who ventured into their communities less frequently.
Qualitative themes identified included decreased feelings of isolation, increased recognition of peer and community support, increased knowledge of alternative mobility options and resources, and a shift from fear to confidence in community participation (see Table 2). During the interviews, participants reported experiencing decreased feelings of isolation; the group meetings may have helped them recognize that their fellow residents faced similar issues. The small group sessions allowed participants to meet neighbors and build relationships. Participants did their Let’s Go homework—going out in the community—together; this practice of newly acquired skills in a group may explain why IPAQ Social Life and Relationships scores improved. During the experiential trip, participants were able to use peer and community supports to meet their community participation and social participation goals. Participants had been unaware of alternative transportation, community resources, and funding options available to them and were grateful for the knowledge and the customized community transportation manual issued to them in Session 2.
The increase in community participation was evidenced by the increase in community trips. Community mobility training may have a positive psychosocial impact by supporting social life and relationships. Holt-Lunstad, Smith, and Layton (2010) found the effect of social participation on wellness to be as significant as the effects of exercise, diet, smoking, and drinking. Participants’ increased knowledge of resources and recognition of peer and community support may have facilitated the decrease in fear and shift to confidence in community mobility. Clemson and colleagues (2004) found that learning in community-based small groups decreased fear of falling and subsequent falls; it is possible that the Let’s Go small groups had a similar effect on fear of community mobility and community participation.
To be well, all people have a right to participate in community-based occupations. Solutions that decrease barriers to participation are needed (Polgar, 2011). Payers do not typically fund community mobility training and participation initiatives. It is imperative that as interprofessional teams create wellness and prevention programs for older adults that garner attention and funding, community mobility programs be included.
Limitations
The small sample size, lack of a control group, and urban setting limit the generalizability of these results. The fact that the researchers delivered the program may have biased the results; the use of blinding may strengthen future results. Also, participation and wellness are multifaceted experiences of which community mobility is but one facet. Future studies should control for multiple variables and explore the impact of community mobility and participation on wellness outcomes. Additionally, although the study demonstrated an increase in community participation and confidence, none of the participation outcomes specifically explored QOL.
Implications for Occupational Therapy Practice
This study confirmed Johansson and Björklund’s (2016) finding that occupation-based health programming can help people maintain or improve community participation. It also illustrates that occupational therapy practitioners can design and implement community programming to meet the needs of marginalized older adults. In addition, it shows that occupation-based community mobility programming can promote outdoor autonomy and social life and relationships, reduce isolation, and increase confidence in and frequency of community participation. Future studies should explore other regions and populations beyond low-income urban-dwelling older adults.
The results of this study have the following implications for occupational therapy practice:
Occupation-based community mobility programs may have a preventative effect on health problems by improving community participation and wellness.
The Let’s Go program can make a significant difference in community mobility–related participation, confidence, isolation, autonomy, and social life for older adults.
Community mobility extends beyond the physical ability to engage in outdoor functional mobility and improves social participation, decreases isolation, and fortifies mental health and therefore wellness.
There is a growing need for occupational therapy practitioners to incorporate community mobility goals, resources, and programming at all levels of care.
Prevention and wellness programs should consider all aspects of participants’ health, including their community participation needs.
Social and community participation have an important impact on health and should be addressed at all levels of care.
Footnotes
Acknowledgments
This study is registered at ![]() (NCT02916758). We thank Kean University and the Kean University Foundation for support of the Let’s Go project through Students Partnering With Faculty and Foundation Faculty Research Awards. Let’s Go and its student researchers were invited to the Clinton Global Initiative University (CGIU) meeting in 2016 and thank CGIU and Kean University for the opportunity. We thank Holly Hardaway at Independent Domain, LLC; Eileen Doremus; and Ann Ferguson for their support and commitment to facilitating wellness for older adults.
(NCT02916758). We thank Kean University and the Kean University Foundation for support of the Let’s Go project through Students Partnering With Faculty and Foundation Faculty Research Awards. Let’s Go and its student researchers were invited to the Clinton Global Initiative University (CGIU) meeting in 2016 and thank CGIU and Kean University for the opportunity. We thank Holly Hardaway at Independent Domain, LLC; Eileen Doremus; and Ann Ferguson for their support and commitment to facilitating wellness for older adults.